a double-edged sword: managing comorbid chronic illness & … · 2019-08-30 · a double-edged...
TRANSCRIPT

A Double-edged Sword: Managing Comorbid Chronic
Illness & DepressionSusan Calloway, PhD, APRN, PMHNP-BC, FNP-BC, FAANP

Disclosures
• I have no disclosures to report

Objectives
• Analyze the prevalence of depression co-morbid with diabetes, CVD & chronic pain
• Evaluate proposed etiologies of depression
• Assess the impact of untreated depression on health outcomes
• Identify key recommendations for screening for depression
• Differentiate screening from diagnosing depression
• Review medications that increase risk for depressive symptoms
• Summarize selected drug classes used for treating depression

Depression Prevalence
• > 16 million adults have MDD in the U.S. and is the leading cause of disability in individuals 15-44 years of age.
• Median age of onset is 32 years *
• Greater prevalence in women (8.5%) than men (4.8%)
• Individuals with medical comorbidities 3 times more likely to suffer depression than those without chronic health issues , yet often overlooked in non-psychiatric care settings
• It is estimated that 35% of adults with MDD are not receiving any treatment.
*With a PMH of a depressive episode as an adolescent consider increased likelihood of Bipolar II disorder… add MDQ along with family Psych HX

Prevalence of major depression (MD) among US adults. *All other groups are non Hispanic or latino **NH/OPI= Native Hawaiian/Other Pacific Islander ***AI/AN= American Indian/Alaskan Native.

Etiology• Mono-amine deficiency hypothesis
1. Patients in 1950s treated with reserpine which prevents uptake of monoamines*
became severely depressed
2. Also patients being treated with INH for T.B. had improved mood. INH prevents the
breakdown of monoamines
Not all patients with low monoamine levels have depression & not all patients with
depression respond to medications designed to increase monoamine levels
Inflammation hypothesis
1. Patients with MDD have high levels of pro-inflammatory cytokines & receptors plus
high levels of acute phase reactants & chemokines
2. 30-50% of Hep C patients treated with interferon alpha (IFN-α), an inflammatory
cytokine, develop depression
Not all patients with depression are found to have elevated levels of pro-inflammatory
cytokines and not all with inflammation get symptom relief with anti-inflammatories a

Etiology• HPA axis hypothesis
1. Alterations in hormone regulation in the HPA axis due to acute & chronic
stressors resulting in elevated cortisol levels are associated with
depression. Up to 50% of individuals experiencing a major life stressor
develop depression
CBT and other mindfulness based therapies along with meditation, yoga
and exercise reduce stress levels thereby reducing cortisol &improve mood
• Genetics & Epigenetics
1. Widely accepted as contributing to depression due to numerous twin &
family studies.
One parent with depression – 10-25% risk in child; both parents- 50% risk
Epigenetic influences due to ACEs & environmental stressors increase
risk

Impact of Depression on Health Outcomes
• Increased medical symptoms
• Increased utilizers of medical services (women > men)
• Impairment in function
• Reduced adherence to treatment plans
• Increases risk of morbidity and mortality
• Individuals with depression die 5-10 years earlier and those with bipolar disorder die 10-20 years earlier, due to CVD, diabetes, COPD and cancer
(Chang, et al, 2011; Katon, 2011)
Depression & Diabetes

Impact of Depression on Outcomes in Diabetics
• 33% to 52% increase in mortality
• 50% increase in morbidity
• Two fold risk of non-cancer and non-atherosclerotic associated mortality
• Two fold risk of foot ulcers
• 2.7 fold increased risk for development of dementia
•Depression greater predictor of functional impairment thandiabetic complications
Impact of Depression on Health Outcomes in CHD
• 2.4 fold increase in all cause mortality
• 2.6 fold increase in CVD mortality
• 2.0 fold increase in new cardiac events
• Increases risk of mortality and cardiac events in patients with CABG and heart failure
• Bi-directional impact on functional impairment, ie. Functional impairment predicts depression and depression predicts functional impairment
• Depression more predictive of functional impairment than severity of illness
• (Katon, 2011)

Impact of Depression on Health Outcomes in CHD
• The correlation between mood disorders and CVD is significant enough that the AHA issued the following statement:
“MDD and BD are tier II moderate-risk conditions associated with accelerated atherosclerosis and early CVD and position MDD and BD as tier II moderate-risk conditions that require the application of risk stratification and management strategies in accordance with Expert Panel recommendations.” (Goldstein, et al, 2015)

