a common elements approach to children's services presented to the the use of evidence in child...
TRANSCRIPT

A Common Elements Approach to Children's Services
Presented to the
The Use of Evidence in Child Welfare Practice and PolicyAn International Perspective on Future Directions
Haruv Institute, Bar-Ilan University, IsraelMay 26, 2010
Richard P. BarthATLANTIC COAST CHILD WELFARE IMPLEMENTATION CENTER
School of Social WorkUniversity of MarylandBaltimore, MD [email protected]

Summary
• Evidence based practices need to be based, primarily, on practice principles and common pracice elements, not on manuals
• Increasing the uptake of evidence based methods will best be achieved by increasing knowledge of common practice elements and common factors
• Adapting evidence based practices to international contexts will require emphasis on common factors

The Alphabet of EBP
What is needed, it seems to me, is some course of study where an intelligent young person can ... be taught the alphabet of charitable science.
Anna Dawes (1883) From a paper given at the International Congress of Charities and
Correction at the Chicago World's Fair.
Source: Lehninger, L. (2000). Creating a new profession: The beginnings of social work education in the United states. Washington, DC: Council on Social Work Education.

The Language of Evidence Based Practices
• Evidence Based Programs– Multi-dimensional
• Evidence Supported Interventions• Common (Practice) Elements• Common Factors (CD OI)
– Client directed– Outcome informed– Coherent treatment strategy
• Practice Principles• Practice (Policy) Framework

A Language for Evidence Supported Interventions for Children and Families
• Specific Competence – Needed to increase the acceptability of services and, possibly, to
improve interventions• Evidence Supported Programs
– Multi-systemic Therapy (MST); – “Wrap Around”– Multi-Dimensional Treatment Foster Care for Adolescents (MTFC-A)
• Evidence Supported Manualized Interventions – e.g., Cohen and Mannarino’s Trauma Focused-CBT
• Common (Practice) Elements Approach – Chorpita and colleagues
• Common Factors Approach and Measurment Feedback Systems (MFS)– Duncan, Lambert and Sparks (CDOI)
• Practice Principles– Hurlburt & Barth Parent Training Programs
• Practice (Policy) Framework– Commitment to “Place Matters” or “Family Focused Services” or “Safety
First”, or Safety, Permanency & Well-Being”

Specific Knowledge of
Problem & Solutions
Evidence Supported Programs
(Manualized Interventions)
Common (Practice) Elements
6“Practice” (Policy) Framework
Common Factors
Not Drawn to Scale Regarding the Number
in Each Set
ARE WE F
OCUING O
N
THE RIG
HT PART O
F THE
PRACTICE S
TRUCTURE?
Practice Principles

Specific Knowledge of Problems & Solutions
• Neglect • Adoption• Sexual Abuse• Trauma• Phobia• Running Away

Evidence Supported Programs and Evidence Supported Interventions
PROGRAMS• Multi-systemic Family Therapy (MST)• Multi-Dimensional Treatment Foster Care-
Adolescent (MTFC-A) and MTFC-Pre– KEEP
EVIDENCE SUPPORTED MANUALIZED INTERVENTIONS
• Trauma Focused CBT• Alternative Family-CBT• Coping Cat

What Makes an Evidence Based Program Work?
• We Really Do Not Know– There has been very little deconstruction
• Multi-Dimensional Treatment Foster Care is a LARGE Collection of Practice Elements– Parent Daily Report– Parent Management Training for Foster and
Biological Family– Behavioral Group Work– CBT for children– Mentoring of Youth

What Makes a Manualized Evidence Supported Intervention Work?
• Trauma Focused CBT is more tightly manualized with a somewhat SMALLER Collection of Practice Elements– Psycho-education– Stress-management– Narrative therapy– Exposure therapy– Cognitive restructuring– Parental treatment
How will I ever master all these
ESI manuals ???

