a critical review of culturally sensitive treatments for ... critical review of culturally sensitive...
TRANSCRIPT

A Critical Review of Culturally Sensitive Treatments for Depression:Recommendations for Intervention and Research
Zornitsa Kalibatseva and Frederick T. L. LeongMichigan State University
Recent meta-analyses and reviews have showed that culturally adapted mental health interventions aremore effective for racial and ethnic minorities than traditional unadapted psychotherapy. Despite theadvances in providing culturally sensitive mental health services, disparities among racial and ethnicminorities still exist. As a body of literature on culturally sensitive treatments accumulates, there is a needto examine what makes a treatment for specific presenting problems culturally sensitive. This articlepresents a critical review of existing culturally sensitive treatments for depression because it is one of themost common and debilitating mental disorders. In particular, we examined what treatment modalitieswere used, what types of adaptations were implemented, and what populations were targeted. Theconceptual framework this review uses to categorize existing culturally sensitive treatments includes atop-down, a bottom-up, or an integrative approach. The review reveals that the majority of culturallysensitive treatments for depression employed an evidence-based bottom-up approach, which involvedgeneral and practical adaptations, such as translating materials or infusing specific cultural values. Moststudies used cognitive–behavioral strategies and included Latinos and African Americans. Recommen-dations and future directions in interventions and research are discussed to decrease mental health caredisparities among ethnic minorities.
Keywords: culturally sensitive treatment, culturally adapted treatment, depression, racial/ethnicminorities, adaptation, therapy
Depression is among the most debilitating disorders and largestcontributors to the world’s global burden of disease (World HealthOrganization [WHO], 2008). Therefore, it has been of paramountimportance to find effective psychosocial treatments for depres-sion and examine what treatments work for whom (Norcross &Wampold, 2011). Previous reviews of psychosocial treatmentswith ethnic minorities (Huey & Polo, 2008; Miranda et al., 2005)and meta-analyses (Benish, Quintana, & Wampold, 2011; Griner& Smith, 2006; Smith et al., 2011) have examined the overalleffectiveness of cultural adaptations in various treatments targetingmultiple disorders. In particular, cultural adaptations appear to bemore effective than no treatment (d � 0.58), treatment as usual(d � 0.22) or unadapted psychotherapy (d � 0.32; Benish et al.,2011; Huey & Polo, 2008) and show moderately strong benefitfrom pre- to post- intervention (d � 0.45; Griner & Smith, 2006).As depression is one of the most prevalent and incapacitatingmental disorders and mental health professionals strive to provideadequate depression treatment to all patients, it is important toexamine in depth the culturally sensitive treatments for depressionin the United States.
Since the existing evidence-based treatments (EBTs) in theUnited States are infused with Western norms, researchers need to
determine whether such treatments are equally effective for otherpopulations (e.g., ethnic minorities or nationals of other countries)or whether new culturally sensitive treatments are necessary (Ber-nal & Domenech Rodríguez, 2012; Gone, 2009). In the last de-cade, several studies explored the development and implementa-tion of culturally sensitive treatments (CSTs) for depression fordifferent ethnic groups. However, this growing body of literaturehas not been reviewed and analyzed. The goal of this article is toprovide a critical review of the literature on culturally sensitivetreatments for depression and to establish what makes a depressiontreatment culturally sensitive, how effective such treatments are,and what populations CSTs targeted. Conceptually, this reviewexamines the existing culturally sensitive treatments using a top-down approach or surface adaptations, a bottom-up approach ordeep adaptations, and an integrative approach or a combination oftop-down and bottom-up approaches. In the final section, we offerrecommendations for future research and implementation of CSTsfor depression with the goal to reduce mental health disparitiesamong culturally diverse groups.
CSTs entail “the tailoring of psychotherapy to specific culturalcontexts” (Hall, 2001, p. 502). Bernal and Domenech Rodríguez(2012) examined cultural adaptations within the framework ofevidence-based practice. The authors discussed the relationshipbetween psychotherapy and culture, which can range from “invis-ible” or “absent” to “inseparable” or “intertwined” (Bernal &Domenech Rodríguez, 2012, p. 4). Multiple terms have been usedto describe the variability and gradation in the relationship be-tween culture and psychotherapy, such as “culturally adapted,anchored, appropriate, centered, competent, congruent, informed,relevant, responsive, and sensitive” (p. 4). For example, the term
Zornitsa Kalibatseva and Frederick T. L. Leong, Department of Psy-chology, Michigan State University.
Correspondence concerning this article should be addressed to ZornitsaKalibatseva at the Department of Psychology, 127B Psychology Building,Michigan State University, East Lansing, MI 48824-1116. E-mail:[email protected]
Psychological Services © 2014 American Psychological Association2014, Vol. 11, No. 4, 433–450 1541-1559/14/$12.00 DOI: 10.1037/a0036047
433

culturally embedded implies the strongest relationship such thatpsychotherapy is considered an integral part of the context,whereas culturally adapted suggests systematic changes to theprotocol of an existing treatment in order to make features of thetreatment relevant to the culture of the target population. Morespecifically, cultural adaptation is “any modification to anevidence-based treatment that involves changes in the approach toservice delivery, in the nature of therapeutic relationship, or incomponents of the treatment itself to accommodate the culturalbeliefs, attitudes, and behaviors of the target population” (Whaley& Davis, 2007, pp. 570–571). The term culturally sensitive is usedin this review to indicate varying degrees of integration of culturein psychotherapy, which may range from culturally embeddedpsychotherapy to one or two specific cultural adaptations, such aschanging the language or hiring bicultural staff.
Culture, Race, Ethnicity, and Disparities in ServiceUtilization Among Ethnic Minorities
In the last two decades, there has been an increased awarenessof the influence of culture on psychopathology and psychotherapy(Leach & Aten, 2010; López & Guarnaccia, 2000). Workingdefinitions of race, ethnicity, and culture are provided below asthese concepts are often used interchangeably (Betancourt & Lo-pez, 1993). Race refers to similar observable physical character-istics, such as skin color, hair type and color, eye color, and facialfeatures. It often implies biological variation as the physiognomicfeatures specific to one race are associated with populations withinisolated geographic locations (Betancourt & Lopez, 1993). Ethnic-ity usually refers to groups that share characteristics, such asnationality, language, history, traditions, race, and/or culture. Typ-ically, ethnic characteristics occur simultaneously with race andculture, which may contribute to the common interchangeable useof these terms.
Culture refers to “highly variable systems of meanings, whichare learned and shared by a people or an identifiable segment of apopulation” (p. 630; Betancourt & Lopez, 1993; Rohner, 1984).Psychologically relevant elements that constitute culture represent“social norms, roles, beliefs, and values” (Betancourt & Lopez; p.630) and may include topics, such as familial roles, gender roles,communication styles, affective styles, values of authority or per-sonal control, individualism, collectivism, and spirituality amongothers (Betancourt & Lopez). These culturally relevant elementsmay influence how people report and conceptualize their experi-ence of distress, determine if they seek and/or stay in treatment aswell as their treatment outcome (U.S. Department of Health andHuman Services [DHHS], 2001).
Data from the Collaborative Psychiatric Epidemiology Surveysrevealed that lifetime prevalence rates of depression among U.S.racial and ethnic groups varied. Approximately 13.5% of Hispan-ics, 11.4% of Native Americans, 10.8% of non-Hispanic Blacks,17.9% of non-Hispanic Whites, and 9.1% of Asian Americans metcriteria for major depressive episode (Beals et al., 2005; Breslau etal., 2006; Takeuchi, Hong, Gile, & Alegría, 2007). Researchershave found significant disparities in depression treatment amongethnic minorities in the United States despite the similar or lowerprevalence rates of depression compared to non-Hispanic Whites(Alegría et al., 2008; Harman, Edlund, & Fortney, 2004). In anationally representative sample, Alegría et al. (2008) identified
significant ethnic differences in utilization of mental health ser-vices among people diagnosed with past-year depressive disorder,with 63.7% of Latinos, 68.7% of Asians, and 58.8% of non-Hispanic Blacks, compared with 40.2% of non-Hispanic Whites,failing to access services. Moreover, there were disparities in thelikelihood of both having access to and receiving adequate care fordepression for Asian Americans and non-Hispanic Blacks in con-trast to non-Hispanic Whites. These findings are consistent withthe disparities in service utilization reported in the supplement tothe U.S. Surgeon General Report Mental health: Culture, race,and ethnicity (U.S. DHHS, 2001). The supplement provided anoverview of the limited mental health research with ethnic minor-ities and described the lack of information as a “critical disparity”(p. 159, U.S. DHHS, 2001).
Evidence-Based Treatments and Culturally SensitiveTreatments
The recognition of mental health service utilization disparitiesand the scarcity of research on psychological treatments withethnic and racial minority populations necessitated the carefulexamination of all available information in this field. Two majorreviews of psychosocial treatments with ethnic minority youth andadults (Huey & Polo, 2008; Miranda et al., 2005) concentrated onanswering the question of whether or not EBTs that have beenpredominantly tested with White middle-class English-speakingclients can generalize to ethnic minorities. Evidence-based treat-ments (EBTs) refer to “the interventions or techniques (e.g.,cognitive–behavioral therapy for depression, exposure therapy foranxiety) that have produced therapeutic change in controlled tri-als” (Kazdin, 2008, p. 147). Since the majority of “possibly effi-cacious” EBTs have been developed and tested primarily withWhite, middle-class, English-speaking women, mental health pro-fessionals have questioned their efficacy with ethnic minorities(Bernal & Scharrón-del-Río, 2001; Miranda et al., 2005).
Based on a limited number of EBT studies the earlier reviewconcluded that cognitive–behavioral therapy (CBT) and interper-sonal therapy (IPT) are effective for African Americans and Lati-nos (Miranda et al., 2005). In the second review, Huey and Polo(2008) focused on the effectiveness of evidence-based treatmentsfor ethnic minority youth and found that based on Chambless andHollon’s (1998) criteria there were no “well-established” treat-ments. Yet, the review suggested that there were some “probablyefficacious” and “possibly efficacious” treatments for anxiety-related problems, attention-deficit/hyperactivity disorder, depres-sion, conduct problems, substance abuse problems, and trauma-related syndromes.
Both review papers concluded that the existing EBTs that havebeen tested with ethnic minorities showed promising results. How-ever, these reviews included both traditional EBTs and culturallysensitive or adapted EBTs with ethnic minorities (e.g., Kohn,Oden, Muñoz, Robinson, & Leavitt, 2002; Rossello & Bernal,1999). Combining both types of treatments in reviews or analysesmay be problematic because it would be difficult to determine ifthe treatment outcome is associated with the traditional treatmentor the culturally sensitive elements.
In the last decade, a growing number of CST studies adaptedEBTs (e.g., Kohn et al., 2002) or developed treatments for specificpopulations with the help of focus groups (e.g., Stacciarini, 2008).
434 KALIBATSEVA AND LEONG