(Goldstein, et al, 2015)

Impact of Depression on Health Outcomes in Chronic Pain
• Most common mental disorder with chronic pain (estimates are 50%).
• Less engagement inpleasurable activities , increased feeling of distress & helplessness due to chronic pain contribute to depression.
• 75% of patients with depression also report pain (Vadivelu, et. al, 2017).
• With depression increase in pain-related catastrophizing (Craig, et al., 2017)
• Poorer treatment response & decreased functioning
• With moderate & severe depression have higher odds of opioid misuse (Feingold, 2018)
• Best treatment outcomes in treating both simultaneously (Miller, R. et al, 2018)

Rationale for screening
• Early identification and treatment
• In spite of similar diagnoses, black patients >50% less likely to use antidepressants
• 50% of patients with depression are unrecognized in medical settings.
• Median duration of delay in treatment initiation after seeing an HCP for depression is 8 years.
• Suggested that under treatment is higher in minority and underserved populations
Are You Routinely Screening & Managing Patients with Co-morbid Depression & Chronic Illness?
Reasons for not Screening
• Not imbedded in the electronic health record
• Lack of time
• Lack of confidence in knowledge base for using DSM 5 criteria to accurately diagnose mood disorders
• Additional time to discuss findings and initiate interventions
• Difficulty in securing timely referral sources for mental health specialty care
• Liability concerns
Jha et al. (2019)

PHQ-2


Diagnosis of Major Depressive Disorder
• At least one of these over a two week period either by subjective report or observation by others
1. Depressed mood
2. Anhedonia- loss of interest or pleasure in all or almost all activities
________________________________________________________________________________________
• Plus 4 > symptoms over that same two week period that occur nearly every day
1. Significant weight loss when not dieting or weight gain or decrease or increase in
appetite nearly every day
2. Insomnia or hypersomnia nearly every day
3. Psychomotor agitation or retardation
4. Fatigue or loss of energy nearly every day
5. Feels of worthlessness or excessive or inappropriate guilt
6. Diminished ability to think or concentrate, or indecisiveness
7. Recurrent thoughts of death, recurrent suicidal ideation or suicide attempt or plan ( American Psychiatric Association, 2013)
Differentials for MDD
• Rule out medical causes
CNS diseases
Thyroid disorders
Inability to convert folic acid to L-methylfolate
Sleep related disorders
Alcohol use and substance use disorders
Infectious diseases such as HIV, lyme disease, syphilis,
SLE

Medications Associated with Depression
Beta blockers –propranolol
Reserpine & methyldopa
Acne treatment – Isotretinoin
Smoking cessation – varenicline
Hep C treatment –Peginterferon alfa
H2 blockers, ie.
ranitidine, cimetidine•
HIV medications- numerous
Steroids
Sex hormones
Sedatives
Muscle relaxants
Appetite suppressants

Antidepressant Drug Classes
Class DrugsSSRIs Citalopram, escitalopram, fluoxetine, fluvoxamine,
paroxetine, sertraline, vilazodone*, vortioxetine**SNRIs Venlafaxine, desvenlafaxine, duloxetineTCAs Amitriptyline, desipramine, doxepin, imipramine,
nortriptyline,
protriptylineMAOIs Isocarboxazid, phenelzine, selegiline, tranylcypromineMiscellaneous Bupropion, mirtazapine, trazodone, esketamine
*
*Also a 5-HT1A partial agonist **Serotonin modulator & stimulator (SMS)

Drug Class Major Side Effects
Class Major Side Effects
SSRIs Headaches, GI distress, insomnia, fatigue, anxiety, sexual dysfunction, weight gain. Citalopram
increases QTc above 40mg. Use lower dose in elderly. Hyponatremia, GI bleeding
SNRIs Nausea, insomnia, dry mouth, headache, increased blood pressure, sexual dysfunction, weight gain.
Venlafaxine can elevate B/P in particular. Hyponatremia, GI bleeding
TCAs Weight gain, sedation, dry mouth, nausea, blurred vision, constipation, tachycardia. Fatal in overdose,
increases QTc.
MAOIs Weight gain, fatigue, sexual dysfunction, hypotension, hypertensive crisis – avoid foods with tyramine
& do not combine with other antidepressant drug classes
Miscellaneous Bupropion loss of appetite, weight loss, insomnia, agitation , headache. Lowers seizure threshold, avoid in patients with h/o seizures and patients with eating disordersMirtazapine – Sedation at lower doses and increased appetiteTrazodone – Sedation, nausea and priapism
*

