a nursing conceptual model for contamination
TRANSCRIPT
A Nursing Conceptual Model forContaminationijnt_1195 10..17
Pauline M. Green, PhD, RN, CNE, and Laura V. Polk, PhD, RN
Pauline M. Green, PhD, RN, CNE, is a professor at the College of Nursing and Allied Health, Howard University,Washington, DC; Laura V. Polk, PhD, RN, is a professor at the Health Sciences Division, College of SouthernMaryland, La Plata, Maryland.
Search terms:Biopreparedness, contamination,nursing language, nursing model
Author contact:[email protected], with a copy tothe Editor: [email protected]
PURPOSE: To propose a nursing model of contamination that describesthe key features of contamination at a level of abstraction needed forclinical decision making.DATA SOURCES: Relevant literature on contamination, bioprepared-ness, and classic epidemiologic literature were reviewed and analyzed.DATA SYNTHESIS: A model of contamination was created along with adescription of benefits of use in practice, education, and research.DISCUSSION: The nursing profession is called to respond to contamina-tion incidents on a local, national, and global level. Achieving optimumhealth outcomes while managing contamination incidents is enhanced bynurses’ use of a model that incorporates six elements to identify andname instances of contamination and select suitable outcomes andinterventions.
Introduction
Environmental health concerns related to con-tamination now span international borders and callfor a unified response from the nursing profession.Fears about contamination following earthquakes,nuclear explosions, and bioterrorism have focusedour thoughts in an attempt to understand the natureof the health effects on citizens and the role nursingcan play in response to similar incidents. Contami-nation is defined as exposure to contaminants indoses sufficient to cause adverse health effects(NANDA International, 2008). Nurses are often frontline professionals during acute contamination inci-dents. Similarly, nurses are often the first to seepatients with chronic symptoms indicating house-hold or community contamination. A nursing modelof contamination would provide cognitive support toimprove our understanding and thinking about thecentral phenomena and processes involved in con-tamination. In addition, such a model would providesupport for nurses in analyzing, thinking, anddeciding in the midst of complex and chaotic situa-tions. In less acute situations, a nursing model
would provide a framework for identifying risks forcontamination, preventing contamination, and pro-moting health. Rather than viewing each contamina-tion incident as wholly unique, a nursing modelwould provide nurses with a global view of contami-nation with its critical features during episodesof increased risk, actual contamination, andrehabilitation.
The authors propose a model that contains sixelements: clinical judgment, antecedents of contami-nation, focus of care, time of care, consequences ofcontamination, and health outcomes (Figure 1). Themodel provides a comprehensive view of contamina-tion with the key elements needed for integratingnursing knowledge and skills essential for preventing,identifying, and responding to contamination inci-dents. Achieving optimum health outcomes whilemanaging the complexity of contamination incidentsis enhanced by health professionals’ use of standard-ized language to identify and name instances of con-tamination and select appropriate outcomes andinterventions. The model of contamination will serveas a basis for investigating physiological, psychologi-cal, and social processes of concern, for decision
