a comparison of functional capabilities of...
TRANSCRIPT

227
1053-0487/99/1200-0227$16.00/0 C 1999 Plenum Publishing Corporation
Injuries to fingers remain the most pervasive nonfatal occupational injuries to the upperextremities in U.S. industries. It is logical to expect that work-related performance of in-dividuals with finger disabilities (e.g., amputated fingers) will be inferior to those with allfingers intact and fully functional. However, the published literature does not provide anyindication how much the functional capabilities of individuals with finger injuries differfrom normal individuals. Knowledge of the nature and extent of decline in the functionalcapabilities of individuals with finger disabilities is necessary in order to make accom-modations in the work place (including job, task, and equipment design), and meet ADAcompliance. This laboratory investigation reports on the differences in the functional ca-pabilities of individuals with and without simulated finger disabilities (amputations) whenperforming routine industrial tasks and standardized strength tests. Twelve male volun-teers participated in the study. The finger disability simulated was of an extreme nature,and was defined as the loss of the use of four fingers in the preferred hand and the thumbin the nonpreferred hand. Subjects performed a variety of dexterity and strength exertiontasks. The dexterity tasks simulated finger dexterity in assembly work and manipulation ofcommon hand tools and included: Modified Purdue Pegboard Test, O 'Connor Tweezer Dex-terity Test, Pennsylvania Bimanual Work Sample Test, and Hand-Tool Dexterity Test. Thestrength exertion tasks determined maximum volitional torque exertion capabilities whenusing common nonpowered hand tools, the psychophysical lifting strength, and standard-ized isometric arm, shoulder, back, and composite lifting strengths, and isokinetic liftingstrength. Results indicated a significant reduction in performance for all dexterity tasks(p > 0.01). In comparison to normal individuals, the dexterity task performance timesof individuals with finger disabilities increased by as much as 190%. The psychophysi-cal lifting strength of the disabled was also significantly lower (<0.01), by as much as35%. In contrast, reductions in standardized strength exertion capabilities of the disabledwere smaller (between approximately 10% and 17%) and, for most tests, not significant(p > 0.10). Strength exertion capabilities with hand tools reflected mixed results. While thetorque capability of the disabled with both screwdrivers and wrenches went down, only thedecline with screwdrivers was significant (p < 0.025). Overall, the results indicated that
1Ergonomics and Engineering Controls Reasearch Laboratory, University of Cincinnati, Cincinnati, OH 45221-0116.
2Correspondence and requests for reprints should be directed to Anil Mital, Ergonomics and Engineering ControlsResearch Laboratory, Industrial Engineering, University of Cincinnati, Cincinnati, OH 45221-0116.
Journal of Occupational Rehabilitation, Vol. 9. No. 4, 1999
A Comparison of Functional Capabilities of IndividualsWith and Without Simulated Finger Disabilities:An Exploratory Study
Arunkumar Pennathur1 and Anil Mital1,2

228 Pennathur and Mital
the performance of tasks that depended upon finger dexterity for completion, even those thatrequired significant force exertions (e.g., psychophysical lifting strength exertion capabil-ity), declined significantly. While tasks that did not require appreciable dexterity and couldbe performed by the palm of the hand and thumb, or fingers, forming the two claws didnot show a significant decline in capability. It is worth noting that the decline in capabilityin such cases, even though statistically insignificant, was very appreciable and of greatpractical consequence.
KEY WORDS: finger disability; isometric strengths; isokinetic strengths; dexterity; psychophysical liftingstrength; nonpowered hand tools; volitional torque exertion capability.
INTRODUCTION
According to the Bureau of Labor Statistics (BLS) (1), from 1993 to 1995, injuries tothe fingers were the most numerous among all upper extremities (including hands, arms,wrists, and fingers) in all U.S. industries. Even though more recent data are not yet available,these trends have been prevalent for many years and are expected to remain unchanged formany years. The data on the distribution of finger injuries and impairments by industrytype show that finger impairments are most prevalent in manufacturing industries (38%)and wholesale and retail trade industries (29%). A majority of the injuries to the fingersare the result of contact with objects (contact including fingers being struck by or againstobjects, or being caught in objects). Machinery, tools and equipment, and other parts andmaterials are the major sources of injuries and impairments to the fingers. Among all U.S.occupations, operators, fabricators, and laborers are most susceptible to finger injuries. In1995, nearly 40% of injuries to fingers resulted in a workday loss of more than 6 days. Inthe same year, nearly 85% of all injuries to fingers were to the age group between 20 and 54years; this age group is considered the normal industrial working age group. Men sufferedmore injuries to the fingers than women (131, 967 in 1995 compared to 43,748 for womenin 1995). As stated earlier, the BLS data also indicate that the incidence and nature of fingerinjuries have not decreased or changed in recent years.
The injury data presented above, when viewed in concert with the requirement foremployers to make "reasonable accommodations" for their disabled workers, necessitatesconsideration of a variety of approaches to disability management. Worker accommodationis an integral part of these disability management approaches. Mital and Pennathur (2),among others (3,4), have argued for multidisciplinary approaches to disability manage-ment and occupational rehabilitation of injured workers. Specifically, they have advocatedintegration of design and engineering knowledge with common management and admin-istrative practices in rehabilitation. Ergonomics can help disabled individuals overcometheir limitations by analyzing and matching physical and mental work requirements (mea-sured by attributes such as task frequency and duration), and their capabilities (measuredby attributes such as body strength, reach, finger dexterity, hand force, perception, sensoryabilities, and psychomotor and cognitive abilities). The final accommodation (from an em-ployer's perspective) can take the form of task modification or design and use of specialpurpose assistive devices. However, proper and successful accommodation of the disabledand injured does require that specific functional capability design data be available and usedin making such accommodations.
The scientific literature does not address the issue of functional work capability designdata for the injured/disabled adequately. In the context of finger disabilities resulting from