SGAsFDA approved to augment antidepressants for patients who have failed conventional treatment .
Aripiprazole (causes the least weight gain of the SGAs listed)
Brexiprazole
Olanzapine with fluoxetine- (causes the greatest weight gain of SGAs)
Quetiapine XR
Avoid in the elderly & in patients with cardiovascular disease due to:
Sudden cardiac death
Hypertension
Orthostatic hypotension
Obesity
Dyslipidemia

Treatment of Depression & CVD
• SSRIs inhibit platelet activity and suggest a lower stroke risk in patients with CVD (Katon, 2011)
• Escitalopram reduced risk of cardiovascular events over placebo 40.5% versus 53.6% . The same benefit has not been shown in patients with heart failure treated with escitalopram.
• Studies suggest treatment > 6months provides improved quality of life and reduced depression post CABG
• Reduction in depression severity was associated with improved survival in the antidepressant plus CBT trial
• Exercise reduces depression and all cause mortality in patients with heart failure
• Cardiac rehabilitation reduces depressive symptoms.73% lower mortality and 63% lower depressive symptoms

Treatment of Depression & Diabetes
• Duloxetine is a good choice due to dual indication for treating neuropathic pain
• Otherwise select an antidepressant with less risk of weight gain such as bupropion
• Avoid paroxetine as this causes the most weight gain of the SSRIs & SNRIs
• Avoid mirtazapine due to increase in appetite & potential for weight gain
• Cognitive behavioral therapy has the highest evidence for success in treating depression followed by behavioral activation, problem-solving therapy and interpersonal therapy

Treating Depression & Chronic Pain
• Patients treated with an antidepressant had a 50% reduction in depression. (Singh, 2019).
• Duloxetine has FDA approval for depression and peripheral neuropathy, musculoskeletal pain & fibromyalgia. (A benefit of doses > 60 mg per day has not been demonstrated.) Cannot be used in hepatic or renal impairment.
• TCAs have also shown a benefit but due to side effects are not used first line.
• Speak openly that research has demonstrated that both pain and depression increase when a spouse is critical and hostile. Suggest counseling if this is an issue. (Burns, et al, 2018).
• Cognitive behavioral therapy has the highest evidence for success in treating depression followed by behavioral activation, problem-solving therapy and interpersonal therapy

Psychotherapy• BarriersPersonal
Stigma
Misunderstanding of what occurs in psychotherapy
Reluctant to discuss emotional issues
Want an “easy, quick” fix
Bootstrap thinking
Prior negative experience
Financial
Insurance does not cover or high co-pays or therapist takes cash only
Cost of childcare while seeing therapist
Time
Finding an hour a week for 9-12 weeks or more in an already crowded
schedule is difficult

Counteracting Barriers to Psychotherapy
• Use motivational interviewing techniques to initiate change in considering psychotherapy for those who reject this recommendation
• Discuss that evidence demonstrates “changing thought processes” improves outcomes in chronic illness
• Recommend self-directed CBT either on-line or through a workbook
• Recommend on-line therapy as opposed to in person visits –offers privacy, saves time and is effective
• Suggest apps such as Daylio Mood Tracker, Breathe2Relax, Youper, Happify, Headspace & MoodKit

Take Home Points
• Screen all patients with chronic illness for depression using the PHQ-2
• Conduct further screening with PHQ-9 if PHQ-2 is positive (Always ask about suicidal ideation and high risk protocols)
•Obtain family psych history and screen with Mood Disorder Questionnaire that might suggest risk for BPII
•Develop management plan based on patient specific factors & in collaboration with the patient
• Educate patients that treating depression will help
• improve overall health outcomes.

Patient Resources • CBT workbooks for adults
Gillihan, S. (2016). Retrain your brain: CBT in 7 weeks: a workbook for managing depression and anxiety
Greenberger, D. (2015). Mind Over Mood, 2nd edition. Guildford Press.
• CBT workbooks for children & adolescents
Phifer, L. (2017). CBT Toolbox for Children and Adolescents: Over 200 Worksheets & Exercises for Trauma, ADHD, Autism, Anxiety,
Depression & Conduct Disorders, PESI Publishing
• Apps
Breathe2Relax “ A simple, intuitive, and attractive mobile app designed by the National Center for Telehealth & Technology to teach
breathing techniques to manage stress.”
Daylio-Mood Tracker - “Ever notice that your moods tend to fluctuate at certain times? Daylio can help you pinpoint these trends sooner
so you can make the adjustments you need.”
Happify “ is a self-guided app that aims to increase positive emotions through exercises and games supported by positive psychology and
mindfulness research”
Headspace “Targeted to anyone who wants to learn meditation to reduce anxiety and stress and improve their attention and awareness;
good for a beginner to establish a regular meditative routine.”
Moodkit “ This app will help individuals with depression, anxiety disorders, anger management issues, etc. “
Youper AI Assistant “Chat back and forth with your assistant, who asks prompts that encourage you to think about your thought patterns and
behaviors. The app walks you through techniques you may need in the moment based on your responses. It then summarizes your
conversationsand interactions into insights that help you understand more about your emotional well-being.”

