a common theme? - intensivistenopleiding consumer powerhouse euro health consumer index 2013 report...
TRANSCRIPT

Crew Resource Management A common theme?
J.G. van der Hoeven

Health Consumer Powerhouse Euro Health Consumer Index 2013 report
23
4.1 Results Summary In order to help a comparison over time, the Rank numbers ≥ Rank 13 (from UK England down) in the Index matrix above do not include Scotland.
Figure 4.1 EHCI 2013 total scores.
This seventh attempt at creating a comparative index for national healthcare systems has confirmed that there is a group of EU member states, which all have good healthcare systems seen from the customer/consumer’s point of view. The scoring has intentionally been done in such a way that the likelihood that two states should end up sharing a position in the ranking is almost zero. It must therefore be noted that great efforts should not be spent on in-depth analysis of why one country is in 13th place, and another in 16th. Very subtle changes in single scores can modify the internal order of countries, particularly in the middle of the ranking list.
The EHCI 2013 total ranking of healthcare systems shows a much narrowed victory (in 2012, the margin was 50 points) for The Netherlands, scoring 870 points out of 1000, 19 points ahead of runners-up Switzerland at 851 points. After the top two, there is a more than 30-point gap down to three closely-knit Scandinavian countries: Iceland 3rd at 818 points, Denmark in 4th place with 815 and Norway 5th with 813 points. The main reason for the Swiss advance is that in 2013, historic n.a. (not available) scores for this non-EU country have been researched out (with some effort).

Health Consumer Powerhouse Euro Health Consumer Index 2013 report
31
Figure 6.1. These results over the seven years 2006 – 2013 have been normalized to all be calculated the
same way as the EHCI 2007 (with its five sub-disciplines). This means that in 2008 and 2009, “2.1 EPR penetration” was moved back to “1. Patients’ Rights and Information”, and the “e-Health” sub-discipline was taken out. The 2013 edition has had Prevention removed/moved back to Range and Reach. New additional indicators in sub-disciplines 3.Outcomes, 4.Range and Reach of services and 5.Pharmaceuticals are in the post-2007 scores.
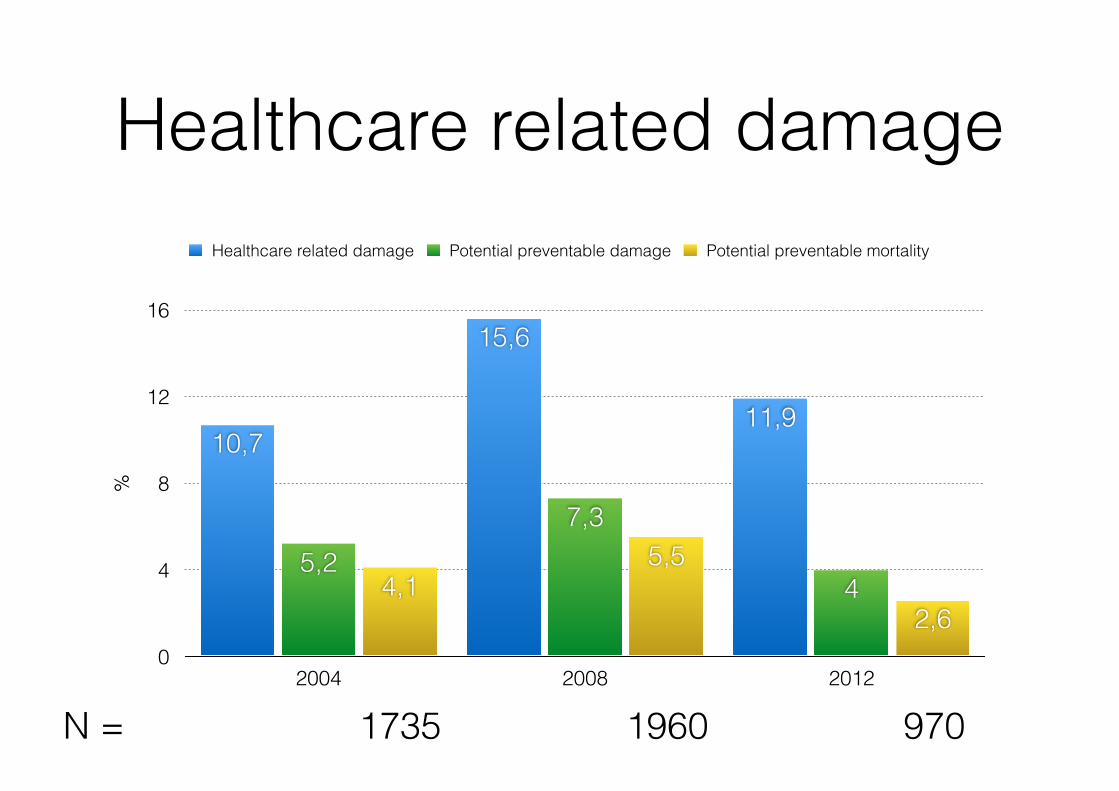
Healthcare related damage%
0
4
8
12
16
2004 2008 2012
2,6
5,54,1 4
7,35,2
11,9
15,6
10,7
Healthcare related damage Potential preventable damage Potential preventable mortality
N = 1735 1960 970

