a critical review of the antioxidant controversy/safety ... moskau 0609.pdf · a critical review of...
TRANSCRIPT
A critical review of the antioxidant controversy/safety issues for fat-
soluble vitamins
Hans K. Biesalski MD PhDDept. Biological
Chemistry
and Nutrition
University Stuttgart-Hohenheim
More than
hundred
studies
exist
describing beneficial
effects
of antioxidants
on
different diseases.
A few
large intervention
studies
could
not confirm
the
results. Some
of them
even
described
harmful
outcome
Nevertheless
„bad news
are
good news“ antioxidants
are
claimed
to be
not
even
unnecessary
but
harmfull!
Mortality
in randomized
trials
of antioxidant supplements
for
primary
and secondary
prevention: systematic
review and meta- analysis.
Bjelakovic
G, Nikolova
D, Gluud
LL, Simonetti
RG, Gluud
C.
CONCLUSIONS:
Treatment with beta carotene, vitamin A, and vitamin E may increase mortality.
Bjelkovic
et al., 2007:
No increase
of mortality
in all 68 RCT
Low risk
of bias: 5% in increase
of mortality
in 47 studies13 Studies
with
less
than
1000 participants: 1% risk
reduction
High risk
of bias: signifcant
decrease
of mortality
21 out of 68 mentioned
mortality
Mean
duration
of vitamin
intake: 2.7 years
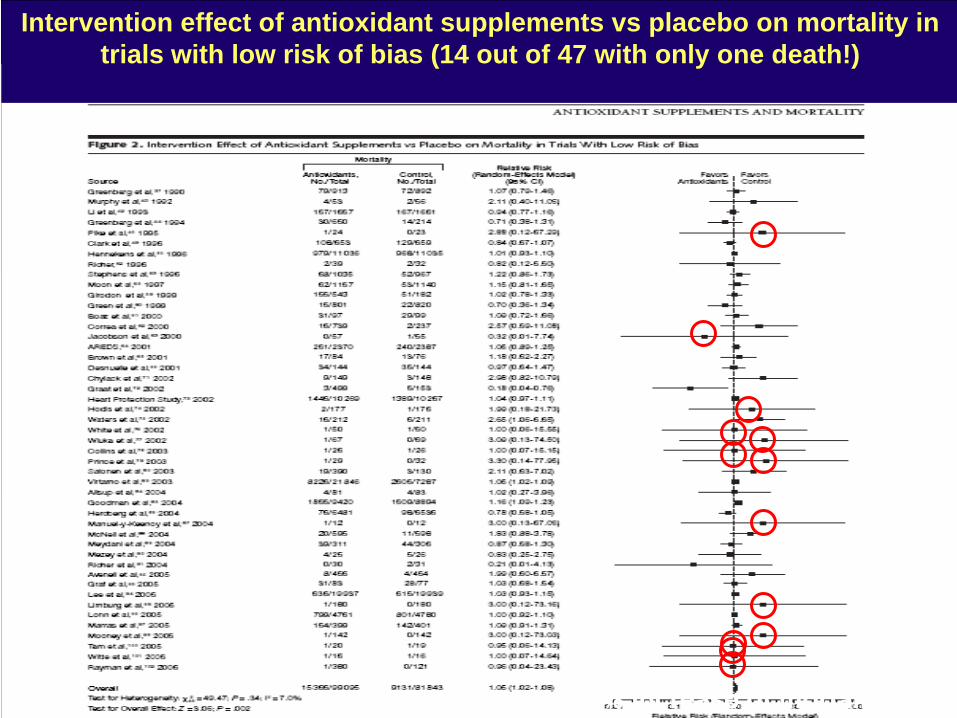
Intervention effect of antioxidant supplements vs placebo on mortality in trials with low risk of bias (14 out of 47 with only one death!)
5% increase
of mortality
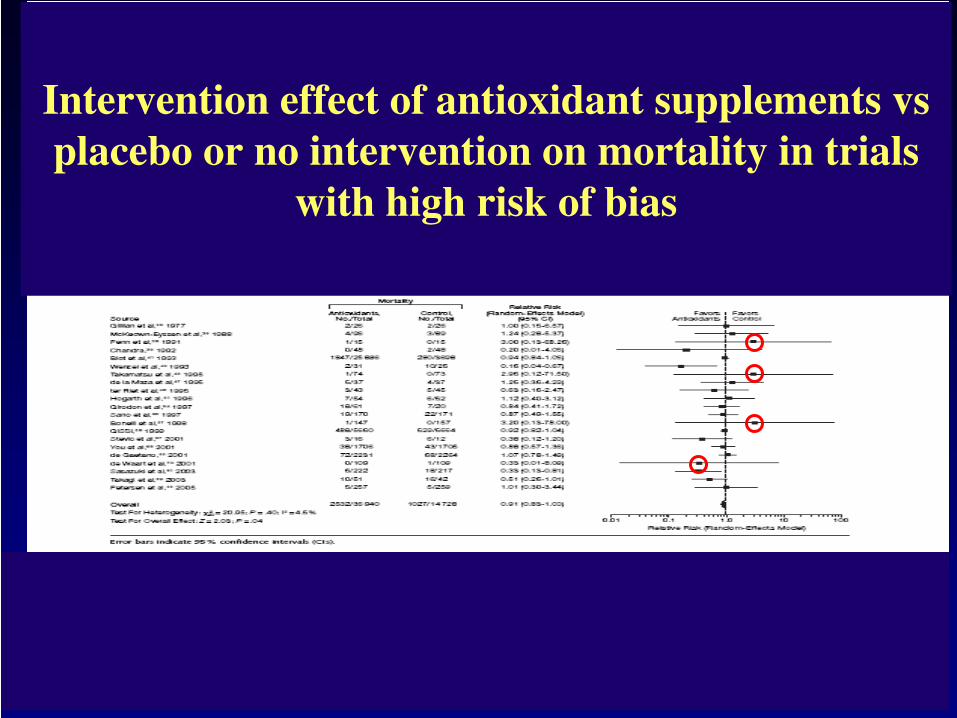
Intervention effect
of antioxidant
supplements
vs placebo
or
no intervention
on mortality
in trials
with
high risk
of bias

