a t 20 a p - university of...
TRANSCRIPT
1
CHAPTER 3
CLINICAL
ASSESSMENT
AND DIAGNOSIS(PP. 72-103)
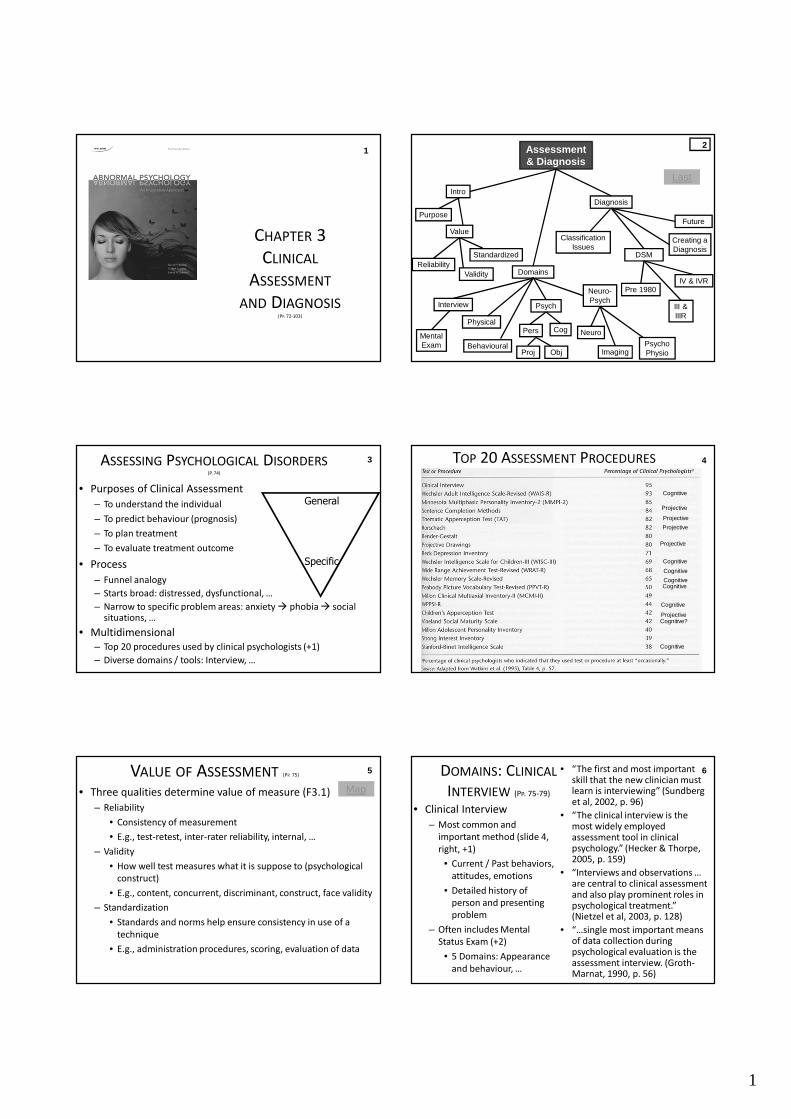
1 Assessment & Diagnosis
Domains
Interview
Value
Standardized
Future
Classification Issues
Mental Exam
Creating a Diagnosis
III & IIIR
IV & IVR
DSM
IntroDiagnosis
Physical
Behavioural
Neuro-Psych
Purpose
Neuro
ImagingPsycho Physio
Pre 1980
Validity
Pers
Psych
Reliability
2
Proj Obj
Cog
Last
• Purposes of Clinical Assessment
– To understand the individual
