a strategy to improve the utilization of pneumococcal vaccine
TRANSCRIPT

A Strategy to Improve the Utilization of Pneumococcal Vaccine
CAROL YN M. CLANCY, MD, DANIEL GELFMAN, MD, ROY M. POSES, MD
Objective: To evaluate the effectiveness o f a computer i zed reminder f o r pne tonococcal vaccinat ion at hospi ta l dis- charge a n d to de termine p a t i e n t a n d phys i c ian character- istics associated with increased use o f the vaccine. Design: Pre- a n d p o s t i ~ n study. Setting: All medical services in a univers i ty teaching hosp i ta l Participants: All pa t i en t s with a t least one ind ica t ion f o r pneumococca l vaccinat ion d ischarged f r o m the hospi ta l d u r i n g one o f two three-month t ime per tods; res ident a n d facu l t y phys ic ians car ing f o r the same pat ients . Intervention: Incorpora t ion o f a pred i scharge reminder f o r pneumococca l vaccinat ion in the hospi ta l i n fo rma t ion system. Measurements and main results: O f 539 eligible pa t i en t s d ischarged dur ing the three months af ter the intervention, 244 (4596) received the vaccine compared with 16 o f 474 (3.4%) before the i ~ o n (p < 0.0001). Following the intertmntion, pa t i en t s d ischarged with a d iagnos is o f aico- hol ism were more likely to receive the vaccine than were those without that diagnos is (58.1% vs. 42. 7%, p < 0.05), while pa t i en t s with a d iagnos is o f cancer were less l ikely to get the vaccine (42 o f 130, o r 32.3%) than were those with- ou t cancer (202 o f 409, 49.3%) (p < 0.01). Patients whose at tending phys i c ians special ized in hemato logy- oncoiogy o r cardiology were also less l ikely to receive the vaccine than were all o therpat tents . With the in tervent ion in place, phys i c ians were move likely to vaccinate pa t i en t s wi th move than one indicat ion f o r ptwunu)coccal vaccine. Conclusions: 1) A pred i scharge reminder is an inexpen- sive, effective method to improve physic ians" u t i l i za t ion o f pnetmu)coccal vaccine in high-rtsk pat tents; 2) add i t iona l improvements in pneumococca l vaccine u t i l i za t ion will re- quire selective componen t s directed toward specific diag- noses o r a t tending phys i c ian subspecial t~s. Key words: pneumococca l vaccine; preven t ive services; phys ic ians; computer reminders; u t i l i za t to~ J GEN INYvw, N MED 1992;7:14-18.
PNEUMOCOCCAL INFECTIONS remain an important cause of morbid i ty and mortal i ty in e lder ly and high-risk pa- tients. 1-3 Although the pneumococca l vaccine has been available in the United States for the past 12 years, less than 20% of the target popula t ion has ever been vaccin- ated. 2 The benefits of vaccinat ion in prevent ing pneu- mococca l bac teremia and pneumococca l p n e u m o n i a have been wel l established, 2, 4.s and economic analyses have est imated that vaccinat ion of high-risk individuals would be cost-effective. 9, lo Vaccination is recom- mended by the Immuniza t ion Practices Advisory Com-
Received from the Department of Internal Medicine, Medical College of Virginia, Richmond, Virginia.
Supported in part by a grant from Lederle Pharmaceuticals. Address correspondence and reprint requests to Dr. Clancy:
Agency for Health Care Policy and Research, Executive Office Center, Room 678, 2101 East Jefferson Street, Rockville, MD 20852-4908.
14
mit tee (ACIP) and o ther exper t panels 2, xl for all per- sons aged over 65 years and for younger persons wi th high-risk conditions. The major factor l imiting the true effectiveness of the vaccine, however , is the poo r deliv- ery of the vaccine to those w h o need it most.
Fedson has demonstra ted in several studies that a majority of patients wi th pneumococca l bac te remia and pneumon ia due to all causes have had a previous hospitalization in the past five years, and has advocated a pol icy of immuniz ing high-risk patients at hospital d i scharge) T M Klein and Adachi showed that 78% of vaccine-el igible patients on medical inpat ient units can be identified by infection control nurses and vaccin- ated using this approach. 15 While this strategy is un- deniably effective, it is also labor-intensive and this may limit its potent ial usefulness in other settings.