At the same time, a prominent debate in the field of CSTs has beenwhether EBTs should be adapted or not (Atkinson, Bui, & Mori,2001; La Roche & Christopher, 2008). Some researchers believethat EBTs should be used in their original form to preserve theirfidelity, others find a middle ground by proposing cultural adap-tations to existing treatments, and yet others believe that culturecannot be artificially added and culturally sensitive treatmentsshould be generated from specific cultural groups (La Roche &Christopher, 2008).
In an attempt to categorize the existing culturally sensitivetreatments, Cardemil (2008) offered an organizing framework forCSTs that listed three perspectives with their respective advan-tages and limitations. The first perspective states that CST is theproduct of culturally sensitive therapists. The second perspectiveviews CSTs as culturally adapted EBTs. The last perspectiveproposes that CSTs make culture the central focus and mainprinciple in developing the treatment and such approaches areusually described as culturally centered (Bernal & DomenechRodríguez, 2012). Thus, according to the second and third per-spectives, CSTs can encompass cultural adaptations of existingtreatments as well as newly developed treatments for specificgroups of color (Hall & Yee, 2013).
Various researchers have questioned whether it is possible tohave evidence-based treatments that are also culturally sensitive(Atkinson, et al., 2001; Bernal & Scharron-del-Rio, 2001; Hall,2001; La Roche & Christopher, 2008). Therefore, an importantquestion that remains is whether culturally diverse groups wouldbenefit more from culturally sensitive interventions than fromunadapted EBTs.
In support of this idea, Griner and Smith (2006) examined thebenefit of evidence-based culturally adapted mental health inter-ventions. A meta-analysis of 76 studies found an average treatmenteffect size (d � .45) from pre- to postintervention, which indicateda moderately strong benefit of culturally adapted interventions. Inaddition, Griner and Smith found that treatments for groups ofsame-race participants were four times more effective (d � .49)than treatments for groups of mixed-race participants (d � .12).This finding suggests that cultural adaptations for specific groupsmay be more beneficial than general multicultural adaptations.Another important finding was that effect sizes of culturallyadapted treatments increased when participants were older andwhen there was a higher percentage of Hispanic participants. Theauthors attributed the greater benefits of cultural adaptations forthese populations to the impact of acculturation suggesting thatolder populations may be less acculturated than younger popula-tions and some Hispanic populations that do not speak Englishmay be less acculturated. In addition, when the therapist spoke theparticipants’ native language (if not English), the treatment effectwas larger (d � .49) than when the therapist did not speak theparticipants’ native language (d � .21). A logical next step is toreview the nature of the cultural adaptations and test if theycontribute to the already existing treatments.
Smith, Domenech Rodríguez, and Bernal (2011) reviewed ex-isting definitions and means for culturally adapting psychotherapyand provided clinical examples of adapted “traditional” Westerntreatments. The authors conducted a meta-analysis that included8,620 participants from 65 studies and concluded that the cultur-ally adapted treatments had a moderate effect (d � .46). In addi-tion, Smith et al. (2011) suggested that the most effective treat-
ments were those with greater numbers of cultural adaptations.However, none of the existing reviews has primarily focused onthe specific adaptations or elements that would make a treatmentculturally sensitive for a particular disorder.
Cultural Adaptations: Frameworks and Models
Domenech Rodríguez and Bernal (2012) traced the beginning ofcultural adaptation models within positivist approaches to therapy,which emphasize “systematic observation and scientific discov-ery” (p. 23). The authors provided a thorough review of 11 broadframeworks or models for cultural adaptation. Several of theseframeworks were used for culturally sensitive depression treat-ments.
The Multidimensional Model for Understanding Culturally Re-sponsive Psychotherapies (Koss-Chioino & Vargas, 1992) pro-posed two dimensions of psychotherapy: culture and structure. Thedimension of culture included cultural content and cultural contextand the dimension of structure consisted of process and form.Kohn et al. (2002) used a framework that resembled this one toculturally adapt a CBT for African American women.
Another framework that has been used in a number of culturallysensitive treatments is the Ecological Validity Framework (EVF;Bernal, Bonilla, & Bellido, 1995). It consists of eight areas of anintervention that may be culturally adapted. Language refers toculturally relevant oral and written forms of communication (e.g.,translation, specific jargon). The persons dimension captures theclient-therapist dyad dynamics (e.g., ethnic match). Metaphorsinclude expressing ideas in culturally relevant visual and verbalforms (e.g., role models, sayings). Content refers to attending tothe client’s values, traditions, and interpersonal styles (e.g.,familismo, simpatia). The concepts about the treatment, the treat-ment goals, and the treatment methods also need to be consistentwith the cultural values and expectations of the client. Finally, thecontext is taken into consideration in the assessment and interven-tion (e.g., acculturation, country of origin, family constitution,etc.). At least three studies used the EVF (Nicolas, Arntz, Hirsch,& Schmiedigen, 2009; Rossello & Bernal, 1999; Rossello, Bernal,& Rivera-Medina, 2008) to adapt existing cognitive–behavioraland interpersonal treatments for depression for Haitian and PuertoRican adolescents.
Theoretically, this review examines the existing culturally sen-sitive treatments using a top-down, a bottom-up, or an integrativeapproach. In this case, top-down refers to cultural adaptations to anestablished treatment to make it sounds and look more compatibleto the population of interest (e.g., translate materials to the lan-guage of the client, train staff to be warmer in interpersonalinteractions). These types of adaptations may be similar to Resni-cow et al.’s (2002) “surface adaptations.” Alternatively, bottom-uprefers to “deep adaptations” that consider contextual factors influ-encing behavior (e.g., historical, political, and sociocultural con-texts) and often involve collaboration with the potential recipientsof the treatment in the form of focus groups or qualitative research.An integrative approach refers to the use of both top-down andbottom-up adaptations and may include the use of a specificcultural adaptation framework. Although Hwang (2006, 2009)proposed a framework titled Integrating Top-Down andBottom-Up Approach in Adapting Psychotherapy, the use of theterms “top-down” and “bottom-up” in this review does not include
435CULTURALLY SENSITIVE DEPRESSION TREATMENTS

all of the elements that Hwang listed. Additionally, this reviewutilizes Leong’s Cultural Accommodations Model (CAM; Leong& Lee, 2006) to discuss the findings and formulate future recom-mendations for research and practice.
The primary goal of this article is to review the body of litera-ture on culturally sensitive treatments for depression and answerseveral questions that are important for the understanding andevaluation of these treatments and relevant to addressing existingdisparities:
1) What makes a treatment for depression culturally sensi-tive?
2) What types of existing treatments for depression havebeen adapted and/or tested (e.g., theoretical background;individual/family/group) and what are the outcomes?
3) What types of clients are these treatments targeting (e.g.,age, SES, ethnicity/race)?
4) What possible recommendations for future research canbe made?
Literature Review Method
Peer-reviewed articles examining culturally sensitive depressiontreatments were identified using the PsycInfo database in Decem-ber 2012. Keywords and subject terms included depression, de-pressed, treatment, therapy, psychotherapy in conjunction withadaptation, culturally adapted, culturally sensitive, multicultural,culture, ethnicity, race, and ethnic minority. In addition, publishedmeta-analyses (Benish et al., 2011; Griner & Smith, 2006; Huey &Polo, 2008; Smith et al., 2011) and review articles (Horrell, 2008;Miranda et al., 2005) of psychosocial treatments with ethnic mi-norities or nonmainstream populations were reviewed and relevantstudies were drawn. The first author (ZK) conducted the literaturesearch and reviewed the search results. Articles included in thisreview 1) focused on culturally sensitive treatments for depression,2) mentioned at least one element in the treatment related to theclients’ culture, and 3) described the cultural adaptation or frame-work used in the treatment. Culturally sensitive prevention pro-grams for depression were excluded. We identified 16 studies ofculturally sensitive treatments for depression based on these inclu-sion/exclusion criteria presented in Table 1.
Results
Elements of Culturally Sensitive Treatments forDepression
Some of the studies adapted specific elements using a top-downapproach (e.g., Dai et al., 1999), whereas others used frameworksand/or bottom-up and integrative approaches to create new treat-ments (e.g., Nicolas et al., 2009; Stacciarini, 2008). Frequenttop-down adaptations included hiring bilingual and bicultural pro-viders, offering all materials in the language of the group (e.g.,Spanish, Mandarin), and adapting the materials and exercises to beculturally appropriate. All studies that included Spanish-speakingpopulations emphasized the importance of cultural values, such as
respeto and simpatia, and instructed the staff to be warmer andmore personalized in their interactions with Spanish-speaking pa-tients (Kanter et al., 2010; Miranda, Azocar et al., 2003).
The Ecological Validity Model (Bernal et al., 1995) guided thecultural adaptations in a few of the culturally sensitive treatmentsfor depression reviewed in this paper (Nicolas et al., 2009; Ros-sello & Bernal, 1999; Rossello et al., 2008). Thus, these treatmentsincluded systematic adaptations in the eight broad areas listed inBernal et al. (1995). The structure/process and content adaptationsthat Kohn et al. (2002) described resembled the terminology fromKoss-Chioino and Vargas’ (1992) framework.
Some of the bottom-up approaches included generating focusgroups with stakeholders (Stacciarini, 2008), interviews with pro-viders who work with the population of interest (Naeem et al.,2011), and development of partnerships with the community (Ni-colas et al., 2009). Often the qualitative data generated from thesebottom-up approaches would be later integrated with preexistingelements of the treatment (e.g., treatment modules). However,some researchers could choose to reinvent the entire treatment bycreating new treatment modules based on the collected qualitativeinformation.
Whereas some studies provided rationale for the cultural adap-tations they made, others simply described them. For example,Nicolas et al. (2009) described elaborately every step of the cul-tural adaptation process and the reasoning behind it. Some of thesuggested changes that emerged from the focus groups (i.e.,bottom-up approach) included: integration of other theories be-sides CBT theory that explained the etiology of depression (i.e.,integrative approach); the inclusion of metaphors, language, andexamples that are relevant to the life of Haitian adolescents; and theunfamiliarity with some of the homework assignments and activ-ities, such as active listening. Based on the feedback, Nicolas andcolleagues proceeded to make a second wave of adaptations. Suchmultistage adaptations of treatments show the reasoning behindevery action and are important in creating an ecologically validintervention that integrates the community’s opinions. Nicolas etal. only provided a description of their detailed adaptation processbut did not have data available to show how the culturally adaptedtreatment was received by the target group.
Characteristics of Culturally SensitiveTreatments for Depression
Thirteen of the 16 culturally sensitive treatments for depressionreviewed in this article were cognitive–behavioral in nature. Twostudies provided case management (Miranda, Azocar et al., 2003;Yeung et al., 2010) and one (Ngo et al., 2009) tested a qualityimprovement intervention in a primary care setting. A couple ofstudies (Chavez-Korell et al., 2012; Kanter et al., 2010) usedbehavioral activation which is similar to the behavioral componentof CBT. Two studies adapted problem solving therapy (Chavez-Korrel et al.; Chu et al., 2012) for older adults, which is also basedon a CBT framework. Only two of the 16 studies (Rossello &Bernal, 1999; Rossello et al., 2008) tested individual and groupinterpersonal therapy (IPT). There were no differences between theindividual IPT and CBT outcomes, as it has been previously found(Elkin et al., 1989). However, the Group CBT yielded betterresults than the Group IPT (Rossello et al., 2008).
436 KALIBATSEVA AND LEONG

