abg lecture
TRANSCRIPT

Arterial Blood GasIM 2013 (AVM)
COMPONENTS OF AN ABGpH
Measurement of acidity or alkalinity, based on the hydrogen (H+) ions present.
Negative log of the free H+ ion concentration
The normal range is 7.35 to 7.45
COMPONENTS OF AN ABGPaO2
The partial pressure of oxygen that is dissolved in arterial blood.
The normal range is 80 to 100 mm Hg.
SaO2
The arterial oxygen saturation.
The normal range is 95% to 100%.
COMPONENTS OF AN ABGPaCO2
The amount of carbon dioxide dissolved in arterial blood.
Normal range is 35 to 45 mm Hg (40 + 5)
COMPONENTS OF AN ABGHCO3
The calculated value of the amount of bicarbonate in the bloodstream.
The normal range is 22 to 26 mEq/liter (24 + 2)
B.E.
The base excess indicates the amount of excess or insufficient level of bicarbonate in the system.
The normal range is –2 to +2 mEq/liter (0 + 2).
(A negative base excess indicates a base deficit in the blood.)
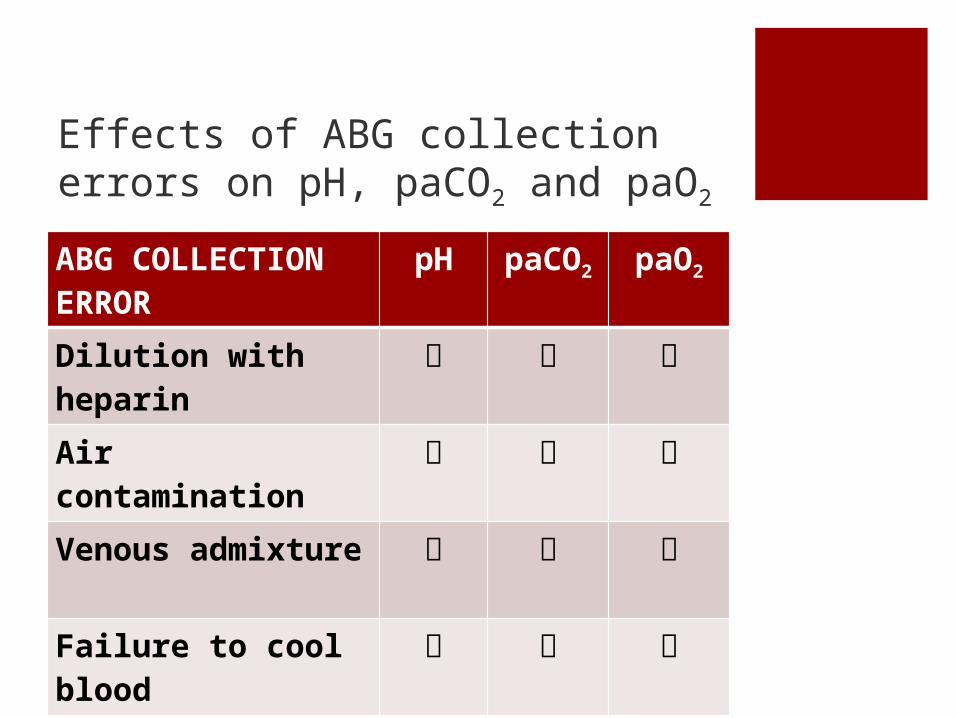
Effects of ABG collection errors on pH, paCO2 and paO2
ABG COLLECTION ERROR
pH paCO2
paO2
Dilution with heparin
Air contamination
Venous admixture
Failure to cool blood
STEPWISE APPROACHObtain clues from the clinical setting
Determine primary disorder
Check the compensatory response
Calculate the anion gap
