abdominal ct: necessity, nephropathy, and allergy myths joe lex, md, facep, faaem temple university...
TRANSCRIPT

Abdominal CT: Abdominal CT: Necessity, Nephropathy, Necessity, Nephropathy,
and Allergy Mythsand Allergy Myths
Joe Lex, MD, FACEP, FAAEMJoe Lex, MD, FACEP, FAAEMTemple University School of MedicineTemple University School of Medicine
Philadelphia, PAPhiladelphia, [email protected]
Joe Lex, MD, FACEP, FAAEMJoe Lex, MD, FACEP, FAAEMTemple University School of MedicineTemple University School of Medicine
Philadelphia, PAPhiladelphia, [email protected]

DisclosureDisclosure

Cape Town, SACape Town, SA

July 19 – 22nd
San Diego, California
Four Speakers Only:
Amal Mattu
Ghazala Sharieff
Joe Lex
Greg Henry

Mediterranean Mediterranean Emergency Medicine Emergency Medicine
Congress VCongress V
14-17 September 200914-17 September 2009
Valencia, SpainValencia, Spain
Mediterranean Mediterranean Emergency Medicine Emergency Medicine
Congress VCongress V
14-17 September 200914-17 September 2009
Valencia, SpainValencia, Spain

III Inter-American Conference on
Emergency Medicine –
Buenos Aires
May 2010




ObjectivesObjectives
• Assess the necessity of oral and Assess the necessity of oral and intravenous contrast material intravenous contrast material
• Discuss strategies to avoid Discuss strategies to avoid adverse outcomes from adverse outcomes from intravenous contrastintravenous contrast
• Assess the necessity of oral and Assess the necessity of oral and intravenous contrast material intravenous contrast material
• Discuss strategies to avoid Discuss strategies to avoid adverse outcomes from adverse outcomes from intravenous contrastintravenous contrast

Question #1Question #1
How does oral contrast How does oral contrast affect the accuracy of affect the accuracy of
an abdominal CT scan?an abdominal CT scan?
How does oral contrast How does oral contrast affect the accuracy of affect the accuracy of
an abdominal CT scan?an abdominal CT scan?

Oral ContrastOral Contrast

History of ContrastHistory of Contrast
• ““Step and Scan” replaced by Step and Scan” replaced by helical technologyhelical technology
• Single-beam replaced by multiple Single-beam replaced by multiple beambeam
• Rapid scans eliminate artifact Rapid scans eliminate artifact from movement, respirations, from movement, respirations, peristalsisperistalsis
• ““Step and Scan” replaced by Step and Scan” replaced by helical technologyhelical technology
• Single-beam replaced by multiple Single-beam replaced by multiple beambeam
• Rapid scans eliminate artifact Rapid scans eliminate artifact from movement, respirations, from movement, respirations, peristalsisperistalsis

Importance of ContrastImportance of Contrast
• Many studies show no contrast Many studies show no contrast required in most situationsrequired in most situations
• Confounding variables:Confounding variables:– Scanner: dynamic vs. helical vs. Scanner: dynamic vs. helical vs.
multi-detectormulti-detector
– Contrast: oral vs. IV vs. rectalContrast: oral vs. IV vs. rectal
– Interpreter reliabilityInterpreter reliability
• Many studies show no contrast Many studies show no contrast required in most situationsrequired in most situations
• Confounding variables:Confounding variables:– Scanner: dynamic vs. helical vs. Scanner: dynamic vs. helical vs.
multi-detectormulti-detector
– Contrast: oral vs. IV vs. rectalContrast: oral vs. IV vs. rectal
– Interpreter reliabilityInterpreter reliability

Oral Contrast = Longer StayOral Contrast = Longer Stay
• High volume urban ED: 107,000 High volume urban ED: 107,000 visits / yearvisits / year
• N = 183 patientsN = 183 patients
• Excluded trauma, pediatrics, Excluded trauma, pediatrics, pregnantpregnant
• High volume urban ED: 107,000 High volume urban ED: 107,000 visits / yearvisits / year
• N = 183 patientsN = 183 patients
• Excluded trauma, pediatrics, Excluded trauma, pediatrics, pregnantpregnant
Huynh LN, et al. Emerg Radiol. 2004 Jul; Huynh LN, et al. Emerg Radiol. 2004 Jul; 10(6):310-3.10(6):310-3.

Oral Contrast = Longer StayOral Contrast = Longer Stay
Huynh LN, et al. Emerg Radiol. 2004 Jul; Huynh LN, et al. Emerg Radiol. 2004 Jul; 10(6):310-3.10(6):310-3.
Time from Time from Order to Order to
ScanScan
Average Average Total ED Total ED
StayStay
102 scans: no 102 scans: no oral contrastoral contrast
104 104 minutesminutes
358 358 minutesminutes
81 scans with 81 scans with oral contrastoral contrast
172 172 minutesminutes
599 599 minutesminutes

Oral Contrast: AccuracyOral Contrast: Accuracy
• 118 patients scanned before and 118 patients scanned before and after oral contrastafter oral contrast
• Blinded interpretation by different Blinded interpretation by different radiologistsradiologists
• 118 patients scanned before and 118 patients scanned before and after oral contrastafter oral contrast
• Blinded interpretation by different Blinded interpretation by different radiologistsradiologists
Lee SY, et al. Emerg Radiol. 2006 May; Lee SY, et al. Emerg Radiol. 2006 May; 12(4):150-7. 12(4):150-7.

