a report from nimh - dbsanca - report from nimh depression •affects 6.7% of adult population...
TRANSCRIPT
Mayada Akil, M.D.Mayada Akil, M.D.Senior Advisor to the DirectorSenior Advisor to the Director
National Institute of Mental HealthNational Institute of Mental Health
Advances in Depression Research:Advances in Depression Research: A Report From NIMH

Depression
• Affects 6.7% of adult population
• Women affected twice as much as men
• Leading cause of disability from all medicalillnesses

Causes of Disability by Illness CategoryUnited States and Canada
15-44 years old
0 5 10 15 20 25 30 35 40
Mental Illness*
Alcohol and drug use
Injuries, including self-inflicted
Respiratory disease
Musculoskeletal disease
Sense organ disease
Cardiovascular disease
Migraine
Infectious disease, excluding HIV
WHO World Health Report 2002

0% 5% 10% 15% 20% 25% 30%
Unipolar depressionAlcohol use
Drug use
Bipolar disorderSchizophrenia
Diabetes
Asthma
Hearing loss
Endocrine disorders
Migraine
Top Causes of DisabilityUnited States and Canada
15-44 years old
WHO, World Health Report 2002
Percent Disability Caused by Noncommunicable Diseases

• Total Costs of “Mental Health Care”
• $71 Billion direct for treatment
• $79 Billion indirect (social services)• Both direct and indirect costs are public sector
– Medicaid is the largest single payer of mental health.
– More than 50% of all mental health expenditures are paidfor by the public sector (Medicaid, Medicare, state and localgovernment)
– Individuals with serious mental illnesses represent thesingle largest diagnostic group (35%) on the SSI rolls.
From the President’s New Freedom Commission on Mental Health, 2003
The Economic Costs of Mental Disorders

The Human Cost
NIMH is one of 27 Institutes and Centers atNIMH is one of 27 Institutes and Centers atthe National Institutes of Health (NIH).the National Institutes of Health (NIH).
NIH, is the primary Federal agency forNIH, is the primary Federal agency forconducting and supporting biomedicalconducting and supporting biomedicalresearch and has a public health mission.research and has a public health mission.
What is the NIMH?What is the NIMH?

Reduce the burden of mentalReduce the burden of mentalillness and behavioralillness and behavioral
disorders throughdisorders through
researchresearch on mind, brain on mind, brainand behaviorand behavior
NIMH MissionNIMH Mission
Goals of the NIMH ResearchAgenda for Depression
1. Understanding the biology
2. Prevention
3. Treatment

Discovery to Recovery
Bench Bedside Practice
Discovery to Recovery:Translation is the Key
Bench Bedside
PathophysiologyDiagnostic tests
BiomarkersNew treatments
Practice
Practical trialsServices research
Decade of Discovery: 2000 - 2010
Identifying the players
Revealing basic principles
Translating Discovery into Recovery
Genes Cells Systems Individual Social
Basic Science Opportunities
• Genetics
• Neuroimaging
• Neuroscience
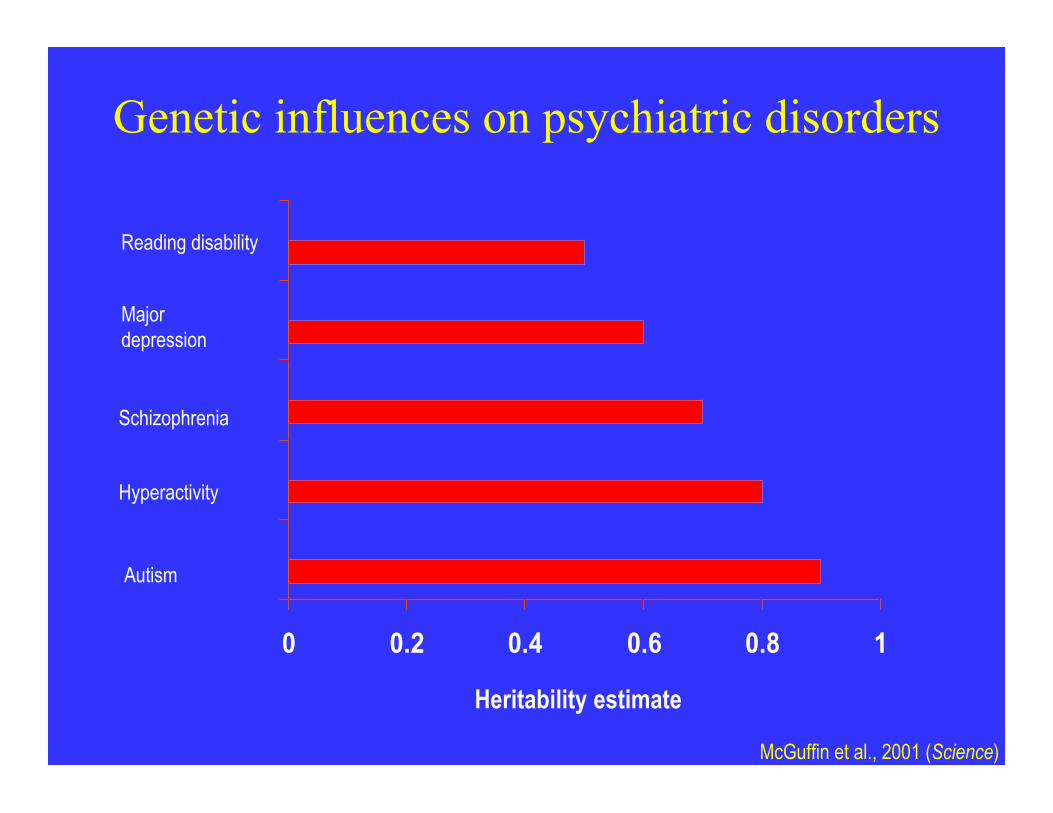
Genetic influences on psychiatric disorders
0 0.2 0.4 0.6 0.8 1
Reading disability
Schizophrenia
Majordepression
Autism
Hyperactivity
Heritability estimate
McGuffin et al., 2001 (Science)
Many Genes Contribute toVulnerability to Depression

