a study of a volunteer caregiver program
TRANSCRIPT
This article was downloaded by: [University of West Florida]On: 09 October 2014, At: 12:30Publisher: RoutledgeInforma Ltd Registered in England and Wales Registered Number: 1072954 Registeredoffice: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK
Activities, Adaptation & AgingPublication details, including instructions for authors andsubscription information:http://www.tandfonline.com/loi/waaa20
A Study of a Volunteer CaregiverProgramTara Jorgenson MS a & Gregory Sanders PhD aa Child Development and Family Science , North Dakota StateUniversity , USAPublished online: 12 Aug 2009.
To cite this article: Tara Jorgenson MS & Gregory Sanders PhD (2003) A Study of a Volunteer CaregiverProgram, Activities, Adaptation & Aging, 27:2, 53-69, DOI: 10.1300/J016v27n02_05
To link to this article: http://dx.doi.org/10.1300/J016v27n02_05
PLEASE SCROLL DOWN FOR ARTICLE
Taylor & Francis makes every effort to ensure the accuracy of all the information (the“Content”) contained in the publications on our platform. However, Taylor & Francis,our agents, and our licensors make no representations or warranties whatsoever as tothe accuracy, completeness, or suitability for any purpose of the Content. Any opinionsand views expressed in this publication are the opinions and views of the authors,and are not the views of or endorsed by Taylor & Francis. The accuracy of the Contentshould not be relied upon and should be independently verified with primary sourcesof information. Taylor and Francis shall not be liable for any losses, actions, claims,proceedings, demands, costs, expenses, damages, and other liabilities whatsoever orhowsoever caused arising directly or indirectly in connection with, in relation to or arisingout of the use of the Content.
This article may be used for research, teaching, and private study purposes. Anysubstantial or systematic reproduction, redistribution, reselling, loan, sub-licensing,systematic supply, or distribution in any form to anyone is expressly forbidden. Terms &Conditions of access and use can be found at http://www.tandfonline.com/page/terms-and-conditions

A Study of a Volunteer Caregiver Program
Tara JorgensonGregory Sanders
ABSTRACT. The purpose of this study was to examine experiences ofparticipation in a Volunteer Caregiver Program in a rural North Dakotacounty. Data were collected from both the volunteer caregivers and thecare receivers. This study examined the participant’s demographic char-acteristics, supports that were needed and services provided, the pro-gram’s strengths and weaknesses, barriers that were involved for familymembers in providing elder care for their relative, and the overall experi-ence among participants in the program. Overall, both the volunteers andcare receivers had very positive experiences with this program. [Articlecopies available for a fee from The Haworth Document Delivery Service:1-800-HAWORTH. E-mail address: <[email protected]> Website:<http://www.HaworthPress.com> © 2002 by The Haworth Press, Inc. All rightsreserved.]
KEYWORDS. Volunteers, caregiver, rural, informal care
While family members provide extensive support to older adults, sit-uations often result in critical gaps in informal support. Currently, fami-
Tara Jorgenson, MS, is a counselor in Cheyenne, Wyoming, and received her mas-ters in Child Development and Family Science at North Dakota State University.
Gregory Sanders, PhD, is Professor of Child Development and Family Science atNorth Dakota State University.
Address correspondence to: Gregory Sanders, Department of Child Developmentand Family Science, North Dakota State University, 283 EML, Fargo, ND 58105(E-mail: [email protected]).
Activities, Adaptation & Aging, Vol. 27(2) 2002http://www.haworthpress.com/store/product.asp?sku=J016
2002 by The Haworth Press, Inc. All rights reserved.10.1300/J016v27n02_05 53
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