Oral Contrast: AccuracyOral Contrast: Accuracy
• 11 had normal non-contrast but 11 had normal non-contrast but abnormal contrastabnormal contrast
• 6 had abnormal non-contrast but 6 had abnormal non-contrast but normal contrast scansnormal contrast scans
• 4 had both scans abnormal, but 4 had both scans abnormal, but disagreement over abnormalitydisagreement over abnormality
• 11 had normal non-contrast but 11 had normal non-contrast but abnormal contrastabnormal contrast
• 6 had abnormal non-contrast but 6 had abnormal non-contrast but normal contrast scansnormal contrast scans
• 4 had both scans abnormal, but 4 had both scans abnormal, but disagreement over abnormalitydisagreement over abnormality
Lee SY, et al. Emerg Radiol. 2006 May; Lee SY, et al. Emerg Radiol. 2006 May; 12(4):150-7. 12(4):150-7.

Oral Contrast: AccuracyOral Contrast: Accuracy
• Post-hoc analysis: one true Post-hoc analysis: one true discordant resultdiscordant result
• Unblinded review: disagreement Unblinded review: disagreement due to inter-observer variabilitydue to inter-observer variability
• Other studies: discrepancy rates Other studies: discrepancy rates up to 38%up to 38%
• Post-hoc analysis: one true Post-hoc analysis: one true discordant resultdiscordant result
• Unblinded review: disagreement Unblinded review: disagreement due to inter-observer variabilitydue to inter-observer variability
• Other studies: discrepancy rates Other studies: discrepancy rates up to 38%up to 38%
Lee SY, et al. Emerg Radiol. 2006 May; Lee SY, et al. Emerg Radiol. 2006 May; 12(4):150-7. 12(4):150-7.

Oral Contrast: AppendicitisOral Contrast: Appendicitis
• Meta-analysis: 23 studies of CT Meta-analysis: 23 studies of CT for appendicitisfor appendicitis
• CT without contrast similar to or CT without contrast similar to or better than CT with contrastbetter than CT with contrast
• Meta-analysis: 23 studies of CT Meta-analysis: 23 studies of CT for appendicitisfor appendicitis
• CT without contrast similar to or CT without contrast similar to or better than CT with contrastbetter than CT with contrast
Anderson BA, et al. Am J Surg. 2005 Sep; Anderson BA, et al. Am J Surg. 2005 Sep; 190(3):474-8.190(3):474-8.

Oral Contrast: AppendicitisOral Contrast: Appendicitis
Without Without contrastcontrast
With With contrastcontrast
SensitivitySensitivity 95%95% 92%92%
NPVNPV 96%96% 96%96%
SpecificitySpecificity 97%97% 94%94%
PPVPPV 97%97% 89%89%
AccuracyAccuracy 96%96% 92%92%
Anderson BA, et al. Am J Surg. 2005 Sep; Anderson BA, et al. Am J Surg. 2005 Sep; 190(3):474-8.190(3):474-8.

Oral Contrast: ConclusionOral Contrast: Conclusion
• Many radiologists very Many radiologists very comfortable interpreting studies comfortable interpreting studies without oral contrastwithout oral contrast
• Although oral contrast takes 90 Although oral contrast takes 90 minutes to opacify bowel, it adds minutes to opacify bowel, it adds 3 hours to ED stay3 hours to ED stay
• Many radiologists very Many radiologists very comfortable interpreting studies comfortable interpreting studies without oral contrastwithout oral contrast
• Although oral contrast takes 90 Although oral contrast takes 90 minutes to opacify bowel, it adds minutes to opacify bowel, it adds 3 hours to ED stay3 hours to ED stay

Oral Contrast: ConclusionOral Contrast: Conclusion
• Oral contrast adds little to Oral contrast adds little to accuracyaccuracy
• Local radiologist may not be Local radiologist may not be comfortable interpreting studies comfortable interpreting studies without oral contrastwithout oral contrast
• Oral contrast adds little to Oral contrast adds little to accuracyaccuracy
• Local radiologist may not be Local radiologist may not be comfortable interpreting studies comfortable interpreting studies without oral contrastwithout oral contrast

Intravenous ContrastIntravenous Contrast

Question #2Question #2
How does intravenous How does intravenous contrast affect the contrast affect the
accuracy of an accuracy of an abdominal CT scan?abdominal CT scan?
How does intravenous How does intravenous contrast affect the contrast affect the
accuracy of an accuracy of an abdominal CT scan?abdominal CT scan?