Several studies have shown that s imple reminders, e i ther manual or computer ized , can significantly en- hance physicians ' use of prevent ive services. 16-2° We tested the effectiveness of integrating a predischarge reminder for pneumococca l vaccinat ion into the dis- charge orders pa thway of a hospital information system (HIS). The study addressed two questions: 1) can a compute r i zed predischarge reminder substantially in- crease del ivery of the pneumococca l vaccine to high- risk patients? and 2) are specific pat ient or physician characterist ics associated with increased use of the vaccine?
METHODS
Intervention
At the Medical College of Virginia Hospital, all pa- tient orders are execu ted through the HIS. A predis- charge reminder for pneumococca l vaccinat ion was in- c luded in the HIS on February 21, 1985. Before discharge orders can be entered, two full-screen mes- sages are displayed. The first message inquires about the pat ient ' s pneumococca l immunizat ion status, and the second screen reminds the physician of current Centers for Disease Control (CDC) recommendat ions for pneumococca l vaccination. Following these mes- sages, the physician is asked whe the r he or she wishes to order the vaccine. If the answer is yes, the pat ient receives the vaccine. The physician is free to disregard the reminder, but cannot discharge a pat ient wi thout encounter ing it. In our hospital, the vast majori ty of discharge orders are entered by the intern caring for the patient. A pr inted copy of all orders entered is stored in the pat ient ' s medical record.
JOURNAL OF GENERAL INTERNAL MEDICINE, Volume 7 (January/February), 1992 15
Subjects
All patients discharged from the medical services during one of two specified three-month t ime periods with at least one indication for the pneumococca l vac- cine were included in the study. We considered any diagnosis associated with an increased risk of serious pneumococca l infection as wel l as age --> 65 years to be indications for pneumococca l vaccination. 2 Patients who previously had received the vaccine and those who had died while in the hospital were excluded, as were patients admitted to the medical service and discharged from another service. There are six to eight inpatient (excluding intensive care unit) teams on the medical service, each staffed by one attending physician, one resident, and two or three interns, in addition to medi- cal students.
Assessment
We compared patients discharged be tween No- vember 1, 1984, and February 1, 1985 (control) , with those discharged be tween March 1, 1985, and May 31, 1985 (intervention). Two independent reviewers, both senior medical students, abstracted charts for the following information: age, dates of admission and dis- charge, number of indications for pneumococca l vac- cine, and whether the patient had been vaccinated be- fore admission. Outpat ient records were reviewed for patients fol lowed in the Medical College