lies are smaller, divorce rates are higher, and women are increasinglyparticipating in the work force resulting in fewer potential family re-sources available for helping an aging parent (Zarit, Johansson, &Jarrott, 1998). Huston (1990) estimated that five million older Ameri-cans need daily help in order to remain living in their homes (Huston,1990). The need for home help often arises from a situation where an el-derly person can no longer cope with daily life and chores because ofworsening functional ability. Although the majority of elderly adultswould prefer informal care, which provides a sense of familiarity, toooften those services are not sufficient to meet their needs (Herlitz,1997). Distance, lack of skills and/or training, or conflict in schedulesare a few reasons why informal care (specifically from family mem-bers) often is not enough to meet the needs of many elders (Herlitz,1997).
One of the goals of elder care has long been to find the right matchbetween need and support. Often, an appropriate match between sup-port and need results in the older adult being able to remain in his/herown home. In rural areas, finding that match can be difficult both be-cause of the family issues mentioned above and because of the lack offormal supports in rural areas. Blieszner, McAuley, Newhouse, andMancini (1987) found that rural elders had more need for assistance inmeal preparation, homemaking, and personal care, yet they were lesslikely to get it through the formal system. The result may be that ruralelders remain in their own homes without the support they need or relo-cate to the nearest nursing home in an environment that may be restric-tive and overly supportive relative to need.
As the number of elderly people increases, so does the need for re-source supports and caring for the elders. Maintaining health and effec-tive functioning may not occur without formal or informal supports atvarious times over one’s life span. Providing support through volun-teers can help fill the gaps between formal supports and family sup-ports. Informal supports represent close, intimate relationships, includingfamily members, and friends; whereas formal supports represent orga-nized, business-like organizations, including facility staff, serviceagencies, and community organizations (Stephens & Christianson,1986). Limitations lie within both informal and formal elderly care ar-rangements.
Ellefson (2001) described the concept of programs organized by for-mal supports utilizing informal volunteers, “Paid staff with formal reg-ulations organize informal supports to fulfill needs specified by elderlypersons” (Ellefson, 2001, p. 15). Such organized volunteer supports can
54 ACTIVITIES, ADAPTATION & AGING
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

provide relief to family caregivers and meet needs not currently beingmet by formal supports or family members and friends.
The current study focused on the experiences of both the volunteersand care receivers in an informal support program called the VolunteerCaregiver Program in a rural North Dakota county. Throughout this pa-per, characteristics of the volunteer caregivers and care receivers, spe-cific services provided by the caregivers and received by the carereceivers, and strengths and weaknesses of the program are describedby both groups. Information about how individuals first learned aboutthe Volunteer Caregiver Program is presented and other experienceswith the program by both volunteers and care receivers are highlighted.
The purpose of this study was to answer the following research ques-tions.
1. What services did volunteer caregivers provide, and what sup-ports were needed by care receivers?
2. How did the respondents first learn about the Volunteer CaregiverProgram?
3. What program strengths and weaknesses did the volunteer care-givers and the care receivers identify?
4. What experiences have care receivers and volunteers had with theVolunteer Caregiver Program?
METHODS
Procedure
The subjects consisted of the volunteer caregivers and the care re-ceivers from a volunteer caregiver program in a rural, North Dakotacounty. The questionnaires for the volunteers were mailed to theirhomes. The questionnaires for the care receivers were administeredthrough face-to-face interviews. Following the initial mailing for thevolunteers, reminder questionnaires were sent following a four-weekperiod to those who had not returned their questionnaires. The reminderquestionnaires added six returned questionnaires. Fifty-three question-naires were sent to the volunteer caregivers, and 40 returned them for areturn rate of 75%.
Sixty-four care receivers were interviewed face-to-face, and one carereceiver was interviewed by telephone. Eleven of the care receiverslisted as being in the program were not able to be interviewed because
Tara Jorgenson and Gregory Sanders 55
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

of death or illness or because they moved away, were in the hospital, orwere in a nursing home. Fourteen refused to participate for unknownreasons. The participation rate of the care receivers was 72%.
Participants
A greater number of females participated as volunteers (70%) thanmales (30%), and almost all (95%) of the volunteers were white. Themajority of the volunteers in this program were older adults and nonewere under the age of 35. Seventy-three percent of the volunteers whoresponded were over the age of 65, and 28% were over the age of 75.Ages 65 to 74 were the largest age group, making up 45% of the totalvolunteers. The second largest age group, ages 75 to 84, made up 28%of the volunteers.
The care receivers in this program represented a wide range of agegroups, from age 35 to over 85-years-old. However, the two largestgroups were aged 85-years-old or over (40%) and 75 to 84 (29%). Agreater number of females received services (85%) than males (15%)and almost all (98%) of the care receivers were white.
Over half (68%) of the volunteers were married and (63%) retired.The majority of the care receivers (60%) were widowed. Seventy-sevenpercent of care receivers lived alone, 18% lived with a spouse, and 5%lived with family. A total of 33% of caregivers were high school/GEDgraduates, while 28% had completed some college and 28% completedtheir bachelors. Thirty-four percent of care receivers completed 6-8grades and 26% completed high school/GED.
Materials
The surveys consisted of checklists, Likert-type items with a five-point response scale (strongly agree to strongly disagree), and open-ended items. The Volunteer Caregiver Questionnaire and the Care Re-ceiver Questionnaire were similar in format, asking basic demographicinformation related to age, gender, ethnicity, education, employment,and marital status. Volunteers were asked to identify specific servicesthey have provided or would like to give and care receivers were askedto identify specific services they have received and would like to re-ceive. Both groups of respondents were asked to identify how they firstlearned of the Volunteer Caregiver Program.
The Volunteer Caregiver Questionnaire included questions regard-ing length of time they had been volunteering with this program and
56 ACTIVITIES, ADAPTATION & AGING
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

