a clinical comparative study to evaluate the efficacy …
TRANSCRIPT

I
RAJIV GANDHIUNIVERSITY OF HEALTH SCIENCES,
BANGALORE, KARNATAKA.
“A CLINICAL COMPARATIVE STUDY TO EVALUATE
THE EFFICACY OF MRUDU VIRECHANA AND
SHAMANA CHIKITSA IN THE MANAGEMENT OF
AMLAPITTA”
The Dissertation submitted to the
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka
In partial fulfillment of requirements for the award of the degree of
DOCTOR OF MEDICINE (AYURVEDA)
In the speciality of
KAYA CHIKITSA
By
Dr.ASHISH KUMAR DUBEY B.A.M.S.
Guide
Dr.ARCHANA.C.P.M.D. (Ayu) Reader
Department of Post Graduate Studies in Kaya Chikitsa,
Ayurvedic Medical College &P.G. Centre, Davangere
Co-guide
Dr. GNANESWARA. L.M. M.D.(Ayu) Reader
Department of Panchakarma,
Ayurvedic Medical College &P.G. Centre, Davangere
DEPARTMENT OF POST GRADUATE STUDIES IN
KAYA CHIKITSA
AYURVEDIC MEDICAL COLLEGE AND P.G. CENTRE
DAVANGERE-577006
2012-2013

II
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka.
DECLARATION BY THE CANDIDATE
I hereby declare that this dissertation entitled “A CLINICAL
COMPARATIVE STUDY TO EVALUATE THE EFFICACY OF MRUDU
VIRECHANA AND SHAMANA CHIKITSA IN THE MANAGEMENT OF
AMLAPITTA” is a bonafide and genuine research work carried out by me under the
guidance of Dr .Archana.C.P. M.D. (Kayachikitsa) Guide & Reader, Dept. of P.G.
Studies in Kayachikitsa, Ayurvedic Medical College & P.G. Center, Davangere.
Date:
Place: Dr. ASHISH KUMAR DUBEY

III
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka.
CERTIFICATE BY THE GUIDE
This to certify that this dissertation entitled “A CLINICAL
COMPARATIVE STUDY TO EVALUATE THE EFFICACY OF MRUDU
VIRECHANA AND SHAMANA CHIKITSA IN THE MANAGEMENT OF
AMLAPITTA” is a bonafide and genuine research work done by Dr. ASHISH
KUMAR DUBEYIn partial fulfillment of the requirement for the degree of
Doctor of Medicine (Ayurveda) in the specialty of Kayachikitsa under my direct
guidance.
Dr.Archana.C.P.. M.D. (Ay).
Guide & Reader
P.G. Department of Kayachikitsa
Date: AyurvedicMedicalCollege&
P.G.Center,
Place: Davangere.

IV
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka.
CERTIFICATE BY THE CO-GUIDE
This to certify that this dissertation entitled “A CLINICAL
COMPARATIVE STUDY TO EVALUATE THE EFFICACY OF MRUDU
VIRECHANA AND SHAMANA CHIKITSA IN THE MANAGEMENT OF
AMLAAPITTA ” is a bonafide and genuine research work done by Dr.
ASHISH KUMAR DUBEY in partial fulfillment of the requirement for the
degree of Doctor of Medicine (Ayurveda) in the specialty of Kaya Chikitsa
under my supervision.
Dr.GNANESWARA L.M ,M.D. (Ay).
Co-Guide & Reader,
Department of Panchakarma
Date: AyurvedicMedicalCollege&
P.G.Center,
Place: Davangere Davangere.

V
Rajiv Gandhi University of Health Sciences, Bangalore, Karnataka.
ENDORSEMENT BY THE HOD, PRINCIPAL/
HEAD OF THE INSTITUTE
This to certify that this dissertation entitled “ A CLINICAL
COMPARATIVE STUDY TO EVALUATE THE EFFICACY OF MRUDU
VIRECHANA AND SHAMANA CHIKITSA IN THE MANAGEMENT OF
AMLAPITTA” is a bonafide and genuine research work done by Dr. ASHISH
KUMAR DUBEYunder the guidance of Dr.Archana.C.P..M.D. (Ayu), H.O.D.&
Reader, Post Graduation Dept. of Kayachikitsa, Ayurvedic Medical College & P.G.
Center, Davangere.
Dr. Jayanthi.C.M.D. (Ayu) Dr.S.Dayananda ,M.D. (Ayu)
H.O.D. & Reader. Principal & Professor,
PG. Dept. of Kayachikitsa, PG. Dept. of Kayachikitsa,
Ayurvedic Medical College & Ayurvedic Medical College &
P.G. Center, P.G. Center,
Davangere. Davangere.
Date: Date:
Place: Place:

VI
COPYRIGHT
DECLARATION BY THE CANDIDATE
I hereby declare that the Rajiv Gandhi University of Health Sciences,
Karnataka shall have the rights to preserve, use and disseminate this dissertation /
thesis in print or electronic format for academic / research purpose.
Date :
Place : Dr. ASHISH KUMAR DUBEY

VII
ACKNOWLEGEMENT
While penning the acknowledgement of the present work, I remember the
moments when I needed someone desperately to come upon for the help. It was the
GODDESS SARASVATI who always transformed strengths in me tout-class every
that nasty things.
I prostrate to the feet of Goddess Sarasvati for standing behind me in every
hurdle of life. It’s beyond the reach of any language to express the pure, warm, sweet
and bright flame of gratefulness to my loving parents Shri. Ramnaresh Dubey and
Smt. Shudha Dubey and my sister Puja and my brothr Punit, Naveen, Abhishek
and my bhabi Priyank Dubey whose love, support and encouragement were the
initiating sources in each and every step of my life.
I express my deepest sense of gratitutde with all humbleness
toDr.Dayananda.SPrincipal andDr.Bharthi .D.A. Incharge Principal of Ayurvedic
Medical college and P.G.Centre.Davan gere.
I owe an irredeemable debt of gratitude to affectionate, intelligent, enthusiastic
and helpful guide Reader. DrArchana.C.P ., who guided each and every aspect of
this study.
Heartiest thanks to respected Dr. Gnaneswara L.M, my co-guide for his
most valuable suggestions and pruning which has shaped this work to a great extent.
I express my deepest sense of gratitutde with all humbleness to Dr.Jayanthi.C
, HOD and Professor P.G. Department of Kayachikitsa, A.M.C and P.G. Centre.
At this juncture I heartily thanks to Dr.Muktha M.H, Dr. Pradeep J.M,
Dr.Rudresh.,Dr.SriHarsha,Dr.Manthesh.,Dr.HarshaMurthyof Kayachikitsa
Department as well as Dr. Bharathi D.A, Dr. Usha Rani.S,Dr.Srikanththe teachers
of this institute for enriching me with their unconfined knowledge during my Post
Graduation.
I am very much thankful to Our College Founders and Management Members
of Ashwini Educational Association, Dr.M.N.Hiremath, Dr.Suresh.V. Ambedkar,
Dr.G.B.Ravindranath, Dr.N.R.SankarNarayan, Dr.K.G.Chandrappa and for
giving me an Opportunity to study in this college.

VIII
I also express my gratitude to Dr. Raaju.U.Rfor his kind guidance and
encouragement throughout the work.
I would like to express a lot of thanks to my beloved friends Dr. Manoj,
Dr.Vinay, Dr. Mumtaj, Dr Shyama, Dr. Sandeep, Dr. Sandesh, Dr.Parvaty, Dr.
Dipti,Dr.veresh for their support and helful nature in my studies.
I am thankful to my department seniors. Dr. Rekha, Dr. Lohit, Dr. Lokesh,
Dr. Mukesh, for their timely help.
I also thankful to Dr.Sangam for helping me in doing statistical work
I also thank Mr. G.P. Sanjeev Kumar of M/s Gundal Computer Center for
the meticulous computerized laser typing and styling of this dissertation work.
I also pay thanks to all those kind people who delivered their support directly
and indirectly to accomplish the work. At last, I seek pardon and apologize for any
errors which might be remained in the work.
Date :
Place : Dr. ASHISH KUMAR DUBEY

IX
ABBREVIATIONS
A. H. - Ashtanga Hridaya
A. S. - Ashtanga Sangraha
B.P. – Bhavaprakasha
B.R. – Bhaishajya Ratnavali
Bh. - Bhela Samhita
Ch. - Charaka Samhita
Chakra. - Chakrapani
Chi. - Chikitsasthana
Dal. - Dalhana
GN - Gadnigraha
Ha. Sam. - Harita Samhita
Ka. - Kashyapa Samhita
M. N. - Madhava Nidana
Ni. - Nidanasthana
Pu. - Purva Khanda
Sha. - Sharangadhara
Si. - Siddhisthana
Su. - Sushruta Samhita
Su. - Sutrasthana
Ut. – Uttartantra
V.S.-Vanga Sena
Vi. - Vimanasthana
Y. R. - Yogaratnakara

X
ABSTRACT
Objectives : To review the literature on Amlapitta to asses the effect of Yasti
madhu churna with Sootashekara vati. To asses the effect of Sootashekara vati.To
intercompare the results of both groups.
Methods : Cases presenting with classical signs and symptoms of amlapitta
were selected. They are randomly allocated in two groups in groupA Yastimadhu
churna with Sootashekara vati and in groupB Sootashekara vatiwas given. The signs
and symptoms of Amlapitta like Aruchi, Avipak, Utklesh, Amloudgar,
Hridahakanthdaha were assessed before, during and after the completion of treatment
Analysis of the overall effects in Group A indicate that 40% of patients
showed major improvement of the illness, 35% of patients showed moderate
improvement where as other 20% of patient showed minor improvement. And 5% of
patients Not improved.
Similarly analysis of the overall effect in the Group B indicate that 30% of
patient showed major improvement of the illness, 35% of patient showed moderate
improvement, where as, 25% of patients showed minor improvement, and 10 % of
patients showed Not improved .
Conclusion : Group A cases showed better improvement out of 40 cases as compared
to Group B.
Key Words - Amlapitta , Mrudu Virechana , Shamana chikitsa , Yastimadhu
Churna , Sootashekara rasa vati.

XI
TABLE OF CONTENTS
Sl.
No. Chapter Name Page No.
1. INTRODUCTION 1-2
2. OBJECTIVES 3
3. REVIEW OF LITERATURE 4-56
4. METHODOLOGY 57- 62
5. OBSERVATION & RESULTS 63 -95
6. DISCUSSION 96 -105
7. CONCLUSION 106
8. SUMMARY 107 -108
9. LIST OF REFERENCES 109-112
10. BIBLIOGRAPHY 113 -114
11. ANNEXURES 115 -122

XII
LIST OF TABLES
Sl.
No. Title
Page
No.
1. The Classical Nidana of Amlapitta 11 -12
2. Showing Roopa of Amlapitta 19 -27
3. Ingredients of Yastimadhu churna 53
4. Ingredients of sootasekar vati 54 -55
5. Distribution of patients according to age group 64
6 Distribution of patients with respect to Sex 65
7 Distribution of patients according to religion 66
8. Distribution of patients according to Education 67
9. Distribution of patients according to Socio – Economic Status 68
10. Distribution of patients according to their Maritial status 69
11. Distribution of patients according to their nature of work 70
12. Distribution of patients according to Manasika Sthithi 71
13. Distribution of patients according to vyasana 72
14. Distribution of patients according to type of Prakruti 73
15. Distribution of patients according to Sara 74
16. Distribution of patients according to Samhanana 75
17. Distribution of patients according to Satva 76
18. Distribution of patients according to Satmya 77
19. Distribution of patients according to Kostha 78
20. Distribution of patients according to Vyayama Shakti 79
21. Distribution of patients according to occupation 80
22. Distribution of patients intake of predominant rasa 82
23. Distribution of patient intake of water 82

XIII
24. Distribution of patients of duration of symptoms 83
25. Didtribution of patients of most of onset of Amlapitta 83
26. Distribution of patients based on Relieving factor 84
27. Showing the effect on Aruchi in group A 84
28. Showing the effect on Aruchi in Group B 85
30. Showing the effect on Avipak in group A 86
31. Showing the effect on Avipak in Group B 86
32. Showing the effect on Utklesh in group A 87
33. Showing the effect on Utklesh in Group B 87
34. Showing the effect on Amloudgar in group A 88
35. Showing the effect on Amloudgar in Group B 88
36. Showing the effect on Hridkanthdaha in group A 89
37. Showing the effect on Hridkanthdaha in Group B 89
38. Comparision of effect of treatment on Aruchi in two groups 90
39. Comparision of effect of treatment on Avipak in two groups 91
40. Comparision of effect of treatment on Utklesh in two groups 92
41. Comparision of effect of treatment on Amloudgar in two groups 93
42. Comparision of effect of treatment on Hridkanthdaha in two groups 94
43. Overall Assessment of each therapy. 95

XIV
LIST OF FIGURES
Sl.
No. Title
Page
No.
1. Schematic representation of Samprapti of Amlapitta 29
2. Showing Yastimadhu Churna 56
3. Showing Sootashekar rasa vati 56

XV
LIST OF GRAPHS
Sl.
No. Title
Page
No.
1. Distribution of patients according to Age group 64
2. Distribution of patients according to Sex 65
3. Distribution of patients according to Religion 66
4. Distribution of patients according to Education 67
5. Distribution of patients according to Socio-Economic Status 68
6. Distribution of patients according to Marital Status 69
7. Distribution of patients according to nature of work 70
8. Distribution of patients according to Manasika Sthithi 71
9. Distribution of patients according to Vyasana 72
10. Distribution of patients according to Type of Prakruti 73
11. Distribution of patients according to Sara 74
12. Distribution of patients according to Samhanana 75
13. Distribution of patients according to Satva 76
14. Distribution of patients according to Satmya 77
15. Distribution of patients according to Kostha 78
.16 Distribution of patients according to Vyayama Shakti 79
17. Distribution of patients according to occupation 80
23. Comparision of effect of treatment on Aruchi in two groups 90
24 Comparision of effect of treatment on Avipaka in two groups 91
25. Comparision of effect of treatment on Utklesh in two groups 92
26. Comparision of effect of treatment on Amloudgar in two groups 93
27. Comparision of effect of treatment on HridKanthadaha in two
groups 94
28. Graph showing overall assessment of each therapy. 95

Introduction
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 1
INTRODUCTION
Amlapitta is a Annavaha and Purishavaha srotas disorder. These srotas are the
basis for the very subsistence of life.Amalapitta is a very common dietary disorder in
india. It is increasing now a days due fasting, eating between meals, worry, hurry,
spicy foods , change in life-style, strain, drugs, etc. This can derange the digestive
procedures. Amlapitta is such pathological condition or disease in which the pitta
exteeds in normal level. Due to above said foctors Amlaguna of Pitta increases
which leads to Vidagdhata of ingested food and finally Amlodgara, Urovidaha,
Chhardi etc., signs and symptoms of Amlapitta are evident clinically.It is very
difficult to correlate Amlapitta with a single disease of Modern science But due to the
similarity in causative factors and signs and symptoms one can correlate this disease
to Hyperacidity, Dyspepsia and Gastritis.
1.1 NEED AND SIGNIFICANCE
Amlapitta has high incidence through out the world, which affects almost
45% people in our country .Person fell constant discomfort though out the day. It
predisposes to an overall reduction in the physical activities of the person in its
chronic course. Though Amlapitta is not a life threatening, if left untreated or
neglected, it may invite major life threatening problem.
The ‘Amlapitta’ is composed of word Amla and Pitta. The term Amla has
been used as an epithet to Pitta. Amlapitta is a condition where excessive secretion of
Amla Guna Pitta takes place causing vidahyadi conditions. This causes various
pathophysiological conditions of Anna and Purishavaha Srotasa, such as of Avipaka,
Klama, Utklesha, Amlodgara, Gaurava, Hrit-Kantha-Daha, Aruchi , etc.
In Modern science the Hyperacidity, Dyspepsia and gastritis is managed
by Antacids, Proton pump inhibitor etc .Which are having own adverse
effects of long term such as constipation, diarrhea, skin rash, headache etc. By
virtue of all the above factors, it warrants prompt attention to find out a treatment
which is safer, effective, affordable for long duration use.

Introduction
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 2
It is well documented in classics that our contemporary Ayurvedic
practitioner treat Amlapitta confidently and give comfort to individual.In Ayurveda,
the administration of the vamana, virechana, basthi, rathamookshana and shamana is
theline of treatment are told for Amlapitta. The virechana is best therapy, where pitta
is manily vitiatied. The virechana is advised for management of Amalapitta. Here an
attempt is made to analyse the therapeutic efficacy of mrudu virechana and shamana
oushadhi-sootashekara rasa vati
Sootashekara rasa vati is one of the herbominaral combination, explained in the
Yogaranthanakara.
1.2 STATEMENT OF PROBLEM
“A Clinical Comparative study to evaluate the efficacy of
mruduvirechana and shaman chikitsa in the management of Amlapitta”
This clinical study is sincerely effort to analyse the therapeutic efficacy
of Mruduvirechana and shaman oushadhi . With this hope, the present work is
carried out. It is also hoped that this work will give a idea to choice the better therapy
for management task Amlapitta, with this noble intention this work is presented.
1.3 DELIMITATION: the study is limited to
Patients in and around Davangere , who have attended OPD , AMCH
Davagere .
Patients age group is between 15- 60 years .
The duration of study was 37 days . The assessment of result is made
on the base of clinical and functional improvements for the clinical
assessment all sign and symptoms .

Objectives
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 3
OBJECTIVES
Literary work on Amlapitta.
To Evaluate the effect of Group A Mruduvirechana.
To Evaluate the effect of Group B Shaman Oushadhi.
To Compare the efficacy of both group in Amlapitta.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 4
DISEASE REVIEW
Historical Review :-
The Entire Core Of The Universe Is Enlightened, In Its True Form, By The
Lamp Of History, The Destroyer Of The Veil Of Ignorance1
The above statement depicts the need for the historical review of the subject
matter.To have a complete knowledge of subject, it is necessary to trace out
itshistorical background.
Vedic Kala :-
No reference found in the Vedas.
SAMHITA KALA :
Charaka Samhita :In Ch Sam. Amlapitta is not mentioned as a separate entity but
the word is discussed at several places like.
While explaining about qualities of dugdha, it has been mentioned as a pathya
in pandu roga, amlapitta etc., diseases2
Kulattha has been considered as chief nidana of Amlapitta3.
The excessive use of Lavana Rasa causes Amlapitta4
Amlapita has been included in the listed of diseases caused by Viruddhahara5
Rajmashes has the property of relieving the amlapitta6
Mahatikta Ghrita has be indicated in amlapitta7
While describing Grahani Dosha, pathogenesis of amlapitta has bee clearly
mentioned8
The list of Paittika Natmaja Vyadi includes Dhumaka, Amlaka, Vidaha which
are the symptoms of Amlapitta9
Indication of Kansaharitaki also includes Amlapitta10
A clear-cut, Samprapti of this disease is available, "Kulattha", Lavana Rasa
and Viruddhahaa were listed as the causes of Amlapitta where as Mahatikta ghrita and

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 5
Kansaharitaki are prescribed for its treatment. Hence, it can be concluded that
duringthe period of Caraka all aspects of Amlapitta disease were considered.
Sushruta Samhita (1000 BC) :Sushruta while describing the disease caused due to
excessive use of Lavana has mentioned a disease Amlika which is similar to
Amlapitta.
Kasyapa Samhita :Kasyapa Samhita is the first available text where Amlapitta has
been mentioned as a separate entity. Not only vivid description of Amlapitta with its
treatment has bee mentioned in it, but suggestion to change them lace for peace of
mind in case where medicine does not work out has also given.
Harita Samhita :Ha. Sa. in has described as a separate disease and given the
treatment.11 He has also given aspecial symptoms Amla Hhikka (Hicough with sour
taste).
Madhav Nidana (7th century AD) :After Kasyapa, Madhava Nidana is the first
available text which gives importance to Amlapitta and described its nidana, roopa
and samprati in details along with two clinical subtypes i.e. Urdhvaga and Adhoga
Amlapitta.
Vrinda Madhava :Vrinda Madhava has described Amlapitta is an independent
disease and also its chithasa explained.
Chakradutta (11th Century AD) :In this classics, Vamana, Virechana, Basti etc
chikitsa are advised for Amlapitta along with its Chikitsa Sutra.
Basavarjiyam : In text in the chapter of Namatmaja yadhi, has included Amlapitta in
the 24 namatmaya vikaras of pitta.
Among the other symptoms svarahinala Jivna and Vak paridaha has been
attributed to Amlapitta which has not been mentioned by any other texts.
Sarangadhar Samhita :Sha.Sa. being a book of pharmacopea has given only
Amlapittahara recipes without describing the aetiopathological concepts of the
disease.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 6
Bhavaprakasha (16th cen. AD) :Two separate chapters on Amlapitta has been
devoted in this text. Upadrava and arista are explained in this text.
Yogaratnakara (17th AD) :This text has added four more Upadravas to the list of
Upadravas of Amlapitta.
Siddhanta Nidana :Here the Upadravas regarding Amlapitta from different classics
can be seen.
Bhaisajya Ratnavalli :Seven new mineral formulations have been added to the
existing formulation starting from Bhaskaramrutabhrakam to Sitamanduram. Two
palatable formulations have been mentioned by the author Govindadas Viz
Amlapittantaka modaka and Saubhagya Shunti Modaka, one of the taila added is
Sribilva Taila.
Previous Work done:
1. The study effect of Eladi choorna in Amlapitta –Mrs Sudhaka P -1995 –
HYDERABAD
2. The study of effect of Lakshadi Guggulu on the treatment of Amlapitta-Mrs Rao
Bhoswanth-1996-HYDERABAD.
3. A Clinical study of Amlaki Kvatha –bhavita shankha bhasma in the patient of
Amlapitta-Mrs Ravikumar T-2001-Lucknow.
4. A clinical study of indigenous composed on Amlapitta –Mrs Shivastava -1999-
Lucknow.
5. Amlapitta Ka Nidana Samprapti – paraka evam Upashyatmaka Adhyayana
Avipattikar choorna evam Kaparda Bhasma Ke pariprekshya mein –Mrs Rawate
R – 1997—Jaipur .