Calculate the delta/deltas
Identify specific etiologies for the acid-base disorder
Prescribe treatment
DETERMINE CLUES FROM THE
CLINICAL SETTING
CLUES FROM CLINICAL SETTING
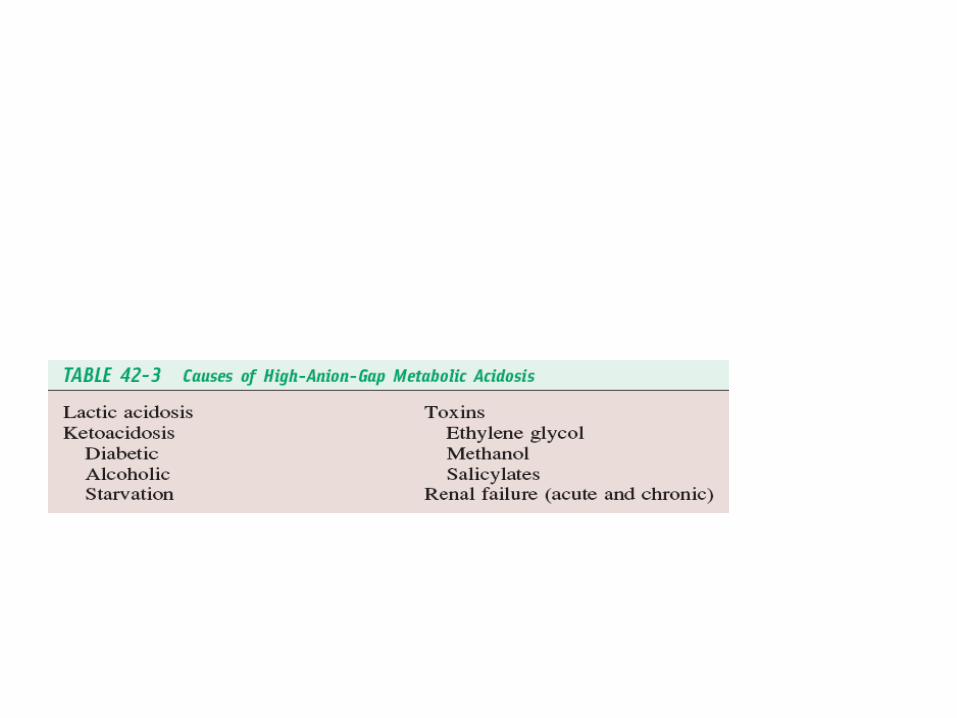
HIGH ANION GAP METABOLIC ACIDOSIS
HIGH AG, normal Cl
Lactic acidosis
Ketoacidosis
Ingestions; alcohol, INH, methanol, ethylene glycol
Renal failure
Massive rhabdomyolysis
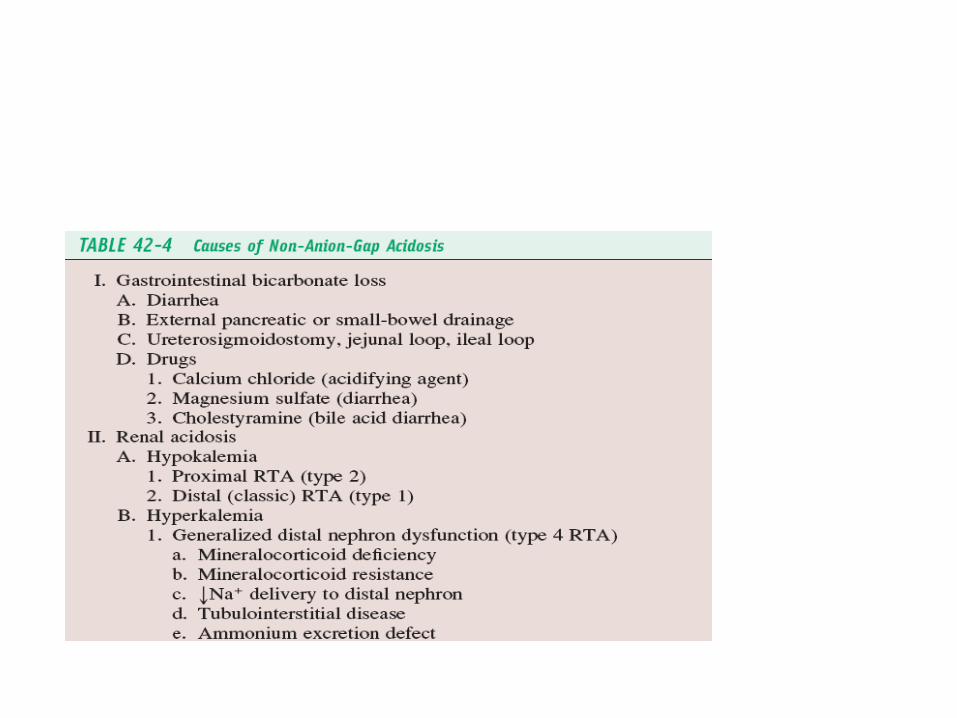
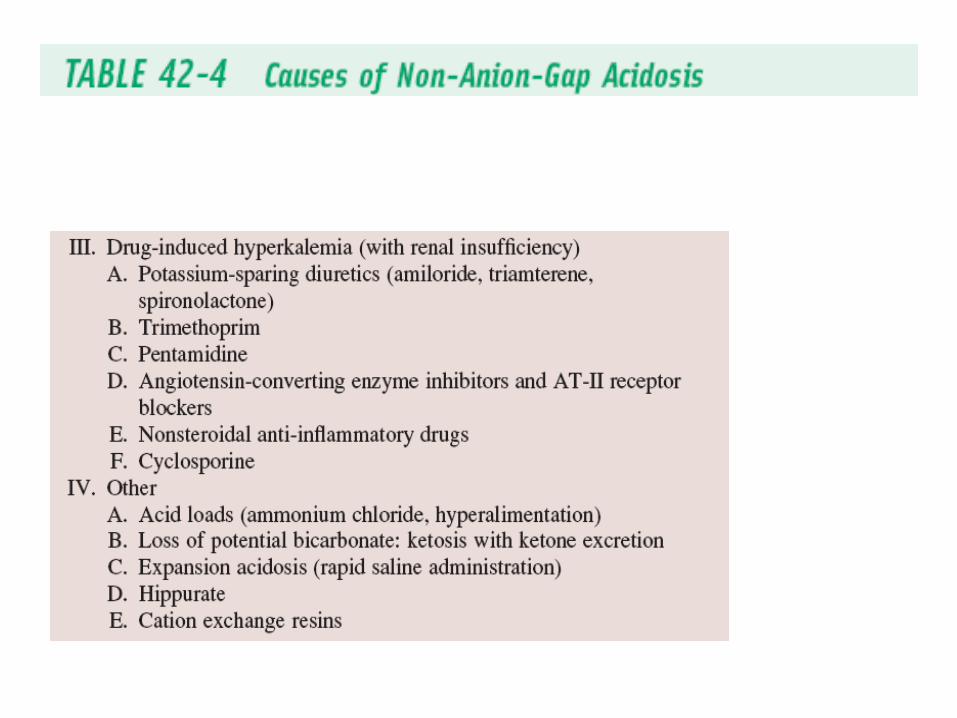
CLUES FROM CLINICAL SETTINGNORMAL ANION GAP METABOLIC ACIDOSIS
Normal AG, HIGH Cl
Diarrhea- GI loss of HCO3
RTA- renal loss of HCO3
Ingestion of ammonium chloride or hyperalimentation fluids
Acetazolamide therapy
CLUES FROM CLINICAL SETTING
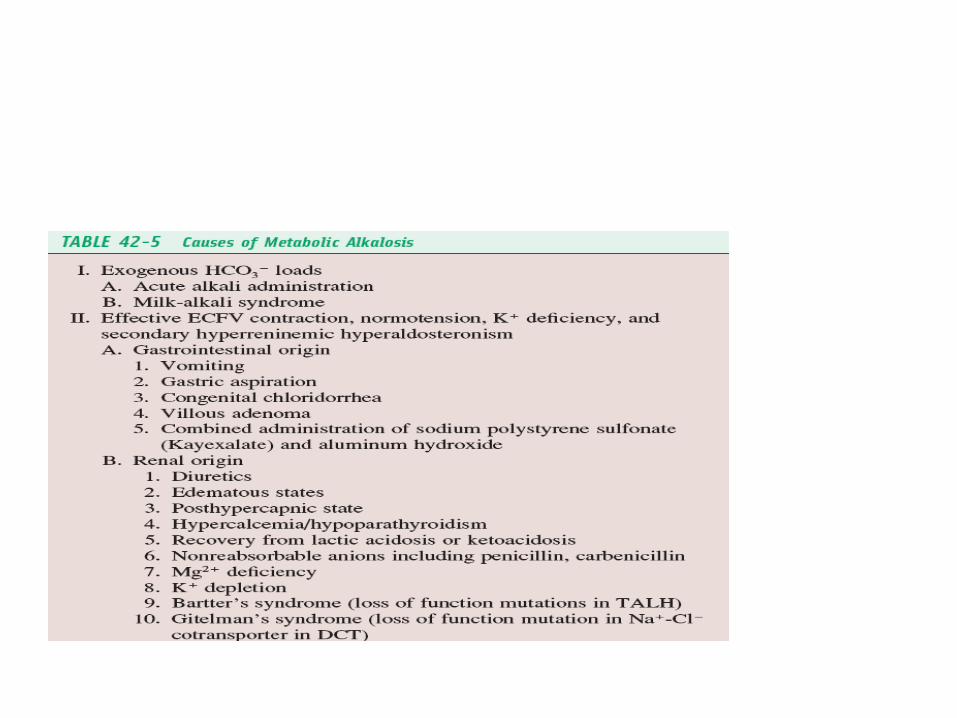
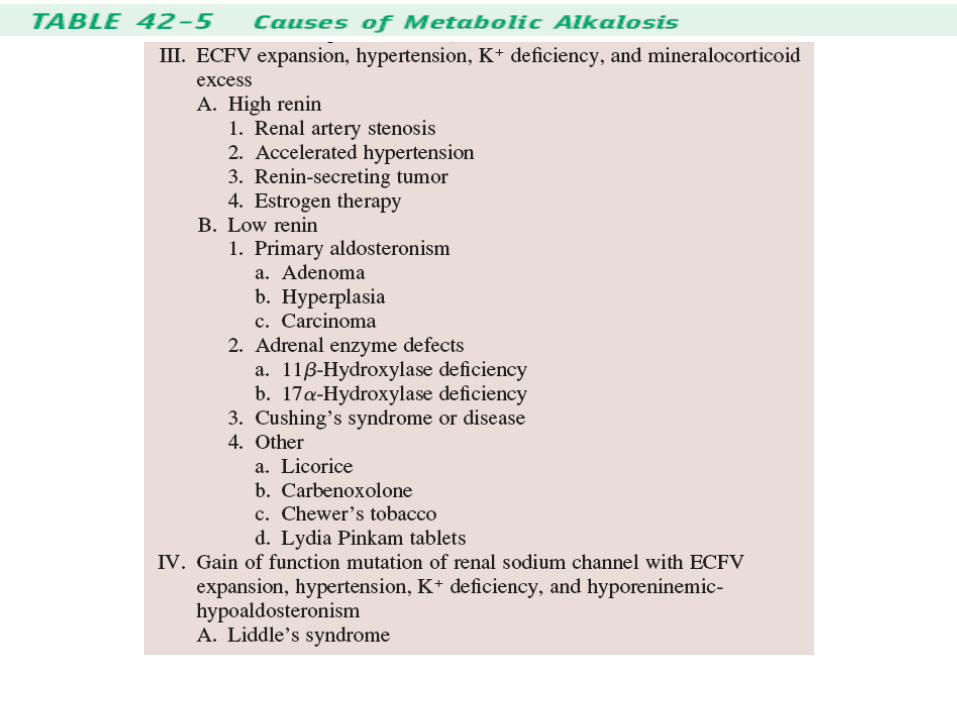
METABOLIC ALKALOSIS
(urine Cl < 10 mEq/d)
Vomiting
Remote diuretic use
Post hypercapnea
Chronic diarrhea
Cystic fibrosis
CLUES FROM CLINICAL SETTING
METABOLIC ALKALOSIS
(urine Cl > 10 mEq/d)
Bartter’s syndrome
Severe potassium depletion
Current diuretic use
Hypercalcemia
Hyperaldosteronism
Cushing’s syndrome
CLUES FROM CLINICAL SETTING
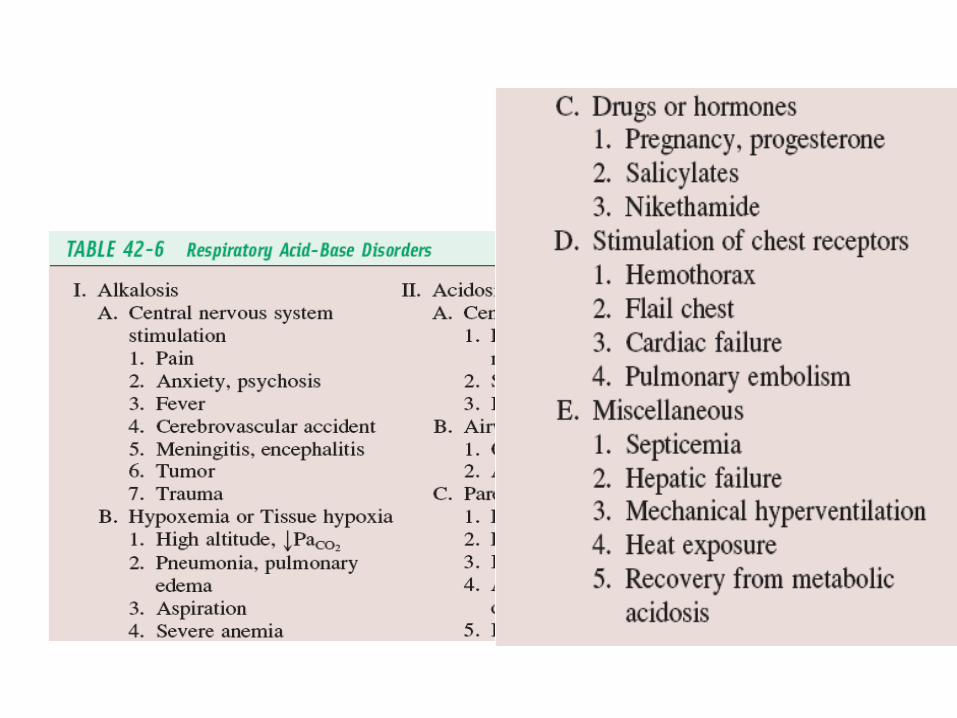
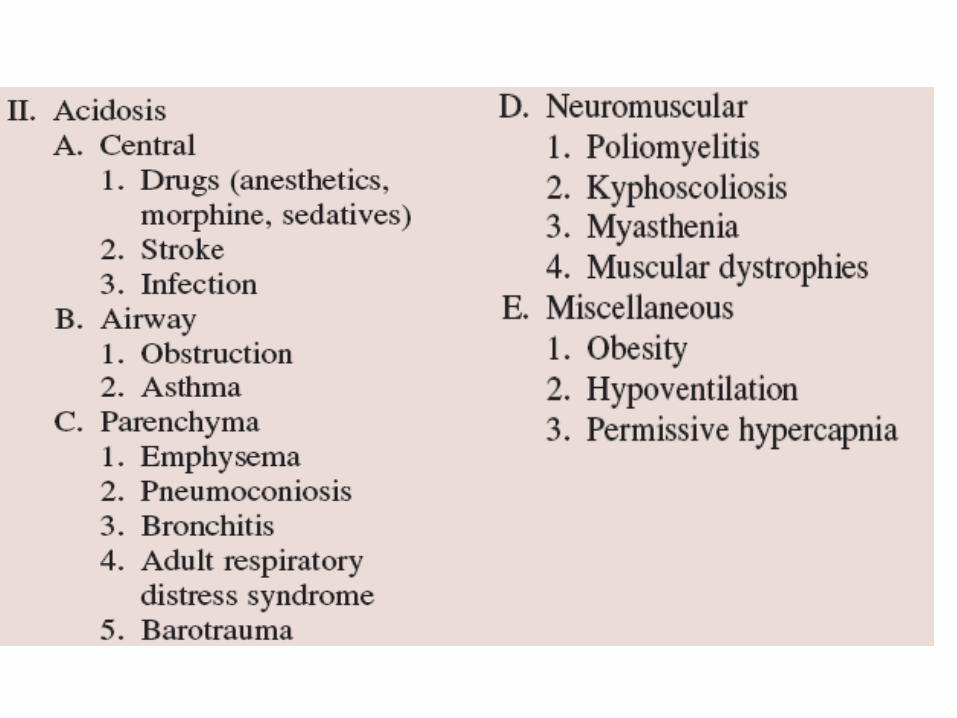
RESPIRATORY ACIDOSIS
CHRONIC: COPD
ACUTE: pneumonia
RESPIRATORY ALKALOSIS