Evaluation of the 68 studies of Bjelakovic according to the study goal:
Total PP SP TT
Positive outcome 27 3 15 9
No effect 36 13 13 10
Negative outcome 5 1 3 1

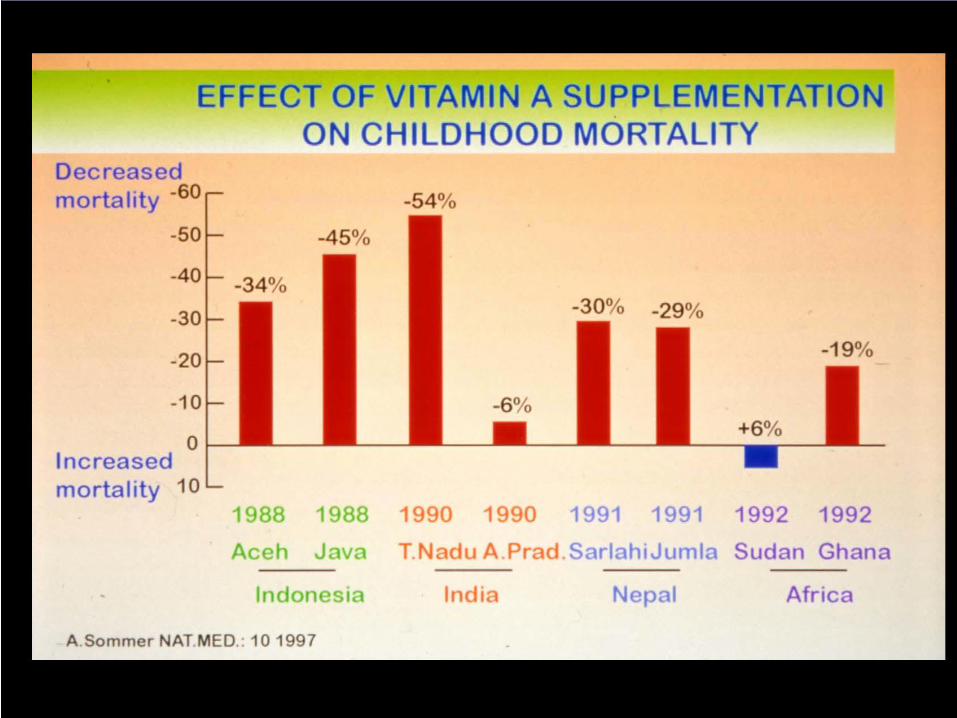
Vitamin deficiencies are not healthy!
Treatment of the deficiency might result in a decrease of mortality.
However, there is no evidence that vitamins can reduce mortality in the absence of a deficiency.
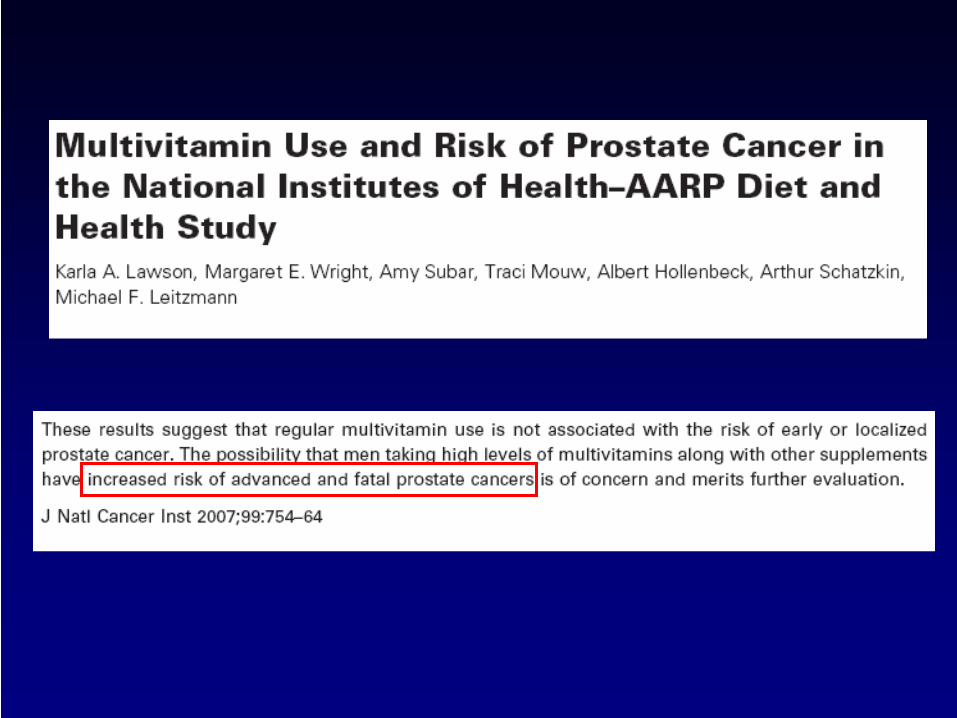
Method
of evaluation:Questionnaire
regarding
multivitamin
intake
in the
last twelve
month
in 10.241 men
with
prostate
cancer
Result: Those
who
supplied
multivitamins
(>7/week) plus selenium
were
primarily
affected.
(RR 5.8 for
fatal prostate
cancer
n=8) men
with
a genetic
history
in the
family
(RR 16.41 n=3)
Genetic
?