10 © 2011, The AuthorsInternational Journal of Nursing Knowledge © 2011, NANDA International
International Journal of Nursing Knowledge Volume 23, No. 1, February 2012
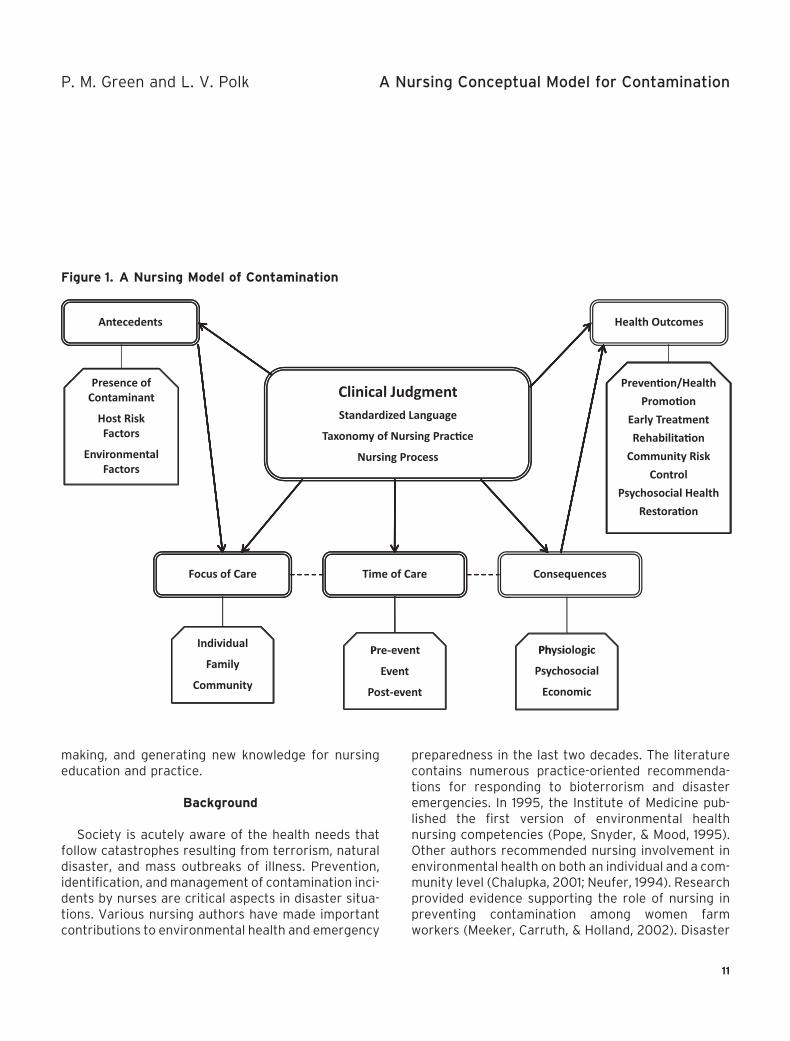
making, and generating new knowledge for nursingeducation and practice.
Background
Society is acutely aware of the health needs thatfollow catastrophes resulting from terrorism, naturaldisaster, and mass outbreaks of illness. Prevention,identification, and management of contamination inci-dents by nurses are critical aspects in disaster situa-tions. Various nursing authors have made importantcontributions to environmental health and emergency
preparedness in the last two decades. The literaturecontains numerous practice-oriented recommenda-tions for responding to bioterrorism and disasteremergencies. In 1995, the Institute of Medicine pub-lished the first version of environmental healthnursing competencies (Pope, Snyder, & Mood, 1995).Other authors recommended nursing involvement inenvironmental health on both an individual and a com-munity level (Chalupka, 2001; Neufer, 1994). Researchprovided evidence supporting the role of nursing inpreventing contamination among women farmworkers (Meeker, Carruth, & Holland, 2002). Disaster
Figure 1. A Nursing Model of Contamination
Health OutcomesAntecedents
Clinical JudgmentSt d di d LStandardized Language
Taxonomy of Nursing Prac�ce
Nursing Process
Presence ofContaminant
Host RiskFactors
EnvironmentalFactors
Focus of Care Time of Care
Preven�on/HealthPromo�on
Early TreatmentRehabilita�on
Community RiskControl
Psychosocial HealthRestora�on
Consequences
PPre-event
Event
Post-event
Individual
Family
Community
Ph i l iPhysio ogic
Psychosocial
Economic
P. M. Green and L. V. Polk A Nursing Conceptual Model for Contamination
11

competencies were developed for all professionalnurses in practice settings (National Emergency Pre-paredness Education Coalition, 2003; Stanley, 2005,Weiner, 2006). In the post-9/11 period, Gebbie andQureshi (2006) advocated for interdisciplinaryresponse skills of healthcare workers in incidents ofmass casualty and environmental disasters. Veenema(2002, 2007) proposed expanding nursing educationcurricula to include bio-preparedness for instancesinvolving chemical, biological, and radiological terror-ism but did so without a conceptual model to structurethe educational process. A position statement by theInternational Council of Nurses (ICN) (2006) called fordisaster preparedness including risk assessment andmultidisciplinary management strategies at systemlevels. While nurses are recognized as essential per-sonnel in treating individuals, communities, and popu-lations following disasters and bioterrorism, studieshave shown that nurses are not prepared to dealreadily with incidents of contamination (De Felice,Guiliani, Alfonsi, Mosca, & Fabiani, 2008; Labeau,Vandijk, Claes, Van Aken, & Blot, 2007). Recently, theICN offered an international perspective on nursinginterventions appropriate for victims of bioterrorism(ICN, 2009b). Still, the dialogue in the nursing litera-ture remains prescriptive in nature without a soundtheoretical foundation.
