aac accepts, published online ahead of print on 19 march...
TRANSCRIPT
1
The combination of doripenem and colistin is bactericidal and synergistic against 2
colistin-resistant, carbapenemase-producing Klebsiella pneumoniae 3
4
Meredith G. Jernigan1, Ellen G. Press2, M. Hong Nguyen2, Cornelius J. Clancy2,3, 5
Ryan K. Shields2 6
7
1 Department of Pharmacy and Therapeutics, University of Pittsburgh 8
2 Department of Medicine, University of Pittsburgh; 9
3 VA Pittsburgh Healthcare System, Pittsburgh, Pennsylvania 10
11
Keywords: Klebsiella pneumoniae, doripenem, colistin, synergy 12
Running Title: Doripenem and colistin are synergistic against KPCs 13
14
15
16
17
18
19
Copyright © 2012, American Society for Microbiology. All Rights Reserved.Antimicrob. Agents Chemother. doi:10.1128/AAC.06364-11 AAC Accepts, published online ahead of print on 19 March 2012
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Abstract 20
We tested two-drug combinations of doripenem, colistin, gentamicin, and doxycycline 21
against 12 carbapenemase-producing Klebsiella pneumoniae (KPC) isolates by time-22
kill. Doripenem and colistin reduced the starting inocula by 2-logs for each isolate 23
(range: 2.02-6.01 log10) and was bactericidal or synergistic against 75 and 50%, 24
respectively. Among colistin- and pandrug-resistant isolates, synergy was identified in 25
60 and 67%, respectively. All other combinations were inferior. We are currently 26
evaluating doripenem and colistin as frontline therapy for KPC infection. 27
28
29
30
31
32
33
34
35
36
37
38
39
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Carbapenemase producing Klebsiella pneumoniae (KPC) are emerging causes 40
of morbidity and mortality at institutions worldwide (4) (12, 14-16). KPC isolates are 41
defined by resistance to the carbapenems and are generally resistant to most other 42
antimicrobial classes. Salvage agents that may retain activity against KPC isolates 43
include colistin, gentamicin, doxycycline and tigecycline (9-10, 18). Resistance to these 44
agents is increasing (3, 7), however, and treatment failures are well-recognized with 45
each (9). Given the dearth of effective antimicrobial agents and poor clinical outcomes 46
among patients with KPC infections, combination therapy has been utilized. 47
Unfortunately, in vitro synergy studies have yielded conflicting results and left clinicians 48
with no clear direction in selecting combination regimens. At our center, we have 49
utilized the combination of doripenem and colistin to treat patients with KPC infections, 50
a decision that was extrapolated from our encouraging preliminary experience in 51
treating extensively drug-resistant (XDR)-Acinetobacter baumannii infections (17). The 52
primary objective of this study was to determine if this combination is active against 53
KPC isolates recovered from our patients. In particular, we focused on colistin-resistant 54
isolates determined in vitro by broth dilution. We also sought to test other two-drug 55
combinations that include commonly employed salvage agents. 56
Toward these ends, we determined the in vitro activity of doripenem, colistin, 57
gentamicin and doxycycline, alone and in combination, against 12 KPC isolates 58
collected over a 3-year period from unique patients at our center. We included 59
doxycycline rather than tigecycline because it is more commonly used at our center, 60
particularly as part of treatment of KPC urinary tract infections. 61
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

We confirmed the presence of KPC for each isolate by modified-Hodge test, and 62
determined minimum inhibitory concentrations (MICs) by standard broth microdilution 63
methods (1). One hundred percent (12/12), 83% (10/12), 83% (10/12) and 58% (7/12) 64
of isolates were resistant to doripenem, colistin, gentamicin and doxycycline, 65
respectively; 50% (6/12) were resistant to all agents. The corresponding MIC90’s were 66
>128, 16, 64 and 16 µg/mL, respectively. Using time-kill assays (2), we found that 67
