a microcomputer-assisted bacteriology reporting and information system
TRANSCRIPT

Acta path. microbiol. immunol. scand. Sect. B. 92: 119-126. 1984
A MICROCOMPUTER-ASSISTED BACTERIOLOGY REPORTING AND INFORMATION SYSTEM
JENS K. MBLLER
Department of Clinical Bacteriology. Statens Seruminstitut,Aarhus Municipal Hospital, Aarhus and Institute of Medical Microbiology, University of Aarhus, Aarhus. Denmark
Msller. J. K. A microcomputer-assisted bacteriology reporting and information system. Acta path. microbiol. immunol. scand. Sect. B, 92; 119-126. 1984.
A microcomputer system for recording and reporting all specimens processed by a routine laboratory of clinical bacteriology is described. The system is based upon two multi-user microcomputers and all functions are carried out within the laboratory by the medical, technical and clerical staff. Data are recorded using visual display units (VDU’s) and the laboratory has issued about 2 7 0 0 final reports per week since January 198 I . Data on all specimens are kept for immediate recall on a VDU for a period of about 6 weeks and herafter stored on floppy disks. The computer system also produces laboratory statistics for internal use, epidemiological information for the surveillance of nosocomial infections. and makes accounting information for the accountants office.
Key words: EDP; microcomputer; clinical microbiology; bacteriology reporting; information system.
J. K. Meller, Institute of Medical Microbiology, Bartholin Building, University of Aarhus. DK-8000 Aarhus. C, Denmark.
Received 3.xi. 8 3 Apart from the single-user microcomputer sys-
tem described by Worbut et al. 198 1 ). the bacterio- logy reporting systems reported so far, are integra- ted parts of a system on larger machines placed outside the laboratory and designed by computer specialists Undrews & Vickers 1974; Mitchison et al. 1978; Williams et al. 1978; Ridgway rt al. 1980). It was our objective to have our own computer within the laboratory and to use a simple programming language that would enable us to do the programming of the system ourselves. This was achieved by means of two multiuser. multitask microcomputers placed inside the laboratory. The outhor planned and programmed the entire system in COMAL. a high level programming language resembling structured BASIC.
For all patients. information about antibiotic therapy (drug(s) used and the lengthk) of therapy) and implantation of foreign bodies is recorded. For selected groups of patients, information on the main diagnosis and the infection is recorded if stated on the request form.
Accepted 28 .xi.8 3 The main objective of the bacteriology reporting system was to make an easily retrievable. perma- nent record of the information produced in the laboratory in such a way that it could be used also for research purposes and in cross-infection control. It was a prerequisite that neither should laboratory staff increase nor should the work-flow pattern in the laboratory be changed due to the computeriza- tion. Furthermore, the system should include all users of the laboratory and the final reports on all examinations done.
The laboratory deals exclusively with bacteriolo- gical examinations and serves twenty hospitals and about 350 general practitioners.
MATERIALS AND METHODS Computer characteristics. The hard-ware consists of two 8 bit microcomputers of Danish design (SPC/I from Danish Data Electronics). One microcomputer supports the current data-base and is a multi-user. multi-task computer with 32 K words for program and data for each user and 32 K words for the operating system
t 19
MIKADOS (danish for Microcomputer Oriented co- routine operating system And Disk Operating System). The construction of SPC/ I is based upon a 100 pin system bus and provides in our version access to a 10 Mbyte Winchester-disk. a I Mbyte floppy disk. a 90 Kbyte mini floppy disk. three matrix-printers and 6 VDU’s. The other SPC/I microcomputer is a similar multi-user (3 users), multitask computer and is used by the clerical staff for recording data from the front page of the request form. The data recorded are later transferred to the other machine using a floppy disk. One of the microcomputers supports a T T Y emulator which enables a modem connection to a larger. central computer.
Softwwrr. The bacteriology reporting system called MADS (Microbiology Adapted Data System) is a series of programs developed and programmed in COMAL by the author. A log in and menu program sees to it that the particular program requested IS read from the Winches- ter-disk and executed. After having completed the task. the program requested returns to the lox in and menu program.