IV Contrast: RisksIV Contrast: Risks
• Associated risksAssociated risks– Allergic and anaphylactoid Allergic and anaphylactoid
reactionsreactions
– Contrast induced nephropathyContrast induced nephropathy
• New scanners adequate to New scanners adequate to diagnose common problems diagnose common problems without IV contrast: appendicitis, without IV contrast: appendicitis, diverticulitis, pancreatitisdiverticulitis, pancreatitis
• Associated risksAssociated risks– Allergic and anaphylactoid Allergic and anaphylactoid
reactionsreactions
– Contrast induced nephropathyContrast induced nephropathy
• New scanners adequate to New scanners adequate to diagnose common problems diagnose common problems without IV contrast: appendicitis, without IV contrast: appendicitis, diverticulitis, pancreatitisdiverticulitis, pancreatitis

IV Contrast: AccuracyIV Contrast: Accuracy
• 164 unenhanced CT of patients 164 unenhanced CT of patients with abdominal painwith abdominal pain
• Diagnosis made in 71 (43%)Diagnosis made in 71 (43%)
• Non-diagnostic given IV contrastNon-diagnostic given IV contrast
• All reviewed by 2 radiologistsAll reviewed by 2 radiologists
• No significant difference with IV No significant difference with IV contrastcontrast
• 164 unenhanced CT of patients 164 unenhanced CT of patients with abdominal painwith abdominal pain
• Diagnosis made in 71 (43%)Diagnosis made in 71 (43%)
• Non-diagnostic given IV contrastNon-diagnostic given IV contrast
• All reviewed by 2 radiologistsAll reviewed by 2 radiologists
• No significant difference with IV No significant difference with IV contrastcontrast
Basak S, et al. Clin Imaging. 2002 Nov-Dec; Basak S, et al. Clin Imaging. 2002 Nov-Dec; 26(6):405-7. 26(6):405-7.

IV Contrast: NecessityIV Contrast: Necessity
• Suspected appendicitis: Suspected appendicitis: unenhanced CT unenhanced CT laparoscopy laparoscopy
• Appendicitis diagnosed…Appendicitis diagnosed………by CT in 83/103 (80.6%)by CT in 83/103 (80.6%)
……at laparoscopy in 87/103 (84.5%)at laparoscopy in 87/103 (84.5%)
• CT sensitivity 95.4%, specificity CT sensitivity 95.4%, specificity 100%100%
• Suspected appendicitis: Suspected appendicitis: unenhanced CT unenhanced CT laparoscopy laparoscopy
• Appendicitis diagnosed…Appendicitis diagnosed………by CT in 83/103 (80.6%)by CT in 83/103 (80.6%)
……at laparoscopy in 87/103 (84.5%)at laparoscopy in 87/103 (84.5%)
• CT sensitivity 95.4%, specificity CT sensitivity 95.4%, specificity 100%100%
in't Hof KH, et al. Br J Surg. 2004 Dec; in't Hof KH, et al. Br J Surg. 2004 Dec; 91(12):1641-5.91(12):1641-5.

IV Contrast: NecessityIV Contrast: Necessity
• Unenhanced CT in 109 patientsUnenhanced CT in 109 patients
• Final diagnosis by surgery or F/U Final diagnosis by surgery or F/U
• 66 TN, 37 TP, 4 FN, 2 FP66 TN, 37 TP, 4 FN, 2 FP– Sensitivity: 90%, Specificity: 97%Sensitivity: 90%, Specificity: 97%
– PPV and NPV: 95%PPV and NPV: 95%
– Accuracy: 94%Accuracy: 94%
• Alternate diagnosis on CT: 22%Alternate diagnosis on CT: 22%
• Unenhanced CT in 109 patientsUnenhanced CT in 109 patients
• Final diagnosis by surgery or F/U Final diagnosis by surgery or F/U
• 66 TN, 37 TP, 4 FN, 2 FP66 TN, 37 TP, 4 FN, 2 FP– Sensitivity: 90%, Specificity: 97%Sensitivity: 90%, Specificity: 97%
– PPV and NPV: 95%PPV and NPV: 95%
– Accuracy: 94%Accuracy: 94%
• Alternate diagnosis on CT: 22%Alternate diagnosis on CT: 22%Lane MJ, et al. AJR Am J Roentgenol. 1997 Lane MJ, et al. AJR Am J Roentgenol. 1997 Feb; 168(2):405-9. Feb; 168(2):405-9.

Conclusions: IV contrastConclusions: IV contrast
• CT technology has evolved CT technology has evolved rapidlyrapidly
• IV contrast adds little to accuracyIV contrast adds little to accuracy
• Local radiologists may not be Local radiologists may not be comfortable interpreting studies comfortable interpreting studies without IV contrastwithout IV contrast
• CT technology has evolved CT technology has evolved rapidlyrapidly
• IV contrast adds little to accuracyIV contrast adds little to accuracy
• Local radiologists may not be Local radiologists may not be comfortable interpreting studies comfortable interpreting studies without IV contrastwithout IV contrast

Radiology Coat of ArmsRadiology Coat of ArmsRadiology Coat of ArmsRadiology Coat of Arms

Allergic ReactionsAllergic Reactions

Adverse Reaction OccurrenceAdverse Reaction Occurrence
• 112,000 patients112,000 patients
• Total reactions: 5.65 %Total reactions: 5.65 %
• 112,000 patients112,000 patients
• Total reactions: 5.65 %Total reactions: 5.65 %
MildMild ModerateModerate SevereSevere
PercentPercent 3.77%3.77% 1.77%1.77% 0.02%0.02%
TotalTotal 42004200 19801980 2222
Shehadi WH. Am J Roentgenol Radium Ther Shehadi WH. Am J Roentgenol Radium Ther Nucl Med. 1975 May;124(1):145-52Nucl Med. 1975 May;124(1):145-52

Question #3Question #3
What is the connection What is the connection between iodine and between iodine and seafood or shellfish seafood or shellfish
allergy and intravenous allergy and intravenous contrast material?contrast material?
What is the connection What is the connection between iodine and between iodine and seafood or shellfish seafood or shellfish
allergy and intravenous allergy and intravenous contrast material?contrast material?

