abnormalities of predictive saccades in...
TRANSCRIPT

Brain (1992), 115, 1147-1165
ABNORMALITIES OF PREDICTIVE SACCADES INHEMI-PARKINSON'S DISEASE
by J. VENTRE,1 D. S. ZEE,2 H. PAPAGEORG1OU2 and S. REICH2
(From the 'Vision et Motricite, INSERM U94, Bron, France and the 1Department of Neurology, TheJohns Hopkins Hospital, Baltimore, USA)
SUMMARY
We studied reflexive and predictive saccades by direct current electro-oculography in nine patients withmild hemi-Parkinson's disease (hemi-PD) and in 16 age-matched controls. In five patients, the neurologicalsyndrome was predominant on the right side of the body (RPD) and in four patients, on the left side (LPD).Reflexive saccades were elicited in response to the random appearance (timing and location) of a light-emitting diode (LED). Predictive saccades were elicited by alternatively illuminating LEDs at 10 degreesright and left, at various fixed frequencies (0.25 — 1 Hz).
In the reflexive task, latency and amplitude of the saccades were normal in both PD groups. In the predictivetask, mean saccade latency was not significantly different between patients and normals but there weretwo significant abnormalities in timing: first, but only in LPD, a directional asymmetry in latency (leftgreater than right, e.g. at 0.25 Hz, mean difference of 90 ms); secondly, especially in RPD, an abnormaltracking pattern, reflected by more variability of the mean value (for each group of patients) of saccadelatency at each point in time, throughout a period of tracking at a given frequency. Predictive saccadeswere also strongly hypometric in both PD groups but especially in LPD (e.g. for rightwards saccades:controls = 19 degrees, SD = 1.6; LPD = 14 degrees, SD = 2.7; RPD = 15.7 degrees, SD = 2.3).These defects in saccadic timing and amplitude during predictive tracking were most salient at lowfrequencies. While these defects were largely bilateral, our findings suggest slightly different contribu-tions of the right and left cerebral hemispheres to the spatial and timing components, respectively, thatcomprise optimal predictive saccadic behaviour.
INTRODUCTION
Parkinson's disease (PD) is a degenerative disorder characterized by a loss of dopa-minergic neurons in the substantia nigra pars compacta (SNPC). In addition to asomatomotor syndrome consisting of tremor, rigidity and bradykinesia, there are alsoabnormalities of eye movements (Kennard and Lueck, 1989; Leigh and Zee, 1991).In patients with mild PD, the saccades are delayed and hypometric in tasks that primarilyreflect internally generated volitional motor programs, such as the response to targetsmoving in a predictable fashion (Bronstein and Kennard, 1985; Nomura et al., 1986;Crawford et al., 19896; Kennard and Lueck, 1989; Lueck et al., 1990). Saccades areless impaired in tasks that test reflexive types of behaviour such as externally triggeredresponses to novel visual stimuli.
Recent electrophysiological studies in the basal ganglia and in the frontal lobes ofmonkeys have linked both of these structures to the generation of more volitional saccades,in the context of learned, remembered or anticipated behaviour (Hikosaka and Wurtz,1983a,b,c,d; Bruce and Goldberg, 1985; Deng etal., 1986; Joseph and Barone, 1987;Goldberg and Segraves, 1989; Hikosaka and Wurtz, 1989; Hikosaka etal., l9S9a,b,c).
Correspondence to: Dr Jocelyne Ventre, INSERM U94, 16 Avenue Doyen Lepine, 69500 Bron, France.
© Oxford University Press 1992

1148 J. VENTRE AND OTHERS
Clinical studies of patients with PD and of patients with Huntington's disease (HD)also suggest that the frontal lobes and basal ganglia participate in the control of voluntarysaccades (Bronstein and Kennard, 1985; Lasker et al., 1987, 1988; Crawford et al.,l9S9a,b; Lueck et al., 1990; Tian et al., 1991).
In the present study, we recorded saccadic eye movements in patients with mild hemi-Parkinson's disease (hemi-PD), using a predictive tracking paradigm to learn (i) if thereare directional asymmetries in predictive behaviour and (ii) if the right and left cerebralhemispheres make different contributions to the spatial and the temporal aspects ofpredictive tracking. Our results confirm a deficit in predictive saccadic tracking in hemi-PD, especially at low frequencies. Surprisingly, the ocular motor deficits were largelybilateral in spite of the striking somato-motor asymmetry. Nevertheless, there was someasymmetry in the ocular motor abnormalities suggesting that there may be a differencebetween the contributions of the left and right cerebral hemispheres to both the temporal(timing) and the spatial (location) components necessary for generating optimal antici-patory responses during a predictive tracking task.