A few authors provided a theoretical basis forreducing environmental health risks. Kleffel (1991)urged a shift from the traditional nursing paradigmthat viewed the environment as centered on the clientand focused on immediate surroundings to a newnursing paradigm of environment that encompassedsocial, political, economic, and cultural conditionsinfluencing health. Butterfield (2002) urged nursesto “think upstream” when examining environmentalhealth problems and environmental health knowledgeand choices of populations. This approach empha-sized a comprehensive view of environment that rec-ognized the social context of environmental healthrisks and problems of populations, as well as individu-als. Dixon and Dixon (2002) proposed an integrative
model for environmental health research to under-stand the environmental health of individuals andcommunities by examining four domains of centralconcern: physiological, vulnerability, epistemological,and health protection. The authors promoted theresearch model as a means of linking symptoms andenvironmental exposures with personal and commu-nity environmental health information and decisionmaking. Jennings-Sanders (2004) described amodel for managing community disasters usingfour phases—pre-disaster, disaster, post-disaster, andclient/population outcomes. A concept analysis ofcontamination clarified the concept and suggested aneed for widespread agreement on its definition,antecedents, and consequences to accurately recog-nize and effectively manage instances of contamina-tion (Green & Polk, 2009).
Development of a nursing model of contaminationwould advance and support nursing theory of envi-ronmental health. The model described in this articleprovides an approach to nursing in the event ofhuman and environmental contamination that usesnursing process and standardized language toachieve health outcomes including prevention of con-tamination, management of contamination incidents,and restoration of health.
Elements and Processes of the Model
Clinical Judgment
The ability to identify and name instances of con-tamination, plan care and select suitable outcomes,implement nursing and collaborative activities, andevaluate goal attainment is optimized through thestructure of a nursing model that incorporates clinicaljudgment as a basis for standardized nursing lan-guage, the Taxonomy of Nursing Practice, and thenursing process as key elements. With its four centraldomains, the Taxonomy of Nursing Practice providesa framework for holistic nursing care. Nurses areencouraged to consider the functional, physiologic,
A Nursing Conceptual Model for Contamination P. M. Green and L. V. Polk
12

psychosocial and environmental factors influencing asituation. Under the umbrella of the InternationalClassification of Nursing Practice, standardized lan-guage provides consistent labeling of nursing phe-nomena addressed by the domains (ICN, 2010).Throughout each phase of the model, nurses have anopportunity to consider the Taxonomy of NursingPractice, apply the nursing process, and usestandardized language to address contaminationconcerns. As a result, the proposed model ofcontamination can guide nurses through the clinicaljudgments needed to prevent contamination, managecontamination incidents, and restore health.
The proposed model encourages a nurse to con-sider each element of the model as an opportunity forcare. Antecedents, focus of care, time of care, conse-quences, and health outcomes can each be addressedthrough the analysis of Taxonomy of Nursing Practicedomains, application of the nursing process, and useof standardized language. Through the assessmentphase of the nursing process, focus is on identifica-tion of defining characteristics or risk factors. Analy-sis of the causative agent along with relatedenvironmental, situational, pathophysiologic, andtreatment-related factors provides key data for diag-nosis and planning. A diagnosis of Risk for Contami-nation or Contamination and an initial determinationof Nursing Outcomes Classification (NOC) ratingsdirect a nurse toward pre-event, event, or post-eventmanagement. Nursing Interventions Classification(NIC) activities are employed that address the focusof care, time of care, and consequences of contami-nation. Evaluation involves a reappraisal of the NOCrating scales to establish whether primary, second-ary, or tertiary prevention interventions have beeneffective in achieving optimal health outcomes.
