a few tricks up its sleeve - ose...
TRANSCRIPT

Equity Research France 360_CR 360 Report
IMPORTANT. Please refer to the last page of this report for “Important disclosures” and analyst(s) certifications.
F Full report
keplercheuvreux.com This research is the product of Kepler Cheuvreux, which is authorised and regulated by the Autorité des Marché Financiers in France.
OSE Immunotherapeutics
France | Pharma & biotech | MCAP EUR 95.9m
20 February 2017
x
A few tricks up its sleeve
Buy (None) Target price EUR 9.00 Current price
Up/downside
Change in TP
Change in EPS none
EUR 6.71
34.1%
none
none 2016E
Main author
Thomas Guillot Equity Research Analyst
[email protected] +33 1 70 98 85 27 Pharma & biotech research team Biographies at the end of the report
What’s it all about? OSE Immunotherapeutics is a biotechnology company specialised in immunotherapy for the treatment of autoimmune diseases and cancer. Our analysis suggests positive optionality for the company thanks to its strong and diversified pipeline. Its strategy consists of out-licensing its non-core assets to rapidly monetise them while externalising all clinical development costs to minimise the related opex. The company’s leading product, Tedopi (currently in phase III), aims to reach the market in 2020, and we estimate peak sales of half a billion euros for this asset. Our in-depth valuation of the company suggests that the street is only including Tedopi, while the company has three under-the-radar, early-stage assets with significant potential.
Kepler Cheuvreux and the issuer have agreed that Kepler Cheuvreux will produce and disseminate investment research on the said issuer as a service to the issuer.

OSE Immunotherapeutics Buy TP EUR 9.00
2 keplercheuvreux.com
360
in 1 minute
Investment case summary We initiate coverage on OSE Immunotherapeutics with a Buy rating.
Tedopi is an asset in late-stage development for the treatment of NSCLC in
2L/3L. We believe that Tedopi is likely to gain value until the phase III
results are released in 2018, as momentum is set to increase. Moreover,
pending Tedopi’s results, we think the advancement of early-stage assets
will also add value to OSE Immunotherapeutics.
Key findings of the report We recommend buying OSE Immunotherapeutics, as we believe Tedopi is
not fairly valued right now, and early-stage assets are not even included in
the company’s value:
We agree with the market that most of the company’s value is in
the Tedopi asset, which presents a risky profile inherent to all
therapeutic vaccines in oncology.
However, even with a 33% probability of success, we are
convinced that the market is not assigning a fair value to Tedopi.
Moreover, we believe that the street does not value the potential
of early-stage assets like FR104 (phase I in partnership with J&J)
and also overlooks Effi-7 (at pre-clinical stage, in partnership with
Servier), which is under the market’s radar screen.
Also, the proprietary product Effi-DEM is a first-in-class candidate
targeting an innovative pathway, with similar potential to that of
the current CKI blockbusters. Although not yet clinically validated,
we believe Effi-DEM is likely to boost OSE Immunotherapeutics’
value in the near future.
Valuation model Our in-depth valuation is based on the potential of: 1) a cautious
positioning of Tedopi in third-line treatment of NSCLC HLA-A2 positive
patient population; 2) FR104 solely in RA (while not taking into account
other potential indications); and 3) Effi-7 in the treatment of ulcerative
colitis. We adopt a discount rate of 15%, in line with our biotech universe.
Our valuation stands at EUR9 per share, and we initiate coverage on OSE
Immunotherapeutics with a Buy rating.

OSE Immunotherapeutics Buy TP EUR 9.00
3 keplercheuvreux.com
Company summary Market data
OSE Immunotherapeutics is a biopharmaceutical company specialised in the development of immunotherapy dedicated to the treatment of cancer and auto-immune diseases. The company's main asset is Tedopi, a therapeutic vaccine developed in NSCLC, currently in phase III, with pivotal results expected in late 2018. Other clinical-stage assets include FR104 which has been out-licensed to J&J as well as Effi-7 in which Servier has an opt-in license option.
Bloomberg Reuters Market cap (EUR) Free float (%) No. of shares outstanding (m) 3m avg. daily vol (EURm) YTD abs. performance 52-week high (EUR) 52-week low (EUR)
OSE FP OSE.PA
95.9m 52.0
14 0
-5.2% 8.15 5.70
Management Key shareholders
Dominique Costantini, CEO
Alexis Peyroles, COO
Maryvonne Hiance, VP, Strategy
Emile Loria 30.6% Dominique Constantini 13.0% Guy Chateain 1.9%
Strengths Weaknesses
One of the fews that has a phase III immunotherapy asset Already monetised non core early-stage assets Effi-DEM is a promising candidate Experienced management
Tedopi is a highly risky development Early-stage nature of the rest of the pipeline Need to sign commercial deal for Tedopi
Opportunities Threats
Tedopi will provide solid value creation if successful NSCLC is a large market Out-licensed candidates bring cash in-flow (FR104/Effi-7) Strong balance sheet
Strong competitive environment for Tedopi in NSCLC Phase III failure for Tedopi/Effi-dem Pricing anticancer therapies
Key financials (please see the end of this report for full financials) Per share data (EUR) 2015 2016E 2017E 2018E
EPS adj and fully diluted -0.01 0.28 -0.66 -0.70
Cash flow per share -0.41 0.51 -0.78 -0.85
Book value per share 4.44 3.92 2.92 2.87
DPS 0.00 0.00 0.00 0.00
Valuation
P/E adjusted and fully diluted na 23.7 na na
P/CF na 13.1 na na
P/BV 2.2 1.7 2.3 2.3
Dividend yield (%) 0.0% 0.0% 0.0% 0.0%
FCF yield (%) -4.3% 7.6% -11.7% -12.6%
EV/Sales 25.3 3.9 na na
EV/EBITDA na 19.9 na na
EV/EBIT na 19.9 na na
Income statement (EURm)
Sales 5.1 20.3 0.0 0.0
% Change +chg 300.1% -chg na
EBITDA adjusted -3.8 4.0 -11.2 -12.1
EBIT adjusted -3.8 4.0 -11.2 -12.1
Adjusted EBIT margin (%) -74.1% 19.7% na na
Net profit reported -0.2 4.0 -9.4 -10.0
Net profit adjusted -0.2 4.0 -9.4 -10.0
Cash flow statement (EURm)
CF from operating activities -5.9 7.3 -11.2 -12.1
Capex 0.0 0.0 0.0 0.0
Free cash flow -5.9 7.3 -11.2 -12.1
Balance sheet (EURm)
Intangible assets 61.1 45.6 57.5 83.9
Tangible assets 0.1 0.1 0.1 0.1
Fin. & other non-current assets 0.1 0.1 0.1 0.1
Total shareholders' equity 63.4 56.0 41.7 41.0
Pension provisions 0.0 0.0 0.0 0.0
Liabilities and provisions 21.9 19.4 34.3 49.3
Net financial debt -9.0 -16.3 -5.1 7.0
Working capital requirement 8.1 4.0 -1.0 -6.0
Invested capital 8.2 4.1 -0.9 -5.9
Ratios
ROE na 6.8% -19.2% -24.3%
ROIC na 43.7% -477.6% na
EV/IC 15.6 19.6 na na
Gearing -14.2% -29.1% -12.2% 17.1%
1 year performance 2011
5.5
6.0
6.5
7.0
7.5
8.0
8.5
Feb 16 May 16 Aug 16 Nov 16 Feb 17Price DJ Stoxx 600 (rebased)

OSE Immunotherapeutics Buy TP EUR 9.00
4 keplercheuvreux.com
Investment case in six charts
Chart 1: OSE Immunotherapeutics portfolio
Chart 2: Overall survival of phase II with Tedopi
Source: OSE Immunotherapeutics Source: Kepler Cheuvreux
Chart 3: Mechanisms of action Effi-DEM
Chart 4: Mechanisms of action FR104
Source: Kepler Cheuvreux Source: Kepler Cheuvreux
Chart 5: Mechanisms of action Effi-7
Chart 6: SOP (EURm)
Source: Kepler Cheuvreux Source: Kepler Cheuvreux
FR104
EFFi-7
Tedopi®
Effi-DEM
Cancer
Immunosuppression
AutoimmuneInflammatory diseases
Allograft rejection
Immune activation and regulationSurvival functionCensored
Time survived (days)
Cu
mu
lati
ve
su
rviv
al
1.0
0.8
0.6
0.4
0.2
0200 400 600 800 1,000
EUR131m
EUR97m EUR12m EUR6m
EUR17m
-
20
40
60
80
100
120
140
160
rNPV Tedopi rNPV FR104 rNPV Effi-7Net cash position Base case

OSE Immunotherapeutics Buy TP EUR 9.00
5 keplercheuvreux.com
Contents
Investment case in six charts 4
Investment case summary 7
Paving the way for value creation 7
Cancer immunotherapy: the core focus 7
FR104 and Effi-7: already monetised 8
Initiating coverage with a Buy rating and a TP of EUR9 8
Paving the way for value creation 9
An attractive pipeline emerged from the merger 9
Unity is strength 10
Strategy: quickly provide value creation from non-core assets 11
Cancer immunotherapy: the core focus 12
Tedopi: a multi-epitope cancer vaccine 12
Tedopi target NSCLC: the largest cancer market 14
Promising phase II needs to be confirmed 18
Effi-DEM: the future immune-oncology blockbuster? 26
FR104 and Effi-7: already monetised 34
FR104: a ground-breaking opportunity in autoimmune diseases 34
J&J: a landmark partner for FR104 36
FR104: looking to grab a piece of the large RA market 37
Competitive environment in CD80/CD28 pathway 41
Effi-7: already monetised to Servier, the right strategic option? 43
Deconstructing the forecasts 48
Cancer drug pricing 48
Tedopi: a place in 2L/3L NSCLC 49
FR104 in RA 51
Effi-7: next milestone payment in five years 53
Initiating coverage with a Buy rating 55
Main risks for Tedopi: finding the right partner for EU/US commercialisation 55
Main assumptions of our rNPV for Tedopi 56
rNPV of Tedopi in NSCLC (EUR97m) 57
rNPV of FR104 in RA (EUR12) 58
rNPV of Effi-7 in UC (EUR6m) 60
SOP summary 61

OSE Immunotherapeutics Buy TP EUR 9.00
6 keplercheuvreux.com
Appendices 62
Shareholders 62
Key people 62
Immune system functions 63
Use of the immune system to fight diseases: immunotherapy 65
Immunotherapy applied to cancer 66
Immunotherapy applied to autoimmune diseases 71
Research ratings and important disclosures 76
Legal and disclosure information 79

OSE Immunotherapeutics Buy TP EUR 9.00
7 keplercheuvreux.com
Investment case summary We initiate coverage on OSE Immunotherapeutics with a Buy rating and a target
price of EUR9. Even though we perceive Tedopi as a highly risky asset (we
believe the product has a 33% chance of succeeding), we think that OSE
Immunotherapeutics’ main candidate is currently undervalued. Moreover, we
feel confident about the prospect of early-stage candidates. We think that the
pipeline is likely to drive value creation until the end of 2018 and the phase III
results of Tedopi, which will be a landmark event for the company. Until then, we
think that the advancement of Effi-DEM, FR104 and Effi-7 will provide
momentum for the company.
Paving the way for value creation
OSE Immunotherapeutics was set up in June 2016 with the merger between
Effimune and OSE Pharma. This led to the creation of a strong player in
immunotherapy with a diversified range of solid blockbuster therapeutic candidates.
The diversification of its pipeline allowed the company to reduce the development
risk inherent to immunotherapy.
Thanks to the merger, OSE Immunotherapeutics is now developing its portfolio both
for autoimmune and oncology conditions. The company’s leading asset is Tedopi, a
therapeutic vaccine provided by OSE Pharma and developed in lung cancer. The
candidate is currently in phase III of development with clinical data expected as
soon as 2018. Effimune provided the rest of the portfolio, which is made up of:
1) Effi-DEM, a preclinical-stage new generation of checkpoint inhibitors developed
in oncology; 2) FR104, a clinical-stage candidate developed in rheumatoid arthritis
and out-licensed to J&J; and 3) Effi-7, a preclinical-stage candidate developed in
autoimmune diseases and out-licensed to Servier.
Cancer immunotherapy: the core focus
OSE Immunotherapeutics mainly focuses on immunotherapy applied to oncology.
The company currently has two proprietary owned products under development:
1) Tedopi, a therapeutic vaccine currently in phase III for the treatment of lung
cancer; and 2) Effi-DEM, a preclinical stage immunotherapy, modulating the tumour
microenvironment.
Tedopi’s phase III results are expected in late-2018. If positive, the product is likely
to boost the value of OSE Immunotherapeutics. That said, we question the prospects
of the asset, due to: 1) the notoriously risky field of therapeutic vaccines applied to
oncology; 2) the fierce competitive environment of late-stage NSCLC candidates;
and 3) the lack of clinical evidence with statistical significance shown in phase II
by Tedopi.
However, we are optimistic about Effi-DEM’s prospects. We believe Effi-DEM is an
under-the-radar asset with the potential to become a blockbuster. Although not yet
clinically validated, based on the scientific literature and preclinical data, we believe
targeting SIRPαpathway holds promise.

OSE Immunotherapeutics Buy TP EUR 9.00
8 keplercheuvreux.com
FR104 and Effi-7: already monetised
FR104 and Effi-7 are two monoclonal antibodies developed for the treatment of
autoimmune diseases. Both assets have already been out-licensed to partners by
OSE Immunotherapeutics.
A partnership agreement has been reached with J&J in relation to FR104, providing
a EUR10m opt-in option payment to OSE Immunotherapeutics in July 2016. In the
event of clinical success, FR104 is likely to become a blockbuster with solid activity
both in rheumatology and in transplant complication management. FR104 is no
longer a source of cost and now represents a cash inflow opportunity for OSE
Immunotherapeutics. Indeed, following its opt-in options, J&J will fund all the
development costs as of now. Therefore, FR104 is now a potential source of cash-in
for OSE Immunotherapeutics.
OSE Immunotherapeutics secured EFFI-7 through an out-license deal with Servier in
December 2016 with an opt-in option after the completion of phase II. Funding until
phase II is also partly secured thanks to a consortium led by OSE
Immunotherapeutics.
We believe these two assets will provide sufficient funding to the company to
finance EFFI-DEM development, therefore significantly derisking the group’s profile.
Initiating coverage with a Buy rating and a TP of EUR9
Our valuation of OSE Immunotherapeutics focuses on three candidates: Tedopi,
FR104, and Effi-7. Even though we do not include Effi-DEM, due to its preclinical
early-stage development, we have emphasised the potential of this candidate and
will look closely at its future development.
We think that OSE Immunotherapeutics is likely to out-license Tedopi in all
territories and will only retain milestone payments and royalties based on
commercial performance. Hence, we do not see any commercial structure or facility
emerging from the company for Tedopi. For FR104, we forecast the royalties and
milestones resulting from the J&J partnership. We are confident that even though
the development time will be lengthy, the candidate has a good chance of reaching
blockbuster status in the event of clinical success, due to its potential in in a broad
range of autoimmune conditions.
The next major milestone will be the positive or negative outcome of the phase III
trial of Tedopi in 2018. In the event of clinical or regulatory failure, we think that the
company is likely to pursue the development of Effi-DEM, thanks to the financing
provided by FR104, and to a lesser degree by Effi-7. We think that the current
valuation does not include the potential of early-stage assets, but it also undervalues
Tedopi. We initiate coverage with a Buy rating and a target price of EUR9.

OSE Immunotherapeutics Buy TP EUR 9.00
9 keplercheuvreux.com
Paving the way for value creation OSE Immunotherapeutics was created in June 2016 through the merger of
Effimune and OSE Pharma, establishing a strong player in immunotherapy with a
diversified range of solid blockbuster therapeutic candidates. The diversification
of its pipeline allowed the company to reduce the development risks inherent to
immunotherapy.
Thanks to the merger, OSE Immunotherapeutics is now developing its portfolio
both for autoimmune and oncology conditions. Its leading asset is Tedopi, a
therapeutic vaccine provided by OSE Pharma and developed in lung cancer. The
candidate is currently in phase III of development with clinical data expected as
soon as 2018. Effimune provided the rest of the portfolio, which is made up of: 1)
Effi-DEM, a preclinical stage new generation of checkpoint inhibitors developed
in oncology; 2) FR104, a clinical-stage candidate developed in rheumatoid
arthritis and out-licensed to J&J; and 3) Effi-7, a preclinical-stage candidate
developed in autoimmune diseases and out-licensed to Servier.
An attractive pipeline emerged from the merger
OSE Pharma history OSE Pharma was founded in April 2012 by Emile Loria and Dominique Costantini.
The two managers created the structure to further develop Tedopi, a lung cancer
therapeutic vaccine that has been under clinical-stage development since 2003.
Tedopi was developed first by Epimmune before a takeover by IDM pharma in 2005,
followed by Takeda in 2007.
Following the acquisition of IDM by Takeda, some of IDM’s assets, including Tedopi,
were deprioritised, and their development halted. Emile Loria decided to pursue the
development of Tedopi. Thanks to positive phase IIb results in specific lung cancer
populations, OSE Pharma decided to seek financing to start a phase III trial and
carried out an IPO in March 2015, raising EUR21.1m.
Effimune history Effimune was founded in 2007 in Nantes, France. The company is a spin-off of
INSERM and the Institute of Transplantation, Urology and Nephrology (ITUN) in
Nantes. Effimune is specialised in immune regulation for clinical application in auto-
immune, transplants, and immuno-oncology (IO).
Thanks to its preliminary research highlighting key immuno-regulator receptors,
Effimune managed to develop three product candidates: FR104, Effi-7, and
Effi-DEM.
Effimune sought to raise EUR5m in 2015 and up to EUR20m in 2016 to speed up its
internal development pipeline. According to the street, due to the lack of financing
solutions and tough equity market conditions, Effimune agreed to merge with OSE
Pharma to form OSE Immunotherapeutics, a leading group with two areas of
expertise: immunology and oncology.
Effimune brought three assets: FR104, Effi-7 and Effi-DEM

OSE Immunotherapeutics Buy TP EUR 9.00
10 keplercheuvreux.com
A diversified pipeline Thanks to the merger, OSE Immunotherapeutics has a well-diversified pipeline, both
in oncology and autoimmune diseases.
Chart 7: OSE Immunotherapeutics’ pipeline
Note: (1) checkpoint inhibitors (PD-1/PD-L1) Source: Kepler Cheuvreux, OSE Immunotherapeutics
Unity is strength
In February 2016, OSE Pharma announced its intention to merge with Effimune. The
purpose of the merger was to create a balanced portfolio in immunotherapy. At the
time, OSE Pharma only had one asset, Tedopi, in late-stage development in lung
cancer, while Effimune had three early-stage candidates. The merger resulted in a
balanced and less risky pipeline portfolio. The all-stock operation closed in June
2016. It resulted in an entity named OSE Immunotherapeutics and 71%-owned by
ex-OSE Pharma shareholders and 29% owned by ex-Effimune shareholders.
Whereas OSE Pharma solely focused on oncology, Effimune has specialised in
restoring the balance of the immune system for oncology and autoimmune diseases.
Thanks to the acquisition of Effimune, OSE Pharma has significantly expanded its
pipeline toward other mechanisms of action and other targeted therapeutic areas.
Chart 8: OSE Immunotherapeutics aims to rebalance the immune system
Source: OSE Immunotherapeutics
Product Mechanism of action Indications Status Related party
Preclinical I II III Reg.
Oncology
Tedopi Multi-epitope cancer vaccine NSCLC - HLA-A2+ Expected registration: 2019
Tedopi + CKI(1) Multi-epitope cancer vaccine NSCLC - HLA-A2+ Expected phase II start: 2017
Effi-DEM SIRP-α inhibitor Solid tumours Expected start clinical stage: H2 2018
Autoimmune diseases
FR104 Anti CD-28 Rheumatoid arthritis Expected start phase II: H2 2017/2018
Effi-7 Anti IL-7 Ulcerative collitis Expected start clinical stage: H2 2018
Clinical Phase
FR104
EFFi-7
Tedopi®
Effi-DEM
Cancer
Immunosuppression
AutoimmuneInflammatory diseases
Allograft rejection
Immune activation and regulation
OSE Immunotherapeutics aims to modulate the immune system to tackle severe immune-related conditions

OSE Immunotherapeutics Buy TP EUR 9.00
11 keplercheuvreux.com
Strategy: quickly provide value creation from non-core assets
We estimate that OSE Immunotherapeutics has sufficient funding until end-2018
with a cash position that we estimate at c. EUR19m. After that, all will depend on
the outcome of Tedopi.
The positive cash position has been made possible thanks to the IPO in 2015
(EUR21.1m raised) and the monetisation of the proprietary assets to partners
through licensing (EUR20.25m added in 2016).
OSE Immunotherapeutics has adopted a cash-in strategy by out-licensing its non-
core assets at an early stage of development. Hence, the company has decided to
partner up for its autoimmune diseases candidates FR104 (J&J) and Effi-7 (Servier)
while keeping the rights for its oncology pipeline (Tedopi and Effi-DEM). While
derisking the company’s profile, this strategy also has its limitations, as OSE
Immunotherapeutics retains a smaller percentage of the value of these assets at an
early stage.
Table 1: Value share figures for Biotech/Pharma deals
Licensor (OSE Immunotherapeutics)
Licensee (Servier / J&J)
Preclinical (Effi-7) 10-20% 80-90% IND (FR104) 20-40% 60-80% Phase IIb/III 40-60% 40-60% Approval 60-80% 20-40%
Source: Bogdan and Villiger
OSE Immunotherapeutics has chosen to outsource most of its R&D development
costs, which gives the company flexibility in its resource allocation. Thus, to perform
its clinical trials and manufacture its drug candidates, OSE Immunotherapeutics uses
contract research organisations (CROs) and contract manufacturing organisations
(CMOs). For example, for Tedopi, the phase III trial is conducted by CRO Simbec
Orion, while production of Tedopi is outsourced to PPL (APIs) and Bacinex
(formulation). To limit its R&D expenses, OSE Immunotherapeutics has chosen to
pay its services provider with stock options. We expect this type of payment to be
moderately dilutive for the company in the near future.
Cash is sufficient until the results of Tedopi in phase III

OSE Immunotherapeutics Buy TP EUR 9.00
12 keplercheuvreux.com
Cancer immunotherapy: the core focus OSE Immunotherapeutics mainly focuses on immunotherapy applied to
oncology. The company currently has two proprietary products under
development: 1) Tedopi, a therapeutic vaccine currently in phase III for the
treatment of lung cancer; and 2) Effi-DEM, a preclinical stage immunotherapy,
modulating the tumour microenvironment.
Tedopi’s phase III results are expected in late-2018. If positive, the product is
likely to boost the value of OSE Immunotherapeutics. That said, we are cautious
on the asset’s prospects, due to: 1) the notoriously risky field of therapeutic
vaccines applied to oncology; 2) the fierce competitive environment of late-
stage NSCLC candidates; and 3) the lack of clinical evidence with statistical
significance shown in phase II by Tedopi.
However, we are optimistic about Effi-DEM, which we believe is an under-the-
radar asset with the potential to become a blockbuster. Although not yet
clinically validated, based on the scientific literature and preclinical data, we
believe that targeting the SIRPαpathway holds promise.
Tedopi: a multi-epitope cancer vaccine
Tedopi is a cancer vaccine that is being developed in non-small lung cancer (NSCLC)
and currently in phase III of development with final results expected in 2018.
Historical development Tedopi, also named OSE-2101, was initially developed by Epimmune between 2001
and 2006. The development of the project was led by Emile Loria, one of the
founders of OSE Pharma. In 2006, Epimmune merged with IDM Pharma before
being taken over by the Japanese pharmaceutical company Takeda in 2009.
Over 2011-12, Emile Loria decided to acquire OSE-2101’s IP from Takeda and the
technology dedicated to this asset (named Memopi) to launch OSE Pharma.
Mechanism of action Tedopi has been engineered to selectively target the Human Leukocytes Antigen
(HLA) of class I (HLA-A2). HLA is a similar name for major histocompatibility
complex (MHC). MHC are cell-surface proteins responsible of the interaction of
antigen-presenting cells (APC) and effector lymphocytes cells (like CD4+ or CD8+).