The Common Elements Approach
Step 1:
Emphasis on evidenced-based treatments
Step 2:
Development of treatment manuals
Step 3:
Information overload: Too many treatment manuals to learn and
manuals change as new knowledge is gained

The Common Elements Approach• Using elements that are found across several evidence-
supported, effective manualized interventions
• “Clinicians ‘borrow’ strategies and techniques from known treatments, using their judgment and clinical theory to adapt the strategies to fit new contexts and problems” (Chorpita, Becker & Daleiden, 2007, 648-649)
• Actual treatment elements become unit of analysis rather than the treatment manual
• Treatment elements are selected to match particular client characteristics

Identifying the Practice Elements
Trained coders reviewed 322 randomized controlled trials for major mental health disorders for children and teens; Over $500 million invested in these research studies Studies conducted over a span of 40 years More than 30,000 youth cumulatively in the study
samples
Approach: What features characterize successful treatments? What strategies are common across effective
interventions?
(Chorpita & Daleiden, 2009)
Coding Process for 322 RCTs:Frequencies of practice elements from
winning treatment groups were then tallied to see what practice elements were most commonly found in effective interventions
41 practice elements identified that were found in at least 3 of the 232 winning treatment groups
Tools to Support the Common Elements Approach
• www.practicewise.com• Subscription-based resources:
–PracticeWise Practitioner Guides–Modular Approach to Therapy for
Children (MATCH)–PracticeWise Evidence-Based Services
Database (PWEBS)–PracticeWise Clinical Dashboards

Common Elements Practitioner Guides
• Summarize the common elements of evidence-based treatments for youth;
• Handouts guide clinician in performing the main steps of the technique
• Currently 29 Treatment elements, including:– Response cost– Modeling– Social Skills– Time out– Engagement with caregiver
• Guide is searchable by: treatment, audience (child, caregiver, family), purpose, objectives
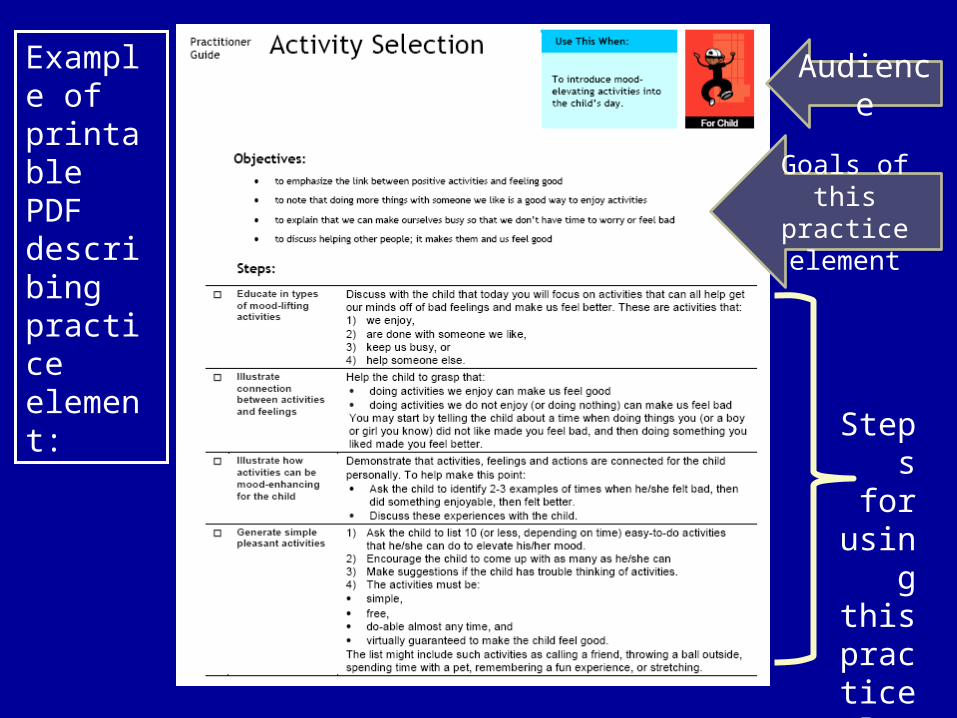
Example of printable PDF describing practice element:
Audience
Goals of this practice element
Steps for
using this
practice
element