Functional Capabilities of Finger Amputees 229
finger injuries (amputations, cuts, burns, etc.), authors were unable to identify any suchstudy in the published literature. The only study that has even approached this issue wasconducted by Mital and Mehta (5) who studied the kinematic parameters of the wrist ofdisabled individuals to determine if the loss of ability to grasp containers (with fingers)would result in significant changes in peak load accelerations during manual lifting tasks.These investigators reported that peak load accelerations were indeed lower for individualswith simulated finger disabilities. The investigators finally concluded that individuals withimpaired fingers are subjected to increased physical stress while performing manual han-dling tasks. The only other data exist in the form of survey data collected from users ofprosthetic devices for the upper limbs (6). These data indicate that users of prosthetic de-vices consider the ability to hold both small and large objects (considered a function) asimportant. Further, these survey data indicate that there is a dire need for the designers ofsuch devices to recognize the versatility of the human hand, and, instead of duplicatingthe human hand in a prosthetic hand, to design only the important functional features insuch devices (7). According to Heckathorne,"... many bilateral upper-limb amputees areconcerned with a single general objective—the ability to efficiently handle a greater varietyof objects and apply higher forces, improved ability to orient the prehensor (especiallywith respect to improved wrist action) and better control of prehension with the inclusionof feedback of prehension force" (8). According to Scott, "... whether it is feasible toachieve independent finger movement, or whether a conformable grip, in which fingersadapt automatically to the shape of an object, would be an adequate response to this need,are questions requiring further study. Balancing the cost versus benefit will be important:costs such as added weight and reduced reliability have defeated many elegant designs inthe past" (9). There is some progress in building powered prosthetic devices that permitindividual finger movements, possibly coupled with direct skeletal attachment (10). Thereis, however, a long way to go in clearly relating finger functions in the disabled and taskperformance.
Given the conclusion reached by Mital and Mehta (5), the preponderance of fingerinjuries in the workplace as evidenced by the BLS injury data, and a dearth of informationon the functional capability of individuals with impaired fingers, it is logical that efforts bedirected to generate functional capability design data for proper workplace accommodationsof individuals who have impaired fingers. However, before undertaking a large study forthis purpose, it would be desirable to know if in fact the functional capabilities of individualswith finger impairments are lower than those with no finger impairments. This work wasundertaken to make this determination. A statistically significant or practically relevantdifference in the capabilities of the two populations would indicate the need for a largerstudy, or a series of studies, to establish functional capability design databases for theafflicted population. This paper reports the results of a laboratory investigation undertakento compare the functional capabilities of individuals with and without simulated fingerdisabilities.
METHODS
In order to achieve the overall objective of this work, a number of individual exper-iments simulating actual tasks and standardized tests were performed. The aim in eachexperiment was to compare the functional capabilities of individuals with and without

230 Pennathur and Mital
simulated finger disabilities. The experiments conducted simulated: (1) tasks requiring fin-ger dexterity, and (2) tasks requiring overall strength exertion capabilities. Many of the tasksin the second category represented standardized strength tests (11).
Following is a description of the disability that was simulated, the subjects who par-ticipated in the study, and the tasks these subjects performed.
The Disability
The disability simulated was defined as the loss of the use of four fingers in the primary(preferred) hand and the thumb in the nonpreferred hand. Figure 1 depicts the disability
Fig. 1. Disability conditions simulated (loss of use of four fingers in the preferredhand and the thumb in the nonpreferred hand.