OSE Immunotherapeutics Buy TP EUR 9.00
13 keplercheuvreux.com
Chart 9: Major histocompatibility complex (MHC) class I and II
Source: Nature
HLA-A2 is a serotype (subcategory) of MHC type I, which is the MHC that triggers
the education of the CD8+ T cells. This serotype is present in 45% of the population,
according to OSE Immunotherapeutics. Due to this moderate frequency, Tedopi
has received orphan drug status in the US.
Tedopi is an off-the-shelf therapeutic vaccine comprising nine epitopes that address
five well-known tumour-associated antigens (TAAs). The tenth synthetic peptide is
the pan-DR epitope (PADRE), a well-known helper T-Lymphocyte (HTL) epitope
included to increase the magnitude and duration of cytotoxic T-lymphocyte (CTLs)
responses. All these epitopes were designed to selectively recognise the HLA-A2
serotype.
Accordingly, Tedopi was designed to induce CTL responses against TAAs frequently
observed in NSCLC (non-small cell lung cancer), such as:
Carcinoembryonic antigens (CEA): glycoproteins involved in cell adhesion, which is present in c. 70% of lung cancers.
P53: Protein p53 is common in cancer and gained functions that help to contribute to malignant progression. The mutation of p53 is present in 40-50% of NSCLC (Korst & Crystal, 2003).
HER-2/neu: HER2 is a member of the human epidermal growth factor receptor (HER/EGFR). This glycoprotein is involved in cellular expansion for some cancer cells. This mutation is found in 22-50% of NSCLC (Korst & Krystal, 2003).
MAGE-2 (melanoma-associated antigen 2): MAGE-2 genes are almost universally expressed in body tissues.
MAGE-3 (melanoma-associated antigen 3): Like MAGE-2, this antigen is expressed in many types of cancer.
All of these mutations are considered as poor prognosis factors for the development
of the cancer, notably in NSCLC. The originality of Tedopi’s formulation is its ability
to generate an immune response against ten epitopes present in five antigens while
traditional therapeutic vaccine formulations only target one antigen.
Peptide Glyco
CD8+
T cellCD4*T cell
MHCClass I
MHCClass II
Antigen-presenting cell
Diverse TCR
Tedopi targets five TAAs evenly found in NSCLC

OSE Immunotherapeutics Buy TP EUR 9.00
14 keplercheuvreux.com
Moreover, Tedopi does not induce B-cell responses, contrary to therapeutic
vaccines based on one or several antigens and only trigger T cell responses thanks to
its specific traits.
A notorious, high-risk field Note that cancer vaccine therapies have suffered numerous setbacks over the past
decade due to the insufficient response they provided. Many companies have faced
clinical development setbacks, in particular in peptide-based vaccines.
Table 2:Recent outcome of peptide-based cancer vaccine
Product Company Formulation Cancer Status Outcome Cause
GV1001 KAEL-GemVax Co Telomerase peptide-based vaccine
Pancreatic cancer Abandoned (June 2013) Failure Efficacy
Stimuvax Merck KGaA / Oncothyreon MUC1-antigen specific
NSCLC Abandoned (December 2012) Failure Efficacy
NeuVax Galena Biopharma HER2-directed cancer immunotherapy
Breast cancer Discontinued (June 2016) uncertain Efficacy
PAS Cancer Advances Anti-G17 & (Gly) G17 vaccine
Pancreatic cancer PIII completed results uncertain n.a. GIST PIII completed results uncertain n.a.
IMA901 Immatics Multipeptide cancer vaccine Renal cell carcinoma PIII (September 2015) Failure Efficacy
Elpamotide/ OTS-102 OncoTherapy Science VEGFR2 epitope based vaccine Pancreatic cancer PIII Failure Efficacy
Source: Kepler Cheuvreux
Only one cancer vaccine has been approved so far by the FDA: Provenge (by
Dendreon, which is now part of Valeant), for its use in prostate cancer. However, the
commercial prospects of the vaccine have been limited due to manufacturing and
logistical issues that have impeded the commercialisation of the product.
Immatics, a German company that developed a multi-epitope based vaccine like
Tedopi, failed to reproduce positive phase II results in its pivotal phase III. The
setback was due to the change of phase III design compared to phase II.
Tedopi target NSCLC: the largest cancer market
Tumour grades at a glance Tumours are an evolving disease and patients are screened according to their grade.
The tumour grade refers to the description of a tumour based on what cancer cells
and tumour tissue look like. This provides doctors with valuable indications about
how quickly a tumour is likely to grow and spread to other parts of the body. While
some types of cancer have their own grading systems, tumours are generally graded
as 1, 2, or 3. A low-grade cancer is likely to grow and spread more slowly than a high-
grade one.
An early diagnosis significantly increases the overall chances of survival
Numerous therapeutic vaccines failed to reproduce early-stage promises

OSE Immunotherapeutics Buy TP EUR 9.00
15 keplercheuvreux.com
Chart 10: Cancer grades
Chart 11: Cancer stages
Source: National Cancer Institute Source: National Cancer Institute
Cancers in the initial stage (grade 1) are the least malignant tumours and are
associated with long-term survival. Cancer cells tend to be growing slowly and
exhibit an almost normal appearance. Importantly, surgery alone can be an effective
treatment for this grade of tumour. Grade 2 cancer cells look slightly abnormal and
tumours grow faster than in the previous grade. The distinction between grades 2
and 3 is not always clear-cut. Nevertheless, the cells of a grade 3 tumour look very
different to normal cells and grow fast in disorganised, irregular patterns. Grade 3
cancer cells start to spread to nearby healthy tissue.
NSCLC at a glance NSCLC (non-small-cell lung cancer) represent 85% of total lung cancer. Tobacco
smoking is by far the leading cause of lung cancer. According to the American Cancer
Society, 80% of lung cancers are thought to be linked to smoking. The number of
cases has reached 560,000 patients in the world’s seven major markets (the US,
Japan, France, Germany, Italy, Spain and UK). Globally, it represents nearly 1.8m
cases. Lung cancer accounts for 20% of all cancer-related deaths and is involved in
1.6m deaths each year, three times more than breast and colorectal cancers
combined (1.3m deaths).
There are three main kinds of NSCLC depending on the type of cancer cell:
adenorcarcinoma (non-squamous cells), squamous cell carcinoma, and large cell lung
cancer. Despite the recent improvement in the treatment and management of
NSCLC thanks to the emergence of immunotherapies, there is still a high unmet
medical need for late-stage cancer (IIIB/IV).
Grade 1
Cancer cells look very similar to
normal cells and are growing
slowly
Grade 2
Cancer cells look unlike normal cells and are
growing more quickly than
normal
Grade 3
Cancer cells look very abnormal
and are growing quickly
1
2
3
Stage 1
The cancer is small and has not spread anywhere
else
Stage 2
The cancer has grown but has not spread
Stage 3
The cancer is larger and may have spread to the
surrounding tissues and/or the lymph nodes
1 2
3
Stage 4
The cancer has spread from where it started to at least one other body
organ
4
The higher the grade, the more dangerous the tumour

OSE Immunotherapeutics Buy TP EUR 9.00
16 keplercheuvreux.com
Table 3: NSCLC treatment and overall survival
Stage Treatment Five-year survival rate at diagnosis
Stage Ia Surgery, consisting of removing either the affected part of the lung or the whole lung. If surgery is not possible, radiotherapy is recommended
49%
Stage Ib Surgery, possibly followed by chemotherapy. If surgery is not possible, radiotherapy is recommended 45%
Stage II Surgery followed by chemotherapy. If surgery is not possible, radiotherapy is recommended 30%
Stage IIIa Chemotherapy, possibly combined with surgery or radiotherapy 14% Stage IIIb Chemotherapy combined with radiotherapy, surgery is an exception 5%
Stage IV Chemotherapy may be combined with other types of treatments (“targeted therapy” on particular mutations for instance)
1%
Source: Cancer.gov, OSE Immunotherapeutics
According to the NIH, 57% of patients are diagnosed with lung cancer at a later
stage when survival chances are lower. Tedopi aims to target the large NSCLC
market for the second and third-line treatment of advanced stage lung cancer.
Treatment of late-stage NSCLC
Usually, early-stage (stage I to II) treatment of NSCLC starts with removal surgery if
the tumour is found to be resecable and the patient is able to tolerate surgery.
Patients often receive radiotherapy and/or chemotherapy or targeted therapy to
avoid tumour relapse. In the event of tumour progression, physicians usually use
chemotherapy as a combination of platinum-based agents (cisplatin or carboplatin)
and other chemotherapy agents called taxans (e.g. Taxotere from Sanofi).
The recent approval of CKIs (checkpoint inhibitors) has led the guideline writers to
significantly change their recommendations. Previously, Taxotere (docetaxel) was
considered to be a standard second-line option and was often used for subsequent
therapy in patients whose cancer had progressed on first-line platinum-based
chemotherapy regimens.
Fierce competition in late-stage NSCLC Checkpoint inhibitors (CKIs) are the new standard of care in 2L
The competitive landscape in immune-oncology (IO) is extremely complex and fast-
moving. Nowadays, the new standards of care in 2L are the CKIs as part of the new
immuno-therapy paradigm. In the US, the NCCN guidelines have recommended
CKIs as preferred agents against Taxotere (docetaxel) based on improved overall
survival rates, higher response rates, longer duration of response, and fewer adverse
events compared with docetaxel therapy. The European guidelines also indicated a
preference for the use of CKIs in the event of positive PD-L1 histology.
NSCLC treatments: a personalised approach
Another aspect of the market to bear in mind is the upcoming maturity of targeted
therapies. NSCLC may be classified according to the mutations as follows:

OSE Immunotherapeutics Buy TP EUR 9.00
17 keplercheuvreux.com
Chart 12: NSCLC types
Source: Roche
Non-squamous cell carcinomas (adenocarcinoma) represent almost 65% of
NSCLC. Within this category, the past couple of years have seen the emergence
of targeted therapies, which are usually developed along with a biomarker to
diagnose the mutation.
Targeted treatments are being developed to overcome the aberrant oncogenic
pathways of these mutant genes. Several epidermal growth factor receptor (EGFR)
and anaplastic lymphoma kinase (ALK) inhibitors have now been approved that
demonstrate a large magnitude of durable overall response rate (ORR) in patients
with NSCLC who harbour certain EGFR mutations and ALK rearrangements.
For instance, Iressa from AstraZeneca has been approved as the first-line treatment
of advanced EGFR+ NSCLC. Other gene-mutation-related treatments have been
approved (e.g. Xalkori for ALK+ cancer) or are being developed (e.g. Tafinlar for
BRAF mutations in NSCLC).
A new generation of treatment is also emerging: Tagrisso from AstraZeneca is a new
generation of targeted therapies for second-line EGFR specific T790M gene
mutation adenocarcinoma. The Aura3 phase III enrolled 419 patients and data
showed an impressive improvement in progression-free survival after 5.7 months
compared to chemotherapy. For patients with brain metastasis, PFS was 8.5 months
with Tagrisso versus 4.2 months for the chemotherapy-based regiment.
AstraZeneca is beginning the life-cycle management phase of this new therapy and
is planning to develop the Tagrisso in 1L EGFR-positive mutation.
12%
11%
4%
1%
1%
19% 18%
35%
KRAS+ adenocarcinoma
EGFR+ adenocarcinoma
ALK+ adenocarcinoma
HER2+ adenocarcinoma
BRAF+ adenocarcinoma
Unknown adenocarcinoma
large cell carcinoma
squamous cell carcinoma

OSE Immunotherapeutics Buy TP EUR 9.00
18 keplercheuvreux.com
Neoantigen vaccines: the biggest threat for Tedopi?
Neoantigen therapeutic vaccine development is a growing paradigm to restore a
specific T cell response against cancer. With advancement in genome sequencing, it
is now possible to identify a new class of tumour-specific antigens derived from
mutated proteins (called neo-antigens) that are only present in the tumour.
This approach differs from that of OSE Immunotherapeutics whose vaccines include
tumour-associated antigen epitopes that are usually found in tumour cells but not in
every tumour’s phenotype. Meanwhile, Tedopi is likely to have a varied impact on
most of the tumours that it targets.
Conversely, these “neoantigens” should provide highly specific targets for
antitumour immunity and create more specific T cell responses. Although many
challenges remain in producing and testing neoantigen-based vaccines customised
for each patient, a neoantigen vaccine offers a promising new approach to induce
highly focused antitumour T cells aimed at eradicating cancer cells.
Table 4: Neoantigen vaccines under development
Company name Product Phase Indication Comments
Gritstone Oncology n.a. Research Lung cancer Established in 2015 with a USD102m series A BioNtech IVAC Phase I Breast cancer/
melanoma In September 2016, BioNtech signed a deal agreement with Genentech
for the development of its mRNA based neoantigen technology Vaccibody VB10.16 HPV-16 cancer-drive,
therapy Raised EUR24m in December 2016 through a private placement
Moderna Therapeutics/ Merck
n.a. Research n.a. Largest funded-biotech ever with more than USD1.4bn financing
Neon Therapeutics NEO-PV-01 Phase I Melanoma, NSCLC and bladder cancer
First patients of the phase I enrolled in November 2016
Source: Kepler Cheuvreux
Overall, we perceive the NSCLC market as a challenging, highly competitive
market with the emergence of breakthrough therapy in the near future. A
personalised approach (kinase inhibitors), a specific cancer approach (neoantigen
vaccines) and the modulation of other immune pathways (tumour
microenvironment, NK cells) are likely to lead to a high degree of competition. Most
of these treatments will be used in combination and not in monotherapy to
strengthen their therapeutic effect.
Promising phase II needs to be confirmed
Phase II showed promising clinical data, with an unconventional design In 2008, Epimmune, the former owner of Tedopi, released the results of the phase II.
The trial enrolled 135 patients, of which 64 were found to be HLA-A2+. These
patients received Tedopi while the HLA-A2 negative patients served as observation.
Hence, Tedopi was used as a second-line treatment in this phase II trial. The
primary endpoint was the comparison of overall survival and secondary endpoints
included progression-free survival and T-cell response to vaccine epitopes.
Tedopi has already been developed in two phase I/II clinical trials and one phase II trial for NSCLC patients.
The therapeutic vaccine showed a strong overall survival threshold.
We think that neoantigen vaccines are more promising treatments than Tedopi but early-stage

OSE Immunotherapeutics Buy TP EUR 9.00
19 keplercheuvreux.com
Tedopi was well tolerated during the trial, with no significant adverse events
observed in hematopoietic, gastrointestinal, ocular, or neurological functions.
Table 5: Overview of phase II results of Tedopi
Arm Number of patients
Median survival (months)
p-value 1- year survival
p-value Response rate (CR&PR)
HLA-2 + 64 17.3 not significant (p=0.063)
59% not significant (p=0.089)
3%
HLA-2 - 72 12 49% n.a.
Source: OSE Immunotherapeutics
Longer survival was associated with a higher number of positive responses to
epitopes in the HLA-A2+ arm. Hence, patients responding to 0 or 1 epitope had an
overall survival of 406 ± 58 days. Those responding to two or three epitopes had a
median survival of 778 ± 72 days, and those responding to four to five epitopes had a
median survival of 875±67 days. Nearly 85% of the tested patients responded to at
least two epitopes and 64% of the population responded to at least three epitopes,
39% to four or more, and 18% to five or more out of ten.
Even though OSE Immunotherapeutics did not reach the primary endpoints, the
company decided to pursue the work done by Epimmune for the following reasons:
HLA-2 positive is an unfavourable survival prognosis (Nagata et al, 2009). According to So et al, its expression in NSCLC is likely to be one of the mechanisms of escape from immune surveillance. Hence, OSE Immunotherapeutics suggest the phase II results may have met its primary endpoint if both arms had been HLA-2 positive.
A 17.3-month median survival rate is an extended lifetime in late-stage cancer (stage III/IV). To consolidate this argument, OSE Immunotherapeutics emphasised that advanced metastases represented 67% of HLA-2+ group population which is a poor prognosis of disease.
A sub-analysis demonstrated potential interest for patients presenting brain metastasis, a poor survival prognosis.
Long-term survival was also very interesting, with a 59% survival rate at one year
and a 25% survival rate at four years. While the five-year survival rate for stage IV
patients is 1% and 5% for stage IIIb, the overall response rate was only 3% (two
partial responses).
Meanwhile, it seems that Tedopi does not shrink the size of the tumour, contrary
to current CKIs, but it manages to control the evolution of metastasis.

OSE Immunotherapeutics Buy TP EUR 9.00
20 keplercheuvreux.com
Chart 13: Overall survival of HLA-A2–positive patients who received vaccines
Source: OSE Immunotherapeutics
That said, we bear in mind the controversial phase II design trial due to:
1. The selected patient population: HLA-2 positive versus HLA-2 negative patients non homogenous, contrary to what was designed in phase III.
2. Tedopi being used as a 2L therapy and not compared with a controlled active arm (e.g. in replacement of Taxotere).
3. The tiny sample of population in the phase II (n=135), of which 64 were in the active arm.
Hence, we question the capacity of OSE Immunotherapeutics to reproduce the
promise seen in phase IIb.
Despite these question marks, OSE Immunotherapeutics planned to launch a phase
III trial including only HLA-2 patients.
What needs to be proved in phase III? First, some definitions:
Progression-free survival (PFS): Time from random assignment until death or first documented relapse, categorised as either locoregional (primary site or regional nodes) failure, distant metastasis or death.
Overall survival (OS): The percentage of people in a study or treatment group who remain alive for a certain period of time after they started treatment of the disease.
Hazard ratios (HR): The ratio of the hazard rate in one group (e.g. a group of treated patients) to the hazard rate in another group (e.g. an untreated control group of patients). The hazard rate is the probability of a specified event, such as death or cancer recurrence, occurring during a short time interval. The hazard ratio, therefore, is a measure of the relative probability of an event occurring at any given point in time.
ORR (overall response rate): ORR is defined as the proportion of patients who achieve a complete or partial response against a clinical trial treatment.
Survival functionCensored
Time survived (days)
Cu
mu
lati
ve
su
rviv
al
1.0
0.8
0.6
0.4
0.2
0200 400 600 800 1,000
The design of phase II may jeopardise the reading of the results

OSE Immunotherapeutics Buy TP EUR 9.00
21 keplercheuvreux.com
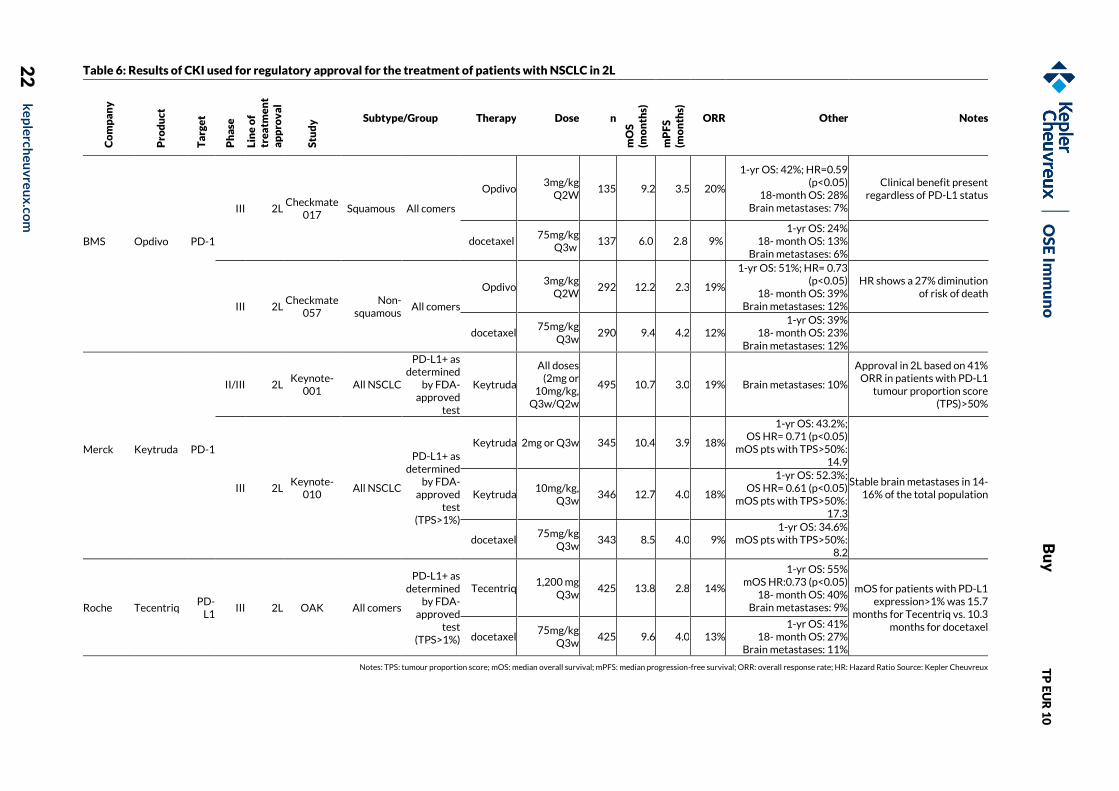
Comparison with current checkpoint inhibitors Checkpoint inhibitors targeting the immune escape system from tumours are now
considered as the standard of care for the treatment of second line NSCLC after
progression with chemotherapy (e.g. docetaxel).
Opdivo from BMS (March 2015) and Keytruda from Merck (October 2015), two anti
PD-1, and one anti PD-L1 Tecentriq from Roche (October 2016) received all the
approvals in second line, leading to a fierce competitive environment.
These nodes were allowed thanks to a significant demonstration of the overall
survival benefit we highlight below.
OS
E Im
mu
no
B
uy
T
P E
UR
10
22
k
ep
lerch
eu
vre
ux
.com
Table 6: Results of CKI used for regulatory approval for the treatment of patients with NSCLC in 2L
Co
mp
an
y
Pro
du
ct
Ta
rge
t
Ph
ase
Lin
e o
f tr
ea
tme
nt
ap
pro
va
l
Stu
dy
Subtype/Group Therapy Dose n
mO
S
(mo
nth
s)
mP
FS
(m
on
ths)
ORR Other Notes
BMS
Opdivo
PD-1
III 2L Checkmate
017 Squamous All comers
Opdivo 3mg/kg
Q2W 135 9.2 3.5 20%
1-yr OS: 42%; HR=0.59 (p<0.05)
18-month OS: 28% Brain metastases: 7%
Clinical benefit present regardless of PD-L1 status
docetaxel 75mg/kg
Q3w 137 6.0 2.8 9%
1-yr OS: 24% 18- month OS: 13%
Brain metastases: 6%
III 2L Checkmate
057 Non-
squamous All comers
Opdivo 3mg/kg
Q2W 292 12.2 2.3 19%
1-yr OS: 51%; HR= 0.73 (p<0.05)
18- month OS: 39% Brain metastases: 12%
HR shows a 27% diminution of risk of death
docetaxel 75mg/kg
Q3w 290 9.4 4.2 12%
1-yr OS: 39% 18- month OS: 23%
Brain metastases: 12%
Merck
Keytruda
PD-1
II/III 2L Keynote-
001 All NSCLC
PD-L1+ as determined
by FDA-approved
test
Keytruda
All doses (2mg or
10mg/kg, Q3w/Q2w
495 10.7 3.0 19% Brain metastases: 10%
Approval in 2L based on 41% ORR in patients with PD-L1
tumour proportion score (TPS)>50%
III 2L Keynote-
010 All NSCLC
PD-L1+ as determined
by FDA-approved
test (TPS>1%)
Keytruda 2mg or Q3w 345 10.4 3.9 18%
1-yr OS: 43.2%; OS HR= 0.71 (p<0.05)
mOS pts with TPS>50%: 14.9
Stable brain metastases in 14-16% of the total population Keytruda
10mg/kg, Q3w
346 12.7 4.0 18%
1-yr OS: 52.3%; OS HR= 0.61 (p<0.05)
mOS pts with TPS>50%: 17.3
docetaxel 75mg/kg
Q3w 343 8.5 4.0 9%
1-yr OS: 34.6% mOS pts with TPS>50%:
8.2
Roche Tecentriq PD-
L1 III 2L OAK All comers
PD-L1+ as determined
by FDA-approved
test (TPS>1%)
Tecentriq 1,200 mg
Q3w 425 13.8 2.8 14%
1-yr OS: 55% mOS HR:0.73 (p<0.05)
18- month OS: 40% Brain metastases: 9%
mOS for patients with PD-L1 expression>1% was 15.7
months for Tecentriq vs. 10.3 months for docetaxel
docetaxel 75mg/kg
Q3w 425 9.6 4.0 13%
1-yr OS: 41% 18- month OS: 27%
Brain metastases: 11%
Notes: TPS: tumour proportion score; mOS: median overall survival; mPFS: median progression-free survival; ORR: overall response rate; HR: Hazard Ratio Source: Kepler Cheuvreux