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 7
DISEASE REVIEW
NIRUKTI
Etymologically the word “Amlapitta” comprises of two components ‘Amla’
and ‘Pitta’.
Amla is derived as ‘Amyatya amlaha’. From the dhatu ‘Am’ meaning to be ill
or be afflicted or diseased.
The word amla has commonly been used to express one of the six kinds of
taste. In this present context the meaning of amla can be taken as one of the properties
of pitta.12
The second component the word pitta is derived from the dhatu ‘Tap’ i.e. to eat
or to burn or to warm. These terms seems to have three meanings, i.e. tap santapae,
tap dahe and tap aishvarya.
1. Tap santapae: it refers to the generation of heat.
2. Tap dahae: it refers to the act of burning of nutrition, which is consumed.
3. Tape aishvarya: it refers to those factors, which are responsible to make one
achieve the eight kinds of benefits.
These references are obtained from Bhattaji’s “Sidhanta Koumudi” and the
words furnish the vyakarana version of the term pitta. In this present context, if from
the word amla we take its meaning as diseased, then etymologically Amlapitta may be
diseased state of pitta.13
Paribhasha:
Chakrapanidatta in his commentary on Charaka Samhita defines Amlapitta
as
“Amlapittam cheti amlagunoudriktam pittam”14
Here pitta, which is acquiring more amla guna, is called as Amlapitta.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 8
Srikantadatta in his Madhukosha vyakya defines
“ Vidahadhyamla gunoudrikta pittam amlapittam”15
That is, the pitta becomes augmented or vidagdha because of excessive
increase of amla guna of pitta.
“Amlam vidagdam cha tat pittam amlapittam”16
The pitta, which attains amla guna and vidagdhata, is called as Amlapitta.
Apart from the above there are some definition of Amlapitta, they are:
Kashyapa explains in Kashyapa Samhita khila sthana that the vidagdha
anna rasa terns to Shukta, this Shukta anna rasa is retained in amashaya and
produces Amlapitta.
Another by Madhava Nidana, the Amlapitta is that condition where the
pitta which has previously accumulated from the self aggravating causes gets
vidagdha due to virudha, dustha, amla, vidahi and pitta provocating foods
and drinks.17
These two definitions to a certain extent would speak of Nidana and Samprapti
of the disease.
By these definitions we come to know that Amlapitta is an abnormal physiological
condition of pitta. In this condition the amla guna of pitta is augmented and its
functions are altered. Hence there will be a loss of doshic equilibrium and digestion
process is affected. This results in Shukta paka and production of ama. This condition
exhibits typical clinical presentation known as Amlapitta.
Paryaya:
The paryayas of Amlapitta signify different aspect of it. Indu in his
commentary of Astanga Sangraha, has given synonyms of Amlapitta as

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 9
1. Prameelaka: The pachyamana vidagdha anna rasa immediately provokes pittadi
dosha, there by producing mukha vairasya, hritshula, sadana, continuous lavana
tiktamla Chardi, burning sensation, excessive sleep, constipation, restlessness,
and watering of the mouth. This state where all these symptoms are stated is
spoken of as prameelaka. In Astanga Sangraha we find this term under kaphaja
vyadhis.18
2. Amlapitta: The implication of the term Amlapitta signifies the abnormal state of
pitta especially in its amla guna. Yoga ratnakara and Kashyapa have used the
terms pittamla and shuktata respectively as synonyms of Amlapitta, though they
are not directly stated so.
3. Pittamla: The term would imply the sense of the term Amlapitta that is
mentioned in Amlapitta chikitsa in Yoga ratnakara.19
4. Shuktata: It is mentioned synonym for Amlapitta 20.
5. Amlaka: It refers to one of the nanatmaja vyadhis of pitta mentioned in the
context of pittaja nanatmaja vyadhis and Indu commenting this says hritsula,
antardaha, Kukshidaha, amloudgara. All these symptoms are totally called as
amlaka.21

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 10
NIDANA
Here the term Nidana refers to the causative factors, which play an important
role in the manifestation of a disease. All diseases stem from indulgence in improper
diet and regimen that may promote the morbidity of the Dosa, go contrary to the well
being of the Dhatu and also vitiate the Srotas. It is said, “The character of a man’s
digestive system moulds and shapes his destiny on this planet:.
This statement holds good as the Annavaha srotas and Ahara have a direct
proximity. Thus a thorough knowledge of the Nidana is imperative such that
preventive measures can be adopted. Nidana parivarjana22forms the first and foremost
step in the treatment of any disease in general and specifically in Amlapitta
In classics a large number of Nidana have been explained in the context of
Amlapitta. After a careful screening and analysis of the nidana of Amlapitta, they may
be discussed under four groups.23
Aharaja Hetu
Viharaja Hetu
Manasika Hetu
AagantajaHetu
A brief resume of these factors may be presented as under.
Aharaja Hetu [dietary factors]: -
The first and the foremost group of nidana of Amlapitta may be considered as
the Aharaja hetu. Under this group the intake of food against the code of dietetics i.e.
Ahara vidhi vidhana 24and Ahara vidhi visheshaayatana25 is included. Various type of
incompatible substances, excess of pitta aggravating factors like Katu, Amla, Vidahi,
etc. and irregular time of consumption of food are the factors against the dietetic code
and they are directly responsible for the annoyance of pitta.
Viharaj Hetu [Habit oriented factors]: -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 11
To maintain the sound and good health, one has to follow the code of habits.
He is required to have regular habits of defecation, eating, and sleeping in time. He
has not to suppress the natural calls, maintain the equilibrium of the body
constituents’ and by that, obviously, he would maintain good health and proper
functioning of the body. If this is not followed regularly, the whole functioning of the
body will be disturbed and in long run, they will cause the disturbances of the
equilibrium of pitta and digestion, which ultimately will lead to Amlapitta.
Manasika Hetu [Psychological factors]: -
Psychology also plays a great role in maintaining the health of a person. An
abnormal psychology of a person in terms of anxiety, anger, greediness, etc. would
affect the physiology of the digestion. These factors tend to affect the secretion of the
pitta and by that, they are disturbing the homeostasis, which interns Amlapitta.
Agantuja Hetu [other related factors]:
Under this group constant and excessive consumption of alcohol, tobacco,
beverages, smoking, or other irritant stuffs, etc are taken. These substances cause a
local irritation in the amashaya, which in turn secrets more pitta, which may be
grouped under this category.
TABLE NO 1 COMPARATIVE TABLE SHOWING THE CLASSICAL
ETIOLOGICAL FACTORS OF AMLAPITTA
Sr Etiological Factors K.S.26
M.N27
. B.P.28 B.R.29
G.N.30
S.S.31
1. Adhyasana (To eat before the
previous food is digested) + - - - - -
2. Abhishyandi Bhojana + - - - - -
3. Ajirna (Indigestion) + - - - - -
4. Ama (Undigested) + - - - - -
5. Ama Pakwanna
(Semi-digested food) + - - - - -
6. Akala Bhojana + - - - - -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 12
(Untimely diet)
7. Amla Sevana
(Eating of acidic substances) + + + + + +
8. Ame Ame Ca Puranant
(To eat without appetite) + - - - - -
9. Antarodaka Prana (To drink
much water during food) + - - - - -
10. Ati-ushna Ahara (Very hot
diet) + + + + + +
11. Ati-snigdha Ahara (Fatty diet) + - - - - -
12. Ati-ruksha Ahara (Coarse diet) + - - - - -
13. Ati-drava- Sevana
(Excess liquid) + - - - - -
14. Atisnana (Lengthy bath) + - - - - -
15. Avagahana (Tub-bath) + - - - - -
16. Bhuktwa – Buktwa + - - - - -
17. Bhrista – Dhanya + - - - - -
18. Dustanna - + + + + +
19. Diwaswapa + - - - - -
20. Gorasa (milky product) + - - - - -
21. Guru Bhojana (Heavy diet) + - - - - -
22. Ikshuvikara
(Sugarcane product) + - - - - -
23. Kulattha Sevana + - - - - -
24. Madya (Alcohol) + + + + + +
25. Paryusitanna + - - - - -
26. Pitta Prakopi Annapana - + + + + +
27. Pistanna + - - - - -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 13
28. Pruthuka Sevana + - - - - -
29. Pulaka Sevana + - - - - -
30. Vidhanya - + + + + +
31. Viruddhasana
(Incompatible diet) + + + + + +
These may again be simplified in a more systemic way as below.
According to the type of ahara:
[a] Kulattha [b] Pruthuka [c] Pulaka (husky food)
According to the quality of food:
[a] Abhishyandi [b] Ati snigdha [c] Ati ruksha [d] Gurubhojya [e] Vidahi anna
According Samskara done on the ahara: -
[a] Apakwa anna [b] Bhrishta Dhanya [c] Ikshu vikaras [d] Pishta anna anna
According to dushti of ahara:
[a] Dushta anna [b] Paryushita anna
According to the pitta provocative properties of ahara:
[a] Adhyashana [b] Ajirnashana [c] Ama Purnata [d] Ati ushna [e] Ati Amla
[f] Ati Drava [g] Ati Tikshana [h] Ati panam [i] Katvannapana [j]
Viruddhashana
According to the capacity of weakening the digestive power by the ahara:
[a] Ati snigdha sevana [b] Ati ruksha.
TABLE – 2 A COMPARATIVE TABLE SHOWING THE CLASSICAL
ETIOLOGICAL FACTORS WITH DOSHA INVOLVEMENT OF
AMLAPITTA

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 14
Nidana
Doshika
Involve-
ment
K.S. M.N. B.P. S.N. H.S. G.N. Y.R. B.S.
Kulattha Sevana P + - - - - - - -
Pulaka Sevana P + - - - - - - -
Pruthuka Sevana P + - - - - - - -
Guru Ahara K + - - - - - - -
Abhishyandi Ahara PK + - - - - - - -
Atisnigdha Ahara PK + - - - - - - -
Ati Ruksha Ahara V - - + + - - - -
Vidahi Annapana P - + + - - + + +
Pistanna Sevana PK + - - - - - - -
Apakwanna Sevana PV + - - - - - - -
Phanita Sevana K + - - - - - - -
Ikshuvikara Sevana K + - - - - - - -
Paryushitanna Sevana VPK + - - - - - - -
Dushtanna Sevana VPK - + + - - + + +
Ati-ushna Ahara P + - - - - - - -
Viruddhahara VPK + + + + + + + +
Ati-amla Ahara PK + + + + + + + +
Ati-tikshna Ahara VP - - - + - - - -
Adhyashana VPK + - - - - - - -
Amapoornata VPK + - - - - - - -
Ajeernashana PK + - - - - - - -
Akala Bhojana KP - - + - - - - -
Kale Anashana V + - - + - - - -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 15
Visamashana V + - + - - - - -
Vegavidharana VPK + - - - - - - -
Bhuktva Divaswapna K + - - - - - - -
Bhukta Avagahanam VK + - - - - - - -
Bhuktva Snanam VK + - - - - - - -
Ati-madya Sevana VPK + - - - - - - -
Pitta Provocative
factors VPK - - + - - - - +
Pathophysiolagy
Shad Ahara Parinamakara Bhavas are responsible for proper digestion.32
Usma :Usma is a quality of Agnimahabhuta. In this regard two terms are to be
considered viz. Agni and Pitta. Sushruta explains that there is no Agni except Pitta in
body. Pachaka Pitta is situated in Aamashaya and it performs the function of Agni.
Various secretion of G.I.T. can be considered under the light of Pachaka-Pitta. It
should be released in proper time and in proper quantity. Usma of Pachaka Pitta is
essential for proper digestion, disturbance of it will lead to complication of Agni.
Vayu :Samana Vayu is seated in Aamashaya, helps the Pachaka Pitta in digestion.
According to Sushruta, there is a vicious cycle between Prana-Apana-Samana, it
means this two also helps to maintain Agni.
The Apakarshana, Grahana and Munchana Karma of Vayu are essential for
proper digestion.
Any exacerbation or cessation in these function will leads to improper
digestion. As certain time is required for proper digestion, delayed emptying will
cause the Shuktapaka and formation of Amavisha, which are the essential factors of
Grahani Dosha. Now it is clear that all secretary regulations can be termed as function
of Samana Vayu. If Samana Vayu is disturbed it will lead to Ajirna stage like and
start the pathogenesis of G.I.T. diseases. The etiological factors like Krodha, Shoka,

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 16
Bhaya, Chinta and other stress factors work through the Vagus chain, which is said to
be mediating through Vayu. Provocation of Vata by any factor will result in hyper-
secretions leading to hyperacidity.
Kleda :This factor is necessary for proper digestion; it loosens and emulsifies the
food. This function is performed mainly by liquid portion of food itself i.e. saliva,
mucosa and liquid portion of various digestive juices. Kledaka and Bodhaka Kapha
may be considered in this regard. Drava has been termed as Kleda in Ahara Parinama
Bhava.
Though Kapha has not been mentioned having Drava quality but Kapha made
up of Apadhatu and so that Kapha must posses Dravata but it depends upon the
temperature. So, the function of Kledaka Kapha can be summarized as Kledana-
Shithilikaran-Mridukarana and Sanghata Bheda. The excessive Klinnata may hamper
the Agni directly as mentioned in the literature, that Dravata ceases the Agni.
Ingestion of any Ati-ushna, Tikshna and Katu Dravya may cause excessive secretion
of mucous, which may interfere with digestion process and cause the Vidagdha
Avastha in excess leading to Ajirna etc. In the same way increase in Kapha causes
Mandagni.
Sneha :Usually Ahara contains Sneha. Kapha is also having the property of Sneha, it
also belongs to Apamahabhuta, Sneha has been described possessing a specific
quality of Apa. Pitta is also having Sneha Guna33. Hence, it can be said that, Sneha is
also the quality of Kledaka Kapha and Pachaka Pitta mainly of saliva and
glycoprotein of stomach as indigenous Sneha and other Sneha coming from Ahara,
Sneha perform the function of Mardava (softness of food stuff). Ultimately it helps in
the proper mastication and churning by stomach musculature, So that the proper
digestion can take place. The decrease in the quality of Sneha may damage the
intestinal mucosa due to roughness of food stuff and also due to Ruksha Guna of
various food materials. Decrease of Sneha in stomach will lead to provocation of
Samana Vayu which imbalances the Agni.
Kala :This is an important factor for every process to carry out. Time required for the
proper secretion of all the digestive factors and for digestion and absorption. Kala

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 17
means mainly the time required for the digestion of ingested food stuff. But other time
considerations are also necessary for proper digestion and absorption of food, i.e.
Kshudhakala, Trishakala, Doshakala and also Charvankala. The food is to be taken
after the proper digestion of pervious meal. The meal taken without proper digestion
of previous meals is called as Adhyashana and this is the main cause of Agnidushti.
Emptying of stomach requires certain time. Retention of food material in
intestine is regulated by Vayu. Any disturbance of Vata will disturb the Grahana and
Munchana period leading to improper digestion and absorption which will lead to
further provocation of doshas. Excessive Dharana of acidified Anna may cause
damage to duodenal mucosa. The Adhyashana and Ajirna-Bhojana, may cause the
Prakopa of all the three Doshas simultaneously Agnidushti.
Samyoga :Equilibrium of all above factors is necessary for the proper digestion of
ingested food material. Ashtavidha Ahara Ayatana should be considered to avoid
Agnidushti. Charaka has given a deep thinking on various aspects of qualities of food
materials, which is obvious from the fact that most of the diseases have a long list of
etiological factors from dietary habits and diet articles. Charaka has formulated
guidelines for a healthy diet selection and same time he has also formulated the rules
for healthy eating.34

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 18
PURVARUPA
Purvarupa are premonitory symptoms, which herald the forthcoming disease
and appear at the onset of Dosa-Dusya sammurcchana..
Chakrapani has classified the purvarupa into two types,35
Vyakta lakshanas i.e. visible.
Avyakta lakshanas i.e. invisible.
In Amlapitta purvarupa are not evident as they probably belong to the latter
category. Even if they are present it is not possible to recognise them, as minor
fluctuation of doshas are common events. Hence no purvarupa have been mentioned
for Amlapitta in classics.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 19
RUPA
The laksana that indicate the disease are called as Rupa. The sources of
knowledge are many viz. Pratyaksa (direct observation), Anumana (inference),
Aptopadesa (instruction), Yukti (reasoning) etc. All the above can be applied
individually or in combination for impeccable knowledge. So also, the Laksana that
have appeared in a disease can be discerned with the aid of the above Pramana for
prompt diagnosis and treatment. The appearance of Laksana in a vyadhi follows
Dosa-dusya sammurcchana and helps to clinch the diagnosis.
These are produced during the Vyakta stage of Kriya Kala. This has been
classified in to two types. Samanya and Visista Rupa. The Samanya Rupa of
Amlapitta and the Laksanas of Amlapitta have been listed in the table below.
Table – 3 Samanya Laksanas of Amlapitta:
Sl. No. Laksanas K.S. M.N. B.P Y.R. V.S.
1 Amlodgara - + + + +
2 Tiktodgara - + + + +
3 Kantavidaha + + + + +
4 Urovidaha + - - - -
5 Kuksidaha - + + + +
6 Utklesa - + + + +
7 Amla Utklesa + - - - -
8 Avipaka - + + + +
9 Hritdaha - + + + +
10 Guru Kostata + - - -
11 Udaradhmana + - - - -
12 Antrakujana + - - - -
13 Vidbheda + - - - -
14 Aruci - + + + +
15 Klama - + + + +
16 Gourava - + + + +
17 Angasada + - - - -
18 Romaharsa + - - - -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 20
The important factors that are involved in the manifestation of Amlapitta are,
1. Vidagdha Pitta
2. Agnimandya
3. Suktapaka
Vidagdha Pitta is the vitiated state of Pitta. This causes Agnimandya. During
this state if the person consumes food, that doesn’t get digested and gets converted in
to Aama. Continued presence of Aama in the Amasaya attains Suktata. This produces
Amlodgara, Utklesha, Hritdaha, Kukshidaha and Kantadaha. The Laksanas produced
by Sukta Paka can be considered as Pratyatma Laksana. Other symptoms Avipaka,
Aruchi, Hrillasa are due to Agnimandya. The persistence of Agnimandya and Aama
causes the improper formation of Rasa Dhatu. Hence the Rasaksaya Laksanas like
Klama, Bhrama, etc. Along with the above the Sarvadaihika Pitta Prakopa Laksanas
like Karadaha, Charanadaha, Angadaha, Usnata etc are seen.
Classification Of Amlapitta:
(A) According to the movement of the Dosha.36
1. Urdhvaga Amlapitta.
2. Adhoga Amlapitta.
(B) According to the Dosha Samsarga,37 Amlapitta has been classified as
follows -
1. Sanila
2. Sakapha
3. Sanilakapha
4. Slesmapittaja