Antecedents
“Antecedents are those events or incidents thatmust occur or be in place prior to the occurrence ofthe concept” (Walker & Avant, 2011, p. 167). Anteced-
ents of contamination include the presence of a con-taminant, its dose and duration of exposure alongwith characteristics of individuals and the communitythat increase risk for exposure and subsequent con-tamination. The variables of age, maturation, nutri-tion, socioeconomic status, behavior, and physicaland social environment serve as a context for a hostof risk factors for contamination. When using themodel, the physical environment would be assessedfor sanitation, pollution, housing, and transportation.The social environment would be assessed for socialsupport in the form of resources, networks, migra-tion, and presence of distinct population groups.Destabilizing forces such as wars, economic recessionor depression, and natural disasters that adverselyaffect physical, social, and economic health and lif-estyles would also be analyzed (ICN, 2009a; WorldHealth Association, 2001). As nurses employ the pro-posed model, they are encouraged to consider theenvironmental, situational, pathophysiologic, andtreatment-related factors that may be reduced oreliminated through application of the nursing processand a focus on primary prevention.
Focus of Care
The term Focus of Care describes the recipient ofnursing care who may be an individual, family, com-munity, or a larger population. Individuals and fami-lies would be assessed using a health and exposurehistory and physical examination. Environmentalhealth beliefs and knowledge of those who are thefocus of care are important considerations for assess-ment (Dixon & Dixon, 2002). Other features to beassessed include ethnicity, language, and literacy. Fora community or population focus, vital statisticsfrom national and regional health departments wouldbe assessed to determine morbidity and mortality,occupational diseases, and other indicators of envi-ronmental health issues. Nursing care focused at theindividual level may be expanded to encompass thefamily, and/or the broader community or geographic
P. M. Green and L. V. Polk A Nursing Conceptual Model for Contamination
13

region. It is essential that the nurse considers thefocus of care within the context of the Taxonomy ofNursing Practice and the nursing process so thatpotential community, social, or global patterns arenot overlooked, and nursing care can be moreinclusive.
Time of Care
The next major element to be considered in theproposed model of contamination is time of care. Thetime line for contamination instances consists ofthe time prior to the event (pre-event), during theevent (event), and after the event (post-event).Nursing process priorities shift depending on the timeof care and individual, family, and community assess-ment of contamination factors provide key informa-tion for planning and implementing care (Green &Polk, 2011; Polk & Green, 2010). Patterns of signs andsymptoms of disease and their geographic distribu-tion and concentration provide data for making judg-ments about the nature and probable effects of thecontamination incident. Interventions are situationspecific and consider the agent of contamination andthe environment in which it occurs. Interventionswould be selected according to the levels of preven-tion required. Primary, secondary, and tertiary levelsof prevention correspond to pre-event, event, andpost-event time periods used in the model.
Primary prevention involves protection of theperson, community, or population from a contaminat-ing agent before an incident occurs. Examples ofprimary prevention methods include environmentalrisk analysis, use of personal protective equipment,and removal of individuals from the site of contami-nation. Primary prevention also incorporates educa-tion of individuals and the community on protectionfrom hazardous substances, contaminant pathways,and signs and symptoms of contamination. Secondaryprevention involves interventions to detect andprovide early treatment for an actual contaminationevent. Early treatment of contamination requires
identification of the agent involved and may includeadministration of an antidote and supportive mea-sures. If needed, a decontamination procedure maybe employed, followed by triage, treatment with spe-cific drugs, and cardio-respiratory and psychologicalsupport. Tertiary prevention of contamination isaimed at those who have experienced contaminationand involves identifying referral and support servicesfor physical and psychological rehabilitation to mini-mize adverse effects of contamination and promotereturn to previous activities.
