abbott prism ... · fusiondiagnosticsr&d,abbott laboratories, abbott park, il 60064. 2nonsdaj...
TRANSCRIPT

CLIN.CHEM.37/9, 1540-1547 (1991)
1540 CLINICALCHEMISTRY,Vol.37, No.9, 1991
Abbott Prism: a Multichannel Heterogeneous Chemiluminescence ImmunoassayAnalyzerOmar S. Khalil,’ Tom F. Zurek, Jeff Tryba, Charles F. Hanna, Robert Hollar, Curt Pepe, Kevin Genger,Charles Brentz, Brian Murphy, Noman Abunimeh, Rich Carver, Pat Harder, Carole Coleman,Eugene Robertson, and Julie Wolf-Rogers
We describe a multichannel heterogeneous immunoas-say analyzer in which a sample is split between dispos-able reaction trays in a group of linear tracks. Thesystem’s pipettor uses noninvasive sensing of the samplevolume and disposable pipet tips. Each assay track has(a) a conveyor belt for moving reaction trays to predeter-mined functional stations, (b) temperature-controlled tun-nels, (C) noncontact transfer of the reaction mixture be-tween incubation and detection wells, and (c single-photon counting to detect a chemiluminescence (CL)signal from the captured immunochemical product. Anovel disposable reaction tray, with separate reaction anddetection wells and self-contained fluid removal, is used inconjunction with the transfer device on the track toproduce a carryover-free system. The linear immunoas-say track has nine predetermined positionsfor performingindividualassay steps. Assay step sequence and timing isselected by changing the location of the assay modulesbetween these predetermined positions.The assay meth-odology, a combination of microparticlecapture and directdetection of a CL signal on a porous matrix, offersexcellent sensitivity, specificity, and ease of automation.Immunoassay configurations have been tested for hepa-titis B surface antigen and for antibodies to hepatitis Bcore antigen, hepatitis C virus, human immunodeficiencyvirus I and II, and human T-cell leukemia virus I and II.
AddItional Keyphrases: microparticle capture viruseslaboratory safety sample handling . screening
Screening for antibodies to human immunodeficiencyvirus (H1V) and hepatitis C virus (HCV), in addition tohepatitis B surface antigen (HBsAg), has increased thenumber of tests performed in blood banks.2 A need hasemerged for a high-throughput screening immunoassayanalyzer to meet the increased testing volume. Auto-mated immunoassay modules based on coated microti-ter plates or coated beads are available, but none ofthese is a totally automated system. Separate pipettors
Diagnostics Division, Abbott Laboratories, Abbott Park, IL60064.
‘Address for correspondence: Department 9YA, AP1A, Trans-fusion Diagnostics R&D, Abbott Laboratories, Abbott Park, IL60064.
2NonsdaJ abbreviations: HBc, hepatitis B core antigen;HBsAg, hepatitis B surface antigen; HCV, hepatitis C virus; HJV1/11, human immunodeficiency virus I/il; HTLV I/il, human T-cellleukemia virus I/fl; CL, chemiluminescence; CLIA, chemilumines-cence immunoaasaay; TSH, thyrotropin; and CEA, carcinoembry-onic antigen.
Received May 14, 1991; accepted July 10, 1991.
and barcode readers are used, and considerable operatorinteraction is required.
The goals of our work were to (a) build a high-throughput immunoassay screening analyzer for bloodbanks and high-volume laboratories; (b) construct acarryover-free system to avoid possible false-positiveresults and hence unnecessary retesting; and (c) achievesensitivities and specificities equal or superior to thoseof current enzyme immunoassay methods.
To accomplish the throughput goal, we used thefollowing strategies: (a) short assay incubation timesthrough use of microparticles as the capture phase inthe immunoassay, (b) large instrument sample capacity(168 samples for early versions and 308 for productioninstruments), and (c) parallel sample processing, sothatimmunoassay tests for as many as six infectious dis-eases per sample could be performed simultaneously;alternatively, up to 11 combined virology and blood-typing tests can be simultaneously performed on thesamples. To accomplish a carryover-free system, weused disposable pipet tips, noninvasive sensing of theliquid level of the sample, and a noncontact method fortransferring the reaction mixture. The sensitivity andspecificity goal was achieved by using chemilwnines-cence (CL) detection, using separate sample-incubationand signal-detection wells, and tightly controlling thetemperature over the duration of the assay.
The instrument we developed to implement thesestrategies comprised an automated pipettor; a stagingarea for samples, controls, and disposables; parallelchemiluminescence immunoassay (CLIA) processingchannels; a solid-waste disposal receptacle; and a con-trolling computer. Here we describe the researchlclini-cal instruments and present the data generated withthese systems. The production units (data not included)have enhanced operator interaction, refrigerated re-agent storage, computer data tracking and diagnostics,and enhanced graphics, but have the same assay perfor-mance and throughput. Subsequent instruments alsoinclude up to two blood-typing channels, where agglu-tinates are detected in microtiter plate wells throughphotometric detection; these instruments have the ca-pability for photometric determination of alanine ami-notransferase and for screening for syphilis.
Because the system is primarily designed for donorscreening in blood banks, we first configured and per-formed assays of HBsAg, anti-HBc, anti-HIV-IIll, anti-HTLV-I/H,and anti-HCV. However, any macromolecu-lar immunoassay can be performed on this system, asillustrated with assays of thyrotropin (TSH) and carci-
SYRINGE PUMP
PRESSURE TRANSDUCER-
SAMPLE TUBE
CLINICALCHEMISTRY,Vol.37, No.9, 1991 1541
#{149}noembryomc antigen (CEA). This analyzer can measureboth short-lived acridinium-labeled CL and long-livedalkaline phosphatase-catalyzed dioxetane CL.