specific issues concerning the amount of time they spent volunteering.Caregivers were asked to rate items regarding why they volunteered forthis program, the strengths and weaknesses of this program, additionalways the program could help, how others could be encouraged to partic-ipate in this program, and under what circumstances would they accepthelp from a volunteer. Responses were based on a five-point scale rang-ing from strongly agree to strongly disagree. Questions concerning thevolunteer’s experience with the Volunteer Caregiver Program were alsopresented in a format using a five-point scale ranging from stronglyagree to strongly disagree. Two open-ended questions were providedfor additional comments and these were coded into categories.
The Care Receiver Questionnaire included a question about previousvolunteer assistance received and whether or not they received courtesytelephone calls from volunteers. Items were designed for the care re-ceivers to rate why they participated in this program, the strengths andweaknesses of the program, the ways the program affects the commu-nity, how others could be encouraged to participate, and how theirneeds would be met if not for this program. Questions concerning thecare receivers experience with the volunteers and the Volunteer Care-giver Program were presented in a format using a five-point scale(strongly agree to strongly disagree). Two open-ended questions wereprovided for additional comments and these were coded into categories.
RESULTS
Question 1. “What services did volunteer caregivers provide, andwhat supports were needed by care receivers?” Table 1 includes fre-quencies and percentages of the caregivers that provided service in eacharea and services they were willing to provide in the future. The fre-quencies and percentages of the services that care receivers received, aswell as services they would like to receive, in the future, are also in-cluded.
Caregivers identified the most frequently provided services as “trans-portation” (63%), “errands” (63%), “companionship” (55%), “shopping”(48%), and “telephone reassurance” (45%). The types of help that thecaregivers would like to provide in the future included “letter writing andshopping” (15%), “companionship and telephone reassurance” (10%),“errands” (8%), “financial/bills, light mending, transportation, and yard
Tara Jorgenson and Gregory Sanders 57
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

work” (5%), and “small housekeeping fix-it-jobs and personal care”(3%).
Care receivers identified the most frequently received services as“transportation” (91%), “telephone reassurance” (37%), “companion-ship” (31%), “errands” (22%), and “shopping” (14%). The types of helpthat the care receivers would like to receive in the future that they cur-rently are not receiving were “errands” (8%), “small housekeepingfix-it-jobs and yard work” (5%), and “letter writing, light housekeep-ing, personal care, transportation, and ‘other’” (2% each).
58 ACTIVITIES, ADAPTATION & AGING
TABLE 1. Volunteer Services Provided/Would Provide (caregivers*) and Vol-unteer Services Received/Would Receive (care receivers*)
Area CG has CG would CR has CR would
Companionship 55% (22) 10% (4) 31% (20) 0
Errands 63% (25) 8% (3) 22% (14) 8% (5)
Financial/Bills 3% (1) 5% (2) 5% (3) 0
Letter Writing 3% (1) 15% (6) 3% (2) 2% (1)
Light Mending 3% (1) 5% (2) 2% (1) 0
Light Housekeeping 5% (2) 0 0 2% (1)
Fix-It Jobs 5% (2) 3% (1) 2% (1) 7% (3)
Shopping 48% (19) 15% (6) 14% (9) 5% (3)
Personal Care 5% (2) 3% (1) 6% (4) 2% (1)
Phone Reassurance 45% (18) 10% (4) 37% (24) 0
Transportations 78% (31) 5% (2) 91% (59) 2% (1)
Yard Work 8% (3) 5% (2) 0 5% (3)
*Respondents could indicate more than one area.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