However…..• Patient safety?
• Expensive
• Efficiency?
The Top Patient Safety Strategies That Can Be Encouraged forAdoption NowPaul G. Shekelle, MD, PhD; Peter J. Pronovost, MD, PhD; Robert M. Wachter, MD; Kathryn M. McDonald, MM; Karen Schoelles, MD, SM;Sydney M. Dy, MD, MSc; Kaveh Shojania, MD; James T. Reston, PhD, MPH; Alyce S. Adams, PhD; Peter B. Angood, MD;David W. Bates, MD, MSc; Leonard Bickman, PhD; Pascale Carayon, PhD; Sir Liam Donaldson, MBChB, MSc, MD; Naihua Duan, PhD;Donna O. Farley, PhD, MPH; Trisha Greenhalgh, BM BCH; John L. Haughom, MD; Eileen Lake, PhD, RN; Richard Lilford, PhD;Kathleen N. Lohr, PhD, MA, MPhil; Gregg S. Meyer, MD, MSc; Marlene R. Miller, MD, MSc; Duncan V. Neuhauser, PhD, MBA, MHA;Gery Ryan, PhD; Sanjay Saint, MD, MPH; Stephen M. Shortell, PhD, MPH, MBA; David P. Stevens, MD; and Kieran Walshe, PhD
Over the past 12 years, since the publication of theInstitute of Medicine’s report, “To Err is Human:
Building a Safer Health System,” improving patient safetyhas been the focus of considerable public and professionalinterest. Although such efforts required changes in policies;education; workforce; and health care financing, organiza-tion, and delivery, the most important gap has arguablybeen in research. Specifically, to improve patient safety weneeded to identify hazards, determine how to measurethem accurately, and identify solutions that work to reducepatient harm. A 2001 report commissioned by the Agencyfor Healthcare Research and Quality, “Making HealthCare Safer: A Critical Analysis of Patient Safety Practices”(1), helped identify some early evidence-based safety prac-tices, but it also highlighted an enormous gap betweenwhat was known and what needed to be known.
For the past 4 years, with support from the Agency forHealthcare Research and Quality, our group (a projectteam from the RAND Corporation; Stanford University;the University of California, San Francisco; Johns HopkinsUniversity; and ECRI Institute) and an international panelof 21 stakeholders and evaluation methods experts con-ducted an evidence-based assessment of patient safety strat-egies (PSSs). Our efforts involved 3 phases. In the firstphase, we developed a framework for reviewing existingstudies and prospectively evaluating new PSS implementa-tion studies (2). This framework identified several keypoints about the importance of theory, context, and imple-mentation (Table 1) (2).
The second phase was a review of current patientsafety strategies. We started with the 79 topics in MakingHealth Care Safer and added practices from the NationalQuality Forum’s 2010 update, the Joint Commission, andthe Leapfrog Group; those we identified in an initial scop-ing search; and those suggested by experts. From this list of158 potential topics, we used several rounds of voting withour stakeholders to narrow the scope to 41 PSSs that theexpert panel judged to be most important to the largestaudience. Given limited time and resources, we prioritizedtopics as needing either a traditional systematic review oronly a “brief review.” The latter generally focused on aspecific aspect of the PSS, such as emerging data or newinsights about implementation.
We chose 18 topics for in-depth reviews. As a first stepfor the reviews, we searched for existing relevant systematicreviews. To assess the potential utility of such reviews, wefollowed procedures proposed by Whitlock and colleagues(3) and asked the following questions: Is the existing re-view sufficiently “on topic” to be of use? Is the review ofsufficient quality to foster confidence in the results? If wedetermined that the existing systematic review was suffi-ciently on topic and of acceptable quality, we took 1 of 2further steps. In some cases, we did an “update” search(that is, we searched databases for all new relevant evidencepublished since the search end date in the existing system-atic review); in others, we conducted searches for “signalsfor updating.” Such searches generally followed the criteriaproposed by Shojania and colleagues (4), which involved asearch of high-yield databases and journals for pivotal stud-ies that could signal that a systematic review is out of date.A pivotal study is one that may call into question the re-sults of a previous systematic review. We added any evi-dence identified in either the update search or signalssearch to the evidence base from the existing systematicreview. Some PSSs had no existing systematic reviews andothers had previous reviews that were not of sufficient rel-evance or quality to be used. In those situations, we con-ducted new searches using existing guidance (5).
Evidence about context, implementation, and adop-tion was a key focus of our reviews. We searched for evi-dence on these aspects of primary studies in 2 ways. First,we sought and extracted data about context, implementa-tion, and unintended harms from articles that evaluatedthe effectiveness of PSSs. Second, we identified “imple-mentation studies” from our literature searches. Thesestudies focus on the implementation processes, particularlyelements demonstrated or hypothesized to be of specialimportance for the success, or lack of success, of the inter-vention. To be eligible, implementation studies needed to
Ann Intern Med. 2013;158:365-368.For author affiliations, see end of text. Annals of Internal Medicine
See also:
Web-OnlyCME quiz (Professional Responsibility Credit)
Annals of Internal Medicine Supplement
www.annals.org 5 March 2013 Annals of Internal Medicine Volume 158 • Number 5 (Part 2) 365
Downloaded From: http://annals.org/ on 06/14/2014
Crew Resource Management
„Application of team management!concepts in healthcare”

