a multinomial phase ii study of lonafarnib (sch 66336) in patients with refractory urothelial...
TRANSCRIPT

A
GRs
tr
TnNm
c
K
1
cs
P
1d
Original article
A multinomial Phase II study of lonafarnib (SCH 66336) in patientswith refractory urothelial cancer�
Eric Winquist, M.D., M.Sc.a,*, Malcolm J. Moore, M.D.b, Kim N. Chi, M.D.c,D. Scott Ernst, M.D.d, Hal Hirte, M.D.e, Scott North, M.D.f, Jean Powersg,
Wendy Walsh, M.Sc.g, Therese Boucherh, Robert Patton, Ph.D.i, Lesley Seymour, M.D.g
a London Regional Cancer Centre, London, Ontario, Canadab Princess Margaret Hospital/University Health Network, Toronto, Ontario, Canada
c BC Cancer Agency, Vancouver, British Columbia, Canadad Tom Baker Cancer Centre, Calgary, Alberta, Canada
e Hamilton Regional Cancer Centre, Hamilton, Ontario, Canadaf Cross Cancer Centre, Edmonton, Alberta, Canada
g National Cancer Institute of Canada Clinical Trials Group, Kingston, Ontario, Canadah Schering-Plough Canada Inc., Point Claire, Quebec, Canada
i Schering-Plough Research Institute, Kenilworth, NJ, USA
Received 29 December 2003; received in revised form 12 November 2004; accepted 15 November 2004
bstract
Purpose: Protein farnesylation by farnesyltransferase (FTase) is required for membrane localization and effective signal transduction by-proteins, including Ras. Lonafarnib inhibits FTase and has shown antitumor activity in both preclinical and clinical settings. As disturbances inas signaling pathways have been implicated in the pathogenesis of transitional cell carcinoma (TCC), the antitumor activity of lonafarnib was
tudied in a National Cancer Institute of Canada Clinical Trials Group Phase II trial in patients with previously treated TCC.Patients and Methods: Patients had at least 1 prior chemotherapy regimen for advanced unresectable or metastatic TCC, or recurrence less
han 1 year after adjuvant or neoadjuvant chemotherapy. Lonafarnib was given at a dose of 200 mg PO twice daily continuously, with cyclesepeated every 4 weeks.
Results: Between December 1999 and December 2000, 19 eligible patients were enrolled at 8 National Cancer Institute of Canada Clinicalrials Group centers. Median time on treatment was 7.1 weeks (range, 0.6–23.9). Drug-related Grade 3 toxicities included fatigue, anorexia,ausea, confusion, dehydration, muscle weakness, depression, headache, and dyspnea. Five patients discontinued the study protocol due to toxicity.o responses were observed in 10 patients who were evaluable. Of 9 patients not evaluable for response, 5 had symptomatic progression, fulfillingultinomial criteria to stop the study after the first stage.Conclusion: No single-agent activity of lonafarnib was observed in this study of patients with aggressive TCC failing prior
hemotherapy. © 2005 Elsevier Inc. All rights reserved.
Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
eywords: Bladder neoplasms; Drug therapy; Farnesyltransferase; Lonafarnib
ttkcilp[l
. Introduction
Cellular Ras proteins are bound to the internal surface of theell membrane and subserve a critical role in growth factorignaling pathways linking cell surface receptors to nuclear
� This study was supported by the National Cancer Institute and Schering-lough Canada Inc.
* Corresponding author. Tel.: �1-519-685-8600; fax: �1-519-685-8624.
dE-mail address: [email protected] (E. Winquist).078-1439/05/$ – see front matter © 2005 Elsevier Inc. All rights reserved.oi:10.1016/j.urolonc.2004.12.012
ranscription factors [1]. Specifically, activated Ras proteinsrigger a cascade of phosphorylation events through the PI3inase/AKT and Raf/Mek/Erk kinase pathways, implicated inell survival and cell proliferation, respectively [2]. Mutationsn Ras proteins typically inhibit guanosine triphosphate hydro-ysis, inducing a continuous mitogenic signal and a malignanthenotype, and these are associated with many human cancers3,4]. Ras signaling may be pharmacologically targeted at theevel of Ras protein expression, Ras protein processing, and
ownstream Ras effectors [5]. Ras proteins require posttrans-
l(aslbenpFTwts(
dcerw[rocPndiciPctns3Dt
A2cT5avs[ahpoea4
hniaoHpic
2
2
hmasrcpmTpd�(�hmttaomtaiHc
2
PrBlfgatt
144 E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
ational isoprenoid lipid modification by farnesyltransferaseFTase) for activity, and a number of drugs with preclinicalctivity as FTase inhibitors (FTI) have been identified andtudied in cancer patients. The HMG-CoA reductase inhibitorovastatin and the limonene derivative perillyl alcohol haveeen studied because of FTI activity but have shown littlevidence of clinically significant antitumor activity [6–8]. Aumber of drugs investigated for FTI activity have shownreclinical evidence of antitumor activity including L-778123,TI-277, FTI-2153, RPR-115135, and RPR-130401 [9–13].hree drugs have shown activity as single agents in patientsith leukemia, myelodysplastic syndromes, or refractory solid
umors, and are undergoing further clinical study either asingle agents or in combination with cytotoxics: tipifarnibR115777), lonafarnib (SCH 66336), and BMS-214662 [5].