Tab
le1
Cul
tura
lly
Sens
itiv
eT
reat
men
tsfo
rD
epre
ssio
n
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Cha
vez-
Kor
ell
etal
.(2
012)
186
Lat
ino
elde
rs8–
12-s
essi
onin
divi
dual
PST
and
BA
1)M
akin
gth
etr
eatm
ent
feas
ible
for
aco
mm
unity
setti
ngto
impr
ove
Lat
ino
elde
rs’
acce
ss,
rete
ntio
n,an
dou
tcom
es;
2)A
dapt
ing/
tran
slat
ing
all
mat
eria
lsan
dco
nduc
ting
all
serv
ices
inSp
anis
h;3)
Ada
ptin
gm
ater
ials
for
popu
latio
nsw
ithlo
wor
nolit
erac
y;4)
Dec
reas
ing
the
ratio
ofpr
ovid
ers
and
clie
nts;
and
5)E
ngag
ing
incu
ltura
llyse
nsiti
vean
dap
prop
riat
etr
eatm
ent
activ
ities
.In
part
icul
ar,
Lat
ino
valu
esof
fam
ilis
mo,
pers
onal
ism
o,re
spet
o,di
gnid
ad,
espi
ritu
alid
ad,
mac
hism
o,an
dm
aria
nism
ow
ere
thou
ghtf
ully
used
intr
eatm
ent
conc
eptu
aliz
atio
n,pl
anni
ng,
and
inte
rven
tion;
Em
phas
ison
war
man
dpe
rson
alin
tera
ctio
ns
6(3
.3%
)18
0(9
6.7%
)N
/AO
utco
me
data
reve
aled
sign
ific
ant
decr
ease
inde
pres
sion
sym
ptom
sw
ith56
.15%
(73
of13
0)of
part
icip
ants
pres
entin
gw
ith50
%or
grea
ter
redu
ctio
nin
depr
essi
vesy
mpt
oms
in6
mon
ths
and
63.2
2%(5
5of
87)
ofpa
rtic
ipan
tspr
esen
ting
with
50%
orgr
eate
rre
duct
ion
in12
mon
ths.
Chu
etal
.(2
012)
1C
hine
seA
mer
ican
elde
rly
12-s
essi
onin
divi
dual
PST
Five
recu
rren
tth
emes
ofcu
ltura
lm
odif
icat
ions
wer
ede
velo
ped
from
stak
ehol
der
feed
back
,lit
erat
ure
revi
ew,
and
pilo
tte
stin
g:1)
Ane
edfo
rfl
exib
ility
;2)
Psyc
hoed
ucat
ion
and
de-
stig
mat
izin
gla
ngua
ge;
3)M
anag
ing
expe
ctat
ions
ofth
epr
ovid
er-c
lient
rela
tions
hip:
hier
arch
y,re
spec
t,ca
sem
anag
emen
t,an
dpr
ovid
ing
sugg
estio
ns;
4)V
isua
lai
dsan
dm
easu
rem
ent;
and
5)A
ccul
tura
tive
proc
esse
s
N/A
N/A
N/A
Rem
issi
onof
clin
ical
depr
essi
on(n
�1)
(tab
leco
ntin
ues)
437CULTURALLY SENSITIVE DEPRESSION TREATMENTS

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Dai
etal
.(1
999)
39(r
ando
miz
ed)
Chi
nese
Am
eric
anel
derl
y
8-se
ssio
ngr
oup
CB
T/
educ
atio
nal
(n�
30)
and
cont
rol
grou
p(n
�9)
Con
duct
edin
Chi
nese
bybi
lingu
alan
dbi
cultu
ral
ther
apis
ts
7(2
3%;
expe
rim
enta
lgr
oup)
;2
(22%
;co
ntro
lgr
oup)
23(7
7%)
N/A
Exp
erim
enta
lgr
oup
show
edim
prov
emen
tin
over
all
depr
essi
vesy
mpt
oms
over
time
com
pare
dto
the
cont
rol
grou
p.In
teri
anet
al.
(200
8)15
His
pani
cs,
93%
fem
ale
(low
-in
com
e,Sp
anis
hsp
eaki
ng)
12-s
essi
onin
divi
dual
CB
T
Prov
ided
inSp
anis
h;In
clud
edet
hnog
raph
ical
asse
ssm
ent
eval
uatin
gcu
ltura
lfa
ctor
sth
atm
ayco
ntri
bute
tode
pres
sion
;E
mph
asiz
edw
arm
and
posi
tive
inte
ract
ions
and
cultu
ral
valu
essu
chas
resp
eto,
sim
pati
a,an
dpo
nien
dode
supa
rte
(doi
ngev
eryt
hing
poss
ible
tohe
lpor
succ
eed)
;L
angu
age
cons
ider
atio
nsin
clud
edth
eus
eof
phra
ses
that
are
com
mon
lyus
edfo
rth
erap
eutic
phen
omen
a(d
esah
ogo,
getti
ngth
ings
off
one’
sch
est,
and
dist
racc
ion,
dist
ract
ion)
and
dich
os(s
ayin
gs);
Spec
ial
atte
ntio
ngi
ven
tofa
mil
ism
o(e
.g.,
clie
nt’s
impr
ovem
ent
will
cont
ribu
teto
fam
ily’s
impr
ovem
ent
infa
mily
func
tioni
ng);
Prov
ided
inpr
imar
yca
re;
Paid
spec
ial
atte
ntio
nto
som
atic
com
plai
nts
and
how
toad
dres
sth
emw
ithth
erap
eutic
tech
niqu
es(e
.g.,
rela
xatio
n,sl
eep
hygi
ene)
4(2
7%)
11(7
3%)
d�
2.71
(pos
ttrea
tmen
t);
d�
2.53
(fol
low
-up)
Part
icip
ants
repo
rted
asi
gnif
ican
tre
duct
ion
inde
pres
sion
sym
ptom
s(5
7%)
atpo
sttr
eatm
ent
and
reta
ined
the
impr
ovem
ent
atth
e6-
mon
thfo
llow
-up
(54%
redu
ctio
nfr
omba
selin
e).
438 KALIBATSEVA AND LEONG

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Kan
ter
etal
.(2
010)
10L
atin
aw
omen
inth
eU
.S.
12-s
essi
onin
divi
dual
BA
Incl
usio
nof
free
,lo
w-c
ost,
and
cultu
rally
sens
itive
activ
atio
nta
rget
s(e
.g.,
wal
king
,at
tend
ing
com
mun
ityac
tiviti
es,
such
aslo
cal
fest
ival
san
dre
crea
tiona
lgr
oups
,go
ing
toch
urch
,bo
rrow
ing
fitn
ess
DV
Ds
from
the
libra
ry,
goin
gto
the
park
);In
corp
orat
ion
ofL
atin
o-sp
ecif
icva
lues
and
belie
fs(f
amil
ism
o,pe
rson
alis
mo,
mar
iani
smo,
and
mac
hism
o)an
dat
tent
ion
toth
eir
effe
cton
activ
atio
n;A
dditi
onof
spec
ific
stra
tegi
esto
addr
ess
trea
tmen
ten
gage
men
tan
dre
tent
ion
inth
efi
rst
sess
ion;
Invi
tatio
nto
incl
ude
fam
ilym
embe
rsin
the
trea
tmen
t;Fa
mily
,so
cial
,an
dco
mm
unity
reso
urce
sut
ilize
dto
the
exte
ntpo
ssib
le.
Tra
nsla
ted
mat
eria
ls;
Bili
ngua
lan
dbi
cultu
ral
staf
f
4(4
0%)
6(6
0%)
d�
1.67
for
com
plet
ers;
d�
1.07
for
inte
nt-t
o-tr
eat
60%
ofpa
rtic
ipan
tsac
hiev
edre
mis
sion
atth
een
dof
trea
tmen
t
(tab
leco
ntin
ues)
439CULTURALLY SENSITIVE DEPRESSION TREATMENTS

