a cross-sectional longitudinal survey into the durability of amalgam restorations
TRANSCRIPT

Journal of Dentistry, 4, 139-l 43
A cross-sectional longitudinal survey into the durability of amalgam restorations C. L. B. Lavelle, PhD, MDS
Department of Oral Biology, Faculty of Dentistry, University of Manitoba
ABSTRACT The durability of amalgam restorations was assessed from a cross-sectional survey based upon 6000 defective restorations and a longitudinal survey based on the amalgam restorations of 400 males and females spanning a 20-year period. The data showed that amalgam restorations are not as durable as traditionally assumed, with failure on the part of the dental surgeon being the pre- dominant defect.
INTRODUCTION OWING to its ease in manipulation, adequate mechanical properties and low cost, amalgam has long been established as the commonest material for dental restorations. However, from a study of 1521 defective amalgam restorations, 50 per cent were designated as arising from improper cavity preparation and 40 per cent due to faulty amalgam manipula- tion (Healey and Phillips, 1949). In another study of 887 amalgam restorations, two types of failure were noted (Allan, 1969). ‘True’ failures were defined as those arising from factors not under the control of the dental surgeon, and essentially resulted from the development of a carious lesion elsewhere in the tooth coupled with pulpal and periodontal lesions. In another study of 907 patients, 45 per cent of their amalgam restorations were considered defective (Moore and Steward, 1967). Similar findings were reported in a study of Canadians (Richardson and Boyd, 1973), although these workers noted that mechanical failure of the amalgam accounted for only 9 per cent of the total number of replacements, whilst 68 per cent of the restorations required
to be replaced owing to recurrent caries, secondary caries and caries beneath the restorations. Finally, scrutiny of the dental records over a period of 20 years showed that some amalgam restorations lasted for only a very short period of time, whereas 25 per cent lasted for more than 20 years (Robinson, 1971).
Despite their ubiquitous use, there are still scant data on the durability of amalgam restorations. The present study was therefore undertaken to examine longitudinal and cross- sectional data for the durability of amalgam restorations.
MATERIALS AND METHODS Cross-sectional survey This survey was based on the examination of equal samples of 3000 defective amalgam restorations in the permanent premolar and molar teeth from males and a similar number from females. Each sample had a similar age distribution (20-40 years), and all the patients were examined whilst attending for routine treatment.
As this was a cross-sectional survey, the history of the restoration, manipulative pro- cedure, technique employed and condition of insertion were unknown. The amalgam restora- tions were examined under standardized con- ditions by the same observer using a mirror, explorer and air syringe. Furthermore, in each instance intra-oral X-rays were examined to confirm that amalgam restorations had failed. A restoration was defined as failed when there was caries either around or under the restora- tion or when the condition of the restoration
140 Journal of Dentistry, Vol. ~/NO. 3
seriously interfered with the normal functional integrity of the tooth. This definition includes a gingival overhang or an incomplete margin, both of which are defects but may not yet be accompanied by recurrent caries. In this study four types of amalgam failure were denoted: (a) fracture; (b) dimensional change; (c) recurrent caries; (d) pulpal or periodontal involvement. Some restorations exhibited more than one type of failure, although for this study only the predominant defect was denoted.
In order to check on the accuracy of the technique of assessment, the amalgam restora- tions of 50 patients, selected at random, were examined by two other observers. In each instance both the detection and classification of amalgam failures were in accord.
Longitudinal survey This survey was based on the records of three dental practitioners who had qualified at the same time from the same dental school; the criteria for amalgam replacement were there- fore assumed to be similar for each patient.
The dental records of equal samples of 200 male and female patients were scrutinized. Each patient had attended at least annually for dental examination or treatment during a 20-year period, and on each occasion was examined by the same practitioner. A note was made of the amalgam restorations present in 1953 (the first year of this survey), and the records were subsequently examined for the ensuing 20 years for the restorations lost due to tooth extraction or replaced by a similar or more extensive restoration or crown. Generally, a restoration was considered to require replacement when fracture, recurrent caries, attrition, erosion or corrosion had caused it to cease functioning adequately.
