abnormal vaginal discharge etiopathogenesis-physiological
TRANSCRIPT
ABNORMAL VAGINAL DISCHARGE -ETIOPATHOGENESIS
Dr. G. Ruben raj

Vaginal discharge is the most common presenting
complaint of females attending op department.
Excessive vaginal discharge may be physiological or
Pathological.
DEFINITION :
Abnormal vaginal discharge (AVD) is defined as any
one of the three presentations,
1. Excessive vaginal discharge not associated with
menstruation; pre, mid and post period.
2. Offensive or malodorous discharge
3. Yellowish or mucopurulent discharge

PREVALANCE It has been estimated that
approximately 1/3 rd of female patients
may complain of Abnormal vaginal
discharge.
It can occur in females of all ages,from
neonatal to the post menopausal period
and it is quite common during pregnancy.
Many clinics have reported that 70%
of pregnant women manifest Abnormal
vaginal discharge due to lower genital
tract infection.

NORMAL DISCHARGE
Floccular in consistency
Whitish and non malodourous
Normal pH is acidic ranging from 3.5
to 4.5 due to Lactobacilli which convert
glycogen to lactic acid
Secondary fermentation of
endocervical mucus by vaginal flora also
contribute to low pH.

Cellular contents of discharge are composed of sloughed cells of cervical
columnar and vaginal squamous epithelium.
Bulk of discharge consists of serous vaginal transudate and lubricating
cervical mucus
VULVO VAGINAL SOURCE
Vaginal canal being ectodermal origin consists of stratified
squamous epithelium.
There are no sweat,sebaceous and other types of secretory
glands in vaginal epithelium.

Upper end is formed by portio vaginalis of cervix
Caudal end is formed by vulva lined by squamous
Epi. containing secretory,sweat and sebaceous gland
Vaginal fluid is largely derived from serum trasudate in vaginal beds
that seeps from capillaries through intercellular channels.Small amount is
derived from Bartholins glands,endometrium and fallopian tubes.
CONTENT -
cellular debris,transudate consisting primarily of water &
electrolytes,facultative micro organisms,fatty acids,proteins and
carbohydrates.
Contd...
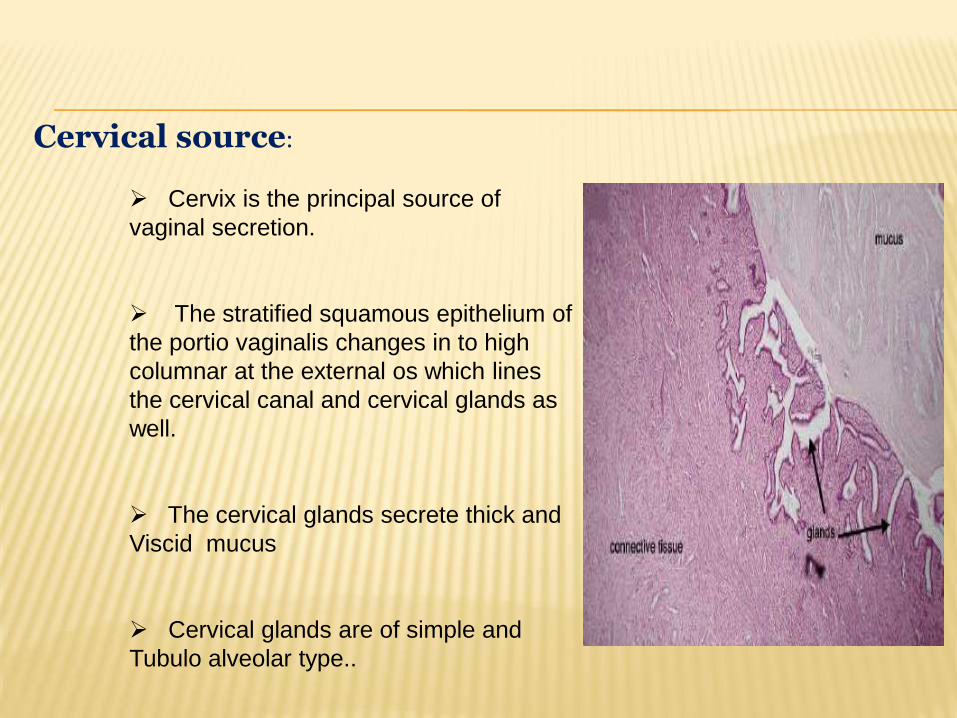
Cervical source:
Cervix is the principal source of
vaginal secretion.
The stratified squamous epithelium of
the portio vaginalis changes in to high
columnar at the external os which lines
the cervical canal and cervical glands as
well.
The cervical glands secrete thick and
Viscid mucus
Cervical glands are of simple and
Tubulo alveolar type..