0.05
0.04
0.03
0.02
0.01
0
-0.01
-0.02
-0.03
10 20 50 100 200 500 1000 2000 IU Vitamin E
Vitamine EHarmful
Vitamin EBeneficial
All
case
mor
talit
yris
kdi
ffere
nce
Meta Analysis: High-Dosage Vitamin E Supplementation MayIncrease All-Cause Mortality. Ann Intern. Med 2004 Miller et al.
135 967 participants in 19 clinical trials. 9 tested vitamin E alone10 tested vitamin E combined with other vitamins and minerals
Non-linearlinear
The lack of a salutary effect was seen consistently for various doses of vitamins in diverse populations.
Our results combined with the lack of mechanistic data for efficacy of vitamin E, do not support the routine use of vitamine E.
D. Vivekananthan et al., Lancet Vol 348 June 14 2003
Use of antioxidant vitamins for the preventionof cardiovascular disease: meta analysis of
randomised trials.
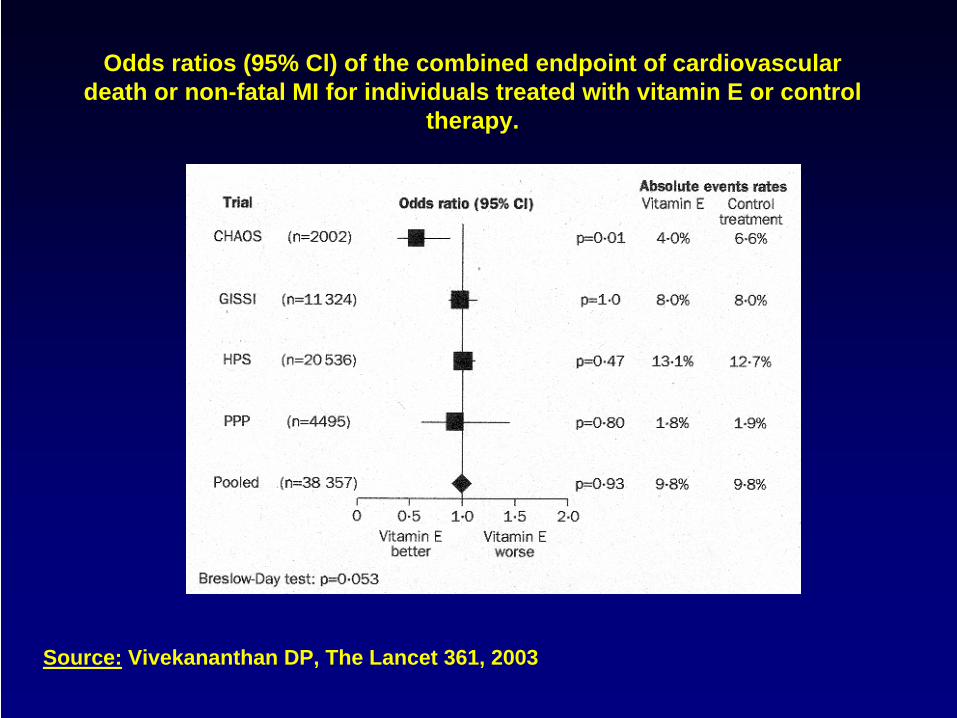
Odds ratios (95% Cl) of the combined endpoint of cardiovascular death or non-fatal MI for individuals treated with vitamin E or control
therapy.
Source: Vivekananthan DP, The Lancet 361, 2003
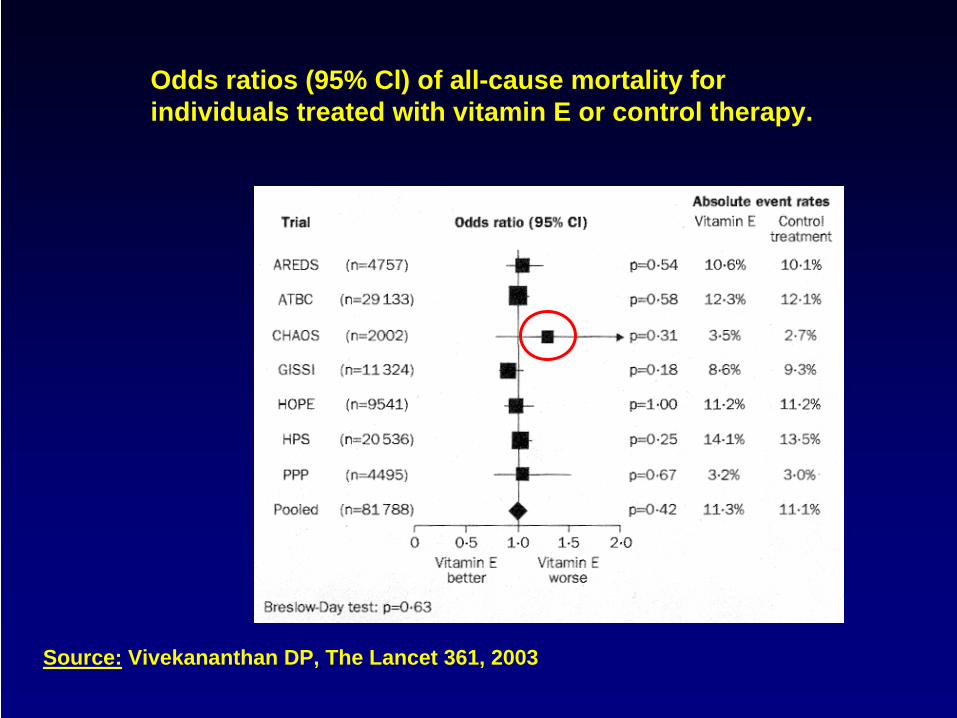
Odds ratios (95% Cl) of all-cause mortality for individuals treated with vitamin E or control therapy.