Owing to some ambiguity of the practice records, the following criteria were adopted in this study:
1. When a tooth was extracted, all the restorations in that tooth were regarded as having failed.
2. When a new restoration of the same denomination was inserted, the original one was considered as having failed, with the
exception of the maxillary first and second molars and the mandibular first premolars where the occlusal morphology frequently pre- disposes to there being two separate occlusal restorations in the occlusal pits.
3. An occlusobuccal restoration was re- corded as indicating failure of a buccal or an occlusal restoration.
4. A mesio-occlusal or disto-occlusal restora- tion was considered as a failure of a mesial or distal restoration and a mesial or distal restoration as a failure of a mesio-occlusal or disto-occlusal restoration.
5. A mesio-occlusal or disto-occlusal restora- tion was regarded as a failure of an occlusal restoration.
6. An occlusal restoration was not regarded as indicative of a failure of a mesio-occlusal, disto-occlusal or occlusobuccal restorations.
7. A restoration was not regarded as a failure simply because the surface had to be involved in providing retention for a new restoration on another surface.
Since it involves clinical judgement, however, no attempt was made to define exactly the criteria employed when deciding to replace a restoration. Generally, a restoration was con- sidered to require replacement when essentially fracture had occurred or caries had recurred.
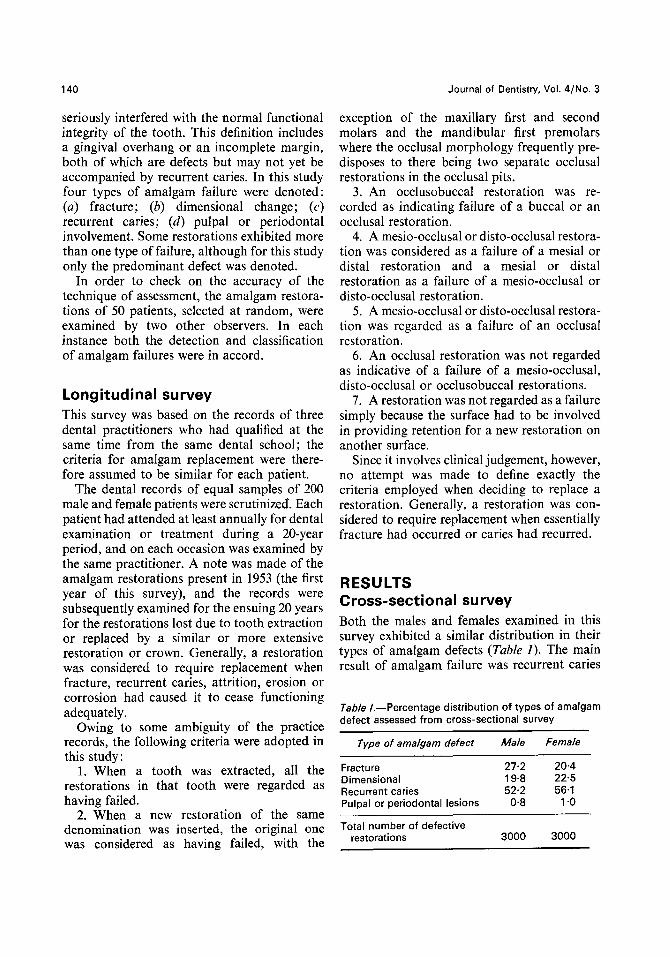
RESULTS Cross-sectional survey Both the males and females examined in this survey exhibited a similar distribution in their types of amalgam defects (Table I). The main result of amalgam failure was recurrent caries
Tab/e /.-Percentage distribution of types of amalgam defect assessed from cross-sectional survey
Type of amalgam defect
Fracture Dimensional Recurrent caries Pulpal or periodontal lesions
Total number of defective restorations
Male Female
27.2 20.4 19.8 22.5 52.2 56.1
0.8 1 .o
3000 3000

Lavelle: Durability of Amalgam Restorations 141
(52 per cent in males and 56 per cent in The range of the number of restorations females). This appeared to arise principally replaced or lost during this 20-year period from faulty cavity preparation as shown by varied markedly (2-l 14) between individual caries around the periphery of the restoration. patients. The number of restorations lasting Furthermore, recurrent caries was detected mainly in occlusal compared with other types of restoration.