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Koh
net
al.
(200
2)10
Afr
ican
Am
eric
anlo
w-i
ncom
ew
omen
16-s
essi
ongr
oup
CB
TSt
ruct
ure/
proc
ess
adap
tatio
ns:
only
Afr
ican
Am
eric
anw
omen
;cl
osed
grou
pto
faci
litat
eco
hesi
on;
expe
rien
tial
med
itativ
eex
erci
ses
atth
ebe
ginn
ing
ofea
chse
ssio
nan
da
term
inat
ion
ritu
al;
chan
ges
inth
ela
ngua
ge.
Con
tent
adap
tatio
ns(f
our
mod
ules
):de
cons
truc
ting
the
“Bla
cksu
perw
oman
”m
yth;
expl
orin
gsp
iritu
ality
and
relig
iosi
ty;
rein
forc
ing
impo
rtan
ceof
fam
ily;
disc
ussi
ngA
fric
anA
mer
ican
fem
ale
iden
tity
and
empo
wer
men
t
2(2
0%)
8(8
0%)
N/A
Whe
nco
mpa
red
with
dem
ogra
phic
ally
mat
ched
wom
en,
the
decr
ease
ofde
pres
sive
sym
ptom
sin
the
cultu
rally
adap
ted
grou
pw
astw
ice
larg
erth
anth
atin
the
regu
lar
CB
Tgr
oup
(-12
.6vs
.-5
.9po
ints
onth
eB
DI)
.
Mir
anda
,A
zoca
r,et
al.
(200
3)19
9 (ran
dom
ized
)A
fric
anA
mer
ican
,L
atin
olo
win
com
ePC
Ps
12-s
essi
ongr
oup
CB
Tvs
CB
T�
case
man
agem
ent
Bili
ngua
lan
dbi
cultu
ral
prov
ider
s;M
ater
ials
inSp
anis
h,T
rain
ing
staf
fto
show
resp
eto
and
sim
pati
a;W
arm
erin
tera
ctio
ns;
Low
erre
adin
gle
vel;
Plea
sant
activ
ities
free
23(3
0%)
ofSp
anis
h-sp
eaki
ngpa
tient
s:16
(40%
)of
CB
Tal
one
and
6(1
7%)
ofC
BT
�D
CM
;44
(36%
)of
Eng
lish-
spea
king
patie
nts:
27(4
4%)
ofC
BT
alon
ean
d17
(28%
)of
CB
T�
DC
M
70%
ofSp
anis
h-sp
eaki
ngpa
tient
s;64
%of
Eng
lish-
spea
king
patie
nts
N/A
The
Span
ish-
and
Eng
lish-
spea
king
patie
nts
resp
onde
deq
ually
wel
lto
cogn
itive
-beh
avio
ral
ther
apy
alon
e.Fe
wer
depr
essi
vesy
mpt
oms
notic
edon
lyfo
rSp
anis
hsp
eaki
ngcl
ient
sin
CB
T�
case
man
agem
ent.
440 KALIBATSEVA AND LEONG

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Mir
anda
,C
hung
,et
al.
(200
3)26
7 (ran
dom
ized
)A
fric
anA
mer
ican
(n�
117)
,L
atin
o(n
�13
4)lo
win
com
ew
omen
8-se
ssio
nC
BT
Bili
ngua
lpr
ovid
ers;
Man
ual
and
mat
eria
lsin
Span
ish;
Span
ish-
spea
king
staf
f;Ps
ycho
ther
apis
tsan
dnu
rse
prac
titio
ners
expe
rien
ced
and
com
mitt
edto
wor
king
with
low
-inc
ome
min
oriti
es
N/A
48(5
3%)
rece
ived
4or
mor
eC
BT
sess
ions
N/A
The
psyc
hoth
erap
yin
terv
entio
nw
asno
tsu
peri
orto
com
mun
ityre
ferr
alin
decr
easi
ngde
pres
sive
sym
ptom
s(p
�.3
2)or
impr
ovin
gro
lefu
nctio
ning
(p�
.58)
,bu
tdi
dre
sult
inim
prov
edso
cial
func
tioni
ng(p
�.0
6).
Nae
emet
al.
(201
1)34
(ran
dom
ized
)Pa
kist
ani
adul
ts9-
sess
ion
indi
vidu
alC
BT
�an
tidep
ress
ant
(n�
17)
and
cont
rol
(n�
17)
Use
dqu
alita
tive
data
from
clin
ical
psyc
holo
gist
sab
out
thei
rex
peri
ence
prov
idin
gC
BT
tode
pres
sed
patie
nts
and
barr
iers
inth
erap
y;C
olle
cted
info
rmat
ion
abou
tsy
mpt
oms,
refe
rral
beha
vior
,at
trib
utio
nst
yles
,an
dac
cept
abili
tyof
ther
apy
from
9de
pres
sed
patie
nts;
Nex
t,co
nduc
ted
focu
sgr
oups
with
colle
gest
uden
tsus
ing
the
“nam
eth
etit
le”
tech
niqu
eto
obta
ineq
uiva
lent
idio
mat
icph
rase
sw
ithou
ttr
ansl
atin
gth
ete
rmin
olog
yin
Urd
ufi
rst;
The
rapi
sts
focu
sed
onph
ysic
alsy
mpt
oms;
Urd
ueq
uiva
lent
sof
CB
Tja
rgon
;A
ppro
pria
teho
mew
ork;
Atte
ndan
ceof
afa
mily
mem
ber;
Folk
stor
ies
and
exam
ples
ofth
elif
eof
Prop
het
Muh
amm
adan
dQ
uran
used
3(1
8%)
atte
nded
few
erth
an6
14(8
2%)
d�
.60
Ina
RC
T,
the
auth
ors
com
pare
da
9-se
ssio
nC
BT
�an
tidep
ress
ants
(n�
17)
and
antid
epre
ssan
ts�
usua
lca
re(n
�17
)an
dob
serv
edsi
gnif
ican
tim
prov
emen
tin
depr
essi
ve,
anxi
ety,
and
som
atic
sym
ptom
sam
ong
patie
nts
who
rece
ived
CB
T.
(tab
leco
ntin
ues)
441CULTURALLY SENSITIVE DEPRESSION TREATMENTS
Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
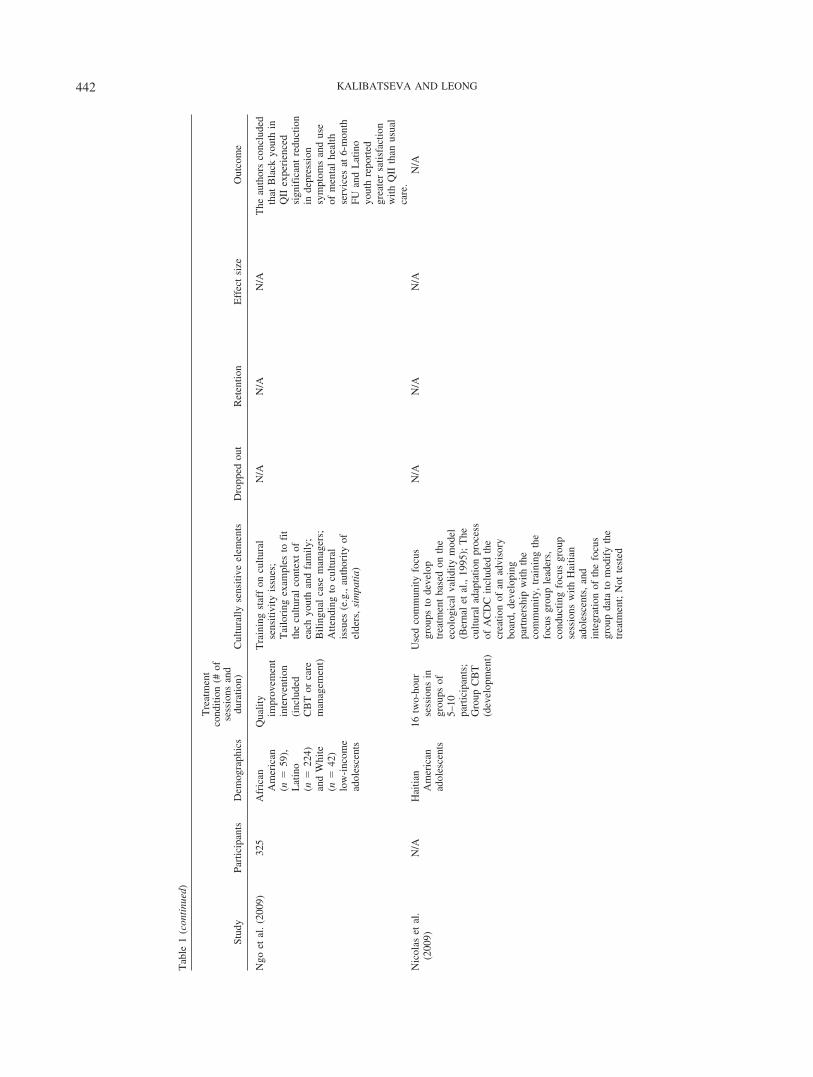
Ngo
etal
.(2
009)
325
Afr
ican
Am
eric
an(n
�59
),L
atin
o(n
�22
4)an
dW
hite
(n�
42)
low
-inc
ome
adol
esce
nts
Qua
lity
impr
ovem
ent
inte
rven
tion
(inc
lude
dC
BT
orca
rem
anag
emen
t)
Tra
inin
gst
aff
oncu
ltura
lse
nsiti
vity
issu
es;
Tai
lori
ngex
ampl
esto
fit
the
cultu
ral
cont
ext
ofea
chyo
uth
and
fam
ily;
Bili
ngua
lca
sem
anag
ers;
Atte
ndin
gto
cultu
ral
issu
es(e
.g.,
auth
ority
ofel
ders
,si
mpa
tia)
N/A
N/A
N/A
The
auth
ors
conc
lude
dth
atB
lack
yout
hin
QII
expe
rien
ced
sign
ific
ant
redu
ctio
nin
depr
essi
onsy
mpt
oms
and
use
ofm
enta
lhe
alth
serv
ices
at6-
mon
thFU
and
Lat
ino
yout
hre
port
edgr
eate
rsa
tisfa
ctio
nw
ithQ
IIth
anus
ual
care
.N
icol
aset
al.
(200
9)N
/AH
aitia
nA
mer
ican
adol
esce
nts
16tw
o-ho
urse
ssio
nsin
grou
psof
5–10
part
icip
ants
;G
roup
CB
T(d
evel
opm
ent)
Use
dco
mm
unity
focu
sgr
oups
tode
velo
ptr
eatm
ent
base
don
the
ecol
ogic
alva
lidity
mod
el(B
erna
let
al.,
1995
);T
hecu
ltura
lad
apta
tion
proc
ess
ofA
CD
Cin
clud
edth
ecr
eatio
nof
anad
viso
rybo
ard,
deve
lopi
ngpa
rtne
rshi
pw
ithth
eco
mm
unity
,tr
aini
ngth
efo
cus
grou
ple
ader
s,co
nduc
ting
focu
sgr
oup
sess
ions
with
Hai
tian
adol
esce
nts,
and
inte
grat
ion
ofth
efo
cus
grou
pda
tato
mod
ify
the
trea
tmen
t;N
otte
sted
N/A
N/A
N/A
N/A
442 KALIBATSEVA AND LEONG