OSE Immunotherapeutics Buy TP EUR 9.00
23 keplercheuvreux.com
Keytruda have shown higher amplitude of difference versus OSE
Immunotherapeutics in overall survival in the Keynote-010 based on TPS> 50%.
Hence the OS was 17.3 months in the highest dose-range arm versus 8.2 months in
the compared arm. The overall response rate is much higher in the CKI arms than in
the phase II study including Tedopi.
Usually, regulatory agencies (FDA and EMA) focus on the comparison of OS for
the approval of oncology drug candidates. But it is worth notice that all recent
CKI approvals were also based on the partial/complete response rate and the
duration of response (the percentage of patients whose cancer shrinks or disappears
after treatment).
A meta-analysis of ORR, PFS and OS in advanced NSCLC trial (Blumenthal et al)
realised by the FDA, recently showed a patient-level association between response
and PFS and OS and a trial-level association between ORR and PFS, but not OS.
Accordingly, FDA guidance suggests that PFS is not well-correlated with overall
survival (OS) in NSCLC. OS is increasingly the gold standard with regulators and IO
companies – Roche developing Tecentriq has stated that it thinks it is the strongest,
most reliable endpoint in PD-L1 trials, and the one most likely to show the true
measure of patient benefit.
Therefore, we think Tedopi will need to show similar mOS while reaching
statistical significance versus the controlled arm in its phase III trial in order to get
the nod from the regulatory agencies.
Atalante 1: the phase III pivotal trial OSE Immunotherapeutics started the pivotal phase III Atalante 1 trial in January
2016. The design of the trial was approved by both the FDA and EMA in June 2014.
The primary endpoint is overall survival at two years and secondary endpoints
include PFS, ORR, tolerance and quality-of-life. OSE Immunotherapeutics expect to
enrol 500 patients across the US (20% of patient inclusion) and Europe (80% of
patient inclusion). Preliminary results are expected in 2018.
In case of positive results, the company expect a regulatory filing in 2019 both in
the US and in Europe.
The design of the study aims to show survival benefits versus Taxotere in second-
line or in third-line in the event of the use of a CKIs in second line.
This is an important difference compared to what was realised during phase II as
Tedopi was used as a second line therapy following chemotherapy.
The location countries will be the following: United States, Czech Republic, France,
Germany, Hungary, Italy, Poland, Spain, and the United Kingdom. As most of the
patients in US and EU5 countries will receive CKI, which is the new standard of
care for NSCLC, we expect the product will be injected following a CKI treatment
except in central and eastern European countries. Hence, we expect a final
regulatory labelling closer to a 3L following the use of a CKI rather than in 2L. It
also means that Tedopi will need to prove a superior effect versus Taxotere in
third line.

OSE Immunotherapeutics Buy TP EUR 9.00
24 keplercheuvreux.com
We bear in mind that PD-L1/PD-1 inhibitors showed a strong one-year OS rate in 2L
trials with a range between 42% to 55% for the PD-L1+ patients in second line,
similar to what was seen with Tedopi (59%) in phase II. Therefore, we consider the
design of the trial to be much more robust, but also significantly more risky for
Tedopi, and we remain cautious on the probability of clinical and commercial
success for the candidate.
To NSCLC in monotherapy…and beyond? Strategic approaches to oncology research targets:
The immune system through immuno-modulators.
The tumour itself (through radiotherapy, chemotherapy and tumour-targeting therapies).
So far, systemic treatments have associated immuno-modulators with treatment
targeting the tumours. However, this has raised some concerns as scientists gain a
better understanding of the tumour microenvironment.
The main issue in immuno-oncology is the ability of tumour cells to activate a
defence mechanism through the active CKIs of the immune-response. Inhibitors of
those checkpoint blockades allow the immune-response against cancer cells to be
restored. However, the complexity and heterogeneity of tumours, and their ability
to develop resistance to single-agent treatments, have fuelled research into
immunology combination therapy for cancer.
A second issue is the weak immunogenicity of tumours, as they are derived from the
body’s own cells. This is true with NSCLC, which is renowned for its weak immunity.
Overcoming resistance and restoring a functional immune surveillance system
requires the leveraging of multiple, complementary mechanisms of action and
agents that act in multiple phases of the cancer-immunity cycle.
The emerging scientific and clinical consensus is that in the future patients will
require both approaches to:
Generate a targeted immune response (e.g. through cancer vaccines like Tedopi).
Disrupt the checkpoint blockade (PD-1/PD-L1) and enhance the activity of activated T cells (OX-40 agonist).
Lower the tumour-associated microenvironment down regulating effect (e.g. with Effi-Dem).
Mechanisms of defence of tumour cells lead to IO treatment failures

OSE Immunotherapeutics Buy TP EUR 9.00
25 keplercheuvreux.com
Chart 14: Rationale for Tedopi and checkpoint inhibitor combination
Source: OSE Immunotherapeutics
Combinations have the potential to address different escape and activation
mechanisms. It is widely thought that these combination therapies based on the use
of cancer vaccines and checkpoint inhibitors could significantly expand the
effectiveness of immuno-oncology by:
Targeting complementary pathways.
Establishing synergistic effects.
Overcoming resistance to monotherapy.
Having a long-lasting effect.
Improving the risk- benefit profile of administered treatments.
In the past, immunotherapy was used primarily as an adjunct to radiotherapy,
chemotherapy or as a complement to surgical resection; however, the new
combination treatments are expected to become the new standard of care for the
treatment of cancer.
OSE Immunotherapeutics is currently preparing a combination study between
Tedopi and a CKI with a launch planned in H2 2017/early 2018. The company expect
to sign a scientific agreement to co-develop Tedopi with a CKI developer partner.
We expect this partner to be one of the marketed owners of CKI meaning BMS
(Opdivo), Merck &Co (Keytruda) or Roche (Tecentriq).
There is a rationale behind combining Tedopi with a CKI. Therefore, we believe the
future development of combination represents a significant upside opportunity
for OSE Immunotherapeutics in the life-cycle-management of Tedopi.
Other potential prospects Tedopi may potentially show efficacy in other tumours, in particular the non-
immunogenic one, also called cold tumour. Hence, in the event of failure in NSCLC,
OSE Immunotherapeutic may orientate its candidates towards cancers such as
pancreas or bladder cancers. The company has not disclosed any development plans
for now.
Activation of tumour-specific T cells
Tumour elimination
Tumour cell
Tumour cell CD80CD86
CD80CD86
CD28
CTLA-4
T cell
Epitope
Costimulatory Signal 2
Activation of tumour-specific T cells
Cell inhibition
Tumour cell
Tumour cell CD80CD86
CD80CD86
CD28
CTLA-4
T cell
Epitope
Costimulatory Signal 2
PD-1 T cells traffic to tumour
PD-1 PD-1PD-L1 PD-L1
Combinations key to successful treatment of cancer

OSE Immunotherapeutics Buy TP EUR 9.00
26 keplercheuvreux.com
Effi-DEM: the future immune-oncology blockbuster?
.
Myeloid-derived cell modulation holds promise Recently approved immune-modulator for the treatment of cancer primarily
explored the T-cell mechanisms corresponding to the adaptive immune system. It
has shown a durable control cancer in some patients by manipulating T cells with
checkpoint inhibitors (primarily PD-1/PD-L1) or co-stimulatory signals (OX-40).
Some of the agents covering these pathways became notorious blockbusters, such
as Opdivo from BMS or Keytruda from Merck&Co.
However, the benefit of these T cell modulating therapies only benefit a small number
of patients, as only 15% of patients respond to these modulators (e.g. checkmate-459
study with Opdivo in NSCLC). Hence, different checkpoints are utilised by different
cell types that contribute to the potency of anti-tumour immune response. Each
tumour being individualised, different tumours utilise different checkpoints.
Since the emergence of immune-therapy as a new paradigm with which to
treat cancer, the large pharmaceutical companies have focused on a small
number of checkpoint inhibitors mainly present in the cancer cells/effector T cells’
(CD8+) interaction.
Chart 15: Fierce competition in the Tumour/T cell checkpoint blockade
Source: Compugen
Effi-DEM is a preclinical candidate targeting the CD47/SIRPα interaction
between myeloid-derived cells and cancer cells. Also, although not yet clinically validated and based on scientific literature and
preclinical date delivered by OSE Immunotherapeutics, we believe targeting the SIRPα CKIs is promising.

OSE Immunotherapeutics Buy TP EUR 9.00
27 keplercheuvreux.com
Today, non-effector cell mechanisms such as myeloid cells are at the forefront of
research to explore new pathways to decrease relapse of tumours and enhance
the response rate for non-responding patients.
Hence, modern tumour immunotherapy is likely to consist of an association between
T cell modulators to release their brake (e.g. PD-1/PD-L1) and an inhibitor of the
suppressive cells in the tumour microenvironment.
OSE Immunotherapeutics aims to develop next-generation CKI targeting myeloid
cells (tumour associated macrophage (TAMs) and myeloid-derived suppressor cells
(MDSCs)) by binding the SIRPα/CD47 interaction.
Chart 16: T-cell effector mechanism for checkpoint (e.g.
Keytruda/Opdivo)
Chart 17: Non effector cell mechanisms (e.g. Effi-DEM)
Note: Non-exhaustive list of MOA Source: Kepler Cheuvreux, adapted from BMS Note: Non-exhaustive list of MOA Source: Kepler Cheuvreux, adapted from BMS
CD47 is shown to overexpress in almost all human cancers examined to date and its
high expression is associated with a poor prognosis of cancer survival.
A very large body of robust preclinical data and early clinical data indicate
CD47/SIRPα pathway as a very promising immuno-oncology target with PD-1-like
potential for treating a broad range of cancers. The solid science and substantial
potential of CD47/SIRPα-targeting have attracted significant industry interest.
Multiple CD47-targeting agents are in development from early discovery to
Phase 1 stage.
Tumour promotion by myeloid-derived cells Macrophages as effector cells
Macrophages are a type of white blood cell typically broken down into two subtypes
depending on their role in either healing (M2) or immune function (M1).
Macrophages are found in tissues throughout the body, but they originate from
monocytes that enter the tissue from blood vessels when damage is incurred by
surrounding cells.
In a classic immunologic model, M1 macrophages carry out their immune function by
recognising foreign pathogens, engulfing them in a process known as phagocytosis
and initiating a cascade of chemical signals that promote inflammation and recruit
the adaptive immune system. Healing macrophages, classified as M2 macrophages,
typically arrive two days after the initiation of an immune response to decrease
T cellActivating checkpointCD137GITROX40
Inhibitory checkpointCTLA4PD1/PDL1Lag3
Inhibitory checkpointCD73CSF1RIDOCTLA4SIRa
RegulatoryT cell
Tumour associated macrophage Dendritic cell
(APC

OSE Immunotherapeutics Buy TP EUR 9.00
28 keplercheuvreux.com
inflammation, increase the formation of new blood vessels, and facilitate tissue
following the elimination of pathogens.
Role of myeloid suppressive cells
Experimental studies indicate that myeloid cells modulate key cancer-associated
activities, including immune evasion, and affect virtually all types of cancer therapy.
Myeloid suppressive cells, including tumour associated macrophages (TAM/M2
macrophage) and myeloid-derived suppressor cells (MDSC), represent an abundant
immune cell type in the microenvironment of solid tumours, where they promote
tumour growth, metastases, angiogenesis, inhibiting anti-tumour immune responses.
Normally, common myeloid progenitor (also called immature myeloid cells) migrate
to different peripheral organs, where they differentiate exclusively into dendritic
cells and macrophages type M1 or polymorphonuclear cells (also named
granulocytes). However, several factors produced in many pathological conditions
promote the accumulation of immature myeloid cells, prevent their differentiation
and induce their activation. These cells exhibit immunosuppressive functions after
activation and were named MDSC (Gabrilovich et al, 2007).
According to the literature, MDSC reduce activated T-cell number and inhibit their
function by multiple mechanisms including depletion of L-arginin by arginase-1
(ARG1), production of NO (nitric oxide).
The second category of myeloid cells, called TAMs, is found to be involved in almost
all of the tumour development pathways:
Tumour cell proliferation.
Angiogenesis (formation of cancer vessels).
Tumour cell invasion.
Immunosuppression.
TAMs cells play an important role in tumour progression

OSE Immunotherapeutics Buy TP EUR 9.00
29 keplercheuvreux.com
Chart 18: The role of myeloid cells in cancer
Source: Engblom et al, 2016
Therefore, there is a certain rationale behind the development of TAM and MDSC
checkpoint inhibitors due to the following reasons:
TAMs and MDSCs are immunosuppressive and act by inhibiting CD8 T cell responses while enhancing recruitment and differentiation of regulatory T cells or Tregs.
TAMs and MDSCs are often correlated with a poor prognosis in cancer patients.
Consequently, targeting myeloid cells could overcome the limitations of current
treatment options, whose activity is inhibited by myeloid-derived cells.
Mechanism of action of Effi-DEM Effi-DEM has a dual effect. It operates through macrophages (innate immune
system) and may exert downstream effects on the adaptive immune system (T cells)
in the tumour environment. Hence, it presents a competitive advantage by acting
on both the adaptive and innate immune systems.
Reactivation of macrophages
Myeloid cells selectively express SIRPα, an immune tyrosine associated inhibitory
receptor (also named CD172a), which controls myeloid functions.
The ligand of SIRPα is CD47. CD47 is expressed in almost all normal human cells. In
case of tumour, it may be an up-regulation of CD47 which leads to several adverse
effects for the immune-control of the tumour. Expression of CD47, and its
interaction with SIRPα, leads to the inhibition of macrophage activation and protects
cancer cells from phagocytosis (the macrophage aims to “eat” the cancer cells).
Therefore, it allows cancer cells to proliferate. Hence, CD47 send a “don’t eat me”
signal to the patrolling macrophages type M1, which is being bound by EFFI-DEM.

OSE Immunotherapeutics Buy TP EUR 9.00
30 keplercheuvreux.com
Chart 19: SIRPα inhibitor (Effi-DEM) allow phagocytosis to be reactivated
Source: Trillium Therapeutics
Reactivation of T cell functions while blocking MDSC/TAMs
TAMs and MDSCs are an important component of the tumour microenvironment
and play a major role in creating the immunosuppressive environment that enables
tumour development. Blocking SIRPα allow MDSCs to differentiate into non-
suppressive tumour cells. According to the literature, it also promotes human
subtype M1 macrophages, which has antitumour effects (pro-inflammatory), while
decreasing the M2 subtype (pro-tumoural effect)
Hence, Effi-DEM may be a first-in-class product tackling myeloid suppressive cells
(MDSC, TAM) while promoting macrophages phagocytosis and therefore dendritic
cell function.
Chart 20: Mechanism of action of Effi-DEM
Source: OSE Immunotherapeutics
The myeloid cell modulation: a hotspot in the biotech space We emphasised that Effi-DEM may be a first-in-class product targeting the SIRPα
receptor. However, there are several players already involved in early-stage
development of inhibitor of its ligand CD47. While in our knowledge no other

OSE Immunotherapeutics Buy TP EUR 9.00
31 keplercheuvreux.com
company target the SIRPα ligand, several anti-CD-47 are being studied by other
biotechnology companies.
Table 7: Competitive environment for Effi-DEM in CD47/ SIRPα pathway
Company Indication Drug Development stage
Note
Celgene/Inhibrx Hematologic malignancies
CC900002 (CD47 mAb) Phase I Celgene acquired CC900002 from Inhibrx for a USD500m deal size in 2012
Trillium Therapeutics Hematologic malignancies
TTI-621(CD47 mAb) Phase I Listed company MC: c. CAD55m
Stanford University Solid tumours CD47 mAb Phase I Tioma Therapeutics Cancer Anti CD47 mAb Pre-clinical Raised USD86m in series A financing in August
2016 led by Novo Venture, Roche and GSK Venture arms
Alexo Therapeutics Cancer SIRPα variants that antagonise CD47 Pre-clinical Raised USD36m in a Series A in May 2015 led by venBio
Forty Seven Hematologic malignancies
Hu5F9-G4, humanised anti- CD-47 mAb Phase I Raised USD75m is a series A in February 2016
Novimmune B-Cell leukaemia/ lymphoma
NI1701 (bispecific CD19xCD47) Pre-clinical Privately-held Swiss biotech founded in 1998
Source: Kepler Cheuvreux
CD47 topic is currently a hotspot in the biotechnology industry. According to data
pooled with EvaluatePharma, FortySeven and Tioma Therapeutics, series A funding
has been among the top ten for a decade in the oncology space (based on a sample of
429 companies).
Competitive advantage versus current CD47 inhibitor
One main difference between both approaches is the targets. CD47 is present in the
tumour while SIRPαis particularly abundant in the myeloid cells. The difference of
location allows Effi-DEM to act on the innate immune function by activating the
phagocytosis and priming the adaptive immune response through the blockade of
MDSCs immunosuppressive function.
Additionally, one major advantage is the selectivity of Effi-DEM for SIRPα. While
CD47 has other binders than SIRPα, which may lead to several off-target effects,
SIRPαsolely binds CD47. Hence, according to OSE Immunotherapeutics, a better
safety clinical profile of Effi-DEM may result from this particular selectivity.
Indeed, CD47 is found in almost all healthy cells, notably red blood cells. CD47 can
interact with the secreted protein thrombospondin-1 (TSP1), in addition to SIRPα
(Expert Opin Ther Targets 2013). Upon binding to TSP1, CD47 transduces signals
that alter cellular calcium, cyclic nucleotide, integrin, and growth factor signalling
and control cell fate, viability, and resistance to stress.
Hence, targeting CD47 is likely to induce potential side effects including altered
blood pressure (Bauer et al, 2010), haemolytic anaemia, and prothrombotic or
antithrombotic activities (Isenber et al, 2008). Another potential side effect which
may be lower by selectively binding SIRPα, is the abundance of CD47 in red blood
cells. This is important, as targeted therapies for CD47 have been found to induce
anaemia and get lower bio-distribution. Hence, the therapeutic window for anti-
CD47 is particularly low.
Effi-DEM is likely to show a better safety profile than peers

OSE Immunotherapeutics Buy TP EUR 9.00
32 keplercheuvreux.com
Safety concerns about anti-CD47 have been recently emphasised through the
drop in the share price of Trillium Therapeutics. On 2 November 2016, Trillium
saw a 52% pullback after its ASH abstract revealed cases of liver toxicity and
thrombocytopenia in the highest dose of 0.3mg/kg in TTI-621’s phase I dose-
escalation trial.
Due to its original mechanism of action, we are enthusiastic about the prospect of
Effi-DEM.
Effi-DEM: an IO blockbuster candidate? So far, OSE Immunotherapeutics has released pre-clinical datasets that have
demonstrated the ability of Effi-DEM to inhibit breast cancer growth in
monotherapy. The company used animal models (murine) to carry out these
preliminary tests.
Chart 21: Inhibition of breast cancer growth (1)
Chart 22: Inhibition of breast cancer growth (2)
Source: OSE Immunotherapeutics Source: OSE Immunotherapeutics
The company has also shown a synergistic effect with an anti PD-L1 antibody in
melanoma and HCC (hepatocarcinoma) as well as a big effect with 4-1BB (co-
stimulatory molecule for T cell) in HCC.
Chart 23: Synergy with PD-L1
Chart 24: Synergy with 4-1BB agonist
Source: OSE Immunotherapeutics Source: OSE Immunotherapeutics
CTRL Ab (n=16)aSIRPa (n=13)
Days
Tu
mo
ur
vo
lum
e(m
m3)
1,500
1,250
1,000
750
500
250
0 5 10 15 20 25 30 350
Control Ab Anti-SIRPa
Week 4
Tu
mo
ur
vo
lum
e
(mm
^3
)
P< 0.01
80
60
40
20
0
800
600
400
200
0
300
200
100
0
1,500
1,000
500
0
Tu
mo
ur
vo
lum
e
(mm
^3
)
Tu
mo
ur
vo
lum
e
(mm
^3
)
Tu
mo
ur
vo
lum
e
(mm
^3
)
Control Ab Anti-SIRPa
Control Ab Anti-SIRPaControl Ab Anti-SIRPa
Week 5
Week 2 Week 3
P< 0.01
P< 0.001 P< 0.05
Ctrl Ab
SIRPa Ab
Time (days)
Pe
rce
nt
surv
iva
l
100
80
60
40
20
0 10 15 20 25 30 35 400
PD-L1 Ab
Combination
5
CTRL AbaSIRPa
Days
Pe
rce
nt
surv
iva
l
100
80
60
40
20
0 10 20 30 40 50 60 700
4-1BB AbCombinationP < 0.05 P < 0.01

OSE Immunotherapeutics Buy TP EUR 9.00
33 keplercheuvreux.com
We think SIRPαmay reveal its potential with such a combination as there is a
rationale to target both the innate and the immune system to avoid immune escape
mechanisms.
Thanks to these positive preclinical data, OSE Immunotherapeutics expects to
enter into clinical by the end of 2018.
That being said, we highlight specific risks that may arise as part of the development
of Effi-DEM:
The CD47/SIRPα pathway is not yet a clinically validated target. Clinical safety concern arised from Trillium Therapeutics following the phase I update, while efficacy data has not yet been released.
Effi-DEM is far from the cusp to reach clinical-stage status as it plans to enter clinical stage in H2 2018; besides, other competitors may arise from there.
While Effi-DEM may limit the safety issue of CD47 inhibitors, OSE Immunotherapeutics did not release any preclinical safety data and there is no evidence that the CKIs will enter the clinical stage.
Intellectual property
So far, Effi-DEM has been protected by three families of patents. The first patents
were granted by the European patent office (EPO) in April 2016. A second family is
being examined by the EPO and the filing date was October 2015. Regarding the US,
a first patent application was initiated in May 2016.
Our analysis suggests positive optionality for OSE Immunotherapeutics’ Effi-DEM
programme.
We think Effi-DEM and modulations of MDSCs through SIRPα/CD47 pathway are
still under the radar for most investors in Europe but are a new hotspot in the US.
Despite positive preclinical data, notably in combination, we think investors do not
sufficiently value this early-stage asset.

