a systematic review and meta-analysis of randomized...
TRANSCRIPT

Review – Neuro-urology
A Systematic Review and Meta-Analysis of RandomizedControlled Trials with Antimuscarinic Drugs for OveractiveBladder
Giacomo Novara a, Antonio Galfano b, Silvia Secco b, Carolina D’Elia b,Stefano Cavalleri b, Vincenzo Ficarra b, Walter Artibani b,*a I.R.C.C.S. Istituto Oncologico Veneto (I.O.V.), Padova, ItalybDepartment of Oncological and Surgical Sciences, Urology Clinic, University of Padua, Italy
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4
avai lable at www.sc iencedi rect .com
journal homepage: www.europeanurology.com
Article info
Article history:Accepted June 25, 2008Published online ahead ofprint on July 9, 2008
Keywords:Overactive bladder
Urgency frequency syndrome
Detrusor overactivity
Muscarinic receptor antagonist
Darifenacin
Emepronium
Fesoterodine
Oxybutynin
Propantheline
Propiverine
Solifenacin
Tolterodine
Trospium
Please visit
www.eu-acme.org/
europeanurology to read and
answer questions on-line.
The EU-ACME credits will
then be attributed
automatically.
Abstract
Context: Anticholinergic drugs are commonly used in patients with overactive bladder
(OAB) who do not achieve symptom relief and quality of life improvement with
conservative management. Several drugs, with different doses, formulations, and
routes of administration are currently available, making the choice quite difficult.
Objective: To evaluate efficacy and safety of different doses, formulations, and route of
administration of the available anticholinergic drugs.
Evidence acquisition: A systematic review of the literature was performed in August
2007 using Medline, Embase, and Web of Science. Efficacy (micturitions per 24 h,
volume voided per micturition, urgency urinary incontinence episodes per 24 h,
incontinence episodes per 24 h) and safety (mainly, adverse events and withdrawal
rates) end points were evaluated in the randomized control trials (RCTs) assessing the
role of anticholinergic drugs in non-neurogenic OAB. Meta-analysis of RCTs was
conducted using the Review Manager software 4.2 (Cochrane Collaboration).
Evidence synthesis: Our systematic search identified 50 RCTs and three pooled ana-
lyses. Tolterodine immediate release (IR) had a more favorable profile of adverse
events than oxybutynin IR. Regarding different dosages of IR formulations, dose
escalation might yield some limited improvements in the efficacy but at the cost of
significant increase in the rate of adverse events. In the comparisons between IR and
extended-release (ER) formulations, the latter showed some advantages, both in terms
of efficacy and safety. With regard to the route of administration, use if a transdermal
route of administration does not provide significant advantage over an oral one.
Conclusion: Many of the available RCTs have good methodological quality. ER formu-
lations should be preferred to the IR ones. With regard to IR formulations, dose
escalation might yield some improvements in the efficacy with significant increase
in the AE. More clinical studies are needed to indicate which of the drugs should be
used as first-, second-, or third-line treatment.
# 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved.
* Corresponding author. Department of Oncological and Surgical Sciences, Urology Clinic,University of Padua, Monoblocco Ospedaliero, IV Floor, Via Giustiniani 2, 35128, Padua, Italy.Tel. +39 049 8212720; Fax: +39 049 8218757.E-mail address: [email protected] (W. Artibani).
0302-2838/$ – see back matter # 2008 European Association of Urology. Published by Elsevier B.V. All rights reserved. doi:10.1016/j.eururo.2008.06.080

Fig. 1 – Flow-chart of meta-analysis. RCTs, randomized control trials, OAB, overactive bladder.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 741
1. Introduction
Overactive bladder (OAB) is a highly prevalentcondition [1,2] with enormous related costs per year[3,4]. First-line treatments for OAB include lifestylemodifications, behavioral therapy, pelvic floormuscle training, and bladder training. Antimuscari-nic drugs are the first-line drug therapy, while othertherapeutic options, such as botulinum toxin injec-tion, neuromodulation, or surgical interventions areused in a smaller percentage of patients who arenon-responders to drug therapies [5,6].
Several antimuscarinic drugs are on the market,including oxybutynin, tolterodine, propiverine,trospium, the recently released solifenacin anddarifenacin, and fesoterodine, which was the lastone to receive the European Medicines EvaluationAgency (EMEA) marketing authorization in 2006.Moreover, some drugs such as oxybutynin, tolter-odine, propiverine, or trospium are available both inimmediate-release (IR) and extended-release (ER)formulations, while oxybutynin is also available in asustained-delivery patch for transdermal adminis-tration [7]. Two meta-analyses evaluated the effi-cacy of the anticholinergic drugs in comparison toplacebo, showing that the use of these drugs resultsin statistically significant improvements in symp-toms and quality of life [8,9]. To date, however, theclinical data available on the active comparisons ofdifferent drugs, formulations, and routes of admin-istration are more limited. Specifically, a Cochranemeta-analysis based on a systematic review per-formed in January 2002 demonstrated that tolter-
odine was as effective as, but better tolerated than,oxybutynin; moreover, ER formulations of oxybu-tynin and/or tolterodine were shown to cause alower risk of dry mouth compared to the IRformulations. Comparing head-to-head the ERformulations, xerostomia was less common inthose patients receiving tolterodine [10]. In a morerecent meta-analysis which mainly focused onplacebo-controlled trials, Chapple et al reportedsome data on the trials of drugs which providedactive drug controls. Solifenacin was shown to bemore effective than tolterodine IR in terms ofreduction of both urgency episodes and numberof micturitions, while oxybutynin ER was shown tobe more effective than tolterodine ER, in terms ofreduction of incontinence episodes. Finally, oxybu-tynin IR 15 mg once daily, solifenacin 5 mg oncedaily, and solifenacin 10 mg once daily were moreeffective than tolterodine IR in increasing thevolume voided per micturitions [8].
The purpose of the present systematic reviewand meta-analysis was to evaluate all the clinicaldata derived from randomized controlled trials inorder to assess the efficacy and safety of differentdoses, formulations, and routes of administrationof the currently available anticholinergic drugs, aswell as head-to-head comparisons of differentdrugs.
2. Methods
The systematic review of the literature was performed in
August 2007 using the Medical Literature Analysis and

Table 1 – Efficacy data from the randomized control trials (RCTs) comparing different doses and formulations of oxybutynin, tolterodine, propiverine, trospium,solifenacin, darifenacin, and fesoterodine
Reference Dose (no. of cases) Treatmentduration
Jadadscore
Mean changein daytime
micturitionsper 24 h
Mean changein nighttimemicturitions
per 24 h
Mean changein micturitions
per 24 h
Mean change involume voided permicturitions (ml)
Mean change inurgency episodes
per 24 h
Mean changein UUI episodes
per 24 h
Mean changein incontinence
episodes per 24 h
Mean changein pads used
per 24 h
Oxybutynin
Nilsson et al 1997 [13] Oxy IR 5 mg bid (17) 8 wk 1 NR NR �2.8 (24%) NR NR NR NR NR
Oxy ER 10 mg qd (16) �2.6 (23%)
Versi et al 2000 [14] Oxy IR different doses (115) variable �3 NR NR NR NR NR �0.6 (76%) �0.7 (75%) NR
Oxy ER different doses (111) �0.4 (83%) �0.5 (81%)
Barkin et al 2004 [15] Oxy IR different doses (41) 6 wk �3 NR NR �2.4 (22%) +40 (18%) �1.3 (41%) NR �2.41 (73%) �0.5 (21%)
Oxy ER different doses (53) �1.8 (16%) +25 (14%) �1.0 (30%) �1.81 (54%) �0.6 (26%)
Corcos et al 2005 [16] Oxy ER 5 mg qd (77) 4 wk �3 NR NR �0.8 (7%) +17.1 (8%) �1.8 (37%) NR NR NR
Oxy ER 10 mg qd (77) �1.1 (11%) +20.5 (10%) �1.5 (34%)
Oxy ER 15 mg qd (83) �1.5 (14%) +44.6 (21%) �2.0 (46%)
Propiverine
Junemann et al 2006 [17] Propi IR 15 mg bid (395) 4 wk 1 NR NR �3.69 (29%) +46.5 ml (32.6%) �2.03 (33%) NR �2.21 (67%) NR
Propi ER 30 mg qd (391) �3.63 (28%) +40.1 ml (27.9%) �2.58 (40%) �2.47 (73%)
Tolterodine
Jonas et al 1997 [18] Tolt IR 1 mg bid (99) 4 wk �3 NR NR �1.4 (12%) +20 ml* NR NR �1.1* NR
Tolt IR 2 mg bid (99) �1.7 (15%) +20 ml* �1.6*
Rentzhog et al 1998 [19] Tolt IR 0.5 mg bid (21) 2 wk 1 NR NR �1.0 (10%) +15%* NR NR �0.7 (35%) 10%*
Tolt IR 1 mg bid (16) �1.1 (10%) +25%* �0.6 (37%) 10%*
Tolt IR 2 mg bid (14) �2.5 (20%) +30%* �0.8 (46%) 29%*
Tolt IR 4 mg bid (16) �2.0 (20%) +30%* �1.6 (60%) 40%*
Millard et al 1999 [20] Tolt IR 1 mg bid (123) 12 wk 1 NR NR �2.3 (20%) +27 (18%) NR �1.7 (44%) NR NR
Tolt IR 2 mg bid (129) �2.3 (20%) +36 (23%) �1.7 (47%)
Jacquetin et al 2001 [21] Tolt IR 1 mg bid (97) 4 wk 1 NR NR �1.4 (13%) +20 (13%) NR �1.1 (41%) NR NR
Tolt IR 2 mg bid (103) �1.4 (13%) +19 (12%) �1.3 (41%)
Malone-Lee et al 2001 [22] Tolt IR 1 mg bid (61) 4 wk �3 NR NR �0.7 (6%) +9 (6%) NR �0.3 (13%) NR NR
Tolt IR 2 mg bid (73) �0.7 (6%) +16 (11%) �0.7 (25%)
Van Kerrebroeck et al 2001 [23] Tolt IR 2 mg bid (514) 12 wk �3 NR NR �1.7 (15%) +29 (21%) NR NR �1.51 (46%) �0.5 (36%)
Tolt ER 4 mg qd (507) �1.8 (16%) +34 (24%) �1.68 (53%) �0.5 (36%)
Swift et al 2003 [24] Tolt IR 2 mg bid (408) 12 wk �3 NR NR �1.7 (15%) +32 (24%) NR NR �1.44 (44%) �0.5 (33%)
Tolt ER 4 mg qd (417) �1.9 (17%) +37.9 (27%) �1.68 (53%) �0.6 (37%)
Solifenacin
Cardozo et al 2004 [25] Soli 5 mg qd (286) 12 wk 2 NR �0.56 (25.3%) �2.37 (20%) +30.75* �2.84 (25%) �1.3 (63%) �1.63 (61%) NR
Soli 10 mg qd (290) �0.71 (38.5%) �2.81 (22%) +35.99* �2.90 (30%) �1.2 (57%) �1.57 (52%)
Chapple et al 2004 [26] Soli 5 mg qd (264) 12 wk 2 NR NR �2.19 (17%) +32.9 (25%) �2.85 (52%) �1.41 (65%) �1.42 (59%) NR
Soli 10 mg qd (261) �2.61 (20%) +39.2 (29%) �3.07 (55%) �1.36 (63%) �1.45 (47%)
Chapple et al 2006** [27] Soli 5 mg qd (552) 12 wk NA NR �0.6* �2.3* +32.3* �2.9* NR �1.5* NR
Soli 10 mg qd (1158) �0.6* �2.7* +42.5* �3.4* �1.8*
Darifenacin
Chapple et al 2005** [28] Dari 7.5 mg qd (337) 12 wk NA NR NR �1.6 (17%) +15 (10%) �2.0 (29%) NR �4.0 (77%) NR
Dari 15 mg qd (334) �1.9 (17%) +27 (17%) �2.3 (29%) �4.8 (79%)
Foote et al 2005** [29] Dari 7.5 mg qd (97) 12 wk NA NR NR �1.8 (18%) +14 (10%) �2.1 (26%) NR �1.6 (67%) NR
Dari 15 mg qd (110) �1.8 (17%) +27 (18%) �2.4 (26%) �1.5 (76%)
Zinner et al 2005 [30] Dari 15 mg qd (58) 2 wk 2 NR NR �1.14 (12%) NR �1.27 (16%) NR �1.44 (92%) NR
Dari 30 mg qd (58) �1.62 (18%) �1.63 (21%) �1.74 (138%)
Hill et al 2006 [31] Dari 7.5 mg qd (108) 12 wk �3 NR NR �1.7 (17%) +17 (10%) �1.8 (29%) NR �1.15 (69%) NR
Dari 15 mg qd (107) �1.9 (18%) +24 (16%) �2.3 (27%) �1.48 (76%)
Dari 30 mg qd (115) �2.2 (21%) +44 (26%) �3.0 (33%) �1.62 (77%)
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
74
0–
76
47
42