Question 2. “How did the respondents first learn about the VolunteerCaregiver Program?” Most (78%; 31) caregivers first learned aboutthe program from another person, 13% (5) heard about it “other” vari-ous ways such as through a speaker at a group, and 5% (2) were in-formed through the newspaper and church. Over half (52%; 34) of carereceivers first learned about the program from another person. A total of17% (11) heard about it in “other” various ways such as the RegionalHuman Service Center and the senior citizen center, and 14% (9)learned of the program through home health care.
Question 3 asked, “What program strengths and weaknesses did thevolunteer caregivers and care receivers identify?” Responses regard-ing program strengths and weaknesses are displayed in Table 2.
A total of 98% of caregivers strongly agreed or agreed that the pro-gram “helps people who need it” and 100% indicated that the program“gets people to appointments/transportation.” The majority of care-givers also strongly agreed or agreed that the program strengths in-cluded “keeps people in their homes” (94%), “social interaction andcommunication” (91%), “community unity/knowing needs” (91%),“convenient” (87%), and “good human resource” (91%).
A total of 98% of care receivers strongly agreed or agreed that the“volunteers” were a strength of the Volunteer Caregiver Program and98% responded that “service provided” was a strength. Care receiversstrongly agreed or agreed that “allows care receiver to live independ-ently” (80%), “courtesy calls” (67%), and “could not get everythingdone without help” (66%) were strengths of the program.
When asked what the program weaknesses were, 80% of caregiversstrongly agreed or agreed that “additional helpers are needed” and 76%responded that the program “needs to reach more people in need.” Care-givers strongly agreed or agreed that more “telephone reassurance/com-panionship” was needed (80%), and “more training and information”(47%) would be helpful. Weaknesses indicated by the Care Receivers(strongly agreed or agreed) were “need for more volunteers/help”(48%) “needs more transportation service” (42%).
Question 4. “What experience, overall, have care receivers andcaregivers had with the Volunteer Caregiver Program?” Five ques-tions were presented to the care receivers to identify their personal ex-perience with the Volunteer Caregiver Program (see Table 3).Ninety-seven percent of care receivers strongly agreed or agreed thattheir “ideas or suggestions were respected by the volunteer.” Ninety-seven percent strongly agreed or agreed that the “volunteer was reli-able”; 98% reported that “the time spent with the volunteer was en-
Tara Jorgenson and Gregory Sanders 59
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

60 ACTIVITIES, ADAPTATION & AGING
TABLE 2. Strengths and Weaknesses Indicated by Volunteer Caregivers of theVolunteer Caregiver Program
Strengths SD D N A SA*
Keeps people in their home 3% 0 3% 20% 74%(1) (0) (1) (7) (26)
Appoint/transportation 0 0 0 15% 85%(0) (0) (0) (6) (33)
Saves money 0 3% 20% 32% 45%(0) (1) (6) (10) (14)
Helps people who need it 0 3% 0 12% 85%(0) (1) (0) (5) (34)
Community unity 0 3% 6% 26% 65%(0) (1) (2) (9) (22)
Convenient 0 0 13% 47% 40%(0) (0) (4) (15) (13)
Good human resource 0 0 9% 44% 47%(0) (0) (3) (14) (15)
Social interaction/communication 0 0 9% 23% 68%(0) (0) (3) (8) (24)
WeaknessesAdditional help(ers) needed 6% 0 14% 22% 58%
(2) (0) (5) (8) (21)
Need to reach more people 0 3% 21% 32% 44%(0) (1) (7) (11) (15)
Telephone reassurance/ 7% 0 13% 48% 32%companionship (2) (0) (4) (15) (10)
Nothing else needed 22% 26% 33% 15% 4%(6) (7) (9) (4) (1)
More training and information 7% 14% 32% 29% 18%(2) (4) (9) (8) (5)
*SD = strongly disagree, D = disagree, N = neutral, A = agree, and SA = strongly agree.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