Consequences
Consequences in the model are the adverse effectsproduced by contaminants. The consequences of con-tamination include the physical, chemical, psychologi-cal, economic, and social effects on individuals andcommunities. Physical effects are caused by contami-nants entering the human system by routes of inges-tion, inhalation, and dermal contact (Agency for ToxicSubstances and Disease Registry [ATSDR], 2008).Systems commonly affected by contaminants arecardiovascular, hematologic, respiratory, centralnervous, renal, hepatic, integumentary, and repro-ductive systems (ATSDR, 2008).
Contamination events increase the likelihood ofharmful organ and cellular processes from chemical,biological, or radiological agents. Inflammatory pro-cesses result in damage to vessel epithelium andcardiovascular disease (Kang, 2008). Chemical injuryto endocrine glands causes toxic effects with endo-crine disruption in normal adrenal, thyroid, pancreas,pituitary, and parathyroid gland functions (Capen,2008). Oxidative stress from oxygen free radicals canproduce cellular damage resulting in genetic damageand carcinogenesis (Klaunig & Kamendulis, 2008).Exposure to harmful substances that cause harm tothe human system may occur suddenly causing anacute episode. Long-term, low level environmentalexposures can also cause symptoms that differ fromthose resulting from acute exposure.
A Nursing Conceptual Model for Contamination P. M. Green and L. V. Polk
14

The model also addresses the psychological, social,and economic effects and their impact on health out-comes. Individuals, families, and communitiesaffected by contamination incidents can respond withanxiety, fear, spiritual distress, and feelings of vulner-ability and powerlessness (Boscarino, Adams, Figley,Galea, & Foa, 2006). The social consequences can beisolation from friends, family, and communitymembers, as well as the loss of a sense of unifiedcommunity. As a result of contamination incidents orthe threat of contamination, individuals may experi-ence job loss and financial hardship, and communitiesmay experience regional economic effects. Each ofthese factors can impact health outcomes at the indi-vidual and population level.
Health Outcomes
Health outcomes describe the positive results ofefforts using the elements of the model to operation-alize nursing process. Health outcomes in the modelinclude prevention of acute exposure, early detec-tion of signs and symptoms of contamination, earlytreatment of acute exposure, decrease in incidenceof environmentally associated diseases such asasthma and lung cancer, and rehabilitation of thosewith environmentally associated chronic disease con-ditions. Additional health outcomes include the levelof community risk control, and psychological, social,and economic health restoration. The systematicapproach suggested by this proposed model canenhance clinical judgment related to contaminationand result in effective achievement of optimal healthoutcomes.
Nursing Implications
The proposed nursing model of contamination isholistic in nature as it recognizes the effect of biologi-cal, chemical, and radiological influences on thehealth of individuals and the responses of individuals
and aggregates in a social, spiritual, cultural, eco-nomic, and political context. By framing the nursingconceptual model of contamination in the context ofthe Taxonomy of Nursing Practice, standardized lan-guage, and the nursing process, nurses are encour-aged to approach care from a systematic perspectiveand communicate using a consistent terminology.Embedding the use of nursing language into themodel provides for clarity during each stage of analy-sis and decision making.
Educators may use the model to introduce stu-dents to the major concepts, relationships, decisionpoints, and possible outcomes related to contamina-tion. This foundation of knowledge will promote stu-dents’ ability to implement nursing process withinstances of contamination and manage care moreeffectively. The nursing model described here is alsoappropriate for use by nurses in practice. The gen-eralist can benefit from the clear depiction of anursing view of contamination which allows forgreater insight into the contribution of nursing inproviding care before, during, and after contamina-tion events. The educational preparation ofadvanced practice nurses supports the use ofnursing models in providing care that includes thediagnosis, treatment, and referral of patients oraggregates with acute and chronic symptoms.Advanced practice nurses contribute to disaster pre-paredness planning by collaborating with healthsystems to develop protocols for handling patients’illnesses caused by contamination agents, byaddressing the health needs of specific populations,by analyzing statistical health data, and mobilizingcommunity resources (Mondy, Cardenas, & Avila,2003). Nursing research conducted in the area ofcontamination can also benefit from this model. Anursing model of contamination can provide thestructure to explore conceptual relationships in clini-cal studies and build validation for components ofcontamination care. This new evidenced-basednursing knowledge can then be translated into prac-tice and policy recommendations.