Ta
ble
1(C
onti
nu
ed)
Refe
ren
ceD
ose
(no
.o
fca
ses)
Tre
atm
en
td
ura
tio
nJa
da
dsc
ore
Mea
nch
an
gein
da
yti
me
mic
turi
tio
ns
per
24
h
Mea
nch
an
ge
inn
igh
ttim
em
ictu
riti
on
sp
er
24
h
Mea
nch
an
gein
mic
turi
tio
ns
per
24
h
Mea
nch
an
ge
inv
olu
me
vo
ided
per
mic
turi
tio
ns
(ml)
Mea
nch
an
ge
inu
rgen
cyep
iso
des
per
24
h
Mea
nch
an
gein
UU
Iep
iso
des
per
24
h
Mea
nch
an
gein
inco
nti
nen
ceep
iso
des
per
24
h
Mea
nch
an
ge
inp
ad
su
sed
per
24
h
Feso
tero
din
e
Nit
tiet
al
2005
[32]
Feso
4m
gq
d(4
4)
8w
k2
NR
NR
�0.9
96
*+
27.9
4*
NR
NR
NR
NR
Feso
8m
gq
d(4
7)
�1.8
15
*+
58.6
9*
Feso
12
mg
(39)
�1.7
84
*+
92.3
4*
Ch
ap
ple
et
al
2007
[33]
Feso
4m
gq
d(2
72)
12
wk
�3
�1.3
7(1
4%
)�
0.3
9(2
9%
)�
1.7
6(1
7%
)+
27.7
2(1
7%
)�
1.8
8(1
8%
)�
1.9
5(8
0%
)N
RN
R
Feso
8m
gq
d(2
88)
�1.4
8(1
7%
)�
0.3
9(2
3%
)�
1.8
8(1
9%
)+
33.6
2(2
2%
)�
2.3
6(1
9%
)�
2.2
2(8
7%
)
Nit
tiet
al
2007
[34]
Feso
4m
g(2
83)
12
wk
�3
�1.0
4(1
0%
)�
0.5
8(2
6%
)�
1.6
1(1
2%
)+
16.5
(11%
)�
1.9
1(1
5%
)�
1.6
5(4
2%
)N
RN
R
Feso
8m
g(2
79)
�1.5
4(1
5%
)�
0.5
5(2
9%
)�
2.0
9(1
7%
)+
33.6
(21%
)�
2.3
(20%
)�
2.2
8(5
9%
)
*Ba
seli
ne
va
lues
no
tp
rov
ided
inth
ep
ub
lish
ed
ma
nu
scri
pt;
**p
oo
led
an
aly
sis
of
RC
Ts;
NR
:n
ot
rep
ort
ed
;N
A,
no
ta
pp
lica
ble
;q
d,
on
ced
ail
y;
bid
,tw
ice
da
ily
.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 743
Retrieval System Online (U.S. National Library of Medicine’s
life science database; MEDLINE), the Excerpta Medica database
(EMBASE), and Thomson-Reuters’ Web of Science. The MED-
LINE search employed a complex search strategy, including
both ‘‘MeSH’’ (Medical Subject Heading) and ‘‘free text’’
protocols. Specifically, the MeSH search was conducted by
combining the following terms retrieved from the MeSH
browser provided by MEDLINE: ‘‘urinary bladder, overactive’’
and ‘‘cholinergic antagonists’’. Multiple free-text searches
were performed applying singularly the following terms
through all the fields of the records: overactive bladder,
detrusor overactivity, bladder overactivity, urgency frequency
syndrome, darifenacin, emepronium, fesoterodine, oxybuty-
nin, propantheline, propiverine, solifenacin, tolterodine, and
trospium. Subsequently, the searches were pooled and limited
to randomized controlled trials (RCTs). No temporal limits
were used.
Searches on EMBASE and Web of Science used only the
free-text protocol, with the same key words. Subsequently, the
queries were pooled without applying any limits. In addition,
other significant studies cited in the reference lists of the
selected papers were considered.
Three of the authors individually reviewed all the abstracts
of the retrieved studies in order to select the papers that were
relevant to the review topic. Specifically, all the full-test
studies including data of efficacy (changes in daytime
micturitions in 24 h, nighttime micturitions in 24 h, micturi-
tions in 24 h, volume voided per micturitions, urgency,
episodes in 24 h, urge urinary incontinence [UUI] episodes
in 24 h, incontinence episodes in 24 h, pads used per 24 h,
quality of life scores) and complications (overall rates of
adverse events, withdrawals due to adverse events, dry mouth
rate, moderate-to-severe or severe dry mouth rate, constipa-
tion, acute urinary retention, vision abnormality, headache,
etc) of anticholinergic drugs comparing different drugs,
formulations, doses, and routes of administration were
considered. Data were extracted separately and indepen-
dently by two of the authors and were cross-checked.
Moreover, the web site of the Food and Drug Administra-
tion (http://www.fda.gov) was searched for RCTs concerning
the same drugs.
The quality of all the retrieved RCTs was assessed using the
Jadad score [11]. All the identified RCTs were included in the
meta-analysis, regardless of the quality score.
Meta-analysis was conducted using the Review Manager
software version 4.2 (The Cochrane Collaboration, Oxford,
UK). Specifically, statistical heterogeneity was tested using the
chi-square test. A p value <0.10 was used to indicate
heterogeneity. In case of lack of heterogeneity, fixed-effects
models were used for the meta-analyses. Random-effects
models were used in case of heterogeneity. The results were
expressed as weighted means and standard deviations for
continuous outcomes and relative risk for dichotomous
variables. Only the RCTs presenting data in this format were
included in the meta-analysis. All the authors whose studies
presented the data in a format not suitable for the meta-
analysis were contacted and asked for the missing figures, but
only three authors provided useful data. The presence of
publication bias was evaluated using a funnel plot [12].
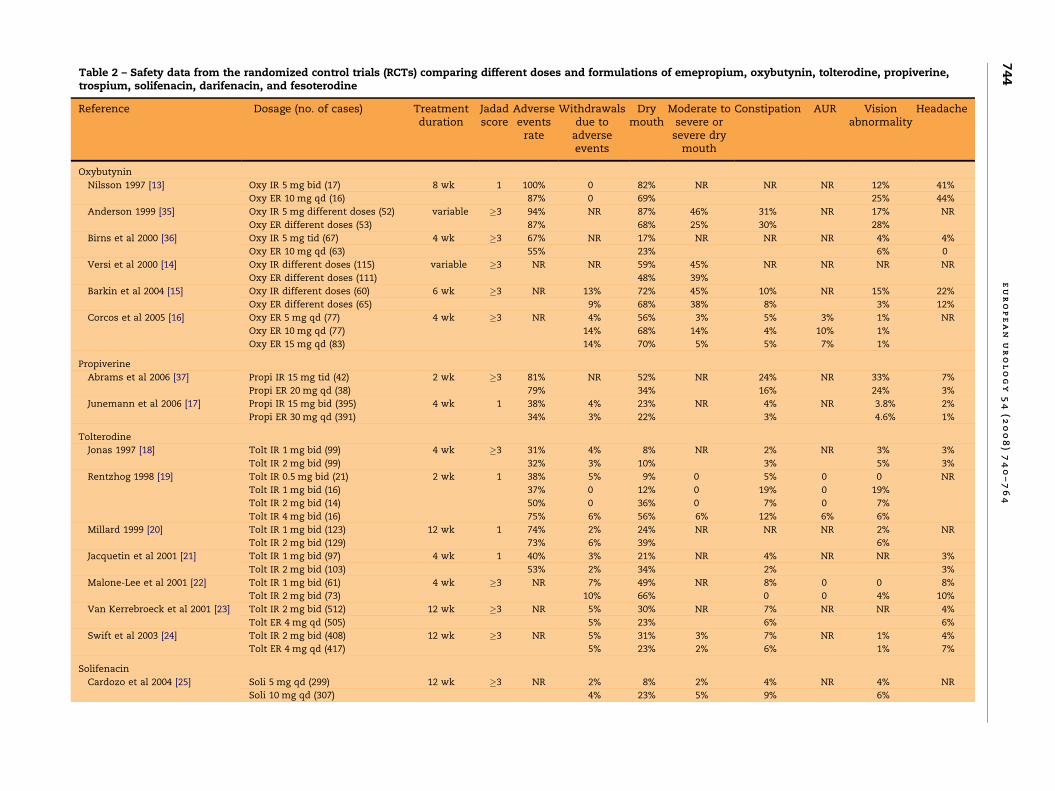
Table 2 – Safety data from the randomized control trials (RCTs) comparing different doses and formulations of emepropium, oxybutynin, tolterodine, propiverine,trospium, solifenacin, darifenacin, and fesoterodine
Reference Dosage (no. of cases) Treatmentduration
Jadadscore
Adverseevents
rate
Withdrawalsdue to
adverseevents
Drymouth
Moderate tosevere or
severe drymouth
Constipation AUR Visionabnormality
Headache
Oxybutynin
Nilsson 1997 [13] Oxy IR 5 mg bid (17) 8 wk 1 100% 0 82% NR NR NR 12% 41%
Oxy ER 10 mg qd (16) 87% 0 69% 25% 44%
Anderson 1999 [35] Oxy IR 5 mg different doses (52) variable �3 94% NR 87% 46% 31% NR 17% NR
Oxy ER different doses (53) 87% 68% 25% 30% 28%
Birns et al 2000 [36] Oxy IR 5 mg tid (67) 4 wk �3 67% NR 17% NR NR NR 4% 4%
Oxy ER 10 mg qd (63) 55% 23% 6% 0
Versi et al 2000 [14] Oxy IR different doses (115) variable �3 NR NR 59% 45% NR NR NR NR
Oxy ER different doses (111) 48% 39%
Barkin et al 2004 [15] Oxy IR different doses (60) 6 wk �3 NR 13% 72% 45% 10% NR 15% 22%
Oxy ER different doses (65) 9% 68% 38% 8% 3% 12%
Corcos et al 2005 [16] Oxy ER 5 mg qd (77) 4 wk �3 NR 4% 56% 3% 5% 3% 1% NR
Oxy ER 10 mg qd (77) 14% 68% 14% 4% 10% 1%
Oxy ER 15 mg qd (83) 14% 70% 5% 5% 7% 1%
Propiverine
Abrams et al 2006 [37] Propi IR 15 mg tid (42) 2 wk �3 81% NR 52% NR 24% NR 33% 7%
Propi ER 20 mg qd (38) 79% 34% 16% 24% 3%
Junemann et al 2006 [17] Propi IR 15 mg bid (395) 4 wk 1 38% 4% 23% NR 4% NR 3.8% 2%
Propi ER 30 mg qd (391) 34% 3% 22% 3% 4.6% 1%
Tolterodine
Jonas 1997 [18] Tolt IR 1 mg bid (99) 4 wk �3 31% 4% 8% NR 2% NR 3% 3%
Tolt IR 2 mg bid (99) 32% 3% 10% 3% 5% 3%
Rentzhog 1998 [19] Tolt IR 0.5 mg bid (21) 2 wk 1 38% 5% 9% 0 5% 0 0 NR
Tolt IR 1 mg bid (16) 37% 0 12% 0 19% 0 19%
Tolt IR 2 mg bid (14) 50% 0 36% 0 7% 0 7%
Tolt IR 4 mg bid (16) 75% 6% 56% 6% 12% 6% 6%
Millard 1999 [20] Tolt IR 1 mg bid (123) 12 wk 1 74% 2% 24% NR NR NR 2% NR
Tolt IR 2 mg bid (129) 73% 6% 39% 6%
Jacquetin et al 2001 [21] Tolt IR 1 mg bid (97) 4 wk 1 40% 3% 21% NR 4% NR NR 3%
Tolt IR 2 mg bid (103) 53% 2% 34% 2% 3%
Malone-Lee et al 2001 [22] Tolt IR 1 mg bid (61) 4 wk �3 NR 7% 49% NR 8% 0 0 8%
Tolt IR 2 mg bid (73) 10% 66% 0 0 4% 10%
Van Kerrebroeck et al 2001 [23] Tolt IR 2 mg bid (512) 12 wk �3 NR 5% 30% NR 7% NR NR 4%
Tolt ER 4 mg qd (505) 5% 23% 6% 6%
Swift et al 2003 [24] Tolt IR 2 mg bid (408) 12 wk �3 NR 5% 31% 3% 7% NR 1% 4%
Tolt ER 4 mg qd (417) 5% 23% 2% 6% 1% 7%
Solifenacin
Cardozo et al 2004 [25] Soli 5 mg qd (299) 12 wk �3 NR 2% 8% 2% 4% NR 4% NR
Soli 10 mg qd (307) 4% 23% 5% 9% 6%
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
74
0–
76
47
44