joyable”; and 95% reported that “the volunteer seemed adequately trained todeal with my particular needs.” Eighty-six percent strongly agreed or agreedthat they were “able to get volunteer help when needed”; however, 5% wereneutral, and 9% disagreed with this statement.
Six questions were presented to the care receivers to identify theirperception of the Volunteer Caregiver Program (see Table 4).Ninety-five percent of care receivers strongly agreed or agreed that theywere “satisfied with the Volunteer Caregiver experience.” Similarly,87% strongly agreed or agreed that the “volunteer is a substitute whenfamily members cannot help”; 81% strongly agreed or agreed that “thevolunteer helps when my family is not available to help”; and 80% re-sponded that “the volunteer adds to the help my family gives.” Otheridentified perceptions among the care receivers in the Volunteer Care-giver Program were that “the volunteer helps to allow my family more
Tara Jorgenson and Gregory Sanders 61
TABLE 3. Strengths and Weaknesses Indicated by Care Receivers of the Vol-unteer Caregiver Program
Strengths SD D N A SA*
Service provided 0 2% 0 6% 92%(0) (1) (0) (4) (58)
Allows care receiver to live 5% 7% 5% 11% 72%independently (3) (4) (3) (7) (45)
Could not get everything 8% 11% 11% 16% 54%done without help (5) (7) (7) (10) (33)
The volunteers 0 0 2% 8% 90%(0) (0) (1) (5) (58)
Courtesy calls 5% 2% 25% 22% 46%(3) (1) (16) (14) (29)
WeaknessesNeed for more volunteers/ 0 5% 47% 13% 35%
help (0) (3) (29) (8) (22)
Need for more transportation 0 10% 48% 3% 39%service (0) (6) (30) (2) (24)
*SD = strongly disagree, D = disagree, N = neutral, A = agree, and SA = strongly agree.
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4
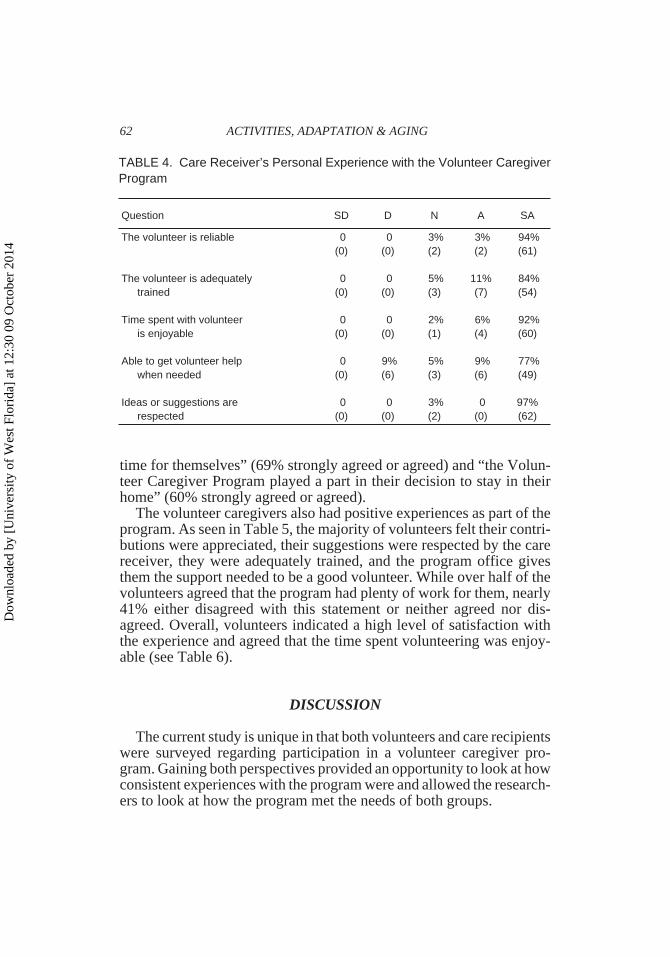
time for themselves” (69% strongly agreed or agreed) and “the Volun-teer Caregiver Program played a part in their decision to stay in theirhome” (60% strongly agreed or agreed).
The volunteer caregivers also had positive experiences as part of theprogram. As seen in Table 5, the majority of volunteers felt their contri-butions were appreciated, their suggestions were respected by the carereceiver, they were adequately trained, and the program office givesthem the support needed to be a good volunteer. While over half of thevolunteers agreed that the program had plenty of work for them, nearly41% either disagreed with this statement or neither agreed nor dis-agreed. Overall, volunteers indicated a high level of satisfaction withthe experience and agreed that the time spent volunteering was enjoy-able (see Table 6).
DISCUSSION
The current study is unique in that both volunteers and care recipientswere surveyed regarding participation in a volunteer caregiver pro-gram. Gaining both perspectives provided an opportunity to look at howconsistent experiences with the program were and allowed the research-ers to look at how the program met the needs of both groups.
62 ACTIVITIES, ADAPTATION & AGING
TABLE 4. Care Receiver’s Personal Experience with the Volunteer CaregiverProgram
Question SD D N A SA
The volunteer is reliable 0 0 3% 3% 94%(0) (0) (2) (2) (61)
The volunteer is adequately 0 0 5% 11% 84%trained (0) (0) (3) (7) (54)
Time spent with volunteer 0 0 2% 6% 92%is enjoyable (0) (0) (1) (4) (60)
Able to get volunteer help 0 9% 5% 9% 77%when needed (0) (6) (3) (6) (49)
Ideas or suggestions are 0 0 3% 0 97%respected (0) (0) (2) (0) (62)
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

