a guide for patients and their loved ones · 2 introduction this guide contains information about...
TRANSCRIPT

1
A guide for patients and their loved ones
4100336 (17-07)

2
Introduction This guide contains information about your surgery and your hospital stay. It aims to increase your understanding, prepare you for your surgery, allow you to actively participate in your recovery and give you daily goals to achieve.
The iERAS Program: Best practices for recovery
The goal of the program is to improve your recovery so you can go home faster. It also aims to improve your satisfaction with the care you receive.
The iERAS program involves several academic hospitals in Ontario. It counts on the participation of surgeons, anesthetists, nurses, dietitians, physiotherapists and other members of your care team who work together to provide you with the best possible care.
As part of this program, we want to collect some information about your surgery and your recovery to assess the success of the program. This guide contains pages on which we would like you to keep track of your activities and diet every day during your hospital stay. Your nurse will help you answer these questions. We also ask you to answer a brief questionnaire on preparations before your stay in the hospital. Give us these pages before leaving to return home.
We thank you in advance for your participation in the program and we wish you a pleasant stay.

3
Table of content
The Bowel ...................................................................................................................... 4
Bowel Surgery ............................................................................................................... 4
Before Your Surgery ...................................................................................................... 5
Day Before and Morning of Your Surgery ...................................................................... 7
Le matin de votre chirurgie .................................................. Erreur ! Signet non défini. Your Surgery ................................................................................................................ 10
After Your Surgery: In the recovery room .................................................................... 11
While You are in The Hospital ..................................................................................... 13
Your Checklist before you leave to go home ............................................................... 20
What you need to know before you leave the hospital ................................................ 21
At Home....................................................................................................................... 22
My Follow-up Appointment .......................................................................................... 23
My Activity Log ............................................................................................................ 23
WARNING
This guide does not replace the advices provided by your healthcare team.
Consult your healthcare team to know if the information contained in this guide suits your situation.
The content of this guide was prepared by the iERAS program and the McGill University Health Centre and adapted by Hôpital Montfort.
4
The bowel When eating, food passes from your mouth, through the esophagus into your stomach. From there it passes into the small bowel (small intestine). This is where your food and nutrients are absorbed.
What is left of the food then goes to the large bowel (large intestine), which is about 6 feet long. This is where the fluid is absorbed from the food and stool is formed (your bowel movement). The stool is then stored in your rectum, until it is passed out of your body through the anus.
Bowel surgery Bowel surgery (also known as colorectal surgery) is the removal of the diseased section of the bowel between your stomach and your anus.
Your surgery can be done in 2 ways:
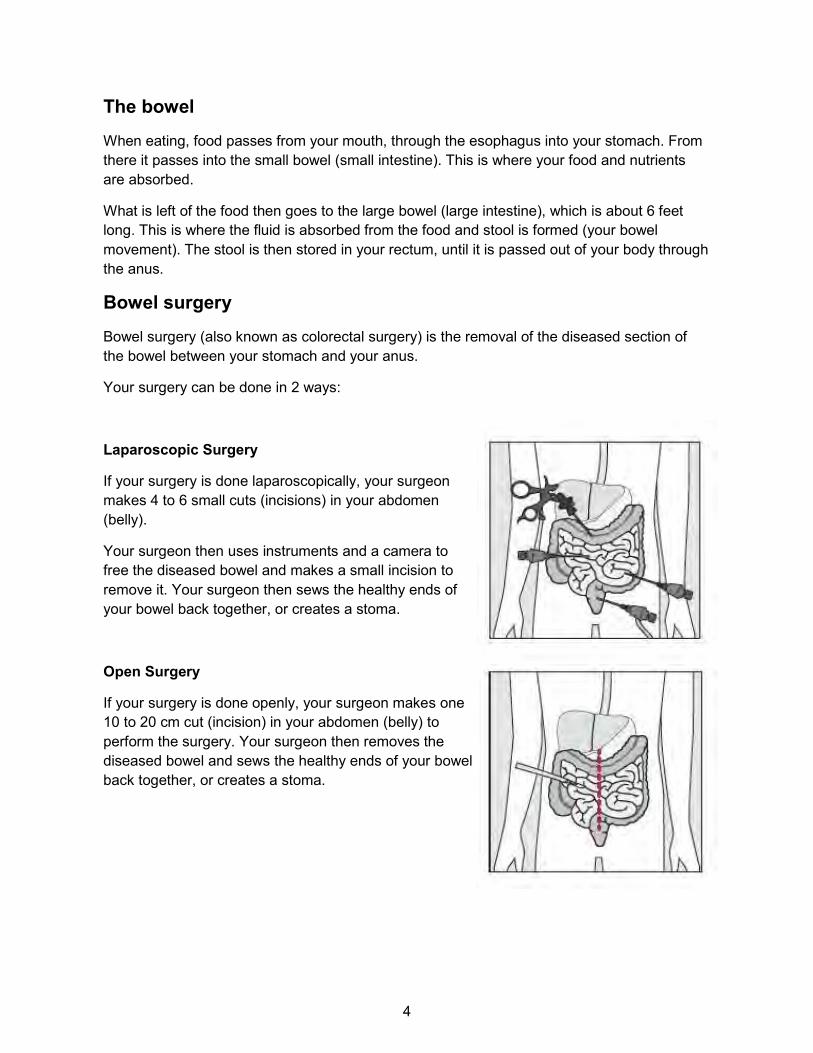
Laparoscopic Surgery
If your surgery is done laparoscopically, your surgeon makes 4 to 6 small cuts (incisions) in your abdomen (belly).
Your surgeon then uses instruments and a camera to free the diseased bowel and makes a small incision to remove it. Your surgeon then sews the healthy ends of your bowel back together, or creates a stoma.
Open Surgery
If your surgery is done openly, your surgeon makes one 10 to 20 cm cut (incision) in your abdomen (belly) to perform the surgery. Your surgeon then removes the diseased bowel and sews the healthy ends of your bowel back together, or creates a stoma.