Functional Capabilities of Finger Amputees 231
that was simulated in all experimental tasks subjects performed in this study. Simulation ofthe disability was achieved by taping, with a nylon tape, four fingers of the preferred handand the thumb of the nonpreferred of each subject. The taping of the fingers did not in anymanner restrict the movement of the thumb or the four fingers. It was also ensured that thetape, while preventing movement of the taped fingers, was not excessively tight to restrictblood flow. It was ensured that the subjects were not in pain when performing the tasksbecause of the restraining tape.
The disability simulated was purposely made severe. Also, the majority of experimentaltasks were designed to require finger dexterity. A lack of finger dexterity, due to the simulateddisability, would make performing these tasks difficult for the disabled subjects to perform,resulting in deteriorated performance. It was rationalized that if there was even a smalldifference in performance of individuals with and without disability, it would be evidentwith such a drastic disability. Any less severe disability would lead to lesser, and verylikely inconsequential, deteriorations in performance. If, on the other hand, the performancedifferences turned out to be large, it would indicate that even minor disabilities could reduceperformance significantly and a host of functional capability design databases, specific tovarious disabilities, will eventually need to be developed.
Subjects
Twelve male student volunteers participated in the study. They were recruited from agraduate class in ergonomics. All twelve subjects performed in both conditions, with andwithout the simulated disability; each subject served as his own control. All subjects werehealthy and had no prior history of any physical ailment. None was on medication. Theirage ranged from 23 years to 40 years. All participants were right-handed (preferred hand).The isometric strengths of these individuals were measured and found comparable to iso-metric strengths of industrial workers (12).
The Experimental Tasks
As stated earlier, the experimental tasks performed primarily required either the dex-terity of the fingers (e.g., tasks such as assembly, manipulation of hand tools, and handlingof objects) or strength (e.g., isometric arm strength, isokinetic lifting strength, and apply-ing torque with wrenches and screwdrivers) for completion. The dexterity tasks performedwere: (1) Modified Purdue Pegboard Test to measure assembly or fingertip dexterity; (2) theO'Connor tweezer Dexterity Test to measure dexterity in work that needs precision andsteadiness in the use of small hand tools such as tweezers; (3) the Pennsylvania BimanualWork Sample to measure finger dexterity of both hands, gross movements of both arms,bimanual coordination, eye-hand coordination, and the individuals ability to use both handsin cooperation in an assembly task; and (4) the Hand-Tool Dexterity Test to measure pro-ficiency in using certain types of mechanics' tools. The details of the equipment and testprocedures for each of these experimental tasks is given below:
1. Modified Purdue Pegboard Test. The equipment used for the test was the Model32020 Purdue pegboard. Subjects were comfortably seated at normal table height(30"). The pegboard was placed directly in front of the subject, with cups containing

Fig. 2. Modified Purdue pegboard test in normal and disabled conditions.
pins, collars, and washers at the far end of the pegboard (Fig. 2). It was ensured thatcups at extreme right and extreme left of the center contained 25 pins each, and thecups immediately to the right and left of the center contained 50 collars and 100washers each, respectively. All subjects were instructed on the goal of the experi-ment (i.e., to determine how quickly and accurately they could perform an assemblytask with their hands). They were then provided instructions on the assembly op-erations involved in the Purdue pegboard test (13). The subjects were allowed topractice assembly operations until they fully understood that both hands had to beoperating all the time during the test, one picking up a pin, one a washer, one a collar,etc. Each subject performed three trials each with and without the simulated disabil-ity. The order in which each subject performed the experimental task with the two
232 Pennathur and Mital

experimental conditions (with and without disability) was randomized. Departingfrom the original Purdue Pegboard Test, that is instead of count data on the numberof assemblies made in one minute, the time taken to completely fill all the 50 holesin the entire pegboard with assemblies was monitored. The protocol was modifiedfrom the original Purdue Pegboard Test in order to reflect a more realistic worksituation—in reality, partial completion of a task has no meaning. In other words,what fraction of the job can be done in 1 minute is irrelevant (as used in the originalPurdue Pegboard Test). What is more important is completion of the "whole" task.
2. O'Connor Tweezer Dexterity Test. The equipment used was a standard 5-7/8"wide x 11-5/8" long O'Connor Tweezer Dexterity board (14). The board con-tained 100 holes 1/16" in diameter and arranged in 10 rows of 10 holes each spaced1/2" apart. Pins, 1" long and 1/16" in diameter, were placed in a pin well 1/2"deep and 4-3/4" in diameter. The subjects were comfortably seated at normal tableheight. Because all subjects were right-handed (preferred hand), the Tweezer Dex-terity Test was placed about a foot from the edge of the table with the tray at theright. All subjects were instructed to pick up one pin at a time with the tweezers andto fill all holes, placing one pin in each hole as fast as they could (Fig. 3). Subjectswere instructed to pick up pins by the end opposite, or farthest away, from them,and fill holes from left to right (because all the subjects were right-handed), andcomplete each row before beginning the next one. They were instructed only touse the hand in which they held the tweezers. The experimenter then demonstratedthe correct procedure to fill the holes with pins, pointing out to the subjects thatthere were enough pins in the tray to make up for any pins that may be droppedwhile attempting to place the pins in the holes. Subjects were asked not to worryabout stopping to pick any dropped pins. They were then allowed to practice fillingthe top row of the board. After a brief period of rest, the subjects were instructed toperform the test. The total time elapsed between the placement of the first and thelast pins was recorded. Each subject performed three trials without the simulateddisability, and three trials with the simulated disability. The order in which each ofthe subjects performed the experimental task with the two experimental conditions(with and without disability) was randomized.
3. Pennsylvania Bimanual Work Sample. The equipment used was the standard Penn-sylvania Bimanual Work Sample Test board (15) consisting of a tray with wellscontaining 105 nuts and 105 bolts at the extremes of the board, and 100 holes inthe center portion of the board (Fig. 4). The subjects were seated comfortably atnormal table height. They were instructed to place a bolt with a nut on it (with atwist just enough to catch the nut) into each of the 100 holes in the board as rapidlyas they could. They were asked not to worry about picking up a dropped nut or abolt (as the wells contained 105 nuts and bolts). Each subject was provided an op-portunity to practice filling the first two rows of holes to ensure that he understoodthe proper motion sequence in performance of the assembly task. After practicing,and after removal of assemblies from the first two rows, subjects were instructedto fill all 100 holes as fast as they could. The total hole filling time was recorded.Each subject performed three trials with and without the simulated disability. Theorder in which each of the subjects performed the experimental task with the twoexperimental conditions was completely randomized.
Functional Capabilities of Finger Amputees 233

