a more dangerous heroin: presented at grand rounds, dept of psychiatry, rush university school of...
TRANSCRIPT

Dan Ciccarone, MD, MPH
Professor, Family and Community
Medicine
University of California, San Francisco
A More Dangerous ‘Heroin’:
Supply Changes, Adulteration and
Users’ Perceptions

DISCLOSURES
• No financial disclosures
• Some biases:
• A public servant
• Focus on public health

OBJECTIVES
• National data on heroin-related overdose
• Trends
• Demographics
• Regional differences
• Heroin and fentanyl supplies
• Qualitative: users’ perceptions

HEROIN IN TRANSITION (“HIT”) STUDY
• NIH: National Institute of Drug Abuse
• DA037820
• Multi-methodological study: quantitative and qualitative aims
• Supply changes – adulteration – overdose
• New drug forms and user perceptions, adaptation, etc.
PUBLICALLY AVAILABLE DATA:
• Centers for Disease Control and Prevention, National Center for
Health Statistics
• US Drug Enforcement Administration: National Drug Threat
Assessment 2016; National Heroin Threat Assessment, 2015

Leading Causes
of Death• Age-adjusted death
rates for the 10
leading causes of
death in 2015
NCHS Data Brief No. 267 December 2016. U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES
Centers for Disease Control and Prevention. National Center for Health Statistics
Mortality in the United States, 2015

0
2
4
6
8
10
12
14
16
Motor Vehicle -Traffic Drug Poisoning
Unintentional
Injury 1999-2012• Age-adjusted death
rates per 100,000 pop.
Produced by: National Center for Injury Prevention and Control, CDC
Data Source: NCHS Vital Statistics System for numbers of deaths. Bureau of Census for population
estimates. Accessed: 11.5.14

An Epidemic of
Crisis Proportion
Numbers of deaths:
• Drug overdose >
• Motor vehicle >
• Gun homicide >
• HIV
Source: New York Times, The Upshot; Josh Katz; April 14, 2017. Data from: Centers for Disease Control
and Prevention, National Center for Health Statistics

US Rx opioid
overdose admissions,
1993-2014:- Apogee reached in 2011

US heroin overdose
admissions,
1993-2014:- Sharp rise, doubling
since 2010

• Rising numbers of
heroin users
• Transitioning from
opioid pills:
• “Intertwined
Epidemics”
• “Every never…”
FUELING HEROIN-RELATED
OVERDOSE
Photo: F. Montero Castrillo

Photo: D. Ciccarone

Google trends: interest
in OxyContin vs heroin
vs _________
• US
• Health category
• Jan. 2006 to Nov.
2014
Data Source: Google Trends (www.google.com/trends)
Search: D Ciccarone, 11.3.14
Analysis: J Unick

NIS: US OVERDOSE RATES (2012-2014)
BY AGE GROUP:
Heroin overdoseOpioid overdose

NIS: OVERDOSE RATES (1993-2014)
BY GEOGRAPHIC REGION:
HOD: Northeast and
Midwest!OPOD: Even –

New England: Large
increases in heroin
OD hospitalizations
for 25-35 yo.

• Rising numbers of
heroin users
• Transitioning from
opioid pills
• Heroin becoming more
dangerous:
• Adulteration
• New forms
FUELING HEROIN-RELATED
OVERDOSE
Photo: D. Ciccarone

FENTANYL LACED HEROIN
• Integrated into heroin supply
• 30-40x stronger than heroin by weight
• Clandestinely-produced fentanyl, not diverted
pharmaceutical fentanyl*
• Analogous: Levamistole as adulterant for
cocaine
*National Heroin Threat Assessment Summary, DEA, 2015

SYNTHETICS
• In addition to fentanyl there are reports of:
Fentanyl analogues:
• Acetyl fentanyl
• Butyryl fentanyl
• Furanyl-fentanyl
• Parafluoro-fentanyl
• Carfentanil
Novel synthetics:
• U47700
• Others…
Photo: D. Ciccarone

FLOW OF FENTANYLS
DEA: National Drug Threat Assessment 2016

CDC: 27 states• Increases in
synthetic opioid
overdose deaths
• Concentrated in
7 states
Gladden RM, Martinez P, Seth P. Fentanyl Law Enforcement Submissions and Increases in Synthetic
Opioid–Involved Overdose Deaths — 27 States, 2013–2014. MMWR

NFLIS: Fentanyl• Testing seized drugs
• Highest rise in rates in
NE and MW
• Recent relative to
earlier rises in
heroin overdose
NATIONAL FORENSIC LABORATORY INFORMATION SYSTEM.
Special Report: Opiates and Related Drugs Reported in NFLIS, 2009–2014. Office
of Diversion Control, DOJ, DEA. 2015