Lonafarnib is an orally, bioavailable tricyclic nonpepti-yl nonsulfhydryl FTI with preclinical activity in humanancers expressing H-ras and K-ras [14]. Phase I trials havevaluated several dosing schedules. Adjei et al identified aecommended Phase II dose (RP2D) of 350 mg PO bidhen lonafarnib was given for 7 consecutive days out of 21
15]. Gastrointestinal toxicity (nausea, vomiting, and diar-hea) and fatigue were dose-limiting toxicities (DLT), andne partial response in a patient with nonsmall cell lungancer was seen. Hurwitz et al identified a RP2D of 200 mgO bid when given for 14 consecutive days out of 28, withausea, diarrhea, and malaise as DLT [16]. In a continuousosing study, Eskens et al reported DLT of Grade 4 vom-ting, Grade 4 neutropenia and thrombocytopenia, and theombination of Grade 3 anorexia and diarrhea, with revers-ble Grade 3 plasma creatinine increase at a dose of 400 mgO bid [17]. After dose reduction, at 300 mg bid, the DLTonsisted of Grade 4 neutropenia, Grade 3 neurocorticaloxicity, and a combination of Grade 3 fatigue with Grade 2ausea and diarrhea. The recommended dose for Phase IItudies was 200 mg bid. Awada et al identified a RP2D of00 mg PO, with continuous once daily dosing with similarLT [18]. No patients with urothelial cancer were studied in
hese trials.Bladder cancer is the fifth most common cancer in North
merican men and caused over 13,000 deaths in the U.S. in003 [19]. Transitional cell cancer (TCC or urothelial can-er) is the most common histologic subtype. MetastaticCC is a virulent but chemosensitive neoplasm. Although0% of patients will have objective response to chemother-py, such as gemcitabine plus cisplatin or methotrexate,inblastine, doxorubicin, and cisplatin (M-VAC); nearly alluccumb to progressive disease within 2 years of treatment20]. Paclitaxel is the most active and commonly used singlegent in TCC refractory to cisplatin-based chemotherapy;owever, the most active paclitaxel-based combination re-orts a response rate of less than 50% and median survivalf 7.5 months [21–23]. Ras mutations occur in 30% ofpithelial cancers, usually K-ras. Only mutations in H-rasre important in TCC and have been detected in 30% to
5% of tumors [24,25]. Increased transcription of Ras genes mas been observed in bladder cancer specimens relative toormal epithelium [26]. Activity of lonafarnib was observedn 1 of 2 bladder tumors using the human tumor cloningssay [27]. Thus, our rationale for this trial was a pragmaticne, based on limited preclinical data, the theoretical role of-ras, and limited efficacy of standard therapies in thisopulation, to evaluate the antitumor activity of lonafarnibn patients with urothelial cancer refractory to first-lineytotoxic treatment.
. Patients and methods
.1. Patients
Eligible patients were at least 18 years of age and hadistologically or cytologically confirmed TCC, and docu-ented evidence of locally advanced unresectable or met-
static disease not amenable to curative radiotherapy orurgery. Patients had a minimum of one prior chemotherapyegimen for advanced disease, or had progressed after re-eiving adjuvant or neoadjuvant chemotherapy within therevious 12 months. Patients were required to have diseaseeasurable by the Response Evaluation Criteria in Solidumors criteria, an Eastern Cooperative Oncology Grouperformance Status � 2, and adequate organ function asefined by: granulocyte count � 1,500/mm3, platelet count
100,000/mm3, serum creatinine � 1.5 upper normal limitUNL) or creatinine clearance � 50 ml/min, serum bilirubin
1.5 UNL, AST � 2.5 UNL or � 5 UNL if documentedepatic metastases, and serum calcium within 10% of nor-al range. Exclusion criteria included known brain or lep-
omeningeal disease, uncontrolled infection, concurrentreatment with other experimental drugs or anticancer ther-py, serious illness or medical conditions, clinical evidencef congestive heart failure, myocardial infarction within 6onths, QTc prolongation more than 440 msec, and bone as
he only site of measurable disease. The study was reviewednd approved by the Research Ethics Board of each partic-pating institution, was conducted in accordance with theelsinki Declaration, and all patients gave written informed
onsent.