Duru-base. The data-base consish of series of random-access files. One series of identically structured files contains the information written on the front page of the request form. Another series of files contains laboratory results. By means of pointers connected parts
of information are chained together. The use of small. random access files containing the same type of data ensures a rapid access to the requested information and facilitates updating and safety-copying. Other files in the system contain tables of constants and strings of text necessary for the processing. for the layout on the VDU. and for the printed reports. The current data-base contains information about the specimens received within the last 6 weeks. Data older than 6 weeks are achieved on floppy disks and kept in two copies.
The s.ssrc’m (MADS). The backbone of the system is two numbers. One is a consecutive laboratory number given to all specimens admitted to the laboratory. and the other identifies the patient. The patient number used is the ten digit civic register number (CPR). which is used by public authorities in Denmark to identify the citizens. By means of these two numbers access to the data-base is easily achieved.
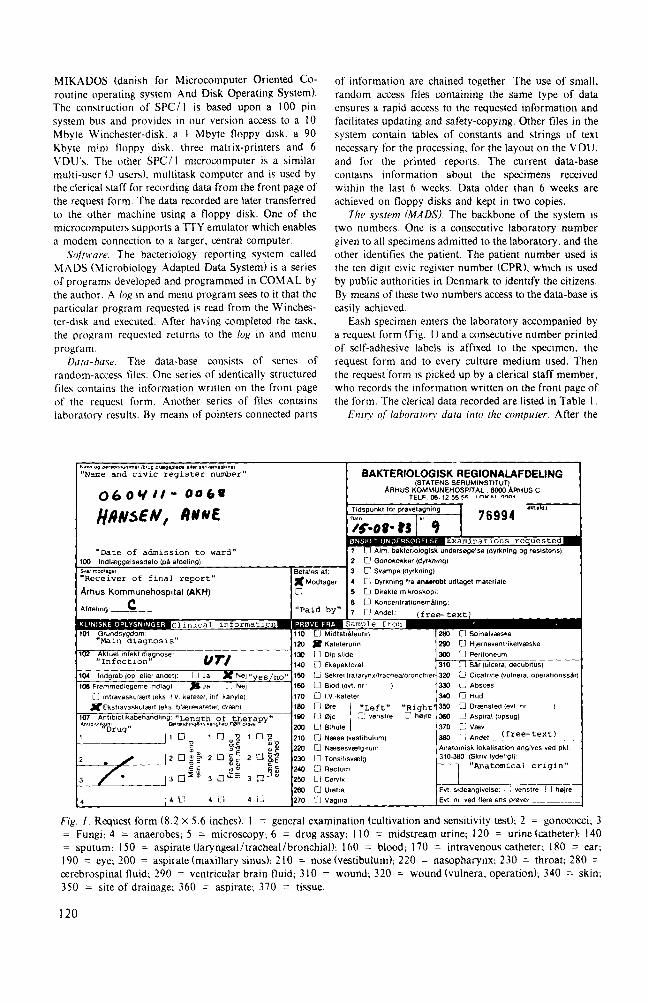
Eash specimen enters the laboratory accompanied by a request form (Fig. I ) and a consecutive number printed of self-adhesive labels is affixed to the specimen, the request form and to every culture medium used. Then the request form is picked up by a clerical staff member. who records the information written on the front page of the form. The clerical data recorded are listed in Table 1 .
E n t n of luboratorv dam inlo the computer. After the
140 L3 Ekspektorat
Fig. 1 . Request form (8.2 X 5.6 inches). 1 = general examination (cultivation and sensitivity test): 2 = gonococci; 3 = Fungi; 4 = anaerobes; 5 = microscopy; 6 = drug assay; I 10 = midstream urine; 120 = urine (catheter): 140 = sputum; 150 = aspirate (laryngeal/tracheal/bronchial); I60 = blood; I70 = intravenous catheter; 180 = ear; 190 = eye; 200 = aspirate (maxillary sinus); 210 = nose(vestibu1um); 220 = nasopharynx; 230 = throat; 280 = cerebrospinal fluid; 290 = ventricular brain fluid; 310 = wound; 320 = wound (vulnera. operation); 340 = skin; 350 = site of drainage; 360 = aspirate; 370 = tissue.