Findings of the current study differ from Hayghe’s (1991) research inthat the caregivers were primarily aged 65 or older and had completedhigh school/GED; however, they were similarly mostly female andwhite. The population of this county is very homogeneous with respectto race and ethnicity. Thus the results regarding ethnicity simply reflectthe population and are not an examination of the likelihood of volun-teering by ethnicity.
The age differences may be attributed to the program’s recruitingmethods. For example, participants of the Volunteer Caregiver Programreported first learning about the program through the newspaper,churches, Regional Human Service Center, and the senior citizen cen-ter. In addition, because the program serves mostly older adults, theremay be a tendency for other older adults to volunteer. Hayghe alsofound that the majority of volunteers held college graduate degrees.However, the education level of volunteers in the current study waslower probably due to the volunteers being primarily 65 or older. Incontrast to Wheeler et al.’s (1998) finding that unmarried persons repre-sented the majority of volunteers, the largest percent of volunteer care-givers in this study were married.
Tara Jorgenson and Gregory Sanders 63
TABLE 5. Care Receivers’ Perception of the Volunteer Caregiver Program
Question SD D N A SA
Satisfied with the VCP 2% 0 3% 0 95%experience (1) (0) (2) (0) (61)
VCP related to decision 17% 9% 14% 11% 49%to stay in home (11) (6) (9) (7) (31)
Volunteer is substitute when 2% 0 11% 6% 81%family cannot help (1) (0) (7) (4) (52)
Volunteer allows family 5% 0 26% 8% 61%time for themselves (3) (0) (17) (5) (39)
The volunteer helps when 5% 0 14% 11% 70%family is not available (3) (0) (9) (7) (46)
The volunteer adds to the 5% 0 15% 8% 72%help family gives (3) (0) (10) (5) (46)
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

A higher percentage of care receivers lived alone than one would ex-pect when comparing population statistics for the appropriate agegroups in North Dakota (Sanders & Bratteli, 1994). This is not surpris-ing considering those living with others have a more readily availablesupport group and may not feel volunteer supports are needed. Thoseliving with others or their family members may also be more reluctantto request needed support than those who live alone. Respite supportmay be particularly appealing to that group and may be a support thatcould be emphasized more by the Volunteer Caregiver Program. Al-though volunteers in this study did not spend the amount of time family
64 ACTIVITIES, ADAPTATION & AGING
TABLE 6. Caregivers’ Perception of the Volunteer Caregiver Program
Question SD D N A SA
My contributions as a volunteer are appreciated0 0 5.1% 15.4% 79.5%
(0) (0) (2) (6) (31)
My ideas or suggestions are respected by the care receiver0 0 8.6% 40.0% 48.6%
(0) (0) (3) (14) (17)
When I am available VC has plenty of volunteer work for me2.7% 8.1% 29.7% 16.2% 43.2%(1) (3) (11) (6) (16)
I am satisfied with the volunteer caregiver experience0 2.6% 5.3% 23.7% 68.4%
(0) (1) (2) (9) (26)
I feel adequately trained to deal with the needs of the care receiver(s) I work with0 2.7% 16.2% 24.3% 56.8%
(0) (0) (9) (7) (46)
The VC office gives me the support I need to be a good volunteer0 0 10.8% 13.5% 75.7%
(0) (0) (4) (5) (28)
The time I spend volunteering is enjoyable0 0 5.0% 15.0% 80.0%
(0) (0) (2) (6) (32)
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

caregivers have been shown to spend (Bagby, 1993), some of the tasksthey help with, including transportation, errands, and companionship,were similar.
The care receivers of the Volunteer Caregiver Program identifiedtransportation as their largest need. When care receivers were askedwhat services they would like to receive that they currently were not,they identified errands and fix-it-jobs. When volunteer caregivers wereasked what services they would like to provide that they currently werenot providing, this group identified these tasks, and also listed compan-ionship and telephone reassurance. Several care receivers shared,through personal interview, that they were not aware of the list of ser-vices they could receive. Being more aware of both possible servicesand volunteers’ skills could benefit the volunteer caregiver by makingbetter use of special talents and interests and benefit the care receiver bymeeting a broader variety of needs.
The majority of respondents indicated they heard about the programby “word of mouth.” A small percentage had heard of the program fromthe newspaper, home health, and the hospital, and a few respondentsheard about it from their church or the radio/television. Through per-sonal interviews with the care receivers, many shared that, because ofthe usefulness of the program, it should be publicized more.
The volunteer caregivers and care receivers identified similarstrengths and weaknesses within this study. Both groups strongly agreedor agreed that “service provided,” and “the volunteers get people to ap-pointments/transportation” were positive qualities of the program.
Weaknesses identified by the two groups varied slightly. The volun-teer caregivers identified the need for more helpers as a weakness, citingthat they repeatedly provide the same care each time they volunteer whenthey would prefer to provide a variety of services. Similar to the volunteercaregivers, the care receivers also reported a need for more volunteers.However, this group also identified the need for more transportation.
Care receivers recognized that the Volunteer Caregiver Programhelps to keep people in their homes. In response to the question “If thevolunteer program was not available, how would your needs be met?”The majority of care receivers strongly agreed or agreed that their needswould be met through friends (65%) and family (66%). A small per-centage (10%) said they would move into a nursing home. However,54% identified that their needs would not be met without the VolunteerCaregiver Program. Based on these responses, somewhere between10% and 54% of the care receivers would be at risk for institutionalizationwithout this program. Rural elders such as these respondents have few
Tara Jorgenson and Gregory Sanders 65
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