of Virginia outpat ient clinics to verify prior vaccination. For exam- ple, a 66-year-old patient with chronic obstructive pul- monary disease had two indications, while any patient 65 or older with no other risk factor for serious pneu- mococcal infection had one indication. The ou tcome measure was an order for the vaccine entered in the compute r at hospital discharge. The unit of analysis was the hospital admission; that is, for a patient who had been admitted more than once, one admission was counted. Once a patient had received the pneumococ- cal vaccine, no additional admission was considered. Last, we ascertained whether patient characteristics (i.e., the number of indications per eligible patient) were predict ive of the probabil i ty of being vaccinated. A 10% sample of records were also reviewed by one of the investigators (CMC) to verify accuracy of coding.
Analysis
We tested the fol lowing hypotheses: 1) eligible patients admitted to the hospital during the interven- tion per iod were more likely to receive the pneumo- coccal vaccine than were comparable patients admit- ted during the control period, 2) physicians were not more likely to vaccinate patients of any disease type, i.e., the l ikelihood of being vaccinated was not disease- specific, 3) physicians were more likely to vaccinate patients with a greater burden of disease, that is, the
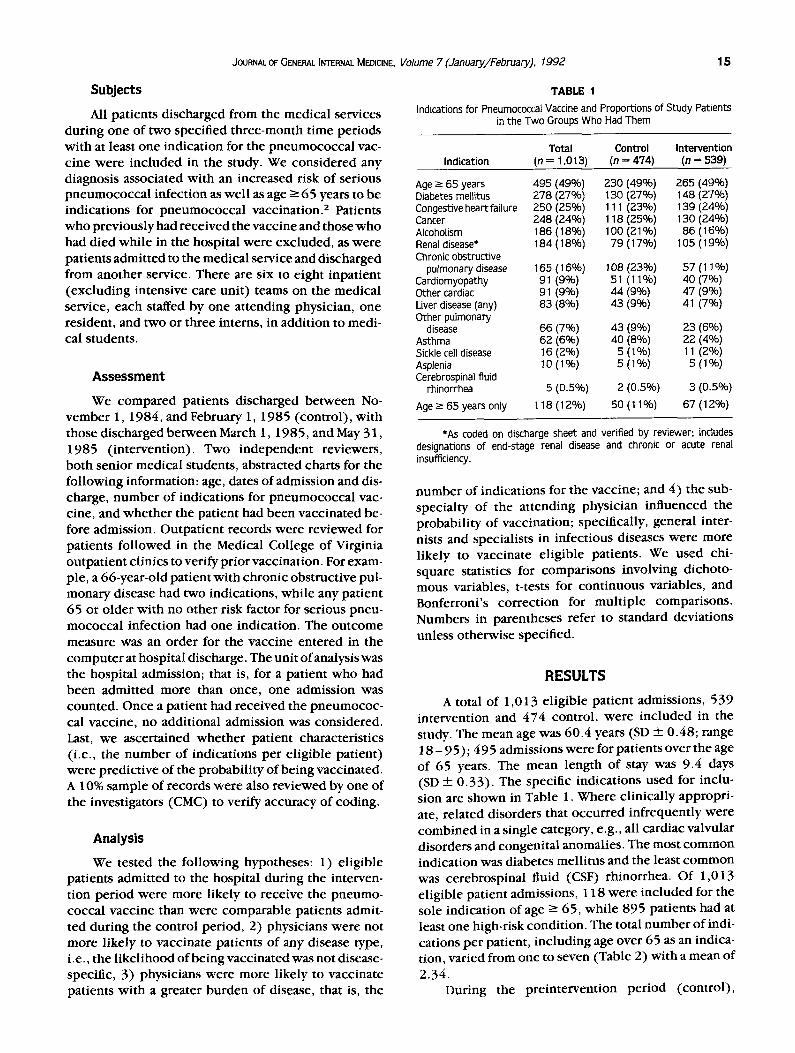
TABLE 1 Indications for Pneumococcal Vaccine and Proportions of Study Patients
in the Two Groups Who Had Them
Total Control Intervention Indication (n = 1,013) (n = 474) (n = 539)
Age - 65 years 495 (49%) 230 (49%) 265 (49%) Diabetes mellitus 278 (27%) 130 (27%) 148 (27%) Congestive heartfailure 250 (25%) 111 (23%) 139 (24%) Cancer 248 (24%) 118 (25%) 130 (24%) Alcoholism 186 (18%) 1 O0 (21%) 86 (16%) Renal disease* 184 (18%) 79 (17%) 105 (19%) Chronic obstructive
pulmonary disease 165 (16%) 108 (23%) 57 (11%) Cardiomyopathy 91 (9%) 51 (11%) 40 (7%) Other cardiac 91 (9%) 44 (9%) 47 (9%) Liver disease (any) 83 (8%) 43 (9%) 41 (7%) Other pulmonary
disease 66 (7%) 43 (9%) 23 (6%) Asthma 62 (6%) 40 (8%) 22 (4%) Sickle cell disease 16 (2%) 5 (1%) 11 (2%) Asplenia 10 (1%) 5 (1%) 5 (1%) Cerebrospinal fluid
rhinorrhea 5 (0.5%) 2 (0.5%) 3 (0,5%)
Age >_ 65 years on ly 118(12%) 50(11%) 67(12%)
*As coded on discharge sheet and verified by reviewer; includes designations of end-stage renal disease and chronic or acute renal insufficiency.
number of indications for the vaccine; and 4) the sub- specialty of the attending physician influenced the probabil i ty of vaccination; specifically, general inter- nists and specialists in infectious diseases were more likely to vaccinate eligible patients. We used chi- square statistics for comparisons involving dichoto- mous variables, t-tests for cont inuous variables, and Bonferroni 's correct ion for mult iple comparisons. Numbers in parentheses refer to standard deviations unless otherwise specified.