MATCH Example: Putting Together Practice Elements
Start

Clinical Dashboards• Microsoft Excel based monitoring tool
– Tracks achievement of treatment goals or other progress measures on a weekly/session basis
– Documents which practice elements were used when• Dashboard can be customized:
– Display up to 5 progress measures;– Write-in additional practice elements
• Potential uses:– Documenting session activities– Tracking client progress– Clinical supervision
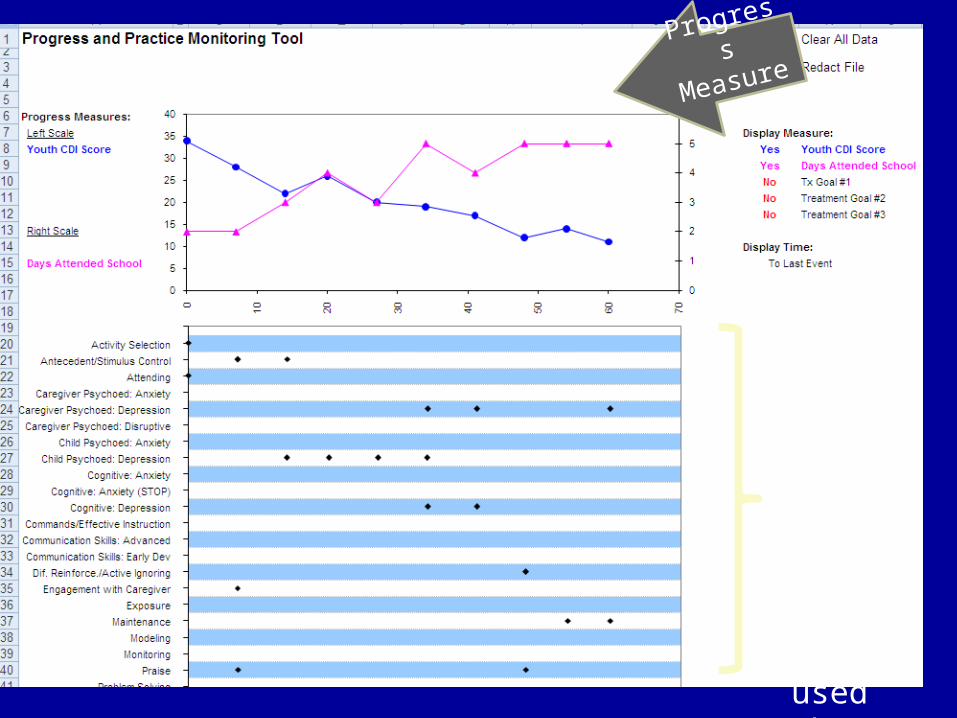
Progress
Measures
Document which practice element was used when
Common Factors (Client Directed Outcome Informed)
• Effective therapy arises from allegiance to a treatment model, monitoring of change, and creating a strong therapeutic alliance– Feedback from clients on their level of functioning– Feedback to therapists on the therapeutic alliance– A coherent treatment approach that encourages
action to change
22Duncan et al., (2010) Heart and Soul of Change: Delivering What Works in Therapy (2nd Edition). Washington, DC: APA
Practice Based Evidence
“A continuous feedback or practice-based evidence approach individualizes psychotherapy
based on treatment response and client preference;
systematic feedback addresses the dropout problem, as well as treatment and therapist
variability…” (p. 702).
Anker, M. G., Duncan, B. L., & Sparks, J. A. (2009). Using client feedback to improve couple therapy outcomes: A randomized clinical trial in naturalistic setting. Journal of Consulting and Clinical Psychology, 77, 693-704.