Hyperventilation
DETERMINE THE
PRIMARY DISORDER
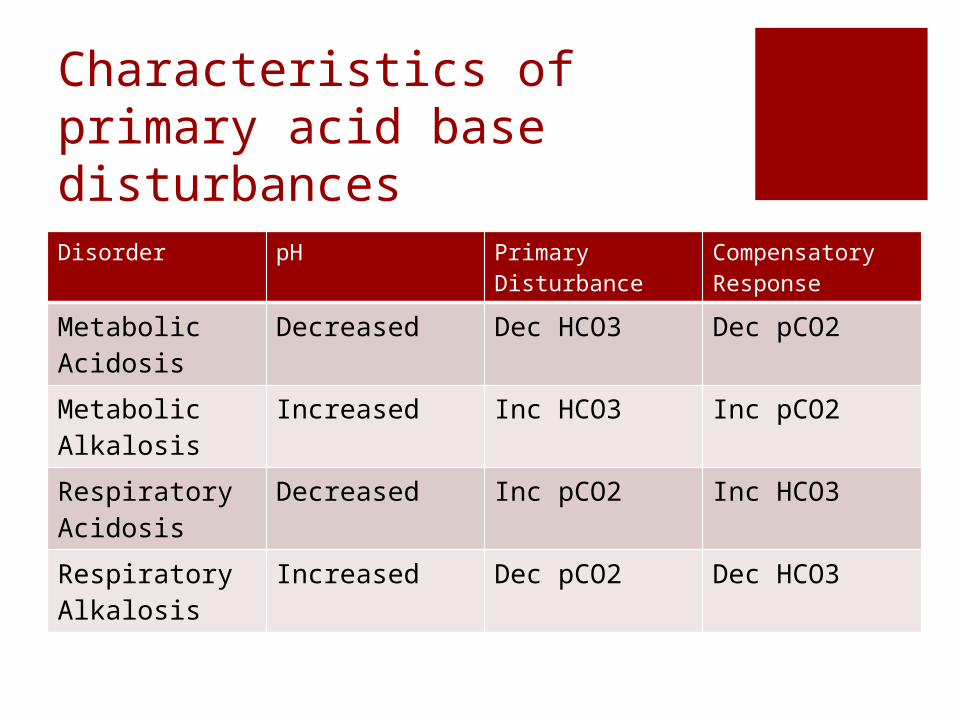
Characteristics of primary acid base disturbancesDisorder pH Primary
DisturbanceCompensatory Response
Metabolic Acidosis
Decreased Dec HCO3 Dec pCO2
Metabolic Alkalosis
Increased Inc HCO3 Inc pCO2
Respiratory Acidosis
Decreased Inc pCO2 Inc HCO3
Respiratory Alkalosis
Increased Dec pCO2 Dec HCO3
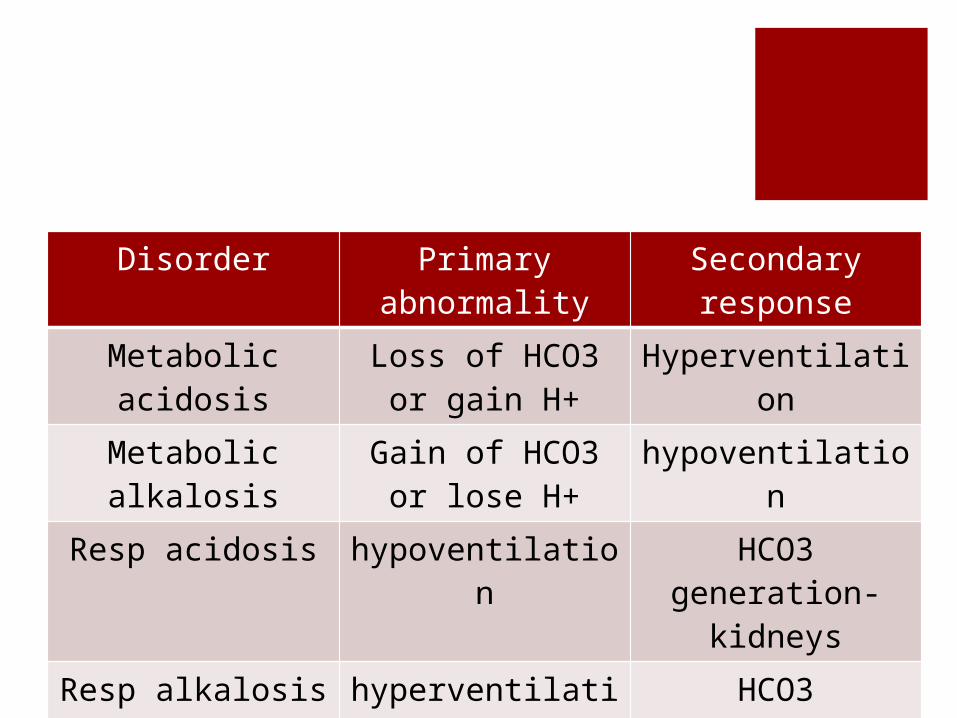
Disorder Primary abnormality
Secondary response
Metabolic acidosis Loss of HCO3 or gain H+
Hyperventilation
Metabolic alkalosis Gain of HCO3 or lose H+
hypoventilation
Resp acidosis hypoventilation HCO3 generation- kidneys
Resp alkalosis hyperventilation HCO3 consumption
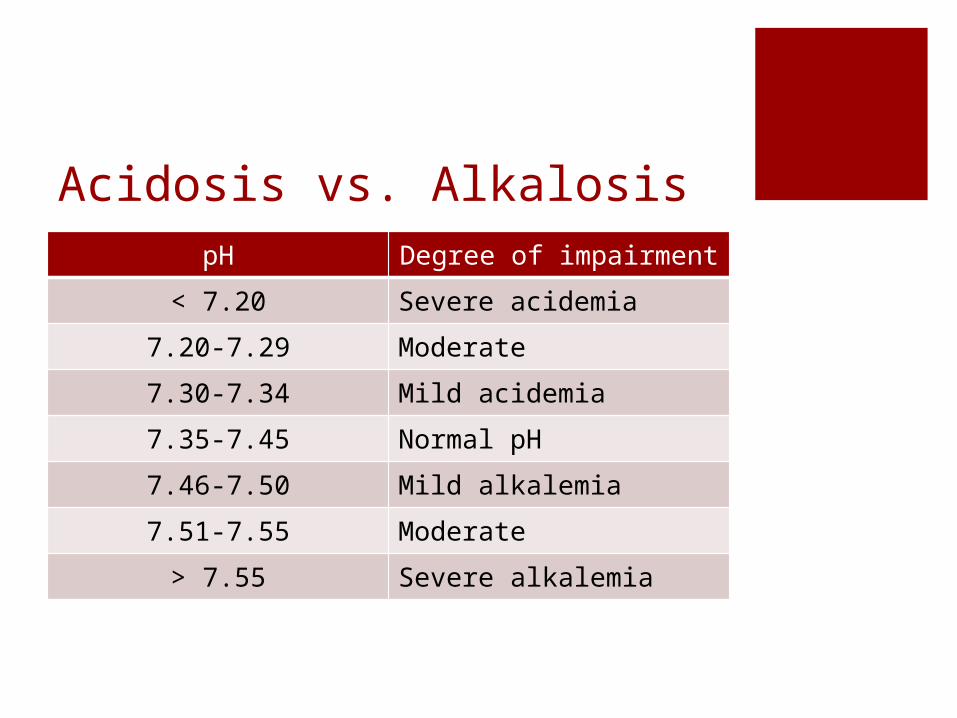
Acidosis vs. AlkalosispH Degree of impairment
< 7.20 Severe acidemia
7.20-7.29 Moderate
7.30-7.34 Mild acidemia
7.35-7.45 Normal pH
7.46-7.50 Mild alkalemia
7.51-7.55 Moderate
> 7.55 Severe alkalemia
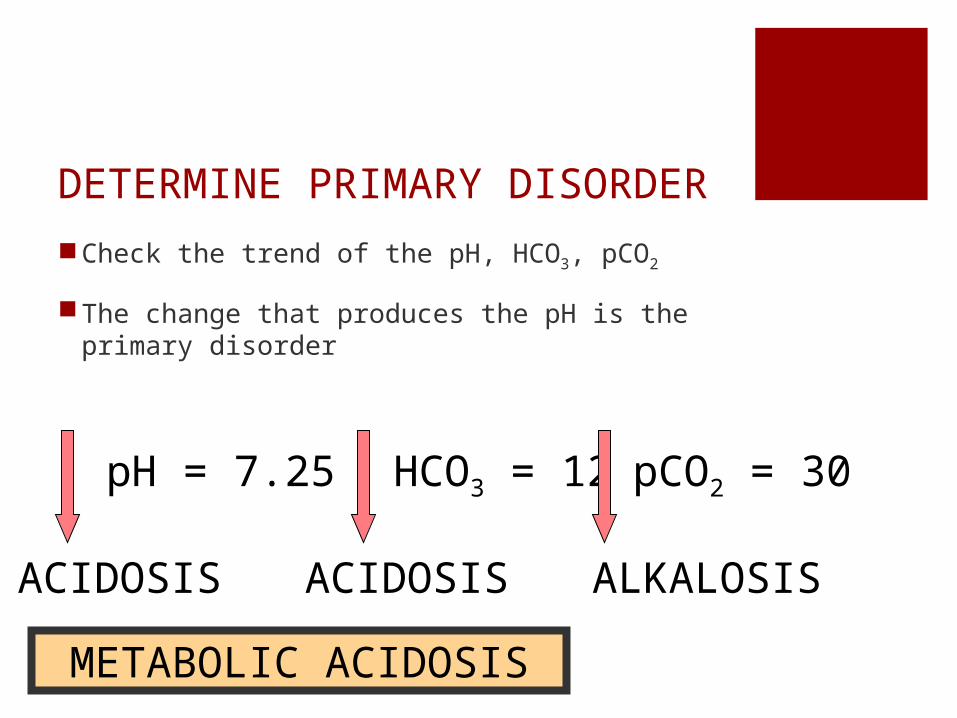
DETERMINE PRIMARY DISORDERCheck the trend of the pH, HCO3, pCO2
The change that produces the pH is the primary disorder
pH = 7.25 HCO3 = 12 pCO2 = 30
ACIDOSIS ACIDOSIS ALKALOSIS
METABOLIC ACIDOSIS
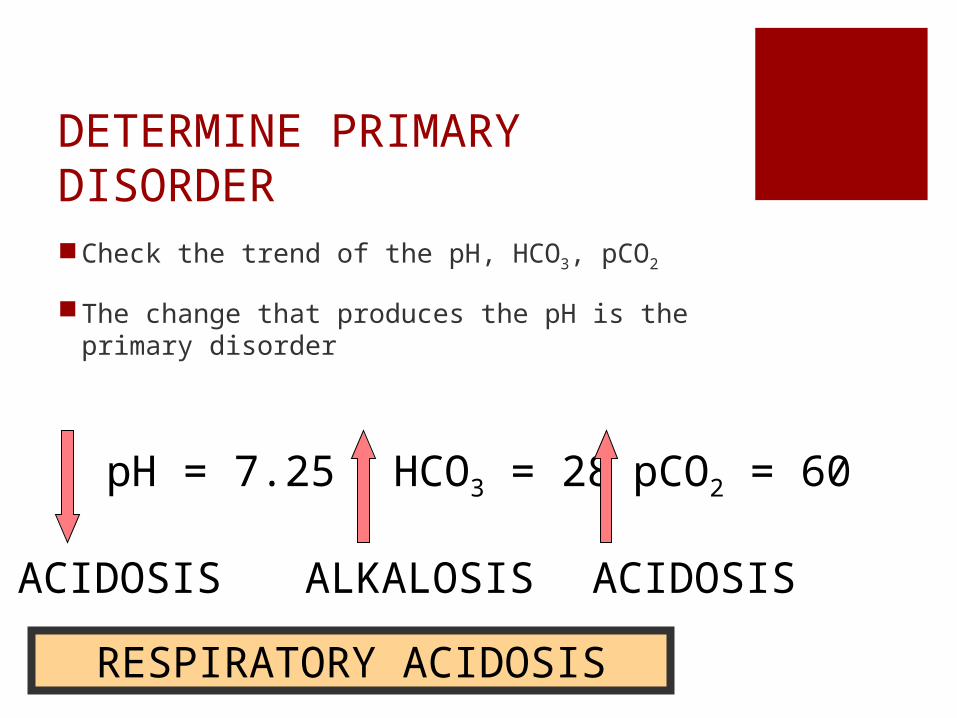
DETERMINE PRIMARY DISORDERCheck the trend of the pH, HCO3, pCO2