Table 2 (Continued )
Reference Dosage (no. of cases) Treatmentduration
Jadadscore
Adverseevents
rate
Withdrawalsdue to
adverseevents
Drymouth
Moderate tosevere or
severe drymouth
Constipation AUR Visionabnormality
Headache
Chapple et al 2004 [26] Soli 5 mg qd (279) 12 wk �3 NR 3% 14% NR 7% NR 4% NR
Soli 10 mg qd (268) 3% 21% 8% 6%
Chapple et al 2006* [27] Soli 5 mg qd (552) 12 wk �3 91% 3% 11% 0.2% 5% NR 4% NR
Soli 10 mg qd (1158) 87% 7% 28% 1% 13% 5%
Darifenacin
Chapple et al 2005* [28] Dari 7.5 mg qd (337) 12 wk NA 54% 1% 20% NR 15% NR NR 4%
Dari 15 mg qd (334) 66% 5% 35% 21% 5%
Foote et al 2005* [29] Dari 7.5 mg qd (97) 12 wk NA 54% 1% 21% NR 19% NR NR 0
Dari 15 mg qd (110) 69% 9% 31% 24% 0
Zinner et al 2005 [30] Dari 15 mg qd (76) 2 wk 2 NR 0 13% NR 10% NR 0 NR
Dari 30 mg qd (76) 1% 34% 21% 0
Hill et al 2006 [31] Dari 7.5 mg qd (108) 12 wk �3 57% 0 23% NR 16% NR 2% 6%
Dari 15 mg qd (107) 68% 2% 40% 25% 0 6%
Dari 30 mg qd (115) 80% 4% 59% 59% 3% 6%
Fesoterodine
Nitti et al 2005 [32] Feso 4 mg qd (43) 8 wk 2 NR 2% 37% 14% NR NR NR NR
Feso 8 mg qd (47) 4% 43% 21%
Feso 12 mg (38) 13% 63% 13%
Chapple et al 2007 [33] Feso 4 mg (272) 12 wk �3 50% 3% 22% NR 3% 0.3% 2% 4%
Feso 8 mg (282) 58% 5% 34% 4% 1% 4% 2%
Nitti et al 2008 [34] Feso 4 mg (283) 12 wk �3 61% 6% 16% NR 5% 1% 0.7% 4%
Feso 8 mg (279) 69% 9 36% 8% 2% 3% 3%
* Pooled analysis of RCTs; NA, not applicable; qd, once daily; bid, twice daily; tid, three times daily; NR, not reported.
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
74
0–
76
47
45
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4746
3. Results
984 records were retrieved by searching MEDLINE:910 records were retrieved from EMBASE, and 669records were retrieved from Web of Science. Thestudies evaluating lower urinary tract storagesymptoms in patients with bladder-outlet obstruc-tions, papers evaluating neurogenic OAB or OAB inchildren, phase I studies, post-hoc analyses of RCTs,and duplicate publications were excluded. Wefinally identified 50 RCTs and three pooled analysesof RCTs for inclusion in this review (Fig. 1).
3.1. Comparisons of different doses and formulations of
the same drug
Tables 1 and 2 summarize the efficacy and safetydata from the available RCTs comparing different
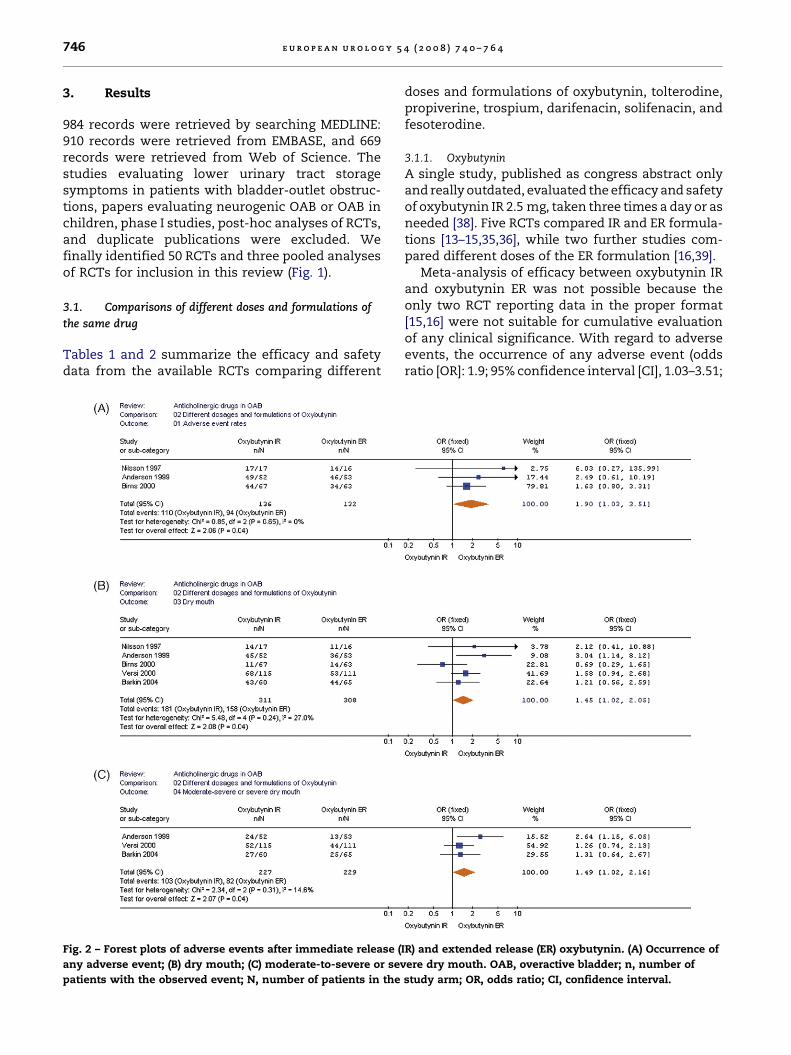
Fig. 2 – Forest plots of adverse events after immediate release (
any adverse event; (B) dry mouth; (C) moderate-to-severe or sev
patients with the observed event; N, number of patients in the
doses and formulations of oxybutynin, tolterodine,propiverine, trospium, darifenacin, solifenacin, andfesoterodine.
3.1.1. Oxybutynin
A single study, published as congress abstract onlyand really outdated, evaluated the efficacy and safetyof oxybutynin IR 2.5 mg, taken three times a day or asneeded [38]. Five RCTs compared IR and ER formula-tions [13–15,35,36], while two further studies com-pared different doses of the ER formulation [16,39].
Meta-analysis of efficacy between oxybutynin IRand oxybutynin ER was not possible because theonly two RCT reporting data in the proper format[15,16] were not suitable for cumulative evaluationof any clinical significance. With regard to adverseevents, the occurrence of any adverse event (oddsratio [OR]: 1.9; 95% confidence interval [CI], 1.03–3.51;
IR) and extended release (ER) oxybutynin. (A) Occurrence of
ere dry mouth. OAB, overactive bladder; n, number of
study arm; OR, odds ratio; CI, confidence interval.

Table 3 – Meta-analysis of adverse events with oxybutynin immediate release (IR) and oxybutynin extended release (ER)
Oxybutynin IR vs oxybutynin ER RCT(no.)
Participants(no.)
OR 95% CI,OR
Test foroverall effect
(p value)
Difference favors
Any adverse event 3 268 1.9 1.03–3.51 0.04 Oxybutynin ER
Withdrawals due to adverse events 2 158 1.51 0.49–4.65 0.47 None
Dry mouth 5 619 1.45 1.02–2.05 0.04 Oxybutynin ER
Moderate-to-severe or severe dry mouth 3 456 1.49 1.02–2.16 0.04 Oxybutynin ER
Headache 3 288 1.77 0.84–3.72 0.13 None
Constipation 2 230 1.11 0.56–2.22 0.76 None
Vision abnormality 4 393 0.92 0.50–1.69 0.79 None
RCT, randomized control trial; IR, immediate release; ER, extended release; OR, odds ratio; CI, confidence interval.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 747
p = 0.04), dry mouth (OR: 1.45; 95% CI, 1.02–2.05;p = 0.04), and moderate-to-severe or severe drymouth (OR: 1.49; 95 CI, 1.02–2.16; p = 0.04) weresignificantly more common with oxybutynin IR(Fig. 2). On the other hand, withdrawals due toadverse events, headache, constipation, and visionabnormality were similar for the two formulationsof oxybutynin (Table 3).
3.1.2. Tolterodine
Eight RCTs compared different doses and formula-tions of tolterodine. Specifically, four studiescompared two different dosages of tolterodine IR1 mg twice daily vs tolterodine IR 2 mg twice daily[18,20–22], while a further study evaluated fourdifferent dosages (0.5 mg twice daily vs 1 mg twicedaily vs 2 mg twice daily vs 4 mg twice daily) [19].Two RCTs compared tolterodine IR 2 mg twice dailyand tolterodine ER 4 mg once daily [23,24], while asingle study compared two dosages of tolterodineER [39].
Table 4 – Meta-analysis of randomized control trials (RCTs) comextended release (ER)
Tolterodine IR vstolterodine ER
RCT (no.) Participants (no.)
Micturitions per 24 h 2 1846
Volume voided per micturition 2 1846
Incontinence episodes per 24 h 2 1846
Pad use per 24 h 2 1846
Adverse events RCT (no.) Participants (no.) O
Withdrawals due to
adverse events
2 1846 0.
Dry mouth 2 1846 1.
Headache 2 1846 0.
Constipation 2 1846 1.
IR, immediate release; ER, extended release; UUI, urgency urinary inconti
odds ratio.
With regard to efficacy analysis, four paperspresented the data in a format unsuitable formeta-analysis [18,19,22,39]. Comparing the tolter-odine IR 1 mg and tolterodine IR 2 mg doses,micturitions per 24 h (weighted mean difference[WMD], 0.11; 95% CI, �0.45–0.66; p = 0.70), volumevoided per micturition (WMD,�8.68; 95% CI,�18.62–1.26; p = 0.09), and UUI episodes per 24 h (WMD,�0.06; 95% CI, �0.51–0.39; p = 0.81) were similar forboth doses. With regard to adverse events, only drymouth was significantly more frequent in thosepatients taking tolterodine IR 2 mg (OR: 0.52; 95% CI,1.037–0.72; p < 0.0001).
Regarding the comparison of tolterodine IR andtolterodine ER formulations, patients randomized totolterodine ER formulation experienced a lowernumber of micturitions per 24 h (WMD, 0.34; 95%CI, 0.02–0.66; p = 0.03) and a higher volume voidedper micturition (WMD, �9.12; 95% CI, �14.13–�4.12;p = 0.0004), but a similar number of incontinenceepisodes and pad use per day (Table 4). Evaluating
paring tolterodine immediate release (IR) and tolterodine
WMD 95% CI, WMD Test foroverall effect
( p value)
Difference favors
0.34 0.02–0.66 0.03 Tolterodine ER
�9.12 �14.13–4.12 0.0004 Tolterodine ER
0.09 �0.15–0.32 0.46 None
0 �0.15–0.15 1 None
R 95% CI, OR Test foroverall effect
( p value)
Difference favors
98 0.65–1.48 0.92 None
39 1.13–1.71 0.002 Tolterodine ER
53 0.34–0.81 0.004 Tolterodine IR
10 0.76–1.59 0.63 None
nence; WMD, weighted mean difference; CI, confidence interval; OR,

Fig. 3 – Forest plots of efficacy and safety after tolterodine immediate release (IR) and tolterodine extended release (ER). (A)
Micturitions per 24 h; (B) volume voided per micturition; (C) dry mouth; (D) headache. OAB, overactive bladder; N, number of
patients in the study arm; SD, standard deviation; WMD, weighted-mean difference; CI, confidence interval.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4748
the adverse events with the use of the twoformulations of tolterodine, patients treated withtolterodine ER formulations had a significantlylower rate of dry mouth (OR: 1.39; 95% CI, 1.13–1.71; p = 0.002) but a higher rate of headache (OR:0.53; 95% CI, 0.34–0.81; p = 0.004). Withdrawals due to
Fig. 4 – Forest plots of adverse events after different dosages of
15 mg: (A) Occurrence of any adverse event; (B) withdrawals du
Darifenacin 15 mg versus darifenacin 30 mg: (E) dry mouth; (F) co
with the observed event; N, number of patients in the study ar
adverse events and constipation were similarlyprevalent in both cases (Table 4; Fig. 3).
3.1.3. Propiverine
A single study evaluated the efficacy of 21-dtreatment with different doses of propiverine IR
darifenacin (Dari). Darifenacin 7.5 mg versus darifenacin
e to adverse events; (C) dry mouth; (D) constipation.
nstipation. OAB, overactive bladder; n, number of patients
m; OR, odds ratio; CI, confidence interval.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 749