5
Quitting smoking 3 weeks before your surgery can
decrease breathing problems, chances of infection
after surgery and favor your recovery.
Talk to your healthcare team about quitting smoking.
Before your surgery
Things to do to prepare yourself
• Move and exercise. • Do not drink alcohol or smoke for 24 hours before your surgery. Alcohol can interact
with some medications. Tell your healthcare team if you need help to stop smoking. • Make sure that everything is ready for you when you get home after your surgery. Fill
your freezer and cupboards with easy to prepare meals so that you will not have to go to the grocery store.
• You should be able to walk, eat and care for yourself as usual, but you might need some help from friends and family when you first get home from the hospital.
• Tell your nurse if you are worried concerning your return home • You will not be able to drive a vehicle for the 24 hours following your surgery. Plan for
a means of transportation to return home. • You must be accompanied back home and someone should stay with you for the 24
hours following your surgery. • If you are having a surgery to your colon and there is no complication you should
leave to go home 3 days after the intervention. • If you are having a surgery to your rectum and there is no complication you should
leave to go home 4 days after the intervention.
You may need help with these activities after your surgery: • Personal hygiene • Making meals • Laundry and cleaning • Driving
• Paying bills • Caring for pets • Watering plants
6
Do not remove any body hair before your surgery.
Doing so can increase your chance of getting an
infection. If hair needs to be removed for your surgery,
a clipper will be used once you get to the hospital.
Visiting the pre-admission clinic
You will be seen at the pre-admission clinic several days or weeks before your surgery. This is a place where information is shared: we will learn more about you and your health, and you will learn more about your surgery. You will be seen by a nurse, possibly an anesthesiologist (pain doctor) and other doctors if needed.
Speak with your nurse in pre-admission if you have questions concerning what you can bring to the hospital when you come in for surgery.
A nurse will go over the following with you: • Medications: Your past medical history and your current medications. A list of non-
prescribed medication including natural products. Bring a recent list of your actual medication with you
• Bowel preparation: Your nurse will let you know if you need or not a bowel preparation before your surgery
• Body cleansing: Do not remove any body hair before your surgery (no waxing, shaving or clipping). Doing so can increase your risk of infection. You may be asked to shower with special soap before your surgery.
• Diet: When you should stop eating and drinking before your surgery and what and when you can eat after surgery.
• Activity level: How much you should be moving around after your surgery. • Going home after surgery: You will be asked about your home and any supports you
already have in place (family, friends). This will help to plan for your return home with the services you may need.
Your anesthesiologist will go over the choices you have to control pain and what type of anesthesia will be administered to you.