Materials and Methods
InstrumentationLevel sensing and automated sample pipetting: The
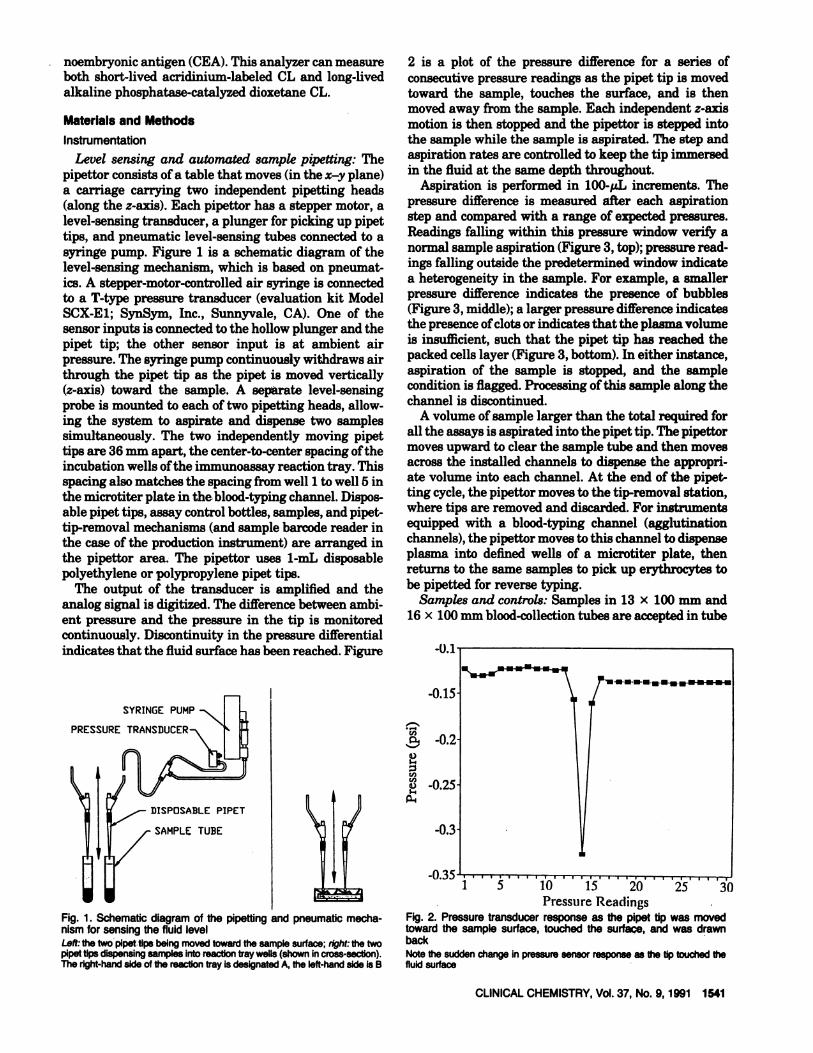
pipettor consistsof a table that moves (in the x-y plane)a carriage carrying two independent pipetting heads(along the z-axis). Each pipettor has a stepper motor, alevel-sensing transducer, a plunger for picking up pipettips, and pneumatic level-sensing tubes connected to asyringe pump. Figure 1 is a schematic diagram of thelevel-sensing mechanism, which is based on pneumat-ics. A stepper-motor-controlled air syringe is connectedto a T-type pressure transducer (evaluation kit ModelSCX-E1; SynSym, Inc., Sunnyvale, CA). One of thesensor inputs is connectedto the hollow plunger and thepipet tip; the other sensor input is at ambient airpressure. The syringe pump continuously withdraws airthrough the pipet tip as the pipet is moved vertically(z-axis) toward the sample. A separate level-sensingprobe is mounted to each of two pipetting heads, allow-ing the system to aspirate and dispense two samplessimultaneously. The two independently moving pipettips are 36 mm apart, the center-to-center spacing of theincubation wells of the immunoassay reaction tray. Thisspacing also matches the spacing from well 1 to well 5 inthe microtiter plate in the blood-typing channel. Dispos-able pipet tips, assay control bottles, samples, and pipet-tip-removal mechanisms (and sample barcode reader inthe case of the production instrument) are arranged inthe pipettor area. The pipettor uses 1-mL disposablepolyethylene or polypropylene pipet tips.