– To predict behaviour (prognosis)
– To plan treatment
– To evaluate treatment outcome
• Process
– Funnel analogy
– Starts broad: distressed, dysfunctional, …
– Narrow to specific problem areas: anxiety � phobia � social situations, …
• Multidimensional
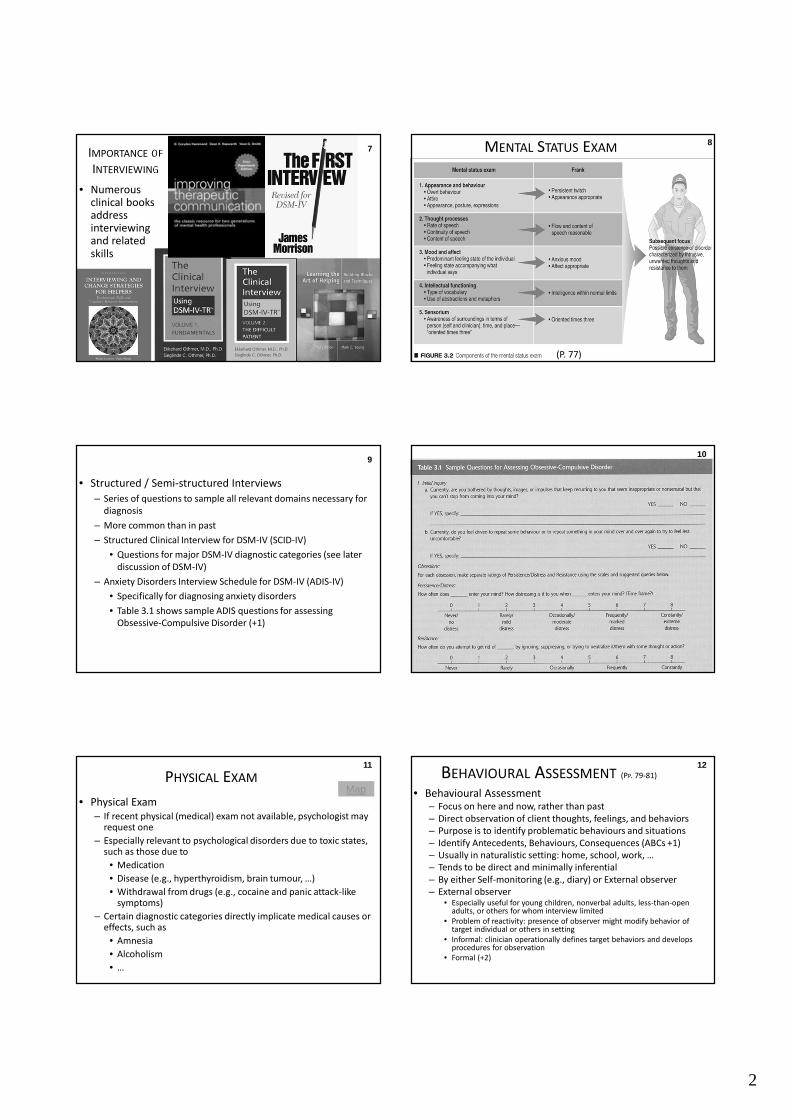
– Top 20 procedures used by clinical psychologists (+1)
– Diverse domains / tools: Interview, …
ASSESSING PSYCHOLOGICAL DISORDERS(P. 74)
3
General
Specific
4
TOP 20 ASSESSMENT PROCEDURES 4
Cognitive?