7
Only drink clear liquids.
Stop drinking 2 hrs before your surgery, or when you
leave home to get to the hospital.
If your surgery is at 11 a.m., stop drinking at 9 a.m.
Day before and morning of your surgery • You can eat solid foods until 8 hours prior to your surgery (unless you had a bowel
preparation, in which case, consult the “Laxative before your surgery” section, on page 8.
• You can drink clear liquids up to 2 hours before your surgery (water, apple juice, tea no milk) or until you leave for the hospital. Milk and orange juice are not clear fluids and should not be taken. Do not drink any “diet” beverage.
High carbohydrate drinks before your surgery
• A drink that is high in carbohydrates is a drink that has a lot of sugar. It is important to have sugary drinks before your surgery to help you feel stronger after your surgery and to recover faster.
• Drink up to 3 glasses (800 ml) of a high carbohydrate drink at bedtime the night before your surgery.
• Drink 1.5 glasses (400 ml) of a high carbohydrate drink up to 2 hours before your surgery.
Apple juice, cranberry juice and iced tea are examples of high carbohydrate drinks.

8
Laxative before your surgery
The evening before your surgery
No laxative Fleet Enema
Get two Fleet enemas from your local pharmacy. This product is available over the counter.
Use the first enema the evening before your surgery, after dinner.
Do not eat any solid food after midnight, the night before your surgery.
Golytely or Peg-lyte
Get a 4 L bottle of Golytely or Peg-lyte from your local pharmacy.
Do not eat any solid food 3 hours before you start drinking Golytely or Peg-lyte. You can drink clear liquids.
Drink 240 ml (8 oz.) of Golytely or Peg-lyte every 10 minutes, starting the evening before your surgery.
The morning of your surgery
Fleet Enema
Use the second enema the day of your surgery, 1½ hour (90 minutes) before you arrive at the hospital.
Do not eat any solid food.
Drink clear liquids and carbohydrates up to 2 hours before your surgery, or when you leave home to get to the hospital.
Do not drink any “diet” beverage.
Golytely or Peg-lyte
Do not eat any solid food.
Drink clear liquids and carbohydrates up to 2 hours before your surgery, or when you leave home to get to the hospital.

9
Things to bring to the hospital
• This information guide • All the medications you are currently taking, or a complete list of them • A bathrobe and comfortable clothing • A credit card (if you want to rent a television or a phone in your room) • Non-slip slippers or shoes • Earplugs (if you wish) • Reading glasses in a case labeled with your name • Magazines or books to read • Personal hygiene items (toothbrush, toothpaste, hair brush, mouthwash, deodorant,
lip balm, hand cream, etc.) • Your cane, crutches or walker, if you usually use them for walking. Label them with
your name. • Your sleep apnea machine, if you use one to sleep. Label it with your name. • Two packs of your favourite gum. Chewing gum will help you recover from your
colorectal surgery. If you cannot chew gum for any reason, please let your surgeon know.
Things to do Take a bath or a shower, and wear freshly washed clothes Do not wear jewelry, body piercings, makeup, lipstick, nail polish (hands and feet),
cream or lotion, deodorant, perfume, hairspray, contact lenses Do not shave