UTERUS AND FALLOPIAN TUBES
Though uterus is lined by highly
secretory columnar epithelium,they
contribute less to the normal vaginal
secretion.
The secretion of the glands undergo
cyclic activity in the elaboration of
glycogen and other nutritive substances in
preparation for pregnancy each month
Tubes normally contribute nothing to
vaginal secretion.
In rare instance of a hydro salphinx
resulting from salphingitis,the tubal
secretions may be expelled through
vagina,in the form of watery discharge.

VAGINAL MICRO ORGANISMS :
The vaginal eco system is a complex environmental condition,consisting of
inter relationships among the endogenous microflora,metabolic products of
microflora,host oestrogen and the pH.
Vaginal infection and inflammation
occurs when vaginal eco system is
altered.
When the balance of micro organism
changes,potentially pathogenic
organisms that are part of normal flora
proliferates and lead on to overt
infection.

Besides lacto bacillus,other organisms in vaginal flora includes—
Bacteroids,Beta haemolytic and non haemlytic stretococci,Candida albicans,
Diptheroids,enterococci,E.coli,mobiluncus,M.hominis,Peptostreptococci spp,
Staph.epidermidis and Ureaplasma urealyticum.
Contd...

VAGINAL ECO SYSTEM

NON INFECTIVE LEUKORRHEA :
Non infective leukorrhea should be considered as the diagnosis when
following criteria are fulfilled.
ENDO CERVICAL SECRETIONS:
Absence of visible mucopus
Absence of microscopic mucopus

Contd...
Vaginal secretion :
Absence of trichomonad motility,
Absence of filamentous elements,
Clue cells less than 20% of vaginal epithelial cells,
Numerous lactobacilli
Polymorpho nuclear leukocytes: Epithelial cell ratio is
1:1 or less
If all seven criteria are fulfilled, vaginal and cervical infections can be safely
excluded.

CAUSES FOR VAGINAL DISCHARGE
PHYSIOLOGICAL :
AGE-DEPENDENCE :
1.NEONATE AND INFANT
2.PRE-PUBERTY
3.CHILD BEARING
4.POST MENOPAUSAL
--
CONTD.

EXCESSIVE SECRETION :1.PREGNANCY
2.SEXUAL AROUSAL
PATHOLOGICAL :
A) NON-INFECTIVE
CHEMICAL IRRITATION –Antiseptics,bath additives
deodorants,detergent spermicides,douches,
perfumed soaps.
-CONTD..
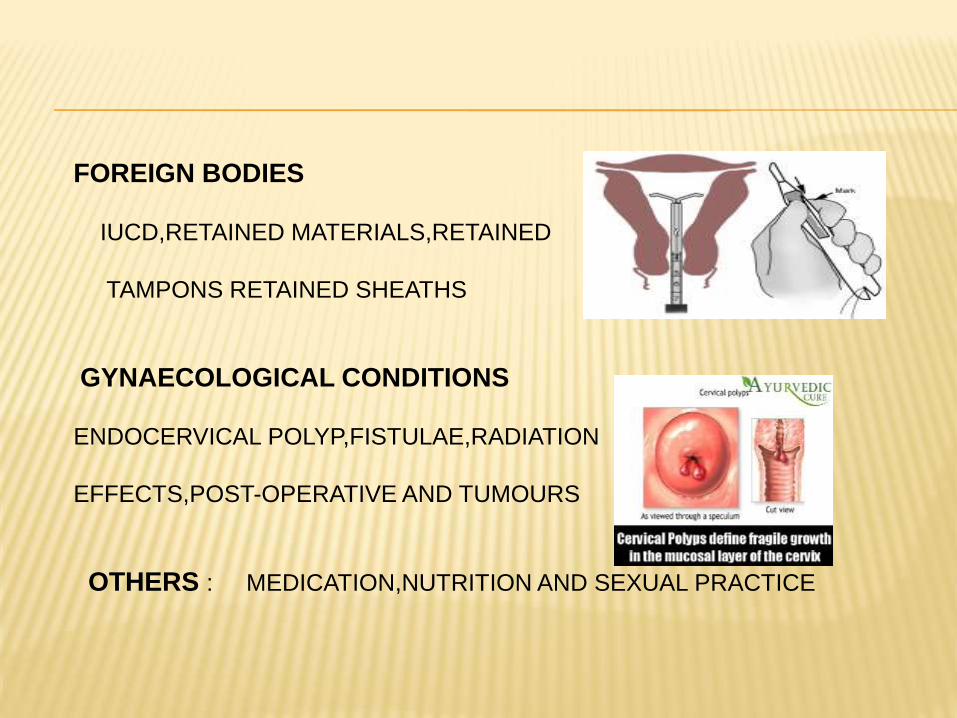
FOREIGN BODIES
IUCD,RETAINED MATERIALS,RETAINED
TAMPONS RETAINED SHEATHS
GYNAECOLOGICAL CONDITIONS
ENDOCERVICAL POLYP,FISTULAE,RADIATION
EFFECTS,POST-OPERATIVE AND TUMOURS
OTHERS : MEDICATION,NUTRITION AND SEXUAL PRACTICE