Single gene with large effectSingle gene with large effect

Multiple genes with small effectsMultiple genes with small effects
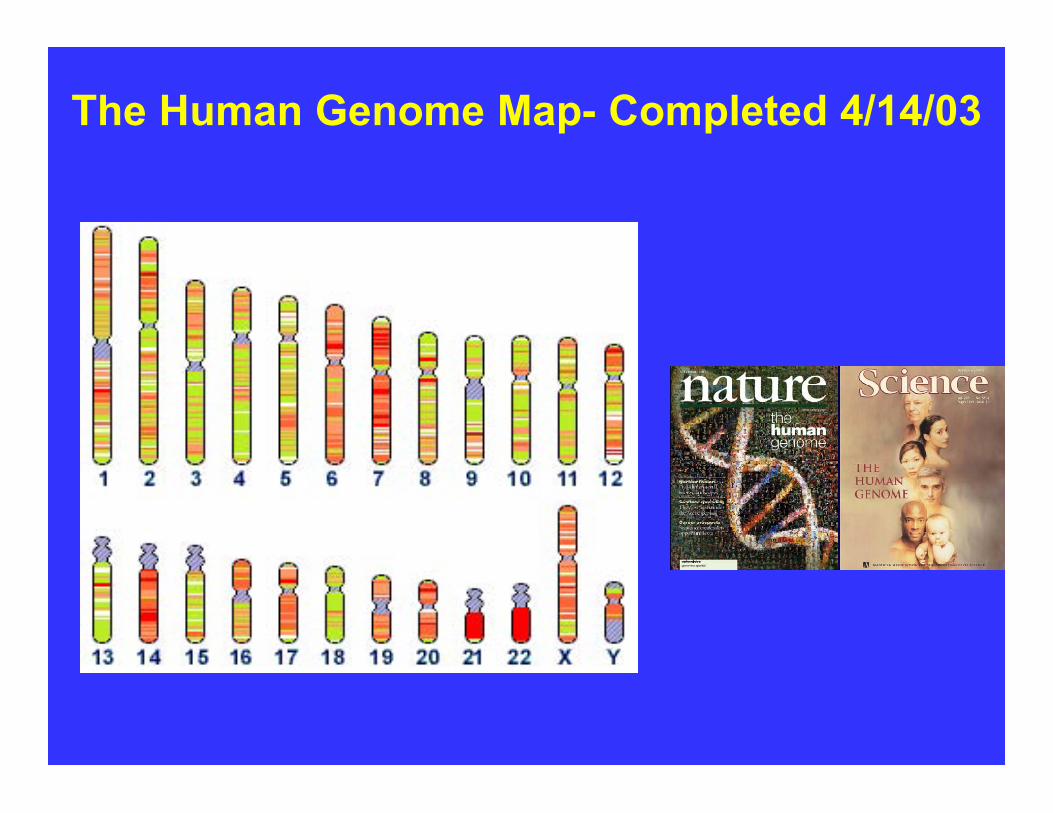
The Human Genome Map- Completed 4/14/03
The Human Genome Map - Completed 4/14/03
Genes: approx 23,000
Genes with known function: less than 5%
Total: 3 billion basesacross 46 chromosomes
Variation : appr 1 SNP every 1000 bases
Variation is the key to understandingvulnerability to disease

www.hapmap.org
3,000,000 points of variationPredicted by 300,000 SNPs!!!
HapMap gives whole genome studies of variation >10 fold advantage.
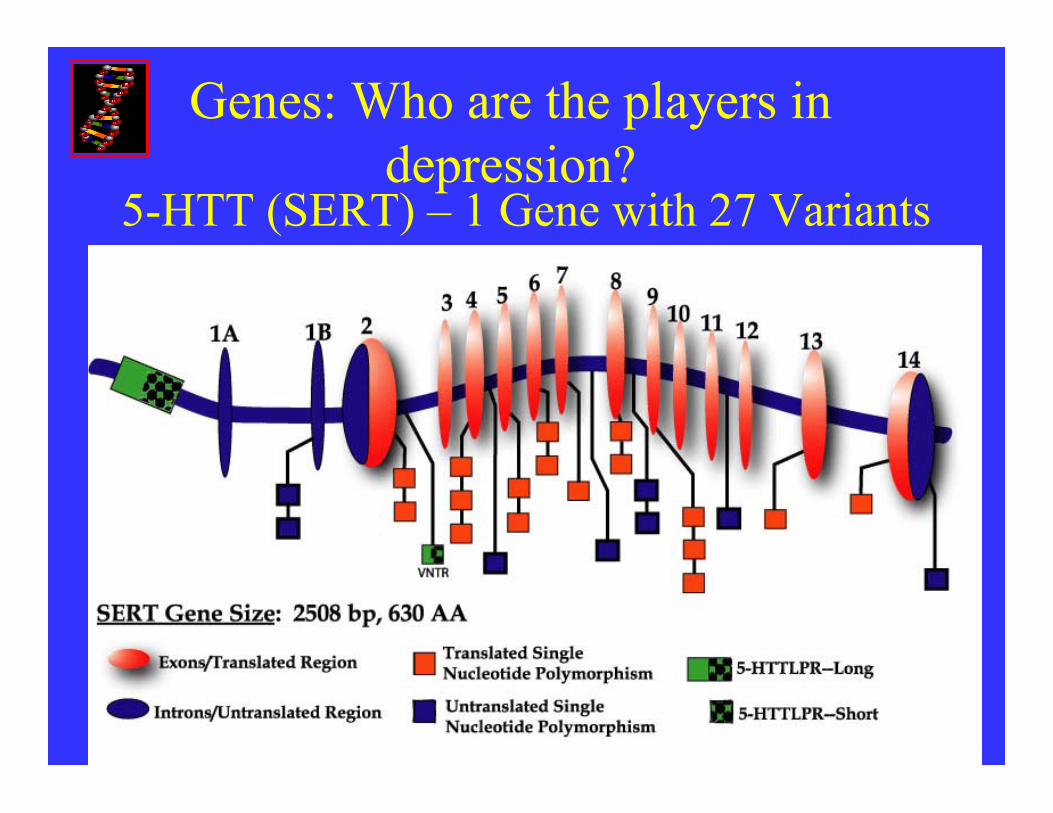
5-HTT (SERT) – 1 Gene with 27 Variants
Genes: Who are the players indepression?