The change that produces the pH is the primary disorder
pH = 7.25 HCO3 = 28 pCO2 = 60
ACIDOSIS ALKALOSIS ACIDOSIS
RESPIRATORY ACIDOSIS
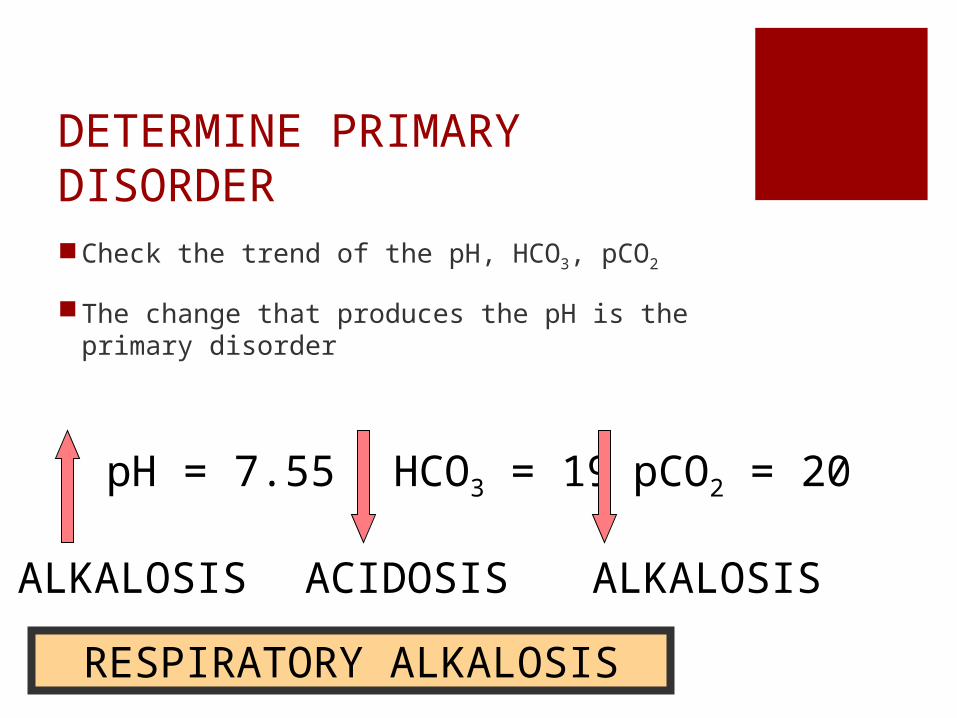
DETERMINE PRIMARY DISORDERCheck the trend of the pH, HCO3, pCO2
The change that produces the pH is the primary disorder
pH = 7.55 HCO3 = 19 pCO2 = 20
ALKALOSIS ACIDOSIS ALKALOSIS
RESPIRATORY ALKALOSIS
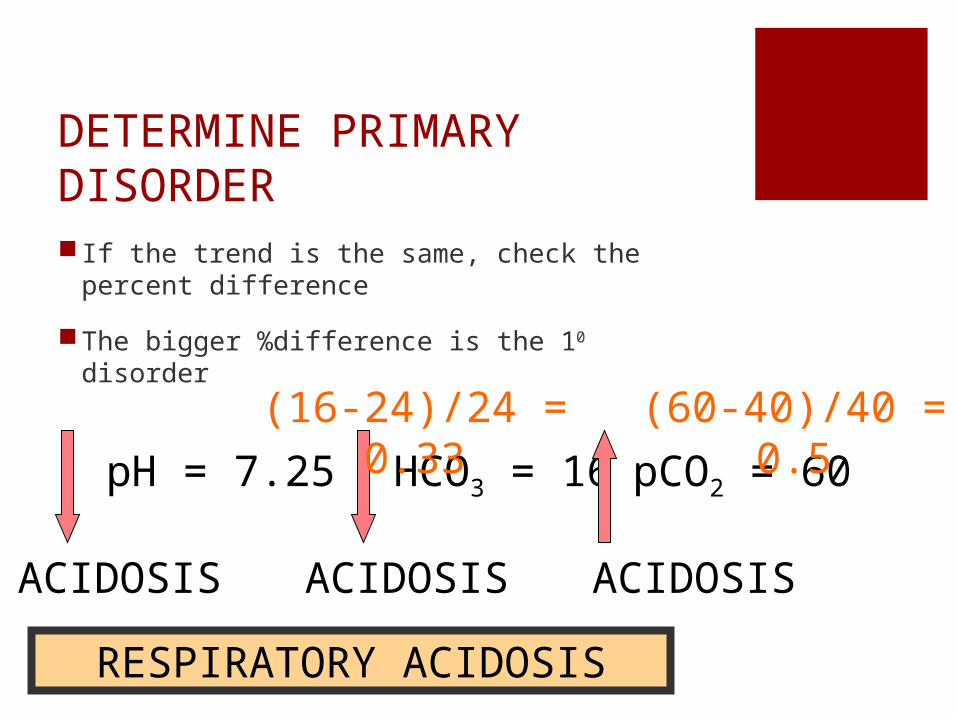
DETERMINE PRIMARY DISORDER If the trend is the same, check the percent
difference
The bigger %difference is the 10 disorder
pH = 7.25 HCO3 = 16 pCO2 = 60
ACIDOSIS ACIDOSIS ACIDOSIS
RESPIRATORY ACIDOSIS
(16-24)/24 = 0.33 (60-40)/40 = 0.5
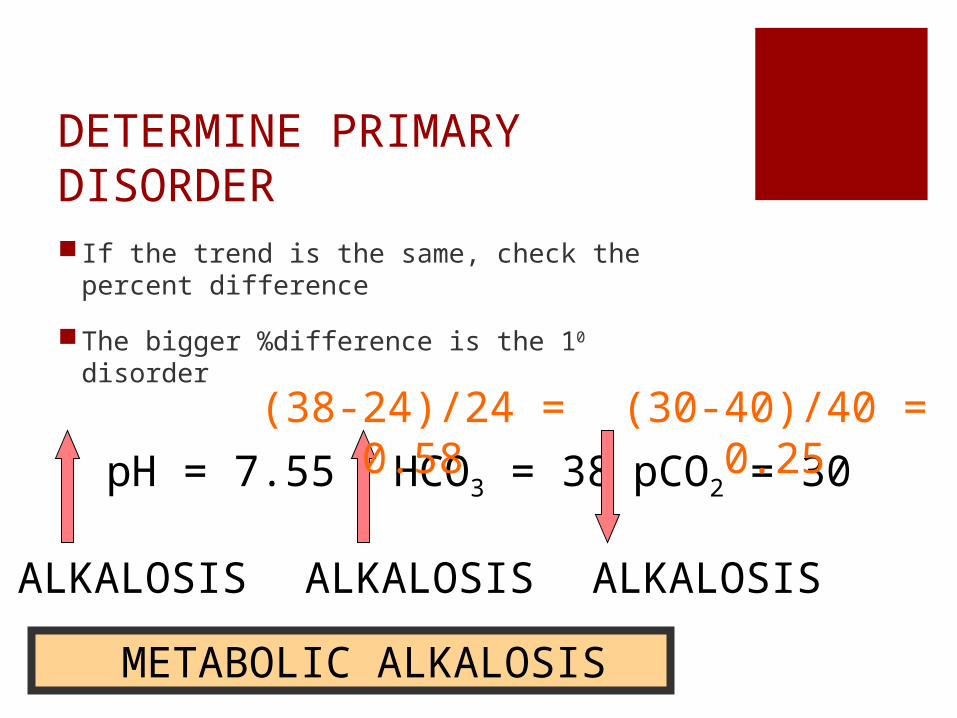
DETERMINE PRIMARY DISORDER If the trend is the same, check the percent
difference
The bigger %difference is the 10 disorder
pH = 7.55 HCO3 = 38 pCO2 = 30
ALKALOSIS ALKALOSIS ALKALOSIS
METABOLIC ALKALOSIS
(38-24)/24 = 0.58(30-40)/40 = 0.25
CHECK THECOMPENSATORY
RESPONSE
COMPENSATED? When a patient develops an acid-base
imbalance, the body attempts to compensate.
Primary buffer response systems in the body: lungs and the kidneys
The body tries to overcome either a respiratory or metabolic dysfunction in an attempt to return the pH into the normal range.