P. M. Green and L. V. Polk A Nursing Conceptual Model for Contamination
15
Conclusion
The nursing profession is making strides to incor-porate disaster preparedness as an essential compe-tency of nurse graduates. Using a nursing model ofcontamination as part of the educational process fornursing students and graduates will build on previousgroundwork and further develop cognitive skillsneeded for clinical decision making in the area ofcontamination. By promoting a holistic approach withthe Taxonomy of Nursing Practice and by incorporat-ing a scientific, biological basis for the health effectsof contaminants on individuals and communities, wecan advance the body of knowledge used for assess-ing and diagnosing contamination. By using a nursingmodel of contamination, planning, implementation,and evaluation may be conducted with knowledge of abroad range of individual and community-risk factors.Standardized language for specifying diagnoses, out-comes, and interventions will aid in incorporatingthe electronic health record for patient care andresearch. A nursing model of contamination based onclinical judgment will aid in further defining theunique contribution of nursing to health care.
References
Agency for Toxic Substances and Disease Registry. (2008). Glos-sary of terms. Retrieved from http://www.atsdr.cdc.gov/glossary.html
Boscarino, J., Adams, R., Figley, C., Galea, S., & Foa, E. (2006). Fearof terrorism and preparedness in New York city 2 years afterthe attacks: Implications for disaster planning and research.Journal of Public Health Management and Practice, 12(6), 505–513.
Butterfield, P. G. (2002). Upstream reflections on environmentalhealth: An abbreviated history and framework for action.Advances in Nursing Science, 25(1), 32–49.
Capen, C. C. (2008). Toxic responses of the endocrine system. In C.D. Klaassen (Ed.), Casarett and Doull’s toxicology. The basicscience of poisons (7th ed., pp. 807–879). New York:McGraw-Hill.
Chalupka, S. M. (2001). Essentials of environmental health. Enhanc-ing your occupational nursing practice. (Part II). AAOHNJournal : Official Journal of the American Association of Occu-pational Health Nurses, 49(4), 194–213.
De Felice, M., Guiliani, A. R., Alfonsi, G., Mosca, G., & Fabiani, L.(2008). Survey of nursing knowledge on bioterrorism. Interna-tional Emergency Nursing, 16, 101–108.
Dixon, J. K., & Dixon, J. P. (2002). An integrative model for envi-ronmental health research. Advances in Nursing Science, 24(3),43–57.
Gebbie, K., & Qureshi, K. (2006). Emergency and disaster prepared-ness: Core competencies for nurses. American Journal ofNursing, 102, 46–51.
Green, P. M., & Polk, L. V. (2009). Contamination: Concept analysisand nursing implications. International Journal of Nursing Ter-minologies and Classifications, 20(4), 189–197.
Green, P. M., & Polk, L. V. (2011). Contamination, risk for contami-nation. In B. J. Ackley & G. B. Ladwig (Eds.), Nursing diagnosishandbook. A guide to planning care (9th ed., pp. 268–273). St.Louis: Mosby.