120
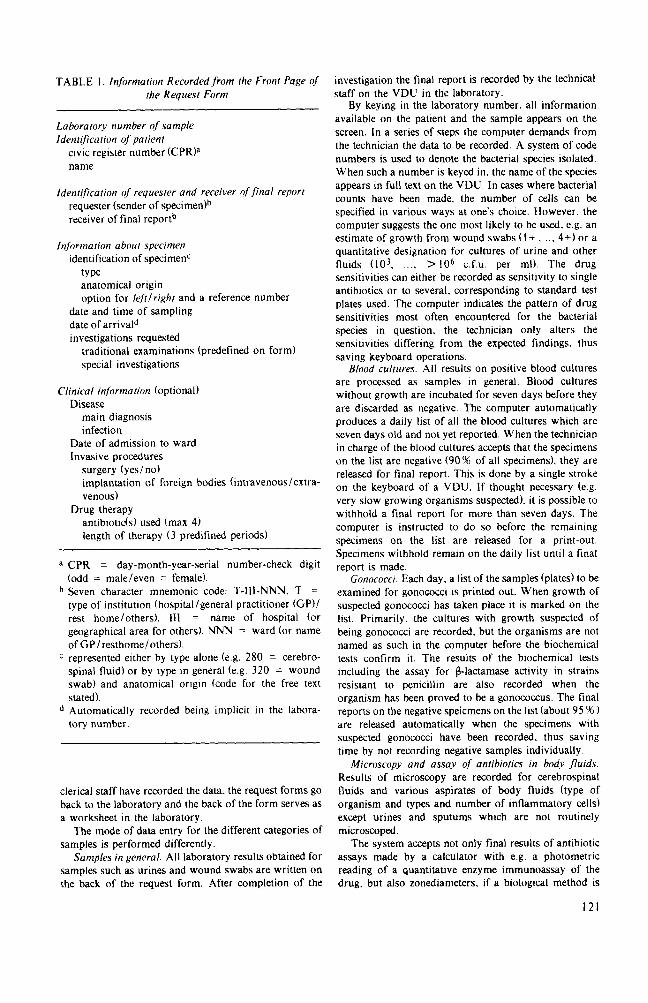
TABLE I . Information Recorded from the Front Page of the Request Form
Laboratory number of sample Identification of patient
civic register number (CPR)a name
Identification of requester and receiver of ,final report requester (sender of specimedh receiver of final reporth
Informarion about specimen identification of specimenC
type anatomical origin option for Iefttlright and a reference number
date and time of sampling date of arrivald investigations requested
traditional examinations (predefined on form) special investigations
Clinical information (optional) Disease
main diagnosis infection
Date of admission to ward Invasive procedures
surgery (yes/no) implantation of foreign bodies (intravenous/extra- venous)
Drug therapy antibiotids) used (max 4) length of therapy (3 predifined periods)
a CPR = day-month-year-serial number-check digit (odd = male/even = female). Seven character mnemonic code: T-111-"N. T = type of institution (hospital/general practitioner (GP)/ rest home/others). 111 = name of hospital (or geographical area for others). NNN = ward (or name of GP /resthome/others). represented either by type alone (e.g. 280 = cerebro- spinal fluid) or by type in general (e.g. 320 = wound swab) and anatomical origin (code for the free text stated). Automatically recorded being implicit in the labora- tory number.
clerical staff have recorded the data. the request forms go back to the laboratory and the back of the form serves as a worksheet in the laboratory.
The mode of data entry for the different categories of samples is performed differently.
Samples in general. All laboratory results obtained for samples such as urines and wound swabs are written on the back of the request form. After completion of the
investigation the final report is recorded by the technical staff on the VDU in the laboratory.
By keying in the laboratory number. all information available on the patient and the sample appears on the screen. In a series of steps the computer demands from the technician the data to be recorded. A system of code numbers is used to denote the bacterial species isolated. When such a number is keyed in. the name of the species appears in full text on the VDU. In cases where bacterial counts have been made. the number of cells can be specified in various ways at one's choice. However. the computer suggests the one most likely to be used. e.g. an estimate of growth from wound swabs ( I + , ... 4+) or a quantitative designation for cultures of urine and other fluids ( lo3. .... > lo6 c.f.u. per ml). The drug sensitivities can either be recorded as sensitivity to single antibiotics or to several, corresponding to standard test plates used. The computer indicates the pattern of drug sensitivities most often encountered for the bacterial species in question, the technician only alters the sensitivities differing from the expected findings, thus saving keyboard operations.