RESULTS
A total of 1,013 eligible patient admissions, 539 intervention and 474 control, were included in the study. The mean age was 60.4 years (SD + 0.48; range 1 8 - 95); 495 admissions were for patients over the age of 65 years. The mean length of stay was 9.4 days (SD + 0 .33) . The specific indications used for inclu- sion are shown in Table 1. Where clinically appropri- ate, related disorders that occurred infrequently were combined in a single category, e.g., all cardiac valvular disorders and congenital anomalies. The most common indication was diabetes mellitus and the least common was cerebrospinal fluid (CSF) rhinorrhea. Of 1,013 eligible patient admissions, 118 were included for the sole indication of age -> 65, while 895 patients had at least one high-risk condition. The total number of indi- cations per patient, including age over 65 as an indica- tion, varied from one to seven (Table 2) with a mean of
2.34. During the preintervent ion per iod (control) ,
16 Clanc.y et aL. PNEUMCEECAL VACCINE UTlUZATION
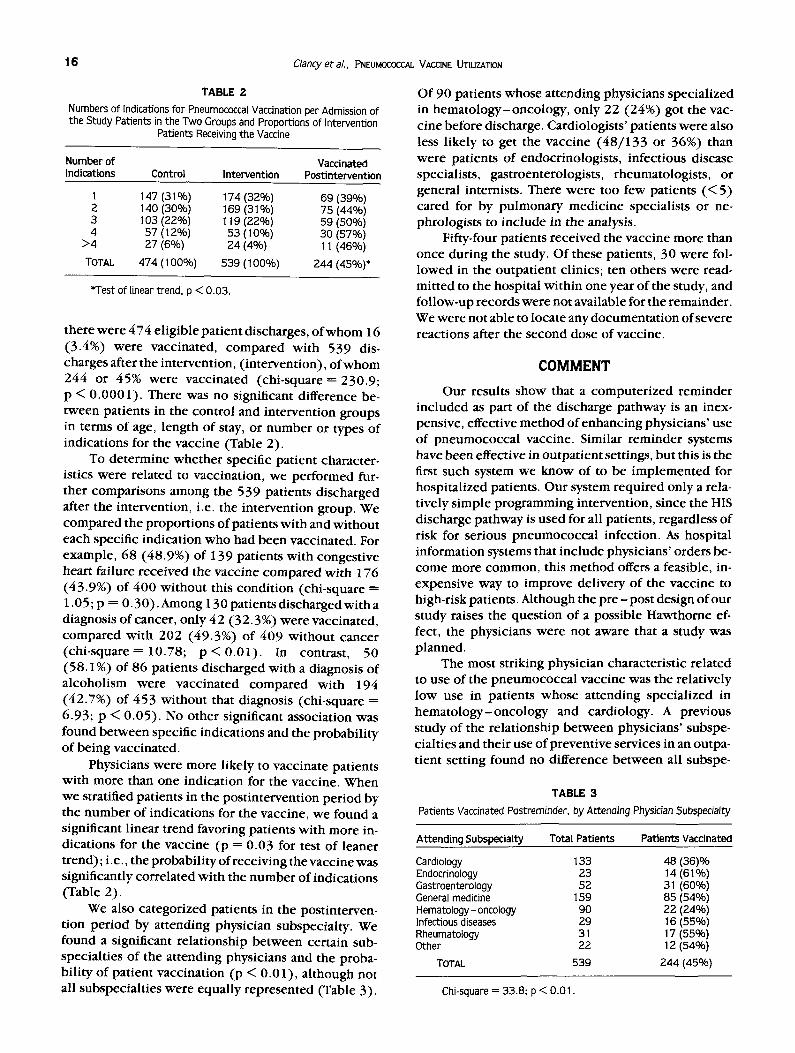
TABLE 2
Numbers of Indications for Pneumococcal Vaccination per Admission of the Study Patients in the Two Groups and Proportions of Intervention
Patients Receiving the Vaccine
Number of Vaccinated Indications Control Intervention Postintervention
1 147 (31%) 174 (32%) 69 (39%) 2 140 (30%) 169 (31%) 75 (44%) 3 103 (22%) 119 (22%) 59 (50%) 4 57 (12%) 53 (10%) 30 (57%)
>4 27 (60) 24 (4%) 11 (46%)
TOTAL 474 (100%) 539 (100%) 244 (45%)*
*Test of linear trend, p < 0.03.
there were 474 eligible patient discharges, of whom 16 (3.4%) were vaccinated, compared with 539 dis- charges after the intervention, (intervention), of whom 244 or 45% were vaccinated (chi-square = 230.9; p < 0.0001). There was no significant difference be- tween patients in the control and intervention groups in terms of age, length of stay, or number or types of indications for the vaccine (Table 2).
