a golden period for cholecystectomy · gallbladder wall 7 mm ... the primary pathophysiology...
TRANSCRIPT

A Golden Period for Cholecystectomy
Fact or Myth ?
Marilyn Ng, MD
Dept. of Surgery M&M Conference
Downstate Medical Center
Aug 9, 2012
www.downstatesurgery.org

Case Presentation
36 yo woman with 1 day hx of
worsening RUQ pain
Nausea & episodes bilious emesis
No fevers, chills or LUTS
www.downstatesurgery.org

Case Presentation
PMHx: asthma, HTN, spina bifida,
hydrocephalus & seizure disorder
SHx: open appendectomy, VP
shunt placement, VP shunt
revision (‘87, ‘98)
SocHx: 6 kids; shelter
www.downstatesurgery.org

On Physical Exam
Vitals: normal
Skin: multiple abdominal scars
Abd: soft, ND, RUQ tenderness,
(+) Murphy’s sign, no hernias
Back: no CVAT
www.downstatesurgery.org

RUQ Sonogram
Gallbladder wall 7 mm thick
Pericholecystic fluid
Cholelithiasis
Common bile duct 4 mm
Acute cholecystitis
www.downstatesurgery.org

Labs
CBC: 8.2>12.1/38.8<355
BMP: 141/3.3/109/23/11/1<117
LFT: 7.7/4.4/25/14/83.0.3 A 102 L 59
U/A: normal
www.downstatesurgery.org

Open Cholecystectomy
RUQ subcostal incision
Loculated ascites
Distended intrahepatic gallbladder
Jackson – Pratt drain
www.downstatesurgery.org

Hospital Course
POD#0:
Advanced to regular diet
JP drainage serosanguinous
POD#1:
JP drain removed
SW case review & discharged to shelter
www.downstatesurgery.org

Timing of Cholecystectomy
Acute cholecystitis (AC)
History of AC management
Timing of cholecystectomy
Conclusion
www.downstatesurgery.org
U.S. Epidemiology
20 million U.S. adults have gallstones
1 - 4% become symptomatic each year
Acute cholecystitis develops in 20% of untreated patients
500,000 cholecystectomies per year
www.downstatesurgery.org

Diagnosis
RUQ abd pain, fever, leukocytosis
Murphy’s sign
Sonographic diagnosis
www.downstatesurgery.org

AC Pathophysiology
Early stages edema & hyperemia
Later stages adhesions, fibrosis, necrosis
Triangle of Calot
www.downstatesurgery.org

Management
Supportive - IV fluid & analgesia
Antibiotics
Gram-negative aerobes
Anaerobes
Surgery is only definitive treatment
www.downstatesurgery.org

History of Cholecystectomy
1882 – 1st successful open cholecystectomy (OC) by Dr. Langenbuch
1st half 20th century – Delayed open cholecystectomy
www.downstatesurgery.org

History of Cholecystectomy
1966 – Dr. Essenhigh advocated superiority of early OC
1985 – 1st laparoscopic cholecystectomy (LC) by Dr. Muhe
www.downstatesurgery.org

Work Leave (days)
Laparoscopic vs. Open
No observed difference in mortality, complications & operative time
Hos
pita
l St
ay (
days
) www.downstatesurgery.org

Timing of Surgery
Early surgery – 24 hrs to 7 days of onset of symptoms
Delayed surgery – at least 6 weeks after symptoms settled
Timing of open cholecystectomy translate similarly with laparoscopy?
www.downstatesurgery.org

** Clinically significant !
Golden 72 Hours
NS
(2/16)
(6/19) (7/25)
Koo et al. Arch Surg, 1996
www.downstatesurgery.org

Lo et al.
NS P=0.174
NS P=0.07
** P<0.001
** P<0.001
Lo et al. Ann Surg, 1998
www.downstatesurgery.org