Blood cultures. All results on positive blood cultures are processed as samples in general. Blood cultures without growth are incubated for seven days before they are discarded as negative. The computer automatically produces a daily list of all the blood cultures which are seven days old and not yet reported. When the technician in charge of the blood cultures accepts that the specimens on the list are negative (90 % of all specimens). they are released for final report. This is done by a single stroke on the keyboard of a VDU. I f thought necessary (e.g. very slow growing organisms suspected), it is possible to withhold a final report for more than seven days. The computer is instructed to do so before the remaining specimens on the list are released for a print-out. Specimens withhold remain on the daily list until a final report is made.
Gonococci. Each day, a list of the samples (plates) to be examined for gonococci is printed out. When growth of suspected gonococci has taken place it is marked on the list. Primarily, the cultures with growth suspected of being gonococci are recorded, but the organisms are not named as such in the computer before the biochemical tests confirm it. The results of the biochemical tests including the assay for fblactamase activity in strains resistant to penicillin are also recorded when the organism has been proved to be a gonococcus. The final reports on the negative speicmens on the list (about 95 96 ) are released automatically when the specimens with suspected gonococci have been recorded, thus saving time by not recording negative samples individually.
Microscopy and assay of antibiorics in body fluids. Results of microscopy are recorded for cerebrospinal fluids and various aspirates of body fluids (type of organism and types and number of inflammatory cells) except urines and sputums which are not routinely microscoped.
The system accepts not only final results of antibiotic assays made by a calculator with e.g. a photometric reading of a quantitative enzyme immunoassay of the drug. but also zonediameters, if a biological method is
121
I : E. C N I l.COO.00.00U c.f.u./al
S U L r n I o E S 0 STREPICh’lYCIN A l l P I C I L l I N 2 NITROFLYlANTOIN TRIETHCQAIII 2 GENTMICIN 2 WIDIXIC ACID 2 R E C I L L I ~ 2
EAKTERIOLOGISK REGIONACAFDECING (Slatens SeruminsliIul\
ARHUS KOMMUNEHOSPITAL 8000 ARHUS C TLF 06 - 12 55 55 Lokal2291
Form 44 16 t60000 3-83
Fig. 2. The final report slip
0 ~ resistent 1 = nedsat l01somhed 2 - fuldt f0lsom OBS! Resistensunders0gelse er ikke I sig selv indikatlon faranttbiotikabehandling
employed. I n the latter case. the computer makes all the calculations based upon a standard curve made on known concentrations of the drug.
The fitral r c p i r i The final report is composed from the data recorded by the clerical and the technical staff and released by a technician (Fig. 2 ) :
tlrr iittie o/ ruttipling. On the upper first line are written. CPR number. name of the patient. date and time of sampling. The next line states the type of specimen. Several reports can be placed on the same page in a patient‘s records. They are all fixed to the left side and if each is vertically displaced a little bit. several reports can be pasted on top of each other. This arrangement allows the upper two lines on each slip t o be easily read and every slip to be lifted aside.
11: Tlir tiutne arid address o/ i/ie receiver. These data are found in the mailing list by means of a seven letter code (Table I ). The address is placed in such a way that the report can be mailed in a window envelope.
111: Restr l is o/ the laboraton itivestigations. Four different kinds of information are given either separately or in various combinations. a: specification of the organismk) isolated and a quantification of the number of bacteria found. b: antibiotic sensitivities of the organisms (0 = resistant. I = reduced sensitivity. 2 = sensitive). The number and kind of drugs examined for depend on the organism isolated. and the character of the specimen. c: laboratory results less often reported as for instance microscopy, 6-lactamase activity or antibiotic assay. d: one or more of a series of predifined stamps e.g. ))No growthcc. ))Normal !lorat(. etc. either serve as a separate report or as an addiiion to a more elaborate report.
I: The idetitificutioti of the paiietit. !,‘pc’ of ~ ~ t ? i p l ~ , and
Rrcull o/ daiu. Apart from printing final reports. recall of data is necessary for answering inquiries on telephone. for making laboratory lists. for collecting data for statistical analyses. and for accounting information.