Decade of Discovery: 2000 - 2010
Identifying the players
Revealing basic principles
Changing the culture of science
Genes Cells Systems Individual Social

Advances in Neuroimaging
2001 2006 Benefit
Spatial Res. 1x1x3mm3 X 4 Seizure fociLesions in ADNerve fiber changes
Temporal Res. X 10 Angiogram
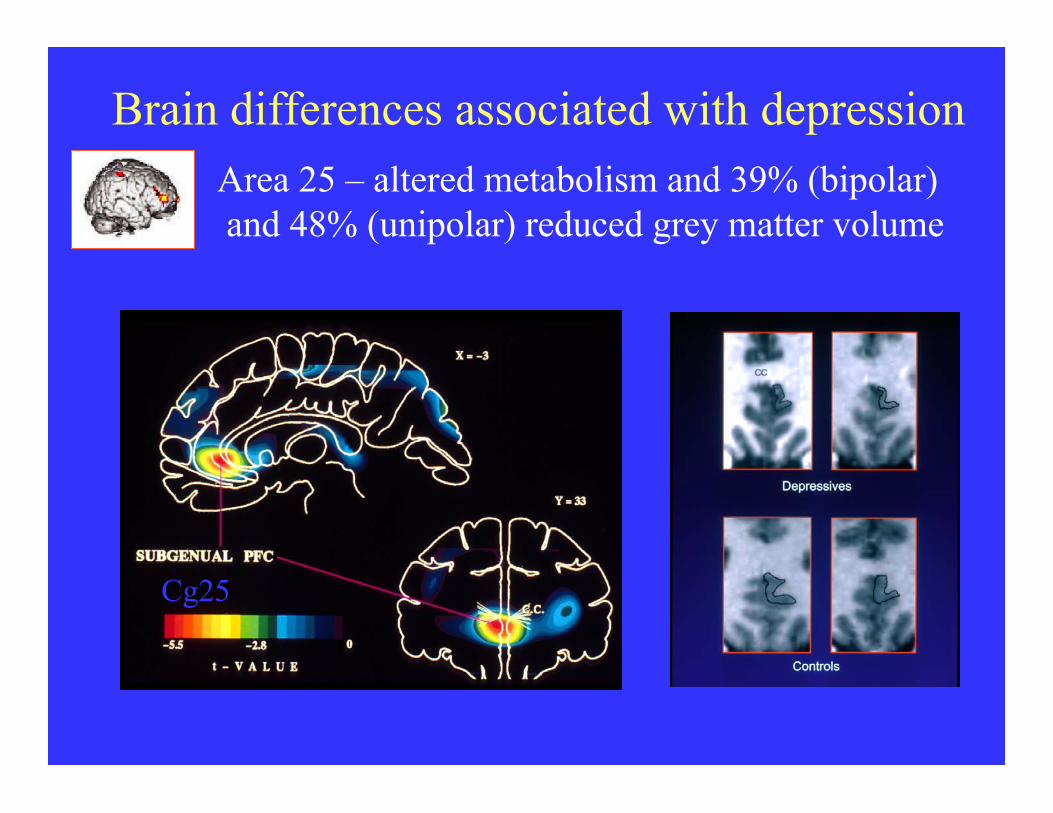
Brain differences associated with depression
Cg25
Area 25 – altered metabolism and 39% (bipolar) and 48% (unipolar) reduced grey matter volume
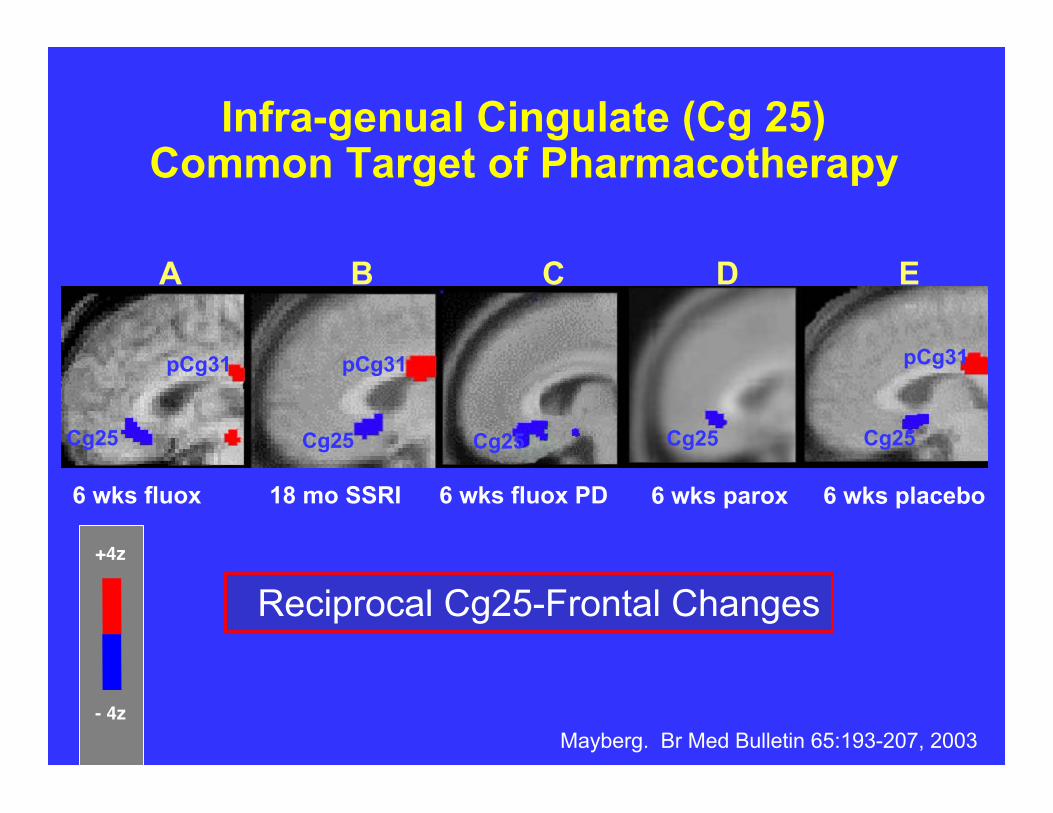
6 wks fluox
Cg25
18 mo SSRI
pCg31
Cg25
6 wks fluox PD
pCg31
Cg25
p
A B C D E
Cg25
6 wks parox
Infra-genual Cingulate (Cg 25) Common Target of Pharmacotherapy
Mayberg. Br Med Bulletin 65:193-207, 2003
Reciprocal Cg25-Frontal Changes
pCg31
Cg25
6 wks placebo
+4z
- 4z
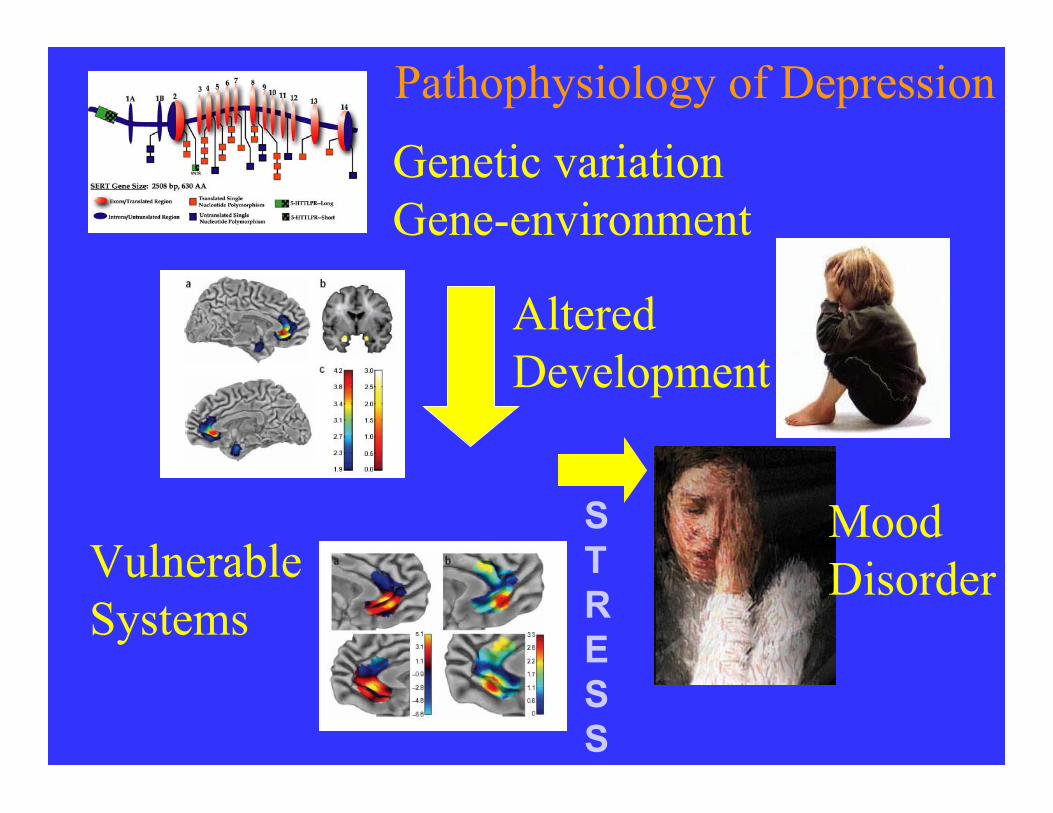
Genetic variationGene-environment
AlteredDevelopment
Pathophysiology of Depression
Vulnerable Systems
MoodDisorder
STRESS