Secondary Outcomes
Operating time
CBD stones
Hospital stay
Work days lost
Quality of life
Cochrane Review 2010
Primary Outcomes
Mortality
Surgery-related morbidity
Wait-time complications
Conversion to OC
www.downstatesurgery.org
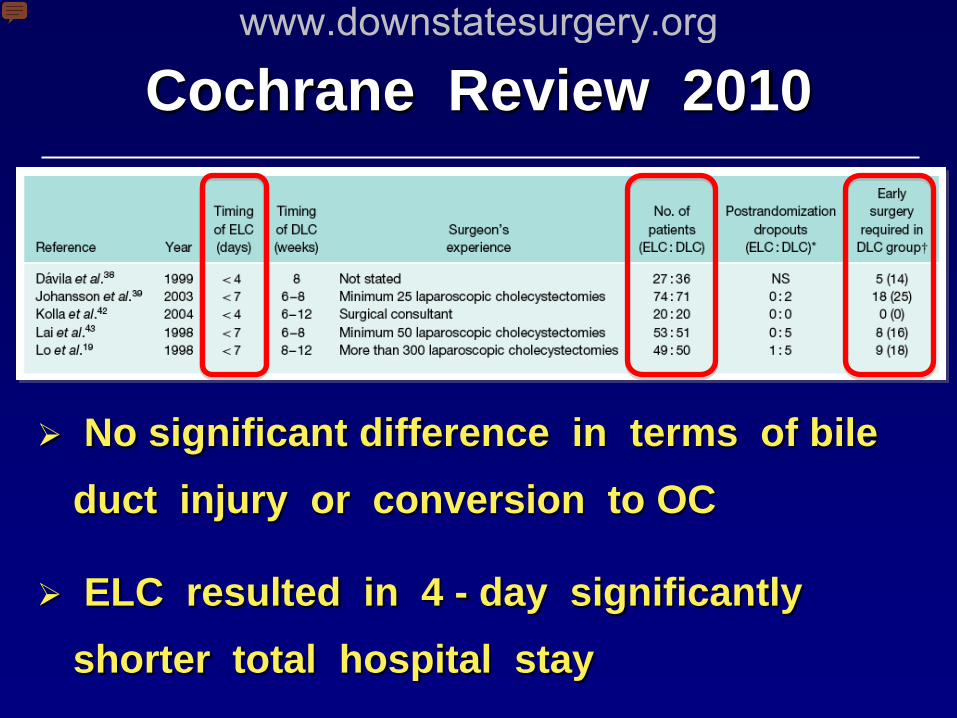
Cochrane Review 2010
No significant difference in terms of bile duct injury or conversion to OC
ELC resulted in 4 - day significantly shorter total hospital stay
www.downstatesurgery.org

Objective: Compare various outcomes of LC for AC at different time points after hospital admission
Study Design: Large, prospective cohort
6 subgroups based on time of surgery
www.downstatesurgery.org

www.downstatesurgery.org

11.9 %
27.9 % *
* P < 0.001
www.downstatesurgery.org

5.7 % 13 % *
* P < 0.001
0.9 % 3 % *
* P < 0.001
www.downstatesurgery.org
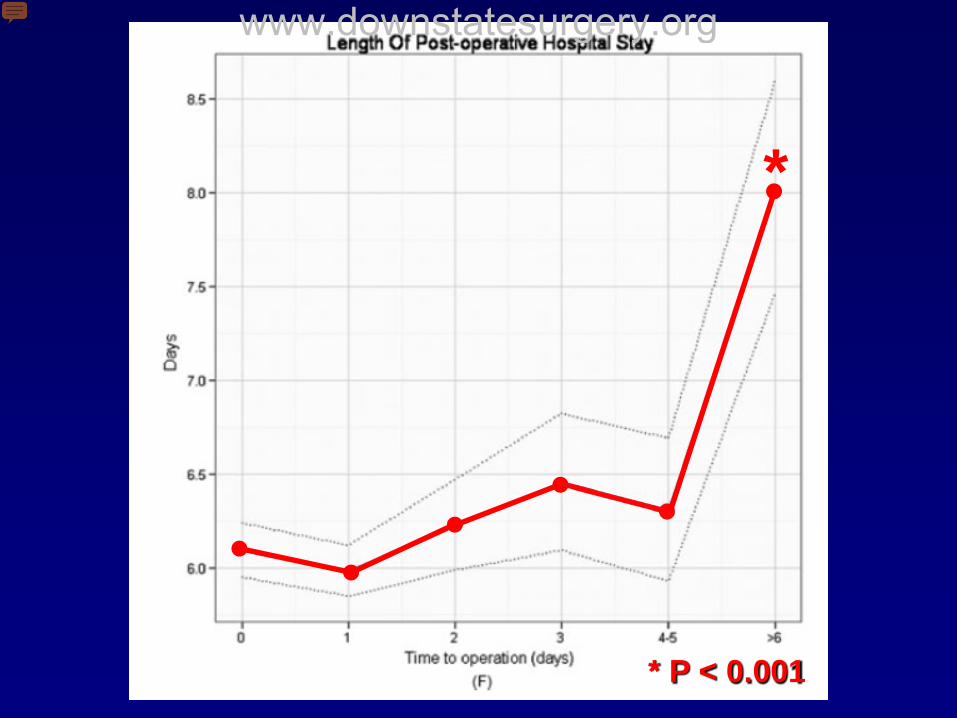
* P < 0.001
*
www.downstatesurgery.org
www.downstatesurgery.org