Crew Resource Management
Situational awareness
Information management
Communication
Stress management
Team dynamics
Leadership
Decision making
Risk management
Five hazardous attitudes„Don’t tell or question me”!
„Do it STAT - no need for double-check”!„It won’t happen to me - I have done this often”!
„I am highly skilled and I can do this”!„What’s the use?”

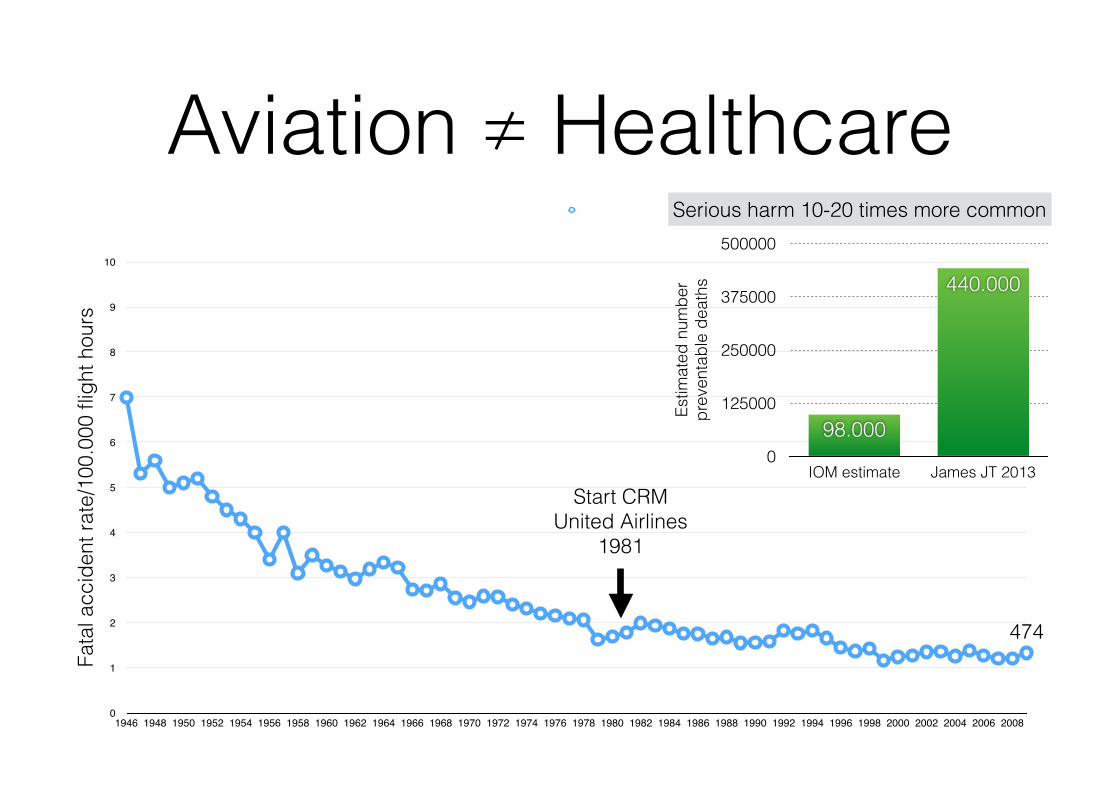
Aviation ≠ HealthcareFa
tal a
ccid
ent r
ate/
100.
000
fligh
t hou
rs
0
1
2
3
4
5
6
7
8
9
10
1946 1948 1950 1952 1954 1956 1958 1960 1962 1964 1966 1968 1970 1972 1974 1976 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008
Start CRM United Airlines
1981
474
Estim
ated
num
ber
prev
enta
ble
deat
hs
0
125000
250000
375000
500000
IOM estimate James JT 2013
440.000
98.000
Serious harm 10-20 times more common
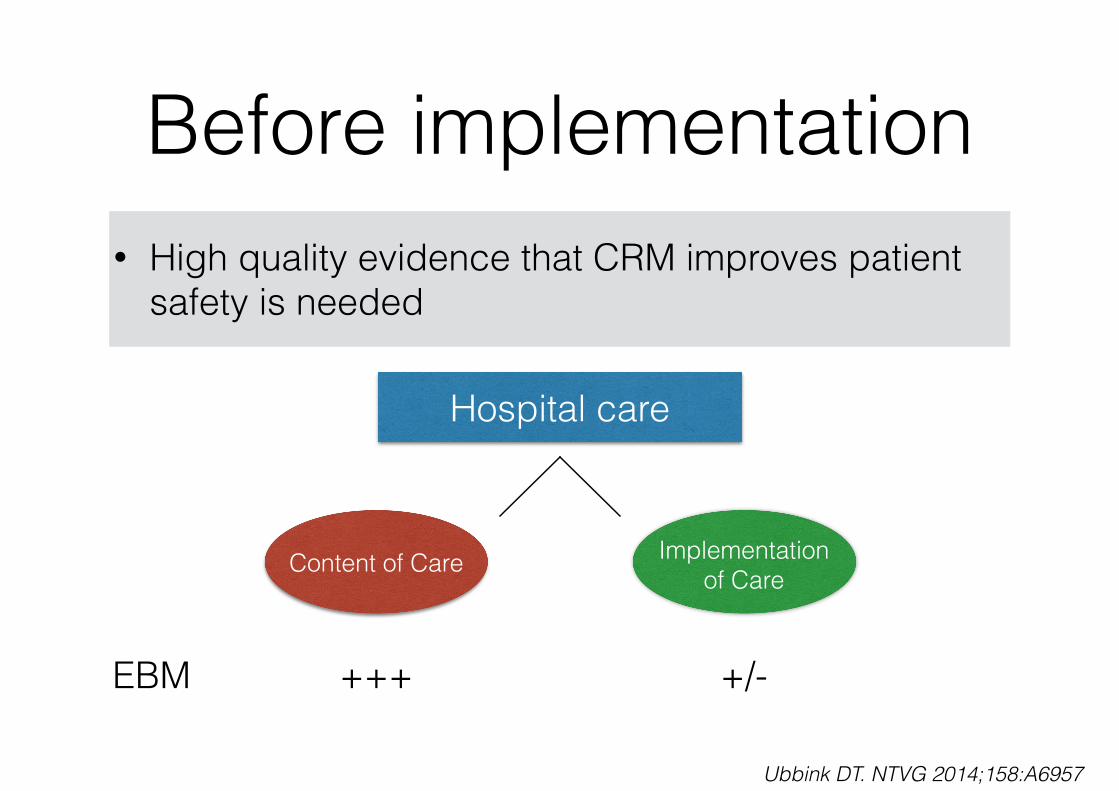
Before implementation• High quality evidence that CRM improves patient
safety is needed
Hospital care
Content of Care Implementation of Care
EBM +++ +/-
Ubbink DT. NTVG 2014;158:A6957

Team-training• Learner reactions usually positive; 80% or more
indicate that covered topics are applicable to their work
• Positive impact on learner knowledge, self-efficacy and teamwork attitudes
• Improvement in team behavior and moderate evidence that team-training improves teamwork climate and safety climate
Weaver SJ. BMJ Qual Saf 2014;23:359-372

Team-training
• Increasing evidence that team-training improves important clinical outcomes but even „high-quality” studies use quasi-experimental pre-post designs
• Strong evidence that improvements in teamwork knowledge, attitudes and processes are sustained for 6 months and and weak evidence that patient outcomes are improved over longer period
Weaver SJ. BMJ Qual Saf 2014;23:359-372