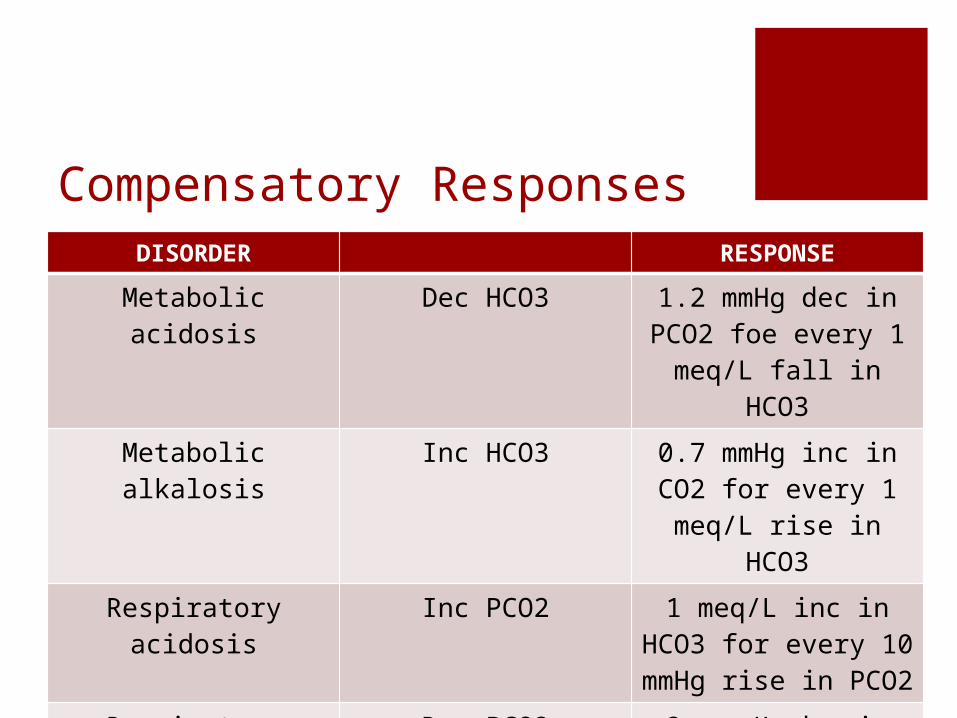
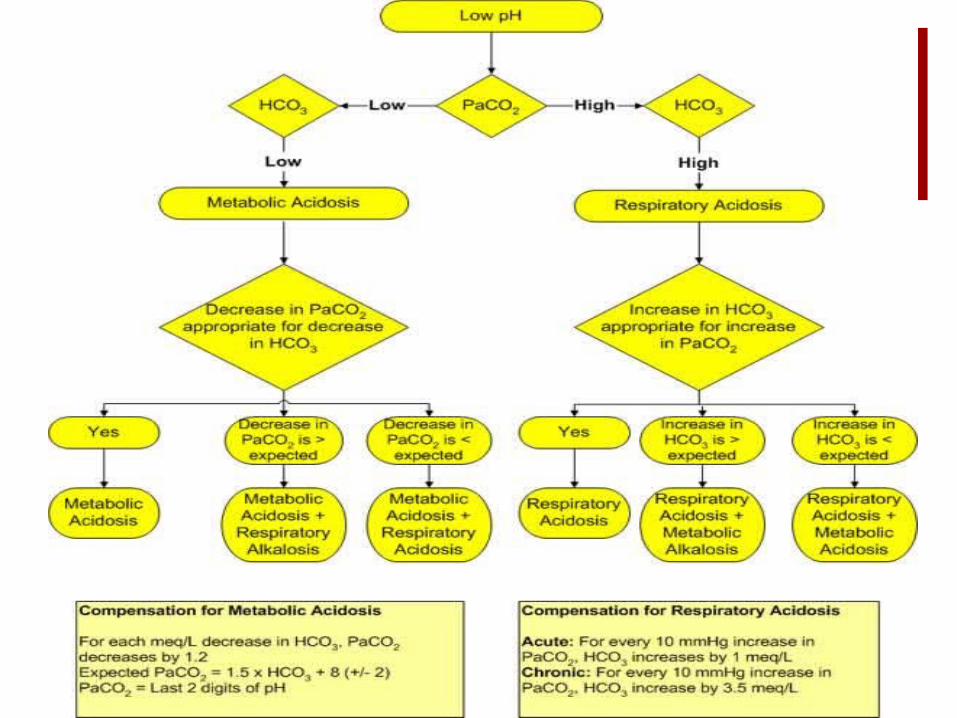
Compensatory ResponsesDISORDER RESPONSE
Metabolic acidosis Dec HCO3 1.2 mmHg dec in PCO2 foe every 1 meq/L fall in HCO3
Metabolic alkalosis Inc HCO3 0.7 mmHg inc in CO2 for every 1 meq/L rise
in HCO3
Respiratory acidosis Inc PCO2 1 meq/L inc in HCO3 for every 10 mmHg
rise in PCO2
Respiratory alkalosis Dec PCO2 2 meq/L dec in HCO3 for every 10 mmHg fall
in PCO2
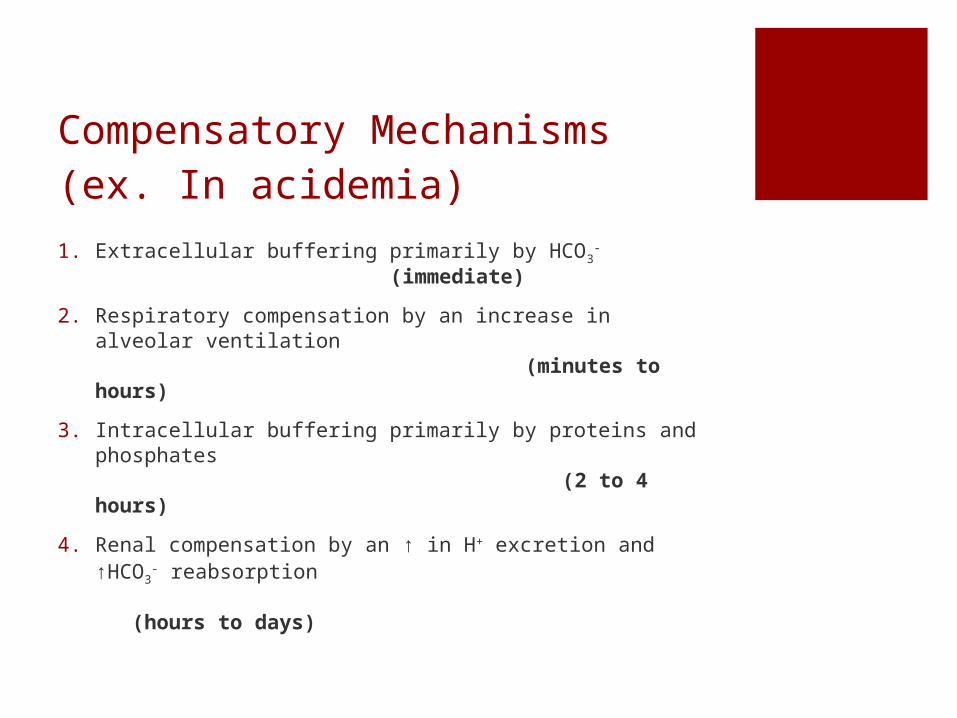
Compensatory Mechanisms(ex. In acidemia)1. Extracellular buffering primarily by HCO3
- (immediate)
2. Respiratory compensation by an increase in alveolar ventilation (minutes to hours)
3. Intracellular buffering primarily by proteins and phosphates (2 to 4 hours)
4. Renal compensation by an ↑ in H+ excretion and ↑HCO3
- reabsorption (hours to days)
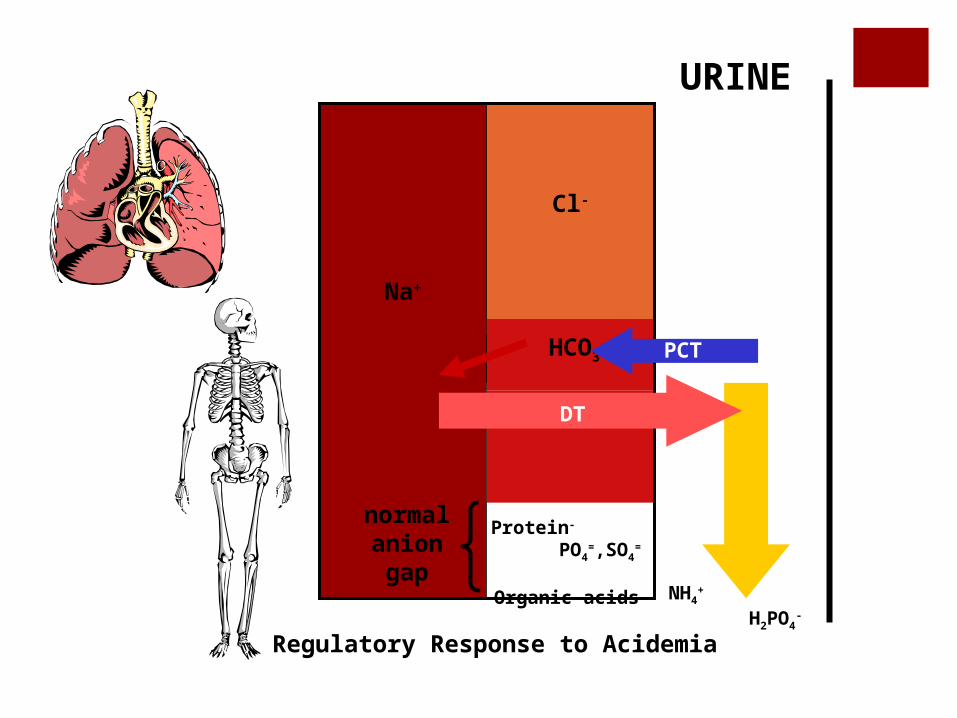
Na+
Regulatory Response to Acidemia
Cl-
H+
Protein- PO4
=,SO4=
Organic acids
normal anion
gap
URINE
HCO3-
NH4+ H2PO4
-
PCT
DT

CompensationIf compensation is < or > predicted then there may be ≥2 disorders:
pCO2 too low: concomitant primary respiratory alkalosis
pCO2 too high: concomitant primary respiratory acidosis
HCO3 too low: concomitant primary metabolic acidosis
HCO3 too high: concomitant primary metabolic alkalosis
CompensationNormal pH but increased pCO2 + increased
HCO3: respiratory acidosis + metabolic alkalosis
Normal pH but decreased pCO2 + decreased HCO3: respiratory alkalosis + metabolic acidosis (e.g., salicylates, DKA)
Normal pH & normal pCO2 & HCO3 but increased AG: HAGMA + metabolic alkalosis (e.g., Alcoholic ketoacidosis w/ vomiting) + respiratory alkalosis (due to hyperventilation of hepatic dysfunction or alcohol withdrawal)
CompensationNormal pH & normal pCO2 & HCO3 & AG: no
disturbance or NAGMA + metabolic alkalosis
Metabolic acidosis + respiratory acidosis: DKA< sedatives.