OSE Immunotherapeutics Buy TP EUR 9.00
34 keplercheuvreux.com
FR104 and Effi-7: already monetised FR104 and Effi-7 are two monoclonal antibodies developed in autoimmune
diseases. Both assets have already been out-licensed to partners by OSE
Immunotherapeutics.
FR104 has been partnered with J&J, providing a EUR10m opt-in option
payment to OSE Immunotherapeutics in July 2016. In the event of clinical
success, FR104 is likely to become a blockbuster with strong activity both in
rheumatology as well as in transplant complication management. FR104 is no
longer a source of cost but, conversely, a cash inflow opportunity for OSE
Immunotherapeutics. Indeed, J&J, following its opt-in options, will fund all
development costs starting from now. Therefore, FR104 is a potential source
of cash-in for OSE Immunotherapeutics.
OSE Immunotherapeutics secured EFFI-7 through an out-license deal with
Servier in December 2016 with an opt-in option after the completion of phase II.
Funding until phase II is also partly secured thanks to a consortium led by OSE
Immunotherapeutics.
We believe these two assets will provide sufficient funding to the company to
finance EFFI-DEM development, therefore significantly derisking the profile of
OSE Immunotherapeutics.
FR104: a ground-breaking opportunity in autoimmune diseases
The role of Treg cells Accumulating scientific data demonstrate that regulatory T-cells (Treg), a
subpopulation of CD4+ T-cells, play an important role in dampening the immune
response. Treg cells appear to suppress the action of other T-cell subsets by a number
of mechanisms. Suppression by Treg is thought to involve the anti-inflammatory
cytokines IL-10 and transforming growth factor beta (TGF-β). Reduced expression of
both molecules, as well as decreased proliferation of the regulatory CD4+ T-cell
subsets producing IL-10, have been demonstrated in RA patients.
Thus, there is a scientific rationale for the use of Treg for the treatment of RA, as it
might allow the T-cell homeostasis to be maintained.
FR104 modulates Treg to enhance autoimmune conditions.
FR104 is developed primarily in rheumatoid arthritis.
FR104 has been out-licensed to J&J, which exercised its opt-in option in July 2016 triggering EUR10m to OSE Immunotherapeutics.
OSE Immunotherapeutics is entitled to receive up to EUR155m in additional payments.

OSE Immunotherapeutics Buy TP EUR 9.00
35 keplercheuvreux.com
Mechanism of action FR104 is a new drug candidate, a pegylated monoclonal antibody fragment inhibitor
of CD28, an essential element of the T-cell signalling pathway. CD28 (cluster of
differentiation) is a costimulatory receptor involved in the CD28/B7/CTLA-4
signalling pathway which balances the immune response to external agents. The
current paradigm holds that CD28 T cell expression (T cell CD4+ or Treg) binds
CD80/86 to provide a co-stimulatory signal that is important for sustaining T-cell
activation. This pathway is involved in the effector T cell expansion and the Treg
inactivation.
According to the literature (Poirier et al, 2010), although CD28 signals are critical
for Treg homeostasis and thymic generation, CD28 engagement by CD80/86
molecules inhibits Treg suppressive activity.
FR104 exerts its immunomodulatory function by blocking CD28 signalling and
preventing effector T cells but not regulatory T cell function, thereby promoting
immune tolerance.
Chart 25: Mechanism of action of FR104
Source: OSE Immunotherapeutics
This approach is markedly different to the current treatment, which targets the
CD80/86 ligands (Nulojix and Orencia from BMS). CD80/86-specific blocking
strategies also inhibit CTLA-4 signals crucial to the suppressive function of Tregs, as
well as the CD80-mediated signals that have a role in the induction of adaptive Tregs
(Perez et al, 2008). Also, the likelihood of inhibiting significant physiological
regulatory pathways seems higher while blocking the CD/80/86 pathway rather
than CD28. Hence, theory suggests a better clinical efficacy and safety profile of
FR104 compared to competitors.
FR104’s closest peers are Nulojix and Orencia from BMS

OSE Immunotherapeutics Buy TP EUR 9.00
36 keplercheuvreux.com
Chart 26: Costimulatory molecules and biological pathways implicated in the targeting of B7s
versus CD28
Source: Porier et al, 2010t
CD80/86 inhibitors, which act both on CD28 and CTLA-4 co-stimulatory pathways,
also have an effect on PDL-1 inhibitory signals of T lymphocytes. These multiple
involvements have led to observe several side effects in approved CD80/86 ligand
inhibitors. Hence, Nulojix from BMS is believed to be involved in a higher incidence
of early transplant rejection compared to current standards of care, which are the
CNI (calcineurin inhibitors) such as commonly used cyclosporine.
J&J: a landmark partner for FR104
Deal with J&J FR-104 candidate was the fruit of a research and discovery carried out by both
Effimune and the French public institute Inserm. In October 2013, Effimune entered
into an option deal with J&J for the development and commercialisation of FR104.
In July 2016, based on the safety profile demonstrated in the phase I, J&J decided to
raise its option for FR104. Under the terms of the agreement signed in 2013, J&J is
responsible for all clinical development, registration and commercialisation of
FR104. The spectrum of indication covers the autoimmune disease and transplants.
The exercise of the option triggered a EUR11m payment to OSE
Immunotherapeutics. The biotech is also eligible to receive up to EUR155m
milestone payments as well as royalties on future sales that we estimate in the
high-single-digit range.
We think the out-licensing of FR104 will provide a cashflow stream to OSE
Immunotherapeutics, allowing the company to develop other internal programmes.
Patent protection There are currently four patent families for FR104, and these patents are registered
in Europe, the US, and Japan.

OSE Immunotherapeutics Buy TP EUR 9.00
37 keplercheuvreux.com
Table 8: FR104 intellectual property
Applicant Filing date Expiry date Status
Family 1 Inserm 2001 2021 Granted: Europe, US, Japan Family 2 Inserm and OSE Immunotherapeutics 2010 2030 Granted: Japan; being examined: US; abandoned: Europe Family 3 Inserm and OSE Immunotherapeutics 2010 2030 Granted: US, Europe Family 4 Inserm and OSE Immunotherapeutics 2011 2031 Granted: US; being examined: Europe, Japan
Source: OSE Immunotherapeutics
Based on current granted patents, in the core US, Japan and European territories,
FR104 is protected until 2031, meaning that no biosimilar should reach the market
before then.
Besides its patent application in core territories, OSE Immunotherapeutics has also
filed application to the patent cooperation treaty to expand its patent protection.
FR104: looking to grab a piece of the large RA market
Rheumatoid arthritis in a nutshell Rheumatoid arthritis (RA) is the most common autoimmune inflammatory arthritis
in adults. It causes premature death, disability, and lowers the quality of life.
According to WHO, over 70m people worldwide are estimated to be affected by RA.
RA is a chronic and progressive, systemic autoimmune disorder involving different
pro-inflammatory cytokines. The inflammation usually affects the lining of the joints
(synovial membrane), but can also affect other organs. This inflamed joint lining
leads to erosion of the cartilage and bone and sometimes causes joint deformity.
Pain, swelling, and redness are common joint symptoms. As the disease worsens,
joint inflammation may lead to irreversible bone damage, loss of mobility, and pain.
Chart 27: Rheumatoid arthritis symptoms
Source: Sanofi
According to the NIH, RA affects about 1.3m adults in the US. In the seven
major pharmaceutical countries, around 5.3m patients are affected by the disease.
RA is 2-3 times more common in women than in men, which may be related to
hormonal factors.

OSE Immunotherapeutics Buy TP EUR 9.00
38 keplercheuvreux.com
The causes of RA are unknown, but it is believed to result from a faulty immune
response. RA can begin at any age and causes fatigue and prolonged stiffness after
rest. There is no cure for the disease, but effective drugs are increasingly available to
treat RA and prevent deformed joints.
Rheumatoid arthritis: current treatment available
Depending on the level of severity and how advanced the disease is, several
different types of drug therapies may be used in monotherapy or in combination:
Non-steroidal anti-inflammatory drugs (NSAIDs).
Analgesic drugs.
Corticosteroids.
Disease modifying antirheumatic drugs (DMARDs).
Current standard-of-care first-line treatments for diagnosed RA are conventional
synthetic disease modifying antirheumatic drugs (csDMARDs) sometimes in
combination with glucocorticoids and NSAIDs or analgesic drugs. csDMARDs
include methotrexate (MTX), leflunomide, hydroxychloroquine and sulfasalazine
and are usually the first treatment used for RA and to control inflammation.
However, more than half of people with RA on conventional DMARDs do not adhere
to their treatment (Engel-Nitz NM, et al, 2012) due to side effects. Indeed, side
effects from csDMARDs are unpleasant and include nausea, vomiting and diarrhoea,
mouth ulcers, hair loss and skin rashes.
Chart 28: Classification of DMARDs
Source: Kepler Cheuvreux
Usually, in case of failure or non-adherence to treatments, physicians prescribe
biological DMARDs (bDMARDs) as an add-on or in monotherapy. Current biologics
have a range of modes of action, targeting the many vulnerable nodes in the
inflammatory cascade. Their main advantage is their long-acting action, meaning
Current RA treatments present serious side effects

OSE Immunotherapeutics Buy TP EUR 9.00
39 keplercheuvreux.com
that a patient only needs an injection monthly or bi-monthly. Cytokine-targeting
biologics include TNFα inhibitors, and Actemra, which blocks the IL-6R classic and
trans-signalling pathways. Cell-targeting biologics include Orencia (which inhibits T-
cell activation by antigen presenting cells) and Rituxan (which depletes B cells).
Most The most prescribed biologic is anti-TNFs, and the most widespread biologic
belonging to this class is Humira from Abbvie. Humira is the world’s top-selling anti-
TNF. It reported c. USD16bn in annual sales in 2016, of which c. 40% are dedicated
to the treatment of RA.
In case of failure of the first biologic, the physician is likely to switch to another class
of biologic or to a different anti-TNFα treatment. In case of approval, FR104 is likely
to be positioned as a new competitor in the boDMARDS market.
A trend currently emerging in RA treatment is the use of new biologics in
monotherapy. The recent guidelines from the American College of Rheumatology
(ACR) in 2015, or from the EULAR in 2012, now support newer mechanisms of
action as first-line treatments, along with the current anti-TNFα biological standard
of care. Hence, EULAR, the European League Against Rheumatism, has recently
endorsed IL-6 (e.g.: Actemra from Roche) for its use in monotherapy.
The penetration of biologics still remains limited in the current treatment paradigm.
Around 86% of rheumatoid arthritis patients are diagnosed, of which 70% are
treated in G7 countries. Finally, only 40% of treated patients in G7 countries take
biologics, with a higher market penetration in the US (60%) than in the EU5 and
Japan (30%).
Chart 29: Expected strategy of development of FR104 in the new RA treatment paradigm
Source: Kepler Cheuvreux,

OSE Immunotherapeutics Buy TP EUR 9.00
40 keplercheuvreux.com
We believe that OSE Immunotherapeutics and its partner J&J will first cautiously
develop FR104 as a third-line (3L) therapy in case of failure of an anti-TNFα and
then in monotherapy or in second-line (2L) therapy in combination with an oral
DMARD (primarily methotrexate) to expand their targeted market.
A large, fiercely competitive market under pricing pressure
The market for RA products is expected to slightly increase at a 2% annual growth
rate until 2022, driven by:
An emerging class of tsDMARD: this corresponds to the JAK inhibitor class.
It includes Xeljanz from Pfizer and two late-stage products: filgotinib from
Gilead/Galapagos and baricitinib from Eli Lilly.
Anti-IL6: it includes Actemra from Roche and the two recently regulatory-
filed products, sarilumab, which was rejected in October 2016 by the FDA
(Sanofi/Regeneron) due to manufacturing issues, and sirukumab (J&J).
Chart 30: boDMARDs and tsDMARDs expected market (USDbn)
Note: do not include neither generics nor biosimilar and csDMARDS source: EvaluatePharma
One downside is that RA treatment is likely to decrease after reaching its 2022
peak, as the market for RA treatments and new therapeutic options will be affected
by the uptake of biosimilar products. Biosimilars are a hot topic in the treatment of
RA and autoimmune disease. RA is at the forefront of the use of emerging
monoclonal antibodies.
The main challenge new treatments are likely to face is the need to show that they
offer improved therapeutic value against the current treatment in order to gain
market share in the crowded RA market. Hence, biosimilar treatments will need to
demonstrate that their therapeutic efficacy compares to current standards of care
such as anti-TNFs in order to gain adequate pricing in a tough pricing environment.
For example, Regeneron/Sanofi’s IL-6 inhibitor sarilumab beat AbbVie’s Humira
(adalimumab) in a head-to-head trial in 2016. Top-line Phase III results showed
sarilumab more significantly improved the signs and symptoms of rheumatoid
arthritis after 24 weeks of treatment than Humira.
22.6 25.0
26.5 27.3 27.1 26.7 26.2 25.5
0
5
10
15
20
25
30
35
2015 2016E 2017E 2018E 2019E 2020E 2021E 2022E
Anti TNF Orencia Anti IL-6 JAK inhibitors Others
RA market is large with slight growth expected, driven by new treatment options
OSE Immunotherapeutics Buy TP EUR 9.00
41 keplercheuvreux.com
We think that FR104 will need to perform similar studies in order to prove its
added-value. With no clinical efficacy results demonstrated so far, we remain
cautious on the future development of FR104 in RA. Moreover, positive clinical
outcomes will not necessarily mean great sales, as seen with the relatively low
expectations in the IL-6 pathway.
Opportunity remains for new treatment options in RA Despite the availability of a wide range of biological and oral therapies, patients
continue to experience inadequate responses to current therapies, and new
therapies are needed. According to Felson et al (2011), less than 10% of patients
with RA treated with biologics achieve complete disease remission.
Accordingly, rheumatologists are getting more comfortable and confident with
newer mechanisms of action, and guidelines recommend using biologics (TNF α and
non-TNF α) when patients are not responding to DMARDs. Therefore, we see room
for new candidates in the crowded RA market.
However, we think that FR104 will need to show significant efficacy and a clean
safety profile versus current competition in order to penetrate the market.
Promising first-in-human study In April 2015, Effimune received authorisation from the Belgian authorities to start
a first-in-human study. The study was conducted from March 2015 to February
2016 with 65 healthy subjects. The volunteers received an IV dose of FR104 ranging
from 0.005mg/kg to 0.5mg/kg over a period of nine months. The primary objective
of the trial was to establish the safety and tolerability of FR104 and assess its
pharmacodynamics and pharmacokinetics. This first-in-human trial served to
prepare the filing of the J&J opt-in options and the future development in
rheumatoid arthritis and kidney transplants.
FR104 showed good tolerance with no evidence of cytokine release syndrome and
no impact on the blood lymphocyte system. According to Poirier et al, the relatively
high incidence of immunogenicity for FR104 is similar to what has been reported for
Cimzia, Remicade and Humira.
Competitive environment in CD80/CD28 pathway
FR104 selectively targets the CD28 pathways to inhibit an immune response. RA
candidate boDMARD therapies under development targeting the CD80 and CD28
pathways are:
1. Orencia, an approved therapy developed by BMS in several autoimmune disease indications.
2. Theraluzumab: a phase-I monoclonal antibody belonging to the superagonist antiCD28 class.
3. Lulizumab pegol, a clinical-stage phase-II candidate, currently developed for the treatment of patients with lupus (autoimmune dermatology condition).
4. CGEN-15001, a pre-clinical stage candidate developed in transplantation and graft-versus-host disease.

OSE Immunotherapeutics Buy TP EUR 9.00
42 keplercheuvreux.com
Orencia SC and IV formulation
Orencia (abatecept) is an anti CD80/CD86 agent that has been developed by BMS.
In the past few years, BMS decided to extend the lifecycle of Orencia by launching a
subcutaneous (SC) formulation. Creating a subcutaneous formulation is a common
marketing strategy used by pharmaceutical companies to develop a lifecycle
management of their biologic and provide a differentiation strategy.
Orencia SC (abatecept subcutanea) was approved in 2011 in the US and in 2012 in
the EU, while the IV (intravenous) formulation was launched in 2006. Quickly, the
subcutanea formulation gained market share on the intravenous formulation, as SC
is much more convenient to inject for patients. For 2016, the SC formulation and the
IV formulation are both expected to record USD1.2bn of sales globally (all
autoimmune indications).
Chart 31: Orencia sales (USDbn)
Source: EvaluatePharma
Orencia is often used in patients whose disease is not controlled by TNF antibodies
(like Humira and Enbrel) in accordance with European label specifications. Hence,
we think that the positioning of the product and its similar mechanism of action to
FR104 make it the closest marketed peer and a potential competitor to FR104. We
also note that both biosimilar companies, Mylan and Momenta, have partnered up to
develop a biosimilar version of Orencia called M834 with a plan to first launch in
2020. Therefore, pricing pressure on Orancia is likely to come with the planned
launch of FR104.
Theraluzumab
Theraluzumab (TAB08/TGN1412) is developed by the Russian biotechnology
TheraMAB. Initially, the monoclonal antibody was known as TGN1412 and was
developed by TeGenero until 2006.
Theraluzumab belongs to the class of CD28 superagonists which are CD-28 specific
monoclonal antibodies able to activate T-cells without overt TCR engagement. In a
preclinical study, theraluzumab showed efficiency in activating Tregs and in
modulating autoimmune diseases in several models such as transplantation and
inflammation. However, a phase-I study of theraluzumab in 2006 resulted in a
0.7 0.9
1.2 1.5
1.7 2.0
2.4 2.6 2.7
2.5 2.5 2.4 2.4
0.0
1.0
2.0
3.0
4.0
2010 2011 2012 2013 2014 2015 2016 2017 2018 2019 2020 2021 2022
Orencia Orencia SC

OSE Immunotherapeutics Buy TP EUR 9.00
43 keplercheuvreux.com
cytokine release syndrome (CRS). CRS is a life-threating side effect that occurs as a
result of a high level of immune activation and modulation. Following the failure of
this phase I trial due to the difference in tolerance between human and pre-clinical
models (macaques), TheraMAB resumed development of theraluzumab. The
company initiated a phase I in 2013 at a much lower dose than the 2006 trial (0.1%
dose-level compared to what had been injected). No side effects were observed, and
the company decided to set up phase-II programmes in autoimmune diseases.
Lulizumab pegol (BMS-931699)
Being developed by BMS and is currently in phase II for the treatment of patients
with lupus; results are expected in 2018. The compounds were tested in a phase I
trial whose results were published in 2016 (Shi et al, 2016). The estimated SC
bioavailability was 68.2%. Lulizumab IV or SC was safe at all doses studied, without
evidence of cytokine release syndrome (CRS).
CGEN-15001
CGEN-15001 targets CGEN-15001T, a protein thought to be a member of the
B7/CD28 costimulatory family, according to Compugen, its developer. CGEN-15001
was acquired by Bayer in 2013 under a USD540m deal structure which also
included another immune-oncology programme. The candidate is currently in the
preclinical stage.
Kidney transplant maintenance: the second targeted indication In preclinical development, OSE Immunotherapeutics focused its development both
on autoimmune and transplantation. In transplantation, the main focus was on two
main transplant complications:
1. Maintenance of immunosuppression in kidney transplants.
2. Graft-versus-host disease, which is a complication of hematopoietic stem cell transplantation (HSCT).
Based on the announcement of the phase I results, we see OSE
Immunotherapeutics and its partner J&J developing FR104 firstly in rheumatoid
arthritis and then in kidney transplantation.
Effi-7: already monetised to Servier, the right strategic option?
EFFI-7: a first-in-class mechanism of action IL-7’s role
Interleukins are signal molecules that are secreted by immune cells to drive
messages.
Main role of IL-7’s main role is controlling T-cell homeostasis (maintaining T-cell
equilibrium). It is either secreted into the circulation or presented in solid tissue by a
Effi-7 is a humanised monoclonal antibody against CD127 in preclinical stage. OSE Immunotherapeutics signed a global development deal with Servier in
December 2016 valued at EUR272m. Effi-7 is developed in ulcerative colitis, an autoimmune bowel disease (IBD) with
a large potential.

OSE Immunotherapeutics Buy TP EUR 9.00
44 keplercheuvreux.com
category of cells called stromal cells. The IL-7 receptor (IL-7R) is expressed on
almost all circulating CD4+ and CD8+ T cells and natural killer B cells, but not on
mature B cells or on Treg. Hence, the IL-7 constitutes a relevant target to modulate
T cell response while sparing Treg and mature B cell modulation.
Chart 32: IL-7R expression by lymphocyte
Source: Mackall al, 2011
The IL-7R is composed of an alpha chain (CD127) and a beta chain (CD132).
Effi-7 presents an interesting profile in IBD
IL-7 is now associated with the pathogenesis of RA and other autoimmune
diseases like multiple sclerosis and GI-tract diseases like ulcerative colitis
(Watanabe et al, 1998), sarcoidosis and primary biliary cirrhosis. By blocking the
alpha chain from the IL-7R, Effi-7 has demonstrated potential interest in the
preclinical model of allogenic transplantation and inflammatory bowel diseases
like ulcerative colitis and Crohn’s disease.
OSE Immunotherapeutics has notably demonstrated in preclinical models that
an IL-7R blockade specifically prevents intestinal human T cell infiltration.