An inquiry program is used to recall data from the database. The data available on a particular specimen are obtained either by keying in the consecutive number of the specimen or by keying in the CPR-number of the patient. By keying in the consecutive number. all data regarding the sample immediately appear on the VDU. Often the laboratory number is unknown but the identity o f the patient known. e.g. when inquiries are made on specimens from a particular patient by a clinical ward. The inquiry can be answered quickly on the telephone by keying in the patient CPR-number which in a few seconds gives a short version of the information regarding all recent specimens from the patient on the VDU. including information about character of speci- men. date of sampling. receiver of the final report. and a characterization of the laboratory investigations ( + /- growth). Through a reference-number. the full extent of the data on any of the single specimens can be obtained. Should the CPR number be unknown. the date of birth gives a similar short version of the information on specimens from all patients born on that particular date.
Statistical analyses are generally made on a special data-base created from the current data-base. Any type of information recorded in the current data-base can be used to delimit the new data-base. As an example, a data- base wanted from a clinical ward of wound swabs requires only that information is provided about the code numbers for wound swab and the seven letter code used to denote the ward. Such a data-base contains only laboratory numbers, which refers to the files containing
122

the data in the current data-base. Such a procudure makes repeated analyses of the selected data possible without a time-consuming run through the current data- base each time.
Information necessary to bill the institutions reques- ting laboratory investigations is collected monthly, and is transmitted to a central computer through the modem and the telephone system. From the central computer site. a magnetic tape containing the data transmitted is sent to the accountants office at the central institute (Co- penhagen).
A series of lists is printed out daily in order to draw attention to unfinished tests and to point out if the final report is overdue. As an example. all specimens not completed within three days from arrival with the exception of blood cultures (see above). are brought to attention by a daily checklist containing the consecutive numbers of the specimens. their date of arrival and the type of sample.
Conlrol meusures. The legislation in Denmark de- mands a rather tight data-security system when medical data associated with personal identification (CPR- numbers) are stored on computers. This means that the use of a VDU requires a personal password and that all activities are logged. The computer site is also equipped with a burglar and fire alarm.
EXPERIENCES
The design of the computer system was started in the autumn 1979 and a pilot trial restricted to a single clinical ward was undertaken in the summer 1980. From the very beginning all types of specimens were included in the data system. A revised version of the system based upon the results of the pilot study was then implemented for a major hospital in the area. During the autumn of 1980 a growing number of users of the laboratory were included and by January 1981 all specimens received were processed. By that time, the system issued some 2700 final reports per week. The system has been developed continuously ever since, and the existing software has gradually become more sophisticated, and new dimensions and programs have been added to the system.
The request form underwent a major revision after one year because the size of the form was found inconvenient and the original system with precoded boxes for marking the type of specimen and the anatomical origin complicated. The altera- tions included a cut in size to half the original because of a change in the number of precoded types of samples from 78 to 28. The latter changes meant that about 85% of the specimens could be placed under one of the precoded types of sample. The remaining specimens had to be stated as a combination of a precoded type of specimen and a free text stating the anatomical origin.
The hardware configuration was changed several times during the period, either because more storage space with faster access time or more VDUs were needed. The additional VDUs eventually made it necessary to purchase another microcomputer in order to relieve the first one.
The clerical staff found no difficulties in recor- ding the data on the front page of the request form. and gradually became capable of taking over the running of the data system. Although the technici- ans in the laboratory were less used to keyboards they quickly achieved the skill in recording the laboratory data on the VDUs.
It was a prerequisite that the computer system should be adapted to the existing departmental workflow and not vice versa. Consequently, the laboratory precedure was not changed with the introduction of the computers. After getting fami- liar with the computers. a growing demand from the technicians for exploiting the possibilities of the system has led to minor changes in the laboratory workflow.
The printing of released reports takes place continuously throughout the day. About one third of the report slips is scrutinized by a senior member of the medical staff. Reports with errors are withheld until corrections have been made. Correc- tions are made by technicians at a VDU in the laboratory.