.2. Study design
This was a multicenter, open-label, single-arm 2-stagehase II study, with a multinomial endpoint that consideredates of both objective response and progressive disease.aseline investigations included physical and ophthalmo-
ogical examination, complete blood count (CBC) and dif-erential CBC, serum chemistries, urinalysis, electrocardio-ram, chest x-ray, abdominal computerized tomography,nd any additional imaging required to image the sites ofumor for baseline measurement. While on treatment, pa-ients were reassessed every 4 weeks with toxicity assess-
ent, repeat physical examination including clinical tumor
memmciwabcBbt
2
wgiSwfotaTd2mdRw
2
RTr
opes
2
eeipst8persftopmsaipnp2cgom
2
TS
S
R
�
01*
a
145E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
easurements, CBC and serum chemistries, urinalysis, andlectrocardiogram. A CBC was performed weekly, and tu-or imaging was obtained every 8 weeks. Protocol treat-ent was discontinued for tumor progression, severe inter-
urrent illness, unacceptable toxicity, or at patient ornvestigator request. Blood for pharmacokinetic analysisas obtained pre-dose day 1 of the first treatment cycle 1,
nd approximately 12 hours after the prior evening dose,efore the morning does, on day 15 of the first 2 treatmentycles, and day 15 of any cycle following dose adjustment.lood for the assessment of FTase inhibition in peripherallood monocytic cells (PBMC) was obtained on day 15 ofhe first treatment cycle.
.3. Toxicity and dose modifications
All patients receiving at least one dose of lonafarnibere considered evaluable for toxicity. Toxicities wereraded using the National Cancer Institute Common Tox-city Criteria Version 2.0 [28]. Lonafarnib was supplied bychering Canada Inc. as 50 mg and 100 mg capsules, andas given at a starting dose of 200 mg twice daily PO with
ood as in previous Phase I studies. If any Grade 3 toxicityr prolongation of QTc more than 500 msec occurred,reatment was discontinued until this resolved to � Grade 1,nd then continued with a 50 mg per day dose reduction.reatment was discontinued if Grade 4 toxicity or 2 priorose reductions for toxicity occurred. Patients completing a8-day cycle without � Grade 2 toxicity could have aaximum of 2 dose increases from 200 to 250 mg PO twice
aily, and from 250 to 300 mg PO twice daily, respectively.outine antiemetics were not used. Patients were suppliedith loperamide and instructions in its use for diarrhea.
.4. Response assessment
Tumor response and progression were evaluated usingesponse Evaluation Criteria in Solid Tumors criteria [29].umor imaging studies were performed at baseline and
able 1tudy design
H0: p1 � 0.05 and p2 � 0
tage I
eject Drug Accept Drug
resp/n1 � prog/n1 � resp/n1 �
/15 * 0/15 4/1/15 7/15 3/15 5/1
9/15 4/15 *
resp/n1, Proportion responding in first stage; prog/n1, proportion progrelternate hypothesis true.
* Denotes all possible values.
epeated every 2 cycles. Patients who had received at least p
ne cycle of therapy and had their disease reevaluated, andatients who had objective disease progression before thend of the first cycle were considered evaluable for re-ponse.
.5. Statistical methods
A primary multinomial endpoint combining response andarly progression was used (Table 1) [30]. To minimize thexpected number of patients treated in the event that the reg-men proved very disappointing, a 2-stage design was used foratient accrual. A multinomial endpoint considering both re-ponse and early progression rates was used to determinereatment activity using a Type I error of 5% and power of0%. This study design was intended to permit termination ofatient accrual after the first 15 patients were treated in thevent that extreme results were observed. If such extremeesults were not observed, a maximum of 30 patients would betudied. It was assumed that the new regimen would not be ofurther interest in TCC if the true tumor response rate was lesshan 5% and that a true response rate of 20% or more would bef considerable interest. Because the response rate was ex-ected to be small, early progression was used as anothereasure of efficacy. Early progression was defined as progres-
ive disease observed within 8 weeks of treatment. It wasssumed that the new regimen would not be of further interestf the true early progression rate was 60% and that a true earlyrogression rate of 40% or less would be of interest. Assumingull hypotheses for response (p1) to be 5% and for earlyrogression (p2) to be 60% versus alternative hypotheses of0% for response and 40% for early progression, stoppingriteria based on both proportions of response and early pro-ression were developed. Median time to progression andverall survival were calculated using the Kaplan-Meierethod [31].