The output of the transducer is amplified and theanalog signal is digitized. The difference between ambi-ent pressure and the pressure in the tip is monitoredcontinuously. Discontinuity in the pressure differentialindicates that the fluid surface has been reached. Figure
Fig. 1. Schematicdiagramof the pipettingandpneumaticmecha-nismforsensingthefluidlevelLeft:the two pipet tips being moved toward the sample surface; right: the twopipet tips dispensingsamples into reaction tray wells (shown in cross-section).The right-hand side of the reaction tray is designatedA, the left-hand side is B
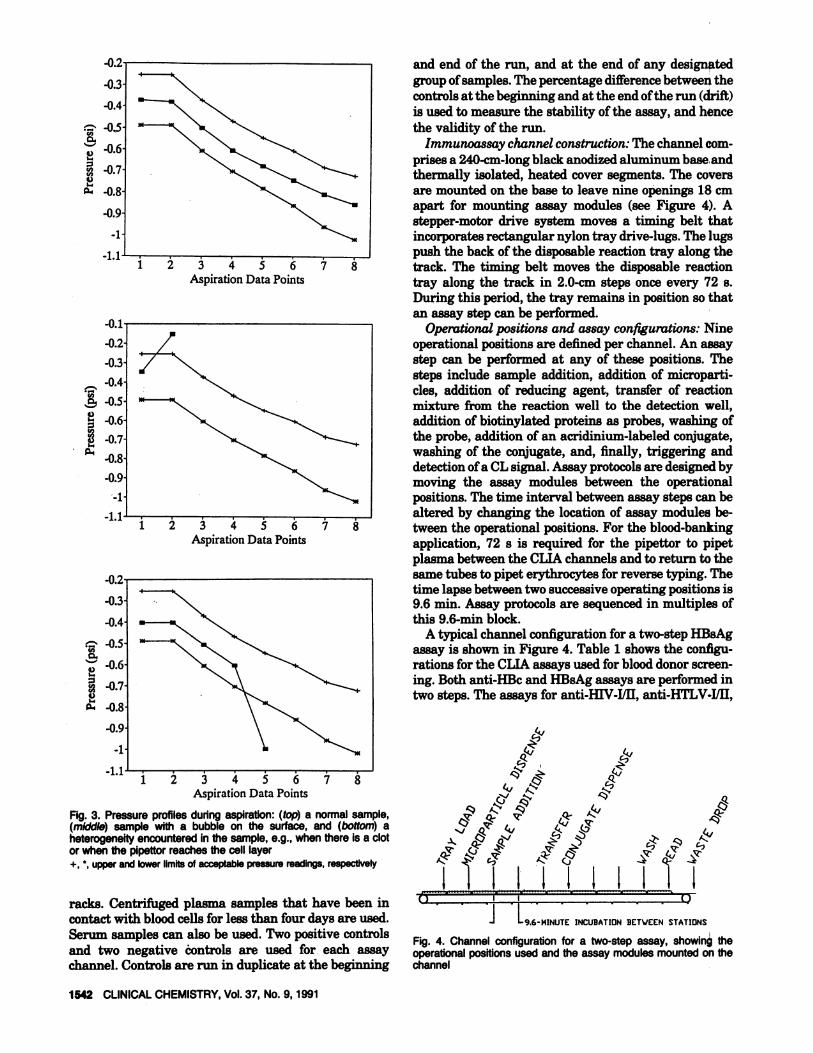
2 is a plot of the pressure difference for a series ofconsecutive pressure readings as the pipet tip is movedtoward the sample, touches the surface, and is thenmoved away from the sample. Each independent z-axismotion is then stopped and the pipettor is stepped intothe sample while the sample is aspirated. The step andaspiration rates are controlled to keep the tip immersedin the fluid at the same depth throughout.
Aspiration is performed in 100-.tL increments. Thepressure difference is measured after each aspirationstep and compared with a range of expected pressures.Readings falling within this pressure window veri1r anormal sample aspiration (Figure 3, top); pressure read-ings falling outside the predetermined window indicatea heterogeneity in the sample. For example, a smallerpressure difference indicates the presence of bubbles(Figure 3, middle); a larger pressure difference indicatesthe presenceof clots or indicates that the plasma volumeis insufficient, such that the pipet tip has reached thepacked cells layer (Figure 3, bottom). In either instance,aspiration of the sample is stopped, and the samplecondition is flagged. Processing of this sample along thechannel is discontinued.
A volume of sample larger than the total required forall the assays is aspirated into the pipet tip. The pipettormoves upward to clear the sample tube and then movesacross the installed channels to dispense the appropri-ate volume into each channel. At the end of the pipet-ting cycle, the pipettor moves to the tip-removal station,where tips are removed and discarded. For instrumentsequipped with a blood-typing channel (agglutinationchannels), the pipettor moves to this channel to dispenseplasma into defined wells of a microtiter plate, thenreturns to the same samples to pick up erythrocytes tobe pipetted for reverse typing.
Samples and controls: Samples in 13 x 100 mm and16 x 100 mm blood-collection tubes are accepted in tube
Cd,
0
U)U)0
p1
10 15 20Pressure Readings
Fig.2. Pressure transducer response as the pipet tip was movedtowardthe sample surface, touched the surface, and was drawnbackNote the sudden change in pressure sensor response as the tip touched thefluid surface
i 343AspirationData Points
23456Aspiration Data Points
7 8
MINUTE INCUBATION BETVEEN STATIONS
1542 CLINICALCHEMISTRY,Vol.37, No.9, 1991
-0.2 and end of the run, and at the end of any designated
-0.3 group of samples. The percentage difference between thecontrols at the beginning and at the end of the run (drift)
-0.4 is used to measure the stability of the assay, and hence‘ -0.5 the validity of the run.