Fig. 3. O'Connor tweezer dexterity test in normal and disabled conditions.
4. Hand-Tool Dexterity Test. The goal of this test was to measure subjects' dexterityin using common mechanics' tools (16). The equipment used for the hand-tooldexterity test consisted of a wooden frame with two uprights (Fig. 5). The entireframe was mounted on the table (considered to be the work bench). Bolts (with theheads of the bolts on the inside) were placed in the holes on the frame upright left ofthe subjects (because all subjects were right-handed). The tools used in the test werecommon wrenches of different sizes. These tools were placed at the center of theframe between the uprights. It was ensured that nuts on the bolts were not too tightnor too loose. Subjects were then instructed on the objective of the experimental task(to remove all the bolts from the left upright and place them on the correspondingrows on the right upright with the heads of the bolts on the inside, using the tools
234 Pennathur and Mital

Fig. 4. Pennsylvania Bimanual work sample test in normaland disabled conditions.
provided) and the protocol to be followed. The experimenter demonstrated theprotocol: all the bolts from the top row of the left upright was removed first, andlaid on the bench. The nuts on all rows were loosened enough to be able to spin offthe nuts with the fingers. The bolts in the middle row was then removed and laidon the bench. As and when each bolt in the bottom row was removed, it was placedin the corresponding hole in the right upright. All smallest bolts were mountedand the nuts were tightened initially with the fingers and then with the use of thetools. The middle row containing the medium sized bolts were then mounted andtightened with nuts. The top row of bolts was then mounted and tightened with nutsfollowing the same procedure. The subjects were explicitly instructed not to applytoo much pressure with the wrenches, but make the fastening tight enough so that
Functional Capabilities of Finger Amputees 235

236 Pennathur and Mital
Fig. 5. Handtool dexterity test in normal and disabled conditions.
the nuts could not be removed with the fingers. After the demonstration, subjectswere asked to proceed with the test. Each subject performed three trials with andwithout the simulated disability. The order in which each subject performed theexperimental task with the two experimental conditions was randomized. The totaltime taken for removing nuts and bolts from all rows on the left upright and mountall the nuts and bolts in corresponding rows on the right upright was recorded.
The tasks requiring strength exertion included the following: (1) exertion of maximumvolitional torque when using a screwdriver and a spanner wrench; (2) maximum isometricarm lifting strength; (3) maximum isometric shoulder lifting strength; (4) maximum iso-metric back lifting strength; (5) maximum isometric composite lifting strength; (6) peakisokinetic dynamic back extension strength at slow and fast speeds of exertion; and (7) max-imum psychophysical lifting strength (maximum acceptable weight of lift) using containers
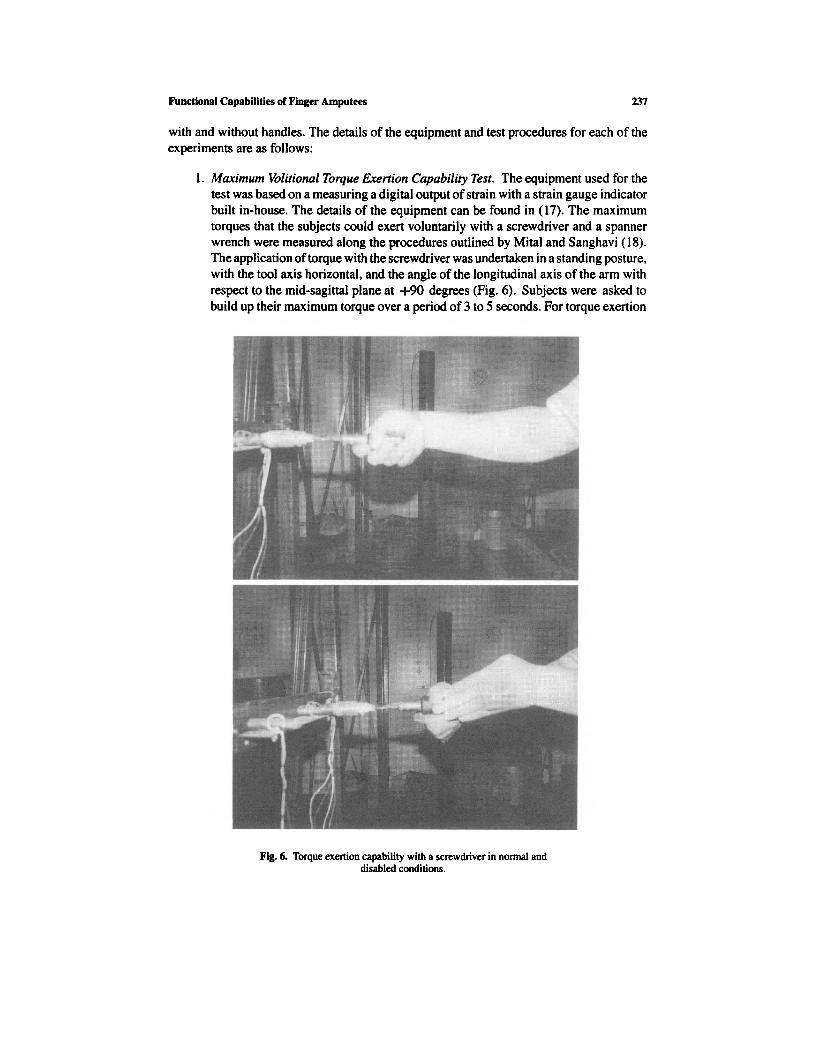
Fig. 6. Torque exertion capability with a screwdriver in normal anddisabled conditions.
with and without handles. The details of the equipment and test procedures for each of theexperiments are as follows:
1. Maximum Volitional Torque Exertion Capability Test. The equipment used for thetest was based on a measuring a digital output of strain with a strain gauge indicatorbuilt in-house. The details of the equipment can be found in (17). The maximumtorques that the subjects could exert voluntarily with a screwdriver and a spannerwrench were measured along the procedures outlined by Mital and Sanghavi (18).The application of torque with the screwdriver was undertaken in a standing posture,with the tool axis horizontal, and the angle of the longitudinal axis of the arm withrespect to the mid-sagittal plane at +90 degrees (Fig. 6). Subjects were asked tobuild up their maximum torque over a period of 3 to 5 seconds. For torque exertion
Functional Capabilities of Finger Amputees 237