Setting (1)• 32-bed ICU in a university hospital
• Mixed adult population including trauma-, cardio- thoracic- and neurosurgery
• Standardized data recording (NICE dataset)
• Standardized recording of ICU related complications (N = 18)

Setting (2)• Two-day CRM awareness training
• Core team that translated action points into clinical practice
• Scenario-based team training during implementation year
• Video feedback for various invasive procedures

Design• Before/after design
• Sample size calculation based on absolute decrease in complication rate of 20/1000 patients
• Safety climate, complication rate, standardized mortality rate
• N = 7271

Perceived safety attitude
Stress recognition
Teamwork climate
Safety climate
Management perception
Working conditions
Job satisfaction
Median total SAQ score
40 50 60 70 80
Before After
**********

CRM - complications

CRM - complications
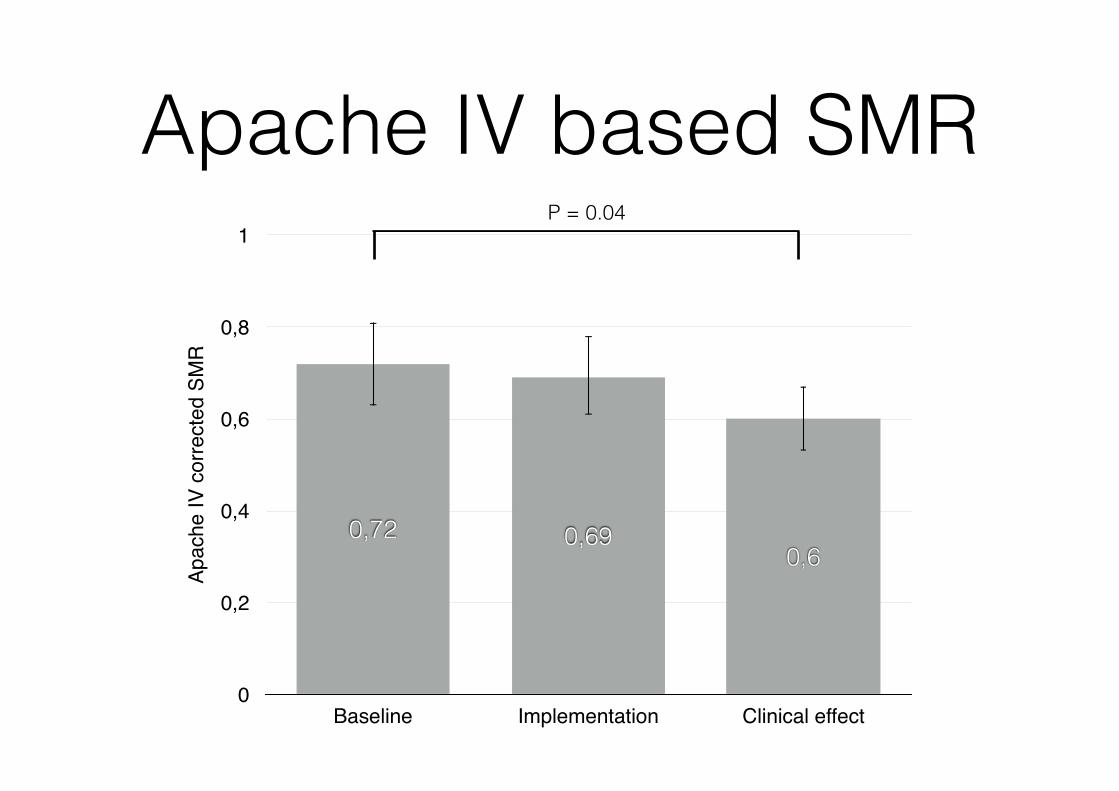
Apache IV based SMRAp
ache
IV c
orre
cted
SM
R
0
0,2
0,4
0,6
0,8
1
Baseline Implementation Clinical effect
0,60,690,72
P = 0.04

Patient-centered
• 24/7 visiting hours
• Active participation of family in physician/nurse rounds
• Presence of family during medical interventions (line placement, tracheostomy), briefing and debriefing procedures and transfers


Equitable and timely: the future of CRM
• Development of a core curriculum including basic training, implementation, refresher course and monitoring/evaluation
• Incorporation of CRM principles in medical- and nursing schools
• Patient empowerment

My conclusions
• CRM has a potential beneficial effect on the 6 dimensions of quality improvement but…..
• Evidence for a positive effect of team-training on patient safety is relatively weak
• Standardization is insufficient