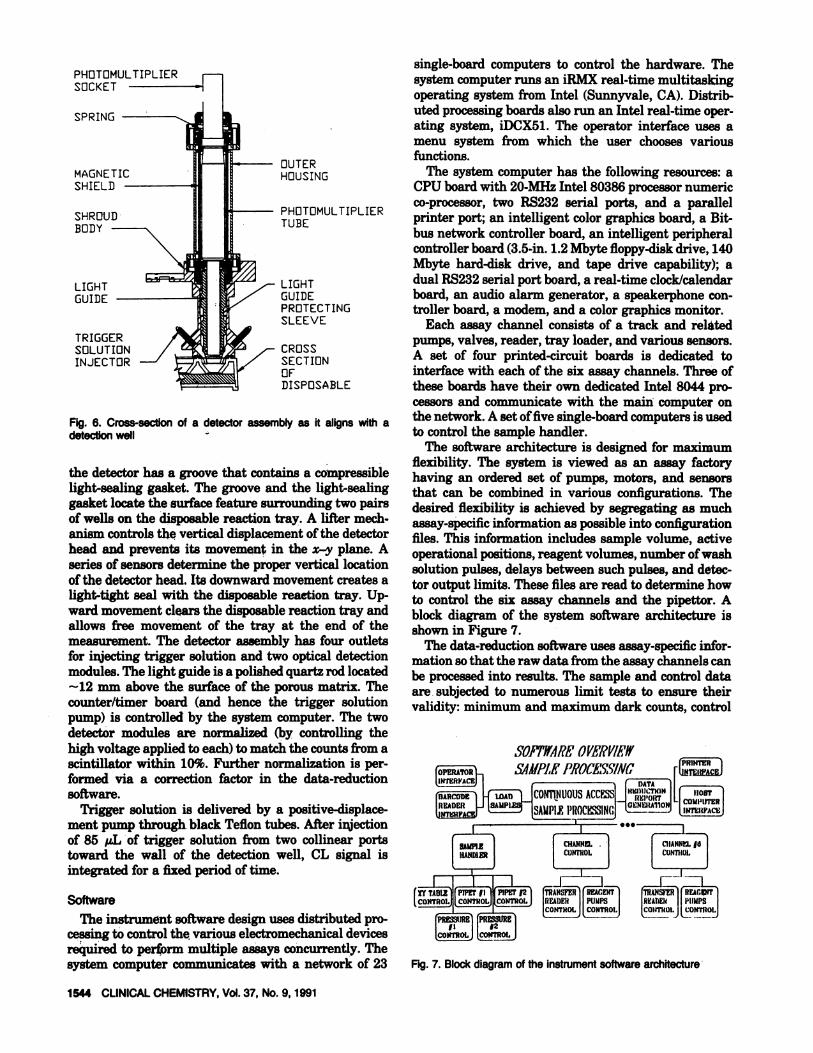
-0.6 Immunoassay channel construction: The channel com-prises a 240-cm-long black anodized aluminum base andthermally isolated, heated cover segments. The covers
-0.8 are mounted on the base to leave nine openings 18 cm
-09 apart for mounting assay modules (see Figure 4). A#{149} stepper-motor drive system moves a timing belt that-1 incorporates rectangular nylon tray drive-lugs. The lugs
-1.1 push the back of the disposable reaction tray along thetrack. The timing belt moves the disposable reactiontray along the track in 2.0-cm steps once every 72 s.During this period, the tray remains in position so thatan assay step can be performed.
-0.1 Operational positions and assay configurations: Nine-0.2 operational positions are defined per channel. An assay
-0.3 step can be performed at any of these positions. The
-04 steps include sample addition, addition of microparti-des, addition of reducing agent, transfer of reaction
0.5 mixture from the reaction well to the detection well,
-0.6 addition of biotinylated proteins as probes, washing of
-0.7 the probe, addition of an acridinium-labeled conjugate,
-08 washing of the conjugate, and, finally, triggering and#{149} detection of a CL signal. Assay protocolsare designed by
0.9 moving the assay modules between the operational-1 positions. The time interval between assay steps can be
-1.1 altered by changing the location of assay modules be-7 8 tween the operational positions. For the blood-banking
application, 72 s is required for the pipettor to pipetplasma between the CLIA channels and to return to the
-02 same tubes to pipet erythrocytes for reverse typing. Thetime lapse between two successiveoperating positions is
-0.3 9.6 miii. Assay protocols are sequenced in multiples of
-0.4 this 9.6-mm block.A typical channel configuration for a two-step HBsAg
-0.5 assay is shown in Figure 4. Table 1 shows the conflgu-
‘‘ -0.6 rations for the CLIA assays used for blood donor screen-
-07 ung.Both anti-HBc and HBsAg assays are performed in#{149} two steps. The assays for anti-HIV-IJll, anti-HTLV-I/II,
Q’ -0.8
-0.9
-1
-1.1 3 4 6
Aspiration Data Points
Fig. 3. Pressure profilesduringaspiration:(top) a normalsample,(middle) sample with a bubble on the surface, and (bottom) aheterogeneityencounteredin the sample,e.g., whenthere is a clotor when the pipettorreachesthe cell layer+, , upper and lower limits of acceptable pressure readings, respectively
racks. Centrifuged plasma samples that have been incontact with blood cells for less than four days are used.Serum samples can also be used. Two positive controls Fig. 4. Channel configuration for a two-step assay, showingtheand two negative controls are used for each assay operationalpositionsusedand the assay modulesmountedon thechannel. Controls are run in duplicate at the beginning channel
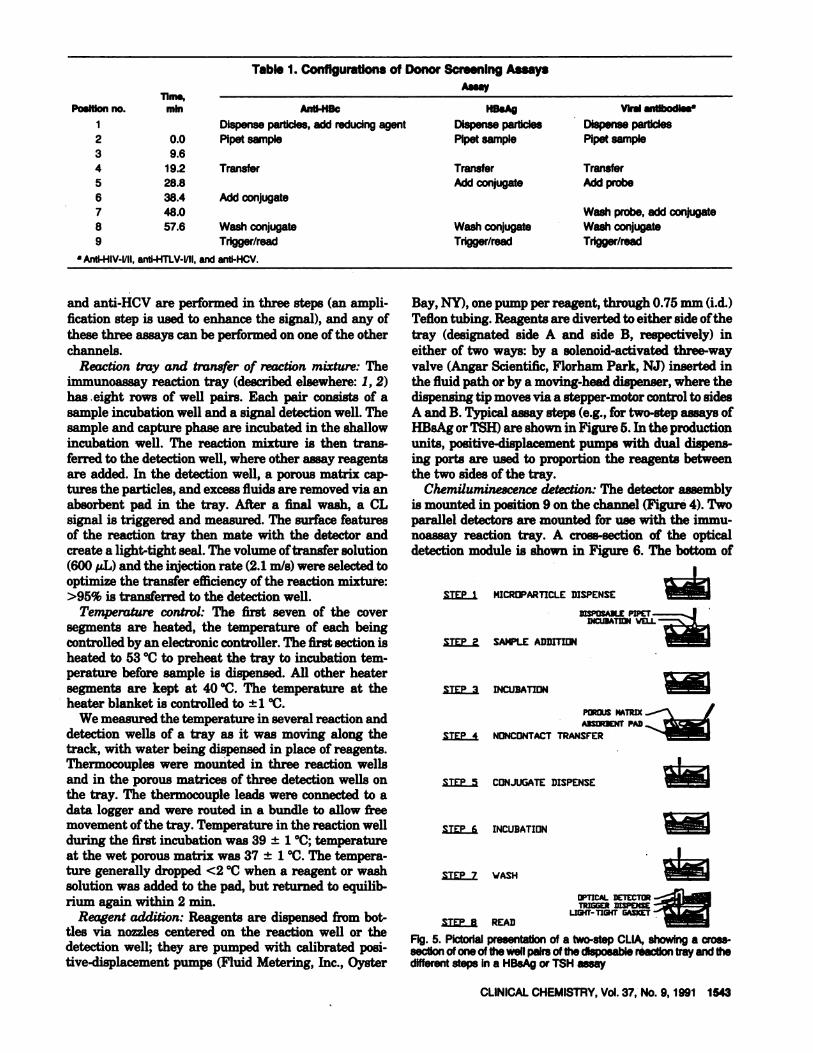
Table 1. ConfIgurations of Donor Screening Assays
Poiftion no
234
56789
lime,mm Anti-NBc
Dispense particles, add reducing agent0.0 Plpet sample
Transfer
Add conjugate
WashconjugateTrigger/read
Wash conjugateTrigger/read
CLINICALCHEMISTRY,Vol.37, No.9, 1991 1543
9.619.228.838.448.057.6
liBsAg
Dispense particlesPipetsample
TransferAdd conjugate
Viral antibOdissa
DispenseparticlesPipetsample
TransferAdd probe
Wash probe, add conjugateWash conjugateTrigger/read
a Anti-HIV-l/lI, anti-HTLV-l/ll, and anti-HCV.
and anti-HCV are performed in three steps (an ampli-fication step is used to enhance the signal), and any ofthese three assays can be performed on one of the otherchannels.