OSE Immunotherapeutics Buy TP EUR 9.00
45 keplercheuvreux.com
Chart 33: Mechanism of action of Effi-7
Source: OSE Immunotherapeutics
Therefore, thanks to positive signals from scientific arguments and validated proof
of concept (Belarif et al), OSE Immunotherapeutics has decided to primarily develop
Effi-7 in ulcerative colitis (UC), a type of gastro-intestinal autoimmune disease.
Targeted indication: ulcerative colitis UC is a chronic, inflammatory disease of the large intestine and rectum
characterised by episodes of increased stool frequency and bloody diarrhoea.
Ulcerative colitis is the most common form of inflammatory bowel disease (IBD)
worldwide, along with Crohn’s disease. Ulcerative colitis patients may also
experience extra-intestinal manifestations such as arthritis and dermatological or
ocular manifestations. Moreover, patients have a significant elevated risk of
developing colon cancer.
While the cause is not known, there is a presumed genetic component to
susceptibility as well as environmental triggers for the disease.
A common disease and an expanding large market potential
More than 3.5m people in the US, the EU, and Japan are expected to have IBD.
About one in every 198 people in Europe and and one in every 402 people in North
America has ulcerative colitis. At the time of diagnosis, around 55% patients have a
moderate to severe form of UC. The most common treatment is 5-aminosalicylic
acid (mesalazine). However it is estimated that 40% of patients receiving the
recommended dose of 5-aminosalicylic acid continue to experience persistent
disease activity flares.
Ulcerative colitis (UC) represents a large market of c. USD4bn which is expected to
grow to USD8.5bn in 2022, according to EvaluatePharma.
A highly unmet medical need in moderate-to-severe UC
There is no cure for ulcerative colitis, and most patients require lifelong medication.
The goal of treatment is to induce remission (diminishing of symptoms or symptom
free). If achieved, this is followed by the administration of maintenance medications
to prevent a relapse of the disease. Standard treatment for ulcerative colitis
depends on the extent of colon involvement and disease severity and includes anti-
UC is a very large market: USD8.5bn expected in 2022

OSE Immunotherapeutics Buy TP EUR 9.00
46 keplercheuvreux.com
inflammatory drugs, immunosuppressive drugs, as well as biological therapies such
as anti-TNF (Remicade and Humira). For patients with chronic active UC not
responding to medical therapy, a colectomy is often the only remaining option.
Chart 34: Current marketed UC treatment
Source: Kepler Cheuvreux, adapted from Receptos/Celgene
Due to the large market potential of the disease and the high level of prevalence of UC,
this market has attracted large players, resulting in an increase in competition to
develop new treatment options. In 2014, Takeda launched Entyvio (an integrin
receptor antagonist), approved both in the US and in Europe. The product is on track
to become a blockbuster with EUR0.7bn sales recorded in 2016. However, long-term
efficacy remains questionable although the product has shown a clean safety profile.
Tysabri from Biogen, another integrin receptor antagonist, is often used off-label to
treat ulcerative colitis but with potential brain side effects.
A fierce competition in UC for new treatment options
Due to the attractiveness of the UC market, numerous players are developing new
treatment options. Hence, Effi-7 is likely to enter into a tough competitive
environment, and numerous new treatment options are in late stage, either orally
available or biologically active (SC or IV).
The most advanced developed treatment is ozanimod, an oral treatment, currently
in phase III and developed by Celgene. This asset was acquired following the
USD7.2bn acquisition of Receptos in July 2015. Celgene seeks to position ozanimod
ahead of anti-TNF in the UC treatment paradigm.
Most of the new drug options in later stages of the pipeline are orally administered
drugs, unlike Effi-7, which is an IV treatment. While their place in the clinical
armamentarium remains to be proven, it is likely that many of oral drugs will find
their place in the treatment algorithm of UC in the next few years. Thus, we think
that Effi-7’s greatest challenge will be to prove superior efficacy and a clean safety
profile against more convenient orally administered treatments.

OSE Immunotherapeutics Buy TP EUR 9.00
47 keplercheuvreux.com
Table 9: Completive environment in ulcerative colitis
Drug candidate Company MOA Administration Clinical stage Expected data
etrolizumab Roche Integrin a4b7/aEb7 SC Phase III H1 2018 ozanimod Celgene/Receptos S1P1 receptor Oral Phase III H2 2018 Xeljanz (tofacitinib) Pfizer Jak inh Oral Phase III Top line published in July
2016 completed results expected in 2018
Stelara (ustekinumab) J&J IL-12/IL-23 inh IV Phase III 2018/19 filgotinib Galapagos / Gilead Jak1 inh Oral Phase II/III 2019 cobitolimod Index Pharmaceutical TLR-9 Oral Phase II H2 2018 etrasimod Arena Pharmaceutical S1P1 receptor Oral Phase II H2 2017 mongersen (GED 0301) Celgene Smad7 Oral Phase II 2017 bertilimumab Immune Pharmaceuticals Eotaxin-1 / CCL11 IV Phase II H1 2017 LY3074828 Eli Lilly IL-23 SC Phase II H2 2017 PF-00547659 Shire (previously Pfizer) MadCAM-1 SC Phase II H2 2017 Otelza (apremilast) Celgene PDE4 inh Oral Phase II 2017 OPRX-106 (oral version of Embrel) Protalix anti-TNF Oral Phase II H1 2017 CCX507 Chemocentryx CCR9 inh Oral Initiation of phase II Pending ABT-494 Abbvie Jak1 inh Oral Phase II 2021
Source: Kepler Cheuvreux
Effi-7 is already monetised! Effi-7 is being developed as part of the Effimab consortium that includes the French
public medical research organisation (INSERM), several public hospitals (APHP, Lille
Hospitals) as well as the CMO company PxTherapeutics, which manufactures Effi-7.
The budget allocated to Effimab is EUR20m, of which EUR9.1m is provided by the
French public investment bank BPI to finance Effi-7 until the end of phase II.
In December 2016, OSE Immunotherapeutics signed an opt-in license deal with
Servier for the global rights of Effi-7. The deal value was EUR272m, including an
upfront payment of EUR10.25m and a two-step payment of EUR30m upon the
exercise of the option license by Servier at the end of the phase II. Thus, the
financing for the development of Effi-7 is secured. While OSE Immunotherapeutics
has emphasised its willingness to quickly monetise its autoimmune assets, we are
cautious about the partnership signed with Servier, for the following reasons:
Servier does not have a commercial presence in the US. We think that the
French pharmaceutical company is likely at term to sub-license Effi-7.
Servier is seeking to develop an autoimmune disease franchise
(GeNeuro/multiple sclerosis; Xoma/rheumatology). However, it does not yet
have any product on the market and does not have a specialty commercial
presence, as it has been historically present in cardiovascular diseases.
Future development of EFFI-7 The preclinical candidate is so far financially backed until phase II. The compound is
expected to enter clinical stage in H2 2018.
Table 10: EFFI-7 patent protection
Applicant Filing date Expiry date Status
Family 1 Inserm and OSE Immunotherapeutics 2012 2032 Being examined: Europe, US, Japan Family 2 Ose ImmunotherapeuticsOSE Immunotherapeutics 2015 2035 Being examined: Europe
Source: OSE Immunotherapeutics
OSE Immunotherapeutics currently protects its intellectual property through the
application of two patent families. Hence, EFFI-7 is protected until 2032 at least.
Financing of Effi-7 is secured until phase II
Servier, the right partner?

OSE Immunotherapeutics Buy TP EUR 9.00
48 keplercheuvreux.com
Deconstructing the forecasts OSE Immunotherapeutics’s main assets are Tedopi for the treatment of NSCLC
and FR104 for the treatment of rheumatoid arthritis; the latter is out-licensed to
J&J. For these two assets, we carry out an in-depth market modelling for NSCLC
and RA, its two lead indications, respectively. We also take into consideration
the future milestones of Effi-7 in UC, although still in preclinical stage, as the deal
with Servier provides more visibility on the product’s development strategy.
However, we have not yet included Effi-DEM in our scenario. Despite strong
positive signals sent by the environment surrounding the CD47/SIRPα mechanism
of action, we believe it is premature to integrate this asset into our model.
We estimate that Tedopi’s sales are likely to reach more than half a billion euros
by 2026, while we think that FR104 could quickly reach blockbuster status (sales
of over EUR1bn) for the RA indication alone. We do not think that Effi-7 will
reach the market before 2028, due to the long development period required for
autoimmune diseases.
Cancer drug pricing
Increasing pricing pressure in the US and Europe has been the big issue hanging over
the pharma sector for the last two years. Reviews of cancer drug pricing (Kantarjian
et al, ASCO JOP, 2014) have resulted in extraordinary price hikes in recent years.
The average cancer drug per year or per course of treatment cost less than
USD10,000 before 2000. This has increased ten-fold, to over USD100,000 per year
of therapy for 12 of the 13 new cancer drugs approved in 2012.
The issue of cancer drug pricing is one that will not go away. Until now, the debate
has largely been restricted to Europe. In the UK, in particular, NICE (the cost-
effectiveness watchdog) has increasingly found a lack of cost-benefit in the absence
of major discounts from the list price. Similarly, Germany has a robust and strict
system that has led to multiple disappointments.
This scrutiny is spreading to the US. The non-profit organisation Institute for Clinical
and Economic Review (ICER) has been hitting the headlines. Sessions at the
American Society of Clinical Oncology (ASCO) are devoted to this issue as well.
However, the US currently still has no agreed system for cost-effectiveness analysis.
We believe that Medicare and pharmacy benefit manager (PBM) pressures (US
government sponsorship of healthcare costs) will continue to focus the administration
on ways to fairly value cancer drugs. In particular, as immuno-oncology starts to
hugely expand the volume of patients receiving this new generation of USD100,000+
per year drugs, the US healthcare system will need to act.
At present, pricing pressure in the US is mainly being driven by PBM competition. As
has been well documented, the negative pricing shocks have come in therapy areas
where therapeutic substitution is possible, i.e. where product-to-product
differentiation is minimal. In the event that little added value is demonstrated in the

OSE Immunotherapeutics Buy TP EUR 9.00
49 keplercheuvreux.com
phase III trial in 2L compared to docetaxel, or in 3L compared to a checkpoint
inhibitor followed by docetaxel, we expect a high level of pricing pressure on Tedopi.
Tedopi: a place in 2L/3L NSCLC
Targeted population: likely to be the third line OSE Immunotherapeutics estimates the targeted market at c. 630,000 patients
(global incidence NSCLC patient population of 1.4m * 45% HLA-A2+ patients) with
global sales of c. EUR2bn. We think the company overestimates its market
opportunity, as we explain below.
Tedopi is currently under investigation (phase III Atalante 1) for its use in second-
line treatment after the failure of platinum-based therapy or in third-line treatment
after the failure of immune checkpoint inhibitors. Taxotere (docetaxel) from Sanofi,
a commonly used chemotherapy drug, is a comparable treatment. We believe most
patients will receive Tedopi in third-line treatment due to:
The 2L new standard-of-care for NSCLC is CKIs as indicated by the ASCO
and ESMO treatment guidelines.
Most of the recruitment centres are based in the EU5 and the US, hence
patients will have medical access to the more costly CKI treatments.
Hence, we believe that even if the phase III trial is a success, Tedopi is likely to be
approved in 2L treatment in the event that platinum-based therapy fails. In practice,
physicians will prescribe Tedopi in third-line treatment after CKIs.
We estimate the targeted population in the G7 (the US, Japan, France, Spain, Italy,
Germany and the UK) is c. 160,000 patients in 2031. We take into account the G7
lung cancer population, from which we remove the number of early-stage diagnosed
cases as well as the large-cell cases. We select 45% of the HLA-A2 population from
which we remove the population not responding to the checkpoint inhibitor which is
estimated to be 70%.
Chart 35: Our Tedopi targeted population
Source: Kepler Cheuvreux
Based on our assumptions, OSE Immunotherapeutics targets one-sixth of the lung
cancer population which is still a significant number of patients.
OSE Immunotherapeutics Buy TP EUR 9.00
50 keplercheuvreux.com
Pricing: pressure likely in the US and Europe We cautiously assume a EUR40,000 annual selling price in Europe and Japan and
EUR50,000 in the US due to the pricing pressure environment which is likely to
continue in the coming years.
Timeframe Tedopi is currently in phase III with preliminary results expected in 2018. OSE
Immunotherapeutics expects a registration filing in 2019 in Europe and the US and a
commercial launch by 2019 in the US and 2020 in Europe. We are more cautious for
the US and forecast a commercial launch in 2020 due to the lack of visibility on the
commercialisation opportunity.
As for the Japanese market, we expect OSE Immunotherapeutics to carry out a
phase III trial in the country following US/EU approval and believe the product will
not reach this market before 2024.
Commercialisation strategy We believe OSE Immunotherapeutics will find a partner to commercialise Tedopi.
Hence, the company is likely to ink deals in the US and in Europe following the
outcome of the phase III trial and the regulatory approval in 2018-19. The value of
deals signed and amount of milestone payments and percentage of royalties
received by OSE Immunotherapeutics will depend on:
The benefit demonstrated in the phase III results.
The labelling given by the regulatory agencies.
As the product has been evaluated both for second-line treatment following
chemotherapy and third-line treatment following CKI in the Atalante 1 clinical
study, we believe a potential partner is likely to wait for the official labelling from the
regulatory agencies. Hence, in the event of 3L approval (which we assume in our
model), a deal is likely to be for a lesser amount than it would be for 2L approval.
Market share We are cautious on our estimates for market penetration of Tedopi due to:
A lack of tangible proven efficacy shown in phase IIb.
The marketing position of the therapeutic vaccine is still unclear as we do
not know if it will be used in 2L or 3L treatment.
We are looking at a highly competitive environment with targeted therapies
and other immuno-oncology candidates.
Therefore, we estimate 15% market share in the US and 10% market share in
Europe, where innovative product market share is usually lower than in the US. We
expect the market share in Japan to around the European level.
A EUR500m opportunity expected We forecast sales in the first ten years of commercialisation, with the start of sales
expected in 2020 in the US and Europe. The patent protecting Tedopi expires in
2024, but the protection has been extended to 2029 thanks to a complementary
certification. We do not expect a significant loss of sales from a biosimilar after

OSE Immunotherapeutics Buy TP EUR 9.00
51 keplercheuvreux.com
2029, but we expect a decrease in market share due to the fierce competitive
environment slightly offset by the uptake of market share in Japan.
Chart 36: Expected sales for Tedopi (EURm)
Source: Kepler Cheuvreux
FR104 in RA
OSE Immunotherapeutics has indicated that J&J will prioritise the development of
FR104 in rheumatoid arthritis. Hence for now, we do not include the prospect of
sales in other autoimmune indications such as transplantation, Graft-versus-host
disease or psoriasis.
Pricing: in line with current treatment We expect the pricing to be in line with what is currently seen on the market. In the
US, the cost of Humira per patient grew from USD21,000 in 2010 to USD46,000 in
2016. Including patient compliance, US revenue per patients for boDMARD market
has risen sharply over the last five years, by a 17% CAGR.
Table 11: US revenues per patient for selected RA products (USD)
Product Company 2011 2012 2013 2014 2015 2016 CAGR (11-16)
Cimzia UCB 12,242 29,523 30,573 40,546 44,079 48,577 32% Orencia SC BMS 23,937 25,072 26,214 37,276 43,210 48,786 15% Humira AbbVie 16,778 18,300 21,278 24,178 29,113 33,535 15% Enbrel Amgen 15,805 16,492 18,230 20,403 23,973 28,644 13% Remicade J & J 11,603 11,528 13,594 15,138 17,202 17,895 9% Average 35,487 17%
Source: Kepler Cheuvreux, EvaluatePharma
We believe the emergence of a biosimilar is likely to put a pressure on price gouging.
Hence, we estimate price increases have hit their peak in the autoimmune market
and new, innovative products are likely to be priced at a EUR30,000 per year per
patient. In Europe, we expect the price to be sharply discounted versus the US at
around EUR25,000 per year.
24 72
121
220
307
425
557 548 523
488 455
407
-
100
200
300
400
500
600
700
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Revenues EU - 5 - Revenues US - Revenues Japan -

OSE Immunotherapeutics Buy TP EUR 9.00
52 keplercheuvreux.com
Timeframe We do not expect FR104 to reach the market before 2024. Indeed, a set of solid
clinical data is essential for it to reach the market for this indication. For example,
sarilumab, an anti-IL6 developed by Sanofi/Regeneron, presented seven studies
from the global SARIL-RA phase III program for its BLA (biological license
application). These clinical trials enrolled 2,500 patients over a near 4.5-year period
after the end of phase II.
Table 12: Lengthy development period for boDMARDS in RA
Product Phase II results First phase III first topline results
BLA filing Notes
sarilumab July 2011 Nov. 2013 Jan. 2016 Sanofi and Regeneron received a complete response letter from the FDA in October 2016 due to manufacturing issues
sirukumab May 2011 Oct. 2015 Oct. 2016
Source: Kepler Cheuvreux, company data
The competitor of sarilumab, sirukumab, another anti-IL-6 developed by J&J/GSK
spent even longer developing its candidate. It took almost five years after its phase II
results before BLA was accepted by the FDA. Both products are still under review
and will not reach the market before 2017.
Hence, we assume a four-year period for the phase III clinical programme for FR104
as well as three years of development for the phase II.
RA Market We see three end-markets for FR104 in RA:
In combination therapy along with methotrexate in 2L.
In combination therapy along with methotrexate in 3L in case of failure of combination 2L therapy with an anti-TNF.
In monotherapy in 2L.
We believe these are the three end-markets for the G7 countries based on the
following assumptions:
Prevalence of 1.4 of RA in EU5 according to Smith et al, 2010.
Prevalence of 1.3M of RA in the US according to the ACR.
Prevalence of 1.2M of RA in Japan according to Yamanaka et al, 2014.
A diagnosed population of 86%, a treated population of 70% and biologic market penetration of 60% in the US versus 30% in Europe and Japan.
Combination therapy represents 55% of first-line therapy following intolerance to or failure of cDMARDs versus 45% for monotherapy.
Around 90% of the patient population takes an anti-TNF as 2L therapy, either in combination or in monotherapy. We estimate this rate to decrease sharply following entrance of anti-IL-6 treatments (sarilumab and sirukumab).
Around 15% market share for FR104 in 3L in combination with methotrexate and a cautious 10% market share in 2L in monotherapy or in

OSE Immunotherapeutics Buy TP EUR 9.00
53 keplercheuvreux.com
combination with methotrexate due to the high competitive environment (biosimilar, new entry candidate).
Table 13: Expected market share of FR104 for the G7 (number of patients in thousands)
Hypothesis 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
- Combination therapy (2L) 55% 414 423 431 440 448 457 467 476 485 495 505 515 525 536 547 - anti-TNF 1L 90% 373 373 372 372 371 371 370 368 367 365 364 362 359 357 354 - Patients not responding to an anti-TNF (3L) 26% 97 97 97 97 97 96 96 96 95 95 95 94 93 93 92 - o/w treated with another biologic than anti TNF (3L) 50% 48 48 48 48 48 48 48 48 48 48 47 47 47 46 46 - o/w market share FR104 (3L) (a) 15% - - - - - - - - 1 3 4 6 7 7 7 - o/w treated with another anti-TNF (3L) 50% 48 48 48 48 48 48 48 48 48 48 47 47 47 46 46 - Other biologic + MTX 2L 10% 41 50 59 68 77 87 97 108 118 130 141 154 166 179 192 - o/w market share FR104 (b) 10% - - - - - - - - - 2 6 9 14 17 19
- Monotherapy (2L) 45% 339 346 353 360 367 374 382 389 397 405 413 421 430 439 447 - o/w anti-TNF + biosimilar 90% 327 330 333 337 340 343 346 350 353 356 359 362 365 369 372 - o/w IL-6r and others 37% 34 44 54 65 76 88 100 113 126 132 136 142 146 155 169 - o/w treated with FR104 (c) 10% - - - - - - - - - 2 6 9 13 16 18
Expected population under FR104 (a+b+c) - - - - - - - - 1 7 16 24 34 41 45
Source: Kepler Cheuvreux
Hence, we expect total market share of 4% for FR0104 in the c. 1m total RA patient
population.
A multi-billion market opportunity Based on the market share of FR104, we estimate sales of FR104 in the G7
countries. We estimate the potential of the candidate to be close to EUR1bn in RA
without considering other potential indications in autoimmune diseases.
Chart 37: Expected sales of FR104
Source: Kepler Cheuvreux
Effi-7: next milestone payment in five years
Thanks to the EUR272m deal signed with Servier, OSE Immunotherapeutics received
a EUR10.25 upfront payment in December 2016. We expect the company to receive
its next fee payment in five years as part of the opt-in two-step option payment of
33
197
409
624
847
998 1,080
-
200
400
600
800
1000
1200
1400
1600
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
FR104 EU - 5 - FR104 US - FR104 Japan -

OSE Immunotherapeutics Buy TP EUR 9.00
54 keplercheuvreux.com
EUR30m. Following this opt-in payment, we think the deal will follow conventional
step payments with clinical payment milestones received in the event of a successful
phase III outcome and regulatory filing as well as commercial milestones.
UC Market: a big opportunity that is far off… As the product is still in its infancy, we forecast a global pool of patients, and for now
we exclude the Japanese market due to Servier’s lack of commercial presence in the
country. Based on global prevalence of UC in the EU5 and the US, we estimate the
patient population treated with Effy-7 to be around 30,000 at its peak based on the
following assumptions:
Around 55% of the UC population have a severe-to-moderate form of UC.
There is a refractory UC form after first-line treatment, with the standard-of-care treatment 5-ASA being used on 40% of the population.
We believe 40% of the refractory population will be treated with a biologic in 2L.
We estimate a cautious 10% market share for Effi-7.
Timeframe We believe the timeframe for the development of Effi-7 is likely to be similar to that
of FR104, as RA and UC treatments both need to demonstrate efficacy in large
phase-III clinical trial programmes.
Pricing In 2014, when Entyvio was launched, the highest annual drug price for IBD
treatment was USD45,000. Our estimates for IBD treatment are slightly lower, and
we estimate the annual wholesale price for Effi-7 should amount to EUR35,000.
Royalties We estimate Servier will pay a tiered royalty amount of c. 15% to OSE
Immunotherapeutics.
Chart 38: Expected revenues from Effi-7 for OSE Immunotherapeutics (EURm)
Source: Kepler Cheuvreux
10 20
7 9
34
61
133
186
-
50
100
150
200
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Royalty from Servier Milestones

OSE Immunotherapeutics Buy TP EUR 9.00
55 keplercheuvreux.com
Initiating coverage with a Buy rating Our valuation of OSE Immunotherapeutics focuses on three candidates: Tedopi,
FR104 and Effi-7. While we do not include Effi-DEM in our valuation due to its
preclinical early-stage development, we emphasise its potential, and we will
closely monitor its future development.
We think OSE Immunotherapeutics is likely to out-license Tedopi in all regions
and will only retain milestone payments and royalties based on commercial
performance. Hence, we do not see any commercial structure or facility
emerging from the company for Tedopi. For FR104, we estimate the royalties
and milestones resulting from the J&J collaboration. We are confident that even
though development will take a long time, this candidate has a great chance of
achieving blockbuster status in case of clinical success due to the wide range of
potential indications.
The next major milestone will be the outcome of the phase III trial for Tedopi in
2018. In the event of clinical or regulatory failure, we think the company is likely
to pursue the development of Effi-DEM thanks to the financing provided by
FR104, and to a lesser extent, by Effi-7. We think the current valuation does not
include the potential of early-stage assets and also undervalues Tedopi. Hence,
we initiate coverage with a Buy rating and a target price of EUR9.
Main risks for Tedopi: finding the right partner for EU/US commercialisation
Scientific Beyond the risk of failure, which is inherent to all clinical programmes, the major risk
we perceive is the lack of strong labelling for Tedopi.
Additional evidence, like a new phase III programme, may be requested by the
regulatory agencies which would lead to a lengthy delay in the commercialisation
of the drug.
Another major risk is a sudden adverse event arising from the current clinical trial.
Considering Tedopi’s safety profile, we are confident this is not likely.
Commercial We believe another important challenge for the group will be to find a partner to
market Tedopi. We expect it to sign a deal in 2018 after the top-line results of the
phase III trial. If an agreement has not yet materialised by that time, the market is
likely to become anxious, which would put pressure on the company’s valuation.
Any delay in signing a deal may significantly decrease the value of the asset due to a
decrease in its commercial prospects.
Lifecycle management Tedopi is being developed solely for the treatment of NSCLC for now. Beyond a
combination with checkpoint inhibitors, no development programme for other

OSE Immunotherapeutics Buy TP EUR 9.00
56 keplercheuvreux.com
indications has been announced. Hence, if the drug fails in the phase III Atalante-1,
its development is not likely to be pursued.
Indeed, this would mean taking on another costly phase II/III development
programme, which we think OSE Immunotherapeutics is unlikely to be able to fund,
unless the company carries out a capital increase.
Main assumptions of our rNPV for Tedopi
Development costs OSE Immunotherapeutics will fund Tedopi’s development costs until the regulatory
filing in the three core regions. Once the drugs are licenced, we do not envisage any
additional costs. The partner will be responsible for manufacturing and marketing.
In Japan, we expect the partner to be responsible for all phase II clinical programmes
receiving approval. We estimate the cost of development programme to be half of
the cost of the Atalante-1 clinical trial (EUR25m).
Special agreement Tedopi was acquired along with the acquisition right for Memopi in 2011, the
technology used to develop Tedopi. At the time, Ose Immunotherapeutics and
Takeda entered into a transfer-and-license agreement. Under the terms of this
agreement, Takeda transferred the proprietary rights and certain patents to OSE
Immunotherapeutics.
In exchange for these rights, Takeda was entitled to the following compensation:
Royalties on future sales of the product at a low-single digit range that we estimate to 4%.
An unknown milestone payment linked to the approval of Tedopi in the US and in Europe, which we estimate to be negligible.
Deal reached in core territories In Europe and the US, we expect the deal to be worth EUR500m of which EUR50m
upfront and expect a gradually increasing double-digit royalty payment on net sales.
In Japan, we expect the deal to be worth significantly less (EUR150m), due to the
fact that OSE Immunotherapeutics will not be responsible for the late-stage
development of the asset there.
Table 14: Expected weight of milestone payments based on commercial performance
Launch 15% Sales > 100 20% Sales > 200 25% Sales > 300 15% Sales > 500 15% Sales > 700 10%
Source: Kepler Cheuvreux
Probability of success We estimate Tedopi has a 33% chance to reach the market based on the data
published by BIO.