Cognitive
Cognitive
Cognitive
CognitiveCognitive
Cognitive
Cognitive
Projective
Projective
Projective
Projective
Projective
• Three qualities determine value of measure (F3.1)
– Reliability
• Consistency of measurement
• E.g., test-retest, inter-rater reliability, internal, …
– Validity
• How well test measures what it is suppose to (psychological
construct)
• E.g., content, concurrent, discriminant, construct, face validity
– Standardization
• Standards and norms help ensure consistency in use of a
technique
• E.g., administration procedures, scoring, evaluation of data
VALUE OF ASSESSMENT (PP. 75)5
Map
DOMAINS: CLINICAL
INTERVIEW (PP. 75-79)
• Clinical Interview
– Most common and
important method (slide 4,
right, +1)
• Current / Past behaviors,
attitudes, emotions
• Detailed history of
person and presenting
problem
– Often includes Mental
Status Exam (+2)
• 5 Domains: Appearance
and behaviour, …
6• “The first and most important skill that the new clinician must learn is interviewing” (Sundberg et al, 2002, p. 96)
• “The clinical interview is the most widely employed assessment tool in clinical psychology.” (Hecker & Thorpe, 2005, p. 159)
• “Interviews and observations … are central to clinical assessment and also play prominent roles in psychological treatment.” (Nietzel et al, 2003, p. 128)
• “…single most important means of data collection during psychological evaluation is the assessment interview. (Groth-Marnat, 1990, p. 56)
2
IMPORTANCE OF
INTERVIEWING
• Numerous clinical books address interviewing and related skills
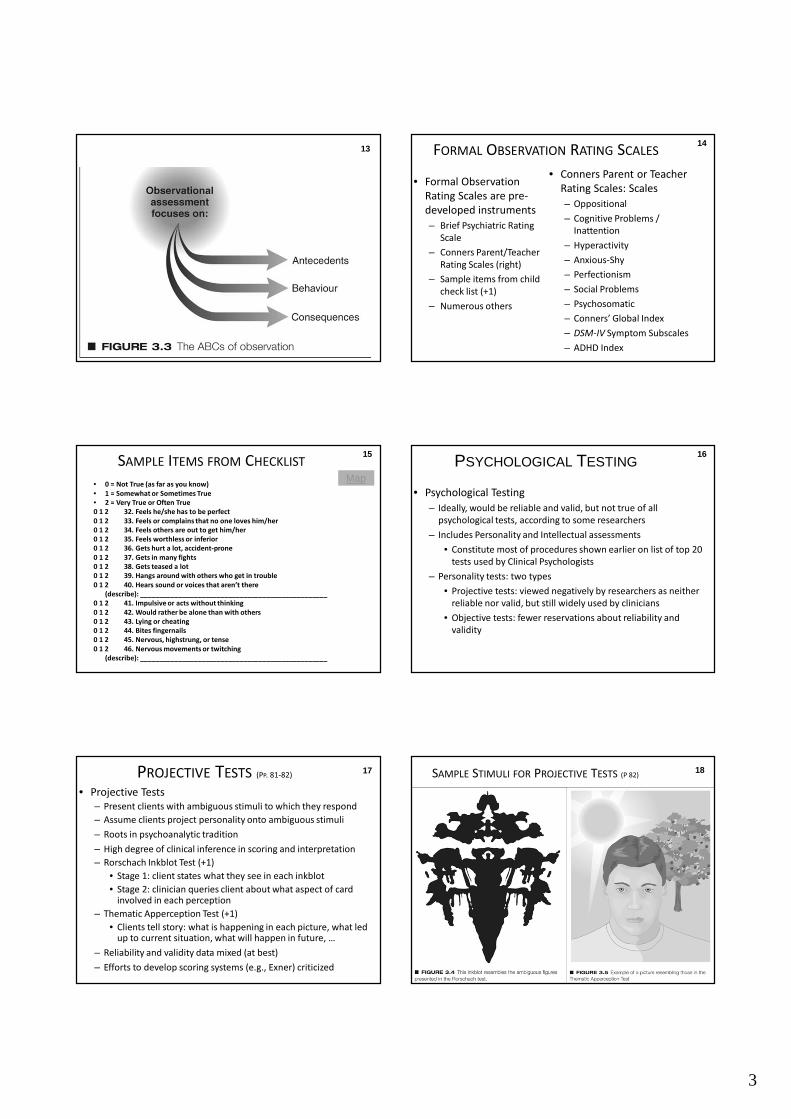
7 MENTAL STATUS EXAM
(P. 77)
8
• Structured / Semi-structured Interviews
– Series of questions to sample all relevant domains necessary for
diagnosis
– More common than in past
– Structured Clinical Interview for DSM-IV (SCID-IV)
• Questions for major DSM-IV diagnostic categories (see later
discussion of DSM-IV)
– Anxiety Disorders Interview Schedule for DSM-IV (ADIS-IV)
• Specifically for diagnosing anxiety disorders
• Table 3.1 shows sample ADIS questions for assessing
Obsessive-Compulsive Disorder (+1)
9
10
10
PHYSICAL EXAM
• Physical Exam
– If recent physical (medical) exam not available, psychologist may request one
– Especially relevant to psychological disorders due to toxic states, such as those due to
• Medication
• Disease (e.g., hyperthyroidism, brain tumour, …)
• Withdrawal from drugs (e.g., cocaine and panic attack-like symptoms)
– Certain diagnostic categories directly implicate medical causes or effects, such as
• Amnesia
• Alcoholism
• …
11
MapBEHAVIOURAL ASSESSMENT (PP. 79-81)
• Behavioural Assessment– Focus on here and now, rather than past
– Direct observation of client thoughts, feelings, and behaviors
– Purpose is to identify problematic behaviours and situations
– Identify Antecedents, Behaviours, Consequences (ABCs +1)
– Usually in naturalistic setting: home, school, work, …
– Tends to be direct and minimally inferential
– By either Self-monitoring (e.g., diary) or External observer
– External observer• Especially useful for young children, nonverbal adults, less-than-open
adults, or others for whom interview limited
• Problem of reactivity: presence of observer might modify behavior of target individual or others in setting