Reaction tray and transfer of reaction mixture: Theimniunoassay reaction tray (described elsewhere: 1,2)
has eight rows of well pairs. Each pair consists of asample incubation well and a signal detection well. Thesample and capture phase are incubated in the shallowincubation well. The reaction mixture is then trans-ferred to the detection well, where other assay reagentsare added. In the detection well, a porous matrix cap-tures the particles, and excess fluids are removed via anabsorbent pad in the tray. After a final wash, a CLsignal is triggered and measured. The surface featuresof the reaction tray then mate with the detector andcreate a light-tight seal. The volume of transfer solution(600 1zL)and the injection rate (2.1 mIs) were selected tooptimize the transfer efficiency of the reaction mixture:>95% is transferred to the detection well.
Temperature control: The first seven of the coversegments are heated, the temperature of each beingcontrolled by an electronic controller. The first section isheated to 53#{176}Cto preheat the tray to incubation tem-perature before sample is dispensed. All other heatersegments are kept at 40#{176}C.The temperature at theheater blanket is controlled to ±1#{176}C.
We measured the temperature in several reaction anddetection wells of a tray as it was moving along thetrack, with water being dispensed in place of reagents.Thermocouples were mounted in three reaction wellsand in the porous matrices of three detection wells onthe tray. The thermocouple leads were connected to adata logger and were routed in a bundle to allow freemovement of the tray. Temperature in the reaction wellduring the first incubation was 39 ± 1#{176}C;temperatureat the wet porous matrix was 37 ± 1#{176}C.The tempera-ture generally dropped <2#{176}Cwhen a reagent or washsolution was added to the pad, but returned to equilib-rium again within 2 miii.
Reagent addition: Reagents are dispensed from bot-tles via nozzles centered on the reaction well or thedetection well; they are pumped with calibrated posi-tive-displacement pumps (Fluid Metering, Inc., Oyster
Bay, NY), one pump per reagent, through 0.75 mm (i.d.)Teflon tubing. Reagents are diverted to either side of thetray (designated side A and side B, respectively) ineither of two ways: by a solenoid-activated three-wayvalve (Angar Scientific, Florhani Park, NJ) inserted inthe fluid path or by a moving-head dispenser, where thedispensing tip moves via a stepper-motor control to sidesA and B. Typical assay steps (e.g., for two-step assays ofHBsAg or TSH) are shown in FigureS. In the productionunits, positive-displacement pumps with dual dispens-ing ports are used to proportion the reagents betweenthe two sides of the tray.
Chemiluminescence detection: The detector assemblyis mounted in position 9 on the channel (Figure 4). Twoparallel detectors are mounted for use with the immu-noassay reaction tray. A cross-section of the opticaldetection module is shown in Figure 6. The bottom of
STEP I MICROPARTICLEDISPENSE
STEP 2 SAMPLE ADDITION
STEP D INCUBATION
DISPOSABLE PIPETcuBAT vW
POPJS MATRIX
STEP 4 NONCONTACT TRANSFERABSBENT PAD
STEP 5 CONJUGATE DISPENSE
STEP INCUBATION
STEP 7 VASH
OPTICAL DETECTITRIGGER DISPENSE
LIT- TICB4T GASKETSTEP B READ
Fig. 5. Pictodal presentation of a two-step CLIA,, showing a cross-section ofone of the well pairs of the disposable reaction tray and thedifferent steps In a HB5Ag or TSH assay
PHOTOMULTIPLIERSOCKET
TRIGGERSOLUTIONINJECTOR
SOP/’JYARZOVgRVfIr _______(JPRINTERL)OPERATOR SAAIPJ PROCi’SSINC IINTERYACE _________
i uO
ICTIONL REI’oR’T -ICOWIER’1SAUPLPROC. INC INTEUPACEI ER?
rHANDIER
1x TAB! 1pipsi,i ) PIPEr Ill1.