colistin was bactericidal (>3 log10 decrease from the starting inoculum) against 33% 68
(4/12), including both colistin-susceptible strains. Doripenem and gentamicin were 69
bactericidal against one isolate each, whereas doxycycline was not bactericidal against 70
any isolate (Table 1). 71
We next assessed the activity of two drug combinations by time-kills using 50mL 72
flasks containing 9.9mL of cation-adjusted Mueller-hinton broth, 0.1mL of organism 73
(starting inoculums of 1 x 106 CFU/mL) and fixed drug concentrations alone and in 74
combination (doripenem: 8 µg/mL, colistin: 1 µg/mL, gentamicin: 2 µg/mL, and 75
doxycycline: 2 µg/mL). Flasks were incubated with agitation at 37°C and viable bacterial 76
colonies were enumerated at 0, 4, 8, 12, and 24 hours as previously reported (17). 77
Antimicrobial concentrations were representative of achievable serum levels. Synergy 78
and antagonism were defined as ≥2 log10 greater and lesser kill in combination versus 79
the most active single agent, respectively (21). The combination of doripenem and 80
colistin was bactericidal against 75% (9/12) of isolates (Table 2), and synergistic against 81
50% (6/12; Table 3). Log-kills ranged from 2.02 to 6.01 log10 CFU/mL (median: 3.95 82
log10 CFU/mL; Table 2), and this was the only combination that reduced the starting 83
inocula of all strains. Moreover, doripenem and colistin was synergistic against 60% 84
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
(6/10) and 67% (4/6) of isolates that were resistant to colistin (MICs: 4 to 64 µg/mL) or 85
resistant to all agents, respectively. 86
Other combinations were less active (Table 3). Colistin and gentamicin was 87
bactericidal and synergistic against 50% (6/12) and 25% (3/12) of isolates, respectively. 88
The next most active combination, gentamicin plus doxycycline, was bactericidal and 89
synergistic against 25% (3/12) and 42% (5/12) of isolates, respectively. Synergy was 90
achieved against isolates that were doxycycline susceptible; bactericidal activity or 91
synergy was not identified among doxycycline-resistant strains. Doripenem and 92
gentamicin was also bactericidal against 25% (3/12), but synergy was evident against 93
only 8% (1/12). The least active combinations were colistin plus doxycycline and 94
doripenem plus doxycycline, which were bactericidal against 17% (2/12) and 8% (1/12) 95
of isolates, respectively. Doripenem and doxycycline was synergistic against 25% 96
(3/12) of isolates, whereas colistin plus doxycycline was synergistic against 8% (1/12). 97
Antagonism was identified with all combinations except doripenem and colistin (Table 98
3). The combination of colistin and doxycycline was antagonistic in 25% (3/12). 99
Doripenem plus colistin or gentamicin were associated with the lowest and 100
highest median AUCs, respectively (Table 4). Indeed, the median AUC for colistin and 101
doripenem was lower than the other combinations (p=0.004), including the individual 102
combinations of gentamicin plus doxycycline (p=0.04) and doripenem plus doxycycline 103
(p<0.0001; Figure 1, GraphPad Prism Software (La Jolla, CA)). 104
Taken together, our data demonstrate that doripenem plus colistin was the most 105
active two-drug combination against KPC isolates. Doripenem and colistin attained the 106
highest levels of bactericidal activity and synergy, and was the only combination that did 107
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
not show any antagonism. Moreover, the combination was effective at clinically-108
achievable concentrations of both drugs (5, 8) and it was particularly active against 109
colistin- and pan-drug resistant isolates. In this regard, our findings are similar to those 110
we reported against XDR-Acinetobacter baumannii isolates from our center (17). 111
Furthermore, our results extend our understanding of in vitro synergy against KPC 112
isolates, which have been studied in colistin-susceptible strains (11, 20, 22) or by 113
checkerboard broth microdilution (6) previously. 114
At present, the treatment options for patients with KPC infections are limited, as 115