Table 5 – Meta-analysis of adverse events with immediate-release (IR) and extended-release (ER) formulations ofpropiverine
Propiverine IR vspropiverine ER
RCT (no.) Participants (no.) OR 95% CI, OR Test foroverall effect
( p value)
Differencefavors
Any adverse event 2 866 1.20 0.90–1.58 0.21 None
Dry mouth 2 866 1.16 0.84–1.58 0.36 None
Headache 2 866 1.54 0.59–4.02 0.38 None
Constipation 2 866 1.29 0.69–2.41 0.42 None
Vision abnormality 2 866 1.95 0.89–4.02 0.10 None
RCT, randomized control trial; OR, odds ratio; CI, confidence interval.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4750
(15 mg twice daily vs 30 mg twice daily vs 45 mgthree times daily vs 60 mg four times daily), showingthat propiverine IR 15 mg twice daily and 30 mgtwice daily were the doses with the most favorableratio of efficacy in micturition frequency to toler-ability [40].
Two studies compared propiverine hydrochlorideIR and propiverine hydrochloride ER formulations[17,37].
Meta-analysis was possible only for complicationrates, in spite of the different dosages of propiverineIR of in the two studies. The two formulations ofpropiverine showed similar rates of adverse events,dry mouth, constipation, headache, and visionabnormality (Table 5).
3.1.4. Solifenacin
Four RCTs evaluated the efficacy of different dosesof solifenacin [25,26,41,42]. The two studies byGittelman et al [41,42] were not included inTables 1 and 2 because it was not possible to obtainthe data in an extended form. Three pooled analysesof these four RCTs sharing similar designs werepublished [27,43,44]. The largest analysis, whichalso included the patients without UUI, evaluated2848 patients out of 3032 randomized patients:552 patients received solifenacin 5 mg, 1158 patientsreceived solifenacin 10 mg, and 1138 patientsreceived placebo [27]. Both doses of solifenacin weresignificantly more efficacious than placebo. Indeed,comparing the two dosages, solifenacin 10 mg wassignificantly better only in terms of the percentageof patients having a�50% reduction in incontinenceepisodes ( p = 0.006). However, withdrawals due toadverse events ( p = 0.0005), dry mouth ( p < 0.0001),and constipation ( p < 0.0001) were significantlymore common among the patients treated bysolifenacin 10 mg [27].
3.1.5. Darifenacin
Our systematic search identified two RCTs evaluat-ing the efficacy of darifenacin at different doses[30,31] and two pooled analyses of RCTs [28,29],
which, however, failed to clearly report the includedtrials. The larger studies evaluated 337 patientsrandomized to receive darifenacin 7.5 mg and334 patients who received darifenacin 15 mg. Theanalysis identified significant dose–response effectsfor change in weekly incontinence episodes [28]. Thestudy from Foote et al [29] was a subgroup analysis ofthe patients aged�65 yr in Chapple et al [28] and wasnot evaluated in our analyses.
Meta-analysis of efficacy between the differentdoses of darifenacin was not possible because all thestudies reported the data in a format that was notsuitable for the evaluation. With regard to adverseevents, darifenacin 7.5 mg was followed by signifi-cantly lower rates of adverse events (OR: 0.62; 95%CI, 0.47–0.81; p = 0.0005), withdrawals due to adverseevents (OR: 0.30; 95% CI, 0.11–0.80; p = 0.02), drymouth (OR: 0.46; 95% CI, 0.34–0.62; p < 0.0001), andconstipation (OR: 0.62; 95% CI, 0.44–0.87; p = 0.006),compared with darifenacin 15 mg. Similarly, com-paring darifenacin 15 mg and darifenacin 30 mg,darifenacin 15 mg was followed by significantlylower rates of dry mouth (OR: 0.40; 95% CI, 0.26–0.63; p < 0.0001) and constipation (OR: 0.27; 95% CI,0.16–0.44; p < 0.0001; Table 6; Fig. 4).
3.1.6. Fesoterodine
Three RCTs compared different doses of fesoter-odine, the most recently released anticholinergicdrug [32–34]. With regard to efficacy analysis, thethree papers presented the data in a formatunsuitable for meta-analysis. Regarding adverseevents, adverse event rate (OR: 0.68; 95% CI, 0.53–0.87; p = 0.002), dry mouth (OR: 0.46; 95% CI, 0.36–0.60; p < 0.0001) and vision abnormality (OR: 0.38;95% CI, 0.17–0.86; p = 0.02) were more common inthose patients receiving fesoterodine 8 mg (Table 7).
3.2. Comparisons of different drugs
Tables 8 and 9 summarize the efficacy and safetydata from the available RCTs comparing differentdrugs.

Table 7 – Meta-analysis of adverse events with different doses of fesoterodine
Fesoterodine 4 mg vsfesoterodine 8 mg
RCT (no.) Participants (no.) OR 95% CI, OR Test foroverall effect
(p value)
Difference in favor of
Any adverse event 2 1116 0.68 0.53–0.87 0.002 Fersoterodine 4 mg
Withdrawal due to adverse event 3 1211 0.60 0.36–1 0.05 None
Dry mouth 3 1211 0.46 0.36–0.60 <0.0001 Fersoterodine 4 mg
Constipation 2 1116 0.67 0.39–1.15 0.15 None
Headache 2 1116 1.66 0.86–3.20 0.13 None
Vision abnormality 2 1116 0.38 0.17–0.86 0.02 Fersoterodine 4 mg
Acute urinary retention 2 1116 0.62 0.20–1.92 0.41 None
RCT, randomized control trial; OR, odds ratio; CI: confidence interval.
Table 6 – Meta-analysis of adverse events with different doses of darifenacin
RCT (no.) Participants (no.) OR 95% CI, OR Test foroverall effect
( p value)
Difference in favor
Darifenacin 7.5 mg vs darifenacin 15 mg
Any adverse event 2 886 0.62 0.47–0.81 0.0005 Darifenacin 7.5 mg
Withdrawal due to adverse event 2 886 0.30 0.11–0.80 0.02 Darifenacin 7.5 mg
Dry mouth 2 886 0.46 0.34–0.62 <0.0001 Darifenacin 7.5 mg
Headache 2 886 0.90 0.50–1.64 0.74 None
Constipation 2 886 0.62 0.44–0.87 0.006 Darifenacin 7.5 mg
Darifenacin 15 mg vs darifenacin 30 mg
Withdrawal due to adverse event 2 374 0.40 0.09–1.74 0.22 None
Dry mouth 2 374 0.40 0.26–0.63 <0.0001 Darifenacin 15 mg
Constipation 2 374 0.27 0.16–0.44 <0.00001 Darifenacin 15 mg
RCT, randomized control trial; OR, odds ratio; CI, confidence interval; NR, not reported.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 751
3.2.1. Oxybutynin versus tolterodine
Twelve RCTs compared efficacy and safety ofoxybutynin and tolterodine [45–54,62,63]. Specifi-cally, eight of these studies compared the IRformulations of the two drugs (oxybutynin 5 mgtwo or three times daily vs tolterodine 2 mg twicedaily) [45–47,49,50,53,62,63].
With regard to the comparisons of the IR formula-tions, only four RCTs provided the data in a formatsuitable for meta-analysis of the efficacy data[47,49,50,53]. Micturitions per 24 h, volume voidedper micturition, UUI episodes, and incontinenceepisodes per 24 h were overlapping for the IRformulations of the two drugs. Regarding adverseevents, occurrence of any adverse event (OR: 2.30;95% CI, 1.70–3.11; p � 0.00001), withdrawal due toadverse events (OR:1.82; 95% CI, 1.33–2.49; p = 0.0002),dry mouth of any grade (OR: 3.98; 95% CI, 3.16–5.02;p � 0.00001), and moderate-to-severe or severe drymouth (OR: 7.21; 95% CI, 4.50–11.52; p � 0.00001)were significantly more common in those patientsreceiving oxybutynin IR (Table 10 and Fig. 5).
A single trial compared oxybutynin ER to tolter-odine IR [48]. After a 12-wk treatment, oxybutynin ERwas shown to be more efficacious than tolterodineIR in terms of reduction in urgency incontinence
episodes ( p = 0.03), total incontinence episodes( p = 0.02), and micturitions ( p < 0.0001), while allthe evaluated adverse events (overall number, drymouth, constipation, blurred vision, headache) wereoverlapping in the two arms [48].
Two further RCTs compared oxybutynin IR andtolterodine ER [52,54]. The larger study, whichenrolled 608 patients with OAB, showed similarefficacy for both drugs in terms of reductions in thenumber of incontinence episodes per week andmicturitions per day, but patients taking oxybutyninIR more frequently experienced dry mouth, severedry mouth, and eye disorders [52]. Similar figureswere provided in the RCT from Homma et al [54]. Theformat used in these two studies to report efficacydata was unsuitable for meta-analysis. With regardto adverse events, dry mouth (OR: 2.44; 95% CI, 1.80–3.30; p < 0.00001) and severe dry mouth (OR: 16.87;95% CI, 3.23–87.95; p = 0.0008) were significantlymore common with the IR formulation of oxybuty-nin.
Finally, a single study compared the formulationsof oxybutynin ER and tolterodine ER [51]. After a12-wk treatment, the average number of weekly UUIepisodes, which was the primary end point of thestudy, was overlapping between the two arms, as

Table 8 – Efficacy data from the randomized control trials (RCTs) comparing different drugs
Reference Dose (no. of cases) Treatmentduration
Jadadscore
Mean changein daytime
micturitionsper 24 h
Mean changein nighttimemicturitions
per 24 h
Mean change inmicturitions
per 24 h
Mean changein VV per
micturitions(ml)
Mean changein urgencyepisodesper 24 h
Mean changein UUI
episodesper 24 h
Mean change inincontinence
episodesper 24 h
Meanchange inpads usedper 24 h
Oxybutynin vs tolterodine
Van Kerrebroeck 1997 [45] Oxy IR 5 mg tid (120) 12 wk 1 NR NR �2.7 * +54 * NR NR NR NR
Tolt IR 2 mg bid (120) �2.1 * +35 *
Abrams et al 1998 [46] Oxy IR 5 mg tid (118) 12 wk �3 NR NR �2.3 (19%) +47 (31%) NR NR �1.7 (71%) NR
Tolt IR 2 mg bid (118) �2.7 (21%) +38 (27%) �1.3 (47%)
Drutz et al 1999 [47] Oxy IR 5 mg tid (112) 12 wk �3 NR NR �2.0 (17%) +50 (33%) NR NR �1.7 (50%) NR
Tolt IR 2 mg bid (109) �2.0 (17%) + 34 (22%) �1.7 (46%)
Appell et al 2001 [48] Oxy ER 10 mg qd(185) 12 wk �3 NR NR �3.5 (27%) NR NR �2.78 (76%) �3.07 (75%) NR
Tolt IR 2 mg bid(193) �2.8 (22%) �2.32 (68%) �2.52 (65%)
Malone–Lee et al 2001 [49] Oxy IR 5 mg bid (188) 10 wk �3 NR NR �1.7 (15%) +34 (23%) NR �1.8 (62%) NR �0.9 (32%)
Tolt IR 2mg bid (190) �1.7 (15%) +33 (22%) �1.3 (54%) �1.1 (35%)
Lee et al 2002 [50] Oxy IR 5 mg bid (116) 8 wk �3 NR NR �1.8 (15%) NR NR NR �1.4 (67%) NR
Tolt IR 2 mg bid (112) �2.6 (20%) �2.2 (76%)
Diokno et al 2003 [51] Oxy ER 10 mg qd (391) 12 wk �3 NR NR �3.75 (28%) NR NR �3.82 (72%) �4.5 (73%) NR
Tolt ER 4 mg qd (399) �3.42 (25%) �3.42 (65%) �4.2 (69%)
Homma et al 2003 [52] Oxy IR 3 mg tid (246) 12 wk �3 NR NR �2.0 (18%) +22.3 (18%) NR NR NR 0
Tolt ER 4 mg qd (240) �2.1 (17%) +17.2 (14%) 0
Giannitsas et al 2004 [53] Oxy IR 5 mg tid (107) 6+6 wk
(crossover)
�3 NR NR �0.8 (9%) +43.8 (22%) NR NR NR NR
Tolt IR 2 mg bid (107) �0.9 (10%) +40.6 (21%)
Homma et al 2004 [54] Oxy IR 3 mg tid (122) 12 wk �3 NR NR 19.1%* +22 * NR NR 87% * NR
Tolt ER 4 mg qd (114) 17.9%* +12.6 * 86% *
Oxybutynin vs propiverine
Madersbacher et al 1999 [55] Oxy IR 5 mg bid (121) 4 wk 2 NR NR �1.6 (13%) NR �3 (24%) NR NR NR
Propi 15 mg tid (126) �1.9 (18%) �3.1 (33%)
Oxybutynin vs trospium
Halaska et al 2003 [56] Oxy IR 5 mg bid (90) 52 wk �3 NR NR �4.2 (34%) NR �3.6 (33%) NR NR NR
Trospium 20 mg bid (267) �3.5 (31%) �3.5 (34%)
Oxybutynin vs darifenacin
Zinner et al 2005 [30] Oxy IR 5 mg tid (58) 2 wk �3 NR NR �1.23 (13%) NR �1.1 (13%) NR �1.65 (122%) NR
Dari 15 mg qd (58) �1.14 (12%) �1.27 (16%) �1.44 (92%)
Dari 30 mg qd (58) �1.62 (18%) �1.63 (21%) �1.74 (138%)
Tolterodine vs trospium
Junemann et al 2000 [57] Tolt IR 2 mg bid (60) 3 wk 1 NR NR �2.6* NR NR NR NR NR
Trospium IR 20 mg bid (57) �3.4*
Tolterodine vs propiverine
Junemann et al 2005 [58] Tolt IR 2 mg bid (101) 4 wk 2 NR NR �3.07* +28.43 * �3.04* NR �0.91* �0.43*
Propi 15 mg bid (100) �2.75* +31.76 * �3.26* �1.2* �0.65*
Tolterodine vs solifenacin
Chapple et al 2004 [26] Tolt IR 2 mg bid (250) 12 wk �3 NR NR �1.88 (15%) +24.4 (20%) �2.05 (38%) �0.91 (58%) �1.14 (59%) NR
Soli 5 mg qd (264) �2.19 (17%) +32.9 (25%) �2.85 52%) �1.41 (65%) �1.42 (59%)
Soli 10 mg qd (261) �2.61 (20%) +39.2 (29%) �3.07 (55%) �1.36 (63%) �1.45 (47%)
Chapple et al 2005 [59] Tolt ER 4 mg qd (599) 12 wk �3 NR �0.63 (33%) �2.24 (19%) +31 (21%) �2.42 (41%) �0.83 (39%) �1.11 (43%) �1.19 (41%)
Soli 5/10 mg qd (578) �0.71 (35%) �2.45 (21%) +38 (26%) �2.85 (47%) �1.42 (61%) �1.6 (58%) �1.72 (53%)
Chapple et al 2007 [60] Tolt ER 4 mg qd (599) 4 wk �3 NR �0.44 (23%) �1.47 (13%) +24.3 (17%) �1.67 (29%) �0.91 (43%) �0.90 (42%) �0.80 (27%)
Soli 5 mg qd (578) �0.51 (23%) �1.71 (14%) +28.5 (19%) �1.98 (33%) �1.22 (53%) �1.30 (53%) �1.21 (37%)
Tolterodine vs fesoterodine
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
74
0–
76
47
52