To determine whether specific patient character- istics were related to vaccination, we performed fur- ther comparisons among the 539 patients discharged after the intervention, i.e. the intervention group. We compared the proportions of patients with and without each specific indication who had been vaccinated. For example, 68 (48.9%) of 139 patients with congestive heart failure received the vaccine compared with 176 (43.9%) of 400 without this condition (chi-square = 1.05; p = 0.30). Among 130 patients discharged with a diagnosis of cancer, only 42 (32.3 %) were vaccinated, compared with 202 (49.3%) of 409 without cancer (chi-square---- 10.78; p < 0.01). In contrast, 50 (58.1%) of 86 patients discharged with a diagnosis of alcoholism were vaccinated compared with 194 (42.7%) of 453 without that diagnosis (chi-square = 6.93; p < 0.05). No other significant association was found between specific indications and the probability of being vaccinated.
Physicians were more likely to vaccinate patients with more than one indication for the vaccine. When we stratified patients in the postintervention period by the number of indications for the vaccine, we found a significant linear trend favoring patients with more in- dications for the vaccine (p = 0.03 for test of leaner trend); i.e., the probability of receiving the vaccine was significantly correlated with the number of indications (Table 2).
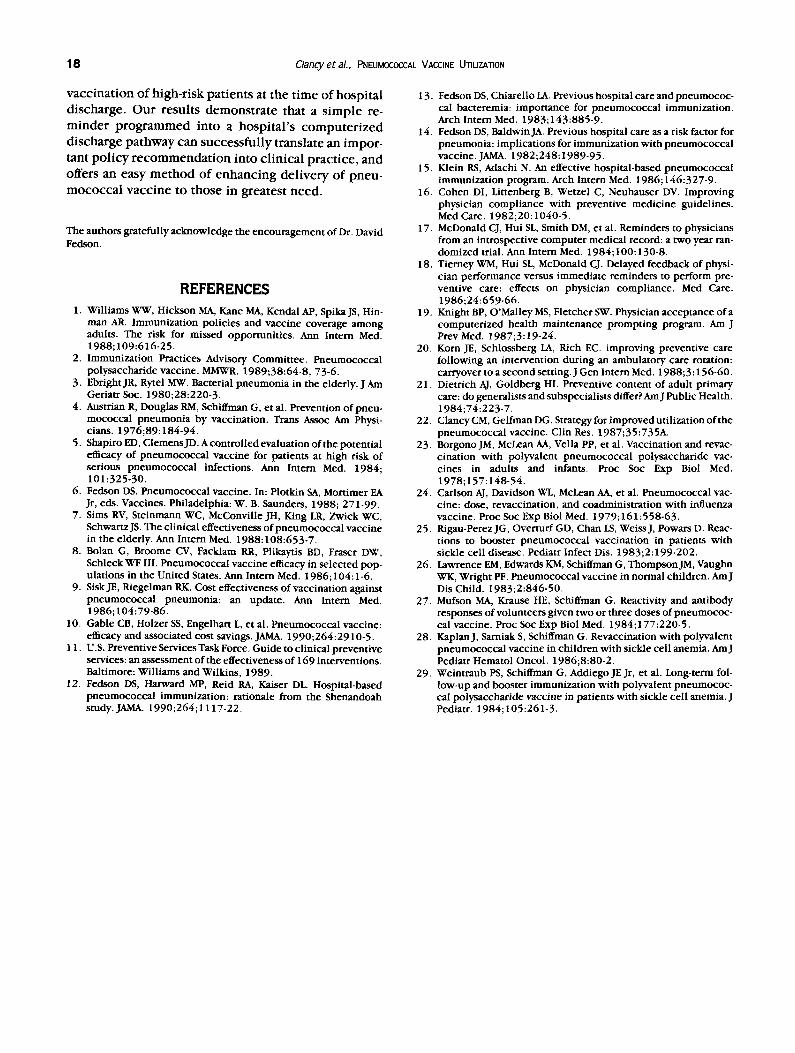
We also categorized patients in the postinterveno tion period by attending physician subspecialty. We found a significant relationship between certain sub- specialties of the attending physicians and the proba- bility of patient vaccination (p < 0.01), although not all subspeciahies were equally represented (Table 3).
Of 90 patients whose attending physicians specialized in hematology-oncology, only 22 (24%) got the vac- cine before discharge. Cardiologists' patients were also less likely to get the vaccine (48/133 or 36%) than were patients of endocrinologists, infectious disease specialists, gastroenterologists, rheumatologists, or general internists. There were too few patients (< 5) cared for by pulmonary medicine specialists or ne- phrologists to include in the analysis.
Fifty-four patients received the vaccine more than once during the study. Of these patients, 30 were fol- lowed in the outpatient clinics; ten others were read- mitted to the hospital within one year of the study, and follow-up records were not available for the remainder. We were not able to locate any documentation of severe reactions after the second dose of vaccine.