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Ros
sello
&B
erna
l(1
999)
71(r
ando
miz
ed)
Puer
toR
ican
adol
esce
nts,
54%
fem
ale
CB
T(n
�25
),IP
T(n
�23
)or
wai
tlist
(n�
23);
12on
e-ho
urin
divi
dual
sess
ions
(CB
T,
IPT
)
Bas
edon
ecol
ogic
alva
lidity
and
cultu
ral
sens
itivi
tym
odel
(Ber
nal
etal
.,19
95);
Tra
nsla
ted
inst
rum
ents
;A
dapt
edtr
eatm
ent
man
uals
tobo
thde
velo
pmen
tal
and
cultu
ral
sens
itive
crite
ria;
Inte
grat
edan
dem
phas
ized
idea
sim
port
ant
inPu
erto
Ric
ancu
lture
such
asfa
mil
ism
o,si
mpa
tia,
resp
eto,
pare
ntal
auth
ority
,pr
esen
ttim
eor
ient
atio
n,an
dso
cioe
cono
mic
cont
ext;
Too
kin
toco
nsid
erat
ion
cultu
ral
aspe
cts
ofth
etr
eatm
ents
that
cons
ider
the
“int
erpe
rson
al”
aspe
cts
ofth
eL
atin
ocu
lture
.
Con
trol
5(2
2%),
IPT
4(1
7%)
and
CB
T4
(16%
)
68%
ofIP
Tan
d52
%of
CB
Tpa
rtic
ipan
tsco
mpl
eted
trea
tmen
t
(d�
.73
for
IPT
and
d�
.43
for
CB
T)
Part
icip
ants
inth
eC
BT
(n�
25)
and
IPT
(n�
23)
grou
psh
owed
asi
gnif
ican
tde
crea
sein
depr
essi
vesy
mpt
oms
com
pare
dto
the
wai
tlist
grou
pw
ithm
oder
ate
effe
ctsi
zes
(d�
.73
for
IPT
and
d�
.43
for
CB
T). (tab
leco
ntin
ues)
443CULTURALLY SENSITIVE DEPRESSION TREATMENTS

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Ros
sello
etal
.(2
008)
112 (r
ando
miz
ed)
Puer
toR
ican
adol
esce
nts
inPu
erto
Ric
o
12-s
essi
onin
divi
dual
CB
T(n
�23
),gr
oup
CB
T(n
�29
),in
divi
dual
IPT
(n�
31),
orgr
oup
IPT
(n�
29)
Bas
edon
ecol
ogic
alva
lidity
and
cultu
ral
sens
itivi
tym
odel
(Ber
nal
etal
.,19
95);
Sam
eas
Ros
sello
&B
erna
l(1
999)
;A
dapt
edgr
oup
man
uals
usin
gth
ecu
ltura
lad
apta
tion
mod
el
1(4
.3%
;in
divi
dual
CB
T),
1(3
.4%
;gr
oup
CB
T),
3(9
.6%
;in
divi
dual
IPT
),an
d1
(3.4
%;
grou
pIP
T)
95.7
%(C
BT
indi
vidu
al);
96.6
%(C
BT
grou
p);
90.4
%(I
PTin
divi
dual
);96
.6%
(IPT
grou
p)
Indi
vidu
alvs
.G
roup
was
d�
.18,
indi
vidu
alth
erap
ybe
tter
by54
%th
angr
oup
ther
apy;
CB
Tvs
.IP
Td
�.4
3,pa
tient
sin
CB
T67
%be
tter
than
IPT
Bot
hIP
Tan
dC
BT
inth
eir
indi
vidu
alan
dgr
oup
form
atpe
rfor
med
wel
l.H
owev
er,
CB
T(c
ombi
ned
grou
pan
din
divi
dual
)re
sulte
din
sign
ific
antly
grea
ter
decr
ease
sin
depr
essi
vesy
mpt
oms,
chan
ges
inse
lf-c
once
pt,
and
redu
ctio
nin
inte
rnal
izin
gan
dex
tern
aliz
ing
beha
vior
sin
com
pari
son
toIP
T(c
ombi
ned
grou
pan
din
divi
dual
).St
acci
arin
i(2
008)
16Pu
erto
Ric
anw
omen
inth
eU
.S.
Com
mun
ity-
base
dgr
oup
inte
rven
tion
(dev
elop
men
t)
Focu
sgr
oups
yiel
ded
the
follo
win
gca
tego
ries
:fa
mily
and
com
mun
ityva
lues
,m
ainl
and/
non-
mai
nlan
dcu
ltura
lva
rian
ces,
com
mun
icat
ion
styl
e,re
ligio
n,ed
ucat
ion
and
occu
patio
nal
vari
ance
s,he
alth
belie
fs,
Puer
toR
ican
trad
ition
s,em
otio
ns,
and
copi
ngsk
ills.
N/A
N/A
N/A
N/A
444 KALIBATSEVA AND LEONG

Tab
le1
(con
tinu
ed)
Stud
yPa
rtic
ipan
tsD
emog
raph
ics
Tre
atm
ent
cond
ition
(#of
sess
ions
and
dura
tion)
Cul
tura
llyse
nsiti
veel
emen
tsD
ropp
edou
tR
eten
tion
Eff
ect
size
Out
com
e
Won
g(2
008)
96(r
ando
miz
ed)
Chi
nese
adul
tsin
Hon
gK
ong,
22%
mal
e
10-w
eek
grou
pC
BT
vs.
wai
tlist
cont
rol
Tra
nsla
tion
ofal
lte
rmin
olog
yto
collo
quia
lex
pres
sion
s,m
odif
icat
ion
ofdy
sfun
ctio
nal
rule
sin
rela
tion
tofa
mily
and
inte
rper
sona
lre
latio
nshi
ps,
activ
ein
volv
emen
tof
grou
ple
ader
s,an
dth
ede
liver
yof
min
i-le
ctur
esab
out
the
exer
cise
san
dw
orks
heet
sto
incr
ease
stru
ctur
ean
dpr
oble
m-f
ocus
edap
proa
ch.
0(0
%;
expe
rim
enta
l),
8(2
0%;
cont
rol)
100%
C-B
DI
d�
.76,
CO
PEd
�57
,D
AS
d�
.88,
and
nega
tive
emot
ions
d�
.59
betw
een
the
expe
rim
enta
lan
dco
ntro
lgr
oup
The
part
icip
ants
inth
eex
peri
men
tal
grou
psh
owed
asi
gnif
ican
tde
crea
sein
the
seve
rity
ofde
pres
sion
sym
ptom
s,ne
gativ
eem
otio
ns,
and
dysf
unct
iona
lbe
liefs
and
bette
rco
ping
skill
sin
com
pari
son
with
the
cont
rol
grou
p.
Yeu
nget
al.
(201
0)10
0 (ran
dom
ized
)C
hine
seA
mer
ican
adul
ts
Usu
alca
reor
care
man
agem
ent
(1in
-per
son
mee
ting,
7ca
llsov
er24
wee
ks)
CSC
Tin
volv
esa
cultu
rally
sens
itive
psyc
hiat
ric
inte
rvie
w,
whi
chco
nsis
tsof
ast
anda
rdps
ychi
atri
cin
terv
iew
and
acu
ltura
lco
mpo
nent
that
uses
Kle
inm
an’s
ques
tions
toex
plor
epa
tient
s’ill
ness
belie
fs;
Info
rmat
ion
abou
tde
pres
sion
intr
oduc
edin
way
sco
mpa
tible
with
patie
nts’
belie
fs
N/A
N/A
N/A
The
two
cond
ition
sdi
dno
tdi
ffer
sign
ific
antly
.Y
eung
etal
.co
nclu
ded
that
the
CSC
Tim
prov
edth
ere
cogn
ition
and
trea
tmen
ten
gage
men
tof
depr
esse
dC
hine
seA
mer
ican
s.
Not
e.A
CD
C�
Ado
lesc
ent
Cop
ing
with
Dep
ress
ion
Cou
rse;
BA
�be
havi
oral
activ
atio
n;C
BT
�co
gniti
vebe
havi
oral
ther
apy;
CSC
T�
cultu
rally
sens
itive
colla
bora
tive
trea
tmen
t;D
CM
�de
pres
sion
care
man
ager
;IP
T�
inte
rper
sona
lth
erap
y;M
DD
�m
ajor
depr
essi
vedi
sord
er;
PCP
�pr
imar
yca
repa
tient
s;PS
T�
prob
lem
-sol
ving
ther
apy;
QII
�qu
ality
impr
ovem
ent
inte
rven
tion.
445CULTURALLY SENSITIVE DEPRESSION TREATMENTS