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 21
(C) According to Acarya Kasyapa:38
Amlapitta is of three types.
1. Vataja
2. Pittaja
3. Kaphaja
Urdhvaga Amlapitta:The tendency of the movement of the Doshas towards upward
direction produces Urdhvaga Amlapitta. Hrithkanthadaha, Utklesha and Chardi are
prominent features. The Laksanas of Urdhvaga Amlapitta mentioned by different
Acaryas are listed in the following table.
TABLE – 4 OF URDHVAGA AMLAPITTA LAKSANAS:
Sl.No. Lakshanas M.N Y.R. B.P. V.S.
1 Vantam Haritam + + + +
2 Vantam Pitam + + + +
3 Vantam Nilam + + + +
4 Vantam Krisnam + + + +
5 Vantam Arunam + + + +
6 Vantam Raktam + + + +
7 Vantam Ativamanam + + + +
8 Vantam Mamsodakabham + + + +
9 Vantam Atipichilam + + + +
10 Vantam Sleshmanugatam + + + +
11 Vantam Rasena Vividham + + + +
12 Vantam Bhukta Vidagdha Amlavami + + + +
13 Vantam Bhukta Vidagdha Tiktavami + + + +
14 Vantam Abhukte Tiktavami + + + +

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 22
15 Vantam Abhukte Amlavami + + + +
16 Tiktodgara + + + +
17 Amlodgara + + + +
18 Hritsula + + + +
19 Kanthadaha + + + +
20 Kuksidaha + + + +
21 Shirasula + + + +
22 Karadaha + + + +
23 Charanadaha + + + +
24 Usnata + + + +
25 Aruchi + + + +
26 Jwara + + + +
27 Kandu + + + +
28 Mandala + + + +
29 Pidaka + + + +
Adhoga Amlapitta:
The movement of the Dosha to downward direction produces Adhoga
Amlapitta. The features related to the Adhopravritti are predominant. The features
mentioned by different Acaryas are Trishna, Daha, Murcha, Bhrama, Moha,
Adhopravahana of Doshas with different colours, Hrillasa, Kota, Analasada, Harsa
and Sweda.394041

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 23
Table.no 5 Showing Lakshana of Adhoga Amalapitta.
Sl.no Lakshana K.S M.N B.R Y.R V.S
1 Trishna + + + + +
2 Daha + + + + +
3 Murcha + + + + +
4 Bhrama + + + + +
5 Moha + + + + +
6 Hrillasa + + _ + _
7 Kota + + + + +
8 Analasada _ + + _ +
9 Harsa + + + + +
10 Sweda + _ _ _ +
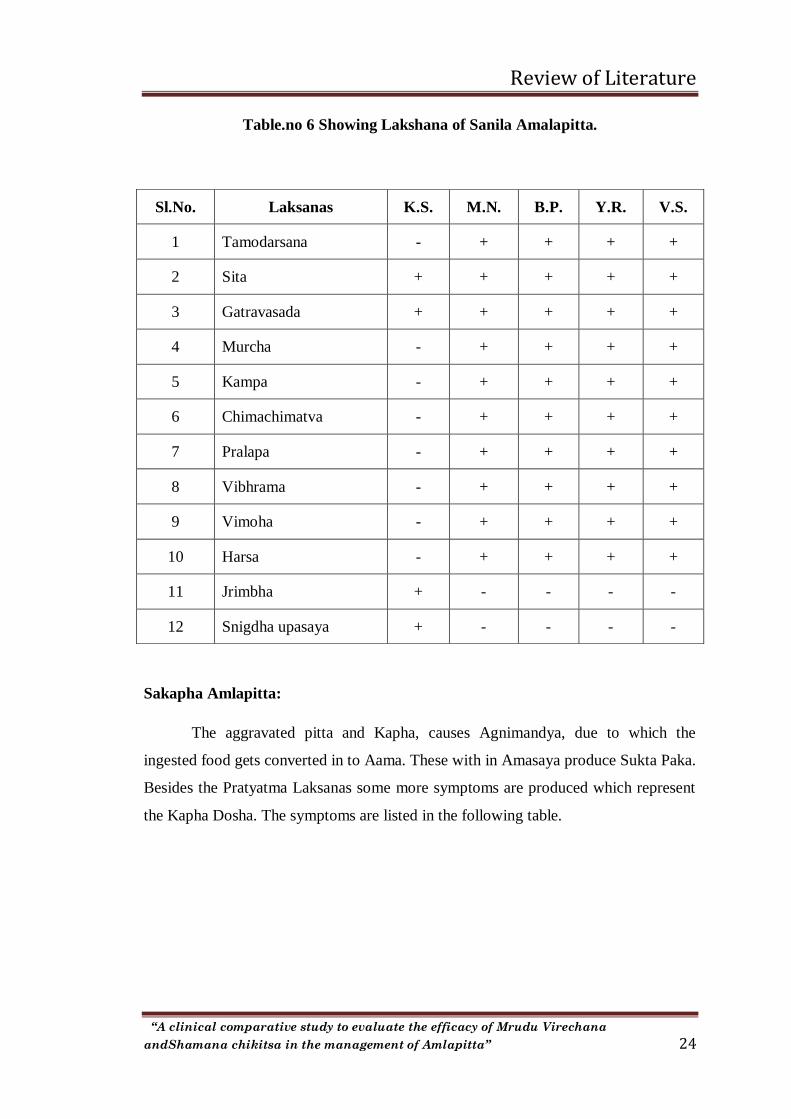
Sanila Amlapitta:
The aggravated Pitta and Vata, causes Agnimandya, due to which the ingested
food gets converted in to Aama. This on retention in Amasaya results in Sukta Paka.
Besides the Pratyatma Laksanas some more symptoms are produced and they
represent the Vata Dosha. The symptoms are listed in the following table
Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 24
Table.no 6 Showing Lakshana of Sanila Amalapitta.
Sakapha Amlapitta:
The aggravated pitta and Kapha, causes Agnimandya, due to which the
ingested food gets converted in to Aama. These with in Amasaya produce Sukta Paka.
Besides the Pratyatma Laksanas some more symptoms are produced which represent
the Kapha Dosha. The symptoms are listed in the following table.
Sl.No. Laksanas K.S. M.N. B.P. Y.R. V.S.
1 Tamodarsana - + + + +
2 Sita + + + + +
3 Gatravasada + + + + +
4 Murcha - + + + +
5 Kampa - + + + +
6 Chimachimatva - + + + +
7 Pralapa - + + + +
8 Vibhrama - + + + +
9 Vimoha - + + + +
10 Harsa - + + + +
11 Jrimbha + - - - -
12 Snigdha upasaya + - - - -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 25
Table.no 7 Showing Lakshana of Sakapha Amalapitta.
Sl.No. Laksanas K.S. M.N. B.P. Y.R. V.S.
1 Kaphastiavan - + + + +
2 Vamana - + + + +
3 Aruchi - + + + +
4 Sleshmaliptasyata - + + + +
5 Gourava + + + + +
6 Jadata - + + + +
7 Shitatva - + + + +
8 Bala Sada - + + + +
9 Anga Sada - + + + +
10 Kandu - + + + +
11 Nidra - + + + +
12 Chardi + + + + +
Sanilakapha Amlapitta:
Vitiated Kapha and Vata Doshas in Aamasaya along with Vaikritha Pitta
produces Agnimandya, which on stasis converts in to suktapaka. The symptoms
pertaining to the vitiated Vata and Kapha Doshas also seen along with the Pratyatma
Laksanas. The mixed features of Sanila and Sakapha Amlapitta are observed.
Slesma Pittaja Amlapitta:
The Laksanas are tabulated, which are mentioned in Madhava Nidana. The
Laksanas represent Pitta and Kapha Dosha and they are similar to Urdhvaga
Amlapitta.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 26
Table no 8 showing laksanas of Shlesma pittaja Amlapitta:
Sl.No. Laksanas K.S M.N B.P Y.R V.S
1 Siroruk - + + + +
2 Praseka - + + + +
3 Chardi - + + + +
4 Tiktodgara - + + + +
5 Amlodgara - + + + +
6 Katukodgara - + + + +
7 Kantadaha - + + + +
8 Kuksidaha - + + + +
9 Alasya - + + + +
10 Murcha - + + + +
11 Bhrama - + + + +
12 Ruksa Upasaya
Usna Upasaya
-
-
+
+
+
+
+
+
+
+
Pittaja Amlapitta:
Pitta gets vitiated without the other Doshas, produce Agnimandya and results
in to Sukta Paka. The Laksanas that are produced are the contribution of the vitiated
Pitta Dosha only.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 27
Table no 9 showing Laksanas of Pittaja Amlapitta:
Sl.No. Laksanas K.S M.N B.P Y.R V.S
1 Bhrama + - - - -
2 Vidaha + - - - -
3 Ruksa Upasaya
Usna Upasaya
+
+
-
-
-
-
-
-
-
-

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 28
SAMPRAPTI
Samprapti means description of physiological derangements and pathological
process, which takes place in a person due to nidana sevana. It helps to understand the
manifestation of clinical features and it also has therapeutic importance. The ancient
scholar has stated that samprapti vighatanameva chikitsa, that is, reversal of
pathogenesis is the complete treatment.
Kashyapa, Madhava and Gananatha sena have maintained specific Samprapti
of Amlapitta as follows.
Over indulgence in above mentioned aetiological factors cause vitiation of
Vata-Pitta Dosha. Anyone of the involved Dosha Slackens the Jatharagni (to below
the normal level) i.e. Jatharagnimandya. During this state, whatsoever food is
consumed becomes Vidagdha. Then it becomes Sukta and it lies in the Amashaya
stagnant. Any food which is taken becomes Vidagdha. At this stage Vidagdhajirna
manifests which is the purvarupa of the disease.
Further vitiated Pitta get mixed with Sukta and causes Pitta Amavisa
Sammurchhana. The Amlapitta with its cardinal symptoms is then born.
If not treated properly in this stage, the disease leads to Bhedavasta where the
typical characteristic of types like Urdhwaga, Adhoga etc. are differentiated.
Further complications like Sitapitta, Udara, Annadrava and Parinama shula etc
may occur in the advanced course of the disease.
Gananath Sen in Sidhanta Nidana has mentioned that when food is dominant
with Amlarasa, then in Amashaya also Amlarasa in produced and when it is taken in
more quantity it irritates the Amashaya. If food is not consumed at proper time, then
the secretion of Amlarasa increase and it then irritates the Amasayakala resulting in
various incurable disorders like Shula etc.
Dr. Harinath Jha et al (1986) has described details regarding the Samprapti of
Amlapitta in 2 ways i.e. the Sushruta concept of Samprapti and Charak concept of
Samprapti.
The Samprapti of Amlapitta may be transformed into a schematic diagram as
follows.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 29
NidanaSevana
Aharaj Viharaj Manasika Agantuj
Pitt
sanchaya
Agni
Dushti
Punaha
Sevana
Pitt
Prakopa
Atiamlata
Agnimand
haya
Avipaka
Vidhagata Ama Rasa
Dushti
Shuktamlata
Pitta Ama Visha
Samurchhana
Amlapitta
Urdhavaga
Adhoga
Diagramatic presentation of the Samprapti of Amlapitta
Atidravatva
Urdhavaga

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 30
Samprapti of Amlapitta (In terms of Charak)
1. Sankhya Samprapti :
a. Two types according to Gati
i. Urdhwaga ii. Adhoga
b. Three types according to Kashayapa
i. Vatolvana ii. Pittolvana iii. Kapholvana
c. Three types according to Madhavakar
i. Vatika ii. Vatakapha iii. Kapha
iv. Also counted fourth types Shleshma Pitta.
2. Vidhi Samprapti :
a. i. Nija ii. Agantuja
b. i. Svantantra ii. Paratantra
c. According to curability
i. Naveena - Curable by factful persuasion
ii. Chirothita - Krichhasadhya
iii. Chirothita - Krichha Sadhya, Yapya
3. Vikalpa Samprapti :
i. Vata - Chala, Ruksha karmataha
ii. Pitta - Dravyataha, Ushna, Teekshna, Sara, Amla, Katu, Drava
iii. Kapha - Dravyataha, Karmataha, Guru, Mridu
4. Pradhanya Samprapti :
i. Pitta - Vriddhatama
ii. Kapha - Vriddhatara
iii. Vata - Vridha

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 31
5. Bala - Kala Vishesha :
a. Seasonal aggravation - i. Sarada ii. Greeshma
b. Day / Night - i. Noon ii. Mid night
c Dietetic time - Bhojanottar
SAMPRAPTI GHATAK OF AMLAPITTA :
1. Dosha - i. Vata - Samana
ii. Pitta - Pachaka
iii. Kapha - Kledaka
2. Dushya - Ahararasa
3. Agni - Jatharagni i. Mandagni
ii. Vishamagni
4. Ama - Jatharagnijanya ama
5. Srotas - i. Rasavaha
ii. Annavaha
iii. Purishavaha
6. Srotodusti - i. Sanga
ii. Vimarga Gamana
7. Adhistana - Amashaya
8. Sancharastana - Mahasrotas
9. Vyaktastana - Amashaya
10. Rogamarga - Abhyantaroga marga
11. Swarupa - Chirakari
12. Prabhav - Danuna
13. Sadhyasadhyata - Sadhyavyadhi

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 32
UPASAYA ANUPASAYA
Specific mentioning about Upasaya and Anupasaya is given only by Kashyapa
while describing dosaja types of Amlapitta.
Vataja Amlapitta - Snigdha Upasaya42
Pittaja Amlapitta - Swadu and Sita Upasaya44
Kaphaja Amlapitta - Ruksa and Ushna Upasaya44
UPADRAVA
The occurrence of another disease in the wake of primary disease is called as
Upadrava45. . These are produced during the Bheda Avastha of the disease. These are
dependent on the primary disease. Unless they are life threatening, don’t need special
treatment. Even still, the presence of the Upadravas helps to identify the
Sadhyasadhyata of the disease.
In Kasyapa Samhita46 the Upadrava of Amlapitta are explained as:
1) Jwara
2) Atisara
3) Pandutva
4) Sula
5) Shotha
6) Aruchi
7) Bhrama
Though Madhavkara has not mentioned the complication of Amlapitta but
included Shoola in its Vatika predominant variety. Hence, Parinama and Annadrava
Shoola can be taken as complications of Amlapitta.
According to Acharya Gananath Sen Upadravas of Amlapitta are -

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 33
1. Amasayakala shopha
2. Grahani Kala Shopha
3. Kandu
4. Mandala
5. Pidaka
6. Shitapitta
7. Udara
8. Vicharchika
9. Vispota
DHATUGATATVA OF AMLAPITTA
Doshas vitiated due to Same Nidana can produce different diseases as per their
lodging w.s.r. to Ashaya and Dushya.47. Though Amlapitta is simple disease but
treatment given in some condition does not give relief, this shows another view to
think over. Each and every dosha resides by the shelter of any of Dhatu. But vitiated
doshas moves in different places, dhatus and leads to Vikruti of that particular dhatu,
this condition is known as Dhatugatatva. If Doshas are following Dhatugatatva then
there should be difference in its treatment.
Dhatugata Doshas are generally Tiryagagata. Doshas might be SAMA or
NIRAMA, that’s why we must think on the line of SAMADOSHA and
TIRYAGAGATA doshas management. They are chronic in nature. So Pachana-
Shamana should be done by observing the State of Dosha-agnibala etc. otherwise
Doshas should be brought into Kostha and thereafter, they should be eliminated out of
the body.
“Dhatu Vaisamya” is nothing but the discordance of the Dhatu.
Dhatu Vaisamya is not actually a disease but it is the former stage of
pathogenesis i.e. it is precondition for “Dosha-Dushya Sammurchana”.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 34
But according to Dr. S.C. Dhyani (1958), Dhatu Vaisamya is not present
before the Dosha-Dushya Sammurchana but will occur during the sammurchana
Avastha only. If one will go through the mode of pathogenesis mentioned for diseases
he will get that Vaisamya Avastha is present before the Dosha-Dushya Sammurchana.
Though Doshas are present all over the body it’s Gata condition specifically indicates
it’s abnormal localization at a particular Dhatu or Asaya. In this condition the
etiological factors are only of Doshas and not of two fold nature i.e. of both Dosha
and Dushya.
Acharya Vagbhata48 has described the Dhatugatatva of Pitta dosha and Kapha
Dosha. Charaka has explained the Gatatva of Vata. In Dhatugata Avastha Dosha
disturbs to Sthayi Dhatu along with Poshaka Dhatu. Generally, it leads to Kshaya
condition of that Dhatu. At such place treatment should be based on that particular
Dhatu. In Raktagata Jwara, there is symptom of Raktasthivanam in such condition
drug used for treatment should have Rakta-Pittahara property so in this condition one
may should use Vasa and Pravala.
Dr. Sadashiva Sharma (1960) have described that, in the Samhitas, Dhatugata
stage of three diseases have been described namely 1) Jwara, 2) Kustha, 3)
Vatavyadhi. He explained that, these diseases are representative of Dhatugatatva of
Pitta, Kapha and Vata diseases respectively. He further explained that Jwara should be
taken as example for all the Pittolvana diseases, Kustha for Kapholvana and
Vatavyadhi for Vatolvana diseases, Raktasthivana shows the establishment of
diseases in Rakta Dhatu.
By the study of symptomatology of Amlapitta and with the help of Jwara
Dhatugata Avastha and Dhatugatatva of Pitta described by Vagbhata, we can describe
the Dhatugatatva of Amlapitta as below ;
Rasagata Amlapitta :Rasagata Amlapitta produces the symptoms like Gaurava,
Jadata, Aruchi, Chhardi, Avasada, Praseka.
Raktagata Amlapitta :Raktagata Amlapitta shows the symptoms like Daha,
Hastadaha, Padadaha, Hritadaha, Kukshidaha. Along with it produces several

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 35
Pittadushtaraktaja Vyadhi as Agnisada, Kandu, Kotha, Mandal, Pidaka, Headache
(severe).
Mansagata Amlapitta :In the stage of Mansagata Manasapaka can be observed
which can be co-related with peptic ulcers, gastritis etc. formation of ulcer after
Amlapitta is the result of progression of pathogenesis into Mamsadhatu. Antardaha
and Trushna also manifest.
Medogata :In this stage, Swedadhikya, Trishna, Pralap, Chhardi, Aruchi, Glani can
be seen.
Asthigata Amlapitta :In this stage, severe Daha all over body, Atisara, Vamana is
observed.
Majjagata Amlapitta :In this stage Tamodarshanam, Murchha, Moha, Bhrama,
Parvashula. Haridravarna in Netra and Nakha is observed, As there is also strong
relation between Majja and Netra.49.
Shukragata Amlapitta :In this stage, Shukra becomes Puyayukta and yellow in
color. Besides this Angasada, Shrama, Sadahalpashukravisarjana, Daurbalya,
Panduta, Mukhasosha etc. symtpms can be observed.
In Dhatugata avastha, diseases shows the symptoms of previously involved
Dhatus also, means Mansagata Amlapitta shows the symptoms of Rasagata and
Raktagata Amlapitta.
In Dhatugata condition of Dosha the Asthi-Majjagata conditions is said to be
untreatable (Asadhya).