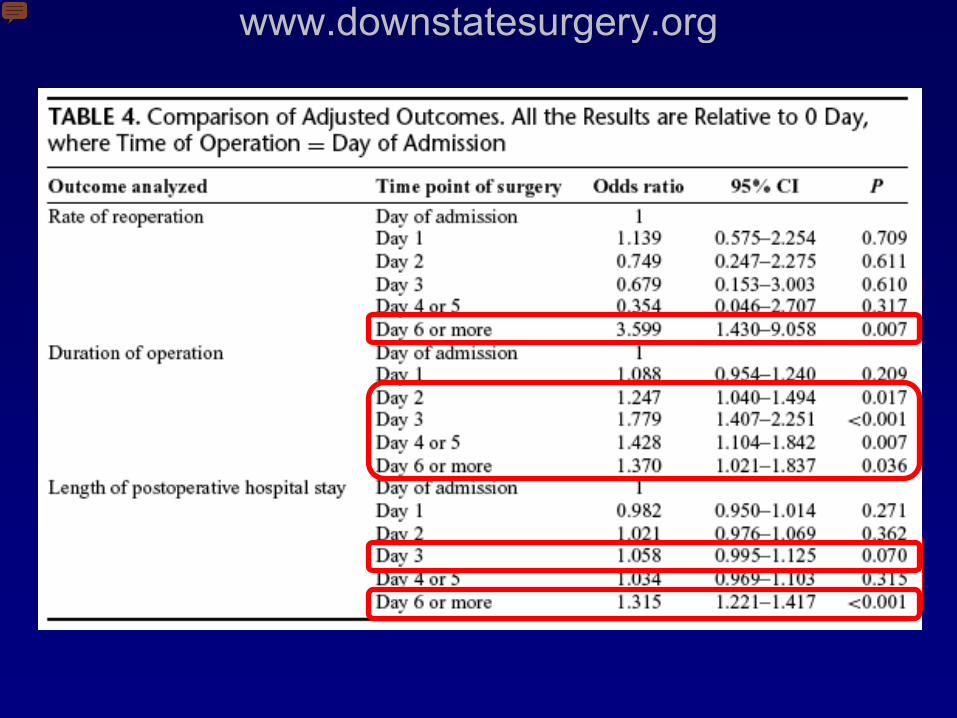
Banz et al - Conclusions
Largest population-based study to date
Delayed LC for AC has no advantage
Early LC avoids increase in:
Conversion rate
Post-operative complications
Postoperative hospital stay
www.downstatesurgery.org

Summary
Know your patient (ASA class)
OC - standard from which to compare
Golden 72 hrs for better outcomes
Converting to open is not a failure
Earlier LC is safe & shortens LOS
Golden 24 hrs for better outcomes
www.downstatesurgery.org

Which of the following is an event in the pathophysiology of acute calculus cholecystitis ?
A. Increased biliary lysolecithin
B. Gallbladder ischemia
C. Bacterial infection
D. Prostaglandin depletion
E. CCK receptor depletion
www.downstatesurgery.org

Which is the preferred treatment of acute calculus cholecystitis?
A. Early laparoscopic cholecystectomy
B. Delayed laparoscopic cholecystectomy
C. Early open cholecystectomy
D. Delayed open cholecystectomy
E. Intravenous antibiotics
www.downstatesurgery.org

Which time-point group in Banz et al. study had fewer overall complications and shorter length of stay?
A. Day of admission
B. Day 1
C. Day 2
D. Day 3
E. Day 4-5
F. Day > 6
www.downstatesurgery.org
References Banz et al. Population-based analysis of 4113 patients wth acute
cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy Ann Surg 2011;254:964-970
Current Surgical Therapy, 10th Ed, pp 408-412
Gurusamy K et al. Meta-analysis of randomized controlled trials on the safety and effectiveness of early versus delayed larparoscopic cholecystectomy for acute cholecystitis. Br J Surg 2010; 97: 141-150
Keus F et al. Laparoscopic versus open cholecystectomy for patient with symptomatic cholecystolithiasis. Cochrane Database Syst Rev. 2006 18;(4): CD006231
www.downstatesurgery.org

References Koo KP et al. Laparoscopic cholecystectomy in acute cholecysitis:
What is the optimal time for operation? Arch Surg 1996; 131:540-545
Lo CM et al. Prospective randomized study of early versus delayed laparoscopic cholecystectomy for acute cholecystitis. Ann Surg 1998 (227)4:461-467.
Reynolds W Jr. The first laparoscopic cholecystectomy. JSLS 2001 (5)1:89-94.
Strasberg SM. Acute calculus cholecystitis. N Engl J Med 2008: 358;2804-2811.
www.downstatesurgery.org