Cannot have respiratory acidosis & respiratory alkalosis simultaneously (one either hypo- or hyperventilates)
Example 1 If patient presents with pH=7.2 and HCO3=16,
what is the normal compensated value for pCO2?
24-16= 8 meq/L 8 x 1.2 = 9.6 mmHg fall in PCO2
40 mmHg-9.6 mmHg = 30.4 mmHg
Normal compensation PCO2 = 30.4 mmHg

Example 2 If patient presents with pH= 7.23. HCO3= 22
meq/L, and pCO2= 9, what is your interpretation?
Note the pH and tell whether it is acidosis or alkalosis?
Note the HCO3 and pCO2 values to determine which causes the primary disturbance?
Determine the compensatory response
What is our diagnosis?
Example 3pH 7.14
HCO3 9
pCO2 25
Example 3pH 7.14
HCO3 9
pCO2 25
Metabolic acidosis with respiratory acidosis
Example 4pH 7.2
HCO3 15
pCO2 40
Example 4pH 7.2
HCO3 15
pCO2 40
Metabolic acidosis with respiratory acidosis
Example 5pH 7.5
HCO3 15
pCO2 20
Example 5pH 7.5
HCO3 15
pCO2 20
Respiratory alkalosis with metabolic acidosis
Example 6pH 7.36
HCO3 26
pCO2 65
Example 6pH 7.36
HCO3 26
pCO2 65
Respiratory acidosis, compensated
Example 7pH 7.379
HCO3 15
pCO2 25.1

Example 7pH 7.379
HCO3 15
pCO2 25.1
Metabolic Acidosis with Respiratory Alkalosis
CALCULATE THE ANION GAP
Calculate Anion GapIf with metabolic acidosis, check for other existing metabolic derangements; compute for the anion gap
AG = Na – (Cl + HCO3) = normal 10-12
Represents unmeasured anions in the plasma
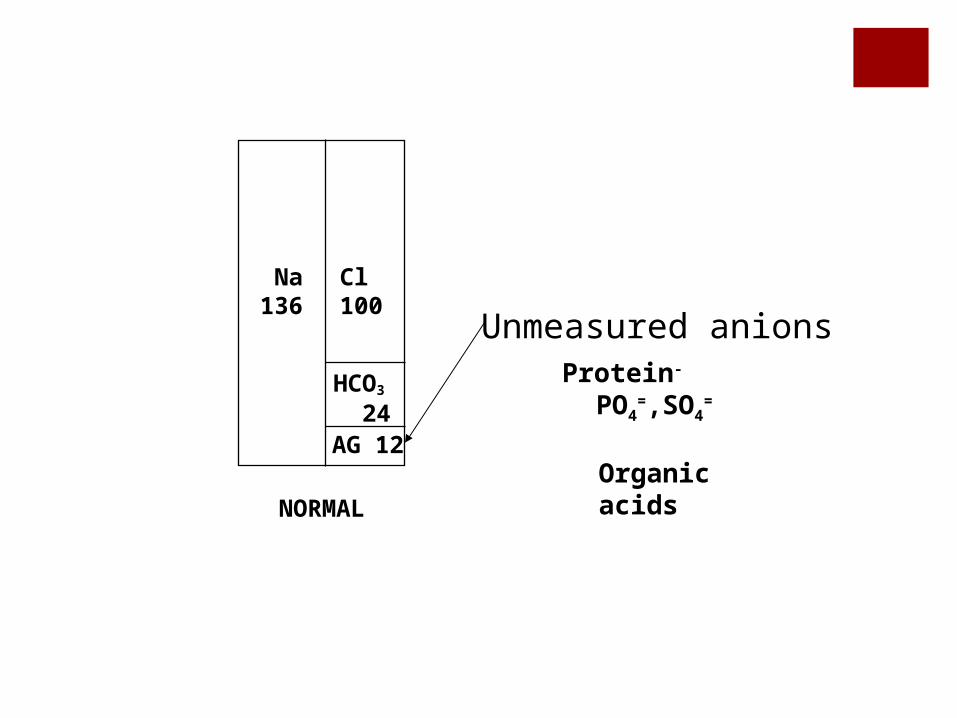
Na136
Cl100
AG 12
HCO3
24
NORMAL