.6. Pharmacokinetic and pharmacodynamic analyses
Lonafarnib plasma concentration was measured using high-
1: p1 � 0.2 or p2 � 0.4
Stage II
Accept Drug
� resp/n � prog/n
1/30 12/30 � � 0.0502/30 13/30 1-� � 0.803/30 14/30 EN0 � 16.64/30 16/30 EN1 � 20.2
first stage; EN0, Sample size if null hypothesis true; EN1, sample size if
.6 vs H
prog/n1
55
ssing in
erformance liquid chromatography/tandem mass spectromet-

rqsKnusmaPcmflp
3
3
pChdyO
mrpcvvdoopn
3
Tnntecttd4s
bwratmtkGt
3
w(dNtbpdftota(
TP
C
MG
P
P
P
S
N
D
146 E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
ic method performed at Taylor Technology, Princeton, NJ. Touantify FTase inhibition, a FTase substrate, HDJ-2, was as-ayed in PBMC at the Schering Plough Research Institute,enilworth, NJ. HDJ-2 is exclusively a substrate for FTase, isot a substrate for geranylgeranyltranferase and, unlike Ras, isbiquitously expressed and can be assayed in PBMC. Farne-ylated and unfarnesylated forms of HDJ-2 show a pronouncedobility shift in sodium dodecyl sulfate-polyacrylamide gels,
nd the amount of each form in a sample can be quantified.ercent inhibition of PBMC FTase activity was calculated byomparing HDJ-2 activity after treatment with day 1 pretreat-ent levels. Buffy coat samples for PBMC were centrifuged,ash frozen, and stored at –70 C until HDJ-2 assays com-leted.
. Results
.1. Patients
Between December 1999 and December 2000, 19 eligibleatients were enrolled at 8 National Cancer Institute of Canadalinical Trials Group centers (Table 2); one additional patientad received 2 prior chemotherapy regimens for metastaticisease and was considered ineligible. The median age was 65ears (range, 49–84 years), and median Eastern Cooperative
able 2atient characteristics
haracteristic No. pts.
edian age (range) 65 years (49–84) 19ender Female 4
Male 15erformance status (ECOG) 0 3
1 132 3
athology Mixed 1Transitional 18
rior therapy Chemotherapy for metastaticdisease
18
Adjuvant chemotherapy 4Chemoradiotherapy 2
ites of disease Lymph nodes 16Bladder/pelvis 10Lung 7Liver 6Bone 4Abdomen 3Subcutaneous 2Adrenal 2
o. sites of disease 1 32 63 44 or more 6
isease extent Distant nodal/visceralmetastases
11
Local/pelvic nodal 8
ncology Group performance Status was 1 (range, 0–2). Pri- (
ary tumor sites were bladder (15 patients), ureter (3), andenal pelvis (1). Disease in 18 patients had progressed despiterior chemotherapy for metastatic disease: gemcitabine plusisplatin (7 patients); gemcitabine (3 who had received adju-ant M-VAC or cytomegalovirus); M-VAC (2); methotrexate,inblastine, mitoxantrone, and carboplatin (2); liposomaloxorubicin (2); cytomegalovirus (1); and carboplatin, meth-trexate, and vinblastine (1). One patient had recurrence withinne year of postoperative adjuvant therapy with vinblastinelus carboplatin. The most common disease sites were lymphodes, bladder or pelvis, and lung.