TRENDS IN MORTALITY – TYPE OF
OPIOID

CDC’S LATEST DATA TO 2016
Source: Julia Lurie, Mother Jones, 9.6.2017
http://www.motherjones.com/politics/2017/09/the-latest-jaw-dropping-numbers-from-the-opioid-crisis/

Photo: D. Ciccarone

US heroin seizures are up
~ 140%, 2010-15
CHANGES IN THE HEROIN SUPPLY
Source: National Seizure System. Reported in the 2016 National Heroin Threat
Assessment Summary; DOJ, DEA, 2016
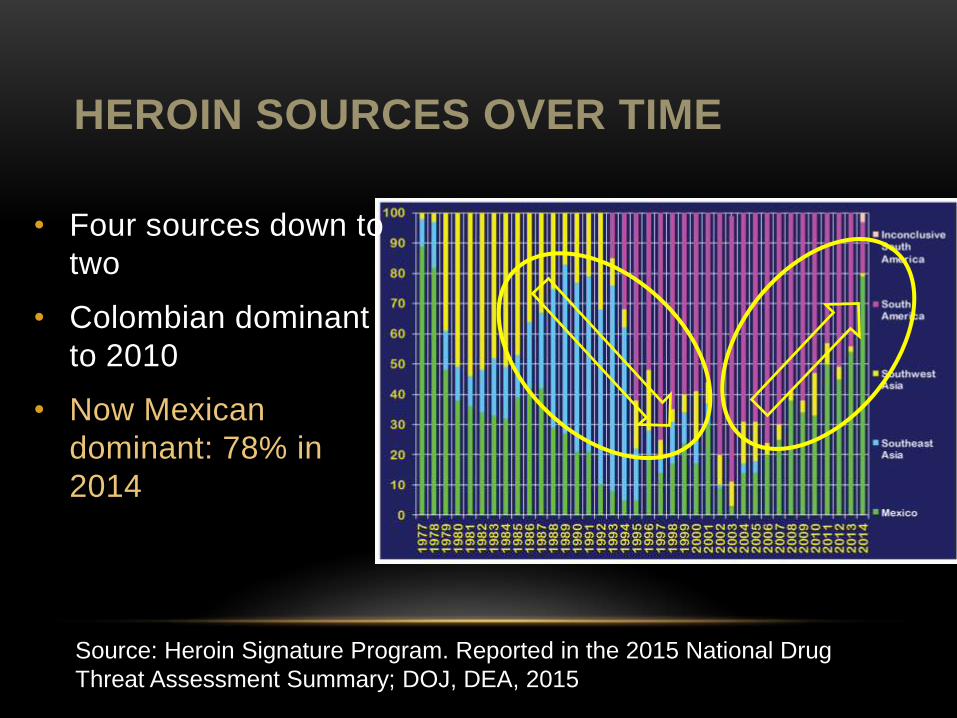
HEROIN SOURCES OVER TIME
Source: Heroin Signature Program. Reported in the 2015 National Drug
Threat Assessment Summary; DOJ, DEA, 2015
• Four sources down to
two
• Colombian dominant
to 2010
• Now Mexican
dominant: 78% in
2014

HEROIN OF UNKNOWN SOURCE
Source: Domestic Monitoring Program. Reported in the 2015 National Drug Threat
Assessment Summary; DOJ, DEA, 2015

MEXICAN TCOs: FLOW OF HEROIN TO
US

MEXICAN-SOURCED HEROIN: CHANGES
• Mexican opium/heroin production has grown while
Colombian production is down 40%
• Explanations for rising HOD in Midwest (in addition to
fentanyl):
• A more purified product coming from Mexico
• “Mexican White:” Colombian mimic
Traditional Colombian-sourced-heroin retail places
Synthetic adulteration > heroin “inconclusive” origin

• The novel entry of Colombian-sourced heroin increased HOD rates; 1993-1999
• New increases in HOD:
• Regional!
• New form of Mexican-sourced heroin
• (+)Fentanyl adulteration
• Wider distribution models
• Young users
SUMMARY: HEROIN IN TRANSITION

Sarah MarsFamily and Community Medicine
University of California, San Francisco
Jeff OndocsinEthnographer and Analyst
HEROIN IN TRANSITION:
THE EXPERIENCES OF
HEROIN INJECTORS

STUDY AIMS
“Hotspot study” where our team of researchers goes to visit
areas in the country where significant changes in the heroin
supply or overdoses have been reported
Baltimore, MD; Lawrence and Lowell, MA; Chicago, IL;
Charleston, West Virginia
Our aim is to understand the experiences and beliefs of the
users themselves and to observe first hand the heroin
currently being used

Photos: D. Ciccarone

1. DEVASTATION: ‘LIKE A ‘COMBAT
STATE’
Now the dope is fentanyl and it’s killing people left and
right. I have over the years, I’ve watched friends [die]—
but on average, it was three a year. Now the last 3 years
it’s been an average of 20 [per year]. I feel like I’m back
in a combat state and I feel like I’m fighting for my life
right now.
Jerry, Lowell, aged 46, using on and off for the
last 20 years