• Informal: clinician operationally defines target behaviors and develops procedures for observation
• Formal (+2)
12
3
13 FORMAL OBSERVATION RATING SCALES
• Conners Parent or Teacher
Rating Scales: Scales
– Oppositional
– Cognitive Problems /
Inattention
– Hyperactivity
– Anxious-Shy
– Perfectionism
– Social Problems
– Psychosomatic
– Conners’ Global Index
– DSM-IV Symptom Subscales
– ADHD Index
14
• Formal Observation
Rating Scales are pre-
developed instruments
– Brief Psychiatric Rating
Scale
– Conners Parent/Teacher
Rating Scales (right)
– Sample items from child
check list (+1)
– Numerous others
• 0 = Not True (as far as you know)
• 1 = Somewhat or Sometimes True
• 2 = Very True or Often True
0 1 2 32. Feels he/she has to be perfect
0 1 2 33. Feels or complains that no one loves him/her
0 1 2 34. Feels others are out to get him/her
0 1 2 35. Feels worthless or inferior
0 1 2 36. Gets hurt a lot, accident-prone
0 1 2 37. Gets in many fights
0 1 2 38. Gets teased a lot
0 1 2 39. Hangs around with others who get in trouble
0 1 2 40. Hears sound or voices that aren’t there
(describe): _________________________________________________
0 1 2 41. Impulsive or acts without thinking
0 1 2 42. Would rather be alone than with others
0 1 2 43. Lying or cheating
0 1 2 44. Bites fingernails
0 1 2 45. Nervous, highstrung, or tense
0 1 2 46. Nervous movements or twitching
(describe): _________________________________________________
SAMPLE ITEMS FROM CHECKLIST15
Map
PSYCHOLOGICAL TESTING
• Psychological Testing
– Ideally, would be reliable and valid, but not true of all
psychological tests, according to some researchers
– Includes Personality and Intellectual assessments
• Constitute most of procedures shown earlier on list of top 20
tests used by Clinical Psychologists
– Personality tests: two types
• Projective tests: viewed negatively by researchers as neither
reliable nor valid, but still widely used by clinicians
• Objective tests: fewer reservations about reliability and
validity
16
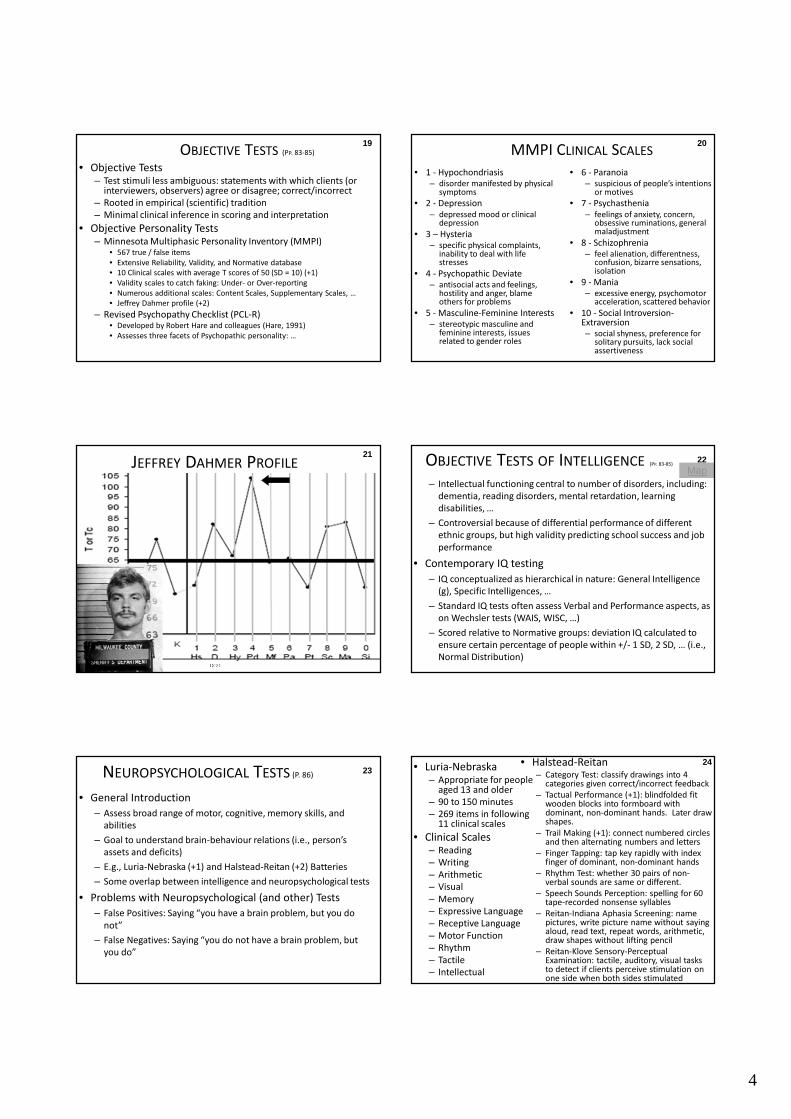
• Projective Tests
– Present clients with ambiguous stimuli to which they respond
– Assume clients project personality onto ambiguous stimuli
– Roots in psychoanalytic tradition
– High degree of clinical inference in scoring and interpretation
– Rorschach Inkblot Test (+1)
• Stage 1: client states what they see in each inkblot
• Stage 2: clinician queries client about what aspect of card involved in each perception
– Thematic Apperception Test (+1)
• Clients tell story: what is happening in each picture, what led up to current situation, what will happen in future, …
– Reliability and validity data mixed (at best)
– Efforts to develop scoring systems (e.g., Exner) criticized
PROJECTIVE TESTS (PP. 81-82)17 18SAMPLE STIMULI FOR PROJECTIVE TESTS (P 82)
4
• Objective Tests– Test stimuli less ambiguous: statements with which clients (or
interviewers, observers) agree or disagree; correct/incorrect
– Rooted in empirical (scientific) tradition
– Minimal clinical inference in scoring and interpretation
• Objective Personality Tests– Minnesota Multiphasic Personality Inventory (MMPI)
• 567 true / false items
• Extensive Reliability, Validity, and Normative database
• 10 Clinical scales with average T scores of 50 (SD = 10) (+1)