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 36
SADHYASADHYATA
Sadhyasadhyata is consider as prognosis of a disease, Acarya caraka difined as
“Sadhyasadhyavibhagajno jnanapurvam cikitsakah /
kale ca arabhate karma yattat sadhayati dhruvam //”50
Prognosis of a disease distinguishes between the curable and the incurable and
gives an idea regarding the modality of treatment to be adopted. In addition to the
general guidelines for deciding the Sadhyasadhyata, the following are specifically
mentioned in Amalapitta.
The prognosis of the disease is not uniformly favorable. Madhavakara has
pointed out that in case the patient has been suffering from Amlapitta recently and is
treated properly the prognosis is good. Chronic cases may either improve a little or
may be relieved completely during the course of treatment. As soon as the patient
deviates from the wholesome diet the disease relapses. When disease is of short
duration then it is Sukhasadhya, it is Yapya when chronic Krucchrasadhya, when the
duration of the disease is long and cured with great difficulty and Asadhya when the
patient will have different Upadravas and symptoms of Dhatu Kshaya.51.
Kashyapa has indicated that in case of patients of Amlapitta gets complicated
by Jwara, Pandu, Shula, Shotha, Aruchi and Bhrama with Dhatu Kshina are
incurable52. Age of maximum occurrence is Yuvavastha which is Pittakala, Prakopa
Kala i.e. Sharad Ritu, is also Pitta Prakopaka Kala and the Hetus also are many in the
causation of this disease i.e. Ahara, Vihara, Manasika etc. These are the factors which
contribute to convert this disease in Krichhrasadhy

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 37
VYVACCEHDAKA NIDANA (DIFFERENTIAL DIAGNOSIS)
A proper examination of the patient is very necessary before going to the
threatment in all the disease.Our science also mentions that ‘Rogamadau pareeksheta
tatonantharamoushadam” before going to the treatment physian should elaborately
examine the patient and come to conclusion about the diagnosis.
The difference between Amlapitta and other diseases which have similar features are
mentioned below.
Vidagdhajeerna: Bhrama, murcha, sadhumaudgara, amloudgara, sweda, daha, pittaja
vividharuja are the lakshanas of vidagdhajeerna which certain symptoms are similar
to Amlapitta. The diffence between these two are only in its chronocity and its course.
Pittaja shula: Teevra shula, trishna, mutra daha, sweda, murcha, bhrama, chosha are
the symptoms which aggravated by pitta prakopaka ahara, madhya dina, madya ratri
and ahara pachyamana kala. And swadu sheeta ahara, snigdha, sheetopachara factors
which relieves the pain.
Parinama shula: This is shula pradhana vyadhi which associated with adhmana,
vibandha, atopa, trishna, atisweda lakshanas. The shula relieves by intake of food,
after the digestion and by doing vamana.
Annadrava shula: Here shula is continuously and only relieved by vamana.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 38
CHIKITSA
Ayurveda has 3 basics of Chikitsa regarding any type of disease.
Nidana Parivarjana53 : Removal of alleviating factors of Ahara and Vihara which
are responsible for causation of the disease. It is to be advised to patient to avoid such
type etiological factors which are responsible for the manifestation of disease.
Apakarshana : Kashyapa has described Vamana as the first line of treatment
followed by Langhana and Laghu Bhojana. Kashyapa opines that just like a tree with
its trunk and branches is destroyed by striking blow at its root. As per Chakradatta,
Yogaratnakara, the second line of treatment is to carry out Mrudu Virechana. The
next regimen consists of Administration of Anuvasana followed by Asthapan in the
chronically afflicted patients. Vangasen and Yogaratnakara added Raktamokshana as
tool if Amlapitta is not cured by Vamana and Virechana,
Vamana : In amalapitta kelada khapa and pachaka pitta endanger the amashaya in
presence of ama hence vamana is best remedy. Drugs used for Vamana are,
Lavanambu, Sukhosna Dugdha, Ikshurasa, Madhudaka and Tiktadravyas.
Vasa, Nibhutvaka, Madanaphala, Sindhava and Madhu.
Gritha, Patholapatra, Triphala, Tvaka, Trayamana, Rohini, Nibha,
Masura and Yashti.
Virechana : When the morbidity is ascertained to have passed on to the pakayashaya
the Virechana would be the measure of choice. Drugs used for Virechana are,
Amalaki swarasa and Trivrit churana.
Avipatikara churana.
Trivrit leha.
Trivrit, Rohini, Katuki, Triphala54
Samsarjana Krama : After every vamana or virechana measure Samsarjana karma
should be followed be by planned and graded diet such as vilepi-yavagu with lagu
ahara constituting deepana-pachana materials. This gradually rejuvenates the jataragni
and then the person should be provided with pathya.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 39
Basti : In vataja amalapitta and in dathugata avastha basti may be optional. So
Anuvasana followed by astapana basti should be given.
Rathamookshana : when sodhana measures fail to subdue the turbulent mobidity and
the case of amalapitta exhibits shishira-alpatha, kota, udarda, visuchika, etc than
Rathamookshana may de resorted.
Prakritivighata : Prakritivighata refers to the use of drugs which suppress the Dosha;
such treatment is termed as Samana therapy. Kashyapa opines that, after Vamana if
the doshas persist, the physician should resort to Samana Chikitsa with the aid of
Laghu, Bhojana, Samana and Pachana Aushadhi. It is forbidden by Acharyas to give
Drava Aushadhi if the doshas are in condition of Utklesha; because if Vamana is not
done the Drava Aushadhi will not be metabolized. When the Dosha Utklesha has
reduced with the help of Ahara and Vihara, physician can give, Ama Pachana and
Bhedana Aushadhi. Once the doshas have been expelled and Aamashaya is devoid of
vitiated Doshas, the physician should ask the patient to take care of the Agni. The
doshas lodged in the Pakvashaya, should be removed with the help of Sramsana
Aushadhi Aragvadha given at Swapna Kala along with cold water.
Mainly Tikta Rasa, Laghu, Snigdha Guna, Katu or Madhura Vipaka, Sheeta
Virya drugs are advocated by all Acharyas. Use of Shamana drugs that opposite to
that of Pitta is beneficial in Amlapitta.
According to Kashyapa :
1. Since the disease is amashaya oriented and Kapha and Pitta are the dominating
Doshas, Vamana should be administered at first.
2. After the Vamana, Samana drug (anti-Pitta, Kapha drugs) should be used. At
the same time Pachana drugs should be given.
3. When the Samsarga doshas are eliminated and stomach becomes clear,
Deepana drug should be administered.
4. If the Doshas have shifted into Pakwashaya, Virechana or Sransana drugs
should be used to eliminate the dosha

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 40
PATHYAPATHYA
“The doctor of the future will give no medicine but will interest their patients in the
care of the human frame, in diet and in the cause and prevention of disease.” 55
Thomas Edison1
The food and the behavior which is compatible to the health is called as
Pathya56. And that which is not conducive to health is called as Apathya. Pathya can
only control the disease. Apathya is similar to Nidana Sevana and it worsens the
disease condition.
Pathya :The following are the Pathyas stated in Amlapitta - Laghu Bhojana,
Shalidhanya, Yava, Godhuma, Mudgayusha, Lajasaktu. The Jangala Mamsa Rasa
Kalayashakha, Karanja Rasa Pushpa, Godugdha, Goghrita, Mudga. The Dravyas that
have Tikta Rasa and Laghu Guna also serve as Pathya. Those Dravyas, which does
not produce Vidaha and the foods or activities which are Sathmya to the body, are
considered as Pathya57.
Apathya:Pitta Prakopaka Ahara and Vihara ie; excess use of Tila, Masha, Kulattha,
Taila, Dhanyamla, Brista Dhanya, Madya and Rasa like Amla, Lavana, Katu are
considered as Apathya
MODERN PERSPECTIVE
It is very much essential to co-relate the diseases which are mentioned in the
classics with the recent disease of Modern medicine for a better comprehension of the
pathogenesis. In modern medical literature, some technical terms have been used to
indicate an abnormal condition resembling to Amlapitta. These terms either explain
the pathological condition of the disease or explain the characteristics of the disease.
It is very difficult to correlate Amlapitta with a single disease of Modern
science. Following is the opinion of scholars till date –

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 41
Year Scholar Disease correlated
1968 Fourth national seminar on Ayurveda
(i) Sri Purushottam Vaidya Acute Gastritis
(ii) Vd. Vishwanath Dwivedi Chronic Gastritis
1982 Tripathi Non ulcer dyspepsia
1986 Harinath Jha Hyperacidity
HYPERACIDITY :This is one of the commonest terms also used by the patients to
subject each gastric discomfort as Hyper acidity. Usually patients having following
signs and symptoms are coming with the chief complaint as hyper acidity Heart Burn,
Chest Pain, Gastric discomfort, Abdominal distention, Sour Belching, Refluxes of the
food taken, Nausea and Loss of Appetite. All these complexes together makes the
disease hyper acidity
Defination :This word is composed of two components i.e. hyper and acidus. Hyper
means over or excess and acidus means sour. So a straight meaning may be derived as
excess of acid i.e. any acid not particularly the HCL in stomach and a disease which
contains this abnormal pathology is defined as hyperacidity.
Pathophysiology :Hyperacidity term indicates about the functional
abnormality i.e. hyper activity of the secreting glands.
Four processes normally take place in the stomach. 1) The conversion of
starch into sugar, begun in the mouth, is carried a stage further. 2) Proteins are
changed into peptones; 3) Fat globules are set free from their envelopes. 4) Milk is
curdled. Delay in digestion may be caused by i) Deficient peristalsis of the stomach
walls, ii) Deficient quality or quantity of the gastric juice, iii) Consumption of
indigestible article or iv) The dilution of the gastric juice by drinking too much fluid
at meal time.
The gastric juice contains HCL, water, pepsin, renin, mineral salts, a little
mucus, and castle’s intrinsic factor. Pepsin and rennin exist in the secretory cells only
as zymogens, which, on secretion into the stomach, become active ferment or

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 42
enzymes. In the healthy state, as the result of digestion, about 30 ml of fluid should be
obtained from the stomach one hour or so after a test – meal (vide – infra), straw
colored, without much odour, without organic acid and with about 0.2% of free HCL.
As regards HCL much depend on the time of examination. Hyperchlorhydria
has come to be somewhat loosely used for “excessive acidity”, and thus to be
confused with the acidity of fermentation (due to organic acid) on the other hand,
after a meal, a negative result on testing for HCL would indicate the absence of peptic
activity as this acid is required for the normal digestive action of pepsin. Excess of
HCL is diminished in catarrhal conditions of the mucus membrane, in anaemia, the
majority of cases of malignant disease, during pregnancy and in states of nervous
exhaustion.
Three organic acids are met in the presence of fermentation in the stomach,
lactic acid, butyric acid and acetic acid. Lactic acid is easily recognized on testing
with uffelman’s reagent and is the only one of diagnostic importance. It is normally
absent in the gastric juice after the digestion has proceeded for one hour, but traces
may be found, due to the ingestion of lactic acid in certain foods, or to fermentation in
the mouth. Fermentation occurs when HCL is deficient or when there is delayed
emptying of the stomach. Lactic acid is most frequently found in cases of gastric
carcinoma with achlorhydria.
The secretion of pepsin is not interfered with, unless there be destruction of
the glands of the stomach. An acid secretion without peptic activity does not occur.
Etiology :These symptomatology may occur due to many under laying causes they
are as discussed below:
General Factors:Vagal effects, Hormonal effects insufficient circulation, shock,
general ischameia, etcConstitutional and environmental factor:Sex, Age,
Temperament, Family history, Social class, Geographical distributions & Occupation,
etc.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 43
Local factor related to stomach
Aggressive Factors: -Hydrochloric acid, Pepsin, Refluxed bile, NSAIDs,
Alcohol, Pancreatic and Proiolytic enzymes, ingested irritants, bacterialtoxins,
psychological trauma.
Defensive Factors: - Mucus, Bicarbonates, Blood flow, restitution of epithelium.
Thus defensive factors are responsible for the enhancement of mucosal
protection. Although no single element may account for mucosal protection, all
may be potentially contributing factors. Insight into mucosal protective
mechanisms was provided by studies performed by Robert. These studies lead to
the introduction of term “Cytoprotection” generally accepted to mean protection
of the gastric mucosal by prostaglandins (PGs) against damaging agents.
Defense of normal gastric mucosa against aggressive factors:Three basic levels of
defense underlined the remarkable ability of normal gastro duodenal mucosal to resist
injury from the acid and peptic activity ingastric juice.
Surface epithelial cells secret mucus and bicarbonates, creating a pH gradient
in the mucous layer and change the very acidic gastric lumen to the nearly
neutral surface of the mucosa.
Gastric mucosal cells have a specialized apical surface membrane that resists
the diffusion of acid back into the cell.
Mucosal cells may directly resist injury by intrinsic mechanisms; such as
extrusion a back diffused hydrogen ions by means of basolateral carriers (e.g.
Sodium-hydrogen or Sodium bicarbonate exchange).
The rapid repair of injury to the mucosa is essential to maintain the mucosal
integrity. Surface epithelial cells continually slough and adjacent cells that
move to fill them by cell replication in response to still unknown trophic
signals reseal the gaps. Blood flow in normal mucosa removes the acid that
has diffuse across a compromised mucosa. Prostaglandins enhance the
mucosa’s resistance to injuries under certain conditions, perhaps by increasing
mucosal blood flow, stimulating the secretion of mucus and bicarbonate,
strengthening of the gastric mucosal barrier, decreasing the gastric motility,
increasing release of endogenous mediators of gastric Cytoprotection like
Sulfhydryls and epidermal growth factors, etc. scavenging of free radicals,

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 44
decreasing release of endogenous mediators of gastric injuries vasoactive
amines and leukotrienes and stimulation of cellular growth and repair.
Role of Infection:Lately some more information has poured in about the prevalence
and changing pattern of the disease, the influence of environmental factors and
speculation on the role of recently characterized bacterial organisms, Helicobacter
pylori, which colonized the gastric mucosa, particularly the antral region.
H. Pylori are a gram-negative spiral bacterium that is found in a patchy
distribution overlaying in gastric epithelium. It was formally named as campylobector
pylori. At present 9 species of Helicobacter genus are available and all excluding
H.plyori, are of animal origin. H. Felis can be introduced into mice to produce intense
colonization and inflammation of stomach.
H.plyori organisms have strong capability of urease production. The bacteria
then split urea and the ammonia thus released may become cause of increased acidity
and hence enabling organism to survive. The released ammonia may also be
cytotoxic.
H.pylori has been implicated in the etiology of belching, indigestion and
chronic peptic ulceration. H.pylori induced gastritis present in about 60% of patient
with gastric ulcer. Until recently pathogenesis of gastric and duodenal ulcers has been
attributed to an imbalance between aggressive factors such as acid and pepsin that
damage the gastric mucosa and protective factors such as prostaglandins that prevent
the damage. Recent evidences relate H.pylori to the pathogenesis of chronic duodenal
ulcer as H.pylori infection and antral gastritis are found together in more than 95% of
patients with duodenal ulcers.
Pathogenesis:
Following factors are important in development of Hyper acidity:
Luminal acid and pepsin are requisite.
Increased mucosal tissue acidosis with subsequent decrease secretion of
bicarbonate (The alkaline ‘tide’).
Reduced mucosal blood flow, whatever its basis (Shock, Drugs, Stress)
causing hypoxic injury & impairing the secretion of bicarbonate.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 45
Disruption of the so-called mucosal barrier (i.e. the intake layer of
surfacemucosal epithelial cells), permitting back diffusion of hydrogen ions
and in turn increased shedding of surface of cell.
Clinical Features: Signs and symptoms are coming with the chief complaint as
hyper acidity Heart Burn, Chest Pain, Gastric discomfort, Abdominal distention, Sour
Belching, Refluxes of the food taken, Nausea and Loss of Appetite.
Treatment:Controlling gastric acidity, hyper motility, and spasm and thus reliving the
associated pain. One or more of the following methods may achieve it.
Uses of antacids, or ion exchange resins.
Stimulating the release of CCK by means of a fatty meal or vegetable oil.
Inhibiting gastric acid secretion by drugs.
Withdrawal of stimulants of, gastric acid secretion such as, alcohol, tobacco
etc.
Surgical removal of the acid producing gastric mucosa by gasterctomy and
vagotomy.
GASTRITIS :Gastritis is inflammation of the gastric mucosa. Gastritis is not a single
disease, rather it is a group of disorders that have inflammatory changes in the gastric
mucosa in common but that have different clinical features, histologic characteristics
and pathogenesis.
Several classifications of gastritis exist. In general, these classifications have
been based on 1) The acuteness or chronicity of the clinical manifestations, 2)
Histologic features, 3) Anatomic distribution or 4) Proposed mechanism of
pathogenesis.
In general on the basis of clinical features, the two principle forms of gastritis
are acute and chronic gastritis.
Acute Gastritis :The onset of H. pylori infection may result in acute gastritis
associated with a transient increase in gastric acid secretion followed by
hypochlorhydria for up to one year. Acute gastritis is characterized by epigastric
pain, nausea, vomiting, anorexia and massive haematemesis.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 46
Chronic gastritis :The inflammatory cell infiltrate in chronic gastritis consists mainly
of lymphocytes and plasma cells. Polymorphonuclear leukocytes and eosinophils may
be present in small numbers. It involves the superficial and glandular areas of the
gastric mucosa initially and progress to glandular destruction.
Chronic gastritis is characterised by the absence of grossly visible mucosal
erosion. But chronic inflammatory changes may lead to mucosal atrophy. Although,
usually it is asymptomatic, but it may be associated with Pernicious Anaemia, Gastric
ulcer, Duodenal ulcer and Gastric carcinoma.
Types of chronic gastrtis
Type A- Body and fundus of stomach is involved
- Less common
- Auto immune in origin
- Asymptomatic
- Gastric cancer chances are high
Type B - Antrum of stomach is involved
- Helicobacter pylori is the causative agen
Chronic non specific gastritis
Chronic gastritis forms (rare)
Common causes of Gastritis :
Acute gastritis (often erosive and haemorrhagic)
Aspirin, NSAIDs
H. Pylori (initial infection)
Alcohol
Drugs e.g. iron preparation
Severe physiological stress, e.g. burns, multi organ failure

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 47
Bile reflux e.g. following gastric surgery
Viral infection e.g. cytomegalovirus (CMV), herpes simplex
Chronic non-specific Gastritis :
H. pylori infection
Auto immune (Pernicious Anaemia)
Post gastrectomy
Chronic specific forms (rare) :
Infections, e.g. CMV, tuberculosis
Gastrointestinal disease e.g. Crohn's disease
Systemic disease e.g. sarcoidosis, graft-versus host disease
Idiopathic e.g. granulomatouos gastritis
Diagnosis :The diagnosis is best established by upper gastro intestinal endoscopy,
which reveals mucosal haemorrhage, erosion, congestion, superficial or deep
ulceration usually in the body or fundus of the stomach. Radiographic examination is
less reliable than endoscopy. Fractional test meal (F.T.M.) or gastric juice analysis
may help in diagnosis.
INVESTIGATIONS :
1. Double contrast Barium meal
2. Endoscopy
3. Biopsy of gastric mucosa
4. Stool routine and gastric analysis : for detection of blood in stool or gastric
aspirate in acute gastritis respectively.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 48
Treatment principles :
1. Acute gastritis :
Prevention of erosive gastritis
Treatment of associated disease
Withdrawal of offending agents
General supporting measures as required
2. Chronic gastritis :
No specific treatment required for type A or type B Chronic gastritis with
or without mucosal atrophy
Pernicious anaemia form of manifestation demands the parenteral vitamin-
B12 administration on indefinite and regular basis.
DYSPEPSIA :
Dyspepsia is the term used by the common man in order to reveal the
symptom complexes as mentioned above under the heading of Amlapitta. In modern
science the same is explained under the heading of Functional dyspepsia. This often
includes symptoms like nausea, vomiting, anorexia, postprandial fullness and bloating
in addition to pain or discomfort.61.
French’s Index of differential diagnosis62 explains it as indigestion with an
upper abdominal discomfort amounting even to pain, nausea, vomiting, heartburn and
distention. Further, the severe pain should be excluded from either dyspepsia or
indigestion.
Similar explanations are quoted in Harrison’s medicine where in, it is a
symptom complex equivalent to indigestion appreciated as upper abdominal
discomfort, associated with intake of food.63
The modern technological advancement has helped to understand the disease
in a better way. With the radiological advancement it was found the majority of the
patients didn’t had the ulcer and the term X-ray negative dyspepsia was introduced.
Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 49
The same was superseded with the introduction of endoscopes and a better description
given was Non – Ulcer Dyspepsia.
Functional dyspepsia 64 and the Non – ulcer dyspepsia65both refer to a similar
condition where a symptomatic individual is not found to have an ulcer or other
structural diseases. The Functional dyspepsia is a condition, characterized by the
presence of chronic intermittent symptoms of epigastric pain often associated with
epigastric fullness, early satiety, bloating and vomiting without mucosal lesions or
other structural abnormalities of the gastrointestinal tract. 66.
Synonyms: Different words have been used for this condition by different authors.
They are Non-ulcer dyspepsia, Nervous dyspepsia, Non-organic dyspepsia, X-ray
negative dyspepsia and Pseudo–ulcer dyspepsia.67.
Prevalence: It is one of the most common disorders. It is estimated that, it effects 20-
30% of the population but amongst only 20-30% of patients with dyspepsia seek
medical care68..
Patients are usually young (< 40 yrs.) and women are affected twice as common as
men69.( D.P.P.M, pg-434).
Etio – pathogenesis:The pathogenesis of Functional dyspepsia is poorly understood;
Most of the patients have normal gastric acid secretion and a relation between
Functional dyspepsia (Non-ulcer dyspepsia) and duodenitis or duodenal ulcer has not
been demonstrated. Similarly a role of Helicobacter pylori and associated chronic
gastritis in causing dyspepsia ulcer is not proved. Disordered gastro duodenal and
small intestinal motility appears to account for some cases of Functional dyspepsia
(Non-ulcer dyspepsia)70.
Clinical features:The symptom complex is described as Functional dyspepsia. It is a
disorder with intermittent symptoms particularly related to the upper abdominal
distress. The patient intermittently develops indigestion. The symptoms are abdominal
pain, which is gnawing or burning type and improve or worsen by intake of food. He
also develops heartburn (retro-sternal pain) due to gastro intestinal regurgitation. The
other symptoms include belching, anorexia, post-prandial fullness, early satiety,