Client-Directed, Outcome-Informed (CDOI) Treatment & Wrap Around
• Adapt to specific individual and family needs based on client feedback
• Move from punitive and restrictive to optimistic and responsive interventions
• Utilize brief and systemic client-report measures throughout therapy
• Strengths-based and culturally responsive
“At its core, wraparound is flexible, comprehensive, and team-based.” (p. 65)
Sparks, J. A., & Muro, M. L. (2009). Client-directed wraparound: The client as connector in community collaboration. Journal of Systemic Therapies, 28, (3), 63-76.

Tools for Feedback: ORS and SRS
• Reliable and valid four-item, self-report instruments used at each meeting
• Scored and interpreted in a collaborative effort between client and therapist
• Rather than the therapist assigning meaning to a client’s feedback, the client explains the meaning behind the mark on the scale
• Help identify alliance strengths and weaknesses in therapy
Sparks, J. A., & Muro, M. L. (2009). Client-directed wraparound: The client as connector in community collaboration. Journal of Systemic Therapies, 28, (3), 63-76.

Individually(Personal well-being)
I ---------------------------------------------------------------------------------------------------- I
Interpersonally(Family, close relationships)
I --------------------------------------------------------------------------------------------------- I
Socially(Work, school, friendships)
I --------------------------------------------------------------------------------------------------- I
Overall(General sense of well-being)
I --------------------------------------------------------------------------------------------------- I
Institute for the Study of Therapeutic Changewww.talkingcure.com
© 2000, Scott D. Miller & Barry L. Duncan
Outcome Rating Scale (ORS): AdultsLooking back over the last week, including today, help us understand how you have been feeling by rating how well you have been doing in the following areas of your life, where marks to the left represent low levels and marks to the right indicate high
levels. If you are filling out this form for another person, please fill out according to how you think he or she is doing.

RelationshipI did not feel heard,
I felt heard,understood, and I -------------------------------------------------------------------------------- I understood, and respected.
Goals and TopicsWe did not work on We worked on and
or talk about what I talked about what I
wanted to work on I ----------------------------------------------------------------------------------------- I wanted to work on or talk about
and talk about.
Approach or MethodThe therapist’s The therapist’s
approach is not a I ------------------------------------------------------------------------------------------- I approach is a good fit for me
good fit for me.
OverallOverall, today’s There was something
session was right for I ------------------------------------------------------------------------------------------ I missing in the session today.
me.
Institute for the Study of Therapeutic Change
www.talkingcure.com
© 2002, Scott D. Miller, Barry L. Duncan, & Lynn Johnson
Session Rating Scale (SRS V.3.0): AdultsPlease rate today’s session by placing a mark on the line nearest to the description that best fits your experience.

Formatted for Children…the CORS and CSRS
• Similar scales designed for use with children ages 6-12
• Written at a third grade reading level • Used to track effectiveness and
therapeutic alliance as reported by children and their parents or caretakers.
• CORS shows strong reliability (alpha=.84) and validity as compared to a longer youth outcome questionnaire (Pearson’s coefficient=.61)
• Gives youth a voice in their own therapy
Duncan, B. L., Sparks, J. A., Miller, S. D., Bohanske, R. T. & Claud, D. A. (2006) Giving youth a voice: A preliminary study of the reliability and validity of a brief outcome Measure for children, adolescents, and caretakers. Journal of Brief Therapy, 5, (2), 71-88.

