abim pgy1 thyroid 2019-2020 with video
TRANSCRIPT

ThyroidCaroline T. Nguyen M.D.
Assistant Professor of Clinical Medicine, Obstetrics, and GynecologyDivision of Endocrinology, Diabetes, and Metabolism
Keck School of MedicineUniversity of Southern California
December 3rd, 2019

Endocrine is 9% of exam and thyroid is < 2%
Internal Medicine Certification Examination Blueprint Purpose of the exam The exam is designed to evaluate the knowledge, diagnostic reasoning, and clinical judgment skills expected of the certified internist in the broad domain of the discipline. The ability to make appropriate diagnostic and management decisions that have important consequences for patients will be assessed. The exam may require recognition of common as well as rare clinical problems for which patients may consult a certified internist. Exam content Exam content is determined by a pre-established blueprint, or table of specifications. The blueprint is developed by ABIM and is reviewed annually and updated as needed for currency. Trainees, training program directors, and certified practitioners in the discipline are surveyed periodically to provide feedback and inform the blueprinting process. The primary medical content categories of the blueprint are shown below, with the percentage assigned to each for a typical exam:
Medical Content Category % of Exam
Allergy/Immunology 2% Cardiovascular Disease 14% Dermatology 3% Endocrinology, Diabetes, and Metabolism 9% Gastroenterology 9% Geriatric Syndromes 3% Hematology 6% Infectious Disease 9% Nephrology/Urology 6% Neurology 4% Obstetrics/Gynecology 3% Medical Oncology 6% Ophthalmology 1% Otolaryngology/Dental Medicine 1% Psychiatry 4% Pulmonary Disease 9% Rheumatology/Orthopedics 9% Other 2% Total 100%
• Hyperthyroidism
• Hypothyroidism
• Thyroiditis
• Thyroid nodules
• Thyroid cancer
• Euthyroid sick syndrome
• Other thyroid disorders
www.abim.org

Exam Format
Every question in the exam will fall into one of the primary medical content categories shown above. There are also other important areas that are addressed in conjunction with this medical content, and these areas are called “cross content categories.” Not all questions have a cross-content classification; the cross-content categories are shown in the following table:
Cross-Content Category Relative Percentage
Critical Care Medicine 10% Geriatric Medicine 10% Prevention 6% Women’s Health 6% Clinical Epidemiology 3% Ethics 3% Nutrition 3% Palliative/End-of-Life Care 3% Adolescent Medicine 2% Occupational Medicine 2% Patient Safety 2% Substance Abuse 2%
Exam format The exam is composed of multiple-choice questions with a single best answer, predominantly describing patient scenarios. Questions ask about the work done (that is, tasks performed) by physicians in the course of practice:
x Making a diagnosis x Ordering and interpreting results of tests x Recommending treatment or other patient care x Assessing risk, determining prognosis, and applying principles from epidemiologic studies x Understanding the underlying pathophysiology of disease and basic science knowledge applicable
to patient care Clinical information presented may include patient photographs, radiographs, electrocardiograms, recordings of heart or lung sounds, and other media to illustrate relevant patient findings. A tutorial including examples of ABIM exam question format can be found at http://www.abim.org/exam/prepare.aspx. The primary medical categories can be expanded for additional detail to show topics that may be covered in the exam. Each primary medical content category is listed below, with the percentage of the exam assigned to this content area. Below each major category are subsection topics and their assigned percentages in the exam. Please note: The percentages below describe content of a typical exam and are approximate; actual exam content may vary.

Outline
• Thyroid physiology
• Thyroid function tests
• Other thyroid studies
• Cases

Thyroid Axis

Thyroid Tests• TSH - thyroid-stimulating hormone• Total T4 and FT4 – total and free thyroxine• Total T3 and FT3 – total and free triiodothyronine• TPO Ab - thyroid peroxidase antibody• TRAB – TSH-receptor antibody• TSI – thyroid-stimulating immunoglobulin• Tg - thyroglobulin• Tg Ab -thyroglobulin antibody

Thyroid Follicle
Walter F., PhD. Boron (2003). Medical Physiology: A Cellular And Molecular Approaoch. Elsevier/Saunders. p. 1300.