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 50
bloating (abdominal distention) flatulence, aero-phagia, nausea and vomiting may be
present. Intermittent dyspepsia is rare and upper abdominal tenderness is usually
present71..
Investigations:The routine blood investigations like hemoglobin percentage, total
count, differential count, erythrocyte sedimentation rate shows normal values and no
mucosal lesions and structural abnormalities are found by radiography and
endoscopes.
Imaging recommended are72
1. Patients over 45 years of age at the onset of symptoms.
2. Patients with symptoms and signs suggesting a more serious disease.
3. Patients who need added reassurance.
4. Younger patients who do not respond rapidly to empiric treatment.
Usual images done are Endoscopes and Barium meal X-ray.
Measurement of gastric acid output may be of value in Zollinger-Ellison
Syndrome un less suspected73.
Food regimen: The diets recommended in functional dyspepsia are
1. Avoid foods known to exacerbate symptoms.
2. Frequent small meals, low in fat.
3. Avoid tea, chocolate, meat extract.
4. Avoid regular and decaffeinated coffee.
5. Avoid heavy alcohol use.
6. Avoid cigarette smoking.
7. Avoid aspirin containing compounds and NSAIDS etc.
Some other activities like stress reduction, physical exercise, relaxation
techniques are beneficial in cases of Functional dyspepsia74.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 51
Differential diagnosis:Amlapitta is a functional disorder, which has to be
differentiated from organic. The following Table distinguish between functional and
organic disease of the gastro intestinal tract75.
Distinguishing between Functional and Organic/Structural disease of
gastrointestinal tract.
Organic
Symptoms Functional Neoplastic Inflammatory Weight loss None Common Sometimes
Diarrhea Day time only Nucturnal Day and Night
Blood loss None Frequent Frequent
Fever None Rate Frequent
Pain Cramping, Minor to severe May be
by defecation localised,
severe
Bowel habit Alternating Constipation Diarrhea or normal
(diarrhea diarrhea/ (rarely diarrhea)
or constipation) constipation change in caliber
Pellet like
stools
Laboratory tests
Hematocrit Normal Often decreased May be decreased
WBC count Normal Usually normal Often elevated
Erythrocyte Normal Usually increased Usually increased
sedimentation rate
The following diseases should be excluded before diagnosing the Functional
dyspepsia.
Gastro esophageal reflux: Heartburn is the major feature that is aggravated by
bending, stooping or lying down positions. The regurgitation of food and acid into the
mouth can occur, only during those positions.
Peptic ulcer disease: Indigestion is a frequent symptom but epigastric pain is the
characteristic feature of ulcer disease along with water brash, heartburn, loss of
appetite and vomiting. The relationship of the pain to food is variable and on the
whole is not helpful in diagnosis. Sometimes the ulcer is completely silent and
express for the first time with anemia due to chronic undetected blood loss, along with
weight loss.

Review of Literature
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 52
Before treating, the similar diseases should be considered and the tentative
diagnosis, be confirmed by laboratory investigations (if necessary).
All these causes, pathogenesis and symptomatology can be correlated with the
disease named Amlapitta in Ayurvedic Literature. Due to the similarity in causative
factors & sing and symptoms, one can easily correlate these diseases as a same
disease to some extent. It is not always necessary that each sign & symptoms of the
diseases should be met with each other but the maximum possible findings are
suggestive of the similarity between both the diseases. So in the present study
Hyperacidity, Gastritis and Non ulcer dysphiea has been taken as Amlapitta
according to the Ayurvedic point of view.

Drug Review
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 53
DRUG REVIEW
Amlapitta is pittaja vikara, virechana is best procedure to eliminate the morbid
pitta dosha from the system. Yashtimadhu churuna has been selected as
Mrudvirechaka draya.
Sootashekara rasa vati is a herbomineral preparation intended to be used in
Amlapitta as Shamana aushadi. This was formulated by Yogarathankara. The chief
ingredients of which are Parada, Gandhaka, Pippile, Maricha, Datoora, Tamar
bhasama, Sunthi, Swarana bhasama, Vathsanaba, Tankana, Shanka bhasama,
Karchoora, Twak, Ela, Patra and Nagakeshara.
The above drugs qualities and compositions are very important, to assess the mode
action in amlapitta.
CONTENTS OF YASTIMADHU CHURNA76
Botanical Name : Glycyrrhiza glycyrrhizaglabra linn
Vernacular Names : Hindi – Mulethi , English – Liquorice
Chemical constituents : Glycyrrhizin , glycyrrhizic acid , liquirtin ,glabrolide..
Properties :
Rasa – Madhura
Guna – Guru , Snigdha
Virya – Sita
Vipaka – Madhura
Karma – Tridoshahara , rasayana , vrshya , cakshusy
Part used : Root
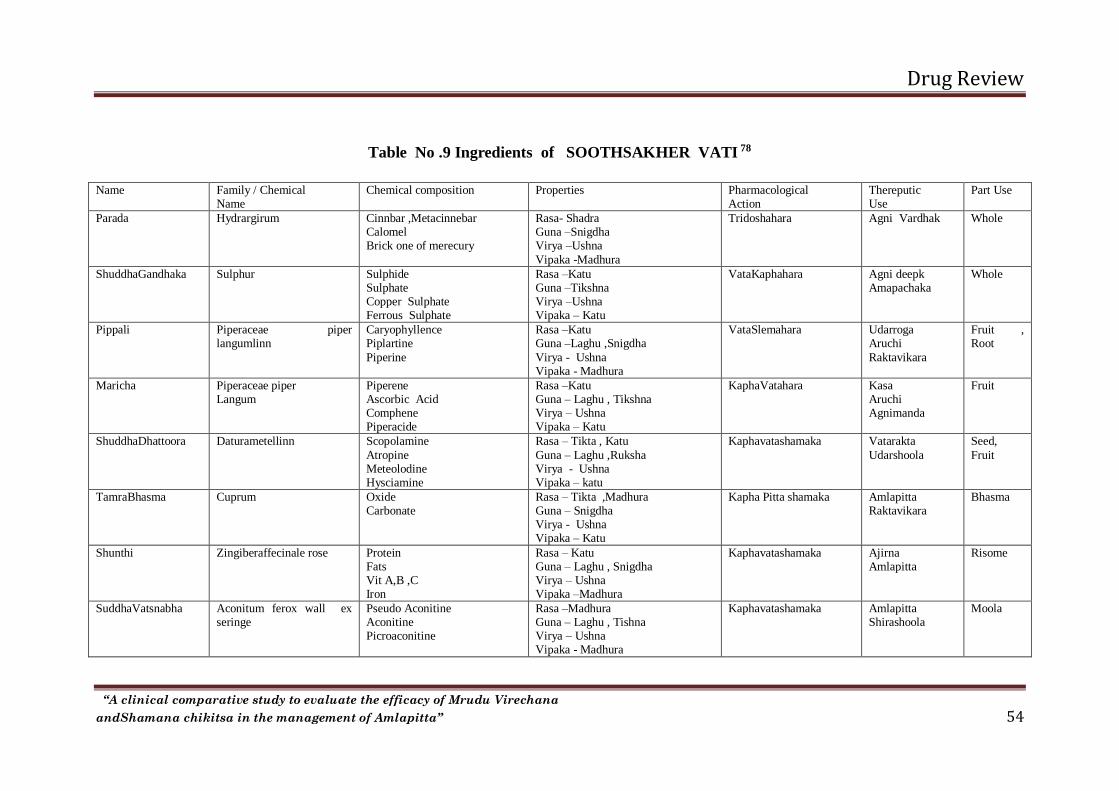
Drug Review
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 54
Table No .9 Ingredients of SOOTHSAKHER VATI 78
Name Family / Chemical Name
Chemical composition Properties Pharmacological Action
Thereputic Use
Part Use
Parada Hydrargirum Cinnbar ,Metacinnebar Calomel Brick one of merecury
Rasa- Shadra Guna –Snigdha Virya –Ushna
Vipaka -Madhura
Tridoshahara Agni Vardhak Whole
ShuddhaGandhaka Sulphur Sulphide Sulphate Copper Sulphate Ferrous Sulphate
Rasa –Katu Guna –Tikshna Virya –Ushna Vipaka – Katu
VataKaphahara Agni deepk Amapachaka
Whole
Pippali Piperaceae piper langumlinn
Caryophyllence Piplartine
Piperine
Rasa –Katu Guna –Laghu ,Snigdha
Virya - Ushna Vipaka - Madhura
VataSlemahara Udarroga Aruchi
Raktavikara
Fruit , Root
Maricha Piperaceae piper Langum
Piperene Ascorbic Acid Comphene Piperacide
Rasa –Katu Guna – Laghu , Tikshna Virya – Ushna Vipaka – Katu
KaphaVatahara Kasa Aruchi Agnimanda
Fruit
ShuddhaDhattoora Daturametellinn Scopolamine
Atropine Meteolodine Hysciamine
Rasa – Tikta , Katu
Guna – Laghu ,Ruksha Virya - Ushna Vipaka – katu
Kaphavatashamaka Vatarakta
Udarshoola
Seed,
Fruit
TamraBhasma Cuprum Oxide Carbonate
Rasa – Tikta ,Madhura Guna – Snigdha Virya - Ushna Vipaka – Katu
Kapha Pitta shamaka Amlapitta Raktavikara
Bhasma
Shunthi Zingiberaffecinale rose Protein Fats Vit A,B ,C Iron
Rasa – Katu Guna – Laghu , Snigdha Virya – Ushna Vipaka –Madhura
Kaphavatashamaka Ajirna Amlapitta
Risome
SuddhaVatsnabha Aconitum ferox wall ex seringe
Pseudo Aconitine Aconitine Picroaconitine
Rasa –Madhura Guna – Laghu , Tishna Virya – Ushna Vipaka - Madhura
Kaphavatashamaka Amlapitta Shirashoola
Moola

Drug Review
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 55
SwarnaBhasma Aurum [Au ] Gold Metallic ,Silica,Iron ,potas, sulphate ,copper
Rasa - Madhura Guna – Sheeta Virya – sheeta Vipaka - Madhura
Vata Pitta shamaka AAyuvardhaka Bhasm
ShuddhaTankana Sodium Pyroborate Sodium Pyroborate
Rasa – Katu Guna – Ruksha ,Tikshna Virya – Ushna Vipaka - Madhura
Kapha Pitta shamaka Atishar Kasa
Bhasm
ShankhaBhasma Calcium bi carbonate Sulphate Megnsium
Rasa – katu Guna –Sheeta Virya –Ushna
Vipaka –Katu
Grahi –deepanaPachana Amlapitta Gulma
Bhasm
Karchoora Curcuma zedoaria Rosc
Pitabh Starch
Rasa –Katu ,Tikta Guna – Laghu , Tikshna Virya –Ushna Vipaka – Katu
Kapha Pitta hara Aruchi Amlapitta
Kand
Twak Cinnamomnm Zeylanicum
Cinnamic Acid Tanin
Rasa – Katu ,Tikta , Madhura
Guna – Laghu , Tikshna ,Ruksha Virya- Ushna Vipaka –Katu
Pitta shamaka Aruchi Amlapitta
Twak
Ela Eletteria cardomum
Terpinyl acetate Cineale Terpincol
Rasa –Katu , Madhura Guna – Laghu , Ruksha Virya - Sheeta Vipaka - Madhura
Vatahara Swasa Kasa
Beeja
Patra Cinnamomum zeylanicum
Rasa – Madhura Guna –Laghu, Picchia Virya - Ushna Vipaka – Katu
GrahiDeepanaPachana Amlapitta Shoola Gulma
Patra
Nagakeshara Mesuaferrea Hexadeoicacid,octadecatriefoliicacid,mesuaferrol,sisterol are present in seed oil
Rasa – Katu , Tikta Guna - Laghu , Ruksha Virya – Ushna
Vipaka - Katu
Kapha Pitta Nashak Amlapitta Aruchi
Stamens ,leaf

Drug Review
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 56
Showing of Yasti madhu churna
Showing of Sootasakher vati

Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 57
METHODOLOGY
This clinical study is based on classical explanation. The Mrudhu virechana is
done with Yasthimadhu churana along with Sootashekara rasa vati as shamana
aushadi is given, which can be presented as follows
Materials And Methods
Materials taken for the study
1) Yastimadhu churana for mrudhu virechana
2) Sootashekara rasa vati as Shamana.
Preperation Yastimadhu churana :The fresh Yashtimadhu roots were collected and
were washed properly to remove mud and other physical impurities. The cleaned
roots were made into small pieces and dried in driyer at 60oC. Completely dried
pieces are made into sookshma choorna.
Sootashekara rasa vati: The detail description of the drugs of this trail yoga is
mentioned in drug review. The ingredient of Sootashekara rasa vati are shown in
Table 10 –Showing ingredients of Sootashekara Vati
Sl.no Name of Ingredient Quantity
1 Parada 1 part
2 Shuddha Gandhaka 1 part
3 Swarna Bhasma 1 part
4 Shuddha Tankana 1 part
5 Shuddha Dhattoora Beej 1 part
6 Shankha Bhasma 1 part
7 Tamra Bhasma 1 part
8 Ela 1 part
9 Tvak 1 part
10 Patra 1 part
11 Sunthi 1 part
12 Pippali 1 part
13 Nagakeshara 1 part
14 Karchoora 1 part
15 Maricha 1 part
16 Bang swarasa 1 part

Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 58
Preperation of Sootashekhar Rasa : The Kajjali is prepared by equal quantity of
Parada and Gandhaka. Than kajjiali should mixed with equal quantity of Bhasama
and churana of other drugs. Than the mixture of drugs given mardana with Bhang
swarasa for one day, then vatis are prepared in rati pramana uniformly
METHODS :
Objective :
Literary work on Amlapitta .
To evaluate the effect of Group A mrudu virechana in Amlapitta .
To evaluate the effect of Group B shaman oushadhi in Amlapitta .
To compare the efficacy of both group in Amlapitta .
Study Design :
The total number of patient are ramendely divided into two groups ,
Group A 20 patient and Group B 20 patient .
Group A: Mrudu virechana by yashti madhu choorna 6 grm with hot water
in empty stomach early morning for 7 days. After mrudu virechana , shaman
oushadhi sootashekhar rasa 2 vati bd with water for 30 days .
Group B : Shaman oushadhi sootashekhar rasa 2 vati bd with water 30 days .
Anupana : Sukoshna jala.
Study duration: Prospective clinical trials for 37 days i.e., the abservation study was
conducted. A further follow up of patients for 30 days was done the effect of yoga
was analysed according to clinical functional response before and after the treatment.
Posology :2 vati two times aday
Source ofdata :
The study were carried out on the patients attending the OPD and
IPD of AMCH and ATMH, Davangere .
Special Free camps conducted by AMCH and ATMH.

Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 59
Method of collection data:
Study will be carried out on the patients of 16-60 years of age, irrepective or
sex, religion, economical status and occupation.
About 40 patients will be selected for the study and will be divided into two
Groups, Group A & Group B , each consisting of 20 patients.
The parameter of evaluation of the study is based on clinical signs and
symptoms of Amalpitta and result will be analysed on and statistical data.
Inclusion Criteria :
Patients presenting symtoms of Amlapitta like Avipaka , Aruchi
Patient of age group between 15 to 60 yearrs were selected .
Exclusion Criteria:
Patients with other systemic diseases were excluded .
Complication which will intervene with the treatment were excluded .
Patients below 15 year and above 60 year were excluded from the study .
Diagonstic Criteria : Diagnosis were made on the cardinal sign and symptoms
of Amlapitta as explained in the classics .
Investigation :
Blood - Hb% ,TLC ,DLC ,ESR
Routne Urine examination – Sugar , Albumine , Microscopic
If needed ECG , Endoscopic , USG
Assessment of response to treatment: The state of the disease change after the
intervention was observed before, during and after the treatment. Standard methods of
scoring the symptoms likeAruchi, Avipaka,,Utklesh,Amloudgar,Hrida-Kanthadaha
was assessed before during and after the administration of shamana aushadi at the
interval of 7 days for 30 days.

Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 60
Assessment Criteria: The state of the disease Amlapitta change after the
interventions improvement was assessed by seeing the reduction in the signs and
symptoms of the disease like Avipaka,Aruchi,Utklesh,Amloudgar,Hrida-Kanthadaha.
Similarly other symptoms were also given scores on the basis of this before and after
treatment score, The statistical analysis was done using paired ‘t’ test and S.D., S.E.
and p Value were calculated.
GRADING OF PARAMETERS
Aruchi :
Patient is taking food normally without hesitation -0
Patient is taking food in moderate quantity twice a day -1
Patient is taking food in less quantity twice a day -2
Patient is taking food in less quantity once a day.-3
Patient is not taking food at all.-4
Avipaka :
No Avipak -0
Avipak occurs occasionally 2-3 times per week. -1
Avipak occurs daily but not distrube the patient -2
Avipak occurs daily with more than 2-3 Ajirna ahara lakshan’s like
Ashuddha, /Udgara / Guruta / Glani / distrube the patient -3
Avipak occurs daily which does not subside with medicine or langhana
and which disturbed the routine of patient. -4
Utklesha :
No Utklesha
Occasional episode of Utklesha -1
Frequent and prolonged Utklesha, No Vomiting -2
Utklesha; Followed by one attack of Vomitting -3
Continous Utklesha; Followed by many time vomiting-4
Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 61
Amloudgara:
No Amloudgar at all -0
Amloudgar some times during the day -1
Amloudgar during day and night but does not disturbe the patient -2
Amloudgar during day and night disturbing the patient -3
Small amount of fluid regurgitating from patient’s mouth -4
Hrid-Kanthadaha
No Daha - o
Daha in any area of udara, uras, kantha but not disturbing the patient-1.
Daha which relived by milk,cold drinks or antacids -2
Daha involving Hrita, Kantha .and relived after digestion of food or
vomiting to some extend only-3.
Daha involving major areas of abdomen or whole body like hand, feets
and does not relive by any measure mentioned above -4
Assessment of overall effect: For assessing the overall effect of the treatment, the
total scores of sign and symptoms of Amalapitta after the treatment was considered
as per the reduction in the total scores ofAvipaka, Aruchi, Utklesh, Amloudgar, Hurd-
Kanthadaha .The overall effect is calculated as under.
Major Improvement :Reduction in more than 75% of the initial score after the
treatment.
Moderate Improvement:Reduction in more than 50 % of the initial score.
Minor Improvement: Reduction more than 25 % of the initial score.
Not responded:Reduction less than 25% of the initial score.
Adopting the scoring method, symptoms of the illnesslike Avipaka, Aruchi,
Utklesh, Amloudgar, Hurd-Kanthadaha parameters are take as assessment criteria in
this study.