Me(How am I doing?)
I ---------------------------------------------------------------------------------------------------- I
Family(How are things in my family?)
I --------------------------------------------------------------------------------------------------- I
School(How am I doing at school?)
I --------------------------------------------------------------------------------------------------- I
Everything(How is everything going?)
I --------------------------------------------------------------------------------------------------- I
Institute for the Study of Therapeutic Changewww.talkingcure.com
© 2003, Barry L. Duncan, Scott D. Miller & Jacqueline A. Sparks
Child Outcome Rating Scale (CORS)How are you doing? How are things going in your life? Please make a mark on the scale to let us know. The closer to the smiley face, the better things are. The closer to the frowny face, things are not so good. If you are a caretaker filling out this form, please fill out according to how you think the child is doing.
ListeningDid not always
listen to me I ---------------------------------------------------------------------------- I Listened to me.
How ImportantWhat we did and talked What we did and
about was not talked about
really that I --------------------------------------------------------------------------- I were important
important to me. to me.
What We DidI did not like I liked what we
What we did I --------------------------------------------------------------------------- I did today.
today.
OverallI wish we could I hope we do the
do something I --------------------------------------------------------------------------- I same kind of
different. things next time.
Institute for the Study of Therapeutic Change
www.talkingcure.com• © 2003, Barry L. Duncan, Scott D. Miller, Jacqueline A. Sparks, and Lynn D. Johnson
Child Session Rating Scale (SRS V.3.0)How was our time together today? Please put a mark on the lines below to let us know if how you feel.

Measurement Feedback Systems• A MFS is a battery of comprehensive measures administered frequently
concurrent with treatment, providing timely feedback to clinicians and supervisors to report on clinical processes and treatment adherence (Bickman, 2008). A good MFS should have measures that are:– short, – Psychometrically sound, and – useful in everyday practice by clinicians
• MFSs should assess several domains by multiple reporters that include treatment progress (e.g. youth and family outcomes) and treatment processes (e.g. therapeutic alliance and treatment activities).
• A MFS provides systematic feedback that can be used to enhance clinical decision-making, improve accountability, drive program planning, and inform treatment effectiveness (Chorpita et al. 2008; Kelley & Bickman 2009).

Client Feedback as a Common Factor (or Element)?
• This study provides reliable support for alliance building and monitoring treatment progress for clients and therapists in couple therapy.
• Feedback tools (e.g., ORS and SRS) that are not linked with a certain therapy or method can be used in community settings more easily than specific treatment packages.
• Further research may show the extent to which the increased therapeutic engagement or allegiance effects can influence the positive effect of the feedback tools.
Anker, M. G., Duncan, B. L., & Sparks, J. A. (2009). Using client feedback to improve couple therapy outcomes: A randomized clinical trial in naturalistic setting. Journal of Consulting and Clinical Psychology, 77, 693-704.

First CDOI/MFS RCT
• Couples using the feedback measure, ORS,
(N=103) at pre- and posttreatment and follow-up, compared to couples receiving treatment as usual (TAU) (N=102):– Achieved almost 4 times the rate of clinically significant change– Maintained a significant advantage on the ORS at 6-month
follow-up– Showed greater marital satisfaction and lower rates of
separation or divorce
• The feedback condition showed a moderate to large effect size (0.50)
Anker, M. G., Duncan, B. L., & Sparks, J. A. (2009). Using client feedback to improve couple therapy outcomes: A randomized clinical trial in naturalistic setting. Journal of Consulting and Clinical Psychology, 77, 693-704.

Other Common Elements/MFS: The Parent Daily Report

Project KEEP: (MTFC-Lite)• Foster Parent Groups
– Good behavioral group work a la Sheldon Rose– Appreciate the foster parents efforts– Reward their successes– Demonstrate and role play skills– Pre-teaching (shaping the antecedents)
• Parent Daily Report (PDR)– Which of these problems occurred in the last 24 hours?– How stressful did you find it?