2. CHANGES IN ‘HEROIN’ Users reported and our ethnographers observed wide
variations in the appearance of and effects due to
substances sold as ‘heroin’
Supply not demand driven changes:
– Users surprised and dismayed
– Range of desirability
– No cultural idioms
– Dealers even surprised

We’re supposedly buying dope that doesn’t have any
fentanyl in it, but when I started showing up dirty with
heroin, I started showing up dirty with fentanyl… When
we cut the dope, we don’t use fentanyl. The problem
was that we were buying the dope already dirty with
that and we didn’t know it.
Hector, aged 42, using heroin for 26 years
Lawrence, MA


3. VARIATION AND
UNPREDICTABILITY
Heroin varied by:
- Color: powder and solution
- Intensity of onset or ‘rush’
- Intensity of effect
- Duration of effect (from 45 minutes to 12 hours)
- Types of effect eg sleepy or stimulating

HEROIN SOURCE-FORMS
“Black Tar” Heroin: Mexican
Brown powder Heroin:
Colombian/SWA
White powder Heroin: SEA

NEW HEROIN FORMS



4. DESIRABILITY
The high is wonderful. It’s splendidly wonderful. It’s
magnified heroin feeling by a great number.
Tim, aged 45, using heroin for 25 years, Baltimore
I know a couple of people have done died from that, with
fentanyl, yeah. […] And I have a lot of associates that are
letting me know, “Don’t go to that place because they
selling fentanyl”.
Montana, 39 year old woman using for 21 years,
Baltimore


5. DISCERNMENT
Hierarchy:
- Physiological >
- Taste on the tongue >
- Solution color >
- Powder color

When you add the water to it and pull it back it’s almost
like clear. Heroin’s dark and brown. It’s brown. …but the
fentanyl is like, like water kinda, like a little bit yellowish...
The regular heroin …it can be dark brown or light brown
but it’s never yellow like that.
Kristin, 19 years old, using heroin for 5 years,
Lowell, MA


6. GENERATIONAL CHANGES
• 50 yo African American male, Englewood Chicago about violence in Chicago and the increase in homicides:
• A: A lot of guys are older now, like me. I’m 50 years old. My gang banging days have been over a long time ago. So you got a lot of people with a lot of rank they’re going to jail and they ain’tgetting out no time soon.
• Q: So the youngsters take over?
• A: So the young, so yeah they’re trying to recruit younger guys and these younger guys they’re recruiting they’re putting guns in their hand and they just going buck wild. They’re not following the rules or the laws of the gang that they’re in, they’re trying to rewrite the laws and do what they want to do.

7. TAKING PRECAUTIONS
Like when I get stuff I don’t know what it is I do a little bit
before I do something that I feel. Like I want to kind of
scale out how much I want to do. Because I don’t want to
die. But these people are just doing a gram shot and
just… my friend just died two days ago.
Liz, in her 20s, using heroin for 1.5 years
Lawrence, MA

GO SLOW, STAY IN CONTROL

SUMMARY
Devastation is rampant: individual, social, cultural
Changes in heroin: supply driven
Variation in potency, compounded by fentanyl: ‘Russian
roulette’
Mixed desirability for fentanyl
Some degree of discernment
A new generation needs risk reduction guidance
Some organic harm reduction > pay attention to this!

An Epidemic of
Crisis Proportion
• Crisis with Epic
Opportunity
• Treatment and
Prevention can
work!
Source: New York Times, The Upshot; Josh Katz; April 14, 2017

CRISIS RESPONSE
• Prescription pills ≠ Heroin/fentanyl
• Better surveillance is needed
• Hint: fentanyl as poisoning epidemic
• More evidence-based treatment
• CARA is good but not enough
• Faster responses to overdose
• Stigma remains our biggest enemy
• Harm reduction saves lives, is cost-effective and can bridge people into treatment
• Public safety – Public health collaborations


ACKNOWLEDGEMENTS
Heroin in Transition study:
Jay Unick, Univ. of Maryland
HIT team: Sarah Mars, Jeff Ondocsin, Eliza Wheeler, Mary Howe, Fernando Castillo, Philippe Bourgois, Dan Rosenblum
NIH/NIDA funding: R01DA037820
Chicago:
Dan Bigg, Chicago Recovery Alliance
Baltimore City Health Dept.
Mishka Terplan, Derrick Hunt, Jeffrey Long and NEP staff
Massachusetts:
Gary Langis, Harry Leno, Irving
West Virginia:
Mike Brumage, Tina Ramirez;
Staff and volunteers at Kanawha-Charleston Health Dept.
Jon E. Zibbell
Participants!
Photo credits: Dan Ciccarone, Fernando Castillo