Methodology
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 62
STATISTICAL ANALYSIS :
Descriptive data that included mean, std. Deviations and percentages were
calculated for all the variables in each group.
Post treatment changes were assessed by paired t-test and difference between groups
by unpaired t-test.
For all tests a p-value of 0.05 or less was considered for statistical significance.
Formulae used for statistical analysis
Mean, X =x:
n i = 1,2,………………. 12.
Standard deviation 𝑺𝒅 = √∑(𝑿: −𝑿)
𝟐
𝒏−𝟏
Standard error, 𝑺𝑬 = 𝑺𝑫
√𝒏
Paired t -test 𝒕 = 𝑴𝒆𝒂𝒏 𝒐𝒇 𝒅𝒊𝒇𝒇𝒆𝒓𝒆𝒏𝒄𝒆𝒔
𝑺𝒕𝒅.𝑬𝒓𝒓𝒐𝒓 𝒐𝒇 𝒅𝒊𝒇𝒇𝒆𝒓𝒆𝒏𝒄𝒆𝒔 =
𝒅
𝒔𝒅/√𝒏
Unpaired t- test, t = Difference in means x1 - x2
Std. Error of difference combined Sd x 1/n1 + 1/n2

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 63
OBSERVATION AND RESULTS
In the present study 40 patients suffering from Amlapitta, fulfilling inclusion
criteria were selected. Patient were randomly categorized in to Group -A yastimadhu
churna with Mrudu Virechana & Sootashekar vati as shaman aushadi and Group B
sootashekara vati as shaman aushadi .
Following pages contain descriptive statistical analysis of the patients studied
along with the observation and result are listed below.
Demographic related data.
Data related to disease.
Statistically analysis of the assessment of the patients before and after the
treatment in individual group’s asses efficacy of treatment by the paired ‘t’ test.
Statistically analysis of the assessment of the patients following the unpaired
‘t’test to compare the effect of treatment in two groups.
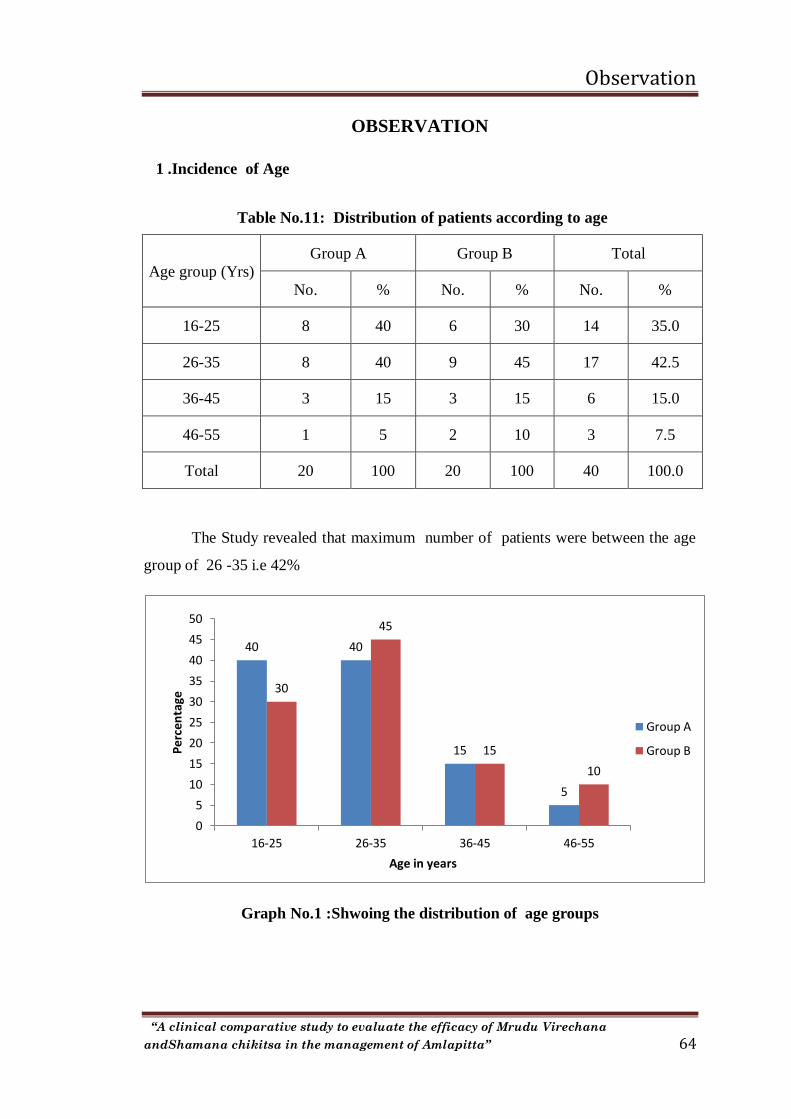
Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 64
OBSERVATION
1 .Incidence of Age
Table No.11: Distribution of patients according to age
Age group (Yrs)
Group A Group B Total
No. % No. % No. %
16-25 8 40 6 30 14 35.0
26-35 8 40 9 45 17 42.5
36-45 3 15 3 15 6 15.0
46-55 1 5 2 10 3 7.5
Total 20 100 20 100 40 100.0
The Study revealed that maximum number of patients were between the age
group of 26 -35 i.e 42%
Graph No.1 :Shwoing the distribution of age groups
40 40
15
5
30
45
15
10
0
5
10
15
20
25
30
35
40
45
50
16-25 26-35 36-45 46-55
Per
cen
tage
Age in years
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 65
2 .Incidence of Sex
Table No. 12: Distribution of patients according to Gender
Gender
Group A Group B Total
No. % No. % No. %
Male 15 75 14 70 29 72.5
Female 5 25 6 30 11 27.5
Total 20 100 20 100 40 100.0
The Sex incidence of patients in the study that majority of patients were
male i.e 72 . 5 %
Graph No.2 : Distribution of patients according to sex
0
10
20
30
40
50
60
70
80
Group A Group B
7570
2530
Per
cen
tage Male
Female

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 66
3 .Incidence of Religion
Table No.13: Distribution of patients according to Religion
Religion
Group A Group B Total
No. % No. % No. %
Hindu 18 90 20 100 38 95.0
Muslim 2 10 0 0 2 5.0
20 100 20 100 40 100.0
In the present study 38 patients were hindu is 95% .
Graph No.3 : Distribution of patients according to religion
0
20
40
60
80
100
Group A Group B
90
100
100
Per
cen
tage Hindu
Muslim

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 67
4 . Incidence of Education
Table No.14: Distribution of patients according to Education
Education
Group A Group B Total
No. % No. % No. %
Graduate 11 55 11 55 22 55.0
Illiterate 5 25 4 20 9 22.5
P Graduate 1 5 2 10 3 7.5
U Graduate 3 15 3 15 6 15.0
Total 20 100 20 100 40 100.0
In the present study majority of the graduate ie, 22 patients out of 40
patients .
Graph No.4 : Distribution of patients according to education
25
15
55
5
20
15
55
10
0
10
20
30
40
50
60
Illiterate U Graduate Graduate P Graduate
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 68
5 . Incidence of Socio-Economic status
Table No. 15: Distribution of patients according to S E S
SES
Group A Group B Total
No. % No. % No. %
L M C 3 15 1 5 4 10.0
M C 14 70 14 70 28 70.0
Poor 3 15 5 25 8 20.0
Total 20 100 20 100 40 100.0
Study of socio economic status revealed that majority of patients
belonging to Middle Class i.e 70%
Graph No.5 : Distribution of patients according to SES
0
10
20
30
40
50
60
70
M C L M C Poor
70
15 15
70
5
25
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 69
6 .Incidence of marital status
Table No.16: Distribution of patients according to Marital Status
Marital status
Group A Group B Total
No. % No. % No. %
Married 16 80 18 90 34 85.0
Un Married 4 20 2 10 6 15.0
20 100 20 100 40 100.0
Out of 40 patients registered in the study maximum 85 % of the
patients were married ie , 34 patients .
Graph No.6 : Distribution of patients according to marital status
0
10
20
30
40
50
60
70
80
90
Group A Group B
80
90
20
10
Per
cen
tage Married
Un Married

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 70
7 .Incidence of nature of work
Table No. 17: Distribution of patients according to their Nature of work
Nature of Work
Group A Group B Total
No. % No. % No. %
Laborious 12 60 14 70 26 65.0
Sedentary 0 0 3 15 3 7.5
Standing 7 35 2 10 9 22.5
Travelling 1 5 1 5 2 5.0
Total 20 100 20 100 40 100.0
Maximum 65 % of the patients had laborious work in the present study
Graph No.7 : Distribution of patients according to nature of work
0
10
20
30
40
50
60
70
Laborious Sedentary Standing Travelling
60
0
35
5
70
1510
5
Pe
rcen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 71
8 .Incidence of Manasika sthithi
Table No. 18: Distribution of patients according to Manashika Sthithi
Manashika sthithi
Group A Group B Total
No. % No. % No. %
Bhaya 4 20 6 30 10 25.0
Chinta 8 40 9 45 17 42.5
Krodha 3 15 5 25 8 20.0
Shoka 5 25 0 0 5 12.5
Total 20 100 20 100 40 100.0
In the present study , it was observed that most of the patients under
stress of more than one manasika bhava , causing Amlapitta . Maximum
number of patients i.e , 42 % were practicing chinta as manasika bhava.
Graph No.8 : Distribution of patients according to Manasika Sthithi
0
5
10
15
20
25
30
35
40
45
Bhaya Chinta Krodha Shoka
20
40
15
25
30
45
25
0
Pe
rcen
tage
Group A
Group B
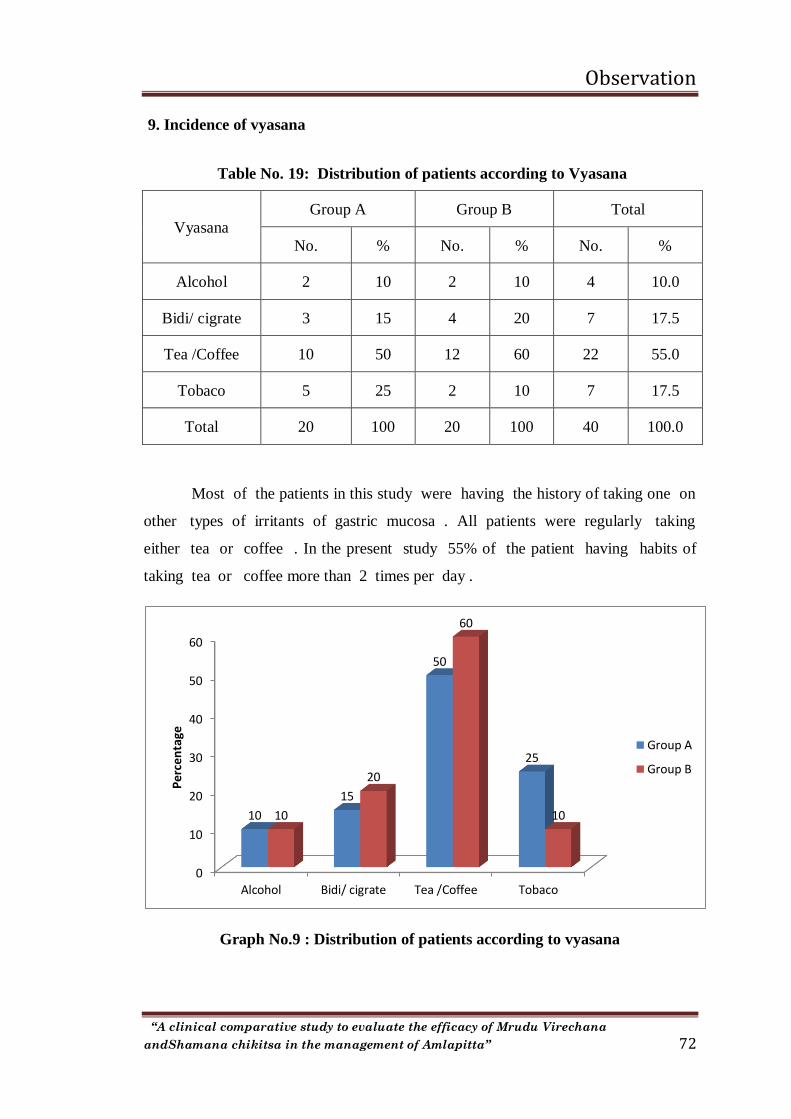
Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 72
9. Incidence of vyasana
Table No. 19: Distribution of patients according to Vyasana
Vyasana
Group A Group B Total
No. % No. % No. %
Alcohol 2 10 2 10 4 10.0
Bidi/ cigrate 3 15 4 20 7 17.5
Tea /Coffee 10 50 12 60 22 55.0
Tobaco 5 25 2 10 7 17.5
Total 20 100 20 100 40 100.0
Most of the patients in this study were having the history of taking one on
other types of irritants of gastric mucosa . All patients were regularly taking
either tea or coffee . In the present study 55% of the patient having habits of
taking tea or coffee more than 2 times per day .
Graph No.9 : Distribution of patients according to vyasana
0
10
20
30
40
50
60
Alcohol Bidi/ cigrate Tea /Coffee Tobaco
10
15
50
25
10
20
60
10
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 73
10 . Incidence of prakruti
Table No. 20: Distribution of patients according to Prakruti
Prakruti Group A Group B Total
No. % No. % No. %
P K 10 50 8 40 18 45.0
V K 6 30 4 20 10 25.0
V P 4 20 8 40 12 30.0
Total 20 100 20 100 40 100.0
Among all patients a predominance of Pitta – Kapha constitution was
observed in the patients with 45 % of evidence .
Graph No.10 : Distribution of patients according to prakruti
0
5
10
15
20
25
30
35
40
45
50
P K V K V P
50
30
20
40
20
40
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 74
11.Incidence of sara
Table No. 21: Distribution of patients according to Sara
Sara
Group A Group B Total
No. % No. % No. %
Avara 2 10 3 15 5 12.5
Madhyama 18 90 15 75 33 82.5
Pravara 0 0 2 10 2 5.0
Total 20 100 20 100 40 100.0
In the present study maximum patients were madhyama sara i.e , 82.5%.
.
Graph No.11 : Distribution of patients according to sara
0
20
40
60
80
100
Avara Madhyama Pravara
10
90
0
15
75
10
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 75
12 .Incidence of samshamana
Table No. 22: Distribution of patients according to Samhanana
Samhanana
Group A Group B Total
No. % No. % No. %
Avara 3 15 7 35 10 25.0
Madhyama 15 75 10 50 25 62.5
Pravara 2 10 3 15 5 12.5
Total 20 100 20 100 40 100.0
The present study revealed that 62.5 % of patients had madhyama
sahanana .
Graph No.12 : Distribution of patients according to samshamana
0
10
20
30
40
50
60
70
80
Avara Madhyama Pravara
15
75
10
35
50
15
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 76
13 . Incidence of satva
Table No. 23: Distribution of patients according to Satva
Satva
Group A Group B Total
No. % No. % No. %
Avara 1 5 4 20 5 12.5
Madhyama 18 90 12 60 30 75.0
Pravara 1 5 4 20 5 12.5
Total 20 100 20 100 40 100.0
Analysis of satva revealed 75 % of the patients had madhyama satva .
Graph No.13 : Distribution of patients according to satva
0
10
20
30
40
50
60
70
80
90
Avara Madhyama Pravara
5
90
5
20
60
20
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 77
14 . Incidence of satmya
Table No.24: Distribution of patients according to Satmya
Satmya Group A Group B Total
No. % No. % No. %s
Madhyama 18 90 12 60 30 75.0
Pravara 2 10 8 40 10 25.0
Avara 0 o 0 0 0 0
Total 20 100 20 100 40 100.0
The study revealed that 75 % patients were showing Madhyama satmya
i.e ., madhyama satmya .
Graph No.14 : Distribution of patients according to satmya
0
10
20
30
40
50
60
70
80
90
Madhyama Pravara
90
10
60
40
Pe
rcen
tage Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 78
15 .Incidence of kostha
Table No. 25: Distribution of patients according to Kostha
Kostha
Group A Group B Total
No. % No. % No. %
Krura 2 10 3 15 5 12.5
Madhyama 13 65 12 60 25 62.5
Mrudu 5 25 5 25 10 25.0
Total 20 100 20 100 40 100.0
In the present study maximum patients is having madhyama Kostha i.e ,
62 % .
Graph No.15 : Distribution of patients according to kostha
0
10
20
30
40
50
60
70
Krura Madhyama Mrudu
10
65
25
15
60
25
Pe
rcen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 79
16 . Incidence of vyayama shakti
Table No. 26: Distribution of patients according to Vyayama
Vyayama
Group A Group B Total
No. % No. % No. %
Avara 1 5 5 25 6 15.0
Madhyama 15 75 12 60 27 67.5
Pravara 4 20 3 15 7 17.5
Total 20 100 20 100 40 100.0
In the present study maximum patients is having Madhyama i.e 67% .
Graph No.16 : Distribution of patients according to vyayama shakti
0
10
20
30
40
50
60
70
80
Avara Madhyama Pravara
5
75
2025
60
15
Pe
rcen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 80
17 . Incidence of Occupation
Table No. 27: Distribution of patients according to Occupation
Occupation
Group A Group B Total
No. % No. % No. %
House work 3 15 5 25 8 20.0
Job 3 15 2 10 5 12.5
Painting 3 15 2 10 5 12.5
Study 2 10 3 15 5 12.5
Worker 9 45 8 40 17 42.5
Total 20 100 20 100 40 100.0
In the Present study maximum patients is having worker i.e 42 % .
Graph No. 17 : Distribution of patients according to occupation
0
5
10
15
20
25
House work Job Painting Study
15 15 15
10
25
10 10
15
Per
cen
tage
Group A
Group B

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 81
DATA RELATED TO DISEASE
1 . Showing incidence of Etiological factor :
Table No .28 Showing the incidence of etiological factors in 40 patients of
Amlapitta .
Sl.
No.
Etiological Factors Total
1 Aharaja
2 Virudhashan 35 %
3 Amlarasatmaka 20 %
4 KatuRasatmaka 10 %
5 Ushna 45 %
6 Fanita 70 %
7 Dadhi 65 %
Vihara
1 Vegadharana 45 %
2 Atisnana 10 %
3 Divaswapna 60 %
4 Santapa 55 %
Manasik Bhava
1 Bhaya 25 %
2 Chinta 42 %
3 Shoka 12.5 %
4 Krodha 20 %

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 82
2 . Showing incidence of predominant of Rasa sevana in 40 patients of
Amlapitta :
In this study maximum patients i.e , 35 % taking katu rasa pradhana
dravya in their daily dite .
Table No . 29 Showing incidence of Rasa sevana
Predominant
ofRasa
sevana
Group A Group B Total
No . Percentage No . Percentage No . Percentage
Madhur 5 25 6 30 11 27.5
Amla 2 10 3 15 5 12.5
Lavana 1 5 02 10 3 7.5
Katu 8 40 6 30 14 35
Tikta 3 15 2 10 5 12.5
Kashya 1 5 01 5 2 5
3 .Incidence of water intake in Amlapitta patients :
In this study maximum patients i.e ,70 % taking 1- 2 liter water in their
daily dite .
Table No . 30 Showing incidence of water intake
IN TAKE
WATER
Group A Group B Total
No . Percentage No . Percentage No . Percentage
< 1 2 10 0 0 2 5
1-2 14 70 14 70 28 70
2-3 4 20 6 30 10 25
>3 0 0 0 0 0 0

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 83
4 .Incidence of Duration of Symptoms :
Table No . 31 Distribution of Patients according to duration of symptoms
Duration of
Symptoms
Group A Group B Total
No . Percentage No . Percentage No . Percentage
0-1 6 30 8 40 14 35
1 – 2 8 40 8 40 16 40
2 – 3 6 30 4 20 10 25
In this study maximum patients i.e, 40% were having symptom of
amlapitta from 1 – 2 months .
5. Incidence Mode of onset of Amlapitta :
Table No .32 Distribution of patients according to Mode of Onset
Mode of
onset
Group A Group B Total
No . Percentage No . Percentage No . Percentage
Sudden 10 50 10 50 20 50
Gradual 10 50 10 50 20 50
In this study both group of sudden and gradual patients i.e, 50% were
having sympom of Amlapitta .