10
Your surgery
When you arrive at the hospital
• Present yourself to the Operating Room reception, room 2A105 • We will come and get you in the waiting room, and help you get ready for your surgery • We will ask you to change into a gown • Your healthcare team will ask you a few questions and answer yours.
Your loved ones can wait in the waiting room next to room 2A105. The area is small, so we ask that you restrain the number of visitors to one or two. The screen in the waiting room indicates the status of the patients in the Operating Room. Your visitors will be able to know in which step you are while in the Operating Room.
In the Operating Room
• You will be move to the Operating Room in a wheelchair by a porter • If you are to receive an epidural, it will be given before you are put to sleep • Antibiotics and anticoagulants (blood thinners) will be given to help decrease your
chance of infection and blood clots • While you are asleep, you may have a tube (catheter) inserted into your bladder to
drain your urine without having to go to the washroom.

11
After your surgery: In the recovery room • After your surgery, we will bring you to the
recovery room. You will be there for about two hours.
• Your nurse will check your blood pressure, your pulse, your pain level and your dressing
• You might receive oxygen through a tube in your nose or a face mask.
• When you will start to wake up, we will ask that you take deep breaths and to move your feet and legs. These exercises will help you prevent complications and blood cloths.
• Do not hesitate to tell how you are feeling (nausea, pain, discomfort, thirsty, itchy, etc.) • You will have an intravenous (IV) drip to receive fluids and medicine. • Visitors are not permitted in recovery.
After surgery: on the ward You will be transported from the recovery room to your ward and installed into your bed in your room. You may receive visitors from this moment on.
The day of your surgery
Lying in bed without moving may cause many problems like pneumonia, blood clots and muscle weakness. It will also slow down your recovery.
The more often you get up, the better you will feel.
Leg exercises
Your healthcare team will help you do the following exercises:
• Sit up and dangle your legs at the side of the bed
• Start doing your leg exercises — see “Leg exercises” on page 14 of this guide
Breathing exercises
If right for you, your healthcare team will show you how to do deep breathing exercises • Perform 10 sets every hour when you are awake — see “Deep breathing exercises”
on page 14 • Try coughing 2-3 times after your breathing exercises. Hug a pillow when you try to
cough.

12
Drinking and eating
As soon as you are in your room after your surgery, you can have sips of clear fluids and then progress to a regular diet.
Catheters
If your have a catheter, it should be removed: • The day after your surgery, if you had a colon surgery • The third day after surgery, if you had a rectum surgery
The catheter needs to be removed as early as possible to decrease risk of bladder infection and will facilitate your movements.
What you might feel • Nervous about getting up
o This is a normal feeling. Your healthcare team will help you to walk.
• Hungry or not hungry o It is safe to have fluids the night of your surgery and food the day after surgery. o Just eat and drink what you feel like. o You will usually feel like eating and drinking more each day.
• Tired
o This is normal. Your body is trying to heal. o After your walks, it is important to rest.
Why is moving around after surgery important?
After bowel surgery, your bowel may stop working. This is called ileus. When this happens, people feel bloated and may have nausea and vomiting. If you have an ileus, this will increase your surgery recovery time.
Pain medicine which contain opioids, like morphine, increase the chance of ileus. Walking and chewing gum help the bowel work faster and speed your recovery.

13
Moving around as much as you can after your
surgery will help reduce the chances of a blood clot
in your legs or lungs.
Do your leg exercises every hour when you are
awake.
While you are in the hospital
Your activities
With the help from your healthcare team, or your loved ones, you will: • Sit up in a chair for all your meals • Be out of bed, either walking or sitting frequently for increasing periods of time • Do your leg exercises • Do your deep breathing exercises

14
Breathing exercises and coughing help to
prevent pneumonia or other infections in your
lungs.
Remember to do your breathing exercises
every hour!
Leg exercises
These will help blood circulation in your legs. Repeat these 4-5 times every hour when you are awake.
Stretch your legs out straight
Wiggle your toes and move your feet up and down
Make circles with your ankles
Deep breathing excercices
• Breathe in slowly and deeply through your nose • Breathe out slowly through your mouth, with your lips pursed. • Repeat 10 times every hour.
Coughing exercises
• While holding a pillow against your incision to support it, give 3 strong coughs.
• If your cough is wet, try to cough more to clear the phlegm