Table //.--Replacement or loss of amalgam
Fracture of amalgam restorations accounted restorations per year: longitudinal survey over 20 Years
for 26 ner cent of the defects in males and 30 ner cent in females, whereas dimensional defects occurred in 20 per cent of males and 23 per cent of females. Finally pulpal or periodontal lesions accounted for 1 per cent of the defects in both males and females.
Longitudinal survey The annual replacement or loss of amalgam restoration determined from the longitudinal survey (Tab/e II) shows considerable annual variation. Nevertheless, the mean annual re- placement or loss of 7 restorations per year for a sample of 100 patients indicated quite a low turnover rate. Also, there appeared to be a slight reduction in the annual loss or replace- ment of amalgam restoration towards the end of the 20-year period.
There were some changes in the distribution of the types of amalgam restoration at the beginning and end of the 20-year period (Table III). For instance, in males at the beginning of the period, 9 per cent of the restorations were occlusal, whereas at the end of the period this type of restoration accounted for 7 per cent. By contrast, restorations with three or more surfaces accounted for 16 per cent at the start and 26 per cent at the end of the 20-year period in males, the restoration
Year Males
1 2 3 4 5 6 7 8 9
10 11 12 13 14 15 16 17 18 19 20 Mean replacement or loss of
amalgams per year Standard error
Mean total number of restorations per patient in 20-year period Standard error
Mean number of teeth per patient at start of 20.year period Standard error
Mean number of teeth extracted per patient in 20-year period
7 6 13 7 10 9 12 12 12 16 16 13 18 16 15 16 16 14 21 17 16 20 24 19 22 17 15 9 16 10 16 14 18 10
6 9 9 5 6 9
7.3 6.3 0.72 0.65
49.6 46.7 4.54 4.30
25.1 26.1 0.66 0.69
4.8 4.6 0.87
200
Females
figures for females being 18 and 14 per cent Standard error 0.99
respectively. Number of patients in sample 200
Tab/e ///.-Percentage distribution of amalgam restorations at start and end of 20-year longitudinal survey
Type of restoration Start of survey End of survey Male Female Male Female
Occlusal 9.3 7.2 6.8 8.9 Other single surfaces 33.7 38.9 28.3 33.5 Occlusobuccal, occlusolingual 5.4 4.9 3.4 8.0 Mesio-occlusal, disto-occlusal 30.9 31.5 35.8 36.3 Three or more surfaces 15.9 17.7 26.0 14.3

142 Journal of Dentistry, Vol. ~/NO. 3
less than 5 years averaged 19 per cent for males and 20 per cent in females, whereas the number of amalgams lasting less than 10 years was 50 per cent in males and 51 per cent in females. In both males and females less than 10 per cent of the amalgam restorations lasted for 20 years or more. Furthermore, although there was no significant difference between the mean number of teeth extracted between males and females during the 20-year period, the actual range for individual patients extended from no extractions to a full clearance (pre- sumably as a result of caries or periodontal disease).
DISCUSSION As the effectiveness of any dental service must ultimately be reflected by its impact on caries or tooth loss to the community (Gray et al., 1970; Sheiham, 1973), the durability of amalgam restorations is of paramount signifi- cance. In this context, it is significant that a number of studies (e.g. Easton, 1941) indicate that the majority of amalgam failures result from poor technical skill rather than from failure of the amalgam itself. This conclusion also emerged from the present cross-sectional survey, where recurrent caries was the principal cause of amalgam failures.
It must be emphasized, however, that the patients included in this study were not randomly selected. In the cross-sectional survey only patients attending for the first time for examination and treatment were included, whereas in the longitudinal survey patients of three dental practitioners were included. Furthermore, the oral hygiene or dietary habit of each patient was not monitored, which may have had a direct bearing on the results of the two surveys. Nevertheless, the data from this study were regarded as sufficiently representa- tive to indicate that the durability of amalgam restorations is not as great as traditionally assumed.