living choices beyond their own home and the local nursing home. Thusthey may be more likely to seek institutional care than urban elders withsimilar care needs. While not directly reflecting a choice between stay-ing in their own home or institutionalization, 60% agree with the state-ment that “the Volunteer Caregiver Program played a part in theirdecision to stay in their home.” Cavanaugh and Nordhus (1998) foundthat care receivers often felt a loss of independence, which can “strikedeeply for many older adults.” While the care receivers were gettingvolunteer help, it is likely that their sense of independence was stillhigher than it would be with institutional care. With the high cost of in-stitutional care, it seems apparent that this type of program has both apersonal and financial benefit.
Limitations of Study
The following are limitations of this study:
1. The study of the Volunteer Caregiver Program was based in ruralNorth Dakota. Applicability of findings is limited due to the loca-tion of the program (rural areas). Urban care receivers’ needs differfrom rural care receivers’ needs (Salmon, Nelson & Rous, 1993).
2. Applicability to other populations is also limited due to the partic-ular demographic group of volunteers studied. The demographicgroup represented was white and over the age of 35 (73% wasover the age of 65). A number of researchers have studied racialand ethnic differences in support needs and use of formal and in-formal supports (Carlton-LaNey, 1992; Hays & George, 2002;Hornung, Eleazer, Strothers, Wieland, Eng, McCann, & Sapir,1998; Miner, 1995). This research should be carefully consideredin adapting this type of program to a more diverse audience.
Implications for Program Planning
The following implications for the Volunteer Caregiver Program arerecommended based on the current study:
1. The Volunteer Caregiver Program would benefit from increasingpublicity, utilizing methods recognized by all three groups. Thesemethods include contacting senior citizen centers and churches,and developing a pamphlet for community leaders to distribute tothose individuals that may benefit from this program either as care
66 ACTIVITIES, ADAPTATION & AGING
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

recipients or volunteers. A special effort to attract younger volun-teers through mechanisms such as university service learning proj-ects may expand the volunteer pool and provide excellent experi-ence to tomorrow’s caregivers.
2. The Volunteer Caregiver Program would benefit from recogniz-ing the volunteer caregivers’ specific skills. This process wouldallow the volunteer caregivers to utilize those skills through thevolunteer experience. To increase activity, the Volunteer Care-giver Program could allow volunteer caregivers to utilize theirlearned skills through volunteering. For example, a volunteer whowas employed as a secretary may have more learned budgetingskills than would a volunteer who was employed as a carpenter,which may result in a more positive volunteer experience and anincreased life satisfaction.
3. Consider gathering family member information from care receiversand allowing the family members to be an increased part of this ex-perience. This program could mail (annually, semi-annually, monthly,etc.) newsletters informing them of the program and the servicesthat are available to their relative. Gathering family member infor-mation from the care receivers would allow future Volunteer Care-giver Program studies to have increased involvement from familymembers, allowing an additional viewpoint on how well the pro-gram is meeting the needs of care recipients.
4. This program should continue to be studied both to gain an under-standing of how such programs evolve over time and to get a lon-gitudinal perspective on volunteers and care receivers who partici-pate in this type of program.
5. Explore care receivers’ feeling of loss of independence in this pro-gram as compared to an institutional population. Results of such astudy might demonstrate another strength of the current programbut may also suggest the need for additional supports. The resultsmay imply, for example, that it would be valuable to provide carereceivers more opportunities to also be volunteers thus experienc-ing the program as more of an exchange than a dependency.
6. This program could provide more extensive training for volun-teers, especially targeted to build skills in areas of currently unmetneeds. Volunteers already skilled in these specific areas mightalso be sought out.
The present study found the Volunteer Caregiver Program to be ef-fective in providing informal support to care receivers. Volunteer care-
Tara Jorgenson and Gregory Sanders 67
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