Ta
ble
8(C
onti
nu
ed)
Refe
ren
ceD
ose
(no
.o
fca
ses)
Tre
atm
en
td
ura
tio
nJa
da
dsc
ore
Mea
nch
an
gein
da
yti
me
mic
turi
tio
ns
per
24
h
Mea
nch
an
ge
inn
igh
ttim
em
ictu
riti
on
sp
er
24
h
Mea
nch
an
ge
inm
ictu
riti
on
sp
er
24
h
Mea
nch
an
ge
inV
Vp
er
mic
turi
tio
ns
(ml)
Mea
nch
an
ge
inu
rgen
cyep
iso
des
per
24
h
Mea
nch
an
ge
inU
UI
ep
iso
des
per
24
h
Mea
nch
an
ge
inin
con
tin
en
ceep
iso
des
per
24
h
Mea
nch
an
ge
inp
ad
su
sed
per
24
h
Ch
ap
ple
et
al
2007
[33]
To
ltE
R4
mg
qd
(290)
12
wk
�3
�1.3
5(1
4%
)�
0.4
(25%
)�
1.7
3(1
4%
)+
23.6
4(1
5%
)�
2.0
3(1
6%
)�
1.7
4(7
0%
)N
RN
R
Feso
4m
gq
d(2
72)
�1.3
7(1
4%
)�
0.3
9(2
9%
)�
1.7
6(1
7%
)+
27.7
2(1
7%
)�
1.8
8(1
8%
)�
1.9
5(8
0%
)
Feso
8m
g(2
88)
�1.4
8(1
7%
)�
0.3
9(2
3%
)�
1.8
8(1
9%
)+
33.6
2(2
2%
)�
2.3
6(1
9%
)�
2.2
2(8
7%
)
VV
,v
oid
ed
vo
lum
e;
UU
I,u
rge
uri
na
ryin
con
tin
ence
;Q
D,
on
ced
ail
y;
BID
,tw
ice
da
ily
;T
ID,
thre
eti
mes
da
ily
;N
R,
no
tre
po
rted
.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 753
well as the number of incontinence episodes of anytype. Indeed, patients taking oxybutynin ER had agreater decrease in the mean weekly micturitionfrequency compared with tolterodine ER partici-pants ( p = 0.003). Regarding adverse events, theoccurrence of dry mouth was significantly lesscommon in the patients randomized to tolterodineER ( p = 0.02), although in most of the cases it was ofmild degree [51].
3.2.2. Oxybutynin versus propantheline
Two studies compared oxybutynin IR 5 mg threetimes daily and propantheline 15 mg three timesdaily [61,64]. The larger study evaluated 154 patients,63 patiented receiving the oxybutynin dosage and54 patients receiving the propantheline dosage. Thepropantheline arm showed a higher mean grade ofimprovements in visual analogue scale, counter-balanced by higher rate of adverse events in theoxybutynin arm [61]. The data from the two studieswere unsuitable for meta-analysis.
3.2.3. Oxybutynin versus propiverine
Two studies compared oxybutynin with propiverine[55,65]. In the larger study, the two drugs weresimilarly effective in terms of both bladder diaryvariables and urodynamic parameters, although drymouth and severe dry mouth were less frequent inthe propiverine arm [55].
3.2.4. Oxybutynin versus trospium
A single trial compared efficacy and safety ofoxybutynin IR 5 mg twice daily and trospium IR20 mg twice daily [56]. This study is of particularclinical relevance because the treatments werecontinued for 52 wk. This study showed similarefficacy for the two drugs in terms of both bladderdiary variables such as mean change in micturitionsand in the number of of urgency episodes per 24 h,and in terms of urodynamic parameters, such aschange in maximum cystometric capacity andchange in volume at first contraction. The occur-rence of any adverse event ( p = 0.045) and dryness ofthe mouth ( p = 0.021) were significantly less com-mon in those patients receiving trospium [56].
3.2.5. Oxybutynin versus darifenacin
Zinner et al evaluated the efficacy of oxybutynin IRand darifenacin in a four-way crossover study [30].With regard to efficacy, darifenacin 15 mg once dailywas comparable to oxybutynin in terms of theimprovement in OAB symptoms, with both drugssimilarly reducing the number of incontinenceepisodes per week and the number of micturitionsand urgency episodes per day after a 2-wk treat-

Table 9 – Safety data from the randomized control trials (RCTs) comparing different drugs
Reference Dose (no. of cases) Treatmentduration
Jadadscore
Adverseevents rate
Withdrawal dueto adverse events
Drymouth
Moderate-to-severeor severe dry mouth
Headache Constipation AUR Visionabnormality
Oxybutynin vs propantheline
Thuroff et al 1991 [61] Oxy IR 5 mg tid (63) 4 wk 1 63% 3% 48% 27% 1% 3% NR 3%
Propantheline 15 mg tid (54) 44% 5% 31% 18% 5% 0 4%
Oxybutynin vs tolterodine
Van Kerrebroeck et al 1997 [45] Oxy IR 5 mg tid (120) 12 wk 1 93% 21% 78% 23% NR NR NR NR
Tolt IR 2 mg bid (120) 63% 11% 38% 3%
Abrams et al 1998 [46] Oxy IR 5 mg tid (118) 12 wk �3 97% 17% 86% NR NR NR NR NR
Tolt IR 2 mg bid (118) 89% 8% 50%
Drutz et al 1999 [47] Oxy IR 5 mg tid (112) 12 wk �3 90% 21% 69% 44% 10% NR NR NR
Tolt IR 2 mg bid (109) 78% 6% 30% 9% 15%
Appell et al 2001 [48] Oxy ER 10 mg qd (185) 12 wk �3 NR 8% 28% NR 8% 7% 3% 2%
Tolt IR 2 mg bid (193) 8% 33% 9% 6% 3% 1%
Malone-Lee et al 2001 [49] Oxy IR 5 mg bid (188) 10 wk �3 81% 15% 61% 15% 10% 6% NR 5%
Tolt IR 2mg bid (190) 69% 12% 37% 4% 11% 8% 5%
Lee et al 2002 [50] Oxy IR 5 mg bid (116) 8 wk �3 NR 16% 63% 28% 5%. NR NR NR
Tolt IR 2 mg bid (112) 10% 35% 9% 4%
Leung et al 2002 [62] Oxy IR5 mg bid (53) 10 wk �3 49% 15% NR NR NR NR NR NR
Tolt IR 2 mg bid (53) 60% 17%
Diokno et al 2003 [51] Oxy ER 10 mg qd (391) 12 wk �3 NR 5% 30% 7% 6% 6% NR NR
Tolt ER 4 mg qd (399) 5% 22% 5% 6% 8%
Homma et al 2003 [52] Oxy IR 3 mg tid (244) 12 wk �3 NR 17% 54% 8% 4% 6% 3% 3%
Tolt ER 4 mg qd (239) 5% 33% 0.4% 4% 7% 0.4% 1%
Homma et al 2004 [54] Oxy IR 3 mg tid (122) 12 wk �3 NR NR 61% 3% NR NR NR NR
Tolt ER 4 mg qd (114) 37% 0
Altan-Yacioglu et al 2005 [63] Oxy IR 5 mg tid (24) 4 wk 2 NR NR 83% 83% NR NR NR 58%
Tolt IR 2 mg bid (28) 50% 28% 43%
Oxybutynin vs propiverine
Madersbacher et al 1999 [55] Oxy IR 5 mg bid (145) 4 wk 2 72% NR NR NR NR NR NR 18%
Propi 15 mg tid (149) 64% 27%
Abrams et al 2006 [37] Oxy IR 5 mg tid (41) 2 wk �3 93% NR 83% NR 15% 10% NR 22%
Propi 15 mg tid (42) 81% 52% 7% 24% 33%
Propi 20 mg qd (38) 79% 34% 0 16% 24%
Oxybutynin vs trospium
Halaska et al 2003 [56] Oxy IR 5 mg bid (90) 52 wk �3 77% 7% 50% NR 9% NR NR 6%
Trospium 20 mg bid (267) 68% 4% 33% 4% 3%
Oxybutynin vs darifenacin
Zinner et al 2005 [30] Oxy IR 5 mg tid (76) 2 wk �3 NR 5% 36% NR NR 8% NR 3%
Dari 15 mg qd (76) 0 13% 10% 0
Dari 30 mg qd (76) 1% 34% 21% 0
Tolterodine vs trospium
Junemann et al 2000 [37] Trospium IR 20 mg bid (76) 3 wk 1 34% NR 29% NR NR NR NR NR
Tolt IR 2 mg bid (77) 32% 27%
Tolterodine vs propiverine
Junemann et al 2005 [58] Tolt IR 2 mg bid (101) 4 wk 2 43% 6% 19% NR NR NR NR 7%
Propi 15 mg bid (100) 42% 6% 20% 9%
Tolterodine vs solifenacin
Chapple et al 2004 [26] Tolterodine IR 2 mg bid (263) 12 wk �3 NR 2% 19% NR NR 3% NR 1%
Soli 5 mg qd (279) 3% 14% 7% 4%
Soli 10 mg qd (268) 3% 22% 8% 6%
eu
ro
pe
an
ur
ol
og
y5
4(2
00
8)
74
0–
76
47
54