International Council of Nurses. (2006). Position statement. Nursesand disaster preparedness. Retrieved from http://www.icn.ch/images/stories/documents/publications/position_statements/A11_Nurses_Disaster_Preparedness.pdf
International Council of Nurses. (2009a). Nursing matters: ICN ondisplaced persons: A global challenge. Retrieved from, http://www.icn.ch/images/stories/documents/publications/fact_sheets/5b_FS-Displaced_Persons.pdf
International Council of Nurses. (2009b). Nursing matters: Terror-ism and bioterrorism: Nursing preparedness. Retrieved fromhttp://www.icn.ch/images/stories/documents/publications/fact_sheets/5c_FS-Terrorisme_bioterrorism.pdf
International Council of Nurses. (2010). International Classificationfor Nursing Practice (ICNP). Retrieved from http://www.icn.ch/pillarsprograms/about-icnpr/
Jennings-Sanders, A. (2004). Teaching disaster nursing by utilizingthe Jennings disaster nursing management model. Nurse Edu-cation in Practice, 4, 69–76.
Kang, Y. J. (2008). Toxic responses of the heart and vascularsystem. In C. D. Klaassen (Ed.), Casarett and Doull’s toxicology.The basic science of poisons (7th ed., pp. 699–739). New York:McGraw-Hill.
Klaunig, J. E., & Kamendulis, L. M. (2008). Chemical carcinogenesis.In C. D. Klaassen (Ed.), Casarett and Doull’s toxicology. The basicscience of poisons (7th ed., pp. 329–379). New York: McGraw-Hill.
Kleffel, D. (1991). Rethinking the environment as a domain ofnursing knowledge. Advances in Nursing Science, 14(1), 40–51.
Labeau, S., Vandijk, D. M., Claes, B., Van Aken, P., & Blot, S. I. (2007).Critical care nurses’ knowledge of evidence-based guidelinesfor preventing ventilator—Associated pneumonia: An evaluationquestionnaire. American Journal of Critical Care, 16(4), 371–377.
Meeker, B. J., Carruth, A., & Holland, C. B. (2002). Health hazardsand preventive measures of farm women. AAOHN Journal :Official Journal of the American Association of OccupationalHealth Nurses, 50(7), 307–314.
Mondy, C., Cardenas, D., & Avila, M. (2003). The role of an advancedpractice public health nurse in bioterrorism preparedness.Public Health Nursing, 20(6), 422–431.
A Nursing Conceptual Model for Contamination P. M. Green and L. V. Polk
16

NANDA International. (2008). Nursing diagnoses. Definitions andclassification 2009–2011. (p. 334). Philadelphia: Author.
National Emergency Preparedness Education Coalition. (2003).Educational competencies for registered nurses Responding tomass casualty incidents. Retrieved from http://www.nursing.vanderbilt.edu/incmce/competencies.html
Neufer, L. (1994). The role of the community health nurse in envi-ronmental health. Public Health Nursing, 11(3), 155–162.
Polk, L. V., & Green, P. M. (2010). Contamination. In L. J. Carpenito-Moyet (Ed.), Nursing diagnosis. Application to clinical practice(13th ed., pp. 191–198). Philadelphia: Lippincott Williams &Wilkins.
Pope, A. M., Snyder, M., & Mood, L. H. (1995). Nursing, health, andthe environment. Strengthening the relationship to improve thepublic’s health. Washington, DC: National Academies Press.
Stanley, J. (2005). Disaster competency development: An integra-tion in nursing education. Nursing Clinics of North America, 40,453–467.
Veenema, T. G. (2002). Chemical and biological terrorism. Currentupdates for nurse educators. Nursing Education Perspectives,23(2), 62–71.
Veenema, T. G. (2007). Disaster nursing and emergency prepared-ness for chemical, biological, and radiological terrorism andother hazards (2nd ed.). New York: Springer.
Walker, L. O., & Avant, K. C. (2011). Strategies for theory construc-tion in nursing (5th ed.). Upper Saddle River, NJ: Prentice Hall.
Weiner, E. (2006). Preparing nurses internationally for emergencyplanning and response. Online Journal of Issues in Nursing, 11(3),manuscript 3. doi:10.3912/OJIN.Vol11No03Man03
World Health Association. (2001). Community health needs assess-ment. Retrieved from http://www.euro.who.int/_data/assets/pdf_file/0018/102249/E73494.pdf
P. M. Green and L. V. Polk A Nursing Conceptual Model for Contamination
17