METHODS
Subjects
Nine right-handed patients with hemi-PD (four females, five males; mean age 59 yrs, range 51 —69 yrs)and 16 right-handed, age-matched normals (11 females, five males; mean age 54 yrs, range 29-70 yrs)were investigated (Table 1). The patients were all followed in the movement disorder clinic and the
TABLE I. CHARACTERISTICS OF PATIENTS
PDpatients
RPD M.A.R.L.U.T.P.J.C.B.A.K.R.K.
LPD A.D.L.L.H.
Q.L.D.S.E.V.
Sex
FFMFF
MM
MM
Age(yrs)
6655515652
6965
6357
lUnessduration
(mths)
18119405632
7671
479
New YorkUniversitydisability(max. 52)
95
134
10
1510
87
TremorMax./side = 8
R62300
00
00
L00000
53
33
RigidityMax. /side = 8
R22434
21
I1
L00202
43
32
Bradykinesia
BLUL*UL**U L "UL
UL*UL**
BLUL»*
Anti-PDmedication
SinemetArtaneSinemet, Eldepryl
Sinement, ArtaneSinemet, EldeprylAmantadineSinemetSinemet
Tremor was evaluated at the hand and rigidity at the elbow. Bradykinesia was scored on the basis of the timed-fingerand foot-tapping tasks. • = mild; ** = severe asymmetry; UL = unilateral; BL = bilateral.
age-matched normals were a mixture of spouses of patients and hospital employees and their relatives.All the patients were clinically examined by a neurologist (S.R.) and the PD disability was scored usingthe New York University rating scale with a maximal score of 52 (Lieberman, 1974). A score of 0 to4 is assigned to the following abnormalities: tremor, rigidity, bradykinesia, gait and postural stability.Bradykinesia was evaluated using timed finger and foot tapping. All subjects gave informal consent toparticipate in this study. The patients were divided into two groups according to the affected side of theirneurological syndrome: five patients had a right hemi-PD (RPD) and four patients a left hemi-PD (LPD).

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE 1149
Apparatus and eye-movement recordings
The subjects were seated in a dark room in front of an arc (radius 123 cm) supporting light-emittingdiodes (LED). The target lights subtended 0.1 degree of visual angle and were located at 10, 20 and 30degrees right and left from the centre (0 degree). Head movements were restricted by a chin rest.
Horizontal saccades were recorded from the right eye by direct-current electro-oculography. Eye blinkswere monitored by vertical eye movements recordings. Electro-oculography signals were amplified andfiltered with a low-pass analogue filter (40 Hz). The filtered analogue signals were digitized at a samplingrate of 100 Hz by computer and saved for off-line analysis.
Procedure and paradigms
Both non-predictive and predictive saccades were tested.Non-predictive paradigm (non-predictive stimulus). Each trial began with fixation of the centre LED.
A peripheral LED was illuminated and simultaneously the centre LED was switched off and a non-localizedbeep, 100 ms in duration, sounded. The peripheral LED was presented at a random time (1400-2400 ms),direction (right or left) and amplitude (10, 20 or 30 degrees). Subjects were told to move their eyes towardsthe peripheral light as quickly and accurately as possible.
Predictive paradigm (predictive stimulus). Targets alternated between two fixed locations (10 degreesright and left) at various fixed frequencies in the following sequence: 0.25, 0.5, 1, 0.33 and 0.75 Hz.For each target frequency, 25 cycles of responses were collected. Subjects were told to move their eyesin time with the movement of the light.
Data analysis
An interactive computer program was used for saccade analysis; the accuracy of saccade identificationwas verified by visual inspection of each trial on a video monitor. For the non-predictive paradigm, saccadeswere calibrated independently for each eccentricity of targets. For the predictive paradigm, separatecalibrations were obtained for each frequency of target motion. This calibration procedure minimizedinaccuracy due to any fluctuations in the amplitude of the corneo-retinal potential.
For the non-predictive paradigm, the latency and the amplitude of the initial saccade in response to thetarget stimulus were computed.