givers prefer to provide service as a sense of helping others, socialinteraction, and a means for communication with others. The majorityof care receivers are in need of assistance that is not available from fam-ily members due to distance, other family obligations, or health. Thesetypes of programs would seem to be particularly relevant to rural areaswhere distance and lack of resources may create gaps in available sup-ports that enhance the quality of life for elders and prevent prematureplacement in long-term care institutions.
REFERENCES
Bagby, B. H. (1993, Spring). Elder care: Where families and businesses meet. Journalof Home Economics, 12-16.
Blieszner, R., McAuley, W. J., Newhouse, J. K., & Mancini, J. A. (1987). Rural-urbandifferences in service use by older adults. In T. H. Brubaker (Ed.), Aging, health,and family: Long-term care (pp. 162-174). Newbury Park, CA: Sage Publications.
Carlton-LaNey, I. (1992). Elderly Black farm women: A population at risk. SocialWork, 37, 517-523.
Cavanaugh, J. C., & Nordhus, I. H. (Eds.). (1998). Friendships and social networks amongolder people. Clinical Geropsychology. Baltimore, MD: United Book Press, Inc.
Ellefson, K. A. (2001). An evaluation of the Richland County Volunteer Caregiver Ex-change Program. The North Dakota Journal of Human Services, 3, 14-23.
Hayghe, H. V. (1991). Volunteers in the US: Who donates the time? Monthly LaborReview, 114, 17-23.
Hays, J. C. & George, L. K. (2002). The life course trajectory toward living alone: Ra-cial differences. Research on Aging, 24, 283-307.
Herlitz, C. (1997). Distribution of informal and formal home help for elderly people inSweden. Gerontologist, 37, 117-125.
Herzog, A. R., & House, J. S. (1991). Productive activities and aging well. Genera-tions, 15, 49-54.
Hornung, C. A., Eleazer, G. P., Strothers, H. S III, Wieland, G. D, Eng, C., McCann,R., & Sapir, M. (1998). Ethnicity and decision-makers in a group of frail older peo-ple. Journal of the American Geriatrics Society, 46, 280-286.
Huston, P. G. (1990). Family care of the elderly and caregiver stress. American FamilyPhysician, 42, 671-677.
Miner, S. (1995). Racial differences in family support and formal service utilizationamong older persons: A nonrecursive model. Journals of Gerontology: Series B:Psychological Sciences and Social Sciences, 50, S143-S153.
Piercy, K. W., & Blieszner, R. (1999). Balancing family life: How adult children linkelder-care responsibility to service utilization. Journal of Applied Gerontology, 18,440-459.
Salmon, M. P., Nelson, G. M., & Rous, S. G. (1993). The continuum of care revisited:A rural perspective. The Gerontological Society of America, 33, 658-666.
68 ACTIVITIES, ADAPTATION & AGING
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4

Sanders, G. F., & Bratteli, M. J. (1994). Aging North Dakota: A profile of older adults.University of North Dakota, Resource Center on Gerontology: Grand Forks.
Stephens, S. A., & Christianson, J. B. (1986). Informal care of the elderly. Boston,MA: Lexington Books.
Wheeler, J. A., Gorey, K. M., & Greenblatt, B. (1998). The benefit effects of volunteer-ing for older volunteers and the people they serve: A meta-analysis. The Interna-tional Journal of Aging & Human Development, 47, 69-79.
Zarit, S. H., Johansson, L., Jarrott, S. E., & Nordhus, I. H. (Eds.). (1998). Familycaregiving: Stresses, social programs, and clinical interventions. Clinical Geropsychology.Baltimore, MD: United Book Press, Inc.
RECEIVED: 09/02REVISED: 01/03
ACCEPTED: 01/03
Tara Jorgenson and Gregory Sanders 69
For FACULTY/PROFESSIONALS with journal subscriptionrecommendation authority for their institutional library . . .
Please send me a complimentary sample of this journal:
(please write complete journal title here–do not leave blank)
If you have read a reprint or photocopy of this article, would you like tomake sure that your library also subscribes to this journal? If you havethe authority to recommend subscriptions to your library, we will send youa free complete (print edition) sample copy for review with your librarian.
1. Fill out the form below and make sure that you type or write out clearly both the nameof the journal and your own name and address. Or send your request via e-mail [email protected] including in the subject line “Sample Copy Request”and the title of this journal.
2. Make sure to include your name and complete postal mailing address as well as yourinstitutional/agency library name in the text of your e-mail.
[Please note: we cannot mail specific journal samples, such as the issue in which a specific article appears.Sample issues are provided with the hope that you might review a possible subscription/e-subscription withyour institution's librarian. There is no charge for an institution/campus-wide electronic subscriptionconcurrent with the archival print edition subscription.]
I will show this journal to our institutional or agency library for a possible subscription.Institution/Agency Library: ______________________________________________
Name: _____________________________________________________________
Institution: __________________________________________________________
Address: ___________________________________________________________
City: ____________________Return to: Sample Copy Department,The Haworth Press, Inc.,
10 Alice Street, Binghamton, NY 13904-1580
State: __________ Zip: ____________________
Dow
nloa
ded
by [
Uni
vers
ity o
f W
est F
lori
da]
at 1
2:30
09
Oct
ober
201
4