15

16

17
Chewing gum after surgery will help you pass
gas, which is a sign that your bowels are
working.
Chew gum for at least 5 minutes,
at least 3 times a day.
Food and drink
You will be given your first meal the day after your surgery.
You can eat as much and whatever you want. Your family can bring you food if you prefer, but check with your nurse first to ensure it is right for you. You can bring non-perishable foods to eat when you are hungry.
You should always sit in a chair at meal time, even if you eat very little.
You should chew gum starting the day after your surgery. You should chew one piece of gum for at least 5 minutes, at least 3 times per day.
Chewing gum after surgery will help you pass gas, which is a sign that your bowels are working. Again, if you cannot chew gum for any reason, let your surgeon know.
Tell your nurse if you are sick to your stomach (nauseous), or if you feel bloated during or after eating.

18
Different ways to manage your pain Pain is an unpleasant feeling that is different for every person. There are many words people use to describe pain, like ‘soreness’, ‘discomfort’, or ‘aching’.
There are different medicines you can take after surgery to help manage your pain. There are also different ways of receiving your medicine. You and your healthcare team will discuss your different options before your surgery and together you will decide which options are best for you. Sometimes, you may receive more than one type of medicine and more than one way of receiving it. The most common ways to receive medicine are:
Intravenous (IV) pain medicine
Pain after surgery is frequently treated with strong medicine (opioids) given through your intravenous (IV) line. You will most likely be given a pain pump to use. This method of pain relief is called “patient controlled analgesia” (PCA). Pain medicine from the PCA pump goes into your IV and then into your body. When you use PCA, you are in control of how much pain medicine you get and when you get it. If you are having pain, you push a button that is attached to the pump. You can push the button at any time you feel pain. You will hear a beep from the pump to let you know that the pain medicine is going into your intravenous. After the beep, it takes only a few minutes for the medicine to work. You do not need to call the nurse to get pain medicine. The pump is set up to make sure that you do not get too much. However, it is very important that only you and no one else push the button on the pain pump. Do not let your family or friends push the button.
If for some reason, you are unable to use your pump, your nurse will give you the pain medicine that you need. If you are in pain call your nurse.
You may also be given pain pills by mouth in addition to using the IV pump.
Epidural analgesia
An epidural is a small tube placed in your back by an anesthesiologist. It is placed in a space outside your spinal cord to give you medicine to reduce your pain after surgery.
Medicine is given through the tube to provide pain relief. This medicine is usually local anesthetic (or “freezing”) plus an opioid. Epidurals are usually inserted before your surgery.
After your operation, your epidural will be connected to an epidural pump, which will deliver a steady dose of pain medicine. Sometimes, you may be able to control the pump yourself (PCA). If you choose an epidural, you will have it for the first 48-72 hours after your surgery.
Oral Pain Medicine
You will be given different types of pain medicine on a regular basis after your surgery, including acetaminophen (Tylenol TM), to help manage your pain. Each pill works differently in your body and reduces the need for large amounts of strong pain medicine, such as opioids. If the medicine does not control your pain, please tell your nurse. Additional or different pain medicine can be given.

19
Having your pain well controlled is important because it helps you to: • Decrease the stress in your body so you can recover faster • Accelerate your recovery • Facilitate your breathing and coughing • Facilitate your movement • Sleep better • Do things that are important to you
When do I treat my pain?
The pain rating scale can help you decide when to do something to relieve your pain. Use the scale from 0 to 10 to determine how much pain you are having.
You may find that your pain is less when you are resting and more when you are moving. If your pain is 4 or more you should treat it. If the pain is stopping you from moving, you should also treat your pain.