238 Pennathur and Mital
Fig. 7. Torque exertion capability with a wrench in normal and disabledconditions.
with a spanner wrench (Fig. 7), a standing posture was adopted. The tool axis waskept vertical (upward), and the angle of the longitudinal axis of the arm with respectto the mid-sagittal plane was at -90 degrees. Each subject performed three trialswith and without the simulated disability. The order of exertion was randomizedacross subjects, tools, and the two experimental conditions. A rest period of at least5 minutes was provided after each trial to avoid any fatigue that may be causedbecause of the isometric torque exertion.
2. Isometric Arm Lifting Strength. The equipment used for measuring the isometricarm lifting strength was a Prototype Strength Testing Device. To determine armlifting strength, the long handle in the equipment was adjusted such that the subject's

forearms were flexed at 90 degrees (perpendicular to the subject's torso), and theupper arms were vertical (parallel and adjacent to the torso). The subject wasinstructed to stand erect, with legs and back straight and with feet flat, exert anupward vertical force generated only by the arm muscles, and to avoid any jerkexertion on the fixed handle, and any movement of the shoulder. Once the desiredposture was achieved, the subject built the maximum strength by trying to lift thehandle upwards gradually over a 3- to 5-second period, and held at the maximumstrength for about one second. A load cell connected to the column and the platformon which the subject stood while performing the task, provided the output on adigital strain indicator. Three readings, within 10% of each after were recorded foreach subject under both conditions (with and without the simulated disability). Theorder of exertion was randomized across subjects and experimental conditions. Abrief rest break of at least a 2 minutes was provided after each exertion to recoverfrom any fatigue that may have built up.
3. Isometric Shoulder Lifting Strength. The same equipment used for measuring iso-metric arm strength was also used for measuring the isometric shoulder liftingstrength. The long handle in the equipment was adjusted such that the forearms ofthe subject were vertical (parallel and adjacent to the torso), and the upper armshorizontal (perpendicular to the torso). The position of the feet and back remainedthe same as in the case of arm strength measurement. The rest of the procedure wasthe same as for isometric arm strength.
4. Isometric Back Lifting Strength. The equipment used for measurement of the backstrength was the same as in the case of arm and shoulder strengths. The long handlewas located at about 15 inches from the platform on which the subject stood,and approximately 15" in front of the medial malleolus. The subject's feet wereseparated at shoulder width. It was ensured that both feet were at an equal distancefrom the column anchor point in the equipment. The subjects were instructed toflex the torso in order to grip the fixed handle, and exert an upward vertical force byextending the torso. It was ensured that the elbows and knees were fully extendedand that the eyes were looking straight ahead. The rest of the procedure was thesame as for isometric arm and shoulder strengths.
5. Isometric Composite Strength. The long handle in the strength testing equipmentwas replaced with a shorter handle to let the subject assume a semi-squat positionsuch that the hands were between the legs, at approximately 38 cm height. It wasensured that the individual's elbows were extended and that there was no contactbetween the upper and the lower extremities. It was also ensured that the feetremained flat and that the subject look straight ahead. Rest of the experimentalprocedure was the same as for other isometric strengths.
6. Isokinetic Dynamic Back Extension Strength. The equipment used was a Super IIMini-Gym with a mechanical speed control device. This equipment measures themaximal voluntary contraction when a subject pulls a handle attached to a rope,at constant speed. In this case, the maximum isokinetic floor-elbow strength (floorto approximately 80 cm) for a single exertion was measured. The protocol usedwas the same as in the case of isometric back strength. The speed control devicewas adjusted to set the speed of exertion at 0.30 m/s (considered slow speed). Thesubjects were instructed to assume a free-style posture, and pull the handle up as
Functional Capabilities of Finger Amputees 239