COMMENT
Our results show that a computerized reminder included as part of the discharge pathway is an inex- pensive, effective method of enhancing physicians' use of pneumococcal vaccine. Similar reminder systems have been effective in outpatient settings, but this is the first such system we know of to be implemented for hospitalized patients. Our system required only a rela- tively simple programming intervention, since the HIS discharge pathway is used for all patients, regardless of risk for serious pneumococcal infection. As hospital information systems that include physicians' orders be- come more common, this method offers a feasible, in- expensive way to improve delivery of the vaccine to high-risk patients. Although the p r e -pos t design of our study raises the question of a possible Hawthorne ef- fect, the physicians were not aware that a study was planned.
The most striking physician characteristic related to use of the pneumococcal vaccine was the relatively low use in patients whose attending specialized in hematology-oncology and cardiology. A previous study of the relationship between physicians' subspe- ciahies and their use of preventive services in an outpa- tient setting found no difference between all subspe-
TABLE 3
Patients Vaccinated Postreminder, by Attending Physician Subspecialty
Attending Subspecialty Total Patients Patients Vaccinated
Cardiology 133 48 (36)% Endocrinology 23 14 (61%) Gastroenterology 52 31 (60%) General medicine 159 85 (54%) Hematology- oncology 90 22 (240/0) Infectious diseases 29 16 (55%) Rheumatotogy 31 17 (55%) Other 22 12 (54%)
TOTAL 539 244 (45%)
Chi-square = 33.8; p < 0.01.
JOURNAL OF GENERAL INTERNAL MEDICINE. Volume 7 (January/February), 1992 17
cialists and generalists. 21 Hemato log i s t -onco log i s t s may bel ieve that vaccinating patients wi th dismal prog- noses is unnecessary, or that their patients are less l ikely to respond to the vaccine. It is less clear why cardiolo- gists at this hospital offered the vaccine to relatively fewer patients than did other at tending physicians.
Physicians were more likely to offer the vaccine to patients wi th a discharge diagnosis of a lcohol ism and to those wi th more than one indication for the vaccine. On the other hand, physicians were less l ikely to vaccinate patients wi th cancer. We speculate that these physi- cians bel ieved the risk of serious pneumococca l infec- t ion is additive, causing the l ikel ihood of vaccinat ion to increase significantly wi th the n u m b e r of individual risk factors. It is less clear why physicians ' behavior varied for patients wi th diagnoses of a lcohol ism and cancer; possibly physicians be l ieved that the fo rmer were less l ikely to obtain fo l low-up care after discharge and the latter were less l ikely to respond to the vaccine. Alternatively, physicians ' sense of futili ty in dealing wi th alcoholics may be at tenuated by providing the vaccine pr ior to discharge.
While this s tudy confirms the results of o ther stud- ies, one might reasonably ask why this and similar re- minder systems are not 1 00% effective; i.e., why d idn ' t these physicians order the pneumococca l vaccine for all el igible patients? We did not provide feedback to physicians on their performance; this might have fur- ther enhanced their use of the vaccine. Our results may offer some insight concerning the interact ion be tween the target of the intervent ion (the physician) and the intervention itself. These findings suggest that physi- cians' responses to the reminder were cognit ive rather than s imply reflexive. While a different type of re- minder system might have been more effective (e.g., high-risk patients could have received the vaccine un- less the physician had ordered that it not be given), this suggests that future improvements in physicians ' use of prevent ive services may require more select ive inter- ventions. Finally, the current recommendat ions for the vaccine are not wi thout controversy, and some physi- cians may have disagreed wi th the recommenda t ions for some patients, or be l ieved that some patients were unl ikely to respond, part icularly patients wi th cancer. It is also possible that some physicians were concerned that patients, would be less l ikely to respond to the vaccine due to possible i l lness-induced (relative) im- munosuppress ion . While there are no data to confirm or refute this possibility, there are ample data that phy- sicians' overall use of the v a c c i n e - - i n any clinical s e t t i n g - - i s less than r ecommended .