OSE Immunotherapeutics Buy TP EUR 9.00
57 keplercheuvreux.com
Table 15: Expected probability of success oncology versus non-oncology programmes
Oncology Non-oncology
Phase I to Phase II 62.8% 63.5% Phase II to Phase III 24.6% 34.3% Phase III to NDA/BLA 40.1% 63.7% NDA/BLA to approval 82.4% 85.9% Phase III to approval 33.0% 54.7%
Source: Kepler Cheuvreux, BIO
Tax rate OSE Immunotherapeutics is set to licence out all of these products. Its revenues will
come from milestone payments and royalties on sales. We estimate a tax rate of 16%
based on French tax regulations for royalty payments (INPI, Institut de la Propriété
Intellectuelle).
Discount rate Ose Immunothearapeutics’s valuation mainly relies on Tedopi’s potential. The main
risk factor for a biotech company is the clinical success of its projects. OSE
Immunotherapeutics’s late-stage pipeline is not diversified; hence we apply a
discount rate of 15%, a level commensurate with the literature on companies at this
stage of development (Valuation in Life Sciences, Bogdan et al.).
Sales & marketing As OSE Immunotherapeutics will out-license Tedopi, we assume the company will
bear no S&M costs to market the candidate.
rNPV of Tedopi in NSCLC (EUR97m)
Chart 39: Expected revenues for OSE Immunotherapeutics from Tedopi
Source: Kepler Cheuvreux
100
137
8 17
137
164
193
222
88 74 77
52 41
-
50
100
150
200
250
300
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Royalty Milestones Upfront

OSE Immunotherapeutics Buy TP EUR 9.00
58 keplercheuvreux.com
Table 16: rNPV of Tedopi for OSE Immunotherapeutics in third-line HLA-A2+ in Europe (EURm)
Hypothesis 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Clinical status PIII PIII Reg. Launch Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Ose EU operating revenues - - 50 68 3 7 16 115 34 155 35 28 21 16 11 R&D cost 10% (5) (5) (5) (5) G&A 2% (1) (1) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) (2) Royalty Takeda 4% 0 0 0 (0) (1) (2) (4) (5) (7) (8) (8) (7) (6) (5) (4) Pre-tax cash flow (6) (6) 43 61 1 3 10 108 25 145 25 19 13 9 5 Tax@16% 16% 1 1 (7) (10) (0) (1) (2) (17) (4) (23) (4) (3) (2) (1) (1) FCF (5) (5) 36 52 0 3 9 91 21 122 21 16 11 7 4 Proba Adj. Hypothesis 100% 100% 40% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% FCF prob. adj Revenues (5) (5) 14 17 0 1 3 30 7 40 7 5 4 2 1 Discount rate 15% rNPV Tedopi in Europe 38
Source: Kepler Cheuvreux
Table 17: rNPV of Tedopi for OSE Immunotherapeutics in third-line HLA-A2+ in the US (EURm)
Hypothesis 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Clinical status PIII PIII Reg. Launch Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Mark. Ose US operating revenues - - 50 69 5 10 112 34 159 58 50 40 31 25 18 R&D (5) (5) (10) Royalty Takeda 4% - - - (1) (2) (3) (5) (7) (9) (12) (11) (10) (9) (8) (7) Pre-tax cash flow 30 (5) (5) 40 68 3 7 107 27 149 47 39 30 22 17 11 Tax@16% 16% 1 1 (6) (11) (0) (1) (17) (4) (24) (7) (6) (5) (4) (3) (2) FCF (4) (4) 33 57 2 6 90 23 126 39 33 25 19 14 9 Proba Adj. Hypothesis 100% 100% 40% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% FCF Prob. Adj Revenues (4) (4) 13 19 1 2 30 8 41 13 11 8 6 5 3 Discount rate 15% rNPV Tedopi in US 49
Source: Kepler Cheuvreux
Table 18: rNPV of Tedopi for OSE Immunotherapeutics in third-line HLA-A2+ in Japan(EURm)
Hypothesis 2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Clinical status PIII PIII PIII Reg. Launch Mark. Mark. Mark. Mark. Mark. Mark. Mark. Ose Japan operating revenues 10 15 0 9 3 6 24 11 11 Royalty Takeda 4% - (0) (1) (2) (3) (4) (4) (4) (4) Pre-tax cash flow 10 15 (1) 7 0 2 19 7 7 Tax@16% 16% (2) (2) 0 (1) (0) (0) (3) (1) (1) FCF 8 12 (1) 6 0 2 16 6 6 Proba Adj. Hypothesis 100% 100% 40% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% 33% FCF Prob. Adj Revenues 3 4 (0) 2 0 1 5 2 2 Discount rate 15% rNPV Tedopi in Japan 10
Source: Kepler Cheuvreux
rNPV of FR104 in RA (EUR12)
J&J raised its opt-in option in July 2016 for the development of FR104. The group
will primarily develop FR104 in RA. Therefore, we only take into account this
indication in our model. However, we emphasise that it could be approved for other
indications, notably in the treatment of transplantation maintenance.

OSE Immunotherapeutics Buy TP EUR 9.00
59 keplercheuvreux.com
Royalty rate We estimate that the royalty payment paid by J&J to OSE Immunotherapeutics will
gradually increase. We estimate it will be the high single-digits (9%).
Milestone payments For the milestone payments, we divide the gross amount of EUR155m by three for
the RA indication. We estimate the rest of milestones will be split between
additional therapeutic indications.
We believe the amount of payments will be distributed between: 1) the US: 50%; 2)
Europe: 30%; and 3) Japan 20%, after assessing the potential of each market.
Inserm payments FR104 was developed as part of collaboration with the French National Institute of
Health and Medical Research (Inserm). According to the agreement for the licence
transfer in 2013, Inserm is entitled to receive royalty payments based on OSE
Immunotherapeutics’s revenues. We expect the tiered royalty rate to be in the mid-
single-digits (c. 5%).
Probability of success We base our probability of success estimate on the data provided by BIO. At this
stage, we estimate 17% probability of approval.
Table 19: Expected probability of success in autoimmune disease
Immunology
Phase II to Phase III 31.7% Phase III to NDA/BLA 62.2% NDA/BLA to approval 86.0% Phase II to approval 17.0%
Source: BIO, Kepler Cheuvreux
rNPV of FR104 in RA (EUR12m)
Table 20: rNPV of FR104 in RA
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
Clinical status PII PII PII PIII PIII PIII PIII Reg. Launch Mark. Mark. Mark. Mark. Mark. Mark. Milestones - - 4 - - - 6 8 12 4 7 4 1 2 1 Royalty - - - - - - - - 2 14 33 56 84 90 97 FR104 operating revenues - - 4 - - - 6 8 14 19 40 61 85 92 98 Inserm royalties - - (0) - - - (0) (0) (1) (1) (2) (2) (3) (4) (4) Pre-tax cash flow - - 4 - - - 5 7 13 18 38 58 81 88 94 Tax@16% - - (1) - - - (1) (1) (2) (3) (6) (9) (13) (14) (15) FCF - - 3 - - - 5 6 11 15 32 48 68 74 78 Proba Adj. Hypothesis 100% 100% 100% 32% 32% 32% 32% 20% 17% 17% 17% 17% 17% 17% 17% FCF Prob. Adj Revenues - - 3 - - - 1 1 2 3 5 8 11 12 13 Discount rate 15% rNPV FR104 in Europe / OSE Immunotherapeutics (EURm)
12
Source: Kepler Cheuvreux

OSE Immunotherapeutics Buy TP EUR 9.00
60 keplercheuvreux.com
rNPV of Effi-7 in UC (EUR6m)
Royalty rate We estimate that the royalty payment paid by Servier to OSE Immunotherapeutics
will gradually increase. We expect it to be in the high single-digit range (9%).
Milestone payments OSE Immunotherapeutics will be entitled to receive up to EUR232m once the phase
II programme has been carried out and if Servier decides to exercise its opt-in
options. We split this amount between the different phases of development. We also
factor in the hypothesis for three indications and split this amount based on a
number of developments (e.g. Sjogren’s syndrome).
Probability of preclinical and clinical success According to the current scientific literature (Paul et al, 2010), the probability of
success from the preclinical to the phase-I stage is around 69%. For later stages of
development, our hypothesis is similar to that used for FR104 for the treatment of
autoimmune disease.
Inserm payments Effi-7 was developed as part of a partnership with the French National Institute of
Health and Medical Research (Inserm). According to the agreement signed for the
licence transfer in 2011, Inserm is entitled to receive royalty payments based on
OSE Immunotherapeutics’s revenues as well as milestone payments of up to
EUR1.4m. We expect royalties to be in the mid-single-digit range (5%).
R&D costs We do not expect Effi-7 to reach the market before 2028. OSE Immunotherapeutics
is responsible for the development of Eff-7 until the end of the phase II trial as part
of the Effimab consortium. The budget allocated for this programme is expected to
amount to EUR20m of which EUR9.1m will be provided by the BPI. We expect OSE
Immunotherapeutics to spend EUR10.9m until the clinical proof-of-concept has
been established for the asset. We split this amount according to the weight of each
step in the development process.
Table 21: rNPV Effi-7
2017 2018 2019 2020 2021 2022 2023 2024 2025 2026 2027 2028 2029 2030 2031
PC PC PI PI PII PII PIII PIII PIII PIII Reg. Launch Mark. Mark. Mark. Milestones - - - - 10 20 - - - 7 9 25 11 2 2 Royalty from Servier - - - - - - - - - - - 9 51 131 184 Ose operating revenues - - - - 10 20 - - - 7 9 34 61 133 186 Inserm royalties - - - - (0) (1) - - - (0) (0) (1) (2) (5) (7) R&D until phase II (1) (1) (2) (2) (3) (3) - - - - - - - - - Tax@16% 0 0 0 0 (1) (3) - - - (1) (1) (5) (9) (21) (29) FCF (1) (1) (1) (1) 5 13 - - - 5 7 28 49 108 150 100% 100% 69% 69% 45% 45% 14% 14% 14% 14% 9% 8% 8% 8% 8% FCF Prob. Adj Revenues (1) (1) (1) (1) 2 6 0 0 0 1 1 2 4 8 12 Dscount rate 15% rNPV Tedopi 6
Source: Kepler Cheuvreux

OSE Immunotherapeutics Buy TP EUR 9.00
61 keplercheuvreux.com
SOP summary
We factor in very conservative estimates of the probability of success of the
company’s various projects. In our view, 2018 is likely to be a critical year for OSE
Immunotherapeutics, as it is due to release the phase-III results for Tedopi. If it
reports positive results, we see significant upside for the company of around
150%. However, even if it fails, we think the company will still be able to develop its
internal proprietary early-stage asset Effi-Dem thanks to the funding provided by
the deal signed with J&J and Servier for FR104 and Effi-7 respectively.
Chart 40: SOP OSE Immunotherapeutics (EURm)
Source: Kepler Cheuvreux
EUR131m
EUR97m EUR12m EUR6m
EUR17m
-
20
40
60
80
100
120
140
160
rNPV Tedopi rNPV FR104 rNPV Effi-7 Net cash position Base case

OSE Immunotherapeutics Buy TP EUR 9.00
62 keplercheuvreux.com
Appendices Shareholders
Chart 41: Shareholder structure as of 30 June 2016
Source: Ose Immunotherapeutics
Key people
Emile Loria, Chairman, MD Dr Emile Loria has more than 25 years of experience in the pharmaceutical and
biotechnology sectors, having held key positions notably at Ciba-Geigy and Sanofi
Pharma. He was a researcher at the Cancer Institute in Villejuif and then at the
Cancer and Immunogenetics Institute (INSERM-CNRS) founded by Professor
Georges Mathé. In 1986, he founded MS Medical Synergy, a drug management
company. He then joined Biovector Therapeutics where he became Chairman and
Chief Executive Officer.
In 2001, Loria was appointed Chief Executive Officer of Epimmune and developed
the epitopes technology, from which stemmed the Tedopi epitopes. He ran this
programme from the initial research stage to the start of the phase-II clinical trial. In
2012, he purchased, via OPI (Geneva), all of the Memopi assets, co-founded OSE
Pharma and became Chairman of its board.
Dominique Costantini, CEO, MD Dr Costantini held a number of management positions at HMR (now Sanofi) where
she led medico-marketing activities to commercialise products (notably in
immunology, endocrinology, infectious illnesses and oncology). While there, Ms.
Costantini also participated in the development of various medicines, from
conception to the product approval and commercialisation stages.
In 1997, Costantini founded BioAlliance Pharma, where she held the position of
Chief Executive Officer until 2011. During her tenure there she led BioAlliance
Pharma’s IPO on Euronext (2005). BioAlliance Pharma originated Livatag, an anti-
cancer nanotechnology in primary liver cancer, currently in phase-III development
(in Europe and the US). In the past, Costantini was instrumental in forming many
31%
13%
2%
55%
Emile Loria Dominique Constantini Guy Chateain Others
OSE Immunotherapeutics consort: 45%

OSE Immunotherapeutics Buy TP EUR 9.00
63 keplercheuvreux.com
international industrial partnerships (Europe, the US, China, Japan and South
Korea). To date, BioAlliance Pharma (renamed Onxeo in 2014) is the only French
biotechnology company to have two FDA drug approvals.
In 2012, Costantini co-founded and led OSE Pharma as CEO.
Immune system functions
Haematopoiesis According to nature review, haematopoiesis refers to the commitment and
differentiation processes that lead to the formation of all blood cells from
haematopoietic stem cells. In adults, haematopoiesis occurs mainly in the bone
marrow (medullary), but it can also occur in other tissues such as the liver, thymus
and spleen (extramedullary).
Hematopoietic stem cells can be broadly separated into two major lineages: the
lymphoid lineage including T, B, and natural killer (NK) cells, or the myeloid lineage
comprised of erythrocytes, megakaryocytes, granulocytes, and monocyte/
macrophage. Another category of important immune cells called dendritic cells are
also of hematopoietic origin.
Chart 42: Haematopoiesis at a glance
Source: Pinterest
The immune system The immune system is composed of a broad variety of specialised cells. These cells
recognise specific chemical structures called antigens. Foreign antigens trigger an
immune response that typically results in resistance to disease-causing agents from
the body. The immune system recognises and generates a response to hundreds of
different foreign antigens.

OSE Immunotherapeutics Buy TP EUR 9.00
64 keplercheuvreux.com
There are two kinds of immune response to an antigen:
The innate immune response functions as the first line of defence against
antigens It consists of soluble factors, such as complement proteins, and
diverse cellular components including granulocytes (basophils, eosinophils
and neutrophils), mast cells, macrophages, dendritic cells and natural
killer cells.
The adaptive immune response is slower to develop, but manifests as
increased antigenic specificity and memory. It consists of antibodies, B cells,
and CD4+ and CD8+ T lymphocytes.
Chart 43: The innate and adaptive immune system
Source: Dranoff et al, Nature reviews
An adaptive immune response is triggered by a specialised class of immune system
cells called antigen-presenting cells (e.g. dendritic cells and macrophage). Antigen-
presenting cells take up antigen from their surroundings and process the antigen
into fragments that are then displayed on the surface of the antigen-presenting
cell. Once displayed, these antigens can be recognised by classes of immune
cells called lymphocytes.
One category of lymphocytes, cytotoxic T lymphocytes (“T CD8+ cells”), combats
disease by killing antigen-bearing cells directly; another class of T lymphocytes,
helper T cells ("T CD4+ cells"), coordinates the activities of cells that directly target
diseased tissue.
A certain amount of these helper T CD4+ cells are responsible for coordinating
defence activities against infectious agents and tumours (effector T CD4+
lymphocytes), while others are responsible for inhibiting unwanted inflammatory
responses (regulatory T lymphocytes or Treg). A second category of lymphocytes, B
lymphocytes (“B cells”), produce specific antibodies when activated. Each antibody
binds to and attacks one particular type of antigen expressed on a cell.

OSE Immunotherapeutics Buy TP EUR 9.00
65 keplercheuvreux.com
Use of the immune system to fight diseases: immunotherapy
Immunotherapy is intended to stimulate and enhance the body’s natural mechanism
from both the innate and adaptive immune system. To date, only one category of cell
in the immune system has been harnessed and targeted by the current approved
therapies: the cytotoxic T lymphocytes (“T CD8+ cells”).
Chart 44: Overview of immune system components which could be targeted by IO therapies
Source: Takeda
Hence, there is still a broad range of targets for IO mechanisms beyond those
addressed by approved products.
Immunotherapeutic approaches to treat disease can be separated into two broad
classes, passive and active, based on their mechanism of action.
Passive immunotherapy (non-specific): Passive immunotherapies do not rely on or
actively stimulate the body’s immune system to initiate the attack on the disease.
Instead, the attack is carried out by the therapy which is manufactured ex vivo, or
outside the body. These therapies are not considered to be personalised and consist
mainly of monoclonal antibodies directed at a single disease-specific enzyme or
protein on the surface of the targeted cells. The goal of these passive
immunotherapies is to prevent targeted cells from dividing or to cause their death.
Active immunotherapy (specific or non-specific): Active immunotherapies, on the
other hand, are designed to trigger or stimulate the body’s own immune system to
fight the disease. They include both traditional T-cell stimulation with antigen and
cell-based immunotherapies. Active immunotherapy is a more specific approach to
immunotherapy than passive immunotherapy because active immunotherapies
contain a particular antigen or set of antigens that are designed to activate the
patient’s own immune system to seek out and kill cells that carry the same antigen.
Active immunotherapies have no direct therapeutic action, but rather rely on the
patient’s immune system to recognize and kill the intended target. Most active
immunotherapies utilise off-the-shelf antigens, also referred to as defined antigens,
rather than antigens that are patient-specific, and are frequently paired with

OSE Immunotherapeutics Buy TP EUR 9.00
66 keplercheuvreux.com
adjuvants, which are agents that non-specifically activate the cells of the immune
system to enhance tumour-specific immune responses. Immunotherapies targeting
the active immune system can be divided into four categories:
1. Immune checkpoint inhibitors (CKIs) and co-stimulatory receptors act on the signalling pathways that slow /increase T cell activation or other immune cells. T cells are the cornerstone of the innate and adapted immune system. There are multiple checkpoint inhibitors (e.g.: anti-CTLA-4, PD-L1, TIM-3) or co-stimulatory pathways (e.g.: ox-40, CD-40, CD137, CD28).
2. Therapeutic vaccines aim to prime the immune system to recognise and attack tumour-associated antigens (TAAs).
3. Oncolytic viruses are viral strains that are genetically modified to selectively infect and kill tumour cells while priming an immune response by releasing TAAs.
4. Adoptive cell therapy consists of the ex vivo expansion and genetic modification of tumour-associated antigen-specific T cells (via T-cell receptors or antibodies recognition) to increase anti-tumour response (e.g.: TCRs, CAR-T). Adoptive cell therapies are currently being developed in early-stage trials mostly in liquid tumours.
Immunotherapy applied to cancer
OSE Immunotherapeutics aims to develop cancer therapies in two core categories:
1) the therapeutic vaccine with Tedopi development; and 2) the immune checkpoint
blockade with EFFI-Dem for non-effective immune cells (macrophage cells).
Chart 45: Anticancer immunotherapy
Source: Galluzzi et al, 2015,

OSE Immunotherapeutics Buy TP EUR 9.00
67 keplercheuvreux.com
Cancer vaccines at a glance Vaccination is an active immunotherapy method that entails the introduction of an
external agent (antigen) into a living organism to create a positive immune response
against this agent. All cancer immunotherapy approaches have a common goal: to
trigger a cytotoxic T lymphocyte (CTL) response against cancer cells. Those
activated lymphocytes (also called CD8+) are considered to be the pillar of the
body’s defences against external agents such as:
Infected cells either by a virus (e.g. HIV) or an intracellular bacteria or protozoal parasites.
Cancer cells.
Allografts tissue following transplant: leading to kidney transplant rejection for example.
CTLs are activated with the help of dendritic cells, which help them to recognise the
cells which need to be targeted thanks to the major histocompatibility complex class
II. Dendritic cells help the CTL by presenting it with an antigen from the cancer cells.
Therefore, once the CTL target has been revealed by the dendritic cells, the CTLs
along with other the lymphocyte CD4+ which allow CD8+ T cell expansion help to
recognise and destroy cancer or virus-infected cells. The immune response is
regulated by numerous cells and mechanisms notably the CD4+ Treg cells and the
myeloid-derived suppressor cells (e.g. tumour-associated macrophages).
Chart 46: Steps in the development of cellular immune response against tumour-associated antigens (TAAs)
Source: Abbreviations: DC: dendritic cells; IFN‑γ, interferon‑γ, Treg: regulatory T cells, CTL: cytotoxic T cells; TCR: T cell receptor; MHC: major histocompatibility complex Source: Melero, I. et al.
Nature Reviews Clinical Oncology 11, 509–524 (2014
Cancer vaccines aim to prime the CD8+ T cell response

OSE Immunotherapeutics Buy TP EUR 9.00
68 keplercheuvreux.com
Current immuno-oncology therapies aim to activate (provide large quantities of
tumour antigens) and expand (stimulate the response system and/or diminish the
checkpoint inhibitors pathways) the tumour-specific CTLs.
Cancer vaccines have a broad range of diversity Many different types of vaccines are now being studied to treat a variety of cancers,
such as:
Tumour cell vaccines: These vaccines are made from actual cancer cells that have
been removed from the patient during surgery. Cells are altered (and killed) in the
lab ex vivo to make them more likely to be attacked by the immune system and are
then injected back into the patient. The patient’s immune system then attacks these
cells and any similar cells still in the body.
Chart 47: Whole tumour cell vaccines
Source: Cancer research institute
Most tumour cell vaccines are autologous, meaning the vaccine is made from dead
tumour cells that have been taken from the same person in whose body they will later
be used. Other vaccines are allogeneic, meaning the cells for the vaccine come from
someone other than the patient being treated. Allogeneic vaccines are easier to make
than autologous vaccines, but it is still not clear whether one type works better than
the other.