Source: Vivekananthan DP, The Lancet 361, 2003
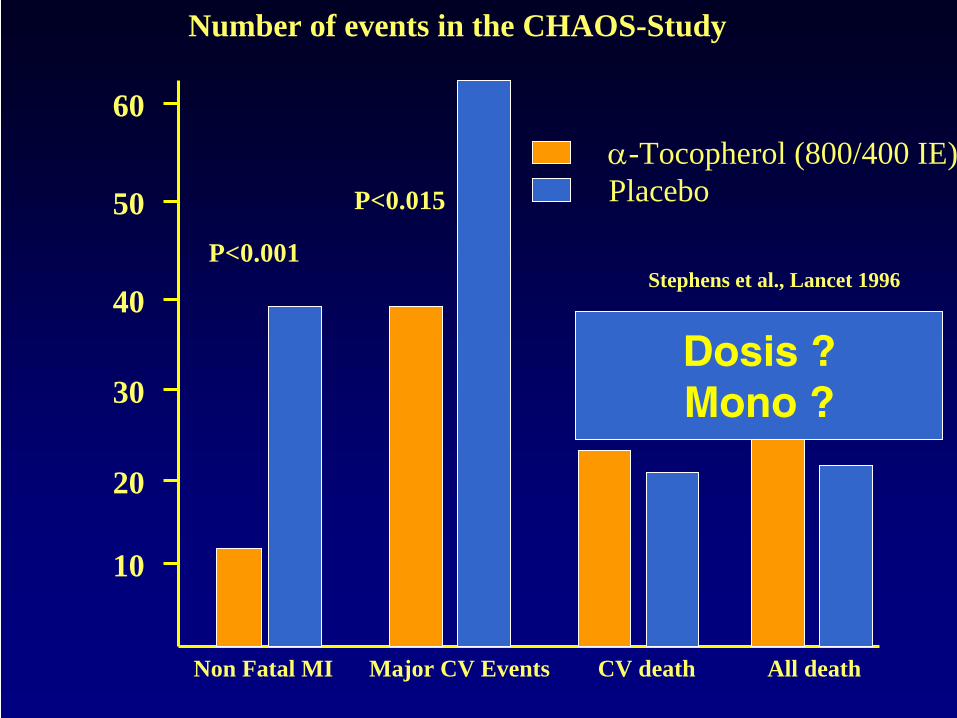
Number of events in the CHAOS-Study
α-Tocopherol (800/400 IE)Placebo
P<0.001
P<0.015
Stephens et al., Lancet 1996
Non Fatal MI Major CV Events CV death All death
60
50
40
30
20
10
Dosis ?Mono ?
Six year effect of combined vitamin C and E supplementation on atherosclerotic progression.
Salonen et al. Circulation 107: 2003
3 years supplementation with 136mg vitamin E and 250mg vitamin C twice daily slowed down progressionof carotid atherosclerosis in men but not in women.
Further slow down of progression in hypercholesteronemic persons.
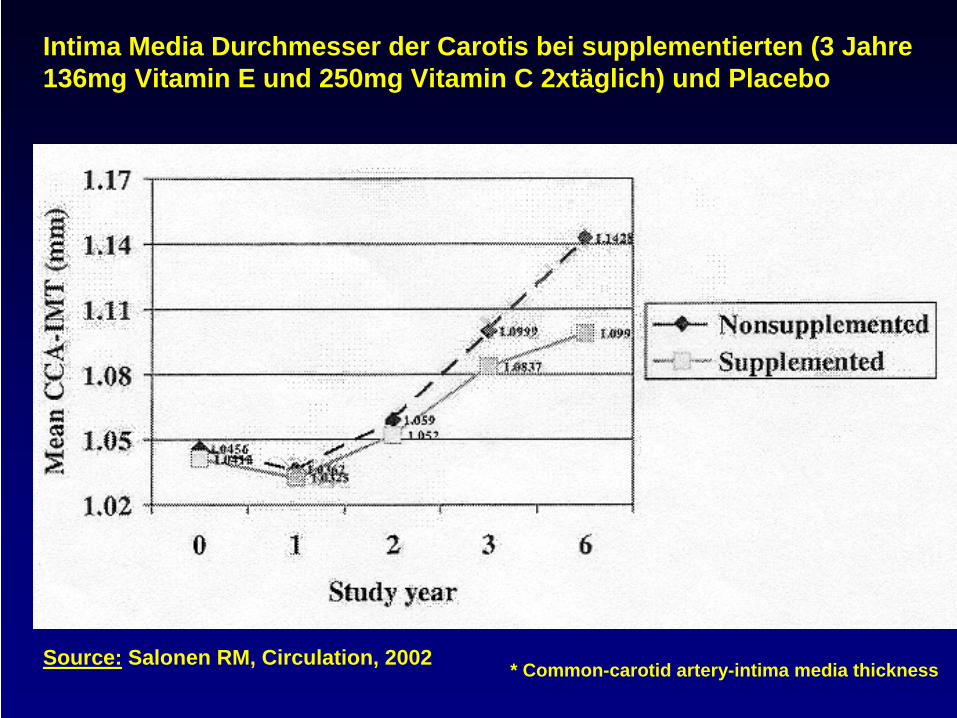
Intima Media Durchmesser der Carotis bei supplementierten (3 Jahre 136mg Vitamin E und 250mg Vitamin C 2xtäglich) und Placebo
Source: Salonen RM, Circulation, 2002 * Common-carotid artery-intima media thickness
What can vitamins (or essential micronutrients) in general really do?
In physiological doses they can act within their usual homoeostatic control and can compensate an inadequate intake and not more!
Consequence: If they work in physiological doses there must have been a deficiency or inadequate supply!
The major question is: what was the reason for the deficiency?