• Validity scales to catch faking: Under- or Over-reporting
• Numerous additional scales: Content Scales, Supplementary Scales, …
• Jeffrey Dahmer profile (+2)
– Revised Psychopathy Checklist (PCL-R)• Developed by Robert Hare and colleagues (Hare, 1991)
• Assesses three facets of Psychopathic personality: …
OBJECTIVE TESTS (PP. 83-85)
19
• 1 - Hypochondriasis– disorder manifested by physical
symptoms
• 2 - Depression
– depressed mood or clinical depression
• 3 – Hysteria– specific physical complaints,
inability to deal with life stresses
• 4 - Psychopathic Deviate– antisocial acts and feelings,
hostility and anger, blame others for problems
• 5 - Masculine-Feminine Interests– stereotypic masculine and
feminine interests, issues related to gender roles
20
• 6 - Paranoia– suspicious of people’s intentions
or motives
• 7 - Psychasthenia
– feelings of anxiety, concern, obsessive ruminations, general maladjustment
• 8 - Schizophrenia– feel alienation, differentness,
confusion, bizarre sensations, isolation
• 9 - Mania– excessive energy, psychomotor
acceleration, scattered behavior
• 10 - Social Introversion-Extraversion– social shyness, preference for
solitary pursuits, lack social assertiveness
MMPI CLINICAL SCALES
C8:21
JEFFREY DAHMER PROFILE21
– Intellectual functioning central to number of disorders, including:
dementia, reading disorders, mental retardation, learning
disabilities, …
– Controversial because of differential performance of different
ethnic groups, but high validity predicting school success and job
performance
• Contemporary IQ testing
– IQ conceptualized as hierarchical in nature: General Intelligence
(g), Specific Intelligences, …
– Standard IQ tests often assess Verbal and Performance aspects, as
on Wechsler tests (WAIS, WISC, …)
– Scored relative to Normative groups: deviation IQ calculated to
ensure certain percentage of people within +/- 1 SD, 2 SD, … (i.e.,
Normal Distribution)
OBJECTIVE TESTS OF INTELLIGENCE (PP. 83-85)22
Map
23
• General Introduction
– Assess broad range of motor, cognitive, memory skills, and
abilities
– Goal to understand brain-behaviour relations (i.e., person’s
assets and deficits)
– E.g., Luria-Nebraska (+1) and Halstead-Reitan (+2) Batteries
– Some overlap between intelligence and neuropsychological tests
• Problems with Neuropsychological (and other) Tests
– False Positives: Saying “you have a brain problem, but you do
not”
– False Negatives: Saying “you do not have a brain problem, but
you do”
NEUROPSYCHOLOGICAL TESTS (P. 86)
24• Luria-Nebraska– Appropriate for people
aged 13 and older
– 90 to 150 minutes
– 269 items in following 11 clinical scales
• Clinical Scales– Reading
– Writing
– Arithmetic
– Visual
– Memory
– Expressive Language
– Receptive Language
– Motor Function
– Rhythm
– Tactile
– Intellectual
• Halstead-Reitan– Category Test: classify drawings into 4
categories given correct/incorrect feedback
– Tactual Performance (+1): blindfolded fit wooden blocks into formboard with dominant, non-dominant hands. Later draw shapes.
– Trail Making (+1): connect numbered circles and then alternating numbers and letters
– Finger Tapping: tap key rapidly with index finger of dominant, non-dominant hands