fast as possible, but without producing any jerking movement, to elbow height.Three readings, within 10% of each other were recorded for each subject underboth treatment conditions (with and without the simulated disability). The order ofexertion was randomized across subjects and the two experimental conditions. Abrief rest break of at least 2 minutes was provided after each exertion to recoverfrom any fatigue that may have built up. The same procedure was repeated for aspeed of 0.75 m/s (considered fast speed) and the values tabulated.
7. Psychophysical Lifting Strength Capability. Psychophysical strength is defined asthe maximum acceptable weight of lift. The procedure required subjects to adjustthe weight of lift according to his/her perception of physical strain. The equipmentused for measuring the psychophysical strength in this consisted of a wooden boxwith handles (0.45 m long in the sagittal plane, 0.15 m high, and 0.30 m wide inthe frontal plane), a set of loose weights, and a wooden platform (at a height ofapproximately 82 cm) on which to place the box. The subjects were instructed toadd or remove the loose weights to/from the box. They were started with either avery heavy load they could not lift, or a very light load they could easily lift. Theywere allowed to make as many adjustments they needed in order to arrive at themaximum acceptable weight of lift for a singular lift (19). Lifting was performedwith or without handles. During lifting without the use of handles, the box washeld at diagonally opposing corners, with the preferred hand at the bottom cornercloser to the body, and the nonpreferred hand at the top corner away from the body).Each subject performed three trials with and without the simulated disability. Theorder in which each of the subjects performed the trials was randomized acrossthe lifting tasks and disability conditions. The final total weight in the box pro-vided the maximum acceptable weight of lift for a single exertion for a particularsubject.
RESULTS
The performance data (means for the two experimental conditions—performance withsimulated finger disability and performance with no finger disability) for each experimentaltask were statistically analyzed. Because there were multiple responses, a correlation anal-ysis was carried out to determine how the responses were related to each other. The highestcorrelation between any two responses was less than 0.5. This indicated that each test (re-sponse) could be treated as an independent experiment and analyzed using a univariateanalysis. In other words, a multivariate t-test was not required. The respective performancedata (with and without the simulated finger disability), therefore, were compared and an-alyzed using a paired t-test. A summary of t-test results for all experimental tasks andstandardized strength tests is presented in Table I.
Overall, the results indicated that subjects' performance deteriorated with the simu-lated finger disability. The decline in performance was statistically significant for all tasksrequiring finger dexterity (p < 0.01). In general, disabled subjects took up to as muchas nearly three times longer to perform dexterity tasks. This represents an increase in taskperformance time by as much as nearly 200%. The minimal increase in performance timewas 70%.
240 Pennathur and Mital