evident by crude mortality rates that are reported to range from 42 to 69% (13-14, 19, 116
24). Mortality rates are higher among patients infected with colistin-resistant isolates 117
(24). Investigators have reported that combination therapy may improve outcomes of 118
KPC infections compared to monotherapy (9, 23), but optimal regimens are not defined 119
and none have been shown to be effective against colistin resistant-isolates. Of note, 120
we reported promising preliminary data in a pilot clinical study using doripenem plus 121
colistin to treat XDR-A. baumannii infections (17). Based on these data and the in vitro 122
findings of the current study, we are currently using the combination as the 123
recommended front-line regimen against KPC infections. 124
The other combinations tested in this study demonstrated inferior bactericidal 125
activity and less synergy. Furthermore, the second most potent combination in vitro 126
(colistin plus gentamicin), is limited in clinical settings by the potential for additive 127
toxicity. Our data suggest that doxycycline and gentamicin may be useful against 128
isolates that retain susceptibility to the former agent, but at our center such isolates are 129
in the minority. In the end, this combination was synergistic against only 25% (3/12) of 130
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
isolates and may be unsuitable for the treatment of severe or life-threatening KPC 131
infections. At present, we reserve doxycycline-containing regimens for the treatment of 132
uncomplicated cystitis at our center. The remaining combinations were even less 133
effective in vitro, and we do not employ them in the clinic. Finally, it is important to note 134
that the number of strains evaluated here are limited and future studies are needed. 135
Towards this, the exact mechanisms underlying the synergistic effects between 136
doripenem and colistin have not been identified and merit further investigation. It is 137
possible that colistin permeabilizes the outer cell membrane of KPC isolates allowing 138
high concentrations of doripenem to access penicillin-binding proteins in the 139
cytoplasmic membrane where the drug acts. 140
In conclusion, it is important to stress that these results were obtained against 141
KPC isolates from a single center. As such, the results may not be applicable to 142
isolates from other centers or geographic locations. It is advisable for centers to test 143
isolates recovered from patients at their institution. Having introduced doripenem and 144
colistin as the recommended therapy for KPC infections at our center, we are in the 145
process of accumulating our clinical experience and assessing the impact of the 146
regimen on preventing the emergence of colistin resistance. 147
148
149
150
151
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Acknowledgements. The project described was supported by Award Number KL2 152
RR024154 from the National Center for Research Resources to R.K.S. The content is solely 153
the responsibility of the authors and does not necessarily represent the official views of the 154
National Center for Research Resources or the National Institutes of Health. 155
156
157
158
159
160
161
162
163
164
165
166
167
168
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

References 169
1. Clinical and Laboratory Standards Institute. 2009. Methods for Dilution 170
Antimicrobial Susceptibility Tests for Bacteria that Grow Aerobically; Approved 171
Standard - Eighth Edition: Approved Standard M07-A8. CLSI, Wayne, PA 172
2. National Committee for Clinical Laboratory Standards. 1999. Methods for 173
determining bactericidal activity of antimicrobial agents. Approved guideline 174
M26-A. National Committee for Clinical Laboratory Standards, Wayne, PA. 175
3. Bogdanovich, T., J. M. Adams-Haduch, G. B. Tian, M. H. Nguyen, E. J. 176
Kwak, C. A. Muto, and Y. Doi. 2011. Colistin-resistant, Klebsiella pneumoniae 177
carbapenemase (KPC)-producing Klebsiella pneumoniae belonging to the 178
international epidemic clone ST258. Clin Infect Dis 53:373-376. 179