““Iodine Allergy”Iodine Allergy”
• Physiologic impossibilityPhysiologic impossibility
• Iodine essential to lifeIodine essential to life
• Found in thyroid hormones, Found in thyroid hormones, amino acidsamino acids
• Shellfish allergy to muscle Shellfish allergy to muscle protein tropomyosinprotein tropomyosin
• Physiologic impossibilityPhysiologic impossibility
• Iodine essential to lifeIodine essential to life
• Found in thyroid hormones, Found in thyroid hormones, amino acidsamino acids
• Shellfish allergy to muscle Shellfish allergy to muscle protein tropomyosinprotein tropomyosin
Huang SW. Allergy Asthma Proc. 2005 Nov-Huang SW. Allergy Asthma Proc. 2005 Nov-Dec;26(6):468-9. Dec;26(6):468-9.

Seafood AllergySeafood Allergy
• Anaphylactoid, not IgE mediatedAnaphylactoid, not IgE mediated
• No response to skin testingNo response to skin testing
• Recurrence: <25% repeatRecurrence: <25% repeat
• Increased risk: foods, asthma, Increased risk: foods, asthma, hay-fever, hives, drug allergieshay-fever, hives, drug allergies
• No additional risk for seafoodNo additional risk for seafood
• Anaphylactoid, not IgE mediatedAnaphylactoid, not IgE mediated
• No response to skin testingNo response to skin testing
• Recurrence: <25% repeatRecurrence: <25% repeat
• Increased risk: foods, asthma, Increased risk: foods, asthma, hay-fever, hives, drug allergieshay-fever, hives, drug allergies
• No additional risk for seafoodNo additional risk for seafood
Schlifke A, et al. Can J Emerg Med. 2003; Schlifke A, et al. Can J Emerg Med. 2003; 5(3):166-168. 5(3):166-168.

Question #4Question #4
If a patient says “I’m If a patient says “I’m allergic to contrast allergic to contrast
dye,” can’t I just give dye,” can’t I just give some diphenhydramine some diphenhydramine
and steroids before and steroids before they’re injected?they’re injected?
If a patient says “I’m If a patient says “I’m allergic to contrast allergic to contrast
dye,” can’t I just give dye,” can’t I just give some diphenhydramine some diphenhydramine
and steroids before and steroids before they’re injected?they’re injected?

Preventing Adverse ReactionsPreventing Adverse Reactions
• ACR recommendation if history ACR recommendation if history of moderate or severe reactionof moderate or severe reaction
50 mg prednisone 13, 7 & 1 hour prior50 mg prednisone 13, 7 & 1 hour prior
50 mg diphenhydramine 1 hour prior50 mg diphenhydramine 1 hour prior
32 mg methylprednisolone 12 & 2 32 mg methylprednisolone 12 & 2 hours priorhours prior
• ACR recommendation if history ACR recommendation if history of moderate or severe reactionof moderate or severe reaction
50 mg prednisone 13, 7 & 1 hour prior50 mg prednisone 13, 7 & 1 hour prior
50 mg diphenhydramine 1 hour prior50 mg diphenhydramine 1 hour prior
32 mg methylprednisolone 12 & 2 32 mg methylprednisolone 12 & 2 hours priorhours prior
http://www.acr.org/s_acr/bin.asp?TrackID=&SID=1&DID=24981&CID=2131&VID=2&DOC=File.PDF

Does Pretreatment Work?Does Pretreatment Work?
• Meta-analysis: six studiesMeta-analysis: six studies
• Four used antihistaminesFour used antihistamines– Pooled RR: 0.4 (95% CI 0.18–0.9)Pooled RR: 0.4 (95% CI 0.18–0.9)
• Insufficient data for pooled Insufficient data for pooled statistic for corticosteroidsstatistic for corticosteroids– Suggested reduction for Suggested reduction for
methylprednisolonemethylprednisolone
• Meta-analysis: six studiesMeta-analysis: six studies
• Four used antihistaminesFour used antihistamines– Pooled RR: 0.4 (95% CI 0.18–0.9)Pooled RR: 0.4 (95% CI 0.18–0.9)
• Insufficient data for pooled Insufficient data for pooled statistic for corticosteroidsstatistic for corticosteroids– Suggested reduction for Suggested reduction for
methylprednisolonemethylprednisolone
Delaney A, et al. BMC Med Imaging. 2006 Apr Delaney A, et al. BMC Med Imaging. 2006 Apr 27;6:2. 27;6:2.

Does Pretreatment Work?Does Pretreatment Work?
• Steroid pretreatment reduced…Steroid pretreatment reduced………respiratory symptoms from 1.4% respiratory symptoms from 1.4%
to 0.4%to 0.4%
……respiratory and hemodynamic respiratory and hemodynamic symptoms from 0.9% to 0.2%symptoms from 0.9% to 0.2%
• NNT to prevent one severe NNT to prevent one severe reaction: 100 – 150reaction: 100 – 150
• Steroid pretreatment reduced…Steroid pretreatment reduced………respiratory symptoms from 1.4% respiratory symptoms from 1.4%
to 0.4%to 0.4%
……respiratory and hemodynamic respiratory and hemodynamic symptoms from 0.9% to 0.2%symptoms from 0.9% to 0.2%
• NNT to prevent one severe NNT to prevent one severe reaction: 100 – 150reaction: 100 – 150
Tramer MR, et al. BMJ. 2006 Sep 30; Tramer MR, et al. BMJ. 2006 Sep 30; 333(7570):675. 333(7570):675.