Optimizing Existing TreatmentsThrough Practical Clinical Trials
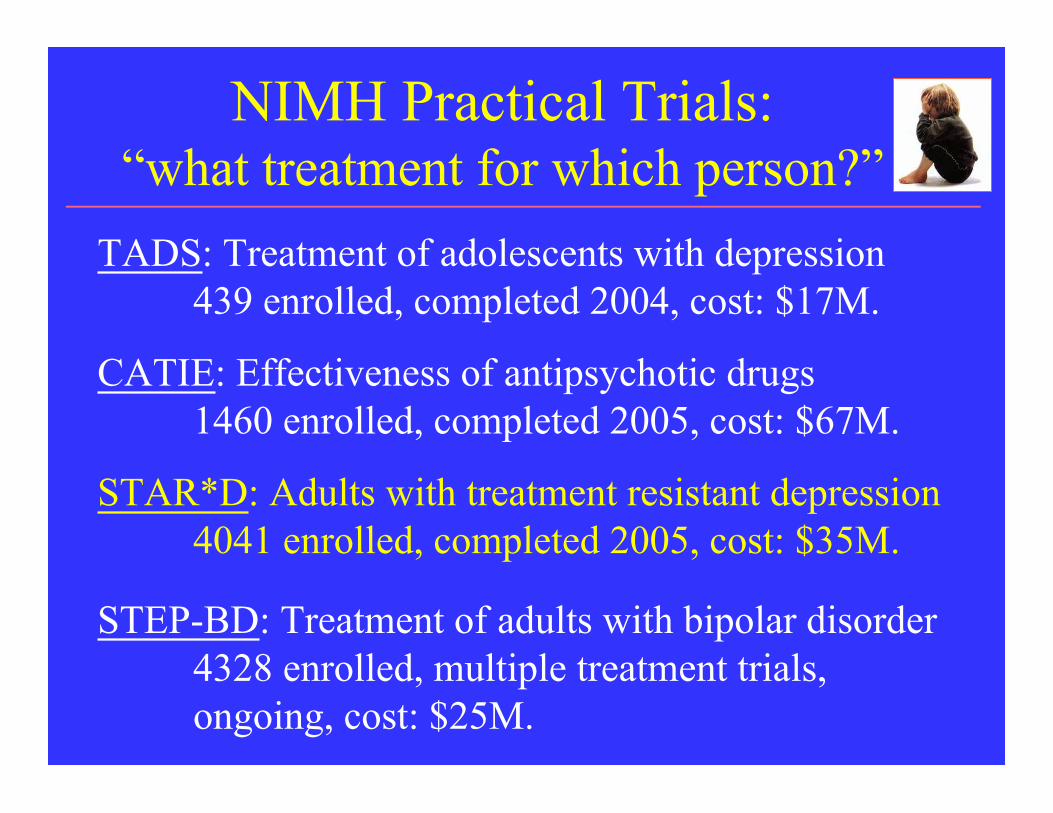
NIMH Practical Trials:“what treatment for which person?”
STEP-BD: Treatment of adults with bipolar disorder4328 enrolled, multiple treatment trials, ongoing, cost: $25M.
CATIE: Effectiveness of antipsychotic drugs1460 enrolled, completed 2005, cost: $67M.
STAR*D: Adults with treatment resistant depression4041 enrolled, completed 2005, cost: $35M.
TADS: Treatment of adolescents with depression439 enrolled, completed 2004, cost: $17M.