Predicted Probability Of Negative Exits By Prior Placements And Intervention Group
KEEP

MTFC and KEEP Implications
• We can change biological characteristics of children—including stress hormones and executive functioning—with consistent responsive social interventions
• The use of the Parent Daily (or Weekly) Report and Support Groups may be common elements of benefit.– Perhaps could also be used more in parent training (a la
PMTO) and post-adoption services

Practice Principles
• Example, Doug Kirby Pregnancy and STI Practice Principles
• Hurlburt and Barth on parenting programs
• MORE ART THAN SCIENCE– Most of these practices have not been
studied in isolation and we cannot tell what their overlap might be—some may be inert.
Basic Components of Effective Parent Training
• Social learning framework • Strengthening parent-child relationship• Effectively use praise and reward • Sets clear and effective limits• Reserves most significant consequences for
targeted, limited behaviors• Strictly limits negative consequences• Parent Training + may have worse outcomes than
parent training alone (CDC)• Addresses family as well as parent-child issues
Hurlburt, M., Barth, R.P., Leslie, L. & Landsverk, J. (in press). Haskins, R., Wulczyn, F., & Webb, M. (Eds). Research on child protection: Findings from NSCAW. Washington, DC: Brookings.

Delivering Effective Parent Training Programs
• Detailed materials corresponding to specific, narrowly focused parenting skills
• Specific means of monitoring changes in parenting practices (e.g., homework)
• Parents take active, participatory role in learning and practicing skills
• Minimum 15 hours of intervention and 25 hours for group format
• Rigor of supervision processes to ensure program delivery with fidelity

Practice Policy Framework
• Lack of clarity about the purposes of societal efforts to protect children, promote their well-being, and support families will undermine the commitment to advance new treatment approaches and handicap efforts to generate measurement feedback systems at the policy level—a crucial flaw.

Thank you for this opportunity
Comments
?
‘S
OR
Partial References IAarons, G. A. (2005). Measuring provider attitudes toward evidence-based practice:
Consideration of organizational context and individual differences. Child and Adolescent Psychiatric Clinics of North America, 14(2), 255-+.
Barth, R. P. (2005). Foster care is more cost-effective than shelter care: Serious questions continue to be raised about the utility of group care use in child welfare services. Child Abuse & Neglect, 29, 623-625.
Barth, R. P., Greeson, J. K. P., Guo, S., Green, R. L., Hurley, S., & Sisson, J. (2007). Outcomes for youth receiving intensive in-home therapy or residential care: A comparison using propensity scores. American Journal of Orthopsychiatry, 77(4), 497-505.
Barth, R. P., Landsverk, J., Chamberlain, P., Reid, J., Rolls, J., Hurlburt, M., et al. (2006). Parent training in child welfare services: Planning for a more evidence based approach to serving biological parents. Research on Social Work Practice.
Bruns, E. J., Hoagwood, K. E., Rivard, J. C., Wotring, J., Marsenich, L., & Carter, B. (2008). State implementation of evidence-based practice for youths, part II: Recommendations for research and policy. Journal of the American Academy of Child and Adolescent Psychiatry, 47(5), 499-504.
Chamberlain, P., Price, J. M., Reid, J. B., Landsverk, J., Fisher, P. A., & Stoolmiller, M. (2006). Who disrupts from placement in foster and kinship care? Child Abuse & Neglect, 30(4), 409-424.
Chambless, D. L., & Ollendick, T. H. (2001). Empirically supported psychological, interventions: Controversies and evidence. Annual Review of Psychology, 52, 685-716.
Chorpita, B. F., & Daleiden, E. L. (2009). Mapping Evidence-Based Treatments for Children and Adolescents: Application of the Distillation and Matching Model to 615 Treatments From 322 Randomized Trials. Journal of Consulting and Clinical Psychology, 77(3), 566-579.
Dawson, K., & Berry, M. (2002). Engaging families in child welfare services: An evidence-based approach to best practice. Child Welfare, 81, 293-317.