For the predictive paradigm, saccades initiated within 100 ms of, or prior to, the target jump were classifiedas anticipatory. A negative latency indicated that the saccade was initiated before the target jumped. Ateach frequency of target motion, responses were divided into two groups: the anticipatory and the non-anticipatory saccades. The percentage of anticipatory saccades was calculated. For all of the predictivesaccades (anticipatory and non-anticipatory saccades) and for each of the subgroup of non-anticipatoryand anticipatory saccades, the analysis of latency and amplitude was performed independently for therightwards and the leftwards responses.
A normal range for each parameter was established from the mean ±2 SD of the control group. Datawere analysed using ANOVA, the Student's / test and the Mann-Whitney test, performed by theSTATGRAPHICS software package. For ANOVA, within-group factors were the subject, the directionof the target and the frequency of the target motion. The dependent variables were the saccade latencyand the saccade amplitude for the non-predictive and predictive paradigms, and also the percentage ofanticipatory saccades for the predictive paradigm. A 95% confidence interval was used to establish statisticalsignificance.
RESULTS
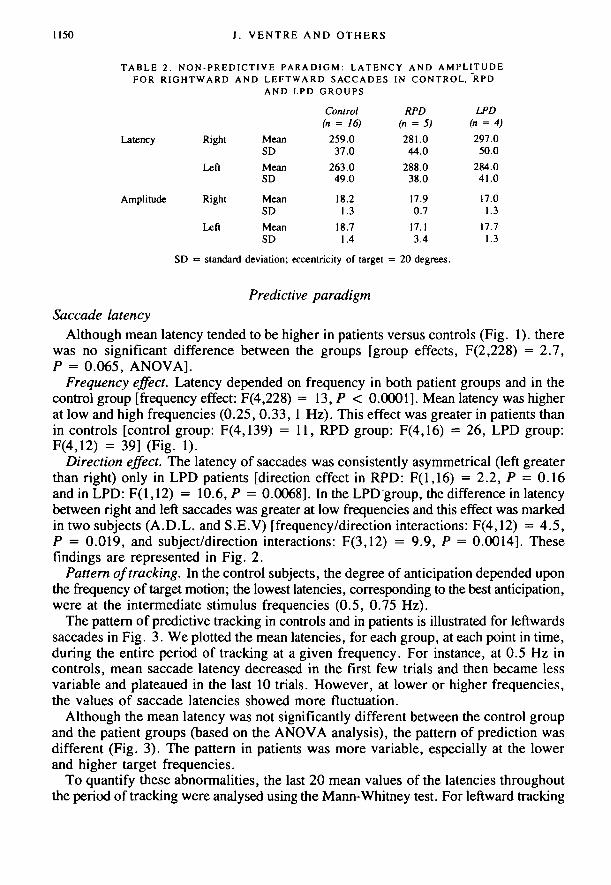
Non-predictive paradigmThe latency of visually triggered saccades was slightly but not significantly (P > 0.05,
t test) increased in both directions for both hemi-PD groups (Table 2). The amplitudefor 20 degree saccades was normal {P > 0.05, t test) for each hemi-PD group (Table 2)though one RPD patient (R.K.) showed an abnormal amplitude (11.1 ±3.2 degrees)for leftward saccades (control group: mean = 18.7 degrees; 2 SD = ±2.8).
MeanSD
MeanSD
MeanSD
MeanSD
Control(n = 16)
259.037.0
263.049.0
18.21.3
18.71.4
RPD(n = 5)
281.044.0
288.038.0
17.90.7
17.13.4
LPD(n = 4)297.050.0
284.041.0
17.01.3
17.71.3
1150 J. VENTRE AND OTHERS
TABLE 2. NON-PREDICTIVE PARADIGM: LATENCY AND AMPLITUDEFOR RIGHTWARD AND LEFTWARD SACCADES IN CONTROL, "RPD
AND LPD GROUPS
Latency Right
Left
Amplitude Right
Left
SD •= standard deviation; eccentricity of target = 20 degrees.
Predictive paradigmSaccade latency
Although mean latency tended to be higher in patients versus controls (Fig. 1). therewas no significant difference between the groups [group effects, F(2,228) = 2.7,P = 0.065, ANOVA].