STAR D
Rush AJ, et al. Biol Psychiatry. 2003;54(5):573-583.

The Sequenced Treatment Alternativesto Relieve Depression Trial (STAR*D):
4,041 enrolled• Is the patient’s depression resistant to treatment with
an SSRI?
• Would switching medications or augmenting theinitial drug be more likely to achieve a remission?
• How do the side effects of the various medicationscompare?
• How effective is psychotherapy compared withmedication for treatment-resistant depression?
• What is the cost-effectiveness of the varioustreatments?

*Defined as nonremission
Obtain Consent
Level 2
Follow-upSatisfactoryResponse
Unsatisfactory Response*
CIT
Level 1

Randomize to OptionsAcross allAcceptableStrategies
SER BUP VEN CT CIT +BUP
CIT +BUS
CIT +CT
SwitchOptions
AugmentationOptions
STAR D: Defining Evidence For Protocols (Level 2)
33
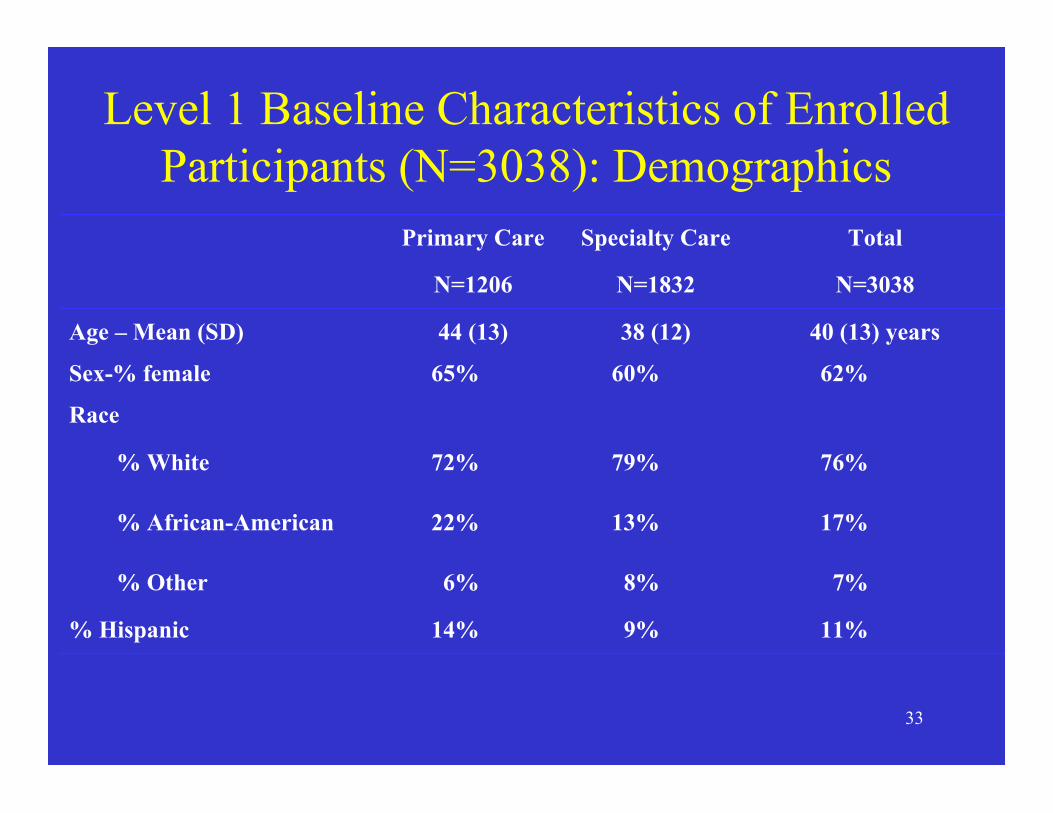
Level 1 Baseline Characteristics of EnrolledParticipants (N=3038): Demographics
N=3038N=1832N=1206
11%9%14%% Hispanic
7%8%6%% Other
17%13%22%% African-American
76%79%72%% White
Race
62%60%65%Sex-% female
40 (13) years38 (12)44 (13)Age – Mean (SD)
TotalSpecialty CarePrimary Care
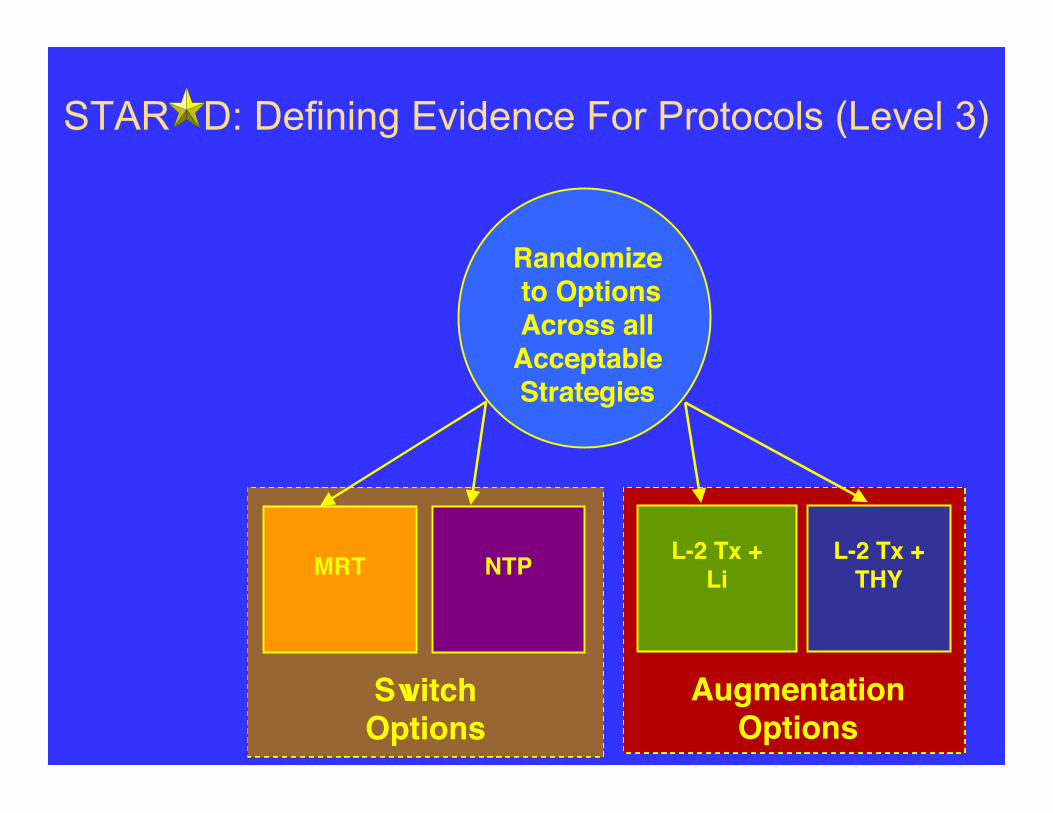
STAR D: Defining Evidence For Protocols (Level 3)
Randomize to OptionsAcross allAcceptableStrategies
MRT NTP L-2 Tx +Li
L-2 Tx +THY
AugmentationOptions
SwitchOptions
TreatmentOptions
Strategies