Unmeasured anionsProtein- PO4
=,SO4=
Organic
acids
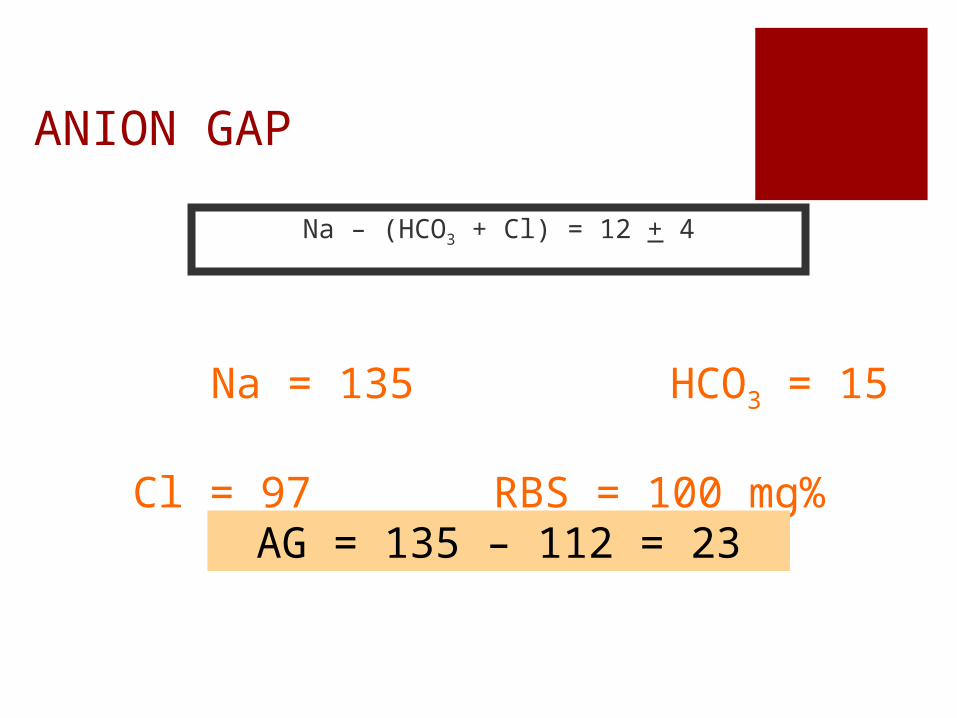
ANION GAP
Na – (HCO3 + Cl) = 12 + 4
Na = 135 HCO3 = 15 Cl = 97 RBS = 100 mg%
AG = 135 – 112 = 23
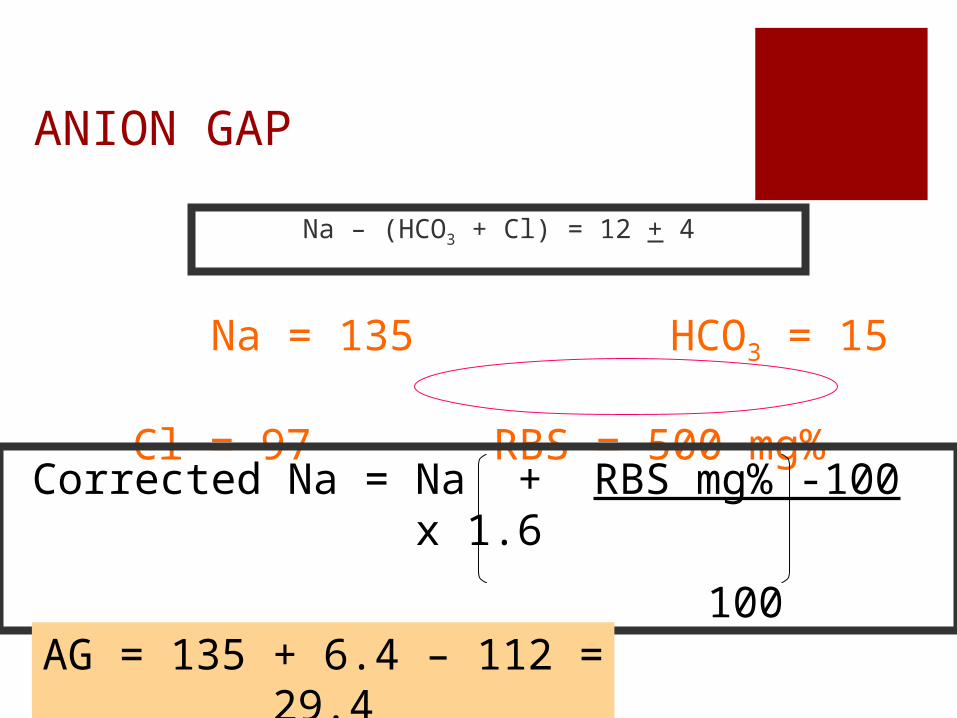
ANION GAP
Na – (HCO3 + Cl) = 12 + 4
Na = 135 HCO3 = 15 Cl = 97 RBS = 500 mg%
Corrected Na = Na + RBS mg% -100 x 1.6
100
AG = 135 + 6.4 – 112 = 29.4
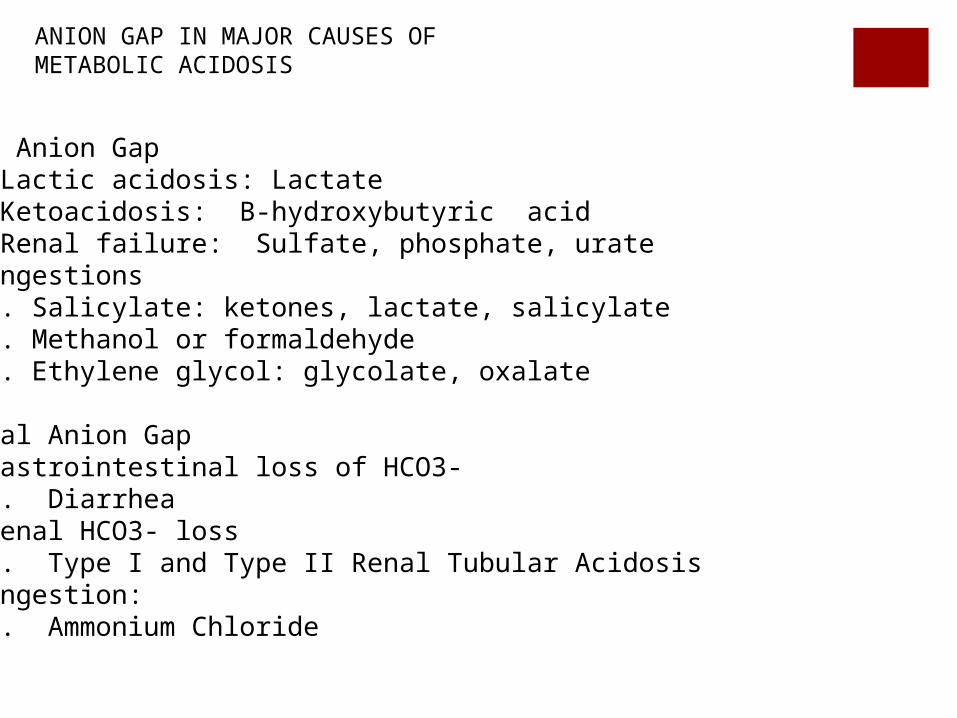
ANION GAP IN MAJOR CAUSES OF METABOLIC ACIDOSIS
High Anion GapA. Lactic acidosis: LactateB. Ketoacidosis: B-hydroxybutyric acidC. Renal failure: Sulfate, phosphate, urateD. Ingestions
1. Salicylate: ketones, lactate, salicylate2. Methanol or formaldehyde3. Ethylene glycol: glycolate, oxalate
Normal Anion GapE. Gastrointestinal loss of HCO3-
1. DiarrheaB. Renal HCO3- loss
1. Type I and Type II Renal Tubular AcidosisC. Ingestion:
1. Ammonium Chloride
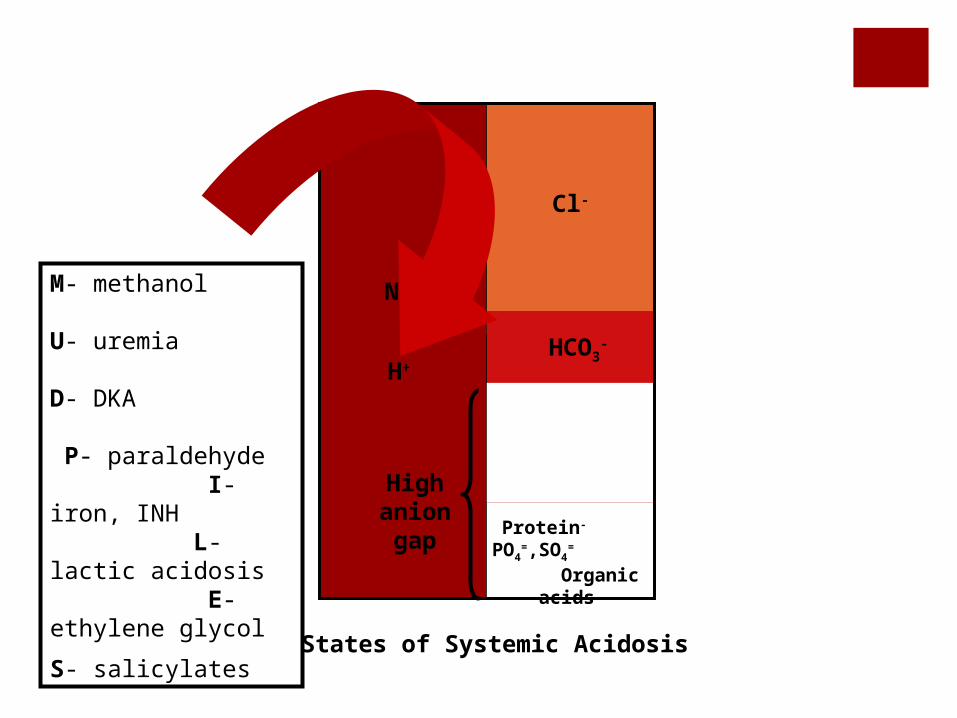
Na+
States of Systemic Acidosis
Cl-
High anion gap
H+
Protein- PO4
=,SO4=
Organic acids
HCO3-
M- methanol U- uremia D- DKA P- paraldehyde I- iron, INH L- lactic acidosis E- ethylene glycol
S- salicylates
CHECK THE DELTA / DELTA
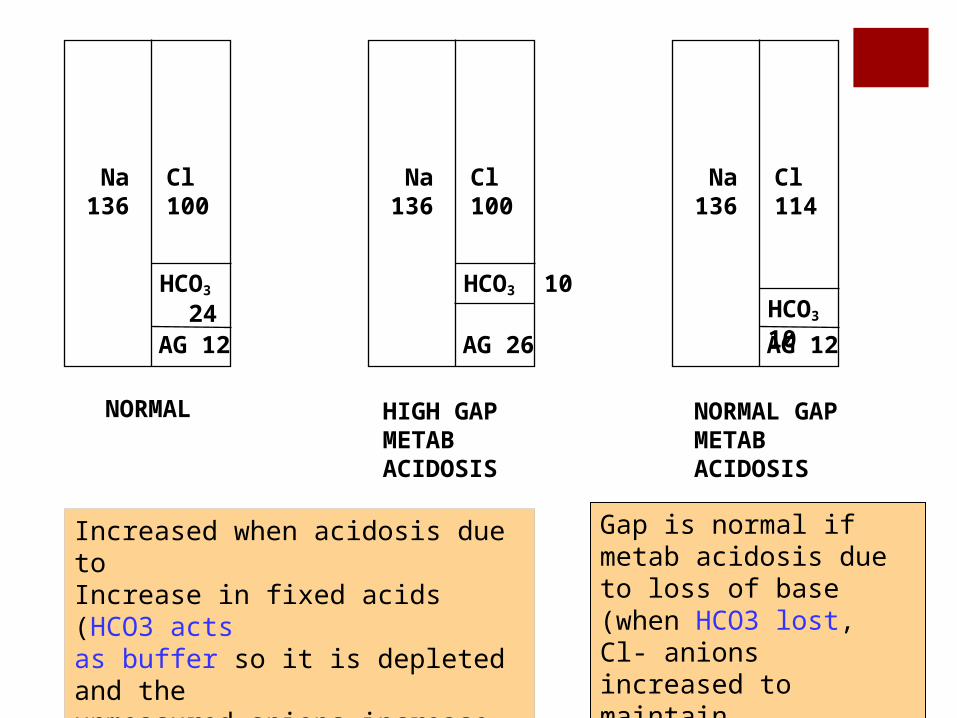
Na136
Cl100
AG 12
HCO3
24
NORMAL
Na136
Cl100
AG 26
HCO3 10
HIGH GAP METABACIDOSIS
Increased when acidosis due toIncrease in fixed acids (HCO3 actsas buffer so it is depleted and theunmeasured anions increase to preserve neutrality)
Na136
Cl114
AG 12
HCO3 10
NORMAL GAP METABACIDOSIS