– Rhythm Test: whether 30 pairs of non-verbal sounds are same or different.
– Speech Sounds Perception: spelling for 60 tape-recorded nonsense syllables
– Reitan-Indiana Aphasia Screening: name pictures, write picture name without saying aloud, read text, repeat words, arithmetic, draw shapes without lifting pencil
– Reitan-Klove Sensory-Perceptual Examination: tactile, auditory, visual tasks to detect if clients perceive stimulation on one side when both sides stimulated

5
25
25
Map• Neuroimaging
– Pictures of Brain obtained in various
ways provide window on brain
structure and function
– Imaging Brain Structure
• Computerized axial tomography
(CAT or CT scan): type of X-ray;
pictures brain in slices (right)
• Magnetic resonance imaging
(MRI) operates via strong
magnetic field around head and
has better resolution than CAT
scan (+1)
NEUROIMAGING AND BRAIN STRUCTURE(P. 86-87)
26
27
MRI SCANS 27 28NEUROIMAGING AND BRAIN FUNCTION(P. 87-88)
• Imaging Brain Function – Positron Emission Tomography (PET +1) and Single Photon
Emission Computed Tomography (SPECT +2)• Both involve injection of tracer substance containing radioactive isotopes
• Radioactive isotopes react with oxygen, blood, and glucose in brain
• Researchers at UBC Mood Disorders Clinical Research Unit used PET to identify brain regions involved in dopamine overactivity
– Functional MRI (fMRI)• Provides view of brief changes in brain activity (+3)
• Advantages and Limitations– Provide detailed information regarding brain function
– Procedures are expensive, lack adequate norms
– Procedures have limited clinical utility
29PET SCAN AND DEPRESSION• Scan on right shows marked increase in Prefrontal brain
activity (top) after recovery from Depression
30SPECT AND DEPRESSION• SPECT scan shows increased activity following 12 sessions
of Magnetic Seizure Therapy

6
31
FUNCTIONAL MRI AND
“ALZHEIMER’S”• Brain activation
during memory task for group with gene related to Alzheimer disease (top) and group without gene (middle)
• Both groups normal, but more activation in group at risk for Alzheimer disease may reflect greater “work” to overcome deficit that does not yet manifest itself
Map 32PSYCHOPHYSIOLOGICAL ASSESSMENT(PP. 88-89)
• Psychophysiological Assessment
– Assess brain structure, function, and activity of nervous system
– Methods
• Electroencephalogram (EEG): Brain wave activity (+1)
• Heart rate and respiration: Cardiorespiratory activity
• Electrodermal response and levels: Sweat gland activity
• Electromyography (EMG): Muscle tension
– Uses of Routine Psychophysiological Assessment
• Disorders involving strong emotional component
• e.g., PTSD, sexual dysfunctions, sleep disorders, headache, and
hypertension
33
EEG• EEG: electrodes at various locations on surface of skull (top image) record overall brain activation
• Pattern of activation
varies across different psychological states (bottom image)
– Waves differ in amplitude, frequency, synchronicity (regularity), …
• EEG abnormal in disorders such as Schizophrenia
Map
34DIAGNOSING PSYCHOLOGICAL DISORDERS(P. 89-90)
• Terminology of Classification Systems
– Taxonomy: Classification in scientific context (i.e., entities / things)
– Nosology: Application of taxonomy to psychological / medical
phenomena