Frequency effect. Latency depended on frequency in both patient groups and in thecontrol group [frequency effect: F(4,228) = 13, P < 0.0001]. Mean latency was higherat low and high frequencies (0.25, 0.33, 1 Hz). This effect was greater in patients thanin controls [control group: F(4,139) = 11, RPD group: F(4,16) = 26, LPD group:F(4,12) = 39] (Fig. 1).
Direction effect. The latency of saccades was consistently asymmetrical (left greaterthan right) only in LPD patients [direction effect in RPD: F(l,16) = 2.2, P = 0.16and in LPD: F(l,12) = 10.6, P = 0.0068]. In the LPD group, the difference in latencybetween right and left saccades was greater at low frequencies and this effect was markedin two subjects (A.D.L. and S.E.V) [frequency/direction interactions: F(4,12) = 4.5,P = 0.019, and subject/direction interactions: F(3,12) = 9.9, P = 0.0014]. Thesefindings are represented in Fig. 2.
Pattern of tracking. In the control subjects, the degree of anticipation depended uponthe frequency of target motion; the lowest latencies, corresponding to the best anticipation,were at the intermediate stimulus frequencies (0.5, 0.75 Hz).
The pattern of predictive tracking in controls and in patients is illustrated for leftwardssaccades in Fig. 3. We plotted the mean latencies, for each group, at each point in time,during the entire period of tracking at a given frequency. For instance, at 0.5 Hz incontrols, mean saccade latency decreased in the first few trials and then became lessvariable and plateaued in the last 10 trials. However, at lower or higher frequencies,the values of saccade latencies showed more fluctuation.
Although the mean latency was not significantly different between the control groupand the patient groups (based on the ANOVA analysis), the pattern of prediction wasdifferent (Fig. 3). The pattern in patients was more variable, especially at the lowerand higher target frequencies.
To quantify these abnormalities, the last 20 mean values of the latencies throughoutthe period of tracking were analysed using the Mann-Whitney test. For leftward tracking

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE
A
115!
300
200.
100-
0 .
•100.
-200.
•300
300
200
100.
0 -
•100-
-200-
-300
1? ! ll
{ .j If[ ^
B
I
T
- i . 00 -0,75 -0.50 -0.25 0 0 25 0.50 0.
Left Right
Target frequency (Hz)
75 1.00
FIG. 1. Rightward and leftward saccade latencies during predictive tracking as a function of the target frequency.A, comparison between control ( • ) and RPD (O) group. B, comparison between control ( • ) and LPD (O) group.
(see Fig. 3), there were significant differences compared with normal for both patientgroups at low frequencies (0.50, 0.33, 0.25 Hz) and for RPD patients also at 1 Hz.For rightward tracking, there were significant differences (P < 0.05) only in RPD patientsand only at some frequencies (0.25, 0.5, 1 Hz).
To summarize, the mean latency was normal in both patient groups. In the LPD grouponly, a directional asymmetry in latency was found between rightward and leftwardsaccades (left greater than right). Furthermore, especially in RPD, the pattern of trackingwas abnormal as reflected in more variability of the mean values of saccadic latencyover time, at a given frequency. These defects in latency were usually more pronouncedat low frequencies.
Saccade amplitudePatients showed a considerable decrease in saccade amplitude compared with normals
[group effect: F(2,228) = 42, P < 0.0001, ANOVA]. The decrease in mean amplitudewas greater in LPD than in RPD patients [F(l,70) = 5, P = 0.026] (Fig. 4).

1152 J. VENTRE AND OTHERS
RPD300 i
200
100
0
-100
200
t :
ll 1 n ' f in1 nil JillJ ' 1: :
1, Jl 11 :
' lUl-300
ti?tQ> <£><$> # r y > rf?r$>
Control B.A.K. L U.T. M.A.R. P.J.C. R.K.
300
200
B 100
S o
LPD
• Bight• Left
ro
-200 •
•300
L In1!JL
Control A.D.L LH O L D SE V
FIG. 2. Saccade latency during predictive tracking at the target frequencies of 0.25 Hz and 0.33 Hz. The mean valuesare represented for the control group (with standard deviation) and for each individual of the patient group. Right,rightward saccades; left, leftward saccades.
Frequency effect. The decrease in amplitude depended on frequency [frequency effect:F(4,228) = 11, P < 0.0001, ANOVA]: the lower the target frequency, the lower thesaccade amplitude (Fig. 4).
