a case of right-sided obstructed hemivagina ipsilateral … · incompetence2 and a rare case of a...
TRANSCRIPT
A Case of Right-sided Obstructed Hemivagina Ipsilateral Renal
Agenesis (OHVIRA).
* Obstructed hemivagina ipsilateral renal agenesis (OHVIRA) is a rare form of mullerian duct anomaly.
* A number of presentations have been reported including pre-pubertal with urinary incontinence1, adolescence with dysmenorrhoea, difficulty with sexual intercourse or using a tampon, as well as delayed diagnosis in pregnancy due to cervical incompetence2 and a rare case of a ruptured gravid uterus3.
* Pre-operative imaging with MRI is essential to define the mullerian duct structures and renal tract4.
* Surgery is ideally a single procedure with drainage of the obstructed hemivagina and resection of the septum to restore normal vaginal function 5,6 .
* A 17-year-old female presented with a 6-month history of offensive vaginal discharge. She had previously achieved coitarche and used tampons with little concern.
* Examination demonstrated a bulge in the right upper vagina.
* USS findings were suspicious for right-sided renal agenesis and uterus didelphis.
* A subsequent MRI demonstrated the classical findings of right-sided OHVIRA. She had uterus didelphis (Fig1b), bicolis and a right sided obstructed hemivagina (Fig 1a).
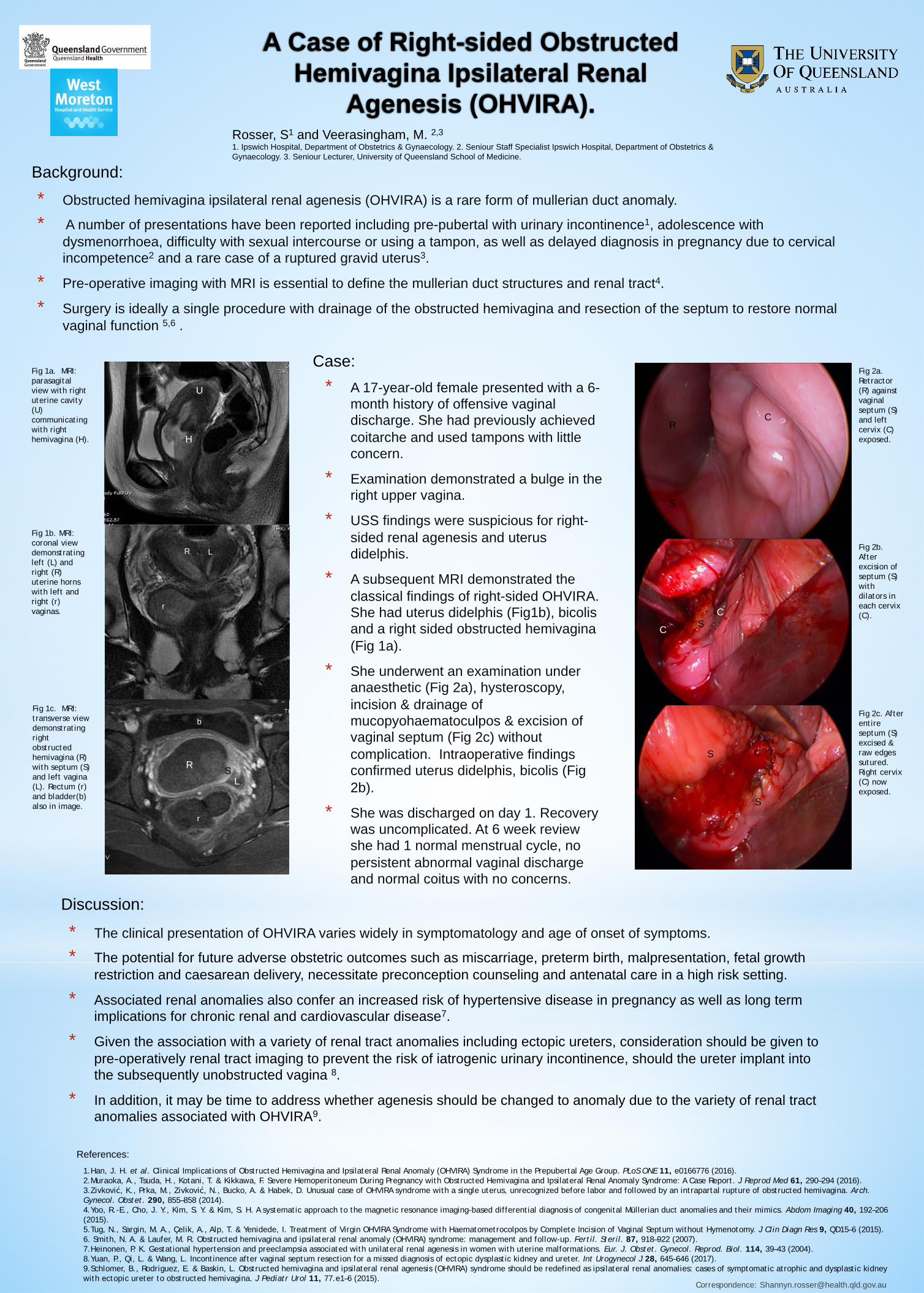
* She underwent an examination under anaesthetic (Fig 2a), hysteroscopy, incision & drainage of mucopyohaematoculpos & excision of vaginal septum (Fig 2c) without complication. Intraoperative findings confirmed uterus didelphis, bicolis (Fig 2b).