Recurrent caries around the periphery of the restoration provided the predominant reason for amalgam failure. It is well known that a space exists between the walls of a cavity and a newly placed restoration, and the ingress of
oral fluids, bacterial toxins and soluble ions of all kinds into this space is termed ‘micro- leakage’. Microleakage can account for stain- ing around the margins of a restoration, pulpal sensitivity and secondary caries (Going, 1972), although the role of microleakage in the failure of the amalgam restorations studied in both cross-sectional or longitudinal surveys could not be assessed. Amalgam restorations have been studied from the standpoint of selection of amalgam alloys (Phillips, 1973), cavity design (Pickard, 1954; Almquist et al., 1973), correct preparation and use of amalgam (Gayler, 1936; Barber and Reisbeck, 1973), retention (Rosenteil, 1957), marginal fit (Eames, 1967; Mahler et al., 1973), corrosion (Eames, 1973) and photo-elastic stress patterns (Robinson, 1964). Nevertheless, as recurrent caries was the predominant cause of amalgam failure, the present study would appear to indicate that the skill of the dental practitioner is probably the principal factor determining the durability of amalgam restorations, as suggested by Wolcott (1958).
REFERENCES ALLAN D. N. (1969) The durability of conservative
restorations. Br. Dent. J. 126, 172-177. ALMQUIST T. C., COWAN R. D. and LAMBERT R. L.
(1973) Conservative amalgam restorations. J. Prosthet. Dent. 29, 524528.
BARBER T. and REISBECK M. H. (1973) Amalgam past, present and future. J. Am. Dent. Assoc. 86, 863-869.
EAMES W. B. (1967) Factors influencing the marginal adaptation of amalgam. J. Am. Dent. Assoc. 75, 629-637.
EAMES W. B. (1973) The effects of saliva con- tamination on dental amalgam. J. Am. Dent. Assoc. 86,652-656.
EASTON G. S. (1941) Causes and prevention of amalgam failures. J. Am. Dent. Assoc. 28, 392- 400.
GAYLER M. L. (1936) The setting of dental amal- gams. Br. Dent. J. 61, 11-18.
GOING R. E. (1972) Microleakage around dental restorations: a summarizing review. J. Am. Dent. Assoc. 84, 1249-1357.
GRAY P. G., TODD J. E., SLACK G. L. and BULMAN J. S. (1970) Adult Dental Health in England and Wales in 1968. London, HMSO.

_.
Lavelle : Durability of Amalgam Restorations 143
HEALEY H. J. and PHILLIPS R. W. (1949) A clinical study of amalgam failures. J. Dent. Res. 28, 439-446.
MAHLER D. B., ADEY J. D. and VAN EYSDEN J. (1973) Microprobe analysis of amalgam. J. Dent. Res. 52, 74-18.
MOORE D. L. and STEWART J. L. (1967) Prevalence of defective dental restorations. J. Prosthet. Dent. 17, 372-378.
PHILLIPS R. W. (I 973) Selection of amalgam alloys : particle form, new formulas. J. Dent. Child. 40, 106-112.
PICKARD H. M. (1954) Everyday procedures in dentistry. Cavity preparation for amalgam fillings. Br. Dent. J. 96,59-65.
RICHARDSON A. S. and BOYD M. A. (1973) Replace- ment of silver amalgam restorations by 50 dentists during 246 working days. J. Can. Dent. Assoc. 39, 556-559.
ROBINSON A. D. (1964) Photoelastic recording of stresses produced by expansion of dental amalgam. Br. Dent. J. 117,145-149.
ROBINSON A. D. (1971) The life of filling. Br. Dent. J. 130,206-208.
ROSENTEIL E. (1957) The retention of inlays and crowns as a function of geometrical form. Br. Dent. J. 103, 388-394.
SHEIHAM A. (1973) An evaluation of the success of dental care in the United Kingdom. Br. Dent. J. 135, 271-279.
WOLCOTT R. B. (1958) Failures in dental amalgam. J. Am. Dent. Assoc. 56, 479-491.