ConclusionsConclusions
Pretreatment…Pretreatment…
……in unselected patients not usefulin unselected patients not useful
……recommended in patients with recommended in patients with prior anaphylaxisprior anaphylaxis
……may not prevent severe or life may not prevent severe or life threatening reactionsthreatening reactions
Life threatening reactions rareLife threatening reactions rare
Pretreatment…Pretreatment…
……in unselected patients not usefulin unselected patients not useful
……recommended in patients with recommended in patients with prior anaphylaxisprior anaphylaxis
……may not prevent severe or life may not prevent severe or life threatening reactionsthreatening reactions
Life threatening reactions rareLife threatening reactions rare

Question #5Question #5
What about the patient What about the patient with a history of with a history of
asthma? Does that asthma? Does that increase the risk of an increase the risk of an
allergic reaction?allergic reaction?
What about the patient What about the patient with a history of with a history of
asthma? Does that asthma? Does that increase the risk of an increase the risk of an
allergic reaction?allergic reaction?

Asthmatics and IV contrastAsthmatics and IV contrast
• Risk of serious reaction Risk of serious reaction increased 5-fold in patients with increased 5-fold in patients with asthma, multiple allergiesasthma, multiple allergies
• Rate of serious reactions still Rate of serious reactions still sufficiently low (0.1%) that pre-sufficiently low (0.1%) that pre-medication not advisedmedication not advised
• Risk of serious reaction Risk of serious reaction increased 5-fold in patients with increased 5-fold in patients with asthma, multiple allergiesasthma, multiple allergies
• Rate of serious reactions still Rate of serious reactions still sufficiently low (0.1%) that pre-sufficiently low (0.1%) that pre-medication not advisedmedication not advised
Morcos SK. Br J Radiol. 2005 Aug; Morcos SK. Br J Radiol. 2005 Aug; 78(932):686-93.78(932):686-93.

Question #6Question #6
Should we do a serum Should we do a serum creatinine on everyone creatinine on everyone
before they get an before they get an intravenous contrast intravenous contrast
load?load?
Should we do a serum Should we do a serum creatinine on everyone creatinine on everyone
before they get an before they get an intravenous contrast intravenous contrast
load?load?

Contrast Induced NephropathyContrast Induced Nephropathy
• Definition of CINDefinition of CIN– Absolute Absolute in Cr of 0.5mg/dL in Cr of 0.5mg/dL
– Relative Relative of 25% in 48 hours of 25% in 48 hours
• Biggest risk: preexisting Biggest risk: preexisting Cr Cr exponentially with Crexponentially with Cr
– Baseline Cr <1.5 mg/dL: 2%Baseline Cr <1.5 mg/dL: 2%
– Baseline Cr >2.5 mg/dL: 20%Baseline Cr >2.5 mg/dL: 20%
• Definition of CINDefinition of CIN– Absolute Absolute in Cr of 0.5mg/dL in Cr of 0.5mg/dL
– Relative Relative of 25% in 48 hours of 25% in 48 hours
• Biggest risk: preexisting Biggest risk: preexisting Cr Cr exponentially with Crexponentially with Cr
– Baseline Cr <1.5 mg/dL: 2%Baseline Cr <1.5 mg/dL: 2%
– Baseline Cr >2.5 mg/dL: 20%Baseline Cr >2.5 mg/dL: 20%
Moore RD, et al. Radiology. 1992 Mar; Moore RD, et al. Radiology. 1992 Mar; 182(3):649-55. 182(3):649-55.

When to Check CreatinineWhen to Check Creatinine
• Age > 70 yearsAge > 70 years
• CHFCHF
• CirrhosisCirrhosis
• DiabetesDiabetes
• Multiple Multiple myelomamyeloma
• AnemiaAnemia
• Age > 70 yearsAge > 70 years
• CHFCHF
• CirrhosisCirrhosis
• DiabetesDiabetes
• Multiple Multiple myelomamyeloma
• AnemiaAnemia
• SepsisSepsis
• HypotensionHypotension
• HypertensionHypertension
• Nephrotoxic Nephrotoxic drug: NSAID, drug: NSAID, ACE inhibitor, ACE inhibitor, furosemidefurosemide
• SepsisSepsis
• HypotensionHypotension
• HypertensionHypertension
• Nephrotoxic Nephrotoxic drug: NSAID, drug: NSAID, ACE inhibitor, ACE inhibitor, furosemidefurosemide

Question #7Question #7
Can I prevent contrast-Can I prevent contrast-induced nephropathy induced nephropathy by giving the patient by giving the patient
NAC or bicarb or NAC or bicarb or something else?something else?
Can I prevent contrast-Can I prevent contrast-induced nephropathy induced nephropathy by giving the patient by giving the patient
NAC or bicarb or NAC or bicarb or something else?something else?