Up to 50% of patients
with
chronic
musculo-sceletal pain
have
an insufficient
Vitamin D supply
(NHANES III)
Supplementation
with
moderate doses
of vitamin
D completely
abolished
pain
Even vitamin
D acts
as a pain
killer
this
effect
is
based on the
compensation
of a vitamin
D-deficiency.
Special risk
groups: Elderly
and Immigrants
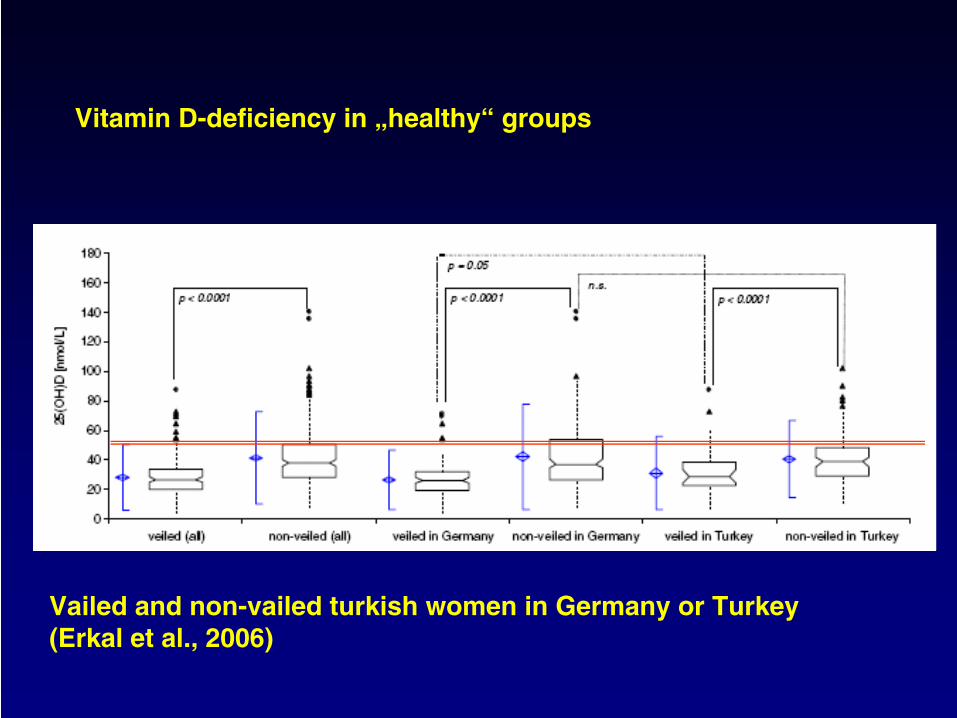
Vitamin D-deficiency
in „healthy“
groups
Vailed
and non-vailed
turkish
women
in Germany or
Turkey(Erkal
et al., 2006)
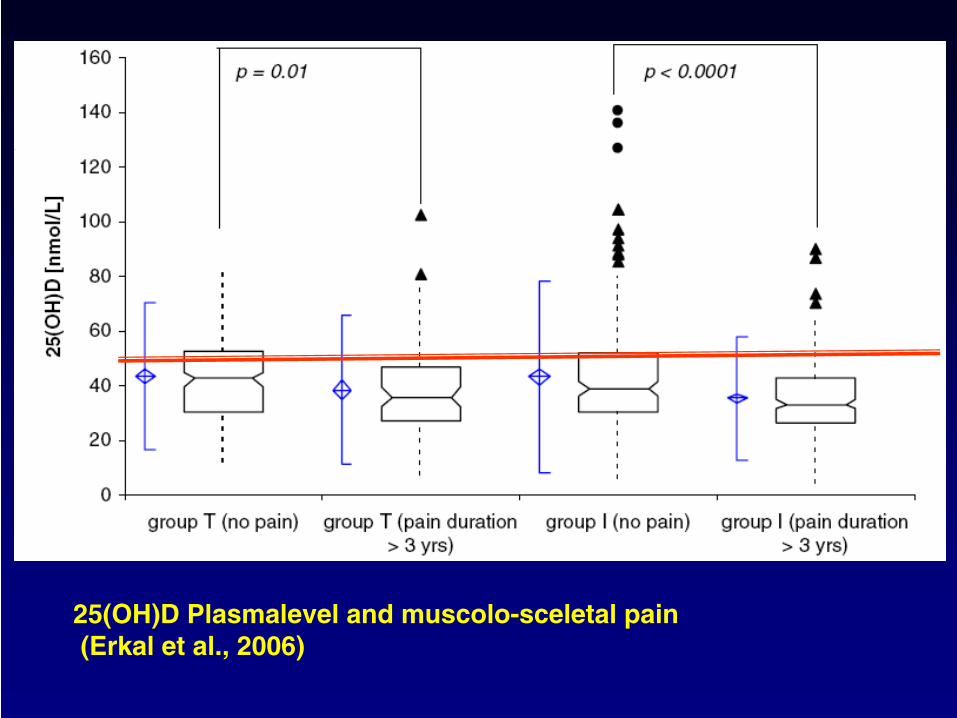
25(OH)D Plasmalevel
and muscolo-sceletal
pain(Erkal
et al., 2006)
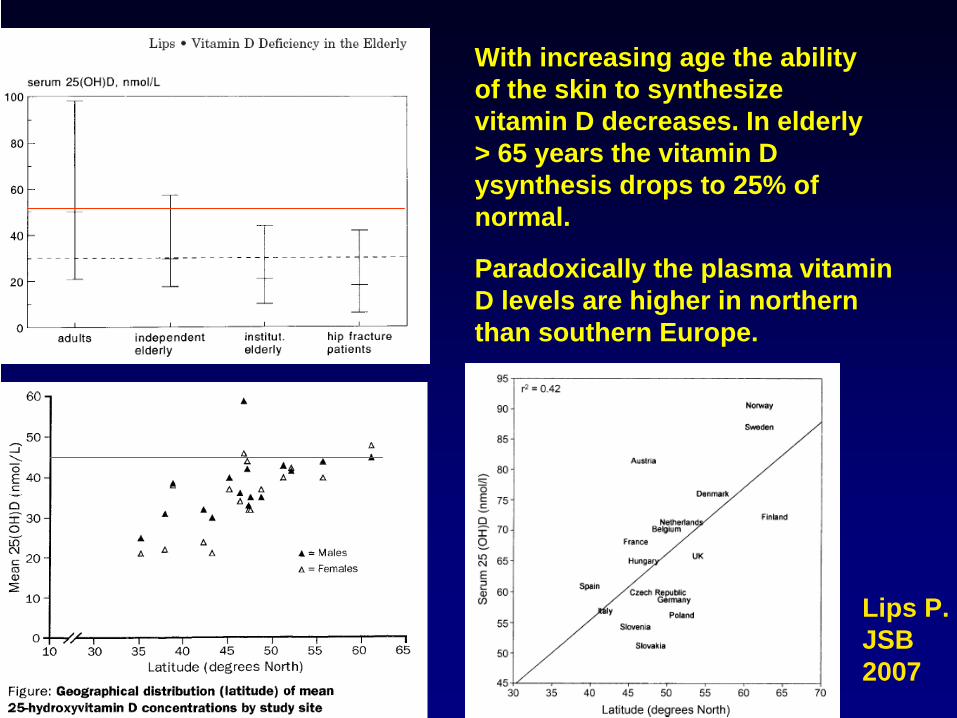
With increasing age the ability of the skin to synthesize vitamin D decreases. In elderly > 65 years the vitamin D ysynthesis drops to 25% of normal.
Paradoxically the plasma vitamin D levels are higher in northern than southern Europe.
Lips P.JSB2007