(RPSURR1 IPRIS$uRilI I’ II SI It0N!!J 2N!J
CHANNEL
CONTROL
ANSiii I REACi)
DEAlER I PUUPS
tc0NTfbIJ
r6CONTROL
DEAlER II P1BPS
LcTEtJ tONrROj
Fig.7. Block diagram of the instrument softwarearchitecture
1544 CLINICALCHEMISTRY,Vol.37, No.9, 1991
OUTERHOUSING
PHOTOMULTIPLIERTUBE
LIGHTGUIDEPROTECTINGSLEEVE
CROSSSECTIONOFDISPOSABLE
Fig. 6. Cross-sectionof a detectorassemblyas it alignswith adetectionwell
the detector has a groove that contains a compressiblelight-sealing gasket. The groove and the light-sealinggasket locate the surface feature surrounding two pairsof wells on the disposable reaction tray. A lifter mech-anism controls the vertical displacement of the detectorhead and prevents its movement in the x-y plane. Aseries of sensors determine the proper vertical locationof the detector head. Its downward movement creates alight-tight seal with the disposable reaction tray. Up-
ward movement clears the disposable reaction tray andallows free movement of the tray at the end of themeasurement. The detector assembly has four outletsfor injecting trigger solution and two optical detectionmodules. The light guide is a polished quartz rod located-12 mm above the surface of the porous matrix. Thecounter/timer board (and hence the trigger solutionpump) is controlled by the system computer. The twodetector modules are normalized (by controlling thehigh voltage applied to each) to match the counts from ascintillator within 10%. Further normalization is per-formed via a correction factor in the data-reductionsoftware.
Trigger solution is delivered by a positive-displace-ment pump through black Teflon tubes. After injectionof 85 L of trigger solution from two collinear portstoward the wall of the detection well, CL signal isintegrated for a fixed period of time.
Software
The instrument software design uses distributed pro-cessing to control the various electromechanical devicesrequired to perform multiple assays concurrently. Thesystem computer communicates with a network of 23
single-board computers to control the hardware. Thesystem computer runs an iRMX real-time multitaskingoperating system from Intel (Sunnyvale, CA). Distrib-uted processing boards also run an Intel real-time oper-ating system, iDCX51. The operator interface uses a
menu system from which the user chooses variousfunctions.
The system computer has the following resources: aCPU board with 20-MHz Intel 80386 processor numericco-processor, two RS232 serial ports, and a parallelprinter port; an intelligent color graphics board, a Bit-bus network controller board, an intelligent peripheralcontroller board (3.5-in. 1.2 Mbyte floppy-disk drive, 140Mbyte hard-disk drive, and tape drive capability); adual RS232 serial port board, a real-time clock/calendarboard, an audio alarm generator, a speakerphone con-troller board, a modem, and a color graphics monitor.
Each assay channel consists of a track and relatedpumps, valves, reader, tray loader, and various sensors.A set of four printed-circuit boards is dedicated tointerface with each of the six assay channels. Three ofthese boards have their own dedicated Intel 8044 pro-cessors and communicate with the main computer onthe network. A set of five single-board computers is usedto control the sample handler.
The software architecture is designed for maximumflexibility. The system is viewed as an assay factoryhaving an ordered set of pumps, motors, and sensorsthat can be combined in various configurations. Thedesired flexibility is achieved by segregating as muchassay-specificinformation as possible into configurationfiles. This information includes sample volume, activeoperational positions, reagent volumes, number of washsolution pulses, delays between such pulses, and detec-tor output limits. These files are read to determine howto control the six assay channels and the pipettor. Ablock diagram of the system software architecture isshown in Figure 7.
The data-reduction software uses assay-specific infor-mation so that the raw data from the assay channels canbe processed into results. The sample and control dataare subjected to numerous limit tests to ensure theirvalidity: minimum and maximum dark counts, control
particles is dispensed in position 1, 100 L of control orsample in position 2, and 30 pL of acridimum-labeledanti-TSH for each fibrous matrix in position 5; the otherassay steps are the same as for HBsAg. Incubation timesare 19.2 mm for sample and rnicroparticles, and 28.8mm for captured microparticles and acridinium-labeledconjugate. CL signal integration time is 1 s.
Anti-HIV, anti-HC V. and anti -HTL V-i/lI assays: Asin the sandwich assay, 50 pL of antigen-coated micro-particles is dispensed in position 1, 100 L of control orsample in position 2, and the incubated reaction mix-ture is transferred in position 4. In position 5, 30 pL ofbiotinylated antigens (probe) is dispensed onto eachfibrous matrix, the captured reaction product and excessprobe are washed in position 7, and 30 L of acridinium-labeled monoclonal anti-biotin (conjugate) is dispensedonto the washed product. The reaction product iswashed in position 8, and signal is triggered in position9.
Results and Discussion
Accuracy and precision of pipetting: The mean of theweight of 15 replicates of a pipetted sample of bovineserum was calculated for each target volume. CVs<1.6% were obtained for volumes of 60-100 pL. The CVof pipetting volumes >100 zL was <1%.
Detector performance: The performance of the detectorand the integrity of the light seals were checked byusing solid plastic scintillators, polyvinyltoluene poly-mer incorporating [‘4C]benzoic acid (Isotope ProductsLabs., Burbank, CA). The beta-emission excites low-level fluorescence from the vinyltoluene polymer. Eachscintillator was polymerized in an aluminum cup and fitin the detection well of the disposable reaction tray. Theintegrated scintillator counts were measured before thestart of a run. Three intensities of scintillators wereused: 1238, 1912, and 3734 counts/s. The integrated
scintillator counts were measured periodically over aperiod of three weeks; the values for each scintillatorvaried by 2.5%, 1.0%, and 4.42%, respectively, duringthat period.