This s tudy has some limitations that should be con- sidered. First, our findings are based on the accuracy of the hospital record. While the HIS ensures increased accuracy for some port ions of the medical record, such as orders, o ther parts of the record are subject to limita- tions similar to those noted in a similar s tudy by Sims et
al.7 Second, we considered the pr imary event of interest to be the decision to vaccinate at hospital discharge, so we used the hospital discharge as the unit of analysis. It might be argued that since the intervention was di- rected at the physician, the unit of analysis should be the physician. Our HIS does not designate individual residents, so we were not able to de termine the n u m b e r of patients per physician. Given the emphasis on work- load equi ty in our training program, and since over 5 0% of the residents in the s tudy were discharging patients in both the control and intervention periods, it seems unl ikely that this would have diminished the overall effect of the intervention. An alternative unit of analysis would be the individual patient. We presented prel imi- nary findings f rom this study previously and found a higher rate of vaccinat ion (5 1%) when present ing the results as the propor t ion of patients vaccinated. 22
Another set of issues relate to the s tructure of our HIS. Due to m e m o r y limitations, it was not possible to prevent the reminder f rom appear ing in the discharge pa thway after the pat ient had been vaccinated, i.e., the reminder was displayed for all discharged patients, re- gardless of pr ior vaccinat ion status. Patients were thus at some risk for being vaccinated more than once if they did not recall having gotten the vaccine previously or if a recent hospital record was not available. While we were not able to documen t evidence of adverse reac- tions in those vaccinated twice, the risk of a more pro- nounced local react ion fol lowing a repeat dose of vac- cine has been observed in one study 23 and suggested in others. 2429 The reminder encourages vaccinat ion if pr ior vaccinat ion status is not known; informal efforts to educate residents and nurses about this p rob lem were under taken after these results became apparent . Also, our database could not provide information con- cerning the number of doses of pneumococca l vaccine administered, so the extent o f " i n a p p r o p r i a t e " utiliza- tion, i.e., vaccinat ion of persons wi th no indication for the vaccine, is not known. In v iew of the numb er of studies document ing cont inued underuti l izat ion of the vaccine, and the low cost and risk of the vaccine, we bel ieve this is a relatively minor concern.
Finally, our conclusions concerning the relat ion of at tending physician subspecia l ty and vaccinat ion utili- zation must be regarded as tentative, since 1) the intern is most often the individual who actually writes the discharge orders and 2) we could not obtain data con- cerning the number of patients per physician. Never- theless, these observations raise concerns about the role of at tending physicians in advising residents about discharge planning and the potent ial for missed oppor- tunities in high-risk patients. If our findings are con- firmed in other settings, then possible modifications focused on specific groups of physicians may improve the overall compl iance rate wi th interventions to im- prove the use of prevent ive services.
There is ample evidence justifying pneumococca l
18 C/amy et aL, PNEUMOC_JDCCAL VACCINE UTILIZATION
v a c c i n a t i o n o f h i g h - r i s k p a t i e n t s a t t h e t i m e o f h o s p i t a l
d i s c h a r g e . O u r r e s u l t s d e m o n s t r a t e t h a t a s i m p l e re-
m i n d e r p r o g r a m m e d i n t o a h o s p i t a l ' s c o m p u t e r i z e d
d i s c h a r g e p a t h w a y c a n s u c c e s s f u l l y t r a n s l a t e a n i m p o r -
t a n t p o l i c y r e c o m m e n d a t i o n i n t o c l i n i c a l p r a c t i c e , a n d
o f f e r s a n e a s y m e t h o d o f e n h a n c i n g d e l i v e r y o f p n e u -
m o c o c c a l v a c c i n e t o t h o s e i n g r e a t e s t n e e d .
The authors gratefully acknowledge the encouragement of Dr. David Fedson.
REFERENCES 1. Williams WW, Hickson MA, Kant MA, Kendal AP, Spika JS, Hin-
man AR. Immunization policies and vaccine coverage among adults. The risk for missed opportunities. Ann Intern Med. 1988;109:616-25.
2. Immunization Practices Advisory Committee. Pueumococcal polysaccharide vaccine. MMWR. 1989;38:64-8, 73-6.
3. Ebright JR, Rytel MW. Bacterial pneumonia in the elderly. J Am Geriatr Soc. 1980;28:220-3.
4. Austrian R, Douglas RM, Schiffman G, et al. Prevention of pneu- mococcal pneumonia by vaccination. Trans Assoc Am Physi- cians. 1976;89:184-94.
5. Shapiro ED, ClemensJD.Acontrol ledevaluat ionofthe potential efficacy of pneumococcal vaccine for patients at high risk of serious pneumococcal infections. Ann Intern Med. 1984; 101:325-30.
6. Fedson DS. Pneumococcal vaccine. In: Plotldn SA, Mortimer EA Jr, eds. Vaccines. Philadelphia: W. B. Saunders, 1988; 271-99.