Functional Capabilities of Finger Amputees 241

The psychophysical lifting capability also declined significantly with the simulatedfinger disability (p < 0.01). The decline in capability, on the average, was approximately33% when containers were lifted without handles. With handles, the average decline incapability was nearly 35% (the declines in the psychophysical lifting capability for handleand no-handle conditions were not significantly different from each other (p > 0.10)).
The results with hand tools were mixed. While the decline in torque exertion capabilitywith screwdriver was significant for the simulated finger disability condition (p < 0.025),it was practically appreciable but not statistically significant for the spanner wrench (p >0.10). The average decline in the torque exertion capability was approximately 16% for thescrewdriver and nearly 8% for the spanner wrench.
Not unexpectedly, all standardized isometric strength tests did not show any significantdecline in strength exertion capability as a result of the simulated finger disability (p > 0.10).The isokinetic lifting strength decline was only weakly significant (p <0.10). However,in all these cases the actual decline in strength exertion capability was practically appreciableand ranged from nearly 10% to 17%.
DISCUSSION
The overall objective of this work was to determine if in fact the simulated fingerdisabilities led to a decline in the functional capabilities of workers and, if so, how much.The results indicated that such functional disabilities lead to a large reduction in physicalcapabilities. While for some experimental tasks the decline in individual functional capa-bilities was statistically significant, for others it was not. However, even in those cases thatdid not show a statistically significant decline in capability, primarily because of large vari-ance in performance data, the decline was appreciable (e.g., standardized strength tests).If one examines the nature of the tasks that were simulated, it is very clear that the taskscan be grouped into two categories: (1) tasks that require finger dexterity for completionand (2) tasks that can be completed without a great deal of reliance of finger dexterity. Thefollowing tasks were in the first category: Purdue Pegboard task, O'Connor Tweezer task,Pennsylvania Bimanual task, Handtool dexterity task, torque exertion with a screwdriver,and the determination of maximal psychophysical lifting capability (singular exertion).The second category included the following tasks: all isometric lifting strength determina-tions, isokinetic lifting strength determination, and the application of torque exertion witha spanner wrench. The performance and completion of tasks in the first category requiressignificant aid from the fingers. For example, grasping the container lying on the floor.Fingers in this case provide substantial assistance in grasping the box. In the absence offingers, or the thumb, this assistance cannot be readily provided by the palm of the hand,which must form one of the jaws in the hand claw (the other is formed by the thumb). Inthe case of missing thumb, the two jaws of the hand claw are formed by the fingers and thepalm. (Note that the missing thumb is only critical in performing those tasks that requireboth hands, e.g., lifting a container.) The dexterity tasks can eventually be performed with-out fingers, or a thumb, but at the cost of additional time and reduction in capability. Theloss in capability is clearly evidenced in the case of torque exertions with a screwdriver.As explained by Mital et al. (20), the transmission of forces generated in the muscles isultimately achieved by the hand-handtool coupling. While on the surface it may appear thatfingers do not play a major role in forming the coupling with a screwdriver, fingers, unlike
242 Pennathur and Mital

when using wrenches, are critical in preventing slippage when using a screwdriver. Theabsence of fingers does not allow this coupling to be proper and strong, resulting in a lossin capability. Thus, there is clear indication that tasks requiring fine motor movements arevastly difficult for individuals with finger impairments.
For category two tasks, however, the nature of the tasks is such that the absence offingers and thumb is adequately compensated by the palm of the hand. The palm of thehand and fingers, for the nonpreferred hand, and the palm and thumb, for the preferred hand,provide more than marginal compensation for the missing jaws (fingers and thumb) in thegrip. Because the nature of the task mandates whole body exertions, the grip merely has toprovide a strong coupling but not the dexterity. In the case of spanner wrench, the shapeof the tool makes the need for fingers less critical as compared to their need when using ascrewdriver. As a result, in all these cases the decline in functional capability did not turnout to be statistically significant. It is noteworthy, however, that the decline in capabilityis appreciable and can have practical consequences. For instance, a reduction in isometricor isokinetic force exertion capability can result in a faster onset of fatigue and reducedendurance time. This observation is supported by a reduction in the psychophysical liftingcapability as well by manual lifting kinematics (5).
The differences in capability reduction for the two categories of tasks also tend to showthat simulation of realistic tasks is absolutely critical in establishing functional capabilitydesign databases for finger impaired individuals. Failure to do so will lead to incorrectcapability estimations (overestimation) and improper accommodation as the results of thisstudy show.
It is also important to note that there are many other factors, not included in this study,that may affect individuals' functional capacity. Evidence shows that in addition to imme-diate loss of grasp strength and security, finger absence may cause marked psychologicaltrauma (21). Further, even though this trauma varies among individuals, the psychologicalimpact of the injury is not related to the magnitude of the amputation. The appearance ofthe prosthetic device, for instance, has been shown to cause significant embarrassment (22).According to Beasley (23), individuals who keep their hands hidden inside their pocketsbecause of embarrassment over appearance are as functionally disabled as a forequarter(scapulothoracic) amputee. It has also been shown that other psychological factors such aspain, emotional distress related to the loss of a finger, anxiety over return to work expecta-tions, and functional self-efficacy expectancies affect functional capacity (24).
The results of this study and the preceding discussion show that there is a definite needto develop job design databases (including information on equipment and tool design) ifthe goal is to provide a proper fit for the finger disabled. Such a database should not onlybe specific to a disability, it should reflect the effect of psychological trauma in the experi-mental simulation. Furthermore, eventually it would be necessary to establish quantitativegains in functional capabilities that may result from surgical interventions, and interven-tions using prosthetic devices (6). For instance, the recent attempt to transplant the humanhand, if successful, widespread, and economical, can have a positive impact on accom-modation. Is such an impact only marginal or significant in terms of functional capabilitygains?
There is also the issue of compensation and adaptation that typically occur over aperiod of time in injured workers with amputations. From a work accommodation per-spective, however, an employer cannot wait for such a natural compensation in a worker
Functional Capabilities of Finger Amputees 243