.2. Treatment and toxicity
Median time on treatment was 7.1 weeks (range, 0.6–23.9).hree patients had dose reductions due to toxicity (Grade 2ausea despite antiemetics; Grade 2 fatigue, anorexia, andausea; and Grade 3 fatigue, depression, and nausea; respec-ively). No patients had dose increase. Disease progression,ither objective (8 patients) or symptomatic (5), was the mostommon reason for discontinuing study treatment. Five pa-ients discontinued study treatment because of the followingoxicities: Grade 3 confusion; Grade 3 anorexia, nausea, andehydration; Grade 2 tachycardia and atrial fibrillation; Gradeanemia and Grade 3 thrombocytopenia; and Grade 2 altered
ense of smell with Grade 2 nausea and vomiting.All 19 patients were considered evaluable for toxicity (Ta-
le 3). No toxic deaths or nonhematological Grade 4 toxicitiesere observed. The most common nonhematological toxicities
elated to lonafarnib were nausea, anorexia, vomiting, diarrhea,nd fatigue. Grade 3 nonhematological toxicities included fa-igue, anorexia, nausea, vomiting, confusion, dehydration,uscle weakness, depression, headache, and dyspnea. Hema-
ological toxicity was mild-to-moderate, with � Grade 3 leu-openia or neutropenia observed in 2 patients, anemia in 3, andrade 3 thrombocytopenia in a single patient. Biochemical
oxicity was mild.
.3. Response
Ten patients were evaluable for response: no responsesere observed (response rate 0% [95% confidence interval
95% CI), 0% to 25.9%]). Two patients had stable disease ofuration 3.5 and 5.9 months, and 8 had progressive disease.ine patients were not evaluable for response. Of these pa-
ients, 1 died and 4 discontinued treatment due to toxicityefore disease reevaluation. The other 4 patients were taken offrotocol for symptoms attributed to cancer progression beforeisease reevaluation (bone metastases, hematuria and renalailure, declining functional status, and diarrhea with dehydra-ion, respectively). Therefore, because more than 60% (12/19)f patients had early progression and the response rate was lesshan 5%, the study met multinomial criteria to stop accrualfter the first stage. Median time to progression was 1.4 months95% CI, 1.3–1.8), and median overall survival was 3.1 months
95% CI, 2.0–5.8).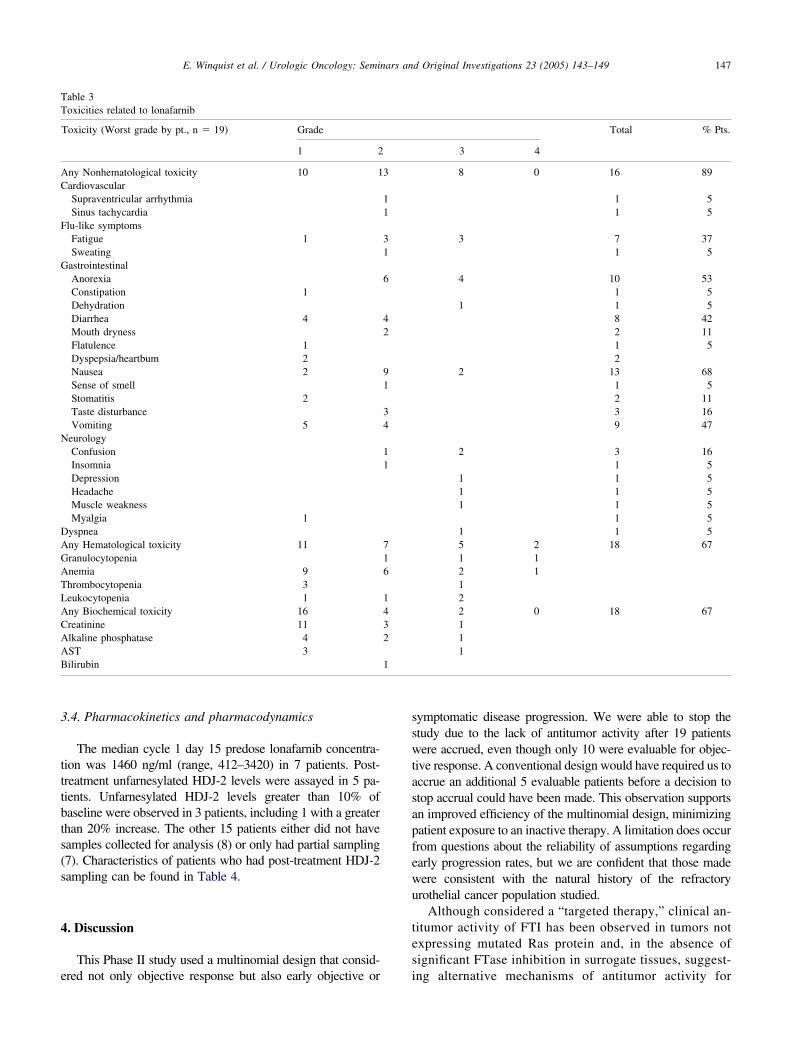
3
tttbts(s
4
e
sswtasapfewu
tes
TT
AC
F
G
N
DAGATLACAAB 1
147E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
.4. Pharmacokinetics and pharmacodynamics
The median cycle 1 day 15 predose lonafarnib concentra-ion was 1460 ng/ml (range, 412–3420) in 7 patients. Post-reatment unfarnesylated HDJ-2 levels were assayed in 5 pa-ients. Unfarnesylated HDJ-2 levels greater than 10% ofaseline were observed in 3 patients, including 1 with a greaterhan 20% increase. The other 15 patients either did not haveamples collected for analysis (8) or only had partial sampling7). Characteristics of patients who had post-treatment HDJ-2ampling can be found in Table 4.