Thyroid Function TestsTSH FT4 Clinical Status
High Low Primary hypothyroidism, thyroiditis
Normal Subclinical hypothyroidism
High Pituitary hyperthyroidism or thyroid hormone resistance
Low High Thyrotoxicosis, thyroiditis
Normal Euthyroid sick syndrome, subclinical hyperthyroidism, MNG with autonomous production
Low Pituitary hypothyroidism

Case 1 A 32 yo W presents to clinic with a 2-week history of palpitations, heat intolerance, fatigue, and mild weight loss of 5 pounds. On exam, the thyroid is homogenously enlarged 1.5x normal, HR is 100 bpm, temperature 37.7 °C, BP 120/65 and she is slightly warm to touch. TSH is 0.01 mIU/L (0.4-4 mIU/L) and her FT4 is 2.67 ng/dL (0.7-1.9ng/dL).
What is the best next step?a. Order a T3 level and TPO-Ab.b. Order radioactive iodine ablation.c. Order a radioactive iodine uptaked. Start methimazole 10mg daily and propranolol 10mg
every 8 hours.

Differential Diagnosis of Hyperthyroidism
ETIOLOGY GLAND EYES TSH T3 & T4 ANTI-TPO TG RAIU
Graves' smooth, soft ++++ UD markedly ++++ high elevated+ bruit elevated
Toxic MNG large,firm ------ UD modestly ------ high normalnodular elevated to high
Autonomous solitary ------ UD elevated ------ high focal uptakenodule nodule in nodule
Subacute 4+ tender, ------ UD minimally ------ high < 1%thyroiditis firm elevated
Postpartum firm, large ------ UD minimally ++++ high < 1% /Painlessthyroiditis
nontender elevated
Factitious nonpalpable ------ UD low T4 & high T3 ------ low lowhigh T4 & low T3
TSH-secreting
large, firm ------ normal modestly ------ high elevated
adenomasmooth to high elevated

RAIUIncreased DecreasedGraves disease ThyroiditisSolitary nodule or toxic multinodular goiter
Excess exogenous T4 or T3
Iodine deficiency Iodine excess (contrast dye, diet, amiodarone)
TSH-secreting pituitary tumor
Ectopic hyperthyroidism (Struma ovarii or metastatic follicular thyroid cancer)
hCG secreting tumor
Normal value at 6 hours: 3-16% Normal value at 24 hours: 8-25%*normal ranges can range according to lab

Thyroid Scan
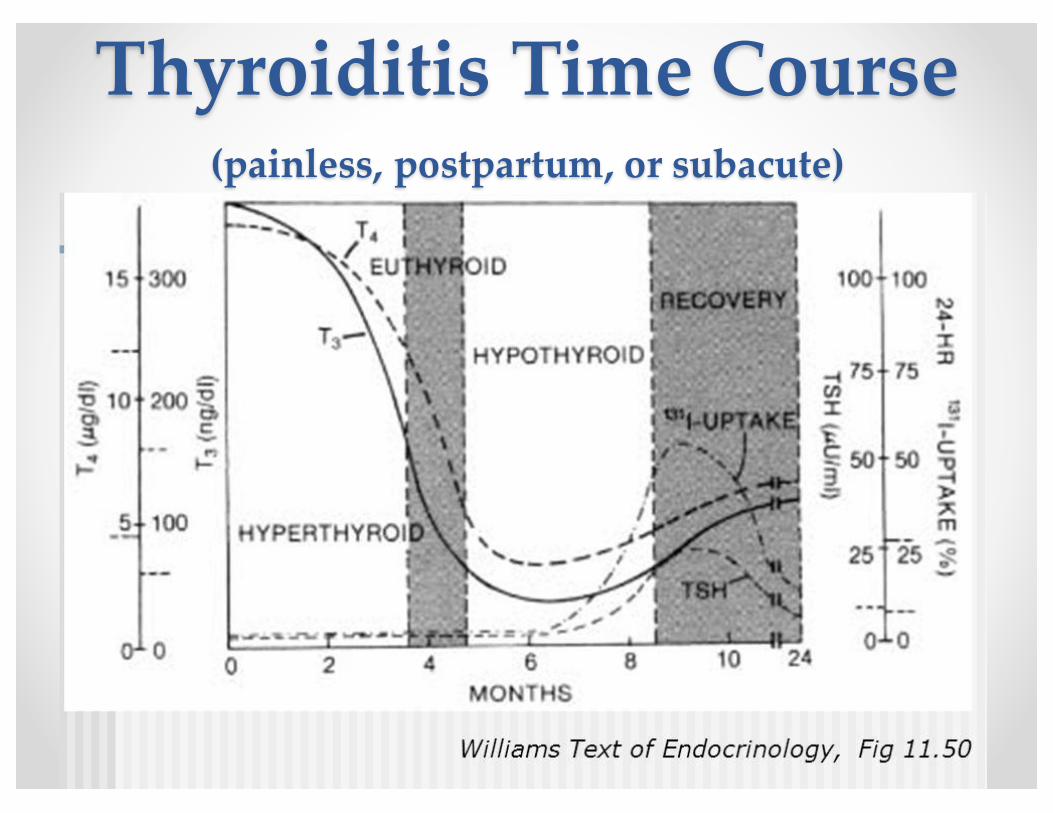
Thyroiditis Time Course (painless, postpartum, or subacute)