ReferencesAbuRuz, M. E. (2019). Patients with ST segment elevation myocardial infarction: moderating effect of perceived control on the relationship between depression and in-hospital complications. BMC Cardiovascular Disorders, 19(1), N.PAG. https://doi-org.ezproxy.ttuhsc.edu/10.1186/s12872-019-1126-z
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders DSM-5 (5th ed.). Washington, DC: American Psychiatric Association.
Bangshan L, Jin L, Wang, M., Zhang Y & Li L (2017). From serotonin to neuroplasticity:evolvement of theories of major depressive disorder. Front Cell Neuroscience, 11 (305). doi: 10.3389/fncel.2017.00305.
Bidari, et al, 2019).A., Moazen-Zadeh, E., Ghavidel-Parsa, B., Rahmani, S., Hosseini, S., & Hassankhani, A. (2019). Comparing duloxetine and pregabalin for treatment of pain and depression in women with fibromyalgia: an open-label randomized clinical trial. DARU, 27, 149–158. https://doi-org.ezproxy.ttuhsc.edu/10.1007/s40199-019-00257-4
Burns, J. W., Post, K. M., Smith, D. A., Porter, L. S., Buvanendran, A., Fras, A. M., & Keefe, F. J. (2018). Spouse criticism and hostility during marital interaction: effects on pain intensity and behaviors among individuals with chronic low back pain. Pain (03043959), 159(1), 25–32. https://doi-org.ezproxy.ttuhsc.edu/10.1097/j.pain.0000000000001037.
Chang C., Hayes, R.D., Perera, G., Broadbent, M., Fernandes, A. C., Lee, W., Hotopf, M., Stewart, R.(2011). Life expectancy at birth for people with serous mental illness and other major disorders from a secondary mental health care case register in London. PL9S One. 65(5):e 19590. doi: 10.1371/journal.pone.0019590
Craig, A., Guest, R., Tran, Y., Nicholson Perry, K., & Middleton, J. (2017). Pain Catastrophizing and Negative Mood States After Spinal Cord Injury: Transitioning From Inpatient Rehabilitation Into the Community. Journal of Pain, 18(7), 800–810. https://doi-org.ezproxy.ttuhsc.edu/10.1016/j.jpain.2017.02.431.