Observation
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 84
6 . Incidence of Relieving factor of Amlapitta :
Table No. 33Distribution of patients according to Relieving factor
Relieving
Factor
Group A Group B Total
No . Percentage No . Percentage No . Percentage
Food 10 50 11 55 21 52.5
Exercise 6 30 4 20 10 25
Seasonal
Variation 4 20 5 25 9 22.5
Others 0 0 0 0 0 0
In this present study 52 . 5 % patients reliving factor of food of
Amlapitta .

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 85
RESULTS
Effect of Mrudhu Virechana with Yasthi Madhu Churna for 7 days
followed by shaman Aushadhi Soothsakher Vati 37 days in A group and
Shaman Aushadhi Soothsakher Vati for 30 days in B group .
Effect of Archi in group A :
Table No. 34 : Effect on Aruchi in Group – A
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T p
Aruchi 3.35 1.30 2.05 61% 0.94 0.21 9.71 <0.001
HS
Effect of treatment with Yasthi Madhu churna and Soothsakher Vati on
Aruchi before and after the treatment in 20 patients of Amlapitta are given below .
In group A statistical analyses revealed that the mean Aruchi score of Amlapitta
Which was 3.35 before the administration of yasthi Madhu Churna and
Soothsakher Vati was reduced to 1.30 after the treatment . The change is statistical
significant . Further details with standard deviation , standard error of mean ‘t’ and
‘p’ values are given below .
Effect of Archi in group B :
Table No. 35 : Effect on Aruchi in Group – B
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T p
Aruchi 3.65 1.65 2.00 56% 1.17 0.26 7.65 <0.001
HS

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 86
As assessement of Aruchi in 20 patients of Amlapitta before and after the
treatment with Soothsakher vati showed marked reduction in the mean of Aruchi
from 3.65 to 1.65 . This change is found to be statistically highly significant .
Effect on Avipaka in Group – A :
Table No. 36 : Effect on Avipaka in Group – A
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Avipaka 3.35 1.20 2.15 64% 0.99 0.22 9.73 <0.001
HS
As revealed by the statistical analysis , the reduction in the symptom
Avipak before and after the treatment in yasti Madhu churna and Soothsakher vati
are given below . The mean score observed in Avipak before administration of
treatment was 3.35 which reduced to 1.20 after the treatment . This improvement in
the symptom after the treatment is highly stastically significant , particularis of
statistical analysis are given below .
Effect on Avipaka in Group – B :
Table No. 37 : Effect on Avipaka in Group – B
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Avipaka 3.60 1.50 2.00 56% 1.26 0.28 7.12 <0.001
HS
The severity of the symptom Avipak assessed before and after the
treatment showed very significant improvement with reduction in the mean score
from 3.60 to 1.50 in the patients of Amlapitta after completion of treatment in group

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 87
B. This change in group B is statistically highly significant . Detailed data with
statistically analysis are given below .
Effect on Utklesha in Group – A :
Table No. 38: Effect on Utklesha in Group – A
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Utklesha 2.80 0.85 1.95 70% 1.00 0.22 8.73 <0.001
HS
According to statistic the reduction in the symptom Utklesh before and after
the treatment by Yasthi Madhu churna and soothsakher vati in the patients of
Amlapitta . showed reduction in the mean score was 2.80 which was reduced to 0.85
after the completion of treatment . Hence It is statistically highly significant .
further details are given below .
Effect on Utklesha in Group – B :
Table No. 39 : Effect on Utklesha in Group – B
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Utklesha 2.75 0.60 2.15 78% 1.14 0.25 8.46 <0.001
HS
On examination the effect of Soothsakher vati on the symptom Utklesh
before and after the treatment was documented.The statistical analysis of the data
in group B revealed the mean score of the symptom utklesha before the treatment was
2.75 which was reduced to 0.60 after the treatment .This change is statistically highly
significant.

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 88
Effect on Amlodgara in Group – A :
Table No. 40: Effect on Amlodgara in Group – A
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Amlodgara 2.75 0.50 2.25 82% 1.07 0.24 9.40 <0.001
HS
As revealed by the statistical analysis , the reduction in the symptom
Avipak before and after the treatment in yasti Madhu churna and Soothsakher vati
are given below. The mean score observed in Avipak before administration of
treatment was 2.75 which reduced to 0.50after the treatment . This improvement in
the symptom after the treatment is highly stastically significant , particularis of
statistical analysis are given below .
Effect on Amlodgara in Group – B :
Table No. 41 : Effect on Amlodgara in Group – B
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Amlodgara 3.20 0.60 2.60 81% 1.10 0.24 10.61 <0.001
HS
An assessement of Amloudgara in 20 patients of Amlapitta before and after
the treatment with soothsakher vati showed with Soothsakher Vati showed marked
reduction in the mean of Amloudgar score 3.20 to 0.60 . This change is found to be
statistically highly significant are given below .

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 89
Effect on Hrikanth Daha in Group – A :
Table No. 42 : Effect on Hrikanth Daha in Group – A
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Hrikanth
Daha 2.90 0.45 2.45 84% 1.05 0.23 10.43 <0.001
As revealed by the statistical analysis , the reduction in the symptom
Hridkanthadaha before and after the treatment in yasti Madhu churna and
Soothsakher vati are given below . The mean score observed in Avipak before
administration of treatment was 2.90 which reduced to 0.45 after the treatment .
This improvement in the symptom after the treatment is highly stastically significant ,
particularis of statistical analysis are given below
Effect on Hrikanth Daha in Group – B :
Table No. 43 : Effect on Hrikanth Daha in Group – B
Parameter
Mean Reduction
in mean
%
reduction
Paired t-test
BT AT4 SD of
mean
SE of
mean T P
Hrikanth
Daha 3.35 0.50 2.85 85% 0.99 0.22 12.90 <0.001
The severity of the symptom Hridkanthadaha assessed before and after
the treatment showed very significant improvement with reduction in the mean
score from 3.35 to 0.50 in the patients of Amloudgar after completion of treatment in
group B. This change in group B is statistically highly significant . Detailed data
with statistically analysis are gven below

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 90
UNPAIRED ‘t’ test :
Comparison of treatment on Archi between group A and group B :
Table No. 44 : Comparison of effect of treatment on Aruchi between two groups
Groups No.of
patient
BT –
AT
mean
Difference
in means SD SEM PSE
Unpaired t-test
t P Remarks
A 20 2.05 0.05
0.94 0.21 0.34 0.15 0.88 NS
B 20 2.00 1.17 0.26
Graph No.18: Comparison of effect of treatment on Aruchi in two groups
In the present study the effect on Aruchi in the patients of Amlapitta was
observed . Marked reduction was observed in both the group . The difference in
mean Aruchi score after administration of Mrudhu Virechana and Shaman Aushadi
in group A was 2.05 and this mean score was more than the difference in mean
Aruchi scores of group B which was 2.00 ,this difference in mean score is stastically
not significant .Here group A is better than group B .
0.0
0.5
1.0
1.5
2.0
2.5
Group A Group B
2.05 2.00

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 91
Comparison of effect of treatment on Avipaka between two groups :
Table No. 45 : Comparison of effect of treatment on Avipaka between two
groups
Groups No.of
patient
BT –
AT
mean
Difference
in means SD SEM PSE
Unpaired t-test
T P Remarks
A 20 2.15 0.15
0.99 0.22 0.36 0.42 0.68 NS
B 20 2.00 1.26 0.28
Graph No.19 : Comparison of effect of treatment on Avipaka in two groups
In the present study the effect on Avipak in the patients of Amlapitta was
observed . Marked reduction was observed in both the group . The difference mean
score in group A was 2.15 this mean is comparatively more than group B which
was 2.00 this difference in mean score is stastically not significant

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 92
Comparison of effect of treatment on Utklesha between two groups :
Table No. 46 : Comparison of effect of treatment on Utklesha between two
groups
Groups No.of
patient
BT –
AT
mean
Difference
in means SD SEM PSE
Unpaired t-test
t P Remarks
A 20 1.95 0.20
1.00 0.22 0.34 0.59 0.56 NS
B 20 2.15 1.14 0.25
Graph No.20: Comparison of effect of treatment on Utklesha in two group
In the present study the difference in mean Utklesh score in group A was
1.95 .This is compartitively more than the difference in mean utklesh score in group
B which was 2.15 on statistical analysis with un paired ‘t’test it was revealed that
this difference in mean Utklesh score is highly significant .
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
Group A Group B
1.952.15

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 93
Comparison of effect of treatment on Amalodgara between two groups :
Table No. 47 : Comparison of effect of treatment on Amalodgara between two
groups
Groups No.of
patient
BT –
AT
mean
Difference
in means SD SEM PSE
Unpaired t-test
T P Remarks
A 20 2.25 0.35
1.07 0.24 0.34 1.02 0.31 NS
B 20 2.60 1.10 0.24
Graph No.21: Comparison of effect of treatment on Amalodgara in two groups
In the present study the difference in mean Amalodgara score in group A
was 2.25 .This is compartitively more than the difference in mean Amlodgara score
in group B which was 2.60 on statistical analysis with un paired ‘t’test it was
revealed that this difference in mean Utklesh score is highly significant .
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Group A Group B
2.25
2.60

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 94
Comparison of effect of treatment on Hridkanth Daha between two groups :
Table No. 48 : Comparison of effect of treatment on Hridkanth Daha between
two groups
Groups No.of
patient
BT –
AT
mean
Difference
in means SD SEM PSE
Unpaired t-test
t P Remarks
A 20 2.45 0.40
1.05 0.23 0.32 1.24 0.22 NS
B 20 2.85 0.99 0.22
Graph No. 22: Comparison of effect of treatment on Hrikantha Daha in two
groups
In the present study the difference in mean Hridkanthadaha score in group A
was 2.45 .This is compartitively more than the difference in mean Hridkanthadaha
score in group B which was 2.85 on statistical analysis with un paired ‘t’test it
was revealed that this difference in mean Hridkanthadaha score is non significant .
0.0
0.5
1.0
1.5
2.0
2.5
3.0
Group A Group B
2.45
2.85

Results
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 95
Overall assessment in Group A and Group B :
Table No 49 - Overall assessment in Group A and Group B
Response in Percentage Group A Group B
No Percentage No Percentage
Major improvement 8 40% 6 30%
Moderate improvement 7 35% 7 35%
Minor improvement 4 20% 5 25%
Not improved 1 5% 2 10%
Graph No. 23 :Overall assessment in Group A and Group B
Analysis of the overall effects in Group A indicate that 40% of patients
showed major improvement of the illness, 35% of patients showed moderate
improvement where as other 20% of patient showed minor improvement. And 5% of
patients Not improved .
Similarly analysis of the overall effect in the Group B indicate that 30% of
patient showed major improvement of the illness, 35% of patient showed moderate
improvement, where as, 25% of patients showed minor improvement, and 10 % of
patients showed Not improved .
0%
5%
10%
15%
20%
25%
30%
35%
40%
Maj Imp Mod Imp Minor Imp Not imp
40%
35%
20%
5%
30%
35%
25%
10%
Group A
Group B

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 96
DISCUSSION
Discussion is must in each and every aspect of life to add new dimensions and
there by improving its understanding. Here a humble attempt has been made to
discuss the entire work done under following headings.
• Discussion on concept of disease.
• Discussion on materials and method
• Discussion on observation made
• Discussion on the result obtained.
• Mode of action of Yashti Madhu Churna and Soothsakher rasa Vati
DISCUSSION ON CONCEPT OF DISEASE
Today’s life style is completely changed by all means. Our diet pattern, life
style and behavioural pattern is changed and it is not suitable for our normal
physiology of digestion of body. We had developed western culture and it is more
harmful to us. We adopted their diets, behavioral pattern and this is the reason for
most of the diseases. Especially, Amlapitta are mainly caused by dietetic pattern
which is related to our digestion. The food articles which are not according to normal
code and conducts, creates this problem. Western people are mostly suffering from
gastric problem in comparison to Indians. It seems that our old pattern of diet and
behaviour was up to mark for nourishing and carrying physiological processes.
Amlapitta is one of the disorders caused by faulty dietetic and behavioural
pattern. Amlapitta is not a disorder caused only by the habitual, irregular diet schedule
and activities, but also as a result of physiological and psychological aberrations. The
increasing rate of Amlapitta presents a constant challenge to research workers of
Ayurveda.
Charaka Samhita is a first recorded medical literature describing the disease in
systemic pattern. Though the disease Amlapitta is not explained in it as a full-fledged
disease but there are several references regarding Amlapitta. Here discussion was
done on Historical review, Nidana, Porvarupa, Rupa, Samprapti, chikitsa and Pathya.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 97
Sushruta and Vagbhata do not follow the Charkas view and even they did not
mentioned the word ‘Amlapitta’ in Samhita. Charaka has given vivid description of
diseases of Annavaha srotas in Grahani chapter. Kashyapa is the first person, who
described the disease Amlapitta, so elaborately and gives the due importance for its
management.
Madhavakara has described the disease separately by giving a full status to
disease Amlapitta. Srikanthadatta describes the disease by giving different quotation.
Later workers of Sangraha Kala followed the same as Madhava, Kashyapa and
Bhavamishra added Sleshma pitta as one more type. Gastritis,Hyperacidity and non-
ulcer dyspepsia have been correlated with Amlapitta by several scholars of Ayurveda.
Kashyapa and Madhvakara have given the long list of Nidanas of Amlapitta.
They have different opinion in giving the etiological factors. Kashyapa has mentioned
the Nidanas which represents the involvement of all three doshas, means he gives the
list of Nidanas which are responsible for provocation of Tridoshas, Where as
Madhavakara has mainly given the Pitta prakopaka factors. In the Nidanas mentioned
for Amlapitta, there is stated the strong role of Manasika factors too. Mental stress
and strain is related with digestion and metabolism and thus it is related with disease.
Amlapitta too, as it produces Ama as mentioned by Charaka.
Factors responsible for manifestation of the disease of Annavaha srotas are
almost similar. Diet which is against Ashtavidha Ahara vidhi vishesayatana, dietetic
code and conduct are mostly responsible for most of the disease.
These factors mostly perform the function of Agnidushti, Dosha Prakopa,
Kha-vaigunya and Dushya daurbalya. The Nidanas mostly disturb the digestion
process and are responsible for such diseases.
Viruddhahara, Diwaswapa, Antarodaka Pana, Vidahi Anna, Sheetajalapana
are the few common factors mentioned by all Acharyas. Mandagni or Agnidushti
caused by any nidana is responsible for such diseases. This first vitiate the doshas and
further dushya and samprapti progresses.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 98
Kashyapa has mentioned Rasa as a dushya of disease Amlapitta. The disease
involves mainly Rasavaha and Annavaha srotas. The Purvarupa of disease is not
mentioned in any classics..
Madhavakara has given general symptom of Amlapitta as Avipak, Klama,
Utklesh, Amloudgara, Gourava, Hritkanthadaha, Aruchi etc. It is mostly Chirakari in
nature. This is caused by Jivha-Laulya, as patients are aware of the Nidanas and still
he tries to consume the nidana. When the disease progresses it leads into Dhatugatatva
and creates complications like Parinama Shula etc.
Charaka has given the detailed description of digestion process and described
vividly the samprapti of diseases of Annavaha srotas in Grahani roga. Kashyapa has
described the samprapti of Amlapitta, he says that any one dosha among vatadi after
their provocation causes mandagni and if unwise person consume any food in such
condition it leads into vidagdha state and if it mixes with Pitta produces the disease
Amlapitta. Madhavakara as usual has not given the samprapti of Amlapitta.
Madhavakara has accepted the pitta as arambhaka dosha of disease, which is also
supported by Charaka in Grahani. Kashyapa has mentioned the involvement of three
doshas in this disease.
The Samprapti of Annavaha srotas disorder constitutes the different stages and
each stage has been accepted as a separate disease entity like Ajirna, Amlapitta,
Parinama Shula etc.
There are two types of Amlapitta; Urdhvaga and Adhoga mentioned in
classics. Madhavakara has mentioned three more type as vatika, vata-kapha and
kapha. Kashyapa has mentioned vatolvana, pittolvana and kapholvana types.
The similar treatment of Amlapitta has been mentioned by all the Acharyas.
Vamana and Virechana have been given as a shodhana process followed by Basti.
As Pitta and kapha dosha are a chief dosha involved in the disease; The selection of
shamana drug, it should have madhura and tikta rasa, sheeta virya, laghu and snigdha
property and madhura vipaka..
So for the shaman chikitsa and Mrudu virechana,soothsakher vati is selected
as its maximum drugs are madhura and tikta in rasa, virya is samashitoshna , laghu