Thyroiditis• Painful
o Subacuteo Infectiouso Radiationo Palpation/trauma
• Painlesso Painlesso Post-partumo Drug-induced
• Interferon-alpha, interleukin-2, amiodarone, lithium, TKIs, Checkpoint inhibitor immunotherapy
o Fibrous thyroiditis (Riedel’s)

Subclinical hyperthyroidism
• TSH low or suppressed• T4 normal• Confirm lab results in 3-6 months. • Patients typically asymptomatic• Treat if TSH <0.1mIU/L, patients >60 yo, history of
tachyarrhythmias or heart disease, postmenopausal with low bone density, or very symptomatic.
• Treat with methimazole or RAIA

Case 2• 46 yo W presents with 3-day history of severe pain that
began suddenly in her right neck, but now has spread to her right jaw. She took ibuprofen for two days without relief. ROS significant for a URI last month. On exam, there is significant tenderness to palpation of her right neck. Thyroid is mildly enlarged 1.5x. No palpable masses. No signs of trauma or erythema. No evidence of Graves ophthalmopathy. HR 100 bpm. Temp 37.2°C. WBC is normal. ESR is elevated at 65 mm/hr. Her TSH is 0.04 mIU/L and FT4 2.14 ng/dL.
What is the best next step?a. Check FT3 and TPO-Abb. Order a CT of the neckc. Order a radioactive uptake and scand. Treat with corticosteroids

Case 3• 27 yo W presents with irregular periods for 6 months then
amenorrhea for the past 3 months. A review of systems is notable for weight gain of 15 pounds over the past 6 months, worsening fatigue, cold intolerance, and a white discharge from her breast bilaterally for the past month. Her gynecologist checked her labs and prolactin was 650ng/ml. MRI showed a hypertrophied pituitary gland, but no discrete pituitary adenoma.
• What would the next best step be?a. Start OCP therapyb. Start cabergalinec. Check thyroid function testsd. Refer for transphenoidal surgery

Hypothyroidism can lead to hyperprolactinemia
• Mechanism is not knowno Enhanced hypothalamic synthesis of TRH
which can increase secretion of prolactino Increased pituitary responsiveness to TRH
• Treatment is to treat the hypothyroidism

Treatment hypothyroidism
• Standard first line treatment is levothyroxine (T4)• T3 may sometimes be added• T4 has a long half-life and takes weeks to equilibrate• Can start patients on 50-100mcg/day. Often we start 1.6mcg/kg.• Adjust dose in 6-8 weeks by increments of 12.5-25mcg.• Conventional thinking is to start elderly patients or patients with
severe CAD on lower dose and slowly titrate up.• If TSH is still elevated (>10mIU/L) in a patient taking
>200mcg/day, think non-adherence.• Other considerations:
o Drugs that may interfere with absorption of thyroxine: calcium, iron, PPIs
o Malabsorption syndromes, cholestyramine, resin-binderso Alterations in TBG (ie.,estrogens)
• Pregnant women - thyroid hormone requirements increase by 30%-50%.