Seven of the adapted treatments were offered in a group format.Only one of the studies (Kohn et al., 2002) indicated that the groupwas closed after the start of the group, although it appeared thatother group treatments worked similarly (Dai et al., 1999; Rosselloet al., 2008) but it was not clear if the closed group format wouldbe preserved in a nonresearch setting. Depending on the format ofthe treatment (individual or group), the duration varied between 8and 16 sessions (between 60 and 120 minutes per session). Over-all, dropout rates for CSTs were low (ranged from 0% to 40%),which resulted in relatively high retention rates (from 60% to100%) for the culturally sensitive treatment conditions.
The majority of the reviewed CSTs for depression revealedmedium to large effect sizes for pretreatment to posttreatment (d �2.71 post treatment in Interian et al., 2008; d � 1.67 for completersin Kanter et al., 2010). Two studies compared a CST condition toa control condition and also found evidence for medium effectsizes in favor of the CST (d � .73 for CBT and d � .43 for IPTvs. control in Rossello & Bernal, 1999; d � .76 for adapted CBTvs. control in Wong, 2008) Another study found that culturallyadapted CBT in combination with antidepressants yielded betterresults than antidepressants only (d � .60; Naeem et al., 2011).Finally, Rossello et al. compared group and individual CBT andgroup and individual IPT and discovered that individual treatmentsperformed slightly better than group treatments (d � .18) andculturally adapted CBT performed better than culturally adaptedIPT (d � .43).
Participant Characteristics
The participants in five of the reviewed studies were low-income individuals, and there was a wide range of age groups.Three studies (Kohn et al., 2002; Miranda, Chung et al., 2003;Stacciarini, 2008) focused on therapy for depressed women only.Even studies that did not plan on limiting the recruitment towomen enrolled predominantly female participants (93%; Interianet al., 2008; 100%; Kanter et al., 2010). Three of the reviewedstudies developed culturally sensitive treatments for older adultsand four concentrated on adolescents.
In terms of ethnicity and race, Hispanics and African Americanswere most studied; three studies assessed a culturally adapteddepression treatment for Asian Americans (Chu et al., 2012; Dai etal., 1999; Yeung et al., 2010), and we located no study thatexamined a CST for depression for Native Americans. Two inter-national studies examined culturally adapted depression treatmentsin Hong Kong and Pakistan. In addition, the treatments wereprovided in a number of settings varying from primary care (In-terian et al., 2008) to outpatient hospital clinics (Miranda, Azocaret al., 2003). Generally, the existing culturally sensitive treatmentswere diverse in serving different age groups and targeting popu-lations at risk for depression.
All of the reviewed studies that provided data found significantdecreases in depressive symptomatology posttreatment. However,none of the studies examining these culturally sensitive treatmentshas empirically assessed directly the specific role of the adapta-tions. Kohn et al. (2002) used a comparison group of demograph-ically matched participants to compare the reduction in depressivesymptoms among African American women in the culturallyadapted CBT and the traditional CBT and found that the decreaseof symptoms was doubled in the culturally adapted CBT group.
Chavez-Korell et al. (2012) reported that IMPACT had been usedin its unadapted form with Latino elders in the past and was foundas effective as it was for the overall population. Apart from thesestudies, there is little evidence to support that the cultural adapta-tions are the main mechanism responsible for the favorable out-comes. Nonetheless, all studies had relatively high retention (over60%) and high social and ecological validity.
Discussion
We identified 16 studies that met inclusion criteria for culturallysensitive treatments for depression. The studies widely varied inthe description and assessment of cultural adaptations. The major-ity of the reviewed CSTs were behavioral or cognitive–behavioralin nature. This finding may not be surprising since CBT is con-sidered an EBT for depression (Chambless et al., 1998). In addi-tion, Domenech Rodríguez and Bernal (2012) pointed out thatwithin a pragmatist paradigm, cultural adaptation models werepredominantly developed to work with behavioral and cognitive–behavioral interventions.
Several of the CSTs for depression were in a group formant.Group therapies may be advantageous because they are morecost-effective, provide care for more people, and encourage closerelationships and support among group members. However, thegroup format may be troublesome for people whose cultural valuesrelate to stigma of mental disorders and may be especially unpop-ular in small communities, where people may know each other.Alternatively, a few studies used culturally adapted treatments inan individual therapy format (Interian et al., 2008; Kanter et al.,2010; Rossello & Bernal, 1999). It may be easier to make culturaladaptations in the process of individual therapy given that mostculturally competent therapists are likely to do some adaptationsalready. However, if such adaptations in individual therapy weremade but not documented, it may be difficult to assess theireffectiveness.
At the same time, Muñoz and Mendelson (2005) suggested thatchanges in existing interventions for depression should inviteethnic minority involvement in development, include cultural val-ues particular to the ethnic group, incorporate spirituality andreligion if relevant, take into account the clients’ acculturationlevel, address race, prejudice, and discrimination, and offer strat-egies to empower the clients. The inclusion of community mem-bers in the process of adapting or developing a treatment is ofutmost importance if the researcher wants to attract and retainparticipants. However, only three of the reviewed studies hadinvited community members to assist them in the adaptation (Chuet al., 2012; Nicolas et al., 2009; Stacciarini, 2008).
A number of the CSTs for depression targeted ethnic minorityand low SES women. In general, low SES and being a female maybe considered two of the risk factors for depression (Piccinelli &Wilkinson, 2000; Simonds, 2001). Therefore, these demographiccharacteristics may be overrepresented within the ethnic minoritygroups that have received culturally sensitive treatments for de-pression.
Additionally, the studies that provided data about dropout andretention rates presented a positive outlook with retention ratesconsistently above 60% and typically much higher. These numberslook promising considering that more than 65% of clients termi-nate psychotherapy before the 10th session and most clients attend
446 KALIBATSEVA AND LEONG

fewer than 6 sessions (Barrett et al., 2008). Moreover, the studiesthat provided effect sizes also suggested that clients’ depressivesymptoms significantly improve from pre to post treatment andcompared to a control group.
Recommendations for Intervention
Our recommendations for intervention from this review can beframed within the Cultural Accommodation Model (CAM) ofpsychotherapy (Leong & Lee, 2006), which involves three steps:“(a) identifying the cultural gaps or cultural blind-spots in anexisting theory that restricts the cultural validity of the theory, (b)selecting current culturally specific concepts and models fromcross-cultural and ethnic minority psychology to fill in the culturalgaps and accommodate the theory to racial and ethnic minoritiesand culturally diverse populations, and (c) testing the culturallyaccommodated theory to determine if it has incremental validityabove and beyond the culturally unaccommodated theory” (Leong& Serafica, 2001; p. 185).
As a proposed model of cross-cultural psychotherapy, a keycomponent of the Cultural Accommodation Model is to examinethe cultural validity of our models of psychotherapy and to identifyculture-specific elements that would fill the gaps of existing mod-els and enrich their utility and effectiveness with culturally diverseclientele (Leong & Kalibatseva, 2011). Furthermore, the CAMrecognizes the importance of using the person-environment inter-action models rather than focusing only on the person and ignoringthe cultural context variables in the lives of these culturally diverseindividuals (Leong & Kalibatseva, 2011). As a result, culturallydiverse clients who experience psychotherapy as congruent withtheir culture may be more likely to stay in treatment and benefitfrom it.
How should we evaluate the cultural validity of our models andwhat culture-specific elements should be selected? Relying on theindividual preferences of psychotherapists (or researchers) cannotbe justified. Instead, Leong and Lee (2006) proposed that inapplying the CAM, the Evidence-Based Practice (EPB) approachcould be utilized to both evaluate our existing models and to selectculture-specific variables to research which can then be applied inclinical practice. This review followed the recommendations of theCAM to identify cultural adaptations that have been successful indepression treatments. Yet, it is important to acknowledge that it isdifficult to compare the cultural adaptations across studies andgeneralize what adaptations work best.
The studies of culturally sensitive treatment for depressionreviewed in this article therefore examine the research evidence toguide the cultural accommodation process in providing treatmentto culturally diverse depressed patients. This review has identifiedculture-specific elements in treatment that have proven to increasethe effectiveness of our interventions. In this review specific todepression, we found that accommodating for language is critical.The effectiveness of bilingual therapists was found across multiplestudies. It is therefore recommended that therapists carefully eval-uate the language ability and needs of their depressed patients bothbefore initiating and during the treatment process. Moreover, thecultural adaptations to most treatments indicated that simple trans-lation may not be enough to make a treatment culturally sensitive.Thus, this recommendation expands beyond translation of materi-als and incorporates verbal and visual forms of communication
(e.g., metaphors, role models) that make the treatment consistentwith the cultural context of the client.
Similar to Leong and Lee (2006), this review also found thatculture-specific values related to interpersonal relationships, fam-ily, and spirituality can play a significant role when providingtherapy to culturally diverse patients. Specifically, our reviewfound that treatments which carefully accommodated for thesedifferences in cultural specific values resulted in better outcomes.For example, culture-specific interpersonal values included res-peto, familismo, and simpatia among Latino patients and religionand spirituality among African American patients. In addition,adaptations that increase the interaction of clients with health careprofessionals, such as care management may also yield betterretention and treatment outcomes. Culturally appropriate assess-ment, exploration of the client’s illness beliefs, and de-stigmatization of depression as an illness also most likely posi-tively contribute to recruitment, retention, and positive treatmentoutcome (Interian et al., 2008). Although very few CSTs in thisreview directly discussed this issue, the concept of depression, thesymptoms that typically are most bothersome, and the stigmaassociated with depression may be grounded within a culturalcontext that needs to be carefully explored. To illustrate this,neurasthenia, a popular cultural syndrome, captures a construct,which may be similar to depression among Asians. Neurasthenia(literally “lack of nerve strength”) is characterized by mental orphysical fatigue, and two of seven symptoms: dizziness, pain in themuscles, tension headaches, inability to relax, irritability, sleepdisturbance, and dyspepsia. It still remains a popular diagnosis inChina, in particular, and scholars have argued that it is commonlyused because of its acceptance as a medical diagnosis that conveysdistress without the stigma of a psychiatric diagnosis (Schwartz,2002).
Finally, the treatment approaches that were used were mostlyproblem-focused and direct. This finding is consistent with argu-ments that culturally diverse individuals may struggle with open-ended and nondirective therapy (Leong, Lee, & Kalibatseva, inpress). Moreover, establishing a warm and trusting relationshipand discussing assumptions about hierarchy and engagement of theclient in therapy were important elements in most of the culturallysensitive treatments for depression. To summarize, health careproviders are strongly encouraged to consider the importance oflanguage beyond translation, the integration of culturally salientvalues, beliefs, and traditions, and the understanding of etiology,symptom presentation, and stigma associated with depressionwhen providing CSTs for depression.
Recommendations for Research
Culturally adapted treatments for depression appear effective insymptom reduction and ethnic minority clients may be more likelyto seek and stay in treatment if they consider the issues discussedin therapy relevant to their culture. An important next step in thisfield is to compare a culturally adapted depression treatment and adepression treatment in its original form in order to find out if andhow much the cultural adaptations contribute to the favorableoutcomes. Future research that examines cultural adaptations asspecific mechanisms for change would contribute to our under-standing of the active and important ingredients of therapy thatproduce beneficial outcomes (Kazdin, 2007).
447CULTURALLY SENSITIVE DEPRESSION TREATMENTS