STAR D: Defining Evidence For Protocols (Level 4)
Randomize
TCP VEN + MRTTreatmentOptions
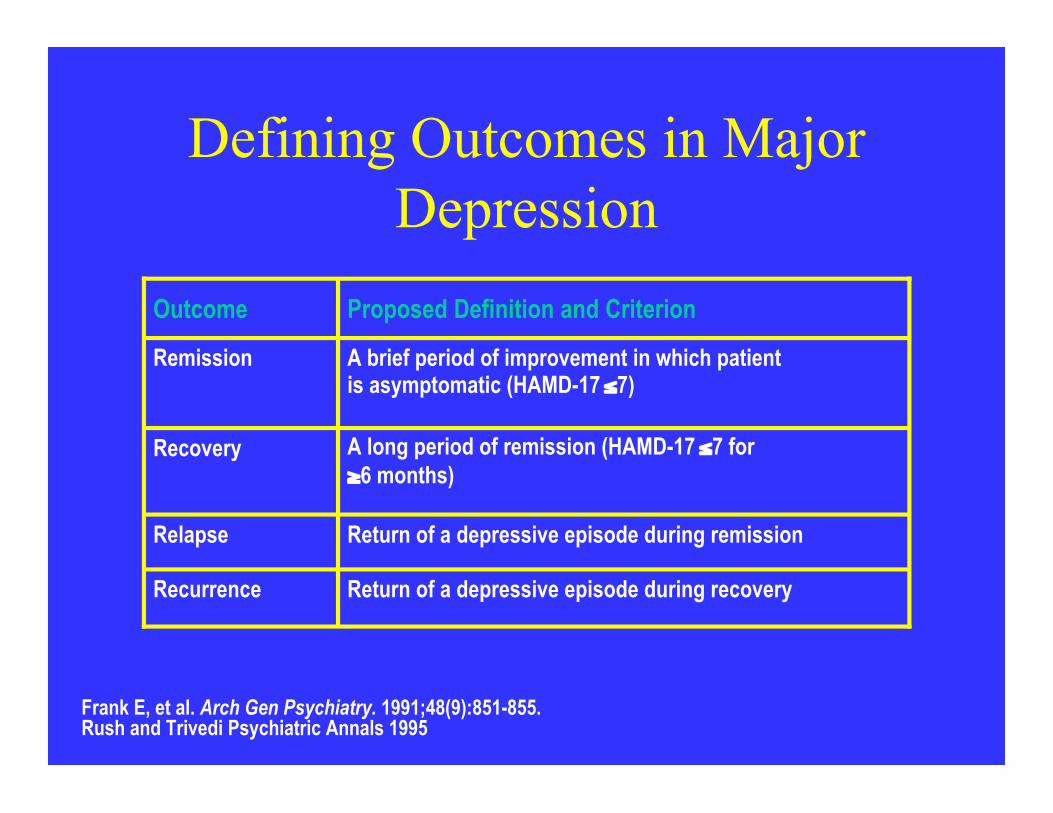
Defining Outcomes in MajorDepression
Return of a depressive episode during recoveryRecurrence
Return of a depressive episode during remissionRelapse
A long period of remission (HAMD-17 ≤7 for≥6 months)
Recovery
A brief period of improvement in which patientis asymptomatic (HAMD-17 ≤7)
Remission
Proposed Definition and CriterionOutcome
Frank E, et al. Arch Gen Psychiatry. 1991;48(9):851-855.Rush and Trivedi Psychiatric Annals 1995
STAR D: Preliminary Results
• Roughly 30% of patients inremission after 12 weeks on CIT
• Switching to Bupropion SR(n=239), Sertraline (n=238) orVenlafaxine ER (n=250) achievedremission in 25% of non responders