20
Your checklist before you leave to go home
You should have no nausea or vomiting You should be able to eat and drink as usual You should be passing gas You do not have to have a bowel movement before you go home You should be passing your urine well You should be able to get in and out of bed on your own You should be walking like you did before surgery. You may not be able to walk far
and that is fine If you have stairs in your home, you should have enough strength and energy to go up
and down the stairs You should have everything organized at home (have food to eat, people who can
help you, etc.) All of your questions or concerns about your recovery at home have been answered
by your healthcare team You need to complete your activity log and return it to your nurse before you leave
Passing gas is a better sign that your gut is
working than having a bowel movement.
You do not need to have a bowel movement
before you leave the hospital.

21
What you need to know before you leave the hospital • About the medicine you were on before your surgery and any new medicine you will
need to take now • If you need a prescription for any pain medicine or other medicine you may need to
take at home • About what you can eat and drink • How to take care of your surgical incision (cut) • When to go back to regular activities (driving, exercise, etc.) • What symptoms are considered medical emergencies and what signs to watch for • Who is going to help take care of you once you are home. If you require home care
services or any other items to help in your recovery at home, discuss it with your healthcare team
• Who to call if you have questions or concerns
Discharge Information
Date and time of your discharge from the hospital: __________________________________
Name and contact information of the person picking you up: __________________________

22
At Home
What you cannot do
• Do not lift more than 10 pounds (1 laundry bin or 2 small bags of groceries) for the first 4-6 weeks after surgery
• Do not do abdominal exercises, high intensity aerobic activities or weight training for 4-6 weeks after surgery
What you can do
• You can shower or take a bath. You do not need to cover your surgical incision (cut)
• You should continue to be active (walk, socialize, etc.). Gradually increase your activity level over the next several weeks.
• It is normal to feel tired after surgery. Listen to your body and take frequent rest breaks as needed throughout the day
• You can resume most normal activities once you are pain free, including sexual intercourse
• You may start to drive when you are no longer taking opioid pain medicine • Your surgeon will tell you when you can return to work. This will depend on your
recovery and your type of work • You might go home with staples in your skin that hold your surgical incision (cut)
together. If so, talk to your nurse about when they need to be taken out
Ask your family and friends to help you with: • Getting meals ready • Grocery shopping • House cleaning • Laundry

23
Signs and Symptoms to Watch For
Call your surgeon or go to the nearest emergency room right away if: • You have a fever (temperature greater than 38°C or 100.4°F) • You are vomiting, bloated or feeling nauseous all the time • You have redness, swelling, odor, pus or increasing pain from your surgical incision • You notice bright red blood from your anus • You have stomach pain that your medicine does not relieve • You have not had a bowel movement 7 days after your surgery
My Follow-up Appointment My follow-up appointment is: ___________________________________________
My Activity Log You receive a questionnaire with this guide. Use it to take note of your daily activities after your surgery. For each activity, check “yes” or “no”.
Do not forget to hand the questionnaire to your nurse before leaving the hospital.

24
Your hospital stay

25
At your surgeon’s office Assessment • You will be assessed by your surgeon.
Examinations • Examinations might also be prescribed before your surgery.
Medication • Inform your surgeon of all the medication you are taking (prescription or otherwise).
Nutrition • Your surgeon will discuss with you the importance of resuming a regular diet soon after your surgery.
Activity • Your surgeon will discuss with you the importance of being physically active after your surgery.
Education • Your surgeon will discuss with you the importance of drinking carbohydrate-rich fluids the day before and 2 to 3 hours before your surgery.
• You will be given this guide. Bring it with you to your appointment at the hospital the day of your surgery. This guide is also available on Montfort’s website.
• Your surgeon will discuss with you the importance of chewing gum after the surgery.
Discharge planning
• Your surgeon will discuss with you the duration of your stay at the hospital. Plan to be at the hospital for 3 days if you are having colon surgery and 4 days if you are having rectal surgery.