Machine breakdowns have been surprisingly few. Over a period of 2 years, only 2 breakdowns caused a standstill for more than one day. Catching up with current requests after breakdowns presented only minor problems especially after the purchase of a second microcomputer. The matrix printers used have been outstandingly reliable and although VDUs do break down occasionally. this has caused no troubles due to a reserve VDU. The daily back- up of the data-base which takes eight minutes on a mini magnetic tape has saved much work when loss of data was caused by hardware errors in the data storage device (Whinchester-disk). However, many of the minor problems are caused by errors in programs and seem to disappear almost completely during periods when changes in existing programs or additions of new ones are omitted.
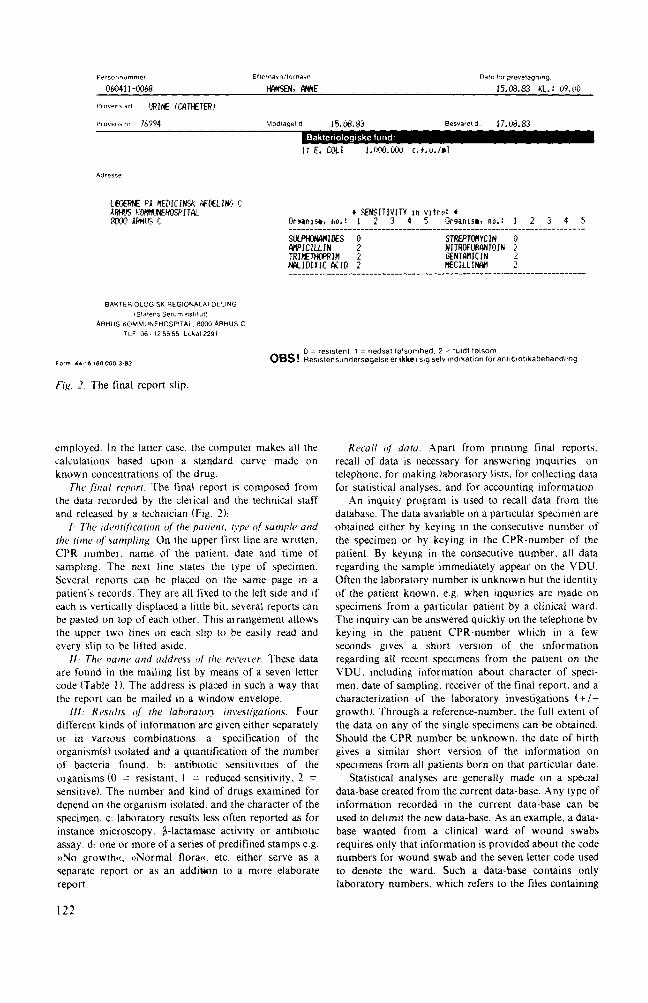
The hospital staff members and the general practitioners have been satisfied with the new reporting system, except with the first edition of the request form. There has been a considerable increase in requests for cumulative data after the introduction of electronic data processing. but it has until now only been possible to supply a few clinical departments regularly with such reports. An example of cumulative data is shown in Fig. 3 . Cumulative reports have been used extensively by
123

i~ NUMBER OF ISOLATES PER WEEK M.A.11.S - 17.08.1983
PEKIOI?: (-13e07.1983 - 07.08.1Y83
NUMBER OF IJEEK: Z6. 27. 28. 29. 30. 31. 00. 00, 00. 00. _ - _ - _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ - - _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ _ - _ STAPH + AUHEUS 1 0 2 8 4 0 0 0 <I 0 STAPH, EPI DERMIDIS 2 2 0 2 3 0 0 0 0 0 E. COLI 1 4 3 4 2 1 0 0 0 0 WEUDOMONAS AERUGINOSA 0 0 0 0 0 3 0 0 0 0 BACTLRO I DES FRAG I LI S 1 0 0 (3 0 0 0 0 0 0 PROTEUS MIRABILIS 0 0 0 1 2 0 0 0 0 0 KLEHS1kLLA PNEUMOhrIAE 0 2 0 1 0 0 0 0 0 0 HAEMOPHILUS INFLUENZAE biotype 2 . 0 0 0 0 1 0 0 0 0 0 HAEMOFHILUS 1NFLUENZAE biotrpr 5 . 0 0 0 1 0 0 0 0 0 0 _ _ _ _ _ _ _ _ _ _ _ _ _ - _ - - - ____-- - - - - - - - - - - - - - -____________________-- - - - - - -~- - -_- -_
FIK 3 Example of cumulative data from a clinical ward
the infection control nurses in their work in wards with major infection problems
An analysis of the total cost of the system has not been worked out. but the price of the hardware alone amounts to about 50000 US$ (purchase-tax excluded) and the outhor spent about 2 man-years developing the system. No extra personnel was needed to implement the data system. The occupa- tion of the clerical staff is now more evenly distributed throughout the day. and their timesav- ings hereby turned to the running of the computer system. The laboratory technicians could leave some tedious statistical work and they save much time because they now can trace previous data on the VDU.