STAR D: Preliminary Results
• Augmentation with Buproprion SR(n=565) or Buspar (n=286) lead toremission in about 30% of nonresponders.


Relation Between Maternal Remission Status andChange in Child’s Specific Diagnoses
Source: Weissman et al. JAMA March 22/29, 2006

STAR D: Preliminary Results
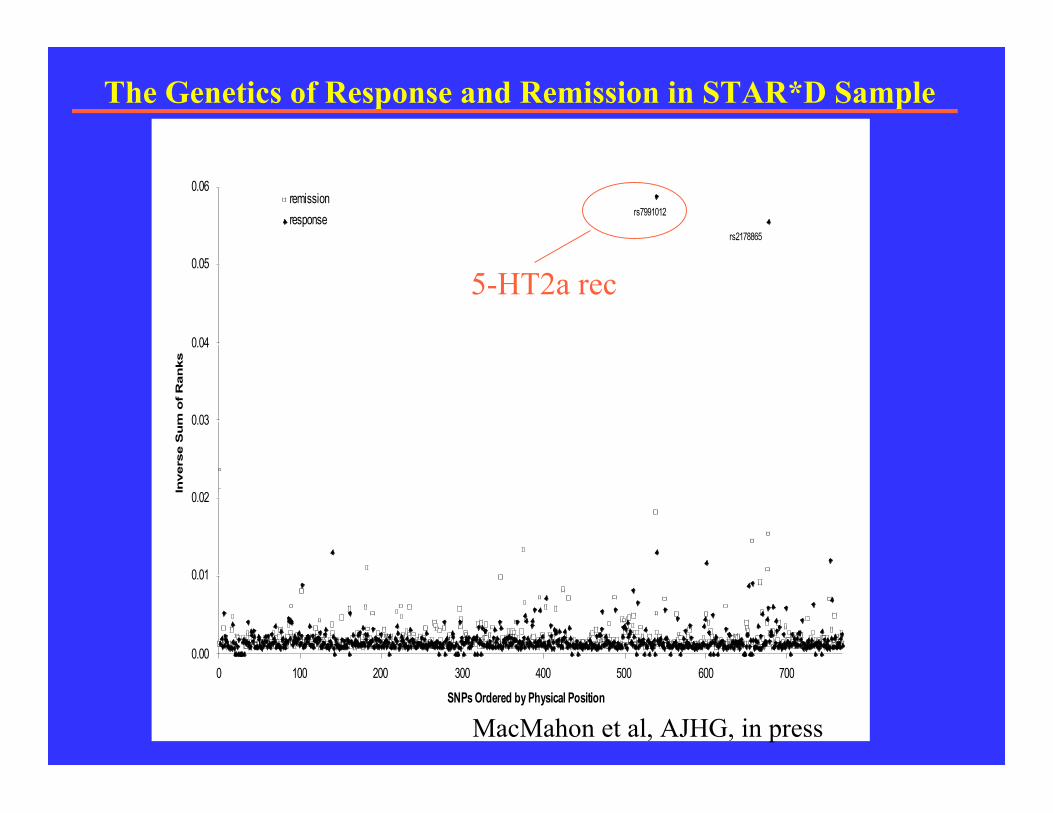
•Having two copies of one version ofa gene that codes for the serotonin2A receptor increased the odds of agood response to antidepressanttreatment by 18%.
0.00
0.01
0.02
0.03
0.04
0.05
0.06
0 100 200 300 400 500 600 700
SNPs Ordered by Physical Position
Invers
e S
um
of
Ran
ks
remission
responsers7991012
rs2178865
The Genetics of Response and Remission in STAR*D Sample
MacMahon et al, AJHG, in press
5-HT2a rec

Questions we have Answers to so far
• Is the patient’s depression resistant to treatment with anSSRI?
• Yes in 70% of the cases
• Would switching medications be more likely to achieve aremission?
• Yes in 25% of the cases• Would augmenting the initial medication with another one be
more likely to achieve a remission?• Yes in ~30% of the cases• Does remission in a mother improve have a positive effect on
her child’s mental health?• Yes.• Can we identify genes involved in treatment response?• Yes.