26
Preadmission Assessment • We will take your temperature, blood pressure, pulse and oxygen level. We
will measure and weigh you. • We will ask you questions about your health, medical history and alcohol and
tobacco consumption. • Tell us if you have allergies and/or intolerances. • Other members of your care team, including an enterostomal therapy nurse
(if you have a stoma), will assess you. • Your surgeon could also ask that you consult an anaesthetist, social worker
and/or dietician.
Examinations • We will do blood tests and, in some cases, an electrocardiogram (ECG).
Medication • If possible, bring your medications in their original container and/or a recent list of medications from your pharmacy.
• After assessing the medications you are taking, we might ask you to stop taking them, in some cases.
• We will give you instructions on the medications to take the day of your surgery.
Nutrition • Your nurse will tell you what you must take the day before your surgery and the time at which you must stop eating or drinking.
Activity • We will encourage you to continue to be physically active before and after your surgery.
Education • A preoperative education class is available to fully prepare you for your surgery and your discharge.
• A member of your care team will review this guide on colorectal surgery with you.
• Your anaesthetist will discuss pain management with you. • Your nurse will tell you if you should take an intestinal preparation the day
before your surgery. • Your enterostomal therapy nurse will give you information on the stoma, if
you are going to have one. • You will be informed of the importance of actively participating in your
recovery after surgery.
Discharge planning
• Your nurse will ask you, as well as your loved ones, if you have planned your departure from the hospital. If you need help planning your discharge, we will take the necessary steps to have you meet with a social worker.
• If you have a stoma, homecare will be provided. • Your discharge is planned for 3 days after your surgery if you are having
colon surgery and 4 days after your surgery if you are having rectal surgery. The day of your departure, plan to leave the hospital at 10 a.m.

27
The day before your surgery Assessment • Your nurse will tell you if you need to take an intestinal preparation the day
before your surgery.
Nutrition • Drink 8 ounces of clear fluids (apple juice, cranberry juice) the day before your surgery.
• Do not eat solid food 8 hours before your surgery.

28
Day 0 (day of your admission) Assessment • We will take your temperature, blood pressure, pulse and oxygen level before
your surgery, and then regularly throughout the day. • We will assess your pain level and ask you to rate it on a scale of 0 (no pain) to
10 (extreme pain). • We will regularly check your dressing. • We will ask you how much fluid you are drinking and urinating.
Examinations • Your surgeon could ask for other blood tests.
Medication • We will insert an intravenous catheter and give you fluids, according to your surgeon’s instructions.
• Your nurse will give you your medications, according to your surgeon’s instructions.
Nutrition • After your surgery, you will be able to drink clear fluids (such as water). • You will then be able to drink and eat normally, depending on your tolerance
level.
Activity • Your care team will help you sit on the edge of the bed. Let your legs swing for at least 10 to 15 minutes, every 2 to 4 hours, after your surgery.
Treatment • Breathe deeply and cough. This exercise helps to clear your lungs and prevent pneumonia.
• We will check the volume of urine in your urinary catheter. • Do ankle and foot movement exercises 2 to 3 times a day. This helps to prevent
blood clot formation and maintains your muscle activity.
Education • Your nurse will make sure that you are properly performing your deep breathing, coughing and ankle movement exercises.
• Your nurse will discuss pain relief with you. • Your care team will often refer to this guide on colorectal surgery. Do not hesitate
to ask all your questions.
Discharge planning
• Your nurse will talk to you and your loved ones about your family situation and discharge plan. If you need help planning your discharge, we will take the necessary steps to have you meet with a social worker.