244 Pennathur and Mital
to occur—the employer has to redesign the work and/or workplace to accommodate theworker.
The study described in this paper simulated a finger injury. While there are advantagesto such a paradigm of simulating injuries (e.g., one does not need an actual injury to occur),the potential usefulness of the paradigm will depend on the fidelity of such a simulation(compared to an actual injury).
CONCLUSIONS
The results of this study and the foregoing discussion lead to the following conclusions:
1. There is a significant decline in the functional capabilities of individuals with sim-ulated finger disabilities compared to individuals without any finger disabilities.
2. The decline in functional capabilities of individuals with simulated finger disabil-ities is particularly marked in tasks requiring the fingers and/or thumb to form acoupling for task initiation, performance, and completion. Even the whole bodyexertion tasks that do not require the coupling effect from fingers are difficult forindividuals with simulated finger disabilities to perform as evidenced by the declinein their capabilities. The declines in capabilities, in such cases, while not significantstatistically, can be appreciable and practically very significant.
3. Investigations studying specific disabilities and functions/tasks need to be carriedout in order to develop design databases for accommodating such individuals in theworkplace. Future investigations also need to study the effect of personal factors,such as gender, on functional capabilities. Such investigations also need to investi-gate how much of a person's functional capability is restored as a result of surgicalintervention. In addition, the effect of psychological and psychosocial factors suchas pain, emotional distress related to the loss of a finger, anxiety over return towork expectations, and functional self-efficacy expectancies, on return to work,need further research.
REFERENCES
1. Bureau of Labor Statistics. BLS news: Workplace injuries and illnesses in 1995: U.S. Department of Labor.Washington, DC: U.S. Government Printing Office, 1995.
2. Mital A, Pennathur A. Musculoskeletal overexertion injuries in the United States: Mitigating the problemthrough ergonomics and engineering interventions. J Occup Rehab 7999; in press.
3. Feuerstein M. A multidisciplinary approach to the prevention, evaluation, and management of work disability.J Occup Rehab 1991; 1: 5–12.
4. Feuerstein M. Workers' compensation reform in the New York State: A proposal to address medical,ergonomic, and psychological factors associated with work disability. J Occup Rehab 1993; 3: 125-134.
5. Mital A, Mehta M. Manual lifting: Kinematics of a disability. In: Mital A, Karwowski W, eds. Ergonomicsin Rehabilitation. London, United Kingdom: Taylor and Francis, 1988, pp. 161-170.
6. Atkins DJ, Heard DCY, Donovan WH. Epidemiologic overview of individuals with upper-limb loss and theirreported research priorities. JPO 1996; 8: 2–11.
7. LeBlanc MA. Expert analysis of the TIRR national upper-limb amputee database. Archived at The Institutefor Rehabilitation and Research in Houston, November 1994.
8. Heckathorne CW. Expert analysis of the TIRR national upper-limb amputee database. Archived at TheInstitute for Rehabilitation and Research in Houston, November 1994.
9. Scott RN. Expert analysis of the TIRR national upper-limb amputee database. Archived at The Institute forRehabilitation and Research in Houston, November 1994.

Functional Capabilities of Finger Amputees 245
10. Childress DS. Expert analysis of the TIRR national upper-limb amputee database. Archived at The Institutefor Rehabilitation and Research in Houston, November 1994.
11. Mital A, Kumar S. Human muscle strength definitions, measurement, and usage: Part I—Guidelines for thepractitioner. Int J Ind Erg 1998; 22: 101–121.
12. Mital A. Comprehensive maximum acceptable weight of lift data base for regular 8-hour work shifts. Erg1984; 27: 1127-1138.
13. Tiffin J, Asher EJ. The Purdue pegboard: Norms and studies of reliability and validity. J App Psych 1948; 32:234–247.
14. Hines M, O'Connor J. A measure of finger dexterity. Pers J 1926; 4: 379–328.15. Roberts JR. Pennsylvania Bi-manual Work Sample. Circle Pines, MN: Educational Test Bureau Division,
American Guidance Service, Inc., 1945.16. Lafayatte Instrument Company. Hand-tool dexterity test. Lafayette, IN, Lafayette Instrument Company Press,
1980.17. Channaveeraiah C. A Study of the effects of grips, postures, and duration of exertion on peak torque exertion
capabilities with common handtools. Unpublished Masters Thesis, University of Cincinnati, Cincinnati, OH,1986.
18. Mital A, Sanghavi N. Comparison of maximum volitional torque exertion capabilities of males and femaleswith common handtools. Int J Ind Erg 1986; 28: 283–294.
19. Mital A, Nicholson AS, Ayoub MM. A Guide to Manual Materials Handling. London, United Kingdom:Taylor and Francis, 1997.
20. Mital A, Sanghavi N, Huston T. A study of factors defining the 'operator-hand tool system' at the workplace.Int J Prod Res 1985; 23: 297–314.
21. Pillet J. The aesthetic hand prosthesis. Orthop Clinics in North Amer 1981; 12: 961–970.22. Buckner H, Michael JW. Options for finger prostheses. JPO 1993; 6: 10–19.23. Beasley RJ. General considerations in managing upper-limb amputations. Orthop Clinics in North Amer
1981; 12: 743-749.24. Lackner JM, Carosella AM, Feuerstein M. Pain expectancies, pain and functional self-efficacy expectancies
as determinants of disability in patients with chronic low back disorders. J Consul Clin Psych 1996; 64:212-220.