Ta
ble
9(C
onti
nu
ed)
Refe
ren
ceD
ose
(no
.o
fca
ses)
Tre
atm
en
td
ura
tio
nJa
da
dsc
ore
Ad
vers
eev
en
tsra
teW
ith
dra
wa
ld
ue
toa
dv
ers
eev
en
tsD
rym
ou
thM
od
era
te-t
o-s
ev
ere
or
sev
ere
dry
mo
uth
Hea
dach
eC
on
stip
ati
on
AU
RV
isio
na
bn
orm
ali
ty
Ch
ap
ple
et
al
2005
[59]
To
ltE
R4
mg
qd
(599)
12
wk
�3
NR
3%
24%
1%
NR
2%
NR
2%
So
li5/1
0m
gq
d(5
78)
3%
30%
2%
6%
1%
Ch
ap
ple
et
al
2007
[60]
To
ltE
R4
mg
qd
(607)
4w
k�
33%
3%
15%
NR
NR
1%
NR
NR
So
li5
mg
qd
(593)
3%
3%
18%
3%
To
ltero
din
ev
sfe
sote
rod
ine
Ch
ap
ple
et
al
2007
[33]
To
ltE
R4
mg
qd
(290)
12
wk
�3
50%
3%
17%
NR
5%
3%
00.3
%
Feso
4m
gq
d(2
72)
50%
3%
22%
4%
3%
0.3
%2.2
%
Feso
8m
gq
d(2
82)
58%
5%
34%
2%
4%
1%
4%
NR
,n
ot
rep
ort
ed
;q
d,
on
ced
ail
y;
bid
,tw
ice
da
ily
;ti
d,
thre
eti
mes
da
ily
.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 755
ment. Concerning adverse events, dry mouth wassignificantly more common in the oxybutynin armthan in the darifenacin 15 mg arm ( p < 0.05), whileoverlapping rates occurred between the oxybutynin30 mg and darifenacin 30 mg arms. On the otherhand, constipation was significantly more frequentin those patients treated by darifenacin 30 mg, but itoccurred in similar percentages in the oxybutynin15 mg arm and the darifenacin 15 mg arm [30].
3.2.6. Tolterodine versus trospium
A single RCT, published as congressional abstract,compared tolterodine IR 2 mg twice daily andtrospium IR 20 mg twice daily. The study showedsimilar efficacy and similar adverse event rates forthe two drugs [57]. The lack of a publication in apeer-reviewed journal does not permit the evalua-tion of the power of the statistical analysis for thecomparisons between tolterodine and trospium.
3.2.7. Tolterodine versus propiverine
A single study compared tolterodine IR 2 mg bid andpropiverine 15 mg bid [58]. The study showed similarefficacy for the two drugs in terms of both bladderdiary variables such as mean change in micturitions,number of UUI episodes per 24 h, and number ofincontinence episodes per 24 h and in terms ofurodynamic parameters, such as change in max-imum cystometric capacity and change in volume atfirst contraction. Similarly, the number of adverseevents was comparable in both treatment groups[58].
3.2.8. Tolterodine versus solifenacin
Two studies reported data on the comparisonsbetween solifenacin and tolterodine [26,59,60]. Thefirst study, designed for the registration of solife-nacin, compared solifenacin 5-mg and solifenacin10-mg to tolterodine IR 2 mg twice daily or placebo[26]. However, the most interesting data came fromthe STAR study, whose primary end point tested thenon-inferiority of solifenacin compared to toltero-dine ER [59]. Solifenacin 5 mg and solifenacin10 mgwere not inferior to tolterodine ER with regard tochange from baseline in the following ways: meannumber of micturitions per 24 h ( p = 0.004 for non-inferiority), reduction in number of urgency epi-sodes per day ( p < 0.05), urge incontinence episodesper day ( p < 0.01), incontinence episodes per day( p < 0.01), and pad usage ( p < 0.002). Dry mouth( p = 0.02) and constipation ( p = 0.002) were signifi-cantly more common in the solifenacin arm,although they were mainly of mild or moderateseverity [59]. A secondary analysis of the same trialwas recently published, limiting all the evaluation
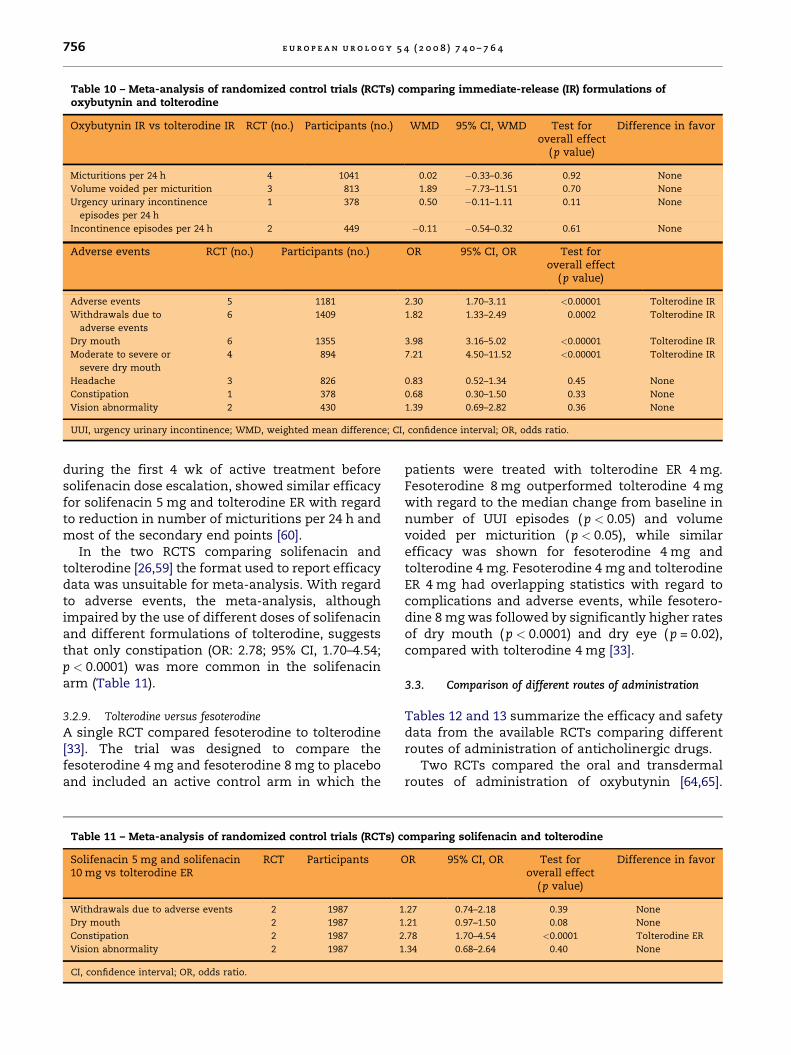
Table 10 – Meta-analysis of randomized control trials (RCTs) comparing immediate-release (IR) formulations ofoxybutynin and tolterodine
Oxybutynin IR vs tolterodine IR RCT (no.) Participants (no.) WMD 95% CI, WMD Test foroverall effect
(p value)
Difference in favor
Micturitions per 24 h 4 1041 0.02 �0.33–0.36 0.92 None
Volume voided per micturition 3 813 1.89 �7.73–11.51 0.70 None
Urgency urinary incontinence
episodes per 24 h
1 378 0.50 �0.11–1.11 0.11 None
Incontinence episodes per 24 h 2 449 �0.11 �0.54–0.32 0.61 None
Adverse events RCT (no.) Participants (no.) OR 95% CI, OR Test foroverall effect
( p value)
Adverse events 5 1181 2.30 1.70–3.11 <0.00001 Tolterodine IR
Withdrawals due to
adverse events
6 1409 1.82 1.33–2.49 0.0002 Tolterodine IR
Dry mouth 6 1355 3.98 3.16–5.02 <0.00001 Tolterodine IR
Moderate to severe or
severe dry mouth
4 894 7.21 4.50–11.52 <0.00001 Tolterodine IR
Headache 3 826 0.83 0.52–1.34 0.45 None
Constipation 1 378 0.68 0.30–1.50 0.33 None
Vision abnormality 2 430 1.39 0.69–2.82 0.36 None
UUI, urgency urinary incontinence; WMD, weighted mean difference; CI, confidence interval; OR, odds ratio.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4756
during the first 4 wk of active treatment beforesolifenacin dose escalation, showed similar efficacyfor solifenacin 5 mg and tolterodine ER with regardto reduction in number of micturitions per 24 h andmost of the secondary end points [60].
In the two RCTS comparing solifenacin andtolterodine [26,59] the format used to report efficacydata was unsuitable for meta-analysis. With regardto adverse events, the meta-analysis, althoughimpaired by the use of different doses of solifenacinand different formulations of tolterodine, suggeststhat only constipation (OR: 2.78; 95% CI, 1.70–4.54;p < 0.0001) was more common in the solifenacinarm (Table 11).
3.2.9. Tolterodine versus fesoterodine
A single RCT compared fesoterodine to tolterodine[33]. The trial was designed to compare thefesoterodine 4 mg and fesoterodine 8 mg to placeboand included an active control arm in which the
Table 11 – Meta-analysis of randomized control trials (RCTs) c
Solifenacin 5 mg and solifenacin10 mg vs tolterodine ER
RCT Participants
Withdrawals due to adverse events 2 1987 1
Dry mouth 2 1987 1
Constipation 2 1987 2
Vision abnormality 2 1987 1
CI, confidence interval; OR, odds ratio.
patients were treated with tolterodine ER 4 mg.Fesoterodine 8 mg outperformed tolterodine 4 mgwith regard to the median change from baseline innumber of UUI episodes ( p < 0.05) and volumevoided per micturition ( p < 0.05), while similarefficacy was shown for fesoterodine 4 mg andtolterodine 4 mg. Fesoterodine 4 mg and tolterodineER 4 mg had overlapping statistics with regard tocomplications and adverse events, while fesotero-dine 8 mg was followed by significantly higher ratesof dry mouth ( p < 0.0001) and dry eye ( p = 0.02),compared with tolterodine 4 mg [33].
3.3. Comparison of different routes of administration
Tables 12 and 13 summarize the efficacy and safetydata from the available RCTs comparing differentroutes of administration of anticholinergic drugs.
Two RCTs compared the oral and transdermalroutes of administration of oxybutynin [64,65].
omparing solifenacin and tolterodine
OR 95% CI, OR Test foroverall effect
( p value)
Difference in favor
.27 0.74–2.18 0.39 None
.21 0.97–1.50 0.08 None
.78 1.70–4.54 <0.0001 Tolterodine ER
.34 0.68–2.64 0.40 None

Table 13 – Safety data from the randomized control trials (RCTs) comparing oral and transdermal formulations ofanticholinergic drugs
Reference Dosage (no. of cases) Treatmentduration
Jadadscore
Systemicadverseeventrate
Localizedapplication
sitereaction*
Withdrawaldue to
adverseevents
Drymouth
(%)
Constipation AUR Visionabnormality
Davila et al 2001 [64] Oxy IR 2.5 mg bid or tid (38) 4 wk �3 NR 23% NR 82% 50% 34% 24%
Oxy TDS twice a week (38) 38% 39% 21% 24% 18%
Dmochowski
et al 2003 [65]
Tolt ER 4 mg qd (123) 12 wk �3 24% 5.7% 2% 7% 6% NR NR
Oxy TDS 3.9 mg qd (121) 19% 26% 11% 4% 3%
AUR, acute urinary retention; NR, not reported; qd, once daily; bid, twice daily; tid, three timse daily.* Placebo transdermal system was used in those patients taking oral anticholinergic drugs.
Table 12 – Efficacy data from the randomized control trials (RCTs) comparing oral and transdermal formulations ofanticholinergic drugs
Reference Dosage (no. of cases) Treatmentduration
Jadad score Mean changein micturitions
per 24 h
Mean changein VV per
micturitions (ml)
Mean changein incontinence
episodes per 24 h
Davila et al 2001 [64] Oxy IR 2.5 mg bid or tid (38) 4 wk �3 NR NR �0.8 (23%)
Oxy TDS twice a week (38) �0.4 (17%)
Dmochowski et al 2003 [65] Tolt ER 4 mg qd (123) 12 wk �3 �2.2 (18%) +29 (19%) �3.2 (64%)
Oxy TDS 3.9 mg qd (121) �1.9 (15%) +32 (19%) �2.9 (62%)
VV, voided volume; NR, not reported; qd: once daily; bid: twice daily; tid: three times daily. Placebo transdermal system was used in those patients taking
oral anticholinergic drugs.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 757
Specifically, Davila et al compared the efficacy andsafety of oxybutynin IR at different doses adminis-tered orally or transdermally [65], while Dmo-chowski et al evaluated transdermal oxybutynin3.9 mg once daily and tolterodine ER 4 mg once daily[65].
Meta-analysis of efficacy showed similar reduc-tion in the number of incontinence episodes per 24 h(WMD: 0.05; 95% CI, �0.58–0.67; p = 0.88). Dry mouth(OR: 3.67; 95% CI, 1.73–7.81; p = 0.0007) and constipa-tion (OR: 2.78; 95% CI, 1.27–6.08; p = 0.01) weresignificantly more common in those patients takingthe drug orally, while localized application sideeffects (OR: 0.26; 95% CI, 0.14– 0.49; p < 0.0001) andwithdrawal due to adverse events (OR: 0.14; 95% CI,0.03–0.62; p = 0.01) were significantly more frequentin those patients receiving active transdermalformulations (Table 14; Fig. 6).
Table 14 – Meta-analysis of adverse events with oral and tran
Oral oxybutynin vs transdermaloxybutynin
RCT (no.) Participants (no.
Systemic adverse event 1 244
Localized application site reactions 2 320
Withdrawals due to adverse events 1 244
Dry mouth 2 320
Constipation 2 320
Vision abnormality 1 76
RCT, randomized control trials; OR, odds ratio; CI, confidence interval.
3.4. Publication bias
‘‘Funnel plots’’ of the studies used in this meta-analysis were generated for all of the evaluatedcomparisons. Only four studies [15,21,45,62] layoutside the 95% CI with an even distribution aroundthe vertical, suggesting little evidence of publicationbias (plots not shown).
4. Discussion
Due to the large number of drugs available on themarket, the selection of the most appropriate one forevery single patient might be quite a complex task.The choice of the first drug to be used, the selectionof the most appropriate dosage, formulation, androute of administration, the criteria for selection of a
sdermal formulations of anticholinergic drugs
) OR 95% CI, OR Test foroverall effect
( p value)
Difference favors
1.31 0.71–2.43 0.38 None
0.26 0.14–0.49 <0.0001 Oral
0.14 0.03–0.62 0.01 Oral
3.67 1.73–7.81 0.0007 Transdermal
2.78 1.27–6.08 0.01 Transdermal
1.37 0.45–4.17 0.57 None

Fig. 5 – Forest plots of adverse events after oxybutynin immediate release (IR) or tolterodine IR. (A) Occurrence of any adverse
event; (B) withdrawals due to adverse events; (C) dry mouth of any severity; (D) moderate to severe or severe dry mouth.
OAB, overactive bladder; n, number of patients with the observed event; N, number of patients in the study arm; OR, odds
ratio; CI, confidence interval.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4758