4. Boucher, H. W., G. H. Talbot, J. S. Bradley, J. E. Edwards, D. Gilbert, L. B. 180
Rice, M. Scheld, B. Spellberg, and J. Bartlett. 2009. Bad bugs, no drugs: no 181
ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect 182
Dis 48:1-12. 183
5. Cirillo, I., N. Vaccaro, K. Turner, B. Solanki, J. Natarajan, and R. Redman. 184
2009. Pharmacokinetics, safety, and tolerability of doripenem after 0.5-, 1-, and 185
4-hour infusions in healthy volunteers. J Clin Pharmacol 49:798-806. 186
6. Elemam, A., J. Rahimian, and M. Doymaz. 2010. In vitro evaluation of antibiotic 187
synergy for polymyxin B-resistant carbapenemase-producing Klebsiella 188
pneumoniae. J Clin Microbiol 48:3558-3562. 189
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

7. Elemam, A., J. Rahimian, and W. Mandell. 2009. Infection with panresistant 190
Klebsiella pneumoniae: a report of 2 cases and a brief review of the literature. 191
Clin Infect Dis 49:271-274. 192
8. Garonzik, S. M., J. Li, V. Thamlikitkul, D. L. Paterson, S. Shoham, J. Jacob, 193
F. P. Silveira, A. Forrest, and R. L. Nation. 2011. Population pharmacokinetics 194
of colistin methanesulfonate and formed colistin in critically ill patients from a 195
multicenter study provide dosing suggestions for various categories of patients. 196
Antimicrob Agents Chemother 55:3284-3294. 197
9. Hirsch, E. B., and V. H. Tam. 2010. Detection and treatment options for 198
Klebsiella pneumoniae carbapenemases (KPCs): an emerging cause of 199
multidrug-resistant infection. J Antimicrob Chemother 65:1119-1125. 200
10. Hussein, K., H. Sprecher, T. Mashiach, I. Oren, I. Kassis, and R. Finkelstein. 201
2009. Carbapenem resistance among Klebsiella pneumoniae isolates: risk 202
factors, molecular characteristics, and susceptibility patterns. Infect Control Hosp 203
Epidemiol 30:666-671. 204
11. Le, J., B. McKee, W. Srisupha-Olarn, and D. S. Burgess. 2011. In vitro activity 205
of carbapenems alone and in combination with amikacin against KPC-producing 206
Klebsiella pneumoniae. J Clin Med Res 3:106-110. 207
12. Marchaim, D., T. Chopra, F. Perez, K. Hayakawa, P. R. Lephart, S. 208
Bheemreddy, C. Blunden, A. M. Hujer, S. Rudin, M. Shango, M. Campbell, J. 209
Varkey, J. Slim, F. Ahmad, D. Patel, T. Y. Chen, J. M. Pogue, H. Salimnia, S. 210
Dhar, R. A. Bonomo, and K. S. Kaye. 2011. Outcomes and genetic relatedness 211
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

of carbapenem-resistant enterobacteriaceae at detroit medical center. Infect 212
Control Hosp Epidemiol 32:861-871. 213
13. Nguyen, M., G. A. Eschenauer, M. Bryan, K. O'Neil, E. Y. Furuya, P. Della-214
Latta, and C. J. Kubin. 2010. Carbapenem-resistant Klebsiella pneumoniae 215
bacteremia: factors correlated with clinical and microbiologic outcomes. Diagn 216
Microbiol Infect Dis 67:180-184. 217
14. Patel, G., S. Huprikar, S. H. Factor, S. G. Jenkins, and D. P. Calfee. 2008. 218
Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the 219
impact of antimicrobial and adjunctive therapies. Infect Control Hosp Epidemiol 220
29:1099-1106. 221
15. Qureshi, Z. A., D. L. Paterson, A. Y. Peleg, J. M. Adams-Haduch, K. A. Shutt, 222
D. L. Pakstis, E. Sordillo, B. Polsky, G. Sandkovsky, M. K. Bhussar, and Y. 223
Doi. 2011. Clinical characteristics of bacteraemia caused by extended-spectrum 224
beta-lactamase-producing Enterobacteriaceae in the era of CTX-M-type and 225
KPC-type beta-lactamases. Clin Microbiol Infect. 226
16. Schwaber, M. J., S. Klarfeld-Lidji, S. Navon-Venezia, D. Schwartz, A. Leavitt, 227
and Y. Carmeli. 2008. Predictors of carbapenem-resistant Klebsiella 228
pneumoniae acquisition among hospitalized adults and effect of acquisition on 229
mortality. Antimicrob Agents Chemother 52:1028-1033. 230
17. Shields, R. K., E. J. Kwak, B. A. Potoski, Y. Doi, J. M. Adams-Haduch, F. P. 231
Silviera, Y. Toyoda, J. M. Pilewski, M. Crespo, A. W. Pasculle, C. J. Clancy, 232
and M. H. Nguyen. 2011. High mortality rates among solid organ transplant 233
recipients infected with extensively drug-resistant Acinetobacter baumannii: using 234