Low 25 hydroxyvitamin D and 1,25- dihydroxyvitamin D levels are independently associated with all cause (RR 2.08) and cardiovascular mortality (RR 2.22). (Dobnig et al., Arch Int Med. 2008)
Women who are vitamin D-deficient have a 253% increased risk for developing colorectal cancer, and women who ingested 1500mg Ca/da and 1100 IU/d vitamin D3 for 4yr reduced risk for developing cancer by 60% (Holick MF JANS 2008)
If there is a deficiency the compensation works!!
For a marginal or subclinical deficiency only a few marker – if at all – exist.
To measure effectiveness of antioxidants it is not enough to look at an „endpoint“
It is of importance to show that supplementaion with antioxidant has indeed an antioxidative effect!
If there is an antioxidative effect, there was a need!
If there is a deficiency the compensation works!!

Time course of reduction in plasma concentration of F2-isoprostanes in participants supplemented with 3200 IU/day Vitamin E
Plasma concentrations of vitamin E measured after 16 weeks of supplementation with variing doses of vitamin E or placebo
Roberts LJ et al., FRBM 43: 2007

Change in F2-isoprostane by quintile of baseline F2 Isopro
Vitamin C supplementation (1000mg/d 2 month) reduced F2Isopro 22% when F2 baseline levels were > 50µg/ml (Block G. FRBM 2008)
One participant died due to a car accident – if not mentioned antioxidants might have killed him!

Baseline F2 Isopro levels > 50µg/ml was strongly associated with BMI and was present in 42% of the sample (Block G et al., FRBM 2008)
The
activity
depends
on the
underlying oxidative
stress

Can Vitamins or antioxidants reduce mortality if supplied in higher doses?
28% risk reduction for mortality in trauma patients (2.272 vs control 2.022) exposed to high doses of antioxidants (Vit. C, E , Se) for 7 days (Collier et al., JPEN 32: 2008)
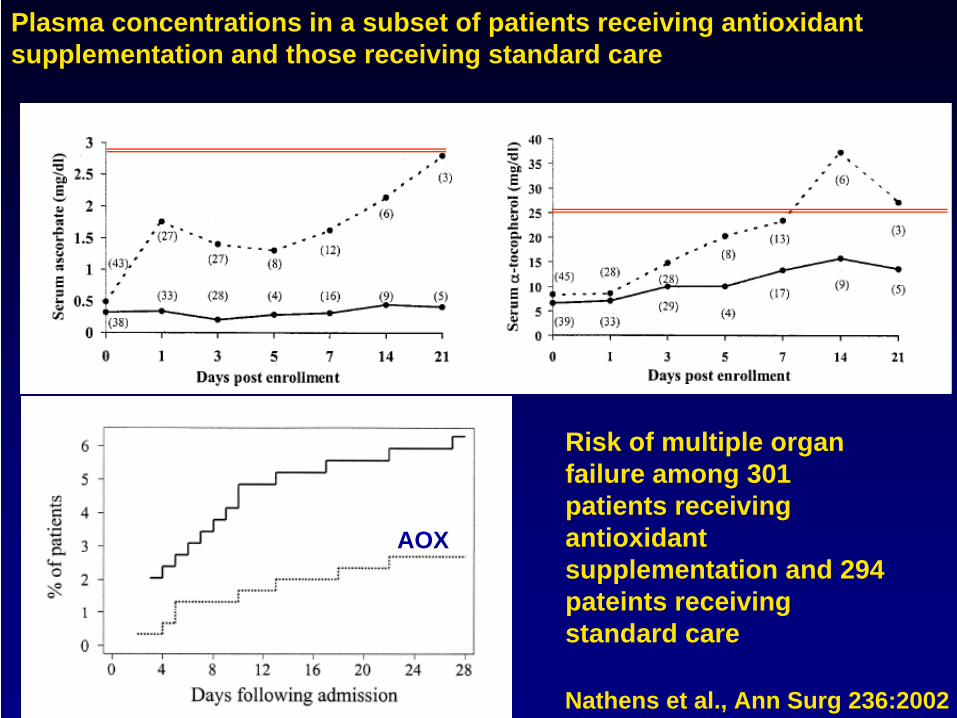
Plasma concentrations in a subset of patients receiving antioxidant supplementation and those receiving standard care
Nathens et al., Ann Surg 236:2002
Risk of multiple organ failure among 301 patients receiving antioxidant supplementation and 294 pateints receiving standard care
AOX

Is
there
a need
for
aditional
vitamins
or should
we
follow
the
general
paradigm:
There
is
enough
nutrition
for all, additional vitamins
are
not
needed!
100%
90
80
70
60
50
40
30
20
10
00VD FA VE Ca VA Mg Zn
B1 B2
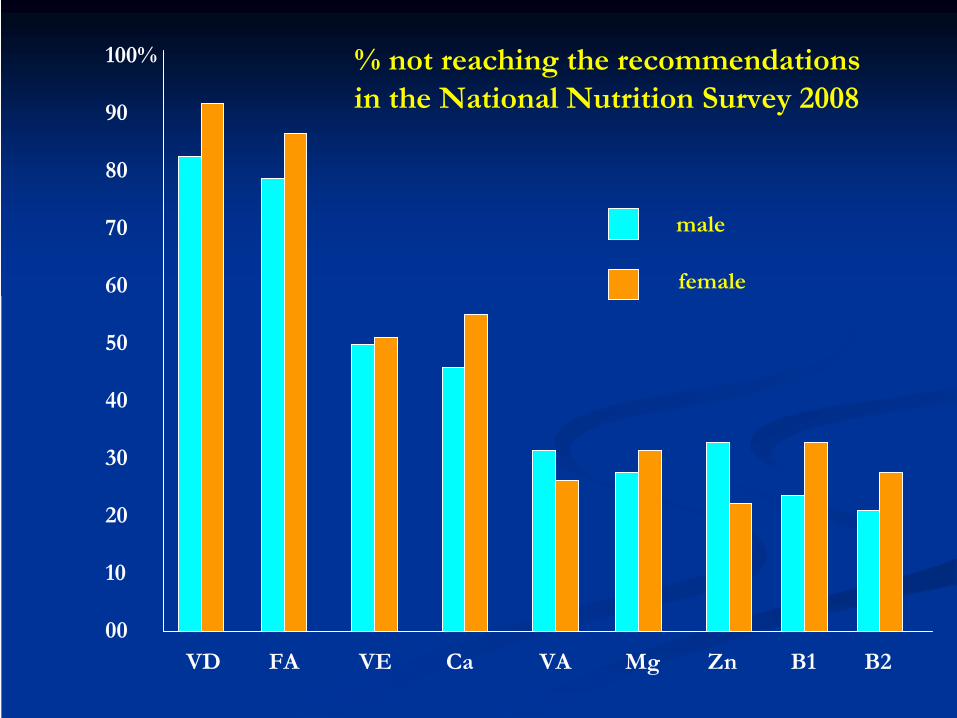
% not
reaching
the
recommendations in the
National Nutrition Survey
2008
male
female