* She was discharged on day 1. Recovery was uncomplicated. At 6 week review she had 1 normal menstrual cycle, no persistent abnormal vaginal discharge and normal coitus with no concerns.
* The clinical presentation of OHVIRA varies widely in symptomatology and age of onset of symptoms.
* The potential for future adverse obstetric outcomes such as miscarriage, preterm birth, malpresentation, fetal growth restriction and caesarean delivery, necessitate preconception counseling and antenatal care in a high risk setting.
* Associated renal anomalies also confer an increased risk of hypertensive disease in pregnancy as well as long term implications for chronic renal and cardiovascular disease7.
* Given the association with a variety of renal tract anomalies including ectopic ureters, consideration should be given to pre-operatively renal tract imaging to prevent the risk of iatrogenic urinary incontinence, should the ureter implant into the subsequently unobstructed vagina 8.
* In addition, it may be time to address whether agenesis should be changed to anomaly due to the variety of renal tract anomalies associated with OHVIRA9.
1.Han, J. H. et al. Clinical Implications of Obstructed Hemivagina and Ipsilateral Renal Anomaly (OHVIRA) Syndrome in the Prepubertal Age Group. PLoS ONE 11, e0166776 (2016). 2.Muraoka, A., Tsuda, H., Kotani, T. & Kikkawa, F. Severe Hemoperitoneum During Pregnancy with Obstructed Hemivagina and Ipsilateral Renal Anomaly Syndrome: A Case Report. J Reprod Med 61, 290–294 (2016). 3.Zivković, K., Prka, M., Zivković, N., Bucko, A. & Habek, D. Unusual case of OHVIRA syndrome with a single uterus, unrecognized before labor and followed by an intrapartal rupture of obstructed hemivagina. Arch. Gynecol. Obstet. 290, 855–858 (2014). 4.Yoo, R.-E., Cho, J. Y., Kim, S. Y. & Kim, S. H. A systematic approach to the magnetic resonance imaging-based differential diagnosis of congenital Müllerian duct anomalies and their mimics. Abdom Imaging 40, 192–206 (2015). 5.Tug, N., Sargin, M. A., Çelik, A., Alp, T. & Yenidede, I. Treatment of Virgin OHVIRA Syndrome with Haematometrocolpos by Complete Incision of Vaginal Septum without Hymenotomy. J Clin Diagn Res 9, QD15–6 (2015). 6. Smith, N. A. & Laufer, M. R. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: management and follow-up. Fertil. Steril. 87, 918–922 (2007). 7.Heinonen, P. K. Gestational hypertension and preeclampsia associated with unilateral renal agenesis in women with uterine malformations. Eur. J. Obstet. Gynecol. Reprod. Biol. 114, 39–43 (2004). 8.Yuan, P., Qi, L. & Wang, L. Incontinence after vaginal septum resection for a missed diagnosis of ectopic dysplastic kidney and ureter. Int Urogynecol J 28, 645–646 (2017). 9.Schlomer, B., Rodriguez, E. & Baskin, L. Obstructed hemivagina and ipsilateral renal agenesis (OHVIRA) syndrome should be redefined as ipsilateral renal anomalies: cases of symptomatic atrophic and dysplastic kidney with ectopic ureter to obstructed hemivagina. J Pediatr Urol 11, 77.e1–6 (2015).
Background:
Case:
Discussion:
References:
Rosser, S1 and Veerasingham, M. 2,3 1. Ipswich Hospital, Department of Obstetrics & Gynaecology. 2. Seniour Staff Specialist Ipswich Hospital, Department of Obstetrics & Gynaecology. 3. Seniour Lecturer, University of Queensland School of Medicine.
Correspondence: [email protected]
Fig 2a. Retractor (R) against vaginal septum (S) and left cervix (C) exposed.
Fig 2b. After excision of septum (S) with dilators in each cervix (C).
Fig 2c. After entire septum (S) excised & raw edges sutured. Right cervix (C) now exposed.
R
S
C
S C
C
S
S
Fig 1a. MRI: parasagital view with right uterine cavity (U) communicating with right hemivagina (H).
Fig 1b. MRI: coronal view demonstrating left (L) and right (R) uterine horns with left and right (r) vaginas.
Fig 1c. MRI: transverse view demonstrating right obstructed hemivagina (R) with septum (S) and left vagina (L). Rectum (r) and bladder(b) also in image.
U
H
R S
L
r
R L
C
r
b