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

in vitro antibiotic combination testing to identify the combination of a carbapenem 235
and colistin as an effective treatment regimen. Diagn Microbiol Infect Dis 70:246-236
252. 237
18. Shields, R. K., M. H. Nguyen, E. J. Kwak, F. P. Silveira, R. C. Abdel Massih, 238
B. A. Potoski, G. Eschenauer, and C. J. Clancy. 2011. Epidemiology, risk 239
factors, and outcomes of klebsiella pneumonia carbapenemase (KPC) infections 240
in solid organ transplant recipients [Abstract K-543]. Presented at the 51st 241
Interscience Conference on Antimicrobial Agents and Chemotherapy (Chicago). 242
19. Souli, M., I. Galani, A. Antoniadou, E. Papadomichelakis, G. Poulakou, T. 243
Panagea, S. Vourli, L. Zerva, A. Armaganidis, K. Kanellakopoulou, and H. 244
Giamarellou. 2010. An outbreak of infection due to beta-Lactamase Klebsiella 245
pneumoniae Carbapenemase 2-producing K. pneumoniae in a Greek University 246
Hospital: molecular characterization, epidemiology, and outcomes. Clin Infect Dis 247
50:364-373. 248
20. Souli, M., I. Galani, S. Boukovalas, M. G. Gourgoulis, Z. Chryssouli, K. 249
Kanellakopoulou, T. Panagea, and H. Giamarellou. 2011. In vitro interactions 250
of antimicrobial combinations with fosfomycin against KPC-2-producing 251
Klebsiella pneumoniae and protection of resistance development. Antimicrob 252
Agents Chemother 55:2395-2397. 253
21. Souli, M., P. D. Rekatsina, Z. Chryssouli, I. Galani, H. Giamarellou, and K. 254
Kanellakopoulou. 2009. Does the activity of the combination of imipenem and 255
colistin in vitro exceed the problem of resistance in metallo-beta-lactamase-256
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

producing Klebsiella pneumoniae isolates? Antimicrob Agents Chemother 257
53:2133-2135. 258
22. Wiskirchen, D. E., P. Koomanachai, A. M. Nicasio, D. P. Nicolau, and J. L. 259
Kuti. 2011. In vitro pharmacodynamics of simulated pulmonary exposures of 260
tigecycline alone and in combination against Klebsiella pneumoniae isolates 261
producing a KPC carbapenemase. Antimicrob Agents Chemother 55:1420-1427. 262
23. Zarkotou, O., S. Pournaras, P. Tselioti, V. Dragoumanos, V. Pitiriga, K. 263
Ranellou, A. Prekates, K. Themeli-Digalaki, and A. Tsakris. 2011. Predictors 264
of mortality in patients with bloodstream infections caused by KPC-producing 265
Klebsiella pneumoniae and impact of appropriate antimicrobial treatment. Clin 266
Microbiol Infect 17:1798-1803. 267
24. Zarkotou, O., S. Pournaras, E. Voulgari, G. Chrysos, A. Prekates, D. 268
Voutsinas, K. Themeli-Digalaki, and A. Tsakris. 2010. Risk factors and 269
outcomes associated with acquisition of colistin-resistant KPC-producing 270
Klebsiella pneumoniae: a matched case-control study. J Clin Microbiol 48:2271-271
2274. 272
273
274
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Table 1. Minimum inhibitory concentrations for KPC isolates
Strain
MIC (mcg/mL) Log Δ from the Starting Inoculum (log10 CFU/mL) †
Doripenem Colistin Gentamicin Doxycycline Doripenem Colistin Gentamicin Doxycycline
1* 64 8 16 8 3.67 -3.76 3.78 -1.40
18 16 64 32 4 -4.96 -2.86 3.75 2.73
82 16 8 8 4 3.64 3.64 3.22 3.95
124* 16 16 64 16 2.99 -1.89 -2.35 2.87
133* 128 16 64 16 3.83 -3.60 3.62 3.70
136 128 4 >64 4 3.53 -2.05 2.78 3.24
141 >128 0.5 1 4 4.44 -3.19 -2.74 3.90
145* >128 16 64 16 2.66 -1.11 -0.03 2.12
167 32 1 16 8 3.75 -4.74 4.43 3.49
180* 32 8 32 16 4.06 -0.47 3.53 3.69
182* 32 8 64 16 2.66 -0.47 3.93 3.98
183 64 16 1 2 4.39 -0.79 -3.70 3.52
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

* Indicates isolates resistant to all agents tested.
† Log Δ = Final inoculum – Starting inoculum (log10 CFU/mL)
Negative numbers represent a decrease from the starting inoculum and positive numbers represent an increase. Fixed concentrations of doripenem (8 µg/mL), colistin (1 µg/mL), gentamicin (2 µg/mL), and doxycycline (2 µg/mL) were used for all isolates.
Note. The following susceptibility breakpoints were used: doripenem and colistin (≤ 2µg/mL) and gentamicin and doxycycline (≤ 4µg/mL).