Fig. 6 – Forest plots of adverse events after oral and transdermal formulations of anticholinergic drugs. (A) Localized
application site reactions; (B) withdrawal due to adverse events; (C) dry mouth of any severity; (D) constipation. OAB,
overactive bladder; n, number of patients with the observed event; N, number of patients in the study arm; OR, odds ratio;
CI, confidence interval.
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 759
second anticholinergic drug in case of insufficientefficacy or intolerable adverse events, and, finally,costs are some of the most important issues thatshould be evaluated.
The data from our systematic review and meta-analyses showed that tolterodine IR had a morefavorable profile of adverse events than oxybutyninIR, while the ER formulations of the two drugs had
similar efficacy and safety profiles. In all thecomparisons among IR and ER formulations, thelatter showed some advantages, either in terms ofefficacy (tolterodine IR vs oxybutynin ER; tolterodineIR vs tolterodine ER) or safety (oxybutynin IR vsoxybutynin ER; oxybutynin IR vs tolterodine ER;oxybutynin IR vs darifenacin). With regard tosolifenacin, a single RCT demonstrated the non-

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4760
inferiority of solifenacin compared to tolterodine ER[59], while our meta-analysis showed similar rates ofadverse events, with the exception of constipation,which was more common in the solifenacin arm.A single trial is currently available on fesoterodine,suggesting that the new drug might be moreefficacious than tolterodine ER. With regard to theroutes of administration, the transdermal routedoes not seem to provide any significant advantagecompared to the oral intake, considering the higherrate of side effects from localized application andwithdrawal due to adverse events.
Providing clear indications for the clinicalpractice, however, is quite difficult. With regardto the selection of the first drug to use in naıvepatients, the RCTs comparing different drugs oftenenrolled a large number of patients who hadpreviously been treated with other drugs. Con-sidering this issue as a mandatory starting point,according to our data, the first drug which mightbe used in naıve patients is oxybutynin ER,tolterodine ER 4 mg, solifenacin 5 mg, or solifena-cin 10 mg. Similarly, darifenacin 15 mg and feso-terodine 4 mg might be considered as valuableoptions, but further evaluation is needed, andfurther RCTs are ongoing.
In case of insufficient clinical efficacy, the choiceof the second drug cannot really be based onevidence because, to our knowledge, no randomizedtrials were aimed at identifying the most efficientdrug in the case of lack of success with some of theother first-line choices. Making assumptions fromthe available data, in case of lack of efficacy of thefirst-line ER drug, fesoterodine 8 mg and solifenacin10 mg might be a possible option, due to the resultsof the two available trials comparing fesoterodine orsolifenacin to tolterodine ER [26,33,59], although anincreased rate of adverse events must be taken intoaccount. In case of failure of the first-line ER drugdue to intolerable adverse events, the availability ofclear evidence-based recommendations is limited.In case of dry mouth, a transdermal formulationmight provide some advantages compared to theoral one, and some authors suggested that it mightbe used as first-line therapy [66], but the meta-analysis suggested that localized application sitereactions are very common and might significantlyimpact the patients’ compliance with this formula-tion. On the other hand, if constipation is the mostbothersome adverse event, it can be managed byshifting from solifenacin to tolterodine ER. However,despite the lack of evidence, it might be wise tosuggest that the patients take one of the other oraldrugs before starting more invasive treatments, butcontrolled studied are needed to provide evidence-
based answers to these clinical questions. Conver-sely, those patients taking IR formulations of anti-cholinergic drugs without successful results mightbe offered dose titration in case the patients did notexperienced significantly adverse events, but ERformulations might be the preferred choice.
The overall quality of the randomized controlledtrials available in the field of OAB was good, withmost of the RCTs having a Jadad score �3. However,almost all the trials evaluated short-term therapy(mostly 12 wk), with only a single study continuingthe drug therapy for 52 wk [56], and some adverseevents, such as the impact on cognitive function,should be better evaluated. Moreover, almost all ofthe studies provided efficacy data derived frombladder diaries [67]; a more suitable evaluationshould also include subjective outcomes, such asthe so-called patient-reported outcomes [7], whichare lacking in most of the studies. However, virtuallyall the evidence has been derived from pharmaceu-tical company–sponsored trials, which, to date, havebeen the only way to realize those very expensive,good-quality, large-scale trials. However, the studies’designs reflect the needs of the companies forregistrational studies, rather than addressing thequestions that are more relevant for clinical practice.
According to the criteria of the Overview QualityAssessment Questionnaire (OQAQ) [68], our sys-tematic review can be considered to be a good-quality review. However, due to the limitations ofthe Review Manager software, which allows theevaluation of continuous variables only if they areexpressed as means and standard deviations, it wasnot possible to perform meta-analysis for someclinically relevant efficacy outcomes due to the lackof data in the published reports. Although all theauthors of the RCTs were contacted with the aim ofobtaining the needed data in the appropriate format,the attempt was not successful in most cases.
5. Conclusions
Many of the available RCTs in the field of muscarinicreceptor antagonists for overactive bladder are ofgood methodological quality. ER formulationsshould be preferred to the IR formulations due tothe more favorable profile of efficacy and adverseevents. With regard to IR formulations, doseescalation might yield some improvements in theefficacy, but at the cost of a significant increase inthe rate of adverse events. More clinical studies areneeded to determine which of the available drugsshould be used as first-, second-, and third-linetreatments.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 761
Author contributions: Walter Artibani had full access to all the
data in the study and takes responsibility for the integrity of
the data and the accuracy of the data analysis.
Study concept and design: Novara, Ficarra, Artibani.
Acquisition of data: Galfano, Secco, D’Elia.
Analysis and interpretation of data: Novara, Galfano, Ficarra,
Artibani.
Drafting of the manuscript: Novara.
Critical revision of the manuscript for important intellectual content:
Galfano, Secco, D’Elia, Cavalleri, Ficarra, Artibani.
Statistical analysis: Novara.
Obtaining funding: None.
Administrative, technical, or material support: Cavalleri.
Supervision: Ficarra, Artibani.
Other (specify): None.
Financial disclosures: I certify that all conflicts of interest,
including specific financial interests and relationships and
affiliations relevant to the subject matter or materials
discussed in the manuscript (eg, employment/ affiliation,
grants or funding, consultancies, honoraria, stock ownership
or options, expert testimony, royalties, or patents filed,
received, or pending), are the following: Dr Novara has been
a consultant, investigator, or speaker for Bioxell, GlaxoS-
mithKleine, Pfizer Inc., and Pierre Fabre. Dr Galfano has been a
consultant or investigator for Astellas, Bayer, Bioxell, Novartis,
and Pfizer Inc. Prof Ficarra has been a consultant, investigator
or speaker for Bioxell, Novartis, and Pfizer Inc. Prof Artibani
has been a consultant, investigator, or speaker for Astellas,
Bayer, Bioxell, Novartis, Pfizer Inc., Pierre Fabre, and UCB. Drs
Secco, D’Elia, and Cavalleri have nothing to disclose.
Funding/Support and role of the sponsor: None.
References
[1] Irwin DE, Milsom I, Hunskaar S, et al. Population-based
survey of urinary incontinence, overactive bladder, and
other lower urinary tract symptoms in five countries:
results of the EPIC study. Eur Urol 2006;50:1306–15.
[2] Chapple CR. Advancing the management of overactive
bladder: new data, new directions. Eur Urol Suppl 2007;
6:1–3.
[3] Reeves P, Irwin D, Kelleher C, et al. The current and future
burden and cost of overactive bladder in five European
countries. Eur Urol 2006;50:1050–7.
[4] Klotz T, Bruggenjurgen B, Burkart M, Resch A. The eco-
nomic costs of overactive bladder in Germany. Eur Urol
2007;51:1654–63.
[5] Toozs-Hobson P, Latthe P. Critical evaluation of the effi-
cacy and safety of anticholinergics in overactive bladder.
Eur Urol Suppl 2007;6:425–31.
[6] Hampel C. Long-term management of overactive bladder
with antimuscarinic agents. Eur Urol Suppl 2007;6:
432–7.
[7] Abrams P, Andersson KE. Muscarinic receptor antagonists
for overactive bladder. BJU Int 2007;100:987–1006.
[8] Chapple C, Khullar V, Gabriel Z, Dooley JA. The effects of
antimuscarinic treatments in overactive bladder: a sys-
tematic review and meta-analysis. Eur Urol 2005;48:5–26.
[9] Nabi G, Cody JD, Ellis G, Herbison P, Hay-Smith J. Anti-
cholinergic drugs versus placebo for overactive bladder
syndrome in adults. Cochrane Database Syst Rev
2006;18:CD003781.
[10] Hay-Smith J, Herbison P, Ellis G, Morris A. Which antic-
holinergic drug for overactive bladder symptoms in
adults. Cochrane Database Syst Rev 2005;3:CD005429.
[11] Jadad AR. Randomised controlled trials. London: BMJ Pub-
lishing Group; 1998.
[12] Rothstein HR, Sutton AJ, Borenstein M. Publication bias in
meta-analysis: prevention, assessment and adjustment.
Chichester, UK: John Wiley & Sons, Ltd; 2005.
[13] Nilsson CG, Lukkari E, Haarala M, Kivela A, Hakonen T,
Kiilholma P. Comparison of a 10-mg controlled release
oxybutynin tablet with a 5-mg oxybutynin tablet in urge
incontinent patients. Neurourol Urodyn 1997;16:533–42.
[14] Versi E, Appell R, Mobley D, Patton W, Saltzstein D, The
Ditropan XL Study Group. Dry mouth with conventional
and controlled-release oxybutynin in urinary inconti-
nence. Obstet Gynecol 2000;95:718–21.
[15] Barkin J, Corcos J, Radomski S, et al. A randomized, dou-
ble-blind, parallel-group comparison of controlled- and
immediate-release oxybutynin chloride in urge urinary
incontinence. Clin Ther 2004;26:1026–36.
[16] Corcos J, Casey R, Patrick A, et al. A double-blind random-
ized dose-response study comparing daily doses of 5 mg,
10 mg, and 15 mg controlled-release oxybutynin: balan-
cing efficacy with severity of dry mouth. BJU Int 2006;
97:520–7.
[17] Junemann KP, Hessdorfer E, Unamba-Oparah I, et al. Pro-
piverine hydrochloride immediate and extended release:
comparison of efficacy and tolerability in patients with
overactive bladder. Urol Int 2006;77:334–9.
[18] Jonas U, Hofner K, Madersbacher H, Holmdahl TH, The
International Study Group. Efficacy and safety of two
doses of tolterodine versus placebo in patients with detru-
sor overactivity and symptoms of frequency, urge incon-
tinence, and urgency: urodynamic evaluation. World J
Urol 1997;15:144–51.
[19] Rentzhog L, Stanton SL, Cardozo L, Nelson E, Fall M,
Abrams P. Efficacy and safety of tolterodine in patients
with detrusor instability: a dose-ranging study. Br J Urol
1998;81:42–8.
[20] Millard R, Tuttle J, Moore K, et al. Clinical efficacy and
safety of tolterodine compared to placebo in detrusor
overactivity. J Urol 1999;161:1551–5.
[21] Jacquetin B,Wyndaele J. Tolterodine reducesthenumber of
urge incontinence episodes in patients with an overactive
bladder. Eur J Obstet Gynecol Reprod Biol 2001;98:97–102.
[22] Malone-Lee JG, Walsh JB, Maugourd MF. Tolterodine: a
safe and effective treatment for older patients with over-
active bladder. J Am Geriatr Soc 2001;49:700–5.
[23] Van Kerrebroeck P, Kreder K, Jonas U, Zinner N, Wein A,
The Tolterodine Study Group. Tolterodine once-daily:
superior efficacy and tolerability in the treatment of the
overactive bladder. Urology 2001;57:414–21.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4762
[24] Swift S, Garely A, Dimpfl T, Payne C, The Tolterodine
Study Group. A new once-daily formulation of tolterodine
provides superior efficacy and is well tolerated in women
with overactive bladder. Int Urogynecol J Pelvic Floor
Dysfunct 2003;14:50–4.
[25] Cardozo L, Lisec M, Millard R, et al. Randomized, double-
blind placebo controlled trial of the once daily antimuscari-
nic agent solifenacin succinate in patients with overactive
bladder. J Urol 2004;172:1919–24.
[26] Chapple CR, Rechberger T, Al-Shukri S, et al. Randomized,
double-blind placebo- and tolterodine-controlled trial of
the once-daily antimuscarinic agent solifenacin in
patients with symptomatic overactive bladder. BJU Int
2004;93:303–10.
[27] Chapple CR, Cardozo L, Steers WD, Govier FE. Solifenacin
significantly improves all symptoms of overactive bladder
syndrome. Int J Clin Pract 2006;60:959–66.
[28] Chapple C, Steers W, Norton P, et al. A pooled analysis of
three phase III studies to investigate the efficacy, toler-
ability and safety of darifenacin, a muscarinic M3 selec-
tive receptor antagonist, in the treatment of overactive
bladder. BJU Int 2005;95:993–1001.
[29] Foote J, Glavind K, Kralidis G, Wyndaele J-J. Treatment of
overactive bladder in the older patient: pooled analysis of
three phase III studies of darifenacin, an M3 selective
receptor antagonist. Eur Urol 2005;48:471–7.
[30] Zinner N, Tuttle J, Marks L. Efficacy and tolerability
of darifenacin, a muscarinic M3 selective receptor antago-
nist (M3 SRA), compared with oxybutynin in the treat-
ment of patients with overactive bladder. World J Urol
2005;23:248–52.
[31] Hill S, Khullar V, Wyndaele JJ, Lheritier K, The Darifenacin
Study Group. Dose response with darifenacin, a novel
once-daily M3 selective receptor antagonist for the treat-
ment of overactive bladder: results of a fixed dose study.
Int Urogynecol J Pelvic Floor Dysfunct 2006;17:239–47.
[32] Nitti V, Wiatrak M, Kreitman L, Lipsitz D. Fesoterodine is
an effective antimuscarinic for patients with overactive
bladder (OAB): results of a phase 2 trial. ICS annual
meeting; 2005. Abstract 306. Available at https://www.
icsoffice.org/publications/2005/PDF/0306.PDF.
[33] Chapple C, Van Kerrebroeck P, Tubaro A, et al. Clinical
efficacy, safety, and tolerability of once-daily fesoterodine
in subjects with overactive bladder. Eur Urol 2007;
52:1204–12, Corrigendum. Eur Urol 2008;53:1319.
[34] Nitti VW, Dmochowski R, Sand PK, et al. Efficacy, safety,
and tolerability of fesoterodine for overactive bladder
syndrome. J Urol 2007;178:2488–94.
[35] Anderson RU, Mobley D, Blank B, Saltzstein D, Susset J,
Brown JS, OROS Oxybutynin Study Group. Once-daily
controlled versus immediate release oxybutynin chlor-
ide for urge urinary incontinence. Urology 1999;161:
1809–12.
[36] Birns J, Lukkari E, Malone-Lee JG. A randomized controlled
trial comparing the efficacy of controlled-release oxybu-
tynin tablets (10 mg once daily) with conventional oxybu-
tynin tablets (5 mg twice daily) in patients whose
symptoms were stabilized on 5 mg twice daily of oxybu-
tynin. BJU Int 2000;85:793–8.
[37] Abrams P, Cardozo L, Chapple C, Serdarevic D, Hargreaves
K, Khullar V, The 1032 Study Group. Comparison of the
efficacy, safety, and tolerability of propiverine and oxy-
butynin for the treatment of overactive bladder syn-
drome. Int J Urol 2006;13:692–8.
[38] Burton G. A randomized crossover trial comparing oxy-
butynin taken three times a day or taken ‘‘when needed’’.
Neurourol Urod 1994;13:351–2, abstract.
[39] Sussman D, Garely A. Treatment of overactive bladder
with once-daily extended-release tolterodine or oxybuty-
nin: the antimuscarinic clinical effectiveness trial (ACET).
Curr Med Res Opin 2002;18:177–84.
[40] Mazur D, Wehnert J, Dorschner W, Schubert G, Herfurth G,
Alken RG. Clinical and urodynamic effects of propiverine
in patients suffering from urgency and urge incontinence.
A multicentre dose-optimizing study. Scand J Urol
Nephrol 1995;29:289–94.
[41] Gittelman MC, Kaufman J. Solifenacin succinate 10 mg
once daily significantly improves symptoms of overactive
bladder. Presented at the 17th International Federation of
Gynecology and Obstetrics World Congress, Abstract 111.
November 2–7, 2003; Santiago, Chile.
[42] Gittelman M. The efficacy and safety of solifenacin in
adults with overactive bladder: a multicenter, placebo-
controlled study. Int J Gynaecol Obstetr 2003;83(Suppl
3):94.
[43] Staskin DR, Te AE. Short- and long-term efficacy of soli-
fenacin treatment in patients with symptoms of mixed
urinary incontinence. BJU Int 2006;97:1256–61.
[44] Cardozo L, Castro-Diaz D, Gittelman M, Ridder A, Huang
M. Reductions in overactive bladder-related incontinence
from pooled analysis of phase III trials evaluating treat-
ment with solifenacin. Int Urogynecol J Pelvic Floor Dys-
funct 2006;17:512–9.
[45] Van Kerrebroeck EV, Serment G, Dreher E. Clinical efficacy
and safety of tolterodine compared to oxybutynin in
patients with overactive bladder. Neurourol Urod
1997;16:478–9, abstract #91.
[46] Abrams P, Freeman R, Anderstrom C, Mattiasson A. Tol-
terodine, a new antimuscarinic agent: as effective but
better tolerated than oxybutynin in patients with an over-
active bladder. Br J Urol 1998;81:801–10.
[47] Drutz HP, Appell RA, Gleason D, Klimberg I, Radomski S.
Clinical efficacy and safety of tolterodine compared to
oxybutynin and placebo in patients with overactive blad-
der. Int Urogynecol J Pelvic Floor Dysfunct 1999;10:283–9.
[48] Appell RA, Sand P, Dmochowski R, et al. Prospective
randomized controlled trial of extended-release oxybu-
tynin chloride and tolterodine tartrate in the treatment of
overactive bladder: results of the OBJECT Study. Mayo Clin
Proc 2001;76:358–63.
[49] Malone-Lee J, Shaffu B, Anand C, Powell C. Tolterodine:
superior tolerability than and comparable efficacy to oxy-
butynin in individuals 50 years old or older with over-
active bladder: a randomized controlled trial. J Urol
2001;165:1452–6.
[50] Lee JG, Hong JY, Choo MS, et al. Tolterodina: as effective but
better tolerated than oxybutynin in Asian patients with
symptoms of overactive bladder. Int J Urol 2002;90:247–52.