7. Sims RV, Steinmann WC, McConville JH, King LR, Zwick WC, Schwartz JS. The clinical effectiveness of pneumococcal vaccine in the elderly. Ann Intern Med. 1988:108:653-7.
8. Bolan G, Broome CV, Facklam RR, Plikaytis BD, Fraser DW, Schleck WF III. Pneumococcal vaccine efficacy in selected pop- ulations in the United States. Ann Intern Med. 1986;104:1-6.
9. Sisk JE, Riegelman RK. Cost effectiveness of vaccination against pneumococcal pneumonia: an update. Ann Intern Med. 1986;104:79-86.
10. Gable CB, Holzer SS, Engelhart L, et al. Pneumococcal vaccine: efficacy and associated cost savings. JAMA. 1990;264:2910-5.
11. U.S. Preventive Services Task Force. Guide to clinical preventive services: an assessment of the effectiveness of 169 interventions. Baltimore: Williams and Wilkins, 1989.
12. Fedson DS, Harward MP, Reid RA, Kaiser DL. Hospital-based pneumococcal immunization: rationale from the Shenandoah study. JAMA. 1990;264;I 117-22.
13- Fedson DS, Chiarello LA. Previous hospital care and pneumococ- cal bacteremia: importance for pneumococcal immunization. Arch Intern Med. 1983; 143:885-9.
14. Fedson DS, Baldwin JA. Previous hospital care as a risk factor for pneumonia: implications for immunization with pneumococcal vaccine. JAMA. 1982;248:1989-95.
15. Klein RS, Adachi N. An effective hospital-based pneumococcal immunization program. Arch Intern Med. 1986;146:327-9.
16. Cohen DI, Littenberg B, Wetzel C, Neuhauser DV. Improving physician compliance with preventive medicine guidelines. Med Care. 1982;20:1040-5.
17. McDonald CJ, Hui SL, Smith DM, et al. Reminders to physicians from an introspective computer medical record: a two year ran- domized trial. Ann Intern Med. 1984;100:130-8.
18. Tierney WM, Hui SL, McDonald CJ. Delayed feedback of physi- cian performance versus immediate reminders to perform pre- ventive care: effects on physician compliance. Med Care. 1986;24:659-66.
19. Knight BP, O'Malley MS, Fletcher SW. Physician acceptance of a computerized health maintenance prompting program. Am J Prev Med. 1987;3:19-24.
20. Korn JE, Schlossberg LA, Rich EC. improving preventive care following an intervention during an ambulatory care rotation: carryover to a second setting. J Gen Intern Med. 1988;3:156-60.
21. Dietrich AJ, Goldberg HI. Preventive content of adult primary care: do generalists and subspecialists differ? AmJ Public Health. 1984;74:223-7.
22. ClancyCM, GelfmanDG. Strategyforimprovedutil izationofthe pneumococcal vaccine. Clin Res. 1987;35:735A.
23. Borgono JM, McLean AA, Vella PP, et al. Vaccination and revac- cination with polyvalent pneumococcal polysaccharide vac- cines in adults and infants. Proc Soc Exp Biol Med. 1978;157:148-54.
24. Carlson AJ, Davidson WL, McLean AA, et al. Pneumococcal vac- cine: dose, revaccination, and coadministration with influenza vaccine. Proc Soc Exp Biol Med. 1979; 161 : 558-63.
25. Rigau-Perez JG, Overturf GD, Chan LS, Weiss J, Powars D. Reac- tions to booster pneumococcai vaccination in patients with sickle cell disease. Pediatr Infect Dis. 1983;2:199-202.
26. Lawrence EM, Edwards KM, schiffman G, ThompsonJM, Vaughn WK, Wright PF. Pneumococcal vaccine in normal children. AmJ Dis Child. 1983;2:846-50.
27. Mufson MA, Krause HE, Schiffman G. Reactivity and antibody responses of volunteers given two or three doses of pneumococ- cal vaccine. Proc Soc Exp Biol Med. 1984;177:220-5.
28. Kaplan J, Sarniak S, schiffman G. Revaccination with polyvalent pneumococcal vaccine in children with sickle cell anemia. AmJ Pediatr Hematol Oncol. 1986;8:80-2.
29. Weintraub PS, schiffman G, Addiego JE Jr, et al. Long-term fol- low-up and booster immunization with polyvalent pneumococ- cal polysaccharide vaccine in patients with sickle cell anemia. J Pediatr. 1984;105:261-3.