Treatment
Efficacy/Tolerability of the treatment
Patient Adherence to the treatment
Are Essential for Sustained Recovery
www.nimh.nih.govwww.nimh.nih.gov
Research = Hope
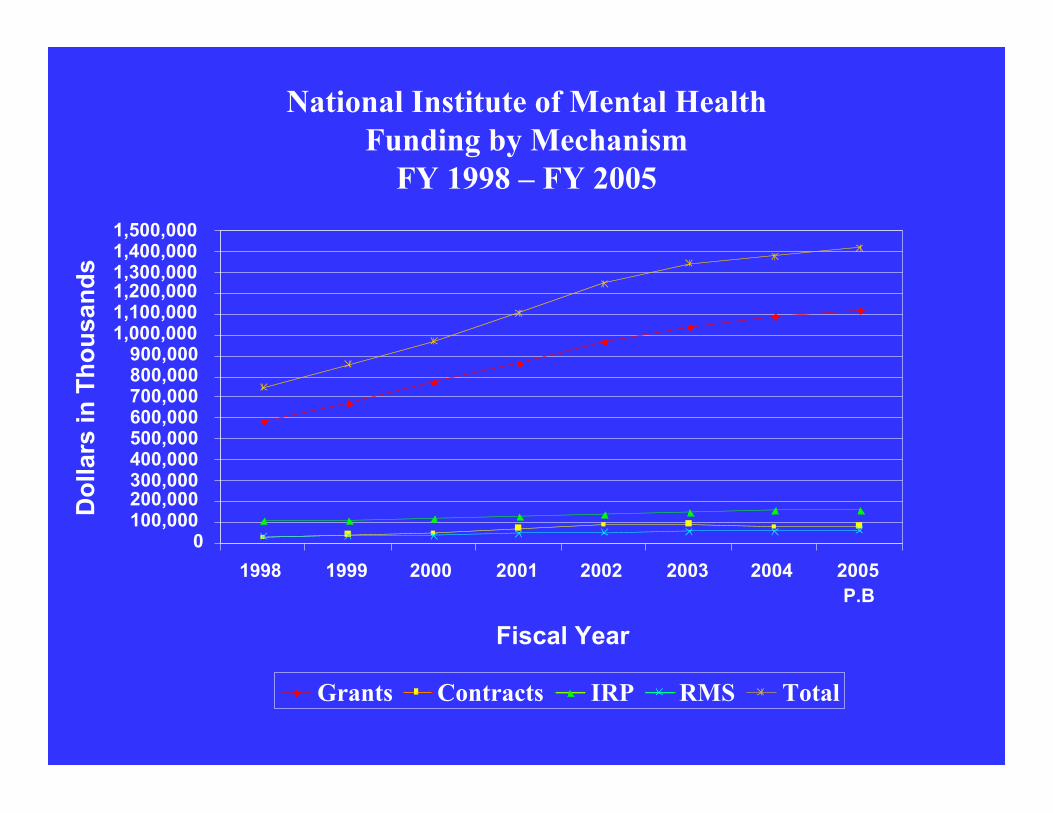
National Institute of Mental HealthFunding by Mechanism
FY 1998 – FY 2005
0100,000200,000300,000400,000500,000600,000700,000800,000900,000
1,000,0001,100,0001,200,0001,300,0001,400,0001,500,000
1998 1999 2000 2001 2002 2003 2004 2005P.B
Fiscal Year
Do
llars
in T
ho
usa
nd
s
Grants Contracts IRP RMS Total

How Does a Practical Clinical Trial Differfrom a Traditional Clinical Trial?
Symptoms and Function(effectiveness)
Symptoms (efficacy)Outcome
MonthsWeeksDuration
Treatment vs. TreatmentTreatment vs. PlaceboDesign
Recruitment relies oncommunity practice settings,including private practicesand state facilities.
Recruitment relies on patientscoming to academic healthcenters.
Setting
InclusiveExclusivePopulation
Practical Clinical TrialsTraditional Clinical Trials
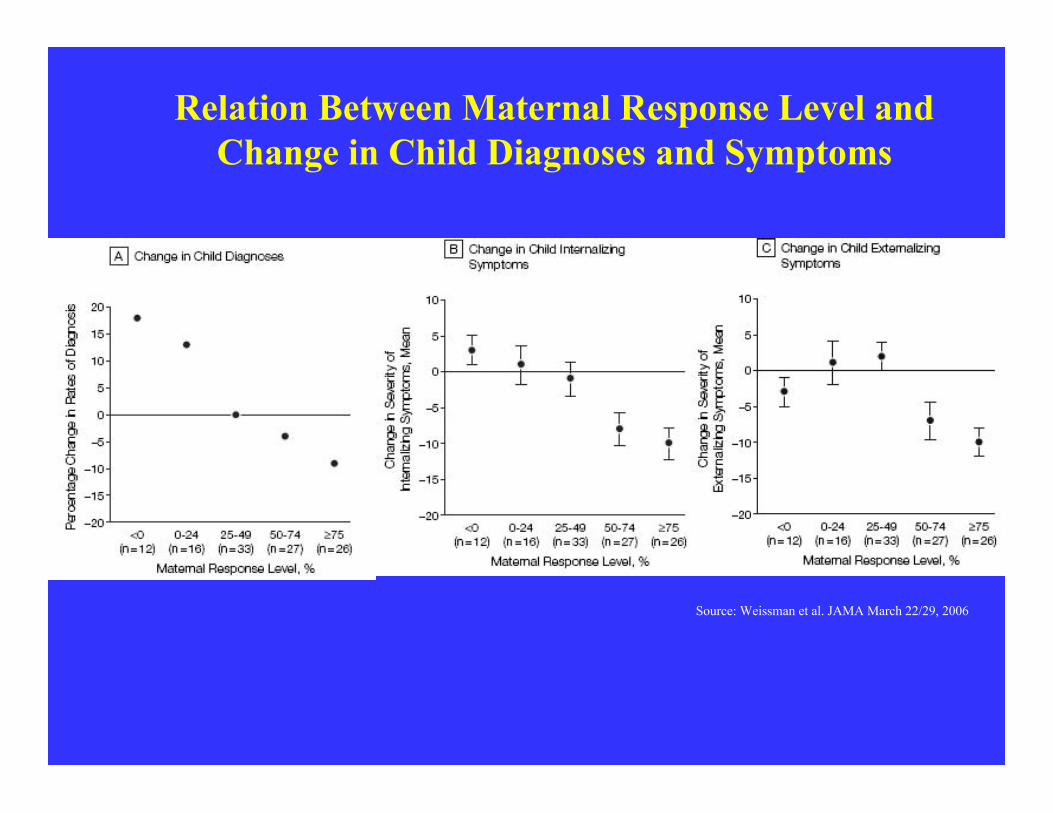
Relation Between Maternal Response Level andChange in Child Diagnoses and Symptoms
Source: Weissman et al. JAMA March 22/29, 2006