. Discussion
This Phase II study used a multinomial design that consid-
able 3oxicities related to lonafarnib
Toxicity (Worst grade by pt., n � 19) Grade
1 2
ny Nonhematological toxicity 10 1ardiovascularSupraventricular arrhythmiaSinus tachycardia
lu-like symptomsFatigue 1Sweating
astrointestinalAnorexiaConstipation 1DehydrationDiarrhea 4Mouth drynessFlatulence 1Dyspepsia/heartbum 2Nausea 2Sense of smellStomatitis 2Taste disturbanceVomiting 5
eurologyConfusionInsomniaDepressionHeadacheMuscle weaknessMyalgia 1
yspneany Hematological toxicity 11ranulocytopenianemia 9hrombocytopenia 3eukocytopenia 1ny Biochemical toxicity 16reatinine 11lkaline phosphatase 4ST 3ilirubin
red not only objective response but also early objective or i
ymptomatic disease progression. We were able to stop thetudy due to the lack of antitumor activity after 19 patientsere accrued, even though only 10 were evaluable for objec-
ive response. A conventional design would have required us toccrue an additional 5 evaluable patients before a decision totop accrual could have been made. This observation supportsn improved efficiency of the multinomial design, minimizingatient exposure to an inactive therapy. A limitation does occurrom questions about the reliability of assumptions regardingarly progression rates, but we are confident that those madeere consistent with the natural history of the refractoryrothelial cancer population studied.
Although considered a “targeted therapy,” clinical an-itumor activity of FTI has been observed in tumors notxpressing mutated Ras protein and, in the absence ofignificant FTase inhibition in surrogate tissues, suggest-
Total % Pts.
3 4
8 0 16 89
1 51 5
3 7 371 5
4 10 531 5
1 1 58 422 111 52
2 13 681 52 113 169 47
2 3 161 5
1 1 51 1 51 1 5
1 51 1 55 2 18 671 12 1122 0 18 67111
3
11
31
6
42
91
34
11
716
1432
ng alternative mechanisms of antitumor activity for

trmltpfcrcseiii
lipebpmaifoHlBw
PbiaaecmsrOeF
tlmtthtdaao
A
tIrRnw
R
TC
12345
tomatic
148 E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
hese drugs [2]. On the basis of this result, as well as theapid progression rate typically observed with these tu-ors, tumor biopsies before and following treatment with
onafarnib were not performed in this study. We intendedo study farnesylation in PBMC, but only a minority ofatients had complete specimen collection. The reasonsor this result are not clear but may be due to a lack oflarity in the trial protocol, leading investigators and theiresearch personnel to consider these studies optional. Thelear implication is that the importance of correlativetudies in studies of molecular therapies cannot be over-mphasized to clinical investigators and patients. Thismplication is of particular importance in negative trials,n which the reasons for the lack of activity are ofnterest.
This study identified no objective antitumor activity ofonafarnib, an orally bioavailable FTI, in patients withncurable urothelial cancer relapsed or progressing afterrior chemotherapy. There are a number of potentialxplanations for the lack of activity observed. Inadequateioavailability is unlikely based on Phase I and our ownharmacokinetic data. Inhibition of FTase activity inalignant cells may have been inadequate but was not
ssayed directly. However, 3 of 5 patients had significantnhibition of farnesylation in PBMC. The study of lona-arnib in urothelial cancer was of interest in part becausef frequent H-ras expression reported in this tumor type.owever, it is possible that mutant Ras expression was
ess frequent than anticipated in the population studied.ecause tumor biopsies were not performed in this study,e did not assay for this.Our results support hypotheses that inhibition of the
I3 kinase/AKT or Raf/Mek/Erk pathways with FTI maye either of less importance or more difficult to achieven refractory urothelial cancer. Disease had progressed inll patients in this study during or after prior chemother-py, and the selection of drug resistant clones would bexpected to ameliorate the effects of any subsequentancer treatment. Rapid disease progression was com-on, suggesting that further study of this drug in this
etting should be performed only with a strong preclinicalationale and in combination with known active agents.ur rationale was an empiric one, as little preclinical
vidence of activity of lonafarnib in TCC was available.