INFECTIVE CAUSES
CERVICITIS1.HERPES GENITALIS
2.MUCOPURULENT CERVICITIS— a) Gonococcal
b) Non gonococcal- Chlamydia
positive and Chlamydia negative
VAGINITIS
1.BACTERIAL VAGINOSIS
2.VAGINAL CANDIDIASIS
3.VAGINAL TRICHOMONIASIS

AGE DEPENDANT PHYSIOLOGICAL CONDITION :
NEONATE AND INFANTS:
Neonatal vagina is lined by st.squamous
epithelium due to influence of maternal oestrogen.
After 1 month to puberty lined by cuboidal
epithelium [PH -7.0].Neonatal physiological discharge results from
maternal estrogen action on vaginal epithelium.
Maternal estrogen is metabolised in 3-4 weeks.

SUSCEPTIBILITY TO INFECTIONS :
EARLY NEONATE Vaginal epithelium susceptible to
T.vaginalis and C.albicans due to peri
natal transmission.
Resistant to N.gonorrhea and
C.trachomatis.
OLDER INFANTS Susceptible--N.gonorrhea&C.trachomatis
Resistant to Candida.
EARLY NEONATE
OLDER INFANTS
PRE-PUBERTY :
Pre puberty physiological discharge is a hall mark
of
Impending onset of menarche
Due to unopposed secretion of estrogen the
ovaries stimulates vaginal and cervical secretions
leading to discharge
It is thin and mucoid and soils under
garments.This discharge may be interpreted as
infection.
It ultimately subsides with the onset of cyclic
progesterone activity.
CHILD BEARING AGE :Causes for increased vaginal secretion during child bearing
age is as follows:
1.Mid cycle stimulation of endo cervical
glands by oestrogen
2. EXOGENOUS-Semen of recent
ejaculation
3. Mid cycle discharge is sufficient to
keep the vagina
moist and usually does not stain the under garments.It may
be associated with
Mittelshmerz or mid cycle unilateral pelvic discomfort.

POST MENOPAUSAL PERIOD
There is atropy of vaginal epithelium due to diminished
estrogen secretion
Thin,serous discharge,occasionally blood
stained and associated with itching and burning.
Small areas of granulation and ulceration along
with slight vaginal bleeding may develop.
Most common cause of
Abnormalvaginaldischarge is Atropic vulvovaginitis.
EXCESSIVE SECRETION
PREGNANCY
o Physiological discharge,floccular in
characteristics,may exceed
1ml of amount on speculum examination.
o Occurs due to increased vascularity,congestion of
pelvic organs
and cervical hyperplasia.
SEXUAL AROUSAL
o In non pregnant women,sexual arousal results in increased
discharge,due to secretion from Bartholins glands.
NON-INFECTIVE CONDITIONS CAUSING AVD
CHEMICAL IRRITANTS
Antiseptics,deodarants,detergent
spermicides,douches and perfumed soaps-
Chemical induced vulvovaginitis
Allergic reaction raraely cause discharge,often
associated with local reaction.
MANAGEMENT- Avoiding irritants and saline baths.

...contd
Long term use of tampons and multiple douching should
generally be avoided
, as they increase the discharge due to drying effect and
alteration of vaginal flora
Commercial preparations leads to abnormal shift in
vaginal flora.
Douching should be generally avoided.But if patient persists
mild vinegar solution and water could be used.

FOREIGN BODIES :
Foreign bodies—cotton wool from tampons often becomes entained with
thread of IUCD and act as source of infection.
Retained tampons & broken sheath may result in persistent infection
producing copious,foul smelling discharge
It is necessary to remove the foreign body and then the vaginal flora will
rapidly return to normal.

GYNAECOLOGICAL CONDITIONS :
DISCHARGE CAUSE
Mucoid and blood tinged Endo cervical polyp
Profuse watery discharge with Uro genital fistula
out mucoid element---Urine
Clear discharge,slight bloody Vaginal vault Granulation tissue
Secretion[following Hysterectomy]
Heavy vaginal discharge Benign tumours
Frank bleeding Malignant tumours
Purulent discharge Bacterial infections

MEDICATION AND SEXUAL PRACTICE
Alternative medicinal drugs,over the counter medicinal products and nitritive
compounds may be associated with infective or non infective discharge
Examples include oral and vaginal metronidazole lead to an increase inlacto
bacilli which persists for 1 month after therapy and Intra vaginal Clindamycin
has caused a decrease in lacto bacilli 1 week post-therapy.
Sexual activities and change in sexual partners may alter the normal vagina
Flora leading to vaginal discharge.