DISCUSSION
This report demonstrates that a bacteriology repor- ting system can be based upon microcomputers. The use of a flexible and expandable multiuser, multi- task microcomputer made it possible to process final reports on at least 140000 specimens per year. Furthermore. cumulative reports have been produ- ced to the benefit of both the hospital and the laboratory staff.
The use of a microcomputer presents both advantages and disadvantages compared with con- ventional (larger) computers. The advantages are that microcomputers are very reliable and simple to operate and take little space in the laboratory. It is not necessary to share computer capacity with others. providing a better possibility for protection of the data-base from undesirable access. On the other hand, it is a disadvantage that the relatively ))modest(( computing power combined with limited data storage capacity makes it rather difficult to work out complex statistical operations, at least during the peak hours when the routine work occupies the microcomputer. The use of a micro-
computer does not preclude direct contact with other computers if a communication system exists (TTY-emulator). Therefore, it is possible to use the Patient Master Index at the hospital computer, and thus also make the microbiology data-base available to the clinicians.
The wish to introduce a computer-assisted bacteriology system raises a series of reflexions. The computer system should be superior to the manual one without causing an extreme rise in cost. In a thorough evaluation and comparison of a manual and a computer-assisted reporting system (Goodwin 1976; Goodwin & Smith 1976) it was concluded that a microbiology computer system that did not meet a substantially part of a series of objectives described probably would be unacceptable in a microbiology department. Examples of such objectives are, 1 : an on-line data-system, 2: all data to be reported should be recorded. 3: monitoring of overdue reports, 4: cumulative reports on any type of information recorded should be possible. 5: a fast recall of past results. 6: alternative methods of reporting available in case of breakdown.
At the time when it was decided to introduce a computer reporting system in the laboratory, there was neither a commercial system available nor was there a noncommercial system operating in any other laboratory in Denmark. If a system had been obtainable and transferable to the computer we wanted to acquire or would have had access to, several modifications might have been needed if it were to be adapted to the laboratory routine. That is especially the case when system from other countries are considered. Based upon such conside- rations, the author chose to work out his own system to suit the specific requirements of the laboratory. thus being able to choose freely among the different ways of recording data and organizing a data-base. Systems based upon paper tape or punch card Witchison et al. 1978; Whitby & Blair 1972) are obsolete and ought not to be considered.
I24
More futuristic alternatives as for instance the recording of spoken words or the use of a light pen should also be left out. Data-input through optical mark reading (OMR) were discarded because of the very expensive equipment this involves and because of the inherent rigidity(( of OMR-documents which makes alterations and additions difficult. Furthermore. the OMR-technique would introduce more paper in the laboratory. On the other hand the OMR-documents constitutes a hard-copy backup if data are lost from the computer system ndrews & Vickers 1974; Williams et al. 1978). That leaves the VDU as an obvious choice for recording data. One advantage of data recording through a VDU is. in addition to the flexibility in the way data are requested by the computer, the possibility of establishing a dialoque between operator and computer. which makes it easy to correct errors. A further advantage is the moderate cost of a VDU allowing many VDUs to be connected with the computer. A VDU also greatly facilitates the recall of data from the system. On the other hand, a disadvantage as compared to the OMR-technique is the necessary keyboard operations. although these can be reduced to a minimum through a carefully planned dialogue between the system and its users.