OSE Immunotherapeutics Buy TP EUR 9.00
69 keplercheuvreux.com
Antigen vaccines: These vaccines boost the immune system by using only one
antigen (or a few), rather than the whole tumour cell. The antigens are usually
proteins or pieces of proteins called peptides.
Chart 48: Antigen-specific vaccines
Source: : Cancer research institute
Antigen vaccines can be specific for a certain type of cancer, but they are not made for
a specific patient like autologous tumour cell vaccines are. OSE Immunotherapeutics
is present in this category of therapeutic vaccines with Tedopi.
So far, no peptide-based vaccine has been approved in Europe or the US. However,
Russian authorities approved Oncophage from Agenus in 2008 despite its failure to
prove a significant advantage in terms of efficacy in renal cell carcinoma.
Dendritic cell vaccines: These vaccines have shown the most success so far in
treating cancer. Sipuleucel-T (Provenge), from Valeant, which is approved for the
treatment of advanced prostate cancer, is an example of a dendritic cell vaccine.
Dendritic cells are special immune cells in the body that help the T cells to recognise
cancer cells. The T cells then start an immune reaction against any cells in the body
that contain these antigens.
OSE Immunotherapeutics is active in the antigen-presented cell vaccine

OSE Immunotherapeutics Buy TP EUR 9.00
70 keplercheuvreux.com
Chart 49: Dendritic cell-based vaccines
Source: Cancer research institute
Dendritic cell vaccines are autologous vaccines which entail a complex and
expensive manufacturing process. The dendritic cells are first engineered outside of
the patient’s body and then injected back into the patient, where they should trigger
an immune response to cancer cells.
Neoantigen-based vaccines: This is the last generation of cancer vaccines which
aims to use the difference of each patient’s tumour genome. The theory behind this
new approach is based on the difference between the DNA of the cancer and that of
the healthy cells. This difference in DNA leads to the creation of new protein
antigens that are specific to tumour cells. These new antigens, known as tumour-
specific neo-antigens (TSNAs), can be recognised and targeted by the immune
system. Rather than pursuing antigens that are “shared” between patients, the study
of neoantigens is aimed at developing more “personalised” vaccines which recognise
the specific characteristics of each tumour in each patient.
Vector-based vaccines: These vaccines use special vector systems to make the
immune response more effective. Vectors are viruses, bacteria, yeast cells, or other
structures. The vectors are often modified to attenuate their immunogenicity.
Vectors can be helpful in making vaccines for a number of reasons. First, they can be
used to deliver more than one cancer antigen at a time, which might make the body’s

OSE Immunotherapeutics Buy TP EUR 9.00
71 keplercheuvreux.com
immune system more likely to mount a response. Second, although attenuated from
their immunogenicity, vectors trigger their own immune responses from the body,
which could help make the overall immune response even stronger. Finally, the
manufacturing process for these vaccines is cheaper than it is for other vaccines.
Checkpoint blockade: the new paradigm of cancer treatment The principle of checkpoint inhibition is to deactivate the tumour’s defence
mechanism and activate a response from the immune system. CKIs work like
molecular brakes, curtailing immune reactions that have already begun in order to
prevent “collateral damage” to the surrounding tissue. This is necessary because
immune reactions need a starting point and an endpoint. Two of these checkpoint
proteins are PD-1 and PD-L1. While PD-1 is located on immune cells (e.g. T-cells),
PD-L1 is located on many different cells throughout the human body.
Cancer cells exploit this principle to camouflage themselves. They evade the immune
system’s attack by accumulating PD-L1 proteins on their surface. These proteins are
recognised by the PD-1 on the T-cells, thus blocking the body’s immune reaction
against cancer. As a result, the tumour cells remain hidden.
Numerous immuno-therapies are currently being developed. They target a wide
range of checkpoints, allowing researchers to explore:
Effector T cell mechanisms (e.g. PD-1).
Natural killer cell mechanisms.
Non-effector cell mechanism (e.g. EFFI-Dem candidate from OSE Immunotherapeutics).
Immunotherapy applied to autoimmune diseases
Autoimmune diseases occur when the immune system attacks the body’s own
organs, tissues and cells. Some of the more common autoimmune diseases include
type1 diabetes, rheumatoid arthritis, systemic lupus erythematosus, and
inflammatory bowel disease.
Although the causes of many autoimmune diseases remain unknown, a person’s
genes, in combination with infections and other environmental exposure, are likely
to play a significant role in the development of disease. Treatments are available for
many autoimmune diseases, but cures have yet to be discovered. Smith and
Germolec state that autoimmune disorders affect approximately 3% of the North
American and European populations, with over 75% of those affected being women.
CKIs are the cornerstone of IO

OSE Immunotherapeutics Buy TP EUR 9.00
72 keplercheuvreux.com
Valuation
FY to 31/12 (EUR) 2015 2016E 2017E 2018E
Per share data (EUR) EPS adjusted -0.01 0.28 -0.66 -0.70 % Change na na na EPS adjusted and fully diluted -0.01 0.28 -0.66 -0.70 % Change na na na EPS reported -0.01 0.28 -0.66 -0.70 % Change na na na EPS Consensus -0.22 -0.37 -0.16 Cash flow per share -0.41 0.51 -0.78 -0.85 Book value per share 4.44 3.92 2.92 2.87
DPS 0.00 0.00 0.00 0.00 Number of shares, YE (m) 14.3 14.3 14.3 14.3 Number of shares, fully diluted, YE (m) 14.3 14.3 14.3 14.3 Share price Latest price / year end 8.5 7.1 6.7 6.7 52 week high (Year high) 11.6 8.3 52 week low (Year low) 8.0 5.7 Average price (Year) 9.6 6.7
Enterprise value (EURm) Market capitalisation 136.9 96.4 95.9 95.9 Net financial debt -9.0 -16.3 -5.1 7.0 Pension provisions 0.0 0.0 0.0 0.0 Market value of minorities 0.0 0.0 0.0 0.0 Market value of equity affiliates (net of tax) 0.0 0.0 0.0 0.0 Others 0.0 0.0 0.0 0.0 Enterprise value 127.9 79.6 90.8 102.9 Valuation P/E adjusted na 23.7 na na
P/E adjusted and fully diluted na 23.7 na na P/E consensus na na na P/BV 2.2 1.7 2.3 2.3 P/CF na 13.1 na na Dividend yield (%) 0.0% 0.0% 0.0% 0.0% Dividend yield preference shares (%) 0.0% 0.0% 0.0% 0.0% FCF yield (%) -4.3% 7.6% -11.7% -12.6% ROE (%) 6.8% -19.2% -24.3% ROIC (%) 43.7% -477.6% na
EV/Sales 25.28 3.93 na na EV/EBITDA na 19.9 na na EV/EBIT na 19.9 na na EV/NOPAT na 29.7 na na EV/IC 15.6 19.6 na na ROIC/WACC 2.9 na na EV/IC over ROIC/WACC 6.7 na na

OSE Immunotherapeutics Buy TP EUR 9.00
73 keplercheuvreux.com
Income statement
FY to 31/12 (EURm) 2011 2012 2013 2014 2015 2016E 2017E 2018E
Sales 0.0 0.0 0.0 0.0 5.1 20.3 0.0 0.0 % Change na na na na na 300.1% na na EBITDA reported na na na na -3.8 4.0 -11.2 -12.1 % Change na na na na na na na na Depreciation and amortisation na na na na 0.0 0.0 0.0 0.0 Goodwill impairment na na na na 0.0 0.0 0.0 0.0 Other financial result and associates na na na na 0.0 0.0 0.0 0.0 EBIT reported na na na na -3.8 4.0 -11.2 -12.1
% Change na na na na na na na na Net financial items na na na na 0.0 0.0 0.0 0.0 Associates na na na na 0.0 0.0 0.0 0.0 Others na na na na 0.0 0.0 0.0 0.0 Earnings before tax na na na na -3.8 4.0 -11.2 -12.1 % Change na na na na na na na na Tax na na na na 3.5 0.1 1.8 2.1
Net profit from continuing operations na na na na -0.2 4.0 -9.4 -10.0 % Change na na na na na na na na Net profit from discontinuing activities na na na na 0.0 0.0 0.0 0.0 Net profit before minorities na na na na -0.2 4.0 -9.4 -10.0 Minorities na na na na 0.0 0.0 0.0 0.0 Net profit reported na na na na -0.2 4.0 -9.4 -10.0 % Change na na na na na na na na Adjustments na na na na 0.0 0.0 0.0 0.0 Net profit adjusted na na na na -0.2 4.0 -9.4 -10.0
% Change na na na na na na na na Gross profit na na na na 5.1 20.3 0.0 0.0 EBITDA adjusted na na na na -3.8 4.0 -11.2 -12.1 EBIT adjusted na na na na -3.8 4.0 -11.2 -12.1 Gross profit margin (%) na na na na 100.0% 100.0% na na EBITDA margin (%) na na na na -74.1% 19.7% na na EBIT margin (%) na na na na -74.1% 19.7% na na Net profit margin (%) na na na na -4.1% 20.0% na na Tax rate (%) na 33.0% 33.0% 33.0% 33.0% 33.0% 33.0% 33.0%
Payout ratio (%) na na na na 0.0% 0.0% 0.0% 0.0% EPS reported (EUR) na na na na -0.01 0.28 -0.66 -0.70 % change na na na na na na na na EPS adjusted (EUR) na na na na -0.01 0.28 -0.66 -0.70 % change na na na na na na na na EPS adj and fully diluted (EUR) na na na na -0.01 0.28 -0.66 -0.70 % change na na na na na na na na DPS (EUR) na na na na 0.00 0.00 0.00 0.00 % change na na na na na na na na DPS,preference shares (EUR) na na na na 0.00 0.00 0.00 0.00 % Change na na na na na na na na
Consensus Sales (EURm) 10.3 6.9 13.1 Consensus EBITDA (EURm) na na na Consensus EBIT (EURm) 10.4 0.1 5.5 Consensus EPS (EUR) -0.22 -0.37 -0.16 Consensus DPS (EUR) na na na

OSE Immunotherapeutics Buy TP EUR 9.00
74 keplercheuvreux.com
Cash flow statement
FY to 31/12 (EURm) 2015 2016E 2017E 2018E
Net profit before minorities -0.2 4.0 -9.4 -10.0 Depreciation and amortisation 0.0 0.0 0.0 0.0 Goodwill impairment 0.0 0.0 0.0 0.0 Change in working capital -2.9 1.5 0.0 0.0 Others -2.8 1.7 -1.8 -2.1 Cash Flow from operating activities -5.9 7.3 -11.2 -12.1 % Change na na na na Capex 0.0 0.0 0.0 0.0
Free cash flow -5.9 7.3 -11.2 -12.1 % Change na na na na Acquisitions -6.2 0.0 0.0 0.0 Divestments 0.0 0.0 0.0 0.0 Dividend paid 0.0 0.0 0.0 0.0 Share buy back 0.0 0.0 0.0 0.0 Capital increases 20.2 0.0 0.0 0.0 Others 0.9 0.0 0.0 0.0 Change in net financial debt 9.0 7.3 -11.2 -12.1 Change in cash and cash equivalents na 7.2 -11.2 -12.1
Attributable FCF -5.9 7.3 -11.2 -12.1 Cash flow per share (EUR) -0.41 0.51 -0.78 -0.85 % Change na na na na FCF per share (EUR) -0.41 0.51 -0.78 -0.85 % Change na na na na Capex / Sales (%) 0.0% 0.0% na na Capex / D&A (%) na na na na
Cash flow / Sales (%) -116.1% 36.1% na na FCF / Sales (%) -116.1% 36.1% na na FCF Yield (%) -4.3% 7.6% -11.7% -12.6% Unlevered FCF Yield (%) -4.6% 9.2% -12.3% -11.8%

OSE Immunotherapeutics Buy TP EUR 9.00
75 keplercheuvreux.com
Balance sheet
FY to 31/12 (EURm) 2015 2016E 2017E 2018E
Cash and cash equivalents 11.6 18.7 7.5 -4.6 Inventories 0.0 0.0 0.0 0.0 Accounts receivable 0.1 0.7 0.7 0.7 Other current assets 12.5 10.1 10.1 10.1 Current assets 24.1 29.6 18.4 6.3 Tangible assets 0.1 0.1 0.1 0.1 Goodwill 0.0 0.0 0.0 0.0 Other Intangible assets 61.1 45.6 57.5 83.9 Financial assets 0.1 0.1 0.1 0.1
Other non-current assets 0.0 0.0 0.0 0.0 Non-current assets 61.3 45.8 57.6 84.1 Short term debt 1.0 0.8 0.8 0.8 Accounts payable 3.0 5.1 5.1 5.1 Other short term liabilities 1.5 1.8 6.7 11.7 Current liabilities 5.4 7.7 12.7 17.7 Long term debt 1.6 1.6 1.6 1.6 Pension provisions 0.0 0.0 0.0 0.0 Other long term provisions 14.9 10.0 20.0 30.0 Other long term liabilities 0.0 0.0 0.0 0.0
Non-current liabilities 16.5 11.7 21.7 31.7 Shareholders' equity 63.4 56.0 41.7 41.0 Minority interests 0.0 0.0 0.0 0.0 Total equity 63.4 56.0 41.7 41.0 Balance sheet total 85.3 75.3 76.0 90.4 % Change na -11.7% 0.9% 18.9% Book value per share (EUR) 4.44 3.92 2.92 2.87 % Change na -11.7% -25.5% -1.6%
Net debt -9.0 -16.3 -5.1 7.0 Net financial debt -9.0 -16.3 -5.1 7.0 Trade working capital -2.9 -4.4 -4.4 -4.4 Working capital 8.1 4.0 -1.0 -6.0 Inventories/sales 0.0% 0.0% na na Invested capital 8.2 4.1 -0.9 -5.9 Net fin. debt / EBITDA (x) 2.4 -4.1 0.5 -0.6 Net fin. debt / FCF (x) 1.5 -2.2 0.5 -0.6 Gearing (%) -14.2% -29.1% -12.2% 17.1% Goodwill / Equity (%) 0.0% 0.0% 0.0% 0.0%

OSE Immunotherapeutics Buy TP EUR 9.00
76 keplercheuvreux.com
Research ratings and important disclosures The term "KEPLER CHEUVREUX" shall, unless the context otherwise requires, mean each of KEPLER CHEUVREUX and its affiliates, subsidiaries and related companies
(see “Regulators” table below).
The investment recommendation(s) referred to in this report was (were) completed on 16/02/2017 17:34 (GMT) and was first disseminated on 20/02/2017 6:18
(GMT).
Prices in this report are taken as of the previous day’s close (to the date of this report) on the home market unless otherwise stated.
Disclosure checklist - Potential conflict of interests Stock ISIN Disclosure (See Below) Currency Price
Novartis CH0012005267 nothing to disclose CHF 75.80
OSE Immunotherapeutics FR0012127173 8 EUR 6.71
Roche CH0012032048 nothing to disclose CHF 241.50
Sanofi FR0000120578 nothing to disclose EUR 81.20
Source: Factset closing prices of 15/02/2017
Companies mentioned Stock Disclosure (See Below)
Abbvie nothing to disclose
Amgen nothing to disclose
Arena pharmaceutical nothing to disclose
BMS nothing to disclose
Celgene nothing to disclose
Chemocentryx nothing to disclose
Compugen nothing to disclose
Galapagos nothing to disclose
Gilead nothing to disclose
immune pharmaceuticals nothing to disclose
Index pharmaceutical nothing to disclose
J&J nothing to disclose
Eli Lilly nothing to disclose
Kerck and co nothing to disclose
Merck KGaA nothing to disclose
Oncotherapy science nothing to disclose
Pfizer nothing to disclose
Protalix nothing to disclose
Regeneron nothing to disclose
Shire nothing to disclose
Trillium Therapeutics nothing to disclose
Key: 1. KEPLER CHEUVREUX holds or owns or controls 5% or more of the issued share capital of this company; 2. The company, or its major shareholder, directly or indirectly, holds or owns or controls 5% or more of the issued share capital of KEPLER CHEUVREUX; 3. KEPLER CHEUVREUX is or may be regularly carrying out proprietary trading in equity securities of this company; 4. KEPLER CHEUVREUX has been lead manager or co-lead manager in a public offering of the issuer’s financial instruments during the last twelve months; 5. KEPLER CHEUVREUX is a market maker in the issuer’s financial instruments; 6. KEPLER CHEUVREUX is a liquidity provider in relation to price stabilisation activities for the issuer to provide liquidity in such instruments; 7. KEPLER CHEUVREUX acts as a corporate broker or a sponsor or a sponsor specialist (in accordance with the local regulations) to this company; 8. KEPLER CHEUVREUX and the issuer have agreed that KEPLER CHEUVREUX will produce and disseminate investment research on the said issuer as a service to the issuer; 9. KEPLER CHEUVREUX has received compensation from this company for the provision of investment banking or financial advisory services within the previous twelve months; 10. KEPLER CHEUVREUX may expect to receive or intend to seek compensation for investment banking services from this company in the next three months; 11. The author of, or an individual who assisted in the preparation of, this report (or a member of his/her household), or a person who although not involved in the preparation of the report had or could reasonably be expected to have access to the substance of the report prior to its dissemination has a direct ownership position in securities issued by this company; 12. An employee of KEPLER CHEUVREUX serves on the board of directors of this company; 13. As at the end of the month immediately preceding the date of publication of the research report Kepler Capital Markets, Inc. beneficially owned 1% or more of a class of common equity securities of the subject company; 14. KEPLER CHEUVREUX and UniCredit Bank AG have entered into a Co-operation Agreement to form a strategic alliance in connection with certain services including services connected to investment banking transactions. UniCredit Bank AG provides investment banking services to this issuer in return for which UniCredit Bank AG has received a consideration or a promise of consideration. Separately, through the Co-operation Agreement with UniCredit Bank AG for services provided by KEPLER CHEUVREUX in connection with such activities, KEPLER CHEUVREUX has also a received consideration or a promise of a consideration in accordance with the general terms of the Co-operation Agreement; 15. KEPLER CHEUVREUX and Crédit Agricole Corporate & Investment Bank (“CACIB”) have entered into a Co-operation Agreement to form a strategic alliance in connection with certain services including services connected to investment banking transactions. CACIB provides investment banking services to this issuer in return for which CACIB has received a consideration or a promise of consideration. Separately, through the Co-operation Agreement with CACIB for services provided by KEPLER CHEUVREUX in connection with such activities, KEPLER CHEUVREUX has also received a consideration or a promise of a consideration in accordance with the general terms of the Co-operation Agreement; 16. UniCredit Bank AG holds or owns or controls 5% or more of the issued share capital of KEPLER CHEUVREUX. UniCredit Bank AG provides investment banking services to this issuer in return for which UniCredit Bank AG has received a consideration or a promise of consideration; 17. CACIB holds or owns or controls 15% of more of the issued share capital of KEPLER CHEUVREUX. CACIB provides investment banking services to this issuer in return for which CACIB has received a consideration or a promise of consideration; 18. A representative of UniCredit Bank AG serves on the board of directors of KEPLER CHEUVREUX; 19. Two representatives of CACIB serve on the board of directors of KEPLER CHEUVREUX. CACIB provides investment banking services to this issuer in return for which CACIB has received a consideration or a promise of consideration; 20. The recommendation presented in this document was disclosed to the issuer prior to publication and dissemination and was subsequently amended; 21. KEPLER CHEUVREUX has received or expected to receive compensation from this company for the provision of services of investments firms set out in Sections A and B of Annex I of Directive 2014/65/EU of the European Parliament and of the Council within the previous twelve months; 22. KEPLER CHEUVREUX owns a net long position exceeding the threshold of 0,5 % of the total issued share capital of the issuer; 23. KEPLER CHEUVREUX owns a net short position exceeding the threshold of 0,5 % of the total issued share capital of the issuer; 24. KEPLER CHEUVREUX and Rabobank (Coöperatieve Rabobank U.A.) have entered into a Co-operation Agreement to form a strategic alliance in connection with certain services including services connected to investment banking transactions. Rabobank provides investment banking services to this issuer in return for which Rabobank will receive a consideration or a promise of consideration. Separately, through a Co-operation Agreement between with KEPLER CHEUVREUX and Rabobank, KEPLER CHEUVREUX provides services in connection with such activities. KEPLER CHEUVREUX also receives a consideration or a promise of a consideration in accordance with the general terms of the Co-operation Agreement; 25. Rabobank (Coöperatieve Rabobank U.A.) holds or owns or controls 5% or more