Direction effect. The mean amplitude depended on saccade direction: the meanamplitude was slightly higher for rightward saccades in the control group and moreso for leftward saccades in both hemi-PD groups. The effect of saccade direction onthe accuracy within each patient group was analysed.
In RPD, all patients except one (R.K.) showed a significant difference in amplitudebetween right and left saccades (left greater than right); this effect was independentof the stimulus frequency (Fig. 5) [main effect of the direction factor F(l ,16) = 17.7,P = 0.0007; subject/direction interactions F(4,16) = 19, P < 0.0001; frequency/direction interactions: F(4,16) = 1, P = 0.38].

PREDICTIVE SACCADES IN HEMI-PARKINSONS DISEASE 1153
400
200
0 •
-200
•400
0.25 Hz
Control
rnr
0.50 Hz
Control
1 Hz
Control
V)
E
£3
400
200
0
-200
-400
RPD
i iII, . il
' ! | 1 • 1 ,1 " l|l
P< 0.001
RPD
= 0.002
RPD
i , . . I l n , l i i h l . i I
P< 0.001
400
200
0
-200
-400
LPD LPD
I I I
P< 0.001
10 20 30
I
LPD
" I ' l l l l l l l ' 1 ' l | | l. 1
l ' l l
NS
30 10 20 30
FIG. 3. Pattern for leftward saccades during predictive tracking at different target frequencies (0.25, 0.50, 1 Hz),for control, RPD and LPD group. Each vertical bar represents the saccade latency averaged at each trial for all thesubjects in each group. Significant abnormalities (P < 0.05, Mann-Whitney test) in the variability of the tracking patternare noticeable between the control and the patient groups. NS = no significance.
In LPD, all patients except one (S.E.V.) showed a difference in amplitude betweenright and left saccades (left greater than right); this effect was greater at low frequencies(Fig. 5) [main effect F(l,12) = 1 3 , P = 0.0035; subject/direction interactions:F(3,12) = 8, P = 0.003; frequency/direction interactions: F(4,12) = 5.6, P = O.0087].
To summarize: the mean amplitude for saccades in both directions was decreasedin both groups of hemi-PD patients. This amplitude defect was more pronounced inLPD group and for the saccades directed to the right.
Amplitude variability. Saccade amplitude was highly variable over the 25 cycles oftracking, especially in the LPD patients. This variability was quantified by calculatingthe standard deviation of the mean value of amplitude for each subject over the last20 trials, at each frequency (Fig. 6). Then, a mean value of the standard deviationswas calculated for all subjects in each group. We found a significant increase (P < 0.05,student's t test) in the mean value of the standard deviations in both patient groups,mainly at low frequencies (Fig. 6).

1154 J. VENTRE AND OTHERS
2 5 ,
20 .
15.
10 .
5-
£ 0
fI B
™ 2 5 ,
20.
15.
10.
5.
\ \ \
-1.00 -0.75 -0.50 0 25 0 0 25 0.50 0 75 1.00
Left RightFrequency
FIG. 4. Saccade amplitude during predictive tracking as a function of the target frequency, A, comparison betweencontrol ( • ) and RPD (O) group. B, comparison between control ( • ) and LPD (O) group.
Anticipatory and non-anticipatory saccades. We further analysed saccades duringpredictive tracking by separating responses into anticipatory and non-anticipatory. Ananticipatory saccade was defined as a saccade initiated with a latency before or within,100 ms of the target jump. The percentage of anticipatory saccades in the patient groupswas slightly but not significantly decreased with respect to the normal group[F(2,228) = 2.8, P = 0.064, ANOVA]. The percentage of anticipatory saccadesdepended on stimulus frequency in both patient and control groups [F(4,228) = 24,P < 0.0001]. As the frequency increased, the percentage increased, only to fall againwhen the frequency reached 1 Hz (Fig. 7).
There was, however, a highly significant abnormality in the amplitude of anticipatorysaccades in both PD groups [group effect: F(2,225) = 67, P < 0.0001]; the amplitudedeficit depended on frequency [frequency effect: F(4,225) = 21, P < 0.0001] and wasmore prominent in the LPD group [F(l,70) = 4.5, P = 0.04] (Fig. 8). The decreasein the amplitude of anticipatory saccade was independent of the response direction

PREDICTIVE SACCADES IN HEM I-PARKINSON S DISEASE 