The computer system was programmed by the author in COMAL. which is a simple and yet powerful high-level programming language. CO- MAL also ensures that a transfer of the system to another computer is possible. Even with professio- nal assistance of computer specialists the microbio- logist must foresee that providing information to a specialist about his wishes and requirements con- cerning the computer system may present a consi- derable workload. Furthermore. it is often difficult to have a commercial program or system changed or supplemented afterwards.
The computer system described has been of benefit to the laboratory in several ways. The quality of information on the request form impro- ved considerably after the introduction of precoded texts. Control of the CPR-number became possible and revealed that several of these unique numbers were stated incorrectly and therefore had to be corrected. Reports from the previous manual system. which were also based upon these numbers, and which could not be found later on, were very likely misplaced due to incorrect CPR-numbers. The instant recall of previous reports on the VDU has been a major advantage. especially in telephone requests. Cumulative reports on a certain patient are now brought on the screen within 10 seconds. A further major advantage is the virtually unlimited possibilities for statistical analyses of data produced and recorded in the laboratory. Several types of
laboratory lists are printed daily and cumulative reports of cross-infection data are produced for several hospital wards. Epidemiological informa- tion hitherto produced by time-consuming manual methods can now be readily accumulated and printed regularly. It has enabled the medical bacteriologist to advise clinicians more effectively and made it easier to convince them about consequences of the misuse of antibiotics. for instance ecological ones.
A direct input of all laboratory results into the computer through VDUs placed at the laboratory benches, rendering manual notes on a work sheet superfluous, has not yet been accomplished. It has mainly been due to a lack of sufficient computing power which under the existing workflow made the continuous readings of many specimens directly into the computer too slow. The introduction of a I6 bit microcomputer combined with the experien- ces gathered so far makes it likely that this goal can be achieved in the future. As pointed out (Williams et al. 1978). the recordihg of all the technicians's findings represents an advance in the use of a computer in clinical microbiology since this enables the computer to do much of the scrutiny and liberates the medical staff to concentrate on clinical problems.
Beyond doubt, microbiological laboratories may draw many advantages from implementing compu- ter assisted reporting systems. This report shows that it is possible for minor as well as major laboratories to use microcomputers. Whether the system reported could be transferred to other clinical microbiological departments remains to be seen. A general version easily adaptable to local requirements would probably be acceptable for other laboratories. The use of such a system in all clinical microbiological departments in Denmark could for instance make a national surveillance of microorganisms causing nosocomial infections pos- sible.
I am most grateful to Professor A . Stenderup for useful discussions and critical reading of the manuscript and to Head of the Department, dr. P. BiiloM' for his advice and support during the study.
This work was supported by grant No. 512-16174 from the Danish Medical Research Council.
REFERENCES
I . Andrews, H . 1. & Vickers, M.: An assessment of one year of computer-assisted microbiology reporting at Charing Cross hospital. J. Clin. Pathol. 27: 18s- 191. 1974.
2. GoodH,iii, C . S.: Computer printing and filing of microbiology reports. 2 Evaluation and comparison with a manual system and comparison of two manual systems. J. Clin. Pathol. 29: 553-560. 1976.
3. GoodH,iii . (. S & Smirh, B ('.: Computer printing and filing of microbiology reports. I Description of the system. J . Clin. Pathol. 29: 543-552. 1976
4. Micdiison. D. A , . Durrrl l. 1. H. di Miichison. R . : A computer-assisted bacteriology reporting and infor- mation system. J . Clin. Pathol. 31: 673-680. 1978.
S . Norbirr. A . M , Foit l is , P R . & K r i q . A . F.: Microcomputer reporting and information system
for microbiology. Am. J . Clin. Pathol. 76: SO-56. 1981.
6. Ridgu.o.v, G L . Botchelor, J . . L i m n , A . & Barnicoar, M . : Data processing in microbiology: an integrated simplified system. J . Clin. Pathol. 33: 744-749. 1980.
7. Whithj,. J . L . . Bluir, J N : Data processing in hospital bacteriology: experience of I8 months' trial. J. Clin. Pathol. 25: 338-343. 1972.
8. Williums, K . N , Daridsoii, J M . F . , Lynn, R . , Rice, t' & Phillips, 1 . . A computer system for clinical microbiology. J . Clin. Pathol. 31: 1193-1201. 1978.
126