29
Day 1 (day after your admission) Assessment • We will check your temperature, blood pressure, pulse and oxygen level.
• We will regularly assess your pain level to make sure that you are able to do your exercises.
• We will examine your dressing. • We will ask you how much fluid you are drinking and urinating. • We will assess your abdominal noises and if you are evacuating gas.
Examinations • Your surgeon will ask for blood tests, if necessary.
Medication • If you are drinking normally and your haemoglobin is normal, we will remove the catheter.
• Your nurse will give you your medication, according to your surgeon’s instructions.
Nutrition • You can eat normally. • Chew gum for at least five minutes, three times a day, to activate your digestive
system.
Activity • Your care team will help you sit in an armchair for your meals. • Your care team will help you with your personal hygiene, if necessary. • You will be encouraged to do your breathing and coughing exercises 10 times an
hour when you are awake. • Get up and walk every 4 to 6 hours and to go to the bathroom. Ask for help if you
need it. • Start completing your activity journal (separate sheets in the guide).
Treatment • If you had colon surgery and you have a urinary catheter, it will be removed today. If you had rectal surgery, your catheter will be removed within the next 48 hours.
• We will monitor the volume of urine in your bladder by means of a bladder scan, if necessary.
Education • Your nurse will discuss pain and nausea relief with you. • Your nurse will make sure that you are properly performing your exercises. • We will review possible complications with you and tell you when to consult your
physician. • Your care team will often refer to this guide on colorectal surgery. Do not hesitate
to ask them all your questions.
Discharge planning
• Your nurse will find out about your family situation and help you carry out your discharge plans.
• Your surgeon will tell you when to make a follow-up appointment and inform you about your prescriptions.
• If you have a stoma, homecare will be provided. • We will explain how to care for your incision.

30
Day 2 Assessment • We will check your temperature, blood pressure, pulse and oxygen level.
• We will regularly assess your pain level. • We will ask you how much fluid you are drinking and urinating. • We will assess your abdominal noises and if you are evacuating gas.
Examinations • Your surgeon will ask for blood tests, if necessary.
Medication • Your nurse will give you your medication, according to your surgeon’s instructions. If you have any questions about your medication, ask your nurse.
Nutrition • You can eat normally. • Chew gum for at least five minutes, three times a day, to activate your
digestive system.
Rest and activity • You will take your meals sitting in an armchair. • You will look after your personal hygiene. • You will be encouraged to do your breathing and coughing exercises 10 times
an hour when you are awake. • Get up and walk every 4 to 6 hours and to go to the bathroom. Ask for help if
you need it. • Continue to complete your activity journal.
Treatment • If you had rectal surgery, your urinary catheter could be removed within 24 hours.
Education • Your nurse will discuss diet, exercises, pain management and lifestyle with you.
• We will review possible complications with you and tell you when to consult your physician.
• Your care team will often refer to this guide on colorectal surgery. Do not hesitate to ask them all your questions.
Discharge planning
• We will help you carry out your discharge plans. • You will go home tomorrow at 10 a.m. Make the necessary arrangements for
your transportation. • Your surgeon will tell you when to make a follow-up appointment and inform
you about your prescriptions. • If you have a stoma, homecare will be provided. • You will be told how to care for your incision.

31
Day 3 (colon) and 4 (rectum) after your surgery
Assessment • Before your departure from the hospital, we will check your temperature, blood pressure, pulse and oxygen level.
• We will assess if you have pain or nausea. • We will assess your diet, exercises and lifestyle. • We will check your incision and if you are evacuating gas.
Medication • Your nurse will give you your medication, according to the surgeon’s instructions.
Nutrition • You can eat normally. Make sure you drink enough to stay hydrated. • Chew gum for at least five minutes, three times a day, to activate your
digestive system.
Rest and activity • You will take your meals sitting in an armchair. • You will look after your own hygiene. • You will be encouraged to do your breathing and coughing exercises 10 times
an hour when you are awake. • Get up and walk every 4 to 6 hours and to go to the bathroom. Ask for help if
you need it. • Continue to complete your activity journal.
Treatment • If you still have a urinary catheter, it will be removed.
Education • We will discuss home pain management with you. • We will review possible complications with you and tell you when to consult
your physician. • Your care team will often refer to this guide on colorectal surgery to give you
instructions on your departure from the hospital and your medical follow-up. Do not hesitate to ask them all your questions.
Planning and discharge
• If you had colon surgery, you will leave today at 10 a.m. • If you had rectal surgery, you will leave tomorrow. • Your surgeon will tell you when to make a follow-up appointment. • We will review your discharge plan with you. • If you have a stoma, homecare will be provided. • We will explain how to care for your incision. • Please give your questionnaire and your activity journal to your nurse before
leaving.

32
713 Montreal Road Ottawa, Ontario K1K 0T2
Phone: 613-746-4621 hopitalmontfort.com