e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4 763
[51] Diokno AC, Appell RA, Sand PK, et al. Prospective, rando-
mized, double-blind study of the efficacy and tolerability
of the extended-release formulations of oxybutynin and
tolterodine for overactive bladder: results of the OPERA
trial. Mayo Clin Proc 2003;78:687–95.
[52] Homma Y, Paick JS, Lee JG, Kawabe K, Japanese, Korean
Tolterodine Study Group. Clinical efficacy and tolerability
of extended-release tolterodine and immediate-release
oxybutynin in Japanese and Korean patients with an
overactive bladder: a randomized, placebo-controlled
trial. BJU Int 2003;92:741–7.
[53] Giannitsas K, Perimenis P, Athanasopoulos A, Gyftopoulos
K, Nikiforidis G, Barbalias G. Comparison of the efficacy of
tolterodine and oxybutynin in different urodynamic sever-
ity grades of idiopathic detrusor overactivity. Eur Urol
2004;46:776–83.
[54] Homma Y, Kawabe K. Health-related quality of life of
Japanese patients with overactive bladder treated with
extended-release tolterodine or immediate-release oxy-
butynin: a randomized, placebo-controlled trial. World J
Urol 2004;22:251–6.
[55] Madersbacher H, Halaska M, Voigt R, Alloussi S, Hofner K.
A placebo-controlled, multicentre study comparing the
tolerability and efficacy of propiverine and oxybutynin in
patients with urgency and urge incontinence. BJU Int
1999;84:646–51.
[56] Halaska M, Ralph G, Wiedemann A, et al. Controlled,
double-blind, multicentre clinical trial to investigate
long-term tolerability and efficacy of trospium chloride
in patients with detrusor instability. World J Urol
2003;20:392–9.
[57] Junemann KP, Al-Shukri S. Efficacy and tolerability of tros-
pium chloride and tolterodine in 234 patients with urge-
syndrome: a double blind, placebo-controlled, multicentre
clinical trial. Neurourol Urodynam 2000;488–90, abstract.
[58] Junemann K-P, Halaska M, Rittstein T, et al. Propiverine
versus tolterodine: efficacy and tolerability in patients
with overactive bladder. Eur Urol 2005;48:478–82.
[59] Chapple CR, Martinez-Garcia R, Selvaggi L, et al. A com-
parison of the efficacy and tolerability of solifenacin suc-
cinate and extended release tolterodine at treating
Editorial Comment on: A Systematic Review andMeta-Analysis of Randomized Controlled Trialswith Antimuscarinic Drugs for OveractiveBladderRufus CartwrightDepartment of Urogynaecology,King’s College Hospital, London, [email protected]
Previous meta-analyses and evidence-basedguidelines concerning antimuscarinic medicationsfor overactive bladder (OAB) have conflicting
overactive bladder syndrome: results of the STAR trial.
Eur Urol 2005;48:464–70.
[60] Chapple CR, Fianu-Jonsson A, Indig M, et al. Treatment
outcomes in the STAR study: a subanalysis of solifenacin
5 mg and tolterodine ER 4 mg. Eur Urol 2007;52:1195–
1203.
[61] Thuroff JW, Bunke B, Ebner A, et al. Randomized, double-
blind, multicenter trial on treatment of frequency,
urgency and incontinence related to detrusor hyperactiv-
ity: oxybutynin versus propantheline versus placebo.
J Urol 1991;145:813–6.
[62] Leung HY, Yip SK, Cheon C, et al. A randomized controlled
trial of tolterodine and oxybutynin on tolerability and
clinical efficacy for treating Chinese women with an over-
active bladder. BJU Int 2002;90:375–80.
[63] Altan-Yaycioglu R, Yaycioglu O, Aydin Akova Y, Guvel S,
Ozkardes H. Ocular side-effects of tolterodine and oxybu-
tynin, a single-blind prospective randomized trial. Br J
Clin Pharmacol 2005;59:588–92.
[64] Davila GW, Daugherty CA, Sanders SW, Transdermal
Oxybutynin Study Group. A short-term, multicenter,
randomized double-blind dose titration study of the effi-
cacy and anticholinergic side effects of transdermal
compared to immediate release oral oxybutynin treat-
ment of patients with urge urinary incontinence. J Urol
2001;166:140–5.
[65] Dmochowski RR, Sand PK, Zinner NR, Gittelman MC,
Davila GW, Sanders SW, Transdermal Oxybutynin Study
Group. Comparative efficacy and safety of transdermal
oxybutynin and oral tolterodine versus placebo in pre-
viously treated patients with urge and mixed urinary
incontinence. Urology 2003;62:237–42.
[66] Cartwright R, Cardozo L. Transdermal oxybutynin: stick-
ing to the facts. Eur Urol 2007;51:907–14.
[67] Colli E, Parazzini F, Olivieri L, et al. Number of daytime
micturitions and volume voided per micturition in the
evaluation of efficacy of drugs for overactive bladder:
findings from randomized clinical trials. Eur Urol
2007;52:525–30.
[68] Oxman AD, Guyatt GH. Validation of an index of the
quality of review articles. J Clin Epidemiol 1991;44:1271–8.
recommendations with no consensus about appro-priate first-line or second-line therapy [1–3]. Withan increasing number of available agents andformulations licensed, the choice of antimuscari-nic for patients with OAB has become complicated.
The authors of this paper [4] have taken on theHerculean task of reviewing and analysing existingrandomised controlled trials (RCTs) that mightpotentially help clinicians to make an evidence-based choice. So, is it a case of cleaning the Augeanstables? The good news is clearly that existingRCTs are generally of high methodological quality.

It is lamentable, however, that even within thelimited scope of the objective outcomes consideredin this review, many trials are still reporting data ina format that is not amenable to meta-analysis.This difficulty in comparing and assimilating datafrom different trials is compounded by the widevariety of outcome measures employed, some ofwhich are of limited relevance to patients.
The increased regulation in the European Unionputs large, multicentre drug trials out of the reachof all but the most organised and determinedbodies. As the authors note, most available anti-muscarinic data are, therefore, from industry-ledtrials. There may be a conflict between so-called‘‘experimercials’’ [5], aiming to increase marketshare, and the needs of clinicians in providingtargeted interventions. The key question, whichremains largely unanswered for this class ofmedication, regards long-term subjective efficacyfor different subgroups of OAB patients. Asefficacious pharmaceutical agents from differentclasses are developed and as different modalities oftreatment become established, it is to be hopedthat long-term, head-to-head studies will helpdefine the roles of different antimuscarinic med-ications and formulations more clearly.
References
[1] Hay-Smith J, Herbison P, Ellis G, Morris A. Which anti-
cholinergic drug for overactive bladder symptoms in
adults. Cochrane Database of Systematic Reviews;2005.
Abstract CD005429.
[2] Chapple C, Khullar V, Gabriel Z, Dooley JA. The effects
of antimuscarinic treatments in overactive bladder: a
systematic review and meta-analysis. Eur Urol 2005;
48:5–26.
[3] National Institute for Health and Clinical Excellence.
Urinary incontinence: the management of urinary incon-
tinence in women [clinical guideline]. Available at: http://
guidance.nice.org.uk/CG40. Accessed June 2008.
[4] Novara G, Galfano A, Secco S, et al. A systematic review
and meta-analysis of randomized controlled trials with
antimuscarinic drugs for overactive bladder. Eur Urol
2008;54:740–64.
[5] Brownlee S. Medicine. In: Blum D, Knudson M, Henig RM,
editors. A Field Guide for Science Writers: The Official
Guide of the National Association of Science Writers.
2nd ed. New York, NY: Oxford University Press; 2006. p.
155–61.
DOI: 10.1016/j.eururo.2008.06.081
DOI of original article: 10.1016/j.eururo.2008.06.080
e u r o p e a n u r o l o g y 5 4 ( 2 0 0 8 ) 7 4 0 – 7 6 4764