Partial References IIDoyle, J. J. (2007). Child protection and child outcomes: Measuring the effects of
foster care. American Economic Review, 97(5), 1583-1610.Flynn, L. M. (2005). Family perspectives on evidence-based practice. Child and
Adolescent Psychiatric Clinics of North America, 14(2), 217-224.Huey, S. J., & Polo, A. J. (2008). Evidence-based psychosocial treatments
for ethnic minority youth. Journal of Clinical Child and Adolescent Psychology, 37(1), 262-301.
Lambert, M. J. (2005). Emerging methods for providing clinicians with timely feedback on treatment effectiveness: An introduction. Journal of Clinical Psychology, 61(2), 141-144.
Lee, B. R., & Thompson, R. (2008). Comparing outcomes for youth in treatment foster care and family-style group care. Children and Youth Services Review, 30(7), 746-757.
McCrae, J. S., Barth, R.P., & Guo, S. (in press). Changes in emotional-behavioral problems following usual care mental health services for maltreated children: A propensity score analysis. American Journal of Orthopsychiatry.
McKay, M., Hibbert, R, Hoagwood, K, Rodriguez, J, Murray, L, Legerski, J, & Fernandez, D. (2004). Integrating evidence-based engagement interventions into “real world” child mental health settings. Brief Treatment and Crisis Intervention 4,2, 177-186.
Miranda, J., Bernal, G., Laua, A., Hwang, W. C., & LaFramboise, T. (2005). State of the science on psychosocial interventions for ethnic minorities. Annual Review of Clinical Psychology, 1, 113-142.
Newnham, E. A., & Page, A. C. Bridging the gap between best evidence and best practice in mental health. Clinical Psychology Review, 30(1), 127-142.
Partial References IIIPalinkas, L. A., Aarons, G. A., Chorpita, B. F., Hoagwood, K., Landsverk, J.,
& Weisz, J. R. (2009). Cultural Exchange and the Implementation of Evidence-Based Practices Two Case Studies. Research on Social Work Practice, 19(5), 602-612.
Pine, B. A., Spath, R., Werrbach, G. B., Jenson, C. E., & Kerman, B. (2009). A better path to permanency for children in out-of-home care. Children and Youth Services Review, 31(10), 1135-1143.
Price, J. M., Chamberlain, P., Landsverk, J., & Reid, J. (2009). KEEP foster-parent training intervention: model description and effectiveness. Child & Family Social Work, 14(2), 233-242.
Ryan, J. P., Marshall, J. M., Herz, D., & Hernandez, P. A. (2008). Juvenile delinquency in child welfare: Investigating group home effects. Children and Youth Services Review, 30(9), 1088-1099.
Saunders, B. E., Berliner, L., & Hanson, R. F. E. (2003). Child physical and sexual abuse: Guidelines for treatment (Final report: January 15, 2003). Charleston, SC: National Crime Victims Research and Treatment Center.
Sundell, K., and Vinnerljung, B. (2004). Outcomes of family group conferencing in Sweden: A 3-year follow-up. Child Abuse & Neglect, 28, 267-287.
Taussig, H. N., Clyman, R. B., & Landsverk, J. (2001). Children who return home from foster care: A 6-year prospective study of behavioral health outcomes in adolescence. Pediatrics, 108, 62-68.

Partial References IVThomlison, B. (2003). Characteristics of evidence-based child
maltreatment interventions. Child Welfare, 82, 541-569.Wang, P. S., Ulbricht, C. M., & Schoenbaum, M. (2009). Improving Mental
Health Treatments Through Comparative Effectiveness Research. Health Affairs, 28(3), 783-791.
Weisz, J. R., Jensen-Doss, A., & Hawley, K. M. (2006). Evidence-based youth psychotherapies versus usual clinical care - A meta-analysis of direct comparisons. American Psychologist, 61(7), 671-689.
Wilensky, G. R. (2006). Developing a center for comparative effectiveness information. Health Affairs, 25(6), W572-W585
Wilson, S. J., Lipsey, M. W., & Soydan, H. (2003). Are mainstream programs for juvemajority youth? A meta-analysis of outcomes research. Research on Social Work Practice, 13(1), 3-26nile delinquency less effective with minority youth than
Wulczyn, F., Barth, R. P., Yuan, Y. Y., Jones Harden, B., & Landsverk, J. (2008). Evidence for child welfare policy reform. New York: Transaction De Gruyter.