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Table 2. Log change (log10 cfu/mL) from the starting inoculum and most active single agent after 24 hours of incubation.
Combination Isolate
1 18 82 124 133 136 141 145 167 180 182 183 Log Δ (log10 CFU/mL)*
Colistin + Doripenem -6.01 -4.12 -2.09 -5.99 -3.57 -3.95 -3.94 -4.65 -5.76 -2.02 -2.73 -3.90
-2.25 0.84 -5.73 -4.10 0.03 -1.90 -0.75 -3.54 -1.02 -1.55 -2.26 -3.11
Colistin + Gentamicin -4.56 -3.07 -3.20 -5.87 -2.07 -2.22 -5.60 1.70 -2.05 -0.60 -0.56 -5.00
-0.80 -0.21 -6.84 -3.52 1.53 -0.17 -2.41 1.73 2.69 -0.13 -0.09 -1.30
Colistin + Doxycycline -1.21 -0.38 0.29 -0.57 -1.06 -0.85 -3.37 -0.24 -5.48 0.02 -0.60 -1.15
2.55 2.48 -3.35 1.35 2.54 1.20 -0.18 0.87 -0.74 0.49 -0.13 -0.36
Doripenem + Gentamicin 3.69 -5.95 -2.40 3.85 4.11 0.99 -4.43 2.63 3.88 3.94 3.40 -5.04
0.02 -0.99 -5.62 6.20 0.49 -1.79 -1.69 2.66 0.13 0.41 0.74 -1.34
Doripenem + Doxycycline 4.47 -0.88 3.90 -3.03 4.13 3.21 3.95 2.70 4.49 -0.43 4.06 -1.99
5.87 4.08 0.26 -5.90 0.89 -0.03 0.05 0.58 1.00 -4.12 1.40 -5.51
Gentamicin +Doxycycline -1.61 -0.54 -5.98 4.01 2.93 -1.38 -5.65 2.74 4.51 3.42 3.73 -5.73
-0.21 -3.27 -9.20 6.36 -0.69 -4.16 -2.91 2.77 1.02 -0.11 -0.20 -2.03
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
* Log Δ is defined as:
Non-shaded rows: Final inoculum – Starting inoculum (log10 CFU/mL). Negative numbers represent a decrease from the starting inoculum and positive numbers represent an increase.
Shaded rows: Final inoculum of the most active single drug – Final inoculum of the two-drug combination (log10 CFU/mL). Negative numbers represent greater killing with two-drugs versus one.
Fixed concentrations of doripenem (8 µg/mL), colistin (1 µg/mL), gentamicin (2 µg/mL), and doxycycline (2 µg/mL) were used for all isolates.
Note. Bold numbers indicate synergy.
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from
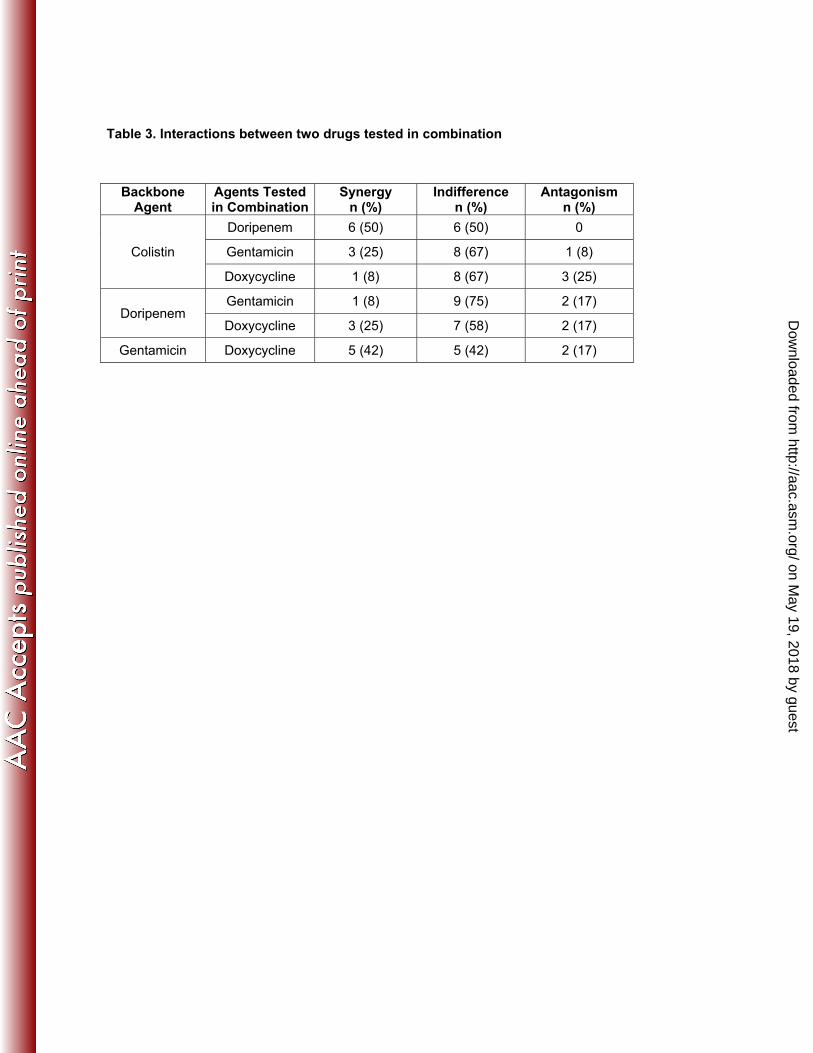
Table 3. Interactions between two drugs tested in combination
Backbone Agent
Agents Tested in Combination
Synergy n (%)
Indifference n (%)
Antagonism n (%)
Colistin
Doripenem 6 (50) 6 (50) 0