able 4haracteristics of patients who had post-treatment HDJ-2 sampling
Pt. No Years of Age/Sex Sites of disease
84/Male Distant67/Male Local59/Male Distant69/Female Local72/Male Local
IN, inevaluable; PD, progressive disease; SD, stable disease; SP, symp
TI are currently being studied in combination with cy-
otoxics, hormonal agents, radiotherapy, and other mo-ecular-based agents [2]. Combination therapy may be a
ore effective approach because recent reports indicatehat lonafarnib may have activity as an inhibitor of mul-idrug resistance [32,33]. Inhibition of farnesylation mayave more influence earlier in the natural history ofransitional cancer. This result would support the study ofrugs such as lonafarnib in superficial urothelial cancer,setting that also provides easy access to both normal
nd malignant transitional epithelium for the assessmentf clinical and pharmacodynamic effects.
cknowledgments
We thank the following investigators who, in addition tohe coauthors, enrolled patients on this study: Dr. Neillscoe, Toronto-Sunnybrook Regional Cancer Centre, To-onto, Ontario, Canada; Dr. Roanne Segal-Nadler, Ottawaegional Cancer Centre, Ottawa, Ontario; and Dr. Ian Tan-ock, Princess Margaret Hospital/University Health Net-ork, Toronto, Ontario.
eferences
[1] Downward J. Targeting RAS signalling pathways in cancer therapy.Nat Rev Cancer 2003;3:11–22.
[2] Haluska P, Dy GK, Adjei AA. Farnesyl transferase inhibitors asanticancer agents. Eur J Cancer 2002;38:1685–1700.
[3] Brandau S, Bohle A. Bladder cancer. I. Molecular and genetic basisof carcinogenesis Eur Urol 2001;39:491–7.
[4] Rodenhuis S. Ras and human tumors. Semin Cancer Biol 1992;3:241–7.
[5] Dancey JE. Agents targeting ras signaling pathway. Curr Pharm Des2002;8:2259–67.
[6] Larner J, Jane J, Laws E, et al. A phase I-II trial of lovastatin foranaplastic astrocytoma and glioblastoma multiforme. Am J Clin On-col 1998;21:579–83.
[7] Bailey HH, Levy D, Harris LS, et al. A phase II trial of daily perillylalcohol in patients with advanced ovarian cancer: Eastern Coopera-tive Oncology Group Study E2E96. Gynecol Oncol 2002;85:464–8.
[8] Hudes GR, Sazarka CE, Adams A, et al. Phase I pharmacokinetic trialof perillyl alcohol (NSC 641066) in patients with refractory solidmalignancies. Clin Cancer Res 2002;6:3071–80.
[9] Hahn SM, Bernhard EJ, Regine W, et al. A phase I trial of thefarnesyltransferase inhibitor L-778,123 and radiotherapy for locallyadvanced lung and head and neck cancer. Clin Cancer Res 2002;8:
Time on treatment(weeks)
Best response � 10% Shift
9 IN (SP) No7.3 IN (SP) ✓
23.9 PD ✓
7.1 PD No8.1 SD ✓ (�20%)
progression.
1065–72.

[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
[
149E. Winquist et al. / Urologic Oncology: Seminars and Original Investigations 23 (2005) 143–149
10] Bolick SC, Landowski TH, Boulware D, et al. The farnesyltransferaseinhibitor, FTI-277, inhibits growth and induces apoptosis in drug-resistant myeloma tumor cells. Leukemia 2003;17:451–7.
11] Sun J, Blaskovich MA, Knowles D, et al. Antitumor efficacy of anovel class of non-thiol-containing peptidomimetic inhibitors of far-nesyltransferase and geranylgeranyltransferase I: Combination ther-apy with the cytotoxic agents cisplatin, Taxol, and gemcitabine.Cancer Res 1999;59:4919–26.
12] Russo P, Arzani D, Trombino S, et al. c-myc down-regulation inducesapoptosis in human cancer cell lines exposed to RPR-115135(C31H29NO4), a non-peptidomimetic farnesyltransferase inhibitor.J Pharmacol Exp Ther 2003;304:37–47.