Results of anti -HBc and HBsAg assays: Precision datafor the anti-HBc assay are given in Table 2. Within-run(n = 14) and between-run CVs (n = 42) were <10% forcontrols with antibody concentration >0.47 Paul Ehr-lich Institute (PEI) unitfmL (Paul Ehrlich Institute,
Frankfurt, F.R.G.). The detection limit for the HBsAg
counts, and expected sample counts as well as thepercentage of front-to-back difference (drift) of bothpositive and negative controls are checked. Nonconfor-mance aborts the data reduction for that assay.
Throughput
The instrument throughput is gated by the pipettorfunction. For blood-screening applications (plasma andcell pipetting), 75 samples can be processed per hour toyield 900 test results per hour. However, using theinstrument as a six-channel CLIA analyzer (no cellpipetting) cuts the pipettor cycle time to 36 s; thisincreases the number of samples processed to 150 perhour, to yield up to 900 test results per hour.
ReagentsCoated microparticles, acridinium-labeled conjugates,
and transfer and wash solutions were from experimen-tal kits prepared for clinical studies (Abbott Labs.,North Chicago, IL) (3-6). Anti-TSH-coated microparti-des, TSH calibrators, and controls were from AbbottIMx kits. Acridinium-labeled anti-TSH was preparedaccording to literature methods (4). Trigger solutionwas prepared daily by dissolving urea peroxide tablets(Abbott) to yield hydrogen peroxide concentration of -3g/L in 0.25 moJJL sodium hydroxide solution.
Assays
Anti-HBc competitive binding assay: With the tray inposition 1, 50 L of a cysteine solution and 50 pL ofHBc-coated microparticles are dispensed into each incu-bation well; 100 pL of control or sample is added inposition 2, and the assay timing is started. Sample andxmcroparticles are mixed by mutual diffusion of eachsolution into the other without external agitation orshaking. In position 4 the reaction mixture is trans-ferred to the detection well after 19.2 mm of incubation.In position 6, 50 L of acridinium-labeled anti-HBc isdispensed onto each fibrous matrix. The tray is furtherincubated, and the transferred microparticles and ex-cessconjugate are washed in position 8. A CL signal istriggered and measured in position 9; signal integrationtime is 6s. Results are expressed as percent inhibition ofthe CL signal:
% Inhibition =
HBsAg sandwich assay: In position 1, 30 L of anti-HBsAg-coated microparticles is dispensed; 200 1.L ofcontrol or sample is dispensed in position 2. The incu-bated reaction mixture is transferred to the detectionwell in position 4. In position 5, 30 pL of acridinium-labeled anti-HBsAg is dispensed onto each fibrous ma-trix. The transferred microparticles and excess conju-gate are washed in position 8, and the CL signal istriggered in position 9; signal integration time is 6 s.Assays of TSH and CEA are performed with this chan-nel configuration: e.g., 30 L of anti-TSH-coated micro-
Table 2. PrecIsion Data for the Antl-HBc Assay
Sample
234
Negativecontrol
[Antl-HBcI,PEI unlts/mL
2.140.750.470.210.0
Grandmean %
Inhibition
CV, %
Withln-run 9.uflb
81.5 2.5 2.958.4 4.8 4.843.9 6.2 6.722.7 11.3 12.7-0.3 (SD = ±3.5) (SD = ±4.3)
= 14, bfl = 42.
CLINICALCHEMISTRY,Vol.37, No.9, 1991 1545
100 x (negative control - sample)
negative control - positive control

0,C
U
0,C
0,
-IC)
0,
0,
0,
C
0,
C
0,C
0,
0,UC
0,0,CE
S0,
[ISHJ milhl.int.unitsll.
Rowno. SldeA
1 9252 981
Side B
10641192
1546 CLINICALCHEMISTRY,Vol.37, No.9, 1991
Table 3. PrecisIon of HBsAg SensitIvIty Panel DataPanel (HB8AgJ, Grand mean Between-run Grand mean Between-run
subtype pg/L signal, counts/S s CV, % signal/noise CV, %
AD 0.74 5032 3.0 5.2 5.3AD 0.41 3422 2.8 3.6 5.0AD 0.31 2655 2.9 2.8 4.3AY 0.67 4707 3.8 4.8 5.0AY 0.44 3619 2.34 3.6 4.6AY 0.14 1909 3.5 2.0 4.8Nogativo 0.0 955 7.1 1.0 7.5control
= 42.
panel is given in Table 3. The data were generated byrepeating the assay of the sensitivity panel samples,and of several aliquots of the negative control, seventimes within a run on both sidesA and B of the channel(n = 14). Between-run CV was calculated from threeindependent runs (n = 42). Within-run and between-runCVs were -5% for samples with concentrations >0.14pg/L. The mean of the CL signal generated from thenegative controls run as samples was 955 counts/6 s(SD= 68, n = 81). The cutoff for the assay was set to twicethe value of the results for the negative controls run assamples: 1910 counts (= mean signal of the negativecontrol samples + 14 SD). Linear-regression analysis ofthe data yields a limit of quantification of 0.166 pg/L forthe Al) (r = 0.998) and 0.154 ug/L for the AY (r = 0.998)antigen subtypes above this set cutoff value.
Carryover in the immunoassays was monitored in aclinical study in a plasma processing center. A stronglypositive sample was observed on one reaction tray.Table 4 list the CL signals from the samples on thesame reaction tray. CL signals generated from negativesamples adjacent to or opposite a highly positive sampleare not statistically different from those for the othernegative samples on the tray. The positive sample wasreassayed in duplicate, giving results of 187 889 and196 671 counts/6 s; the sample was confirmed positiveby neutralization with a known quantity of anti-HBsAgand reassaying.