Based on this review, there are two likely directions for thefuture of CSTs: researchers will continue to adapt existing treat-ments by changing the process and content based on theory andprevious research or they will rely more on using frameworks andcommunity focus groups that will inform them of what to includein the treatment. Both directions seem promising as long as theadaptations are made based on sound reasoning and evidence. Theutilization of focus groups to inform and guide the adaptationprocess may be particularly helpful when treating specific popu-lations that have not received much attention in previous research.No matter which direction researchers choose, it is important todocument every cultural adaptation and the logic behind it. Sim-ilarly, Cardemil (2010) argued that researchers need to investigatethe social validity/acceptability, the efficacy, and the mechanismsof action associated with the cultural adaptations as well aschanges in symptoms and levels of engagement among partici-pants.
Other recommendations focus on the types of demographicgroups that need to be targeted in the future. First, this review didnot find any prior culturally sensitive treatment for depression withNative Americans. Gone and Alcántara’s (2007) review of theliterature on effective mental health interventions for AmericanIndians and Alaska Natives indicated that there were two preven-tive studies of depression. Yet, the lack of research on depressiontreatments with Native Americans needs to be addressed. In addi-tion, there was a general lack of males recruited in most of thereviewed treatments. The lower number of males may be explainedby the higher likelihood of women to suffer from depression(Simonds, 2001). However, researchers have also found that menand, in particular, ethnic minority men may be less likely to seekhelp for depression due to existing stigma in the society andcompliance to masculinity norms (Vogel, Heimerdinger-Edwards,Hammer, & Hubbard, 2011).
Another recommendation for research on culturally sensitivetreatment would be to explore within-group differences. For ex-ample, the DSM–IV–TR and DSM-5 have identified cultural iden-tity as a central moderator when diagnosing and treating persons ofcolor. More research is needed to delineate how these culturallysensitive treatments may need to be modified for clients withvarious levels of cultural identity. For example, cultural adapta-tions of CBT for Mexican Americans should not assume thatMexican Americans are a monolithic group. Instead, acculturationmay mediate the effect of a CST, such that Mexican Americandepressed clients with high or low levels of acculturation mayreact differently to a cultural adapted model of CBT (Villalobos,2009).
Lastly, few of the cultural adaptations addressed the concept ofdepression and what it means to be depressed in one’s culture. Inother words, the core components of the treatments that treatsymptom reduction were mostly kept intact and many of theperipheral elements were adapted (e.g., Chu et al., 2012). Hence,most cultural adaptations seem to be focused on the perspective ofcross-cultural psychotherapy rather than cross-cultural psychopa-thology. Since culture may influence the etiology, symptom ex-pression, diagnosis, and treatment of depression (e.g., Kleinman &Good, 1985), it may be valuable to explore how one’s culturalbackground may impact the way one thinks about what depressionis and how to cure it. Therefore, an ethnographic assessment asproposed in one of the studies (Interian et al., 2008) may be an
important element to include in future culturally sensitive treat-ments for depression. Lastly, depression is a multidimensionalconstruct and it may help to incorporate this idea in culturaladaptations of depression treatments (Kalibatseva & Leong, 2011).Focusing on the interpersonal and cognitive aspects of depressionhas been very effective but there are also somatic, affective, andexistential aspects of depression that may be important to addressin culturally sensitive treatments.
Based on our critical review of the literature, we have offered aseries of recommendations that we hope will guide future researchon culturally sensitive treatments for depression. In addition tofilling the gaps identified in this set of recommendations, we alsoencourage a greater amount of attention to culturally sensitivemeasurement of depression in order to advance the field. As ourassessment of treatment outcome relies on culturally sensitiveassessment, the authors see these two areas as closely related.
References
Alegria, M., Chatterji, P., Wells, K., Cao, Z., Chen, C., Takeuchi, D., . . .Meng, X. L. (2008). Disparity in depression treatment among racial andethnic minority populations in the United States. Psychiatric Services,59, 1264–1272. doi:10.1176/appi.ps.59.11.1264
Atkinson, D. R., Bui, U., & Mori, S. (2001). Multiculturally sensitiveempirically supported treatments - An oxymoron? In J. G. Ponterotto,J. M. Casas, L. A. Suzuki, & C. M. Alexander (Eds.), Handbook ofmulticultural counseling (2nd ed., pp. 542–574). Thousand Oaks, CA:Sage.
Barrett, M. S., Chua, W-J., Crits-Christoph, P., Gibbons, M. B., Casiano,D., & Thompson, D. (2008). Early withdrawal from mental healthtreatment: Implications for psychotherapy practice. Psychotherapy: The-ory, Research, Practice, Training, 45, 247–267. doi:10.1037/0033-3204.45.2.247
Beals, J., Novins, D. K., Whitesell, N. R., Spicer, P., Mitchell, C. M.,Manson, S. M., . . . Manson, S. M. (2005). Prevalence of mentaldisorders and utilization of mental health services in two AmericanIndian reservation populations: Mental health disparities in a nationalcontext. The American Journal of Psychiatry, 162, 1723–1732. doi:10.1176/appi.ajp.162.9.1723
Benish, S. G., Quintana, S., & Wampold, B. E. (2011). Culturally adaptedpsychotherapy and the legitimacy of myth: A direct-comparison meta-analysis. Journal of Counseling Psychology, 58, 279–289. doi:10.1037/a0023626
Bernal, G., Bonilla, J., & Bellido, C. (1995). Ecological validity andcultural sensitivity for outcome research: Issues for the cultural adapta-tion and development of psychosocial treatments with Hispanics. Jour-nal of Abnormal Child Psychology, 23, 67– 82. doi:10.1007/BF01447045
Bernal, G., & Domenech Rodrígiez, M. M. (Eds.). (2012). Cultural adap-tations: Tools for evidence-based practice with diverse populations.Washington, DC: American Psychological Association. doi:10.1037/13752-000
Bernal, G., & Scharrón-del-Río, M. R. (2001). Are empirically supportedtreatments valid for ethnic minorities? Toward an alternative approachfor treatment research. Cultural Diversity & Ethnic Minority Psychol-ogy, 7, 328–342. doi:10.1037/1099-9809.7.4.328
Betancourt, H., & Lopez, S. (1993). The study of culture, ethnicity and racein American psychology. American Psychologist, 48, 629–637. doi:10.1037/0003-066X.48.6.629
Breslau, J., Gaxiola-Aguilar, S., Kendler, K. S., Su, M., Williams, D., &Kessler, R. C. (2006). Specifying race-ethnic differences in risk forpsychiatric disorder in a USA national sample. Psychological Medicine,36, 57–68.
448 KALIBATSEVA AND LEONG

Cardemil, E. V. (2008). Culturally sensitive treatments: Need for anorganizing framework. Culture & Psychology, 14, 357–367. doi:10.1177/1354067X08092638
Cardemil, E. V. (2010). Cultural adaptations to empirically supportedtreatments: A research agenda. The Scientific Review of Mental HealthPractice: Objective Investigations of Controversial and UnorthodoxClaims in Clinical Psychology, Psychiatry, and Social Work, 7, 8–21.
Chambless, D. L., Baker, M. J., Baucom, D. H., Beutler, L. E., Calhoun,K. S., Crits-Christoph, P., . . .Woody, S. R. (1998). Update on empiri-cally validated therapies, II. The Clinical Psychologist, 51, 3–16.
Chambless, D. L., & Hollon, S. D. (1998). Defining empirically supportedtherapies. Journal of Consulting and Clinical Psychology, 66, 7–18.doi:10.1037/0022-006X.66.1.7
Chavez-Korell, S., Rendón, A., Beer, J., Rodríguez, N., Garr, A. D., Pine,C. A., . . . Malcolm, E. (2012). Improving access and reducing barriersto depression treatment for Latino elders: Un Nuevo Amanecer (A NewDawn). Professional Psychology: Research and Practice, 43, 217–226.doi:10.1037/a0026695
Chu, J. P., Huynh, L., & Areán, P. (2012). Cultural adaptation of evidence-based practice utilizing an iterative stakeholder process and theoreticalframework: Problem solving therapy for Chinese older adults. Interna-tional Journal of Geriatric Psychiatry, 27, 97–106. doi:10.1002/gps.2698
Dai, Y., Zhang, S., Yamamoto, J., Ao, M., Belin, T. R., & Cheung, F.(1999). Cognitive behavioral therapy of minor depressive symptoms inelderly Chinese Americans: A pilot study. Community Mental HealthJournal, 35, 537–542. doi:10.1023/A:1018763302198
Domenech Rodríguez, M. M., & Bernal, G. (2012). Frameworks, models,and guidelines for cultural adaptation. In G. Bernal and M. M. Dome-nech Rodríguez (Eds.), Cultural adaptations: Tools for evidence-basedpractice with diverse populations (pp. 23–44). Washington, DC: Amer-ican Psychological Association. doi:10.1037/13752-002
Elkin, I., Shea, M. T., Watkins, J. T., Imber, S. D., Sotsky, S. M., Collins,J. F., . . . Parloff, M. B. (1989). National Institute of Mental Healthtreatment of depression collaborative research program: General effec-tiveness of treatments. Archives of General Psychiatry, 46, 971–982.doi:10.1001/archpsyc.1989.01810110013002
Gone, J. P. (2009). A community-based treatment for Native Americanhistorical trauma: Prospects for evidence-based practice. Journal ofConsulting and Clinical Psychology, 77, 751–762. doi:10.1037/a0015390
Gone, J. P., & Alcántara, C. (2007). Identifying effective mental healthinterventions for American Indians and Alaska Natives: A review of theliterature. Cultural Diversity & Ethnic Minority Psychology, 13, 356–363. doi:10.1037/1099-9809.13.4.356
Griner, D., & Smith, T. B. (2006). Culturally adapted mental healthintervention: A meta-analytic review. Psychotherapy: Theory, Research,Practice, Training, 43, 531–548. doi:10.1037/0033-3204.43.4.531
Hall, G. C. Nagayama. (2001). Psychotherapy research with ethnic minor-ities: Empirical, ethical, and conceptual issues. Journal of Consultingand Clinical Psychology, 69, 502–510. doi:10.1037/0022-006X.69.3.502
Hall, G. C. Nagayama, & Yee, A. H. (2013). Evidence-based practice. InF. Leong, G. Hall, L. Comas-Diaz, J. Trimble, & V. McLoyd (Eds.),APA handbook of multicultural psychology. Washington, DC: AmericanPsychological Association
Harman, J. S., Edlund, M. J., & Fortney, J. C. (2004). Disparities in theadequacy of depression treatment in the United States. PsychiatricServices, 55, 1379–1385. doi:10.1176/appi.ps.55.12.1379
Horrell, S. V. (2008). Effectiveness of cognitive-behavioral therapy withadult ethnic minority clients: A review. Professional Psychology: Re-search and Practice, 39, 160–168. doi:10.1037/0735-7028.39.2.160
Huey, S. J., & Polo, A. J. (2008). Evidence-based psychosocial treatmentsfor ethnic minority youth. Journal of Clinical Child and AdolescentPsychology, 37, 262–301. doi:10.1080/15374410701820174
Hwang, W. C. (2006). The Psychotherapy Adaptation and ModificationFramework: Application to Asian Americans. American Psychologist,61, 702–715. doi:10.1037/0003-066X.61.7.702
Hwang, W. C. (2009). The Formative Method for Adapting Psychotherapy(FMAP): A community-based development approach to culturallyadapting therapy. Professional Psychology: Research and Practice, 40,369–377. doi:10.1037/a0016240
Interian, A., Allen, L. A., Gara, M. A., & Escobar, J. I. (2008). A pilotstudy of culturally adapted cognitive behavioral therapy for Hispanicswith major depression. Cognitive and Behavioral Practice, 15, 67–75.doi:10.1016/j.cbpra.2006.12.002
Kalibatseva, Z., & Leong, F. T. L. (2011). Depression among AsianAmericans: Review and recommendations. Article ID 320902, Depres-sion Research and Treatment. doi:10.1155/2011/320902
Kanter, J. W., Santiago-Rivera, A. L., Rusch, L. C., Busch, A. M., & West,P. (2010). Initial outcomes of a culturally adapted behavioral activationfor Latinas diagnosed with depression at a community clinic. BehaviorModification, 34, 120–144. doi:10.1177/0145445509359682
Kazdin, A. E. (2007). Mediators and mechanisms of change in psycho-therapy research. Annual Review of Clinical Psychology, 3, 1–27. doi:10.1146/annurev.clinpsy.3.022806.091432
Kazdin, A. E. (2008). Evidence-based treatment and practice. AmericanPsychologist, 63, 146–159. doi:10.1037/0003-066X.63.3.146
Kleinman, A., & Good, B. (1985). Culture and depression. Berkeley, CA:University of California Press.
Kohn, L. P., Oden, T., Muñoz, R. F., Robinson, A., & Leavitt, D. (2002).Adapted cognitive behavioral group therapy for depressed low-incomeAfrican American women. Community Mental Health Journal, 38, 497–504. doi:10.1023/A:1020884202677
Koss-Chioino, J. D., & Vargas, L. A. (1992). Through the culture lookingglass: A model for understanding culturally responsive psychotherapies.In A. Vargas & J. D. Koss-Chioino (Eds.), Working with culture:Psychotherapeutic intervention with ethnic minority children and ado-lescents. San Francisco: Jossey-Bass.
La Roche, M. J., & Christopher, M. S. (2008). Culture and empiricallysupported treatments: On the road to a collision? Culture & Psychology,14, 333–356. doi:10.1177/1354067X08092637
Leach, M. M., & Aten, J. D. (2010). Culture and the therapeutic process:A guide for the mental health professionals. New York, NY: Routledge.
Leong, F. T. L., & Kalibatseva, Z. (2011). Comparative effectivenessresearch on Asian American mental health: Review and recommenda-tions. Asian American and Pacific Islander Nexus, 8, 21–38.
Leong, F. T. L., Lee, J. D., & Kalibatseva, Z. (in press). Counseling AsianAmericans: Client and therapist variables. In P. B. Pedersen, J. G.Draguns, W. J. Lonner, J. E. Trimble, & M. Scharrón del Río (Eds.),Counseling across cultures (CAC7).
Leong, F. T. L., & Lee, S. H. (2006). A cultural accommodation model forcross-cultural psychotherapy: Illustrated with the case of Asian Ameri-cans. Psychotherapy: Theory, Research, Practice, Training, 43, 410–423. doi:10.1037/0033-3204.43.4.410
Leong, F. T. L., & Serafica, F. (2001). Cross-cultural perspectives onSuper’s career development theory: Career maturity and cultural accom-modation. In F. T. L. Leong & A. Barak’s (Eds.), Contemporary modelsin vocational psychology: A volume in honor of Samuel H. Osipow (pp.167–205). Mahwah, NJ: Erlbaum.
López, S. R., & Guarnaccia, P. J. J. (2000). Cultural psychopathology:Uncovering the social world of mental illness. Annual Review of Psy-chology, 51, 571–598. doi:10.1146/annurev.psych.51.1.571
Miranda, J., Azocar, F., Ogranista, K. C., Dwyer, E., & Areane, P. (2003).Treatment of depression among impoverished primary care patients
449CULTURALLY SENSITIVE DEPRESSION TREATMENTS