13] Megnin-Chanet F, Lavelle F, Favaudon V. The farnesyl transferaseinhibitor RPR-130401 does not alter radiation susceptibility in humantumor cells with a K-Ras mutation in spite of large changes in ploidyand lamin B distribution. BMC Pharmacol 2002;2:2.
14] Liu M, Bryant MS, Chen J, et al. Antitumor activity of SCH 66336,an orally bioavailable tricyclic inhibitor of farnesyl protein trans-ferase, in human tumor xenograft models and wap-ras transgenicmice. Cancer Res 1998;58:4947–56.
15] Adjei AA, Erlichman C, Davis JN, et al. A phase I trial of the farnesyltransferase inhibitor SCH66336: evidence for biological and clinicalactivity. Cancer Res 2000;60:1871–7.
16] Hurwitz HI, Colvin OM, Petros WP, et al. Phase I and pharmacoki-netic study of SCH66336, a novel FPTI, using a 2-week on, 2-weekoff schedule [abstract]. Proc Am Soc Clin Oncol 1999;18:156a.
17] Eskens FA, Awada A, Cutler DL, et al. Phase I and pharmacokineticstudy of the oral farnesyl transferase inhibitor SCH 66336 given twicedaily to patients with advanced solid tumors. J Clin Oncol 2001;19:1167–75.
18] Awada A, Eskens FA, Piccart M, et al. Phase I and pharmacologicalstudy of the oral farnesyltransferase inhibitor SCH 66336 given oncedaily to patients with advanced solid tumours. Eur J Cancer 2002;38:2272–8.
19] National Cancer Institute. SEER Cancer Statistics Review, 1975–2000. Available at: http://seer.cancer.gov/csr/1975 2000/results_s-ingle/sect_01_table.01.pdf. Accessed January 6, 2005.
20] von der Maase H, Hansen SW, Roberts JT, et al. Gemcitabine and
cisplatin versus methotrexate, vinblastine, doxorubicin and cisplatinin advanced or metastatic bladder cancer: Results of a large,randomized multicenter phase III study. J Clin Oncol 2000;18:3068–77.
21] Dreicer R, Gustin DM, See WA, et al. Paclitaxel in advanced urothe-lial carcinoma: Its role in patients with renal insufficiency and assalvage therapy. J Urol 1996;156:1606–8.
22] Meluch AA, Greco FA, Burris HA, et al. Paclitaxel and gemcitabinechemotherapy for advanced transitional-cell carcinoma of the urothe-lial tract: A phase II trial of the Minnie Pearl Cancer ResearchNetwork. J Clin Oncol 15; 2001;19:3018–24.
23] Bellmunt J, Cos J, Cleries R, et al. Feasibility trial of methotrexate-paclitaxel as a second line therapy in advanced urothelial cancer.Cancer Invest 2003;20:673–85.
24] Orntoft TF, Wolf H. Molecular alterations in bladder cancer. Urol Res1998;26:223–33.
25] Knowles MA. Molecular genetics of bladder cancer. Br J Urol 1995;75:57–66.
26] Vageli D, Kiaris H, Delakas D, et al. Transcriptional activation ofH-ras, K-ras and N-ras proto-oncogenes in human bladder tumors.Cancer Lett 1996;107:241–7.
27] Petit T, Izbicka E, Lawrence RA, et al. Activity of SCH 66336, atricyclic farnesyltransferase inhibitor, against human tumor colony-forming units. Ann Oncol 1999;10:449–53.
28] http://ctep.info.nih.gov/reporting/index.html. Accessed January 6,2004.
29] Therasse P, Arbuck SG, Eisenhauer EA, et al. New guidelines toevaluate the response to treatment in solid tumors. J Natl Cancer Inst2000;92:205–16.
30] Freidlin B, Dancey J, Korn EL, Zee B, et al. Multinomial phase II trialdesigns. J Clin Oncol 2002;20:599.
31] Kaplan EL, Meier P. Nonparametric estimation from incompleteobservations. J Am Stat Assoc 1958;53:457–81.
32] Wang E, Johnson WW. The farnesyl protein transferase inhibitorlonafarnib (SCH66336) is an inhibitor of multidrug resistance pro-teins 1 and 2. Exp Chemother 2003;49:303–8.
33] Nakajima A, Tauchi T, Sumi M, et al. Efficacy of SCH66336, afarnesyl transferase inhibitor, in conjunction with imatinib against
BCR-ABL-positive cells. Mol Cancer Ther 2003;2:219–24.