Feingold, D., Brill, S., Goor-Aryeh, I., Delayahu, Y., & Lev-Ran, S. (2018). The association between severity of depression and prescription opioid misuse among chronic pain patients with and without anxiety: A cross-sectional study. Journal of Affective Disorders, 293–302. https://doi-org.ezproxy.ttuhsc.edu/10.1016/j.jad.2018.04.058
Goldstein, B.I., Carnethon, M.R., Matthews, K.A., McIntrye, R., Miller, G.E., Raghuveer, G. . . . . . McCrindle, B.W. (2015). Major depressive disorder and bipolar disorder predispose youth to accelerated atherosclerosis and early cardiovascular disease: a scientific statement from the American Heart Association. Circulation, 132(10), 965-986. doi: 10.1161/CIR.0000000000000229.
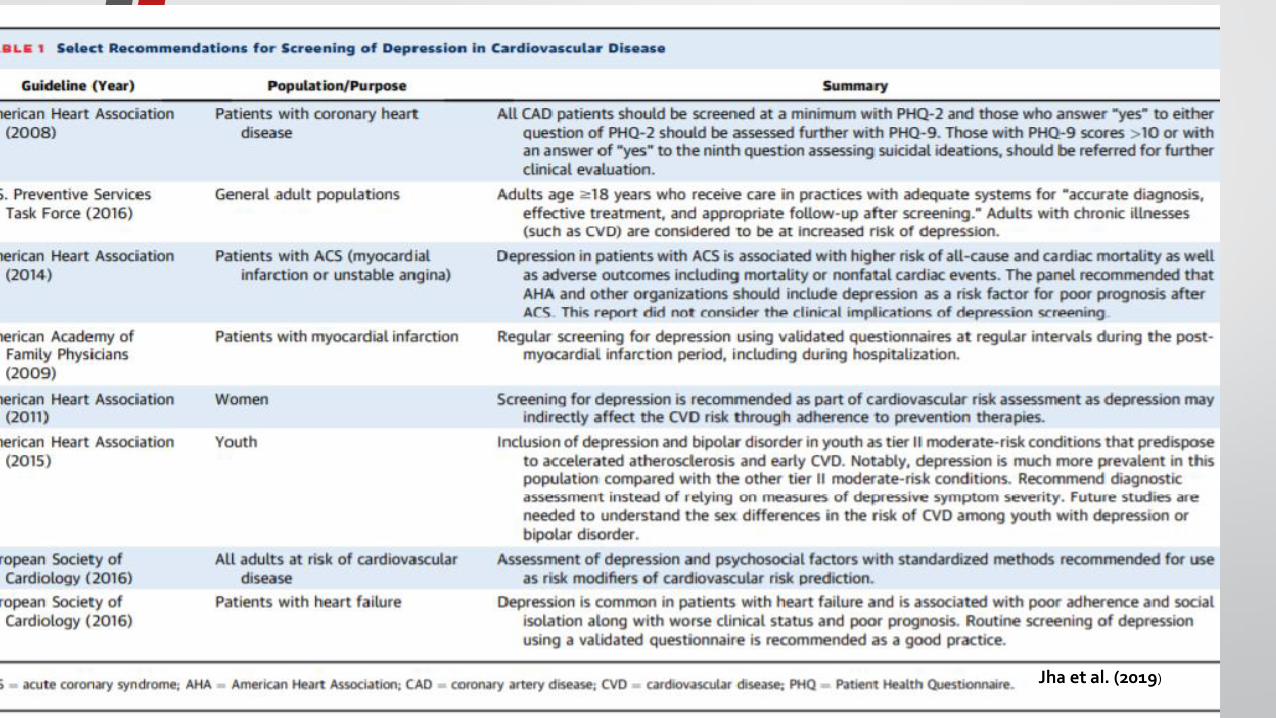
Jha, M. K., Qamar, A., Vaduganathan, M., Charney, D. S., & Murrough, J. W. (2019). Screening and Management of Depression in Patients With Cardiovascular Disease: JACC State-of-the-Art Review. Journal of the American College of Cardiology (JACC), 73(14), 1827–1845. https://doi-org.ezproxy.ttuhsc.edu/10.1016/j.jacc.2019.01.041
Katon W. J. (2011). Epidemiology and treatment of depression in patients with chronic medical illness. Dialogues in clinical neuroscience, 13(1), 7–23.
Miller, R. M., & Kaiser, R. S. (2018). Psychological Characteristics of Chronic Pain: a Review of Current Evidence and Assessment Tools to Enhance Treatment. Current Pain & Headache Reports, 22(3), 1.
Naushad, N., Dunn, L. B., Muñoz, R. F., & Leykin, Y. (2018). Depression increases subjective stigma of chronic pain. Journal of Affective Disorders, 229, 456–462. https://doi-org.ezproxy.ttuhsc.edu/10.1016/j.jad.2017.12.085

Rizvi, S. J., Iskric, A., Calati, R., & Courtet, P. (2017). Psychological and physical pain as predictors of suicide risk: evidence from clinical and neuroimaging findings. Current Opinion in Psychiatry, 30(2), 159–167. https://doi-org.ezproxy.ttuhsc.edu/10.1097/YCO.0000000000000314.Singh, M. (2019). Chronic pain syndrome. Medscape, March 5, 2019.Retrieved from https://emedicine.medscape.com/article/310834-overview
Tsuji, T., Matsudaira, K., Sato, H., & Vietri, J. (2016). The impact of depression among chronic low back pain patients in Japan. BMC Musculoskeletal Disorders, 17, 447. https://doi-org.ezproxy.ttuhsc.edu/10.1186/s12891-016-1304-4.
Vadivelu, N., Kai, A. M., Kodumudi, G., Babayan, K., Fontes, M., & Burg, M. M. (2017). Pain and Psychology-A Reciprocal Relationship. The Ochsner journal, 17(2), 173–180. Retrieved from https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5472077/