– Nomenclature: Labels that comprise the nosology (e.g., Anxiety
Disorders)
– Two major schemes
• APA’s DSM-IV (later)
• WHO’s ICD-10
35CLASSIFICATION ISSUES (PP. 90-92)
• Classification Issues
– Classification central to all sciences
– Assign cases to categories based on shared attributes
• Approaches to Classification
– Classical (or pure) categorical approach
• Strict categories with defining features
• Features necessary and sufficient
– Dimensional approach
• Quantify cognitions, emotions, … along dimensions
– Prototype approach
• Categories defined in terms of “average” or “typical” (i.e., prototypical) cases
• Some cases (exemplars) more typical (dogs in text, chairs +1)
• Example from DSM-IV (+2)36
EXEMPLARS OF CHAIRS

7
37• DSM-IV Criteria for Major Depressive Disorder
– Five (or more) symptoms present during 2 week period; at least
one symptom either #1 or #2
• 1. Depressed Mood most of day
• 2. Diminished interest or pleasure in almost all activities
• 3. Significant weight loss or gain
• 4. Insomnia or hypersomnia nearly every day
• 5. Psychomotor agitation or retardation
• 6. Fatigue or loss of energy nearly every day
• 7. Feelings of worthlessness or excessive guilt
• 8. Diminished ability to think or concentrate or indecision
• 9. Recurrent thoughts of death
– Prototypical approach because different cases will contain
somewhat distinct characteristics, but will have “family
resemblance” to one another
38PURPOSES AND EVOLUTION OF DSM (PP. 93)
• Purposes of DSM and ICD Systems
– Aid communication, evaluate prognosis, need for treatment, and
treatment planning
• History
– DSM-I (1952) and DSM-II (1968)
• Both relied on unproven theories
• Both unreliable
– DSM-III (1980) and DSM-III-R
• Atheoretical, emphasized clinical description
• Multiaxial system with detailed criterion sets for each
disorder
• Problems included low reliability, reliance on committee
consensus
39
• Basic Characteristics
– Five axes describe full clinical presentation (person and environment)
– Clear inclusion and exclusion criteria for disorders, including duration
– Disorders categorized under broad headings
– Prototype approach to classification, empirical basis
• The Five DSM-IV Axes
– Axis I: Most major disorders (+1)
– Axis II: Stable, enduring problems (e.g., personality disorders, mental retardation) (+2)
– Axis III: Medical conditions related to abnormal behaviour
– Axis IV: Psychosocial problems affecting functioning or treatment
– Axis V: Global clinician rating of adaptive functioning
THE DSM-IV (PP. 93-95) MAJOR AXIS I DIAGNOSTIC CATEGORIES
Anxiety disorders Mood disorders
Disorders first diagnosed in infancy and childhood
Substance-related disorders
Schizophrenia and other psychotic disorders
Delirium, dementia, amnestic, and other cognitive disorders
Mental disorders due to a general medical condition
Somatoform disorders
Factitious disorders Dissociative disorders
Other conditions that are the focus of clinical attention
Eating disorders
Sexual and gender identity disorders Impulse-control disorders
Adjustment disorders Sleep disorders
40
DSM AXIS II
• Common Axis II disorders
include
– Borderline Personality
Disorder (PD)
– Schizotypal PD
– Antisocial PD
– Narcissistic PD
– …
– Mild Mental Retardation
41 42DIAGNOSTIC ISSUES
• Reliability