What DOESN’T WorkWhat DOESN’T Work
Diuresis: mannitol, furosemideDiuresis: mannitol, furosemide
• ““Flush” contrast through kidneysFlush” contrast through kidneys
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate
Diuresis: mannitol, furosemideDiuresis: mannitol, furosemide
• ““Flush” contrast through kidneysFlush” contrast through kidneys
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate
Solomon R, et al. N Engl J Med 1994 Nov 24; Solomon R, et al. N Engl J Med 1994 Nov 24; 331(21):1416-30331(21):1416-30

What DOESN’T WorkWhat DOESN’T Work
Common vasodilators: Common vasodilators: dopamine, fenoldopamdopamine, fenoldopam
• Increase renal flowIncrease renal flow
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate
Common vasodilators: Common vasodilators: dopamine, fenoldopamdopamine, fenoldopam
• Increase renal flowIncrease renal flow
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate
Stone GW et al. Rev Cardiovasc Med. 2001;2 Stone GW et al. Rev Cardiovasc Med. 2001;2 Suppl 1:S31-6. Suppl 1:S31-6.

What DOESN’T WorkWhat DOESN’T Work
Other vasodilators: atrial Other vasodilators: atrial natriuretic peptide, calcium natriuretic peptide, calcium channel blockers, ACE- channel blockers, ACE- inhibitors, endothelin receptor inhibitors, endothelin receptor antagonistsantagonists
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate
Other vasodilators: atrial Other vasodilators: atrial natriuretic peptide, calcium natriuretic peptide, calcium channel blockers, ACE- channel blockers, ACE- inhibitors, endothelin receptor inhibitors, endothelin receptor antagonistsantagonists
• Intuitively make sinceIntuitively make since
• Actually increase CIN rateActually increase CIN rate

What DOESN’T WorkWhat DOESN’T Work
Aminophylline / theophyllineAminophylline / theophylline
• Several studiesSeveral studies
• Results conflictingResults conflicting
Aminophylline / theophyllineAminophylline / theophylline
• Several studiesSeveral studies
• Results conflictingResults conflicting
Pannu N et al. JAMA 2006 Jun 21; Pannu N et al. JAMA 2006 Jun 21; 295(23):2765-69 295(23):2765-69

What DOESN’T WorkWhat DOESN’T Work
Aminophylline / theophyllineAminophylline / theophylline
““Theophylline may reduce the Theophylline may reduce the incidence of CIN with an efficacy incidence of CIN with an efficacy that is perhaps comparable to that is perhaps comparable to that reported in studies of N-that reported in studies of N-acetylcysteine. However, findings acetylcysteine. However, findings are inconsistent across studies.”are inconsistent across studies.”
Aminophylline / theophyllineAminophylline / theophylline
““Theophylline may reduce the Theophylline may reduce the incidence of CIN with an efficacy incidence of CIN with an efficacy that is perhaps comparable to that is perhaps comparable to that reported in studies of N-that reported in studies of N-acetylcysteine. However, findings acetylcysteine. However, findings are inconsistent across studies.”are inconsistent across studies.”
Bagshaw SM, et al. Arch Intern Med. 2005 Bagshaw SM, et al. Arch Intern Med. 2005 May 23;165(10):1087-93.May 23;165(10):1087-93.

Preventing CINPreventing CIN
NSS better than D5½NSNSS better than D5½NS
• 1620 patients for angiography1620 patients for angiography
• D5½NS: 2.0% incidence CIND5½NS: 2.0% incidence CIN
• NSS: 0.7% incidence of CINNSS: 0.7% incidence of CIN
NSS better than D5½NSNSS better than D5½NS
• 1620 patients for angiography1620 patients for angiography
• D5½NS: 2.0% incidence CIND5½NS: 2.0% incidence CIN
• NSS: 0.7% incidence of CINNSS: 0.7% incidence of CIN
Mueller C, et al. Arch Intern Med. 2002 Feb 11; Mueller C, et al. Arch Intern Med. 2002 Feb 11; 162(3):329-36.162(3):329-36.
Preventing CINPreventing CIN
NaHCO3 better than NSS (??)NaHCO3 better than NSS (??)
• Replace 150mL in 1 liter DReplace 150mL in 1 liter D55W W
with three amps of NaHCOwith three amps of NaHCO33
• Infuse 3 mL/kg for 1 hour before Infuse 3 mL/kg for 1 hour before and 1 mL/kg for 6 hours after and 1 mL/kg for 6 hours after contrast administrationcontrast administration
• CIN reduced from 13.6% to 1.7%CIN reduced from 13.6% to 1.7%
NaHCO3 better than NSS (??)NaHCO3 better than NSS (??)
• Replace 150mL in 1 liter DReplace 150mL in 1 liter D55W W
with three amps of NaHCOwith three amps of NaHCO33
• Infuse 3 mL/kg for 1 hour before Infuse 3 mL/kg for 1 hour before and 1 mL/kg for 6 hours after and 1 mL/kg for 6 hours after contrast administrationcontrast administration
• CIN reduced from 13.6% to 1.7%CIN reduced from 13.6% to 1.7%Merten GJ, et al. JAMA. 2004 May 19; Merten GJ, et al. JAMA. 2004 May 19; 291(19):2328-34. 291(19):2328-34.