Main dietary
sources
for
Vitamin E
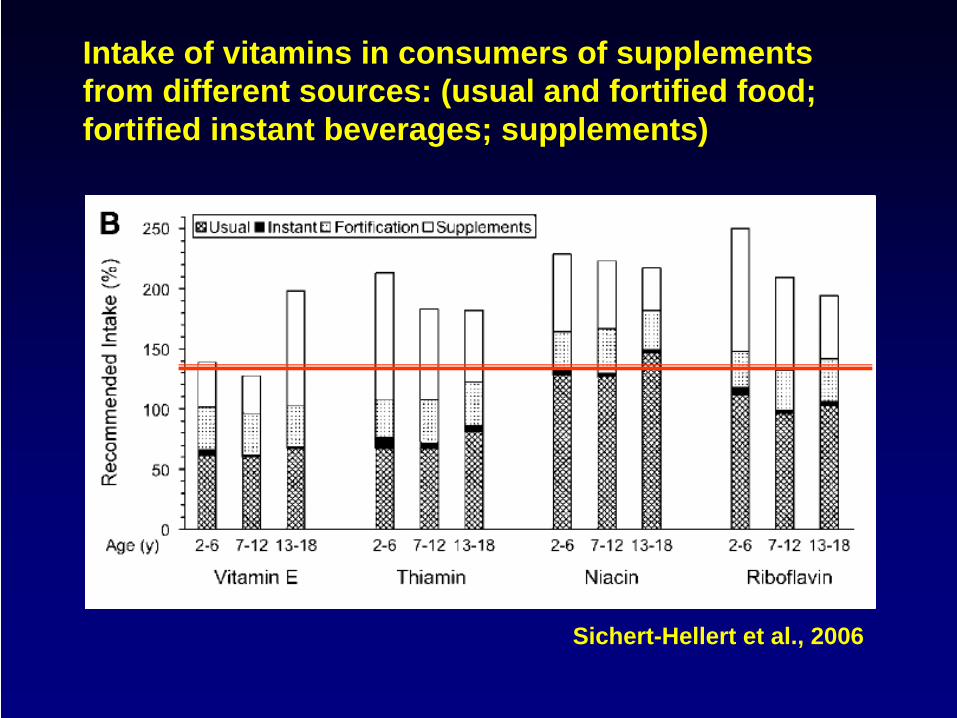
Intake of vitamins in consumers of supplements from different sources: (usual and fortified food; fortified instant beverages; supplements)
Sichert-Hellert et al., 2006
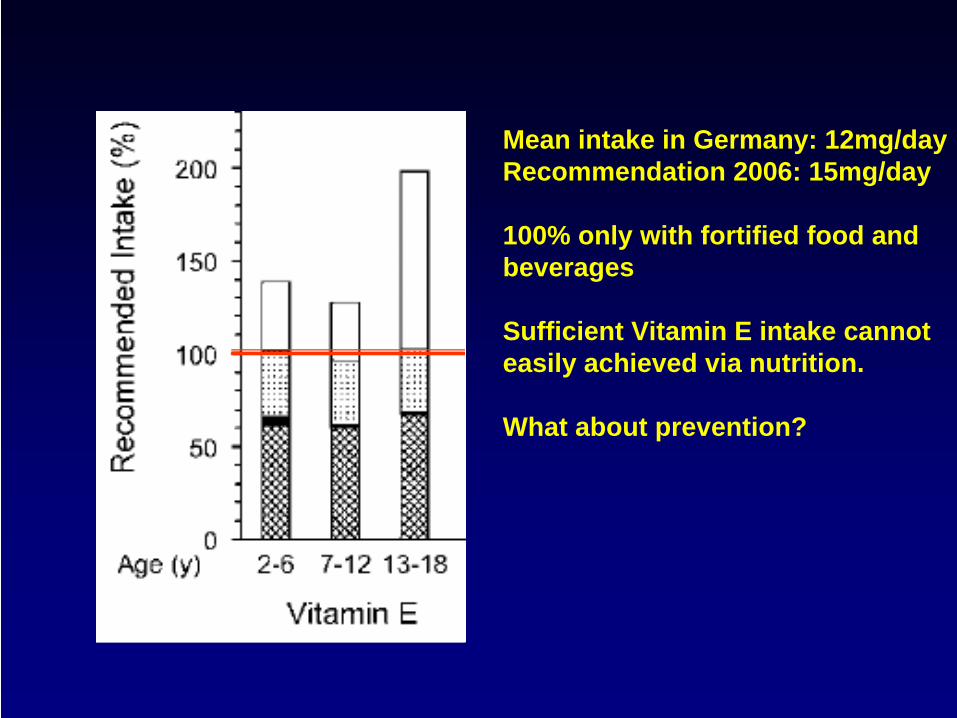
Mean intake in Germany: 12mg/dayRecommendation 2006: 15mg/day
100% only with fortified food andbeverages
Sufficient Vitamin E intake cannot easily achieved via nutrition.
What about prevention?
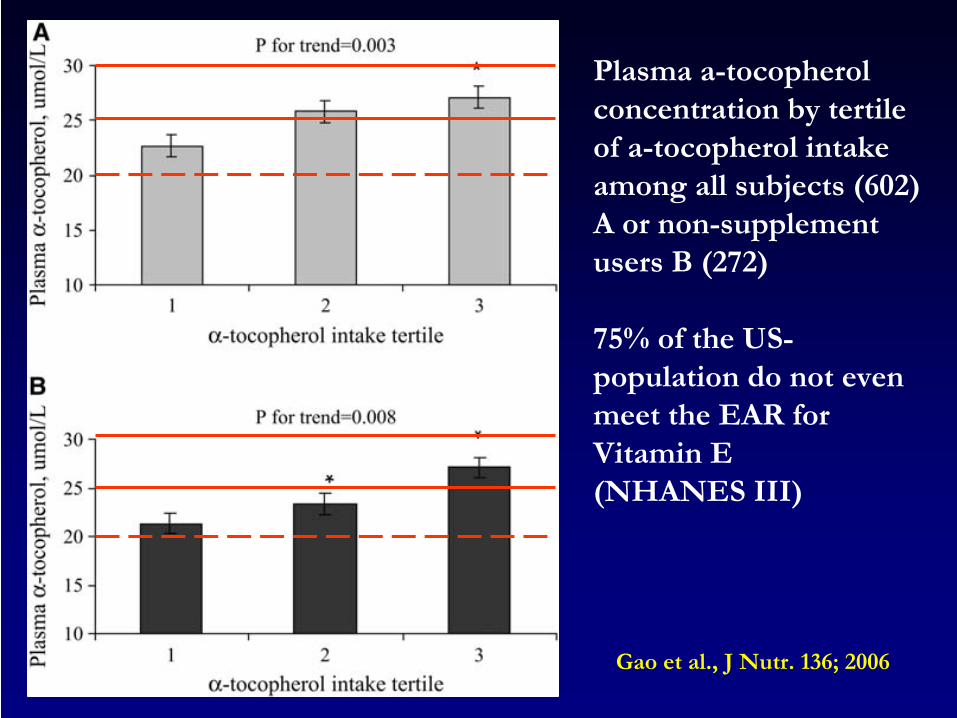
Plasma a-tocopherol concentration
by
tertile
of a-tocopherol
intake among
all subjects
(602)
A or
non-supplement users
B (272)
75% of the
US- population
do not
even
meet
the
EAR for Vitamin E
(NHANES III)
Gao
et al., J Nutr. 136; 2006
What can vitamins (or essentiel micronutrients) in general really do in secondary prevention?
Diseases and xenobiotics have different impacts on micronutrient requirement and turnover.
Consequently, the appropriate dosis to ensure the individual need in a disease state may vary.
Consequently, in secondary prevention the doses needed to compensate an inadequate supply may be higher than the doses needed for primary prevention
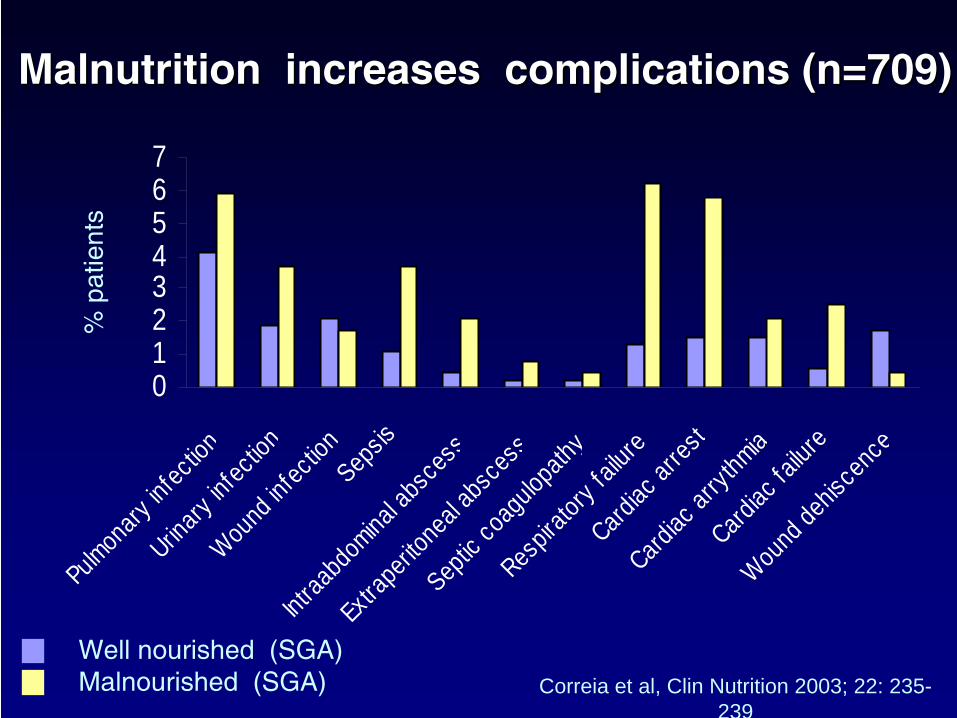
Malnutrition Malnutrition increasesincreases
complications (n=709)complications (n=709)
Correia et al, Clin Nutrition 2003; 22: 235- 239
01234567
Pulmon
ary inf
ection
Urinary
infec
tion
Wound
infec
tionSep
sis
Intraa
bdom
inal ab
sces
s
Extra
perito
neal a
bsce
ss
Septic
coag
ulopa
thy
Respir
atory
failur
eCard
iac ar
rest
Cardiac
arryt
hmia
Cardiac
failur
e
Wound
dehis
cenc
e
Well
nourished
(SGA)Malnourished
(SGA)
% p
atie
nts