Gap is normal if metab acidosis due to loss of base (when HCO3 lost,Cl- anions increased to maintain Neutrality)
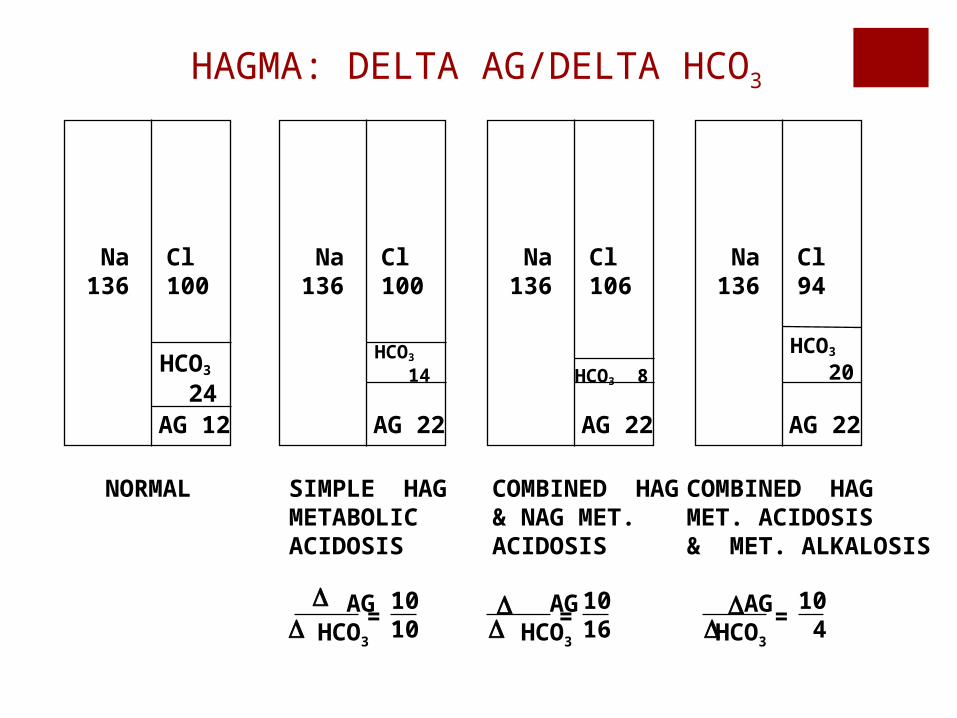
Na136
Cl100
AG 12
HCO3
24
NORMAL
Na136
Cl94
AG 22
HCO3
20
COMBINED HAGMET. ACIDOSIS& MET. ALKALOSIS
AG HCO3
= 10 4
Na136
Cl106
AG 22
HCO3 8
COMBINED HAG& NAG MET. ACIDOSIS
AG HCO3
= 1016
Na136
Cl100
AG 22
HCO3
14
SIMPLE HAGMETABOLICACIDOSIS
AG HCO3
= 1010
HAGMA: DELTA AG/DELTA HCO3
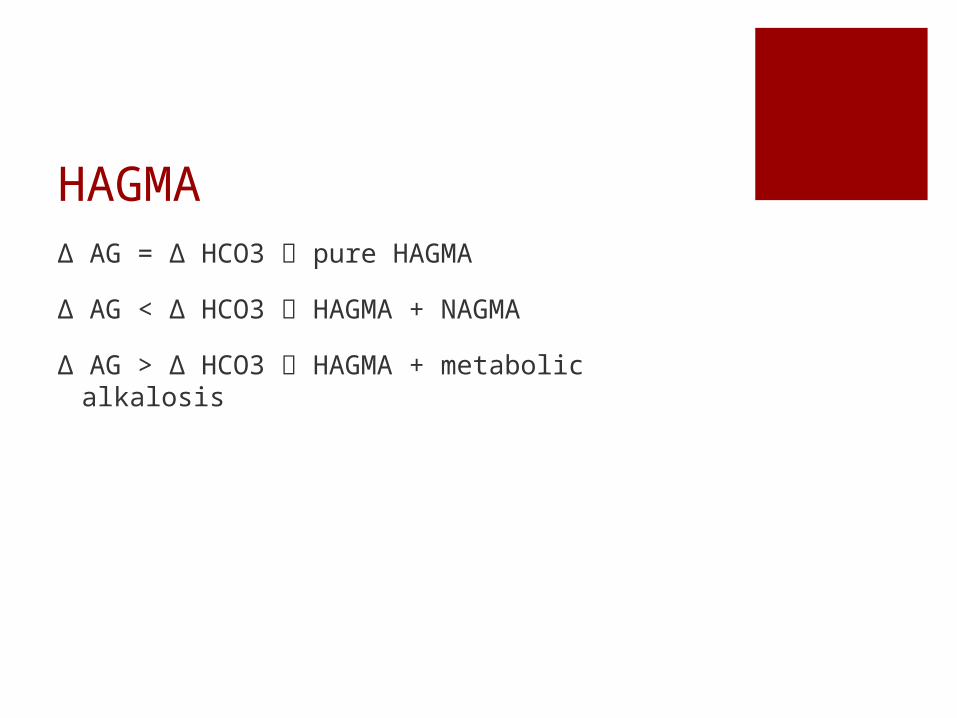
HAGMAΔ AG = Δ HCO3 pure HAGMA
Δ AG < Δ HCO3 HAGMA + NAGMA
Δ AG > Δ HCO3 HAGMA + metabolic alkalosis
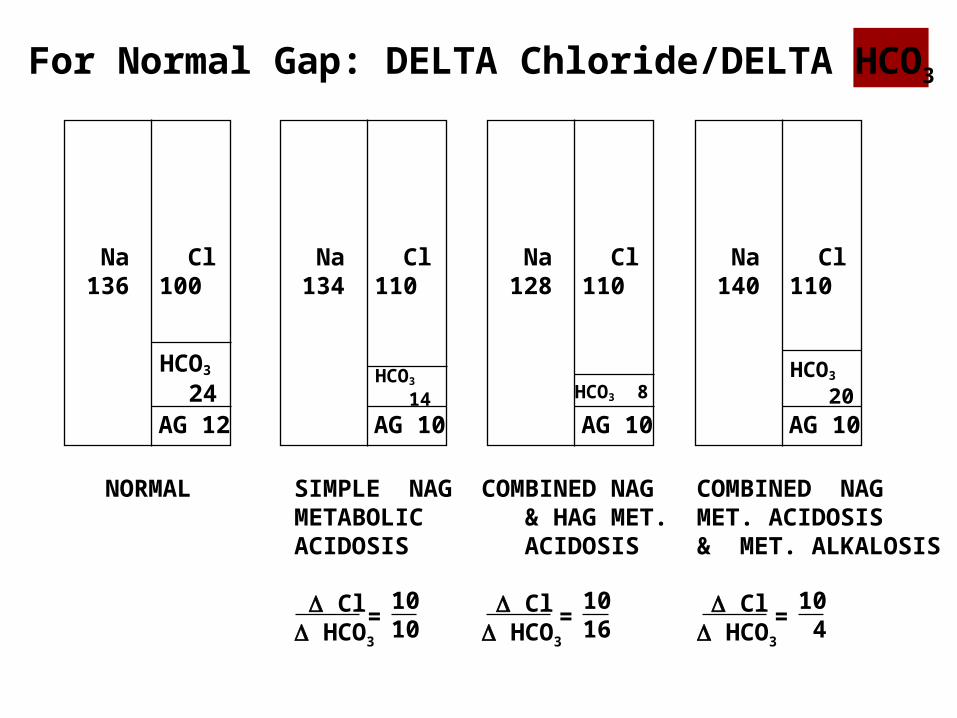
Na136
Cl100
AG 12
HCO3
24
NORMAL
Na134
Cl110
AG 10
HCO3
14
SIMPLE NAGMETABOLICACIDOSIS
Cl HCO3
= 1010
Na128
Cl110
AG 10HCO3 8
COMBINED NAG & HAG MET. ACIDOSIS
Cl HCO3
= 1016
Na140
Cl110
AG 10
HCO3
20
COMBINED NAGMET. ACIDOSIS& MET. ALKALOSIS
Cl HCO3
= 10 4
For Normal Gap: DELTA Chloride/DELTA HCO3
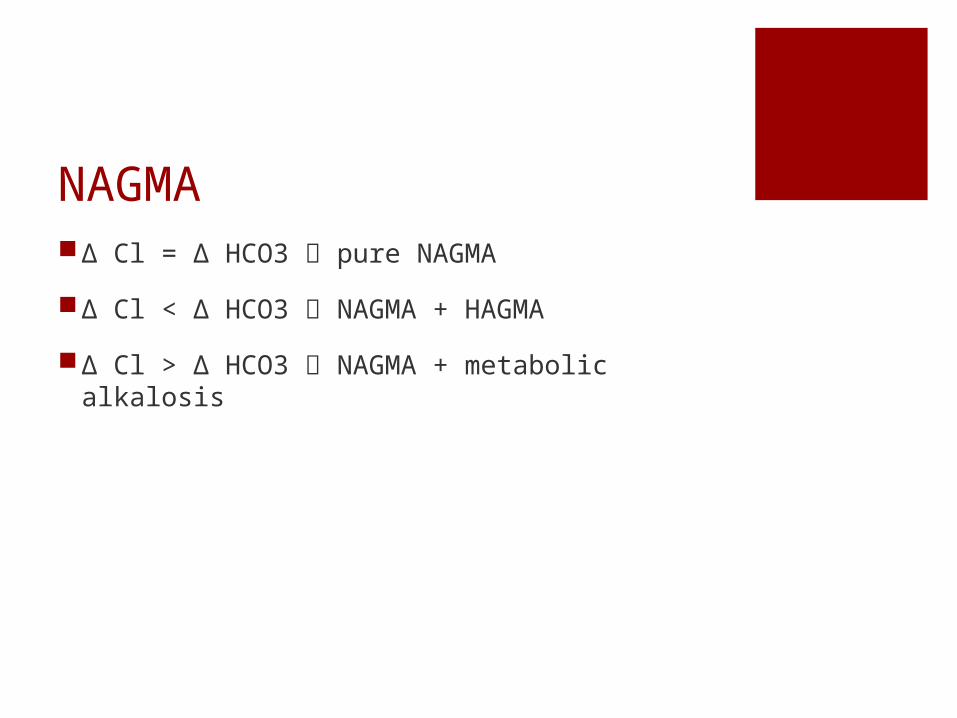
NAGMAΔ Cl = Δ HCO3 pure NAGMA
Δ Cl < Δ HCO3 NAGMA + HAGMA
Δ Cl > Δ HCO3 NAGMA + metabolic alkalosis

MISCELLANEOUS
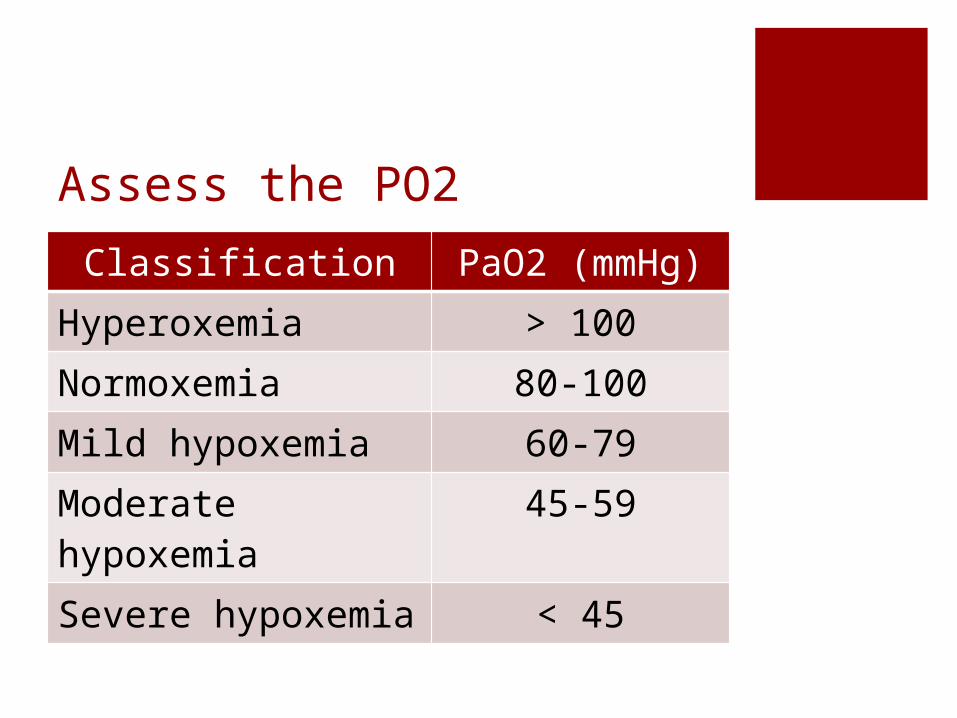
Assess the PO2Classification PaO2 (mmHg)
Hyperoxemia > 100Normoxemia 80-100Mild hypoxemia 60-79Moderate hypoxemia
45-59
Severe hypoxemia < 45
Room air, patient < 60 y.o.Mild hypoxemia paO2 < 80 mm HgModerate paO2 < 60 mm HgSevere paO2 < 40 mm
Hg
For each year > 60 y.o., subtract 1 mm Hg for limits of mild and moderate hypoxemia
At any age, a paO2 < 40 mm Hg indicates severe hypoxemia