Subclinical hypothyroidism
• Elevated TSH • Normal T4• Relatively asymptomatic• Typically treat once TSH >10 mIU/L• Consider treatment in symptomatic patients with
positive TPO-AB as ~5% will progress to hypothyroidism annually.
• Treat patients who are desiring pregnancy (TSH 0.5 –2.5mIU/L) or who are pregnant
• Roughly 5% per year will progress to overt hypothyroidism.

Case 4• 42 yo M presents to ER with fevers, palpitations, shortness of
breath, 18-pound weight loss over the past few months, and difficulty concentrating. His family says he has not been himself. He is agitated and sometimes disoriented. ROS significant for frequent loose stools and a recent productive cough. He has a history of hyperthyroidism, but he stopped taking the medication roughly one year ago for unclear reasons. BP 112/50 HR 126 bpm Temp 38.9 °C RR 22 O2 sat 97% RA. Exam is notable for mild ophthalmopathy, a diffusely enlarged, firm, smooth thyroid gland 3x normal with a thyroid bruit, decreased breath sounds in the lower right lung base, sinus tachycardia, and a tremor. Skin is warm to touch. TSH <0.01 mIU/L FT4 >7.77ng/dL.

Case 4• What is your diagnosis?a. Subacute thyroiditisb. Thyroid stormc. Sick euthyroid illnessd. Toxic multinodular goiter

Diagnosis Thyroid Storm The “USC method”
• Altered mental status• Clinical or biochemical evidence of chronic
hyperthyroidism• Hyperthermia • Precipitating event
o Compensatedè decompensated

Scoring systemThyroid Storm

TreatmentThyroid Storm
• Anti-thyroid medication: o PTU 100-150mg every 6-8 hourso Methimazole 20mg every 12 hours
• SSKIo 5-10 drops every 8 hours 1 hour after anti-thyroid medication
• Glucocorticoidso Decadron 4mg IVPB q 6 hours
• Beta-blockerso Propranolol 40mg every 6 hours as neededo Propranolol 1 mg slow IVP then 1mg/hr if no PO intake or CHFo Target HR 90-100 bpm
• Supportive care: IV fluids, empiric antibiotics• Avoid active cooling and be careful with diuresis

Case 5• 76 yo W is brought in by her family. They say she is less
interactive and spends most of her time in bed. She has gained 10 pounds in the last 6 months and has not had a bowel movement in 5 days. On exam, she is wearing a thick wool sweater, is arousable, alert and oriented x3, but falls asleep during your exam. BP 130/90mmHg, HR 54 bmp, RR 12, Temp 35.2. Her skin is doughy, pale, and dry. She has periorbital edema and her reflexes have a delayed relaxation phase. TSH is 76mIU/L FT4 0.3ng/dL.
• Which is the most appropriate initial treatment?a. Start intravenous liothyronineb. Start intravenous liothyronine and hydrocortisonec. Start intravenous levothyroxined. Start intravenous levothyroxine and hydrocortisone

Delayed Reflexes

Diagnosis Myxedema Coma(Decompensated hypothyroidism)
the USC Method
• Altered mental status• Clinical or biochemical evidence of hypothyroidism• Hypothermia (relative, i.e, normal temp in sepsis)• Precipitating event

Scoring systemMyxedema Coma
Popoveniuc G et al. Endocrine Practice 2013.

Treatment of Myxedema Coma
• Hydrocortisone 100mg IV q8 hours
• Levothyroxine 200-500mcg IV x1 followed by 50-100mcg IV daily. (At USC, we treat with 500mcg IV x1)
• Supportive care: IVF, antibiotics, respiratory support

Case 6• 24 yo W is evaluated for a lump in his neck that he
noticed a few weeks ago. She denies a history of radiation exposure or family history of thyroid cancer. She takes no medications. BP 136/70mmHg HR 87 Temp 37.1 °C. Examination shows a firm left thyroid nodule that moves with swallowing with no lymphadenopathy. US shows a left 1.4x1.9cm solid hypoechoic nodule with microcalcifcations that is taller than wide. No other nodules seen.
• What is the next best step?a. Repeat thyroid US in 3 monthsb. Repeat thyroid US in 6 monthsc. Radioactive iodine uptake and scand. Refer for FNA