OSE Immunotherapeutics Buy TP EUR 9.00
77 keplercheuvreux.com
of the issued share capital of Kepler Cheuvreux. Rabobank provides investment banking services to this issuer in return for which Rabobank has received a consideration or a promise of consideration; 26. A representative of Rabobank (Coöperatieve Rabobank U.A.) serves on the board of directors of KEPLER CHEUVREUX.
Organizational and administrative arrangements to avoid and prevent conflicts of interests KEPLER CHEUVREUX promotes and disseminates independent investment research and have implemented written procedures designed to identify and manage
potential conflicts of interest that arise in connection with its research business, which are available upon request. The KEPLER CHEUVREUX research analysts and
other staff involved in issuing and disseminating research reports operate independently of KEPLER CHEUVREUX Investment Banking business. Information barriers
and procedures are in place between the research analysts and staff involved in securities trading for the account of KEPLER CHEUVREUX or clients to ensure that price
sensitive information is handled according to applicable laws and regulations.
It is Kepler Cheuvreux’ policy not to disclose the rating to the issuer before publication and dissemination. Nevertheless, this document, in whole or in part, and with the
exclusion of ratings, target prices and any other information that could lead to determine its valuation, may have been provided to the issuer prior to publication and
dissemination, solely with the aim of verifying factual accuracy.
Please refer to www.keplercheuvreux.com for further information relating to research and conflict of interest management.
Analyst disclosures The functional job title of the person(s) responsible for the recommendations contained in this report is Equity/Credit Research Analyst unless otherwise stated on the cover.
Name of the Research Analyst(s): Thomas Guillot
Regulation AC - Analyst Certification: Each Equity/Credit Research Analyst(s) listed on the front-page of this report, principally responsible for the preparation and content of all or any identified portion of this research report hereby certifies that, with respect to each issuer or security or any identified portion of the report with respect to an issuer or security that the equity research analyst covers in this research report, all of the views expressed in this research report accurately reflect their personal views about those issuer(s) or securities. Each Equity/Credit Research Analyst(s) also certifies that no part of their compensation was, is, or will be, directly or indirectly, related to the specific recommendation(s) or view(s) expressed by that equity research analyst in this research report.
Each Equity/Credit Research Analyst certifies that he is acting independently and impartially from KEPLER CHEUVREUX sharehold ers, directors and is not affected by any current or potential conflict of interest that may arise from any KEPLER CHEUVREUX activities.
Analyst Compensation: The research analyst(s) primarily responsible for the preparation of the content of the research report attest that no part of the analyst’s(s’) compensation was, is or will be, directly or indirectly, related to the specific recommendations expressed by the research analyst(s) in the research report. The research analyst’s(s’) compensation is, however, determined by the overall economic performance of KEPLER CHEUVREUX.
Registration of non-US Analysts: Unless otherwise noted, the non-US analysts listed on the front of this report are employees of KEPLER CHEUVREUX, which is a non-US affiliate and parent company of Kepler Capital Markets, Inc. a SEC registered and FINRA member broker-dealer. Equity/Credit Research Analysts employed by KEPLER CHEUVREUX, are not registered/qualified as research analysts under FINRA/NYSE rules, may not be associated persons of Kepler Capital Markets, Inc. and may not be subject to NASD Rule 2711 and NYSE Rule 472 restrictions on communications with covered companies, public appearances, and trading securities held by a research analyst account.
Rating ratio Kepler Cheuvreux Q4 2016
Rating Breakdown A B
Buy 52% 57%
Hold 32% 33%
Reduce 15% 6%
Not Rated/Under Review/Accept Offer 2% 4%
Total 100% 100%
Source: Kepler Cheuvreux A: % of all research recommendations B: % of issuers to which material services of investment firms are supplied
12 months rating history The below table shows the history of recommendations and target prices changes issued by KEPLER CHEUVREUX research department (Equity and Credit) over a 12 months period.
Company Name Date Business Line Rating Target Price Closing Price
Novartis (CHF) 12/05/2016 07:24 Equity Research Not Rated 0.00 73.25
07/07/2016 09:47 Equity Research Buy 93.00 79.60
11/08/2016 06:27 Equity Research Buy 92.00 80.45
05/09/2016 06:17 Equity Research Buy 94.00 77.80
26/10/2016 06:39 Equity Research Buy 92.00 72.55
13/01/2017 08:37 Equity Research Buy 90.00 72.80
Roche (CHF) 12/05/2016 07:24 Equity Research Not Rated 0.00 244.00
07/07/2016 09:47 Equity Research Hold 242.00 251.40
22/07/2016 06:15 Equity Research Hold 240.00 250.00
21/10/2016 08:54 Equity Research Hold 238.00 232.50
Sanofi (EUR) 12/05/2016 07:24 Equity Research Not Rated 0.00 69.49
07/07/2016 09:47 Equity Research Buy 91.00 73.71
11/08/2016 06:25 Equity Research Buy 89.00 71.21
03/02/2017 06:52 Equity Research Buy 87.00 74.98
15/02/2017 08:32 Equity Research Buy 88.00 80.50
Credit research does not issue target prices. Left intentionally blank.
Please refer to the following link https://research.keplercheuvreux.com/app/disclosure for a full list of investment recommendations issued over the last 12 months
by the author(s) and contributor(s) of this report on any financial instruments.
Equity research
Rating system KEPLER CHEUVREUX equity research ratings and target prices are issued in absolute terms, not relative to any given benchmark. A rating on a stock is set after assessing the twelve months expected upside or downside of the stock derived from the analyst’s fair value (target price) and in the light of the risk profile of the company. Ratings are defined as follows:
Buy: The minimum expected upside is 10% over next 12 months (the minimum required upside could be higher in light of the company’s risk profile).

OSE Immunotherapeutics Buy TP EUR 9.00
78 keplercheuvreux.com
Hold: The expected upside is below 10% (the expected upside could be higher in light of the company’s risk profile).
Reduce: There is an expected downside.
Accept offer: In the context of a total or partial take-over bid, squeeze-out or similar share purchase proposals, the offer price is considered to be fairly valuing the shares.
Reject offer: In the context of a total or partial take-over bid, squeeze-out or similar share purchase proposals, the offered price is considered to be undervaluing the shares.
Under review: An event occurred with an expected significant impact on our target price and we cannot issue a recommendation before having processed that new information and/or without a new share price reference.
Not rated: The stock is not covered.
Restricted: A recommendation, target price and/or financial forecast is not disclosed further to compliance and/or other regulatory considerations.
Due to share prices volatility, ratings and target prices may occasionally and temporarily be inconsistent with the above definition.
Valuation methodology and risks Unless otherwise stated in this report, target prices and investment recommendations are determined based on fundamental research methodologies and relies on
commonly used valuation methodologies such as Discounted Cash Flow (DCF), valuation multiples comparison with history and peers, Dividend Discount Model (DDM).
Valuation methodologies and models can be highly dependent on macroeconomic factors (such as the price of commodities, exchange rates and interest rates) as well as
other external factors including taxation, regulation and geopolitical changes (such as tax policy changes, strikes or war). In addition, investors’ confidence and market
sentiment can affect the valuation of companies. The valuation is also based on expectations that might change rapidly and without notice, depending on developments
specific to individual industries. Whichever valuation method is used there is a significant risk that the target price will not be achieved within the expected timeframe.
Unless otherwise stated, models used are proprietary. Additional information about the proprietary models used in this report is accessible on request.
Kepler Cheuvreux’ equity research policy is to update research rating when it deems appropriate in the light of new findings, markets development and any relevant
information that can impact the analyst’s view and opinion.
Credit research
Rating system (issuer or instrument level) Buy: The analyst has a positive conviction either in absolute or relative valuation terms and/or expects a tightening of the issuer’s debt securities spread over a 6 months period.
Hold: The analyst has a stable credit fundamental opinion on the issuer and/or performances of the debt securities over a 6 months period.
Sell: The analyst expects of a widening of the credit spread to some or all debt securities of the issuer and/or a negative fundamental view over a 6 months period.
Not covered: Kepler Cheuvreux’ credit research team does not provide formal, continuous coverage of this issuer and has not assigned a rating to the issuer.
Restricted: A recommendation, target price and/or financial forecast is not disclosed further to compliance and/or other regulatory considerations.
Recommendations on interest bearing securities mostly focus on the credit spread and on the rating views and methodologies of recognized agencies (S&P, Moody’s and
Fitch). Ratings and recommendations may differ for a single issuer according the maturity profile, subordination or market valuation of interest bearing securities.
Valuation methodology and risks Unless otherwise stated in this report, recommendations produced on companies covered by KEPLER CHEUVREUX credit research, rely on fundamental analysis
combined with a market approach of the interest bearing securities valuations. The methodology employed to assign recommendations is based on the analyst
fundamental evaluation of the groups' operating and financial profiles adjusted by credit specific elements.
Valuation methodologies and models can be highly dependent on macroeconomic factors (such as the price of commodities, exchange rates and interest rates) as well as
other external factors including taxation, regulation and geopolitical changes (such as tax policy changes, strikes or war) and also on methodologies’ changes of
recognized agencies. In addition, investors’ confidence and market sentiment can affect the valuation of companies. The valuation is also based on expectations that
might change rapidly and without notice, depending on developments specific to individual industries.
Unless otherwise stated, models used are proprietary. If nothing is indicated to the contrary, all figures are unaudited. Additional information about the proprietary
models used in this report is accessible on request.
Kepler Cheuvreux’ credit research policy is to update research rating when it deems appropriate in the light of new findings, markets development and any relevant
information that can impact the analyst’s view and opinion.
Regulators
Location Regulator Abbreviation
KEPLER CHEUVREUX S.A - France Autorité des Marchés Financiers AMF
KEPLER CHEUVREUX, Sucursal en España Comisión Nacional del Mercado de Valores CNMV
KEPLER CHEUVREUX, Frankfurt branch Bundesanstalt für Finanzdienstleistungsaufsicht BaFin
KEPLER CHEUVREUX, Milan branch Commissione Nazionale per le Società e la Borsa CONSOB
KEPLER CHEUVREUX, Amsterdam branch Autoriteit Financiële Markten AFM
Kepler Capital Markets SA - Switzerland, Zurich branch Swiss Financial Market Supervisory Authority FINMA
Kepler Capital Markets, Inc. Financial Industry Regulatory Authority FINRA
KEPLER CHEUVREUX, London branch Financial Conduct Authority FCA
KEPLER CHEUVREUX, Vienna branch Austrian Financial Services Authority FMA
KEPLER CHEUVREUX, Stockholm Branch Finansinspektionen FI
KEPLER CHEUVREUX is authorised and regulated by both Autorité de Contrôle Prudentiel and Autorité des Marchés Financiers.

OSE Immunotherapeutics Buy TP EUR 9.00
79 keplercheuvreux.com
Legal and disclosure information Other disclosures This product is not for distribution to retail clients.
The information contained in this publication was obtained from various publicly available sources believed to be reliable, but has not been independently verified by KEPLER CHEUVREUX. KEPLER CHEUVREUX does not warrant the completeness or accuracy of such information and does not accept any liability with respect to the accuracy or completeness of such information, except to the extent required by applicable law.
This publication is a brief summary and does not purport to contain all available information on the subjects covered. Further information may be available on request.
This publication is for information purposes only and shall not be construed as an offer or solicitation for the subscription or purchase or sale of any securities, or as an invitation, inducement or intermediation for the sale, subscription or purchase of any securities, or for engaging in any other transaction.
Any opinions, projections, forecasts or estimates in this report are those of the author only, who has acted with a high degree of expertise. They reflect only the current views of the author at the date of this report and are subject to change without notice. KEPLER CHEUVREUX has no obligation to update, modify or amend this publication or to otherwise notify a reader or recipient of this publication in the event that any matter, opinion, projection, forecast or estimate contained herein, changes or subsequently becomes inaccurate, or if research on the subject company is withdrawn. The analysis, opinions, projections, forecasts and estimates expressed in this report were in no way affected or influenced by the issuer. The author of this publication benefits financially from the overall success of KEPLER CHEUVREUX.
The investments referred to in this publication may not be suitable for all recipients. Recipients are urged to base their investment decisions upon their own appropriate investigations that they deem necessary. Any loss or other consequence arising from the use of the material contained in this publication shall be the sole and exclusive responsibility of the investor and KEPLER CHEUVREUX accepts no liability for any such loss or consequence. In the event of any doubt about any investment, recipients should contact their own investment, legal and/or tax advisers to seek advice regarding the appropriateness of investing. Some of the investments mentioned in this publication may not be readily liquid investments. Consequently it may be difficult to sell or realise such investments. The past is not necessarily a guide to future performance of an investment. The value of investments and the income derived from them may fall as well as rise and investors may not get back the amount invested. Some investments discussed in this publication may have a high level of volatility. High volatility investments may experience sudden and large falls in their value which may cause losses. International investing includes risks related to political and economic uncertainties of foreign countries, as well as currency risk.
To the extent permitted by applicable law, no liability whatsoever is accepted for any direct or consequential loss, damages, costs or prejudices whatsoever arising from the use of this publication or its contents.
Country and region disclosures United Kingdom: This document is for persons who are Eligible Counterparties or Professional Clients only and is exempt from the general restriction in section 21 of the Financial Services and Markets Act 2000 on the communication of invitations or inducements to engage in investment activity on the grounds that it is being distributed in the United Kingdom only to persons of a kind described in Articles 19(5) (Investment professionals) and 49(2) (High net worth companies, unincorporated associations, etc.) of the Financial Services and Markets Act 2000 (Financial Promotion) Order 2005 (as amended). It is not i ntended to be distributed or passed on, directly or indirectly, to any other class of persons. Any investment to which this document relates is available only to such persons, and other classes of person should not rely on this document.
United States: This communication is only intended for, and will only be distributed to, persons residing in any jurisdictions where such distribution or availability would not be contrary to local law or regulation. This communication must not be acted upon or relied on by persons in any jurisdiction other than in accordance with local law or regulation and where such person is an investment professional with the requisite sophistication to understand an investment in such securities of the type communicated and assume the risks associated therewith.
This communication is confidential and is intended solely for the addressee. It is not to be forwarded to any other person or copied without the permission of the sender. This communication is provided for information only. It is not a personal recommendation or an offer to sell or a solicitation to buy the securities mentioned. Investors should obtain independent professional advice before making an investment.
Notice to U.S. Investors: This material is not for distribution in the United States, except to “major US institutional investors” as defined in SEC Rule 15a-6 ("Rule 15a-6"). KEPLER CHEUVREUX has entered into a 15a-6 Agreement with Kepler Capital Markets, Inc. ("KCM, Inc.”) which enables this report to be furnished to certain U.S. recipients in reliance on Rule 15a-6 through KCM, Inc.
Each U.S. recipient of this report represents and agrees, by virtue of its acceptance thereof, that it is a "major U.S. institutional investor" (as such term is defined in Rule 15a-6) and that it understands the risks involved in executing transactions in such securities. Any U.S. recipient of this report that wishes to discuss or receive additional information regarding any security or issuer mentioned herein, or engage in any transaction to purchase or sell or solicit or offer the purchase or sale of such securities, should contact a registered representative of KCM, Inc.
KCM, Inc. is a broker-dealer registered with the Securities and Exchange Commission (“SEC”) under the U.S. Securities Exchange Act of 1934, as amended, Member of the Financial Industry Regulatory Authority (“FINRA”) and Member of the Securities Investor Protection Corporation (“SIPC”). Pursuant to SEC Rule 15a-6, you must contact a Registered Representative of KCM, Inc. if you are seeking to execute a transaction in the securities discussed in this report. You can reach KCM, Inc. at 600 Lexington Avenue, New York, NY 10022, Compliance Department (212) 710-7625; Operations Department (212) 710-7606; Trading Desk (212) 710-7602. Further information is also available at www.keplercheuvreux.com. You may obtain information about SIPC, including the SIPC brochure, by contacting SIPC directly at 202-371-8300; website: http://www.sipc.org/.
KCM, Inc. is a wholly owned subsidiary of KEPLER CHEUVREUX. KEPLER CHEUVREUX , registered on the Paris Register of Companies with the number 413 064 841 (1997 B 10253), whose registered office is located at 112 avenue Kléber, 75016 Paris, is authorised and regulated by both Autorité de Contrôle Prudentiel (ACP) and Autorité des Marchés Financiers (AMF).
Nothing herein excludes or restricts any duty or liability to a customer that KCM, Inc. may have under applicable law. Investment products provided by or through KCM, Inc. are not insured by the Federal Deposit Insurance Corporation and are not deposits or other obligations of any insured depository institution, may lose value and are not guaranteed by the entity that published the research as disclosed on the front page and are not guaranteed by KCM, Inc.
Investing in non-U.S. Securities may entail certain risks. The securities referred to in this report and non-U.S. issuers may not be registered under the U.S. Securities Act of 1933, as amended, and the issuer of such securities may not be subject to U.S. reporting and/or other requirements. Rule 144A securities may be offered or sold only to persons in the U.S. who are Qualified Institutional Buyers within the meaning of Rule 144A under the Securities Act. The information available about non-U.S. companies may be limited, and non-U.S. companies are generally not subject to the same uniform auditing and reporting standards as U.S. companies. Securities of some non-U.S. companies may not be as liquid as securities of comparable U.S. companies. Securities discussed herein may be rated below investment grade and should therefore only be considered for inclusion in accounts qualified for speculative investment.
Analysts employed by KEPLER CHEUVREUX SA, a non-U.S. broker-dealer, are not required to take the FINRA analyst exam. The information contained in this report is intended solely for certain "major U.S. institutional investors" and may not be used or relied upon by any other person for any purpose. Such information is provided for informational purposes only and does not constitute a solicitation to buy or an offer to sell any securities under the Securities Act of 1933, as amended, or under any other U.S. federal or state securities laws, rules or regulations. The investment opportunities discussed in this report may be unsuitable for certain investors depending on their specific investment objectives, risk tolerance and financial position.

OSE Immunotherapeutics Buy TP EUR 9.00
80 keplercheuvreux.com
In jurisdictions where KCM, Inc. is not registered or licensed to trade in securities, or other financial products, transactions may be executed only in accordance with applicable law and legislation, which may vary from jurisdiction to jurisdiction and which may require that a transaction be made in accordance with applicable exemptions from registration or licensing requirements.
The information in this publication is based on sources believed to be reliable, but KCM, Inc. does not make any representation with respect to its completeness or accuracy. All opinions expressed herein reflect the author's judgment at the original time of publication, without regard to the date on which you may receive such information, and are subject to change without notice.
KCM, Inc. and/or its affiliates may have issued other reports that are inconsistent with, and reach different conclusions from, the information presented in this report. These publications reflect the different assumptions, views and analytical methods of the analysts who prepared them. Past performance should not be taken as an indication or guarantee of future performance, and no representation or warranty, express or implied, is provided in relation to future performance.
KCM, Inc. and any company affiliated with it may, with respect to any securities discussed herein: (a) take a long or short position and buy or sell such securities; (b) act as investment and/or commercial bankers for issuers of such securities; (c) act as market makers for such securities; (d) serve on the board of any issuer of such securities; and (e) act as paid consultant or advisor to any issuer. The information contained herein may include forward-looking statements within the meaning of U.S. federal securities laws that are subject to risks and uncertainties. Factors that could cause a company's actual results and financial condition to differ from expectations include, without limitation: political uncertainty, changes in general economic conditions that adversely affect the level of demand for the company's products or services, changes in foreign exchange markets, changes in international and domestic financial markets and in the competitive environment, and other factors relating to the foregoing. All forward-looking statements contained in this report are qualified in their entirety by this cautionary statement.
France: This publication is issued and distributed in accordance with Articles L.544-1 and seq and R. 621-30-1 of the Code Monétaire et Financier and with Articles 313-25 to 313-27 and 315-1 and seq of the General Regulation of the Autorité des Marchés Financiers (AMF).
Germany: This report must not be distributed to persons who are retail clients in the meaning of Sec. 31a para. 3 of the German Securities Trading Act (Wertpapierhandelsgesetz – “WpHG”). This report may be amended, supplemented or updated in such manner and as frequently as the author deems.
Italy: This document is issued by KEPLER CHEUVREUX Milan branch, authorised in France by the Autorité des Marchés Financiers (AMF) and the Autorité de Contrôle Prudentiel (ACP) and registered in Italy by the Commissione Nazionale per le Società e la Borsa (CONSOB) and is distributed by KEPLER CHEUVREUX. This document is for Eligible Counterparties or Professional Clients only as defined by the CONSOB Regulation 16190/2007 (art. 26 and art. 58).Other classes of persons should not rely on this document. Reports on issuers of financial instruments listed by Article 180, paragraph 1, letter a) of the Italian Consolidated Act on Financial Services (Legislative Decree No. 58 of 24/2/1998, as amended from time to time) must comply with the requirements envisaged by articles 69 to 69-novies of CONSOB Regulation 11971/1999. According to these provisions KEPLER CHEUVREUX warns on the significant interests of KEPLER CHEUVREUX indicated in Annex 1 hereof, confirms that there are not significant financial interests of KEPLER CHEUVREUX in relation to the securities object of this report as well as other circumstance or relationship with the issuer of the securities object of this report (including but not limited to conflict of interest, significant shareholdings held in or by the issuer and other significant interests held by KEPLER CHEUVREUX or other entities controlling or subject to control by KEPLER CHEUVREUX in relation to the issuer which may affect the impartiality of this document]. Equities discussed herein are covered on a continuous basis with regular reports at results release. Reports are released on the date shown on cover and distributed via print and email. KEPLER CHEUVREUX branch di Milano analysts is not affiliated with any professional groups or organisations. All estimates are by KEPLER CHEUVREUX unless otherwise stated.
Spain: This document is only intended for persons who are Eligible Counterparties or Professional Clients within the meaning of Article 78bis and Article 78ter of the Spanish Securities Market Act. It is not intended to be distributed or passed on, directly or indirectly, to any other class of persons. This report has been issued by KEPLER CHEUVREUX Sucursal en España registered in Spain by the Comisión Nacional del Mercado de Valores (CNMV) in the foreign investments firms registry and it has been distributed in Spain by it or by KEPLER CHEUVREUX authorised and regulated by both Autorité de Contrôle Prudentiel and Autorité des Marchés Financiers. There is no obligation to either register or file any report or any supplemental documentation or information with the CNMV. In accordance with the Spanish Securities Market Law (Ley del Mercado de Valores), there is no need for the CNMV to verify, authorise or carry out a compliance review of this document or related documentation, and no information needs to be provided.
Switzerland: This publication is intended to be distributed to professional investors in circumstances such that there is no public offer. This publication does not constitute a prospectus within the meaning of Articles 652a and 1156 of the Swiss Code of Obligations.
Canada: The information provided in this publication is not intended to be distributed or circulated in any manner in Canada and therefore should not be construed as any kind of financial recommendation or advice provided within the meaning of Canadian securities laws.
Other countries: Laws and regulations of other countries may also restrict the distribution of this report. Persons in possession of this document should inform themselves about possible legal restrictions and observe them accordingly.
None of the material, nor its content may be altered in anyway, transmitted to, copied or distributed to any other party, in whole or in part, unless otherwise agreed with KEPLER CHEUVREUX in writing.

Equity Research Local insight, European scale
keplercheuvreux.com
Pharma & biotech research team
Thomas Guillot Main author
+33 1 70 98 85 27
Arsène Guekam [email protected]
+33 1 70 81 57 56
Natalia Bobo [email protected]
+34 91 436 5165
Thomas Guillot is an Equity Research Analyst specialised in the Biotech and Medtech sectors. He joined Kepler Cheuvreux in September 2016. Prior to his appointment, he spent two years as a healthcare M&A analyst at Société Générale, where he advised large and specialty pharmaceutical companies as well as medtech. Previously, he was Equity Research Analyst assistant at Natixis from 2012 to 2014 where he covered the pan-European pharmaceutical sector. Thomas Guillot has a Master's degree in pharmaceutical science from the University of Rouen, in addition to a Master’s of Science in Management from the ESSEC business school in France.
David Evans Co-Head of European Pharmaceutials
+44 (0) 207 621 5197
Oliver Reinberg, CFA Head of Medtech & Services Research
+49 69 7569 140
Maja Pataki Head of Medtech Devices Research
+41 43 333 6623
Pierre Boucheny Head of French Research
+33 1 5365 3506
Mark Belsey, PhD Co-Head of European Pharmaceutials
+44 203 350 5032
Thomas Guillot [email protected]
+33 1 70 98 85 27
Europe
Amsterdam +31 20 573 06 66 Frankfurt +49 69 756 960 Geneva +41 22 361 5151 London +44 20 7621 5100 Madrid +34 914365100 Milan +39 02 85507 1 Paris +33 1 53 65 35 00 Stockholm +46 8 723 51 00 Vienna +43 1 537 124 147 Zurich +41 43 333 66 66
America & Asia
Boston +1 617 295 0100 New York +1 212 710 7600 San Francisco +1 415 255 9802