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 99
and snigdha guna and kapha-pitta shamaka karma. And Yashti Madhu Churna is
madhura in Rasa and virya is Sita , guru and snigdha and tridoshahara karma .
Complications of Amlapitta not described by ancient acharyas except
Kashyapa. He included shula along with other symptoms as complication. Jwara,
Atisara, Pandu, Shula, Shotha, Aruchi, Bhrama are the upadravas mentioned by
Kashyapa.
Pathya in this diseases form an important part of treatment and non-
compliance with pathya, may make this disease incurable. A long list of Pathya for
Amlapitta has been mentioned in Kashayapa Samhita and other sangraha granthas.
Discussion on material and methods :
A Clinical comparative study to evaluate the efficacy of Mrudhu virechana
and Shaman chikitsa in the management of Amlapitta.
In Brahatriya direct reference of Amlapitta is not available but in Laghutriya and
others ayurvedic classics virechaha and shaman chikita are mentioned in the
management of Amlapitta disease. In yogratnakar Amlapitta adhikara acharya has
mentioned sootashekara rasa vati which shows its important is Amlapitta disease.
Rationality behind selection of the treatment :
1) Yasthi Madhu Churna: Ingredients of this preparation possess madhura
Rasa, Seetha virya , guru and snigdha guna and tridoshahara karma. And it is
indicated as best mruduvirechaka
2) Soothsakher rasavati : Its maximum drugs are madhura and tikta in rasa,
virya is samashitoshna , laghu and snigdha guna and kapha-pitta shamaka karma
Posology : Yastimadha churana 6gms or according to kosta with water. Sootashekara
rasa vati 2 vati bd with suksshana jala.
Plan of study : In the present study a total of 40 patients suffering from the disease.
Amlapitta were taken and were selected between the age group of 15-60 years
irrespective of sex, religion etc.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 100
They were randomly divided into two groups. Twenty patient were treated
with yasthimadhu churna for mrudu virechana for 7 days after sootashekara rasa vati
for 30 days and 20 patients were treated with the sootashekara rasa vati for 30 days as
shaman chikitsa.
Inclusion and exclusions criteria:
Patient of both gender were selected for the study between the age group of
15-60 years. Patients presenting with classical sign and symptoms of amlapitta like
Aruchi, Avipak, Utklesh, Amloudgar, Hrida-Kanthadaha were selected for the study.
Patients with other major systemic disorder are excluded.
Diagnostic criteria and assessment criteria :
Diagnosis was based on cardinal signs and symptoms of Amlapitta explained
in the classics. Assessment of lakshnas eg. Avipaka, Aruchi, Utklesh, Amloudgar
Hrida-Kanthadaha was made by grading them and assessed before during and after
the treatment.
Investigation :
1) Blood – Hb% ,TLC ,DLC, ESR
2) Routine urine examination – Sugar , Albumin ,Microscopic
4) if needed ECG , Endoscopic , USG
Discussion on observation:
The observation made on 40 patients of Amlapitta is being discussed here seperately.
Age : Maximum number of patients 42.5%were belonging to 26 - 35 age group
followed by 35.% in 16- 25 years. This indicates that the middle age populations are
affected by this disease more, which is Pitta predominant period of life. This Pitta
predominance makes disease chronic and Krichha sadhya.
Sex : Out of total 40 patients, 72.5% were male. This may be due to faulty dietary
habit, increased stress and strain among males and also due to habits like smoking,
pan etc.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 101
Religion : Maximum 95% patients were Hindu. This may be due to that this region
belongs to more Hindu population and patients from this community were attending
the O.P.D.
Marital Status : Maximum 85% patients were married, because this status is related
to middle age group. Family involved patients were under stress due to various
reasons.
Occupation : Maximum 42% patients were labour (poor). This reflects the general
trend of people attending the hospital. This high incidence may be due to irregular
diet habits among these groups and improper diet.
Educational Status : In this study 55% patients were educated. This incidence is
maximum in educated people due to hurried and worried life, irregular diet habit etc.
Socio-economic Status : 70% patients were from middle class. One reason for this
may be poor peoples are generally attending O.P.D. and secondly due to inadequate
diet pattern, As balanced diet is required for gastric protection. Lower classes people
are generally consuming the more masala diet which provoke the pitta-kapha dosha
predominantly.
Deha Prakruti : 45% patients were having Pitta - Kapha Prakruti and 30 % had vata-
pitta Prakruti.
Sara, Satva, Samhanana : Maximum 82.5% patients were having madhyama sara,
75% patients were madhyama satva and 62.5% patients had madhyama samhanana.
This reflects the general sara, satva, samhanana in the society and this can not be
correlated to disease.
Vyama Shakti : 67.5% were having madhyam vyayama shakti, it does not have any
reaction with disease, which shows that disease has mild progression and not causes
reverse dhatukshaya leading to daurbalya.
Satmyata : Maximum 75% patients were having madhyama satmya.
Kostha : 62.5% patients were having madhyama and 25%patients were having
Mrudu kostha. madhyama kostha is due to kapha. This is responsible for weak
digestion which ensues in diseases.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 102
Vyasana : All patients were taking either tea or coffee. 17.5% and 17.5 patients were
using smoking and tobacco and10% were taking alcohol. These factors are mostly
irritant to gastric mucosa and thus cause daurbalya of amashaya along with vitiation
of dosha mainly pitta-kapha.
Ahara : 35% of patients were consuming Virudhashan,, 45% were having ushna, .
Maximum patients were having one of the faults in their eating habits. This is
responsible for vitiation of dosha which leads into agni-dushti and establishment of
disease, its exacerbation and relapses.
Vihara : 60% were having diwaswapa , 55% patients were having santapa and 45%%
patients were having vegadharana. These all things are responsible for improper
digestion and vitiation of doshas, leading to ama stage.
Manas bhavasa : 42% were having chinta, 20% had krodha and 12.5% had shoka.
Most of the patients were suffering from mental tension and this is responsible for
improper digestion which leads to ajirna like condition as mentioned in ayurvedic
classics. For the process of digestion our manasika bhavas should be under control.
Duration : 40% patients were having symptoms of Amlapitta 1- 2 months and 70%
patients had the symptoms sinces 1 month and 5% from 2-3 months. As this is not
routine life disturbing disease, patients initially does not care of mild symptoms and
keep them on self medication once prescribed by physician just as antacid, milk, cold
drink. They are attending hospital lately and this disease is more over chronic in
nature.
Follow up: will be done after 30 days after completion of treatment. Reoccurrence of
symptom were seen in few patients with respect to disease frequency in comparison
with after completion of treatment scores.
Discussion on result:
The assessment of result was made by adopting the standard methods and
scoring was given to the sign and symptoms of the disease and was assessed
statistically to see the significance. The effect of the therapies on the individual signs
and symptoms are being discussed under the separate heading.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 103
Effect on Aruchi : It was observed in almost all the patients of both groups.61%
result was observed in group A and 56% result was observed in group B in tsshe
symptom of Aruchi. Group A shows comparatively good results in Aruchi.
Effect on Avipaka : This is the symptom of Agnidushti, but it was mostly observed
in patients of Amlapitta.64% relief was observed in group A and 56% result in group
B in Avipaka symptom. It is highly significant result at the level of P<0.001. Here
group A is good result.
Effect on utklesh : Utklesh either occasionally or daily was observed in maximum
patients and this may be due to nauseatic feeling due to the pathogenesis of the
disease. 70% result was observed in group A and 78% relief in group B. This result is
statistically highly significant at the level of P<0.001in both groups. Again group B
shows good results.
Effect on amlodgara : This is the general and mostly observed symptom of the
disease Amlapitta. 82% relief was observed in group A while 81% improvement was
observed in group B. The analysis of the result was statistically highly significant in
both groups. Group A showed comparatively good result but not very much
difference in both groups.
Effect on Hridkanth daha : Daha is very troublesome symptom of disease
Amlapitta. In this symptom 84% relief was observed in group A and 85% relief was
observed in group B. However, the statistical data suggests statistically highly
significant in relieving the symptoms Hridkanta- daha at the level of P<0.001 in both
the groups. Obviously the result provided by group B was better in comparison to
group A, daha is mainly due to the involvement of pitta and rasa srotasa maximum
drug of group B are tikta and madura rasa pradhana dravya reduces pitta and Katu
rasa dravyas reduces Kapha , which was the reason of difference in effect
observed.
Effect on amlodgara : This is the general and mostly observed symptom of the
disease Amlapitta. 82% relief was observed in group A while 81% improvement was
observed in group B. The analysis of the result was statistically highly significant in
both groups. Group A showed comparatively good result but not very much
difference in both groups.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 104
Overall assessment: Analysis of over all effect of the treatment in the patients of
Amlapitta in group A i.e Yashti madhu churna and soothsakher vati revealed that in
group A 40 % cases showed Major improvement , 35% cases Moderate
improvement , 20% cases Minor improvement and 5% cases Not improved .
In group B,30% cases showed Major improvement, 35% cases showed
moderate improvemet ,25% Minor improvement and 10% cases Not improved .
The administration of Yashti Madhu churna and soothsakher rasa vati in A
group for 37 days and soothsakher rasa vati in B group for 30 days shown good
therapeutic effects and the severity of illness therefore had been markedly
reduced . Further the comparison of the therapeutic effect in two groups showed
better improvement in group A .
None of the patients in both the groups developed any complications, or
any untowards symptoms or any side effects during the course of treatment
and therefore these treatment modalities are safe and are of the therapeutic
value .
PROBABLE MODE OF ACTION OF YASTIMADHU CHURNA AS MRUDU
VIRECHAKA
The Aashaya involved in this disease is Aamashaya . The dosha involved is
mainly Pitta, which includes the Pachaka Pitta of Amashaya and Achcha Pitta of
Pittashaya and the Dushya is Rasa. Considering these entire factor it was tried to give
mrudu Virechana to remove the vitiated Dosha, which will be having an ideal
cleansing action on Pitta. The process of Virechana may be able to expel the
excessive Dravata of Pitta and Pitta present in rest of Avayavas can be eliminated out.
Rasa Dushti can be corrected by this process. After the process of Virechana, the
Agni, digestive power is increased so it is beneficial for further digestion. After
mrudu Shodhana patient usually felt lightness. Even just after mrudu Virechana
process there is reduction in severity of symptoms. Aruchi, Avipaka,
Amlodgara,Utklesha, and hrthkantadaha sign and symptoms were lessened just after
Virechana process, which helps in further Shamana therapy, as it is corrected earlier.

Discussion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 105
PROBABLE MODE OF ACTION OF SOOTASHEKARA RASA VATI ON
AMLAPITTA
The contents of sootashekara rasa Vati are Laghu and Ruksha in property.
There is increase of Drava Guna in Amlapitta. Kledaka Kapha and Pachaka Pitta are
Drava in dominancy. So Laghu-Ruksha Guna performs the function of Dravansha -
Shoshana. This formulation is Tikta dominant and it performs the functions of
Pachana rather than Deepana. Tikta Rasa helps in Shoshana of Jala dominant
substances it includes Kleda, Meda, Vasa, Lasika, Pitta and Kapha. Tikta-Kashaya
Rasa help in pacifying the Kapha-pitta both. In these two rasa Tikta is better as it is
Laghu and it does not stagnate the Ama. It performs the function of Pitta-Sleshma
Shoshana as described by Charaka. “Tikta –Vishadyati” can be observed throughout
gastrointestinal tract (G.I.T.).
Conclusion
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 106
CONCLUSION
The purpose of this present study was Based on the conceptual analysis and
observation made in the clinical study, the following conclusion were drawn after
logical interpretation of the results obtained in the clinical study which are listed
below
Amlapitta is such pathological condition or disease in which the pitta
exteeds in normal level. Due to etilogical foctors Amlaguna of Pitta
increases which leads to Vidagdhata of ingested food and finally Amlodgara,
Hridkanthadaha utklesha etc., signs and symptoms are produced
In Brihattrayi Amlapitta has not been considered as a separate disease entity.
But Kashyapa has described Amlapitta as a separate disease. After Kashyapa,
Madhavakar has described elaborately with its two clinical subtypes i.e.
Urdhvaga and Adhoga Amlapitta.
Amlapitta is a commonly occuring psychosomatic disease.
Amlapitta cannot be correlate with a single disease of modern medicine. Some
diseases like Gastritis, Hyperacidity. Non-ulcer dyspepsia etc. show some
similarity to causes, some signs and some symptoms of Amlapitta.
It is well observed that in Group A yastimadhu churna and sootashekara rasa
vati provide better relief in the signs and symptoms of the disease amlapitta
when compared to Group B sootashekara rasa vati only. Inter group
comparison of statistical data proved to be statistically nonsignificant.
No complications were observed in any patient during the study period
Recommendation for the further studies :
The short treatment period did not suffice for total subsidence of all laksana.
This study can be carried out in further studies for better objective analysis

Summary
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 107
SUMMARY
The thesis entitled“A clinical comparative study to evaluate the efficacy of
Mrudu virechana and shaman chikitsa in the management of Amlapitta” comprises of
four parts i.e. Conceptual study, Clinical study, Discussion, Summary and
Conclusion.
In the first Section a brief introduction is given in the beginning of the
dissertation which deals with the need of the study, reason for the selection of the
disease Amlapitta, aims and objectives.
Part I: Conceptual study
The Conceptual study is divided into 2 parts viz Disease Review and Drug
Profile. In Disease Review, description of Amlapitta in details including its historical
back ground, review of previous works, Nidana, Samprapti and its ghataka,
Purvarupa, Rupa, Varieties, Sapeksha Nidana, Sadhyasadhyata and Chikitsa Sutra.
After the Ayurvedic description, modern interpretation of Amlapitta with Gastritis,
Hyperacidity, Non-ulcer dypepsia have been described.
The drug profile part deals with the review of Yastimadhu and sootashekara
rasa vati contents. In this section the detailed description about Name, Family,
Chemical name, chemical composition, Properties and Pharmacological action of
above drugs have been mentioned.
Part II: Clinical study
The materials and methods including selection of patients for study, plan of
study, assessment criteria for results are all elaborated. The observations regarding the
patients and statistical analysis of results obtained from the treatments are put forth.
Part III: Discussion
The interpretations of the conceptual study, clinical study, and probable mode of
action of the medicines are discussed here.

Summary
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 108
Part-IV :The Conclusions drawn from the Observations are presented here.
40 patients of Amlapitta were studied, out of whom, 42% were in the age group
26-35yrs.; 72.5% were male, 85% married and 95% Hindus. 55% of the patients
were Graduates, 65% had laborious of work, 70% middle classes. 65% were
consuming mixed diet, 65% gave a history of visamasana and 55% consumed
tea/coffee excessively. 42.5% of the patients gave a history of mental stress and
50% complained of sleep disturbances. No family history of similar illness was
evident in any patient.
45% of the patients were of pitta and kapha dominance, 82.5% of patients
weremadhyama sara, 62.5% of madhyama samhanana, 75% of madhyama satva,
35% katurasa satmya, 75% of mandagni and 65% of pravara bala. 35% of the
patients gave a history of 6mth-1yr. of illness. Among laksana, 90% had aruchi,
50% had avipaka , amloudgara was seen in 95%, hrid-kanthadaha in 65%
Fourty patients who had completed the clinical trial were considered for
assessment of results.
Group A: In the post treatment period, statistically significant results were obtained
in Laksana like Aruchi – 61%, Avipaka - 64%, Amlodgara – 82%, Utklesh – 70%,and
Hridkantadaha – 84%
Group B: In the post treatment period, statistically significant results were obtained
in Aruchi – 56%, Avipaka - 56%, Amlodgara – 81%, Utklesh – 78%,and
Hridkantadaha – 85%
Over all result,In group A 40% cases showed Major improvement, 35%
showed moderate improvement, while 20% cases showed Minor improvement,5% of
cases showed not improved .In group B, 30% cases showed Major improvement, 35%
cases showed moderate improvement, while 25% cases showed Minor improvement
and in 10% of cases showed Not improved was found .
At the end of the study it was concluded that yastimadhu churna as mrudu
virechaka with sootsshekara rasa vati as shaman oushada provided better and more
effective results when compared to sootashekhar rasa vati as shaman chikitsa.

List of References
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 109
LIST OF REFERENCE
1 BHAGAVAD GITA Adiparva 1/ 27
2 Ca .Su – 1/110
3 Ca .Su – 25/40
4 Ca . Su 26/43
5 Ca .Su 26/103
6 Ca. Su-27/25
7 Ch . Chi 12 /52
8 Ca. Chi-15/ 47
9 Ca. Su -20/ 1
10 Ch. Chi-12/52
11 Ha .Sa . in 24th chapter of 3rd sthana
12 Su. Su – 21 / 11
13 Su .Su - 21 /13
14 Ch . Chi – 15 /47
15 M .Ni - 51 / 1 Madhu Kosha
16 M.Ni. – 51 / 1 Madhu kosha
17 M . Ni - 51 / 1
18 A .S . Su 20 / 16 Indu Teeka
19 Y.R. Amlapitta. Chit/24
20 Ka .Sa . Khi .sth . 16 th chapter
21 A .S . Su -20 / 16
22 A .S . Su - 12 / 6
23 Ma . Ni - 51 / 1

List of References
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 110
24 Ch. Vim 1/ 24
25 Ch . Vim 1/ 21
26 Ka . Khil – 16/ 3- 6
27 M . N - 51 / 1
28 B . P Part 2 – 10 /1
29 B . R - 56
30 G . H – 38 / 1
31 S .S – Sha . Purvakhand 115/118
32 Ch . Su - 6/ 14
33 Ch . Su 7/ 60
34 Ch . Vi - 1/ 21 - 22
35 C . Ch - 1/ 8
36 M . Ni -51/ 3
37 M . Ni - 51 / 8 - 12
38 K .S . Khi – 16/ 16 - 17
39 M .Ni -57 / 3
40 Y . R .Amlapittachikitsa / 3
41 B . P , Madhy Aamakhanda /
42 Ka . Khil 16 / 15
43 Ka . Khil 16/ 16
44 Ka . Khil 16/ 17
45 C . Chi , 21 / 40
46 K .S . Khi , 16 / 49
47 Chakra. Chi , 28
48 A .S . Su , 19/21

List of References
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 111
49 Su . Su , 35
50 C . Ni – 5/15
51 M . Ni – 5/17
52 Ka . Khi – 16/49
53 K .S . Khi – 16/42
54 Ka . Khi - 16
55 Thamas Edison
56 C .Cu . 24 /45
57 K..S .Khi – 16 /33 -40
58 K .S . Khi - 16/ 33 - 40
59 B . R , 56 / 156 - 159
60 K .S . Khi , 16/ 44 - 48
61 C . T .M vol 1 Pg - 641
62 Page No - 307 - 310
63 H .P . I .M Vol 2 Pg - 232
64 C T M Vol 64 1
65 French;s Index of differential diagnosis Pg No 307 - 310
66 5 Minute clinical assessment CIMS Pg 344
67 5 Minute clinical assessment CIMS Pg 345
68 H . P .I . M, Vol 2 Pg - 333
69 D .P . P .M , Pg - 434
70 H . P .I .M Vol 2 Pg - 233
71 5 Minute clinical assessment CIMS Pg - 344
72 5 Minute clinical assessment CIMS Pg - 344
73 H . P .I .M , Vol 2 Pg - 1592

List of References
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 112
74 5 Minute clinical assessment CIMS Pg – 344
75 H . P .I .M , Vol 2Pg - 1582 , table no . 288
76 D. G
77 Yograt chp Amla Pitta chi ,Pg No.244 , shlo No .56 . .

Bibliography
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 113
BIBLIOGRAPHY
Charaka Samhita - Charaka Chandrika Hindi Commentary By Bramhanand
Tripathi.
Kashyapa Samhita - Hindi Comm. By Satyapal, Chaukhambha Sanskrit
Sansthana Varanasi.
Madhava Nidana - Madhukosha Comm. with Hindi Vidyotini Comm. By S.
Shastri. Vol. I & II, Chaukhambha Sanskrit Sansthana, Varanasi.
Yogaratnakara – Vidyotini Hindi Comm. By Laxmipati Shastri, Chaukhambha
Sanskrit Series, Varanasi.
Sushruta Samhita - Hindi Comm. By Ambikadatta Shastri, Chaukhambha
Sanskrit Series, Varanasi.
Ashtanga Hridaya - Nirmala Hindi Commentary By Bramhanand Tripathi,
Chaukhambha Sanskrit Pratisthana, Delhi.
Harita Samhita - Ed. By. Ravidatta Shastri., Shri Krishnadas Academy,
Mumbai.
Chakrapani - Ayurveda Dipika Commentary on Charaka Samhita,
Chaukhambha Surabharati, Varanasi.
Bhavaprakasha - Ed. By Bramhashankar Mishra with Vidyotini Hindi
Commentary Chaukhambha Sanskrit Pratisthana, Varanasi.
Sharangadhara Samhita – Dipika Hindi Comm. By Bramhanand Tripathi,
Chaukhambha Surabharati Prakashan, Varanasi.
Bhaishajya Ratnavali - Ed. By. Rajeshwara Dutta Shastri, Chaukhambha
Sanskrit Sansthana, Varanasi.
Bhela Samhita - Ed. By Vd. Venkatasubrahmanya Shastri & Sri. Rajeshwar
Shastri, C.C.R.A.S., Delhi.
Dalhana - Nibandha Sangraha Comm. on Sushruta Samhita. Ed. By YT.
Acharya, Chaukhambha Orientalia, Varanasi.

Bibliography
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 114
Ashtanga Samgraha - Hindi Commentary By. Pd. Lalchandra Shastri,
Baidhyanath Ayu. Bhavan Ltd., Nagpur.
Chakradatta - Ed. By. Pandit Sadanand Sharma, Meharachand L. Publication,
New Delhi.
Desai Ranjit Rai - Ayurvediya Kriya Sharira, Baidyanath Ayu. Bhavan,
Nagpur.
Desai Ranjit Rai - Nidana Chikitsa Hastamalaka, Baidyanath Ayu, Bhavan,
Nagpur.
Dwarakanath C. - Introduction to Kayachikitsa, 3rd ed., Chaukhambha
Orientalia, Varanasi.
Kasture H. S. - Ayurvediya Panchakarma Vigyana, Baidyanath Bhavan,
Nagpur.
Pathak Ram Raksha - Kayachikitsa, Chaukhambha Bharati Academy,
Varanasi.
Sharma P.V. - Dravya Guna Vigyana, Vol. I & II, Chaukhambha Surabharati
Academy, Varanasi.
Davidson - Principles & Practice of Medicine, 19th edition., Saunders, UK
Harrison - Principles of Internal Medicine, 14th Ed. Mc Gram Hill, New
Delhi.
Kumar & Clark - Clinical Medicine, 5th ed., W.B. Saunders, New York.
Guyton & Hall - Textbook of Medical Physiology, 10th ed., Saunders.
API- Text Book of Medicine – Siddhartha N Saha 7th Edition.
Taber's Cyclopedic Medical Dictionary, 17th Ed., Jaypee Brothers, New
Delhi.
British Medical Journal.

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 115

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 116

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 117

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 118

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 119

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 120

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 121

Annexure
“A clinical comparative study to evaluate the efficacy of Mrudu Virechana
andShamana chikitsa in the management of Amlapitta” 122