US findings and thyroid cancer risk
Good: cystic, regular, spongiformNot Good: microcalcifications, irregular, hypoechoic, taller than wide
ATA guidelines 2015

http://tiradscalculator.com/

US-guided Fine Needle Aspiration (FNA)
• Outpatient procedure• Local anesthetic
Bethesda Classifcation
Diagnostic category Estimated risk of malignancy %
I Non-diagnostic or unsatisfactory
1-4
II Benign 0-3III Atypia/follicular lesion
of undetermined significance
5-15
IV Follicular tumor or suspicious for follicular tumor
15-30
V Suspicious malignancy 60-75VI Malignant 97-99

Case 7• 27 yo W has a L 0.9x0.8x0.7cm hypoechoic well-
circumscribed thyroid nodule with FNA showing Bethesda VI (papillary thyroid cancer). Thyroid US did not show any nodules in the right thyroid lobe or any lymphadenopathy. Patient has no family h/o thyroid cancer or exposure to radiation.
• What is the next best step?a. Lobectomyb. Total thyroidectomyc. Total thyroidectomy and RAIAd. Total thyroidectomy, RAIA, and TSH-suppression with LT4
therapy

ATA Guidelines 2015• Lobectomy is appropriate for <1cm without
extrathyroidal extension and cN0 in the absence of prior head and neck radiation, familial thyroid cancer, and detectable cervical lymphadenopathy
• For >1cm and <4cm without extrathyroidalextension, and without clinical evidence of any lymph node metastases, can proceed with total thyroidectomy or lobectomy.
• Strong recommendation, moderate-quality evidence

Case 8• 68 yo W with a 2-month history of
intermittent difficulty swallowing. She has a 15-yr history of a multinodular goiter. Several FNAs were negative for cancer. Exam shows an enlarged thyroid gland with several firm nodules bilaterally that move with swallowing. SBP 148/89 mmHg HR 89 RR 16 O2 sat 98%. TSH is 0.1mIU/L FT4 1.8ng/dL.
• What is the most appropriate next step?a. Radioactive iodine ablationb. Methimazolec. External beam radiation to the neckd. Total thyroidectomy

Case 9• 76 yo M is intubated and has been in the ICU for 1 week
for severe sepsis for a respiratory infection. He is on broad spectrum antibiotics and levophed. On exam BP 98/66mm Hg HR 88 bmp RR 18/min Temp 37.1°C. He was sedated. Thyroid was not enlarged. No nodules palpated. TSH was 30 mIU/L (high), FT4 0.25 ng/dL (low), TPO-Ab 67 IU/L (high).
• What is the best next step?a. Repeat thyroid function tests nowb. Repeat thyroid function tests in 8 weeks when patient is
out of the ICUc. Treat with hydrocortisoned. Treat with hydrocortisone and levothyroxine

Thyroid function tests in sick euthyroid illness
Official reprint from UpToDatewww.uptodate.com ©2016 UpToDate
®
®
Thyroid function tests in nonthyroidal illness
Schematic representation of the changes in thyroid function tests in patients with nonthyroidalillness of increasing severity.
rT3: reverse triiodothyronine; T3: triiodothyronine; T4: thyroxine; TSH: thyroid-stimulating hormone.
Graphic 61095 Version 2.0
Thyroid function sick patients - UpToDate https://www-uptodate-com.libproxy1.usc.edu/contents/image/pr...
1 of 1 10/26/16 11:40 PM

Sick Euthyroid Illness• TSH is often low in critical illness (0.05 to 0.3mIU/L)• Normalization after recovery from critical illness• TSH <0.01 mIU/L consistent with true hyperthyroidism• TSH >20mIU/L in patients recovering from critical
illness may be suggestive of true hypothyroidism• T4 and FT4 low in critical illness due to issues with
decreased thyroid-hormone binding proteins and possible issues with assay methodology
• The majority of hospitalized patients have low T3 • rT3 may have a role if unable to differentiate
between central hypothyroidism and sick euthyroidillness. rT3 is elevated in the later.

Answers1. C2. D3. C4. B5. D6. D7. A8. D9. D

Thank you