from ethnic minority groups. Psychiatric Services, 54, 219–225. doi:10.1176/appi.ps.54.2.219
Miranda, J., Bernal, G., Lau, A., Kohn, L., Hwang, W.-C., & LaFromboise,T. (2005). State of the science on psychosocial interventions for ethnicminorities. Annual Review of Clinical Psychology, 1, 113–142. doi:10.1146/annurev.clinpsy.1.102803.143822
Miranda, J., Chung, J. Y., Green, B. L., Krupnick, J., Siddique, J., Revicki,D. A., & Belin, T. (2003). Treating depression in predominantly low-income young minority women: A randomized controlled trial. JAMA:Journal of the American Medical Association, 290, 57–65. doi:10.1001/jama.290.1.57
Muñoz, R. F., & Mendelson, T. (2005). Toward evidence-based interven-tions for diverse populations: The San Francisco General Hospital pre-vention and treatment manuals. Journal of Consulting and ClinicalPsychology, 73, 790–799. doi:10.1037/0022-006X.73.5.790
Naeem, F., Waheed, W., Gobbi, M., Ayub, M., & Kingdon, D. (2011).Preliminary evaluation of culturally sensitive CBT for depression inPakistan: Findings from Developing Culturally-Sensitive CBT Project(DCCP). Behavioural and Cognitive Psychotherapy, 39, 165–173. doi:10.1017/S1352465810000822
Ngo, V. K., Asarnow, J. R., Lange, J., Jaycox, L. H., Rea, M. M., Landon,C., . . . Miranda, J. (2009). Outcomes for youths from racial-ethnicminority groups in a quality improvement intervention for depressiontreatment. Psychiatric Services, 60, 1357–1364. doi:10.1176/appi.ps.60.10.1357
Nicolas, G., Arntz, D. L., Hirsch, B., & Schmiedigen, A. (2009). Culturaladaptation of a group treatment for Haitian American adolescents. Pro-fessional Psychology: Research and Practice, 40, 378 –384. doi:10.1037/a0016307
Norcross, J. C., & Wampold, B. E. (2011). What works for whom:Tailoring psychotherapy to the person. Journal of Clinical Psychology,67, 127–132. doi:10.1002/jclp.20764
Piccinelli, M., & Wilkinson, G. (2000). Gender differences in depression.The British Journal of Psychiatry, 177, 486–492. doi:10.1192/bjp.177.6.486
Resnicow, K., Soler, R., Braithwaite, R. L., Ahluwalia, J. S., & Butler, J.(2000). Cultural sensitivity in substance use prevention: Bridging thegap between research and practice in community0based substance abuseprevention. Journal of Community Psychology, 28, 271–290. doi:10.1002/(SICI)1520-6629(200005)28:3�271::AID-JCOP4�3.0.CO;2-I
Rohner, R. P. (1984). Toward a conception of culture for cross-culturalpsychology. Journal of Cross-Cultural Psychology, 15, 111–138.
Rosselló, J., & Bernal, G. (1999). The efficacy of cognitive-behavioral andinterpersonal treatments for depression in Puerto Rican adolescents.Journal of Consulting and Clinical Psychology, 67, 734–745. doi:10.1037/0022-006X.67.5.734
Rosselló, J., & Bernal, G., & Rivera-Medina, C. (2008). Individual andgroup CBT and IPT for Puerto Rican adolescents with depressivesymptoms. Cultural Diversity & Ethnic Minority Psychology, 14, 234–245. doi:10.1037/1099-9809.14.3.234
Schwartz, P. Y. (2002). Why is neurasthenia important in Asian cultures?Western Journal of Medicine, 176, 257–258.
Simonds, S. L. (2001). Why are so many women depressed? In S. Simonds(Ed.), Depression and women: An integrative treatment approach (pp.19–48). New York, NY: Springer, Inc.
Smith, T. B., Domenech Rodríguez, M., & Bernal, G. (2011). Culture.Journal of Clinical Psychology, 67, 166–175. doi:10.1002/jclp.20757
Stacciarini, J.-M. R. (2008). Focus groups: Examining a community-basedgroup intervention for depressed Puerto Rican women. Issues in MentalHealth Nursing, 29, 679–700. doi:10.1080/01612840802128998
Takeuchi, D. T., Hong, S., Gile, K., & Alegria, M. (2007). Developmentalcontexts and mental disorders among Asian Americans. Research inHuman Development, 4, 49–69.
U.S. Department of Health and Human Services. (2001). Mental health:Culture, race, and ethnicity—A supplement to mental health: A report ofthe Surgeon General. Rockville, MD: U.S. Department of Health andHuman Services, Public Health Service, Office of the Surgeon General.
Villalobos, G. (2009). The mediating effects of acculturation on the effec-tiveness of culturally adapted cognitive behavioral therapy with Mexi-can Americans suffering from depression. Retrieved from ProQuest(2011–99070-429).
Vogel, D. L., Heimerdinger-Edwards, S. R., Hammer, J. H., & Hubbard, A.(2011). “Boys don’t cry”: Examination of the links between endorse-ment of masculine norms, self-stigma, and help-seeking attitudes formen from diverse background. Journal of Counseling Psychology, 58,368–382. doi:10.1037/a0023688
Whaley, A. L., & Davis, K. E. (2007). Cultural competence and evidence-based practice in mental health services: A complimentary perspective.American Psychologist, 62, 563–574.
Wong, D. F. K. (2008). Cognitive behavioral treatment groups for peoplewith chronic depression in Hong Kong: A randomized wait-list controldesign. Depression and Anxiety, 25, 142–148. doi:10.1002/da.20286
World Health Organization. (2008). The Global Burden of Disease 2004update. Retrieved from http://www.who.int/healthinfo/global_burden_disease/GBD_report_2004update_full.pdf
Yeung, A., Shuy, I. Fisher, L., Wu, S., Yang, H., & Fava, M. (2010).Culturally sensitive collaborative treatment for depressed ChineseAmericans in primary care. American Journal of Public Health, 100,2397–2402. doi:10.2105/AJPH.2009.184911
Received February 22, 2013Revision received December 18, 2013
Accepted January 8, 2014 �
450 KALIBATSEVA AND LEONG