We used the CLIA to conduct a clinical study withpaid donors’ samples from a plasma processing center.Two channels were tested, for HBsAg and anti-HBc, inparallel. The between-run CV of the HBsAg-negativecontrols was 10.2% (n = 52); for the positive controls, it
Table 4. Carryover Performance of the SystemIntegrated CL signal, counts/S a
3 964 11914 952 10915 942 175635
6 941 1090
7 927 10918 1000 1101
was 4.3% (n = 52); for the control sample, 8.0% (n = 20);and for the HBsAg-negative population, 8.9% (n =
1044). The mean for the negative samples was 12.03 SDbelow the cutoff for the assay. For the anti-HBc channel,the CV of the CL signal for the negative controls was 6%(n = 56); for the control sample, 9.8% (n = 22); and forthe antibody-negative samples, 6.3% (n = 914). Wecalculated the percentage inhibition and set an assaycutoff at 45% of the inhibition value. The mean for thenegative population was 7.34 SD from the assay cutoff.
TSH assay: Figure 8 (top) shows a dose-responsecurve for the TSH assay. The interpolated concentra-tions for the low, medium, and high controls are given inTable 5. Linear-regression analysis of the dilution curvefor the 2.0 milli-int unitsfL TSH calibrator (Figure 8,
6000
00
:__-
0000
1000
0.0 0.2 0.4 0.6 0.0 1.0
(TSH] mull-mt. unlts/L
FIg. 8. Performance oftheCLIAforTSH:(top) dose-response curveandprecision;(boflom) dilutioncurvefor 2.0 mull-mt.unlts/LTSHcalibratordilutedwiththezerocalibrator
CLINICALCHEMISTRY,Vol.37, No.9, 1991 1547
Control
LowMediumHigh
n = 3.
Table 5. Preclslo n of TSH DeterminationsTSH concn, mull-mt. unltalL
Targ.t
0.256.0
50.0
Found Within-run CV, %
0.247 4.75.89 1.7
51.9 1.6
bottom) yields a straight line: integrated signal = 671 +
5438[TSH] (r = 0.9983). The limit of detection, calcu-lated by interpolation to the mean zero dose-responsesignal + 2 SD, is 0.004 milli-int. urnt/L. This valuecompares well with other CLIA assay results of 0.0 15,obtained by using magnetizable microparticles (7), and0.005 obtained with coated tubes (8). The assay of TSHis not optimized, and the nonspecific counts at zeroanalyte concentration may be wash-limited.
In conclusion, we constructed and tested a multichan-nel heterogeneous chemiluminescence immunoassay sys-tem that is free of carryover. The limit for quantifyingHBsAg was <0.2 g/L; for anti-HBc, <0.5 PEI units/mL.The negative population was well separated from thosewith positive results, which decreases the number ofborderline results and unnecessary retesting. In a clini-cal study of HBsAg in a nonselected blood donor popula-tion in two blood banks and a plasma processing center,8964 samples were analyzed with this instrument (6).Seven samples were initially reactive, five of which werereactive in repeat assays; the same five were confirmedpositive by neutralization and overnight enzyme immu-noassay. Thus, assay specificity was 100%. The meansignal-to-noise ratio for the negative population was
separated by 9 SD from the cutoff value of the assay.Although the system is primarily designed to performhigh-sensitivity screening assays for blood-banking ap-plications, preliminary data show that analytes requir-ing wide dynamic range assays such as TSH can also beperformed with this system.
We thank Chester Wood and Mike Routherg for their help withtheelectronics; Robert Jaekel, Rich Wells, Fred Kader,and RobertEnnesser for theirhelp with mechanical problems;Denise Huff forsetting up the clinical studies; Marge Manske for statisticalanalysis; and Jim Butler and Nancy Johnson for experimentalhelp. We also thank Drs. Akhtar Au and John Weare from theassay development team.
References1. Khalil OS, Hanna C, Huff D, Zurek T. Immunoassay devicewith liquid transfer by washing. US patent 5006309,1991.2. Khalil OS,Hanna CF, Huff D, et al. Reaction tray and noncon-tact transfer method for heterogeneous chemiluminescence immu-noassays. Clin Chem 1991;37:1612-7.3. Khalil OS, Zurek T, PepeC, et al. Detection apparatus formultiple heterogeneous chemiluminescence immunoaaaay config-urations. Anal Biochem 1991;196:61-8.4. Wolf-Rogers J, Weare J, Rice K, et al. A chemiluminescentmicroparticle-membrane capture iinmunoassay forthe detection ofantibodies to hepatitis B core antigen. J Immunol Methods1990;133:191-8.5. Wolf.Rogers J, Weare J, Rice K, et al. Chemiluminescentmicroparticle immunoassays for the detection of anti-HBc [Ab-stract]. Transfusion 1989:29:27.6. All A, Coleman C, CugierD, et al. Clinical evaluation of achemiluminescent immunoassay for the detection of H&Ag inhuman plasma [Abstract]. Joint Congress, Amer Assoc of BloodBanks and Inter Soc of Blood Transfusion, Los Angeles, CA,November 1990:16&7. Zucchelli GC, Pilo A, Mansini 5, et al. Methodological evalua-tion of new chemiluminesoence immunoassay for thyrotropin us-ing acridinium-ester labeled antibody. J Biolumin Chemilumin1989;4:620.-6.8. McCapra F, Watmore D, Sumun F, et al. Luminescent labels forimmunoassay from concept to practice [Review]. J BiolununChemilumin 1989;4:51-8.