100
80
60
40
20
10
00
33%
67%
89%
11%
AOX intake between66% to 100% of RDA
AOX intake below66% of RDA
Worsening in oxidative stress (Lipidperoxidation, protein-oxidation) accordingto intake of antioxidant vitamins prior ICU administration in critically ill.
Abiles et al. Crit Care 2006
Higher
ox.stress
Lower
ox.stress
Risk groups for poor antioxidant statusElderlyStrong vegetariansSmokerChronic alcohol intake (more than moderate)ObesityDieting (< 1.500 kcal)DiabetesCOPDChronic imflammatory diseasesCancerFat Malabsorption
Low intake
of antioxidants
may
have
an impact
in the
long term
(CHD, Cancer, Neurological
diseases)

What can vitamins (or essentiel micronutrients) in general really do in primary prevention?
A diet rich in all essentiel micronutrients protects from a couple of diseases in later life.
Consequently, in primary prevention micronutrients protect from deficiency in physiological doses.

What can vitamins (or essentiel micronutrients) in general really do?
In pharmacological doses they can act as micronutrients and in addition by circumventing the homoeostatic control may also act in a different way !
Consequence: If they work in pharmacological doses they may or should be treated like xenobiotics!

Conclusion
The
primary
goal
to supplement
antioxidants is
to ensure
an adequate
supply
adapted
to the
life cycle.
Normal intake
achievable
via nutrition
(RDA) may
be
enough
in a healthy
status. However,
diseases
may
result
in a higher
need.
Antioxidants
are
not
recommended
to increse life span
but
to improve
life quality
in chronic
diseases