Gentamicin 3 (25) 8 (67) 1 (8)
Doxycycline 1 (8) 8 (67) 3 (25)
Doripenem Gentamicin 1 (8) 9 (75) 2 (17)
Doxycycline 3 (25) 7 (58) 2 (17)
Gentamicin Doxycycline 5 (42) 5 (42) 2 (17)
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Table 4. Area under the curve for two-drug combinations after 24 hours of incubation
NA = Not applicable; area under the curve was not calculated for antagonistic combinations.
Isolate Colistin plus Doripenem plus Gentamicin
plus Doripenem Gentamicin Doxycycline Gentamicin Doxycycline Doxycycline
1 62.34 88.02 NA 209.5 NA 106.6
18 69.6 103.9 NA 81.7 NA 134.2
82 74.8 57.4 141.0 62.8 150.6 52.9
124 47.8 37.46 132.5 NA 128.2 NA
133 87.9 110.2 NA 176.5 168.5 206.0
136 84.8 121.4 138.5 202.9 213.6 143.4
141 59.4 29.1 99.9 22.4 156.7 50.8
145 81.5 139.0 157.4 NA 195.3 NA
167 33.9 NA 51.0 207.6 207.4 220.1
180 118.3 132.4 146.7 155.4 138.7 203.7
182 112.3 137.0 135.5 183.8 164.8 168.2
183 82.1 10.0 132.1 15.9 107.5 26.4 Median (Range)
78.2 (33.9 – 118.3)
103.9 (10.0 – 139.0)
135.5 (51.0 – 157.4)
165.9 (15.9 – 209.5)
160.8 (107.5 – 213.6)
138.8 (26.4 – 220.1)
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from

Figure 1. Representative area under the curve (AUC) for isolates alone and in combination for the following drug combinations: a) colistin and doripenem;
b) gentamicin and doxycycline; and c) doripenem and doxycyclineb) gentamicin and doxycycline; and c) doripenem and doxycycline
a) Representative AUC for colistin (light grey), doripenem (dark grey),or both (striped)
10
5
log
(CFU
/mL) c) Representative AUC for doripenem (light grey), doxycycline (dark grey),
or both (striped)10
U/m
L)
0 5 10 15 200
Time of Incubation (Hours)
0 5 10 15 200
5
log
(CFU
b) Representative AUC for gentamicin (light grey), doxycycline (dark grey),or both (striped)
10
/mL)
Time of Incubation (Hours)
0 5 10 15 200
5
log
(CFU
/
Figure 1 Legend. Representative AUC graphs of three synergistic combinations. Shading with t i t th AUC f t d0 5 10 15 20
Time of Incubation (Hours)stripes represents the AUC for two‐drug combinations.
on May 19, 2018 by guest
http://aac.asm.org/
Dow
nloaded from