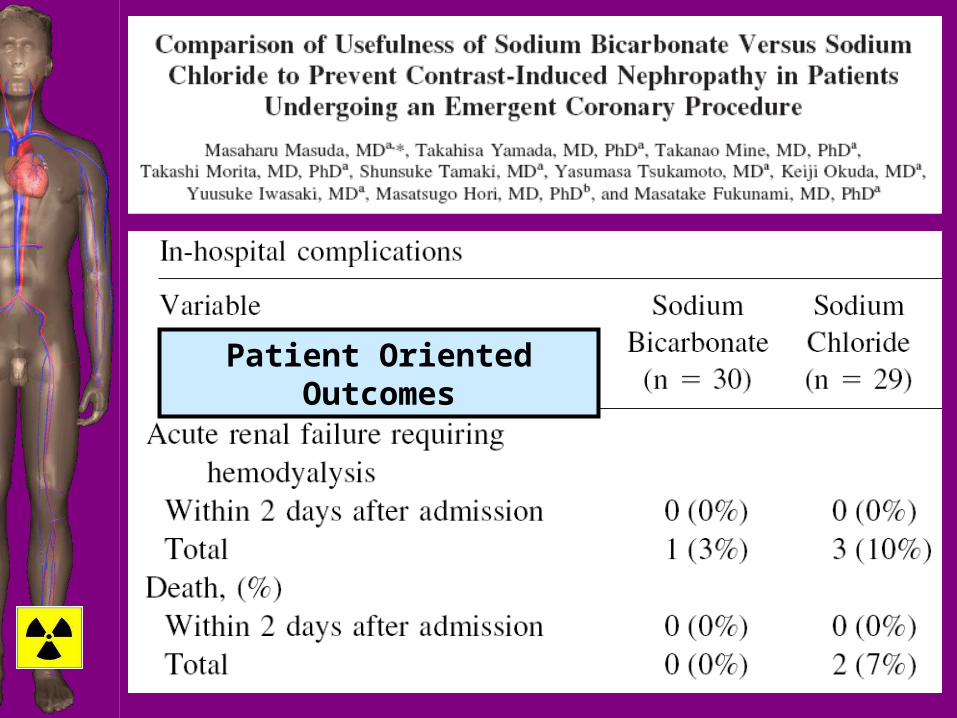
Patient Oriented Outcomes


Preventing CINPreventing CIN
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• Suggest NAC does nothing to Suggest NAC does nothing to prevent CINprevent CIN
• Rather it interferes with proper Rather it interferes with proper measurement of serum Crmeasurement of serum Cr
• DOE rather than POEM??DOE rather than POEM??
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• Suggest NAC does nothing to Suggest NAC does nothing to prevent CINprevent CIN
• Rather it interferes with proper Rather it interferes with proper measurement of serum Crmeasurement of serum Cr
• DOE rather than POEM??DOE rather than POEM??
Hoffman U et al. J Am Soc Nephrol. 2004 Hoffman U et al. J Am Soc Nephrol. 2004 Feb; 15(2):407-410.Feb; 15(2):407-410.

Preventing CINPreventing CIN
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• 87 adults with renal insufficiency 87 adults with renal insufficiency
• Half received 900-mg injection of Half received 900-mg injection of NAC one hour before and NAC one hour before and another immediately after another immediately after contrast medium injectedcontrast medium injected
• Other half: hydration onlyOther half: hydration only
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• 87 adults with renal insufficiency 87 adults with renal insufficiency
• Half received 900-mg injection of Half received 900-mg injection of NAC one hour before and NAC one hour before and another immediately after another immediately after contrast medium injectedcontrast medium injected
• Other half: hydration onlyOther half: hydration only
Poletti PA, et al. AJR Am J Roentgenol. 2007 Poletti PA, et al. AJR Am J Roentgenol. 2007 Sep;189(3):687-92. Sep;189(3):687-92.

Preventing CINPreventing CIN
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• Serum creatinine and cystatin C Serum creatinine and cystatin C measured at admission and on measured at admission and on days 2 and 4 after CT days 2 and 4 after CT
• 25% or greater increase in SCr in 25% or greater increase in SCr in 9/43 (21%) in control group and 9/43 (21%) in control group and in 2/44 (5%) in NAC groupin 2/44 (5%) in NAC group
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• Serum creatinine and cystatin C Serum creatinine and cystatin C measured at admission and on measured at admission and on days 2 and 4 after CT days 2 and 4 after CT
• 25% or greater increase in SCr in 25% or greater increase in SCr in 9/43 (21%) in control group and 9/43 (21%) in control group and in 2/44 (5%) in NAC groupin 2/44 (5%) in NAC group
Poletti PA, et al. AJR Am J Roentgenol. 2007 Poletti PA, et al. AJR Am J Roentgenol. 2007 Sep;189(3):687-92. Sep;189(3):687-92.

Preventing CINPreventing CIN
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• 25% or greater increase in 25% or greater increase in cystatin C concentration in 9/40 cystatin C concentration in 9/40 (22%) in control group and in (22%) in control group and in 7/41 (17%) in NAC group7/41 (17%) in NAC group
N-acetylcysteine (NAC)N-acetylcysteine (NAC)
• 25% or greater increase in 25% or greater increase in cystatin C concentration in 9/40 cystatin C concentration in 9/40 (22%) in control group and in (22%) in control group and in 7/41 (17%) in NAC group7/41 (17%) in NAC group
Poletti PA, et al. AJR Am J Roentgenol. 2007 Poletti PA, et al. AJR Am J Roentgenol. 2007 Sep;189(3):687-92. Sep;189(3):687-92.