– Consistency with which clinicians assign cases to diagnostic categories
– Much variability in reliability of diagnosis of different disorders, especially in earlier versions of DSM
• E.g., diagnosis of Personality Disorders quite unreliable
• Validity
– Various types: criterion, predictive, …
– Special emphasis on Construct Validity
• Diagnosis relates in expected ways to measures of diverse other constructs: correlation between diagnosis of depression and suicide, happiness scales, …
• Diagnosis distinct from conceptually distinct constructs: depression and antisocial personality disorder distinct

8
43EVALUATION OF DSM-IV• Stronger empirical foundations
than earlier schemes
– Reviewed available scientific
literature and conducted
additional studies if necessary
• Reliability and Validity of criteria
generally better
– Generally better (right), but still
concerns in some areas
– Criteria to identify pathological
gambling problem discriminate
between general population and
people in treatment program for
gambling (+1)
44
• What are Optimal Thresholds for Diagnosis?
– Examples include level or distress, impairment, number of required
symptoms
• Somewhat Arbitrary Time Periods in Definitions
• Other Axes?
– Examples include premorbid history, treatment response, family
functioning
• Is DSM-IV System Optimal for Designing Treatments or
Research?
– Problem of comorbidity
– Defined as two or more disorders for the same person
– High comorbidity is the rule clinically
– Comorbidity threatens the validity of separate diagnoses
UNRESOLVED ISSUES IN DSM-IV(PP. 95-101)45 46
• Social and Cultural Considerations
– Increased interest in implications of culture (nationality, ethnicity, religion, …) for psychopathology
– Certain groups more likely to manifest criteria for disorder
• e.g., eating disorders and young women in West
– Some cultures view psychological disorders more or less negatively. Problem of stigma widespread.
– People with disorders fare better in some cultures
• e.g., recidivism rates for recovered schizophrenics LOWER in less developed countries
Per 100,000
Suicide across the
World
47CREATING A DISORDER
• How diagnostic categories included / excluded
– Mixed Anxiety Depression
• Frequency of co-morbid (but moderate intensity) symptoms led to proposal for Mixed Anxiety Depression category (i.e., Negative Affect)
• International study found many people fitting this category, and with considerable dysfunction
• Placed in Appendix for DSM-IV, perhaps to become full diagnostic category in future versions with more research
– Premenstrual Dysphoric Disorder
• More extreme symptoms than Premenstrual Syndrome (PMS)
• Controversial for various reasons, including possible stigmatization of women and association with past problematic disorders (Hysteria)
Map
48SUMMARY OF CLINICAL
ASSESSMENT AND DIAGNOSIS
• Clinical Assessment and Diagnosis
– Designed to provide complete picture of client
– Designed to aid in understanding and ameliorating human
suffering
– Require reliable, valid, and standardized information
• Dangers of Diagnosis
– Problem of reification
– Problem of stigmatization
• Clinical Assessment and Diagnosis: The Core of Abnormal
Psychology
– Multidimensional perspective of persons who are suffering