CIN: ConclusionsCIN: Conclusions
• Virtually all studies require Virtually all studies require pretreatment 12 hours or more in pretreatment 12 hours or more in advance of procedureadvance of procedure
• Hydration helps: no controversyHydration helps: no controversy
• NAC impractical for EM practice, NAC impractical for EM practice, MAY helpMAY help
• Bicarbonate: no protectionBicarbonate: no protection
• Vitamin C: no protectionVitamin C: no protection
• Virtually all studies require Virtually all studies require pretreatment 12 hours or more in pretreatment 12 hours or more in advance of procedureadvance of procedure
• Hydration helps: no controversyHydration helps: no controversy
• NAC impractical for EM practice, NAC impractical for EM practice, MAY helpMAY help
• Bicarbonate: no protectionBicarbonate: no protection
• Vitamin C: no protectionVitamin C: no protection

Question #7Question #7
What if my patient What if my patient takes metformin?takes metformin?
What if my patient What if my patient takes metformin?takes metformin?

Metformin and IV ContrastMetformin and IV Contrast
• Metformin-associated lactic Metformin-associated lactic acidosis (MALA): complication acidosis (MALA): complication
• Recommendation #1: withhold Recommendation #1: withhold metformin 48h before IV contrastmetformin 48h before IV contrast
• Recommendation, modified: Recommendation, modified: withhold metformin for 48h after withhold metformin for 48h after IV contrast IV contrast
• Metformin-associated lactic Metformin-associated lactic acidosis (MALA): complication acidosis (MALA): complication
• Recommendation #1: withhold Recommendation #1: withhold metformin 48h before IV contrastmetformin 48h before IV contrast
• Recommendation, modified: Recommendation, modified: withhold metformin for 48h after withhold metformin for 48h after IV contrast IV contrast

Metformin Contraindications Metformin Contraindications
• HypersensitivityHypersensitivity• DKADKA• Diabetic comaDiabetic coma• Chronic liver Chronic liver
diseasedisease• CHFCHF• Vitamin B-12 Vitamin B-12
deficiencydeficiency
• HypersensitivityHypersensitivity• DKADKA• Diabetic comaDiabetic coma• Chronic liver Chronic liver
diseasedisease• CHFCHF• Vitamin B-12 Vitamin B-12
deficiencydeficiency
• Recent MIRecent MI
• ShockShock
• Severe Severe systemic systemic diseasedisease
• Pulmonary Pulmonary insufficiencyinsufficiency
• Recent MIRecent MI
• ShockShock
• Severe Severe systemic systemic diseasedisease
• Pulmonary Pulmonary insufficiencyinsufficiency

MALAMALA
Comprehensive review: 18 casesComprehensive review: 18 cases
• Literature reviewLiterature review
• Data reported to manufacturersData reported to manufacturers
• Reports to FDAReports to FDA
Comprehensive review: 18 casesComprehensive review: 18 cases
• Literature reviewLiterature review
• Data reported to manufacturersData reported to manufacturers
• Reports to FDAReports to FDA
McCartney MM, et al. Clin Radiol. 1999 Jan; McCartney MM, et al. Clin Radiol. 1999 Jan; 54(1):29-33.54(1):29-33.

MALAMALA
• Most were taking metformin Most were taking metformin despite contraindicationsdespite contraindications
• Exactly Exactly one caseone case of MALA of MALA reported in patient with normal reported in patient with normal renal functionrenal function
• Most were taking metformin Most were taking metformin despite contraindicationsdespite contraindications
• Exactly Exactly one caseone case of MALA of MALA reported in patient with normal reported in patient with normal renal functionrenal function
McCartney MM, et al. Clin Radiol. 1999 Jan; McCartney MM, et al. Clin Radiol. 1999 Jan; 54(1):29-33.54(1):29-33.

MALA: ConclusionMALA: Conclusion
• Although evidence is scanty, it is Although evidence is scanty, it is prudent to withhold metformin for prudent to withhold metformin for 48 hours following contrast study48 hours following contrast study
• Although evidence is scanty, it is Although evidence is scanty, it is prudent to withhold metformin for prudent to withhold metformin for 48 hours following contrast study48 hours following contrast study
Some Final ThoughtsSome Final Thoughts
• Much has changed from early Much has changed from early days of CT scanningdays of CT scanning
• What was accepted ten years What was accepted ten years ago is no longer trueago is no longer true
• Talk with your radiologists Talk with your radiologists about their comfort levelsabout their comfort levels
• Much has changed from early Much has changed from early days of CT scanningdays of CT scanning
• What was accepted ten years What was accepted ten years ago is no longer trueago is no longer true
• Talk with your radiologists Talk with your radiologists about their comfort levelsabout their comfort levels

Some Final ThoughtsSome Final Thoughts
• There is probably no way to There is probably no way to prevent allergic reactionsprevent allergic reactions
• There may be no way to There may be no way to prevent CIN in ED patientsprevent CIN in ED patients
• There is probably no way to There is probably no way to prevent allergic reactionsprevent allergic reactions
• There may be no way to There may be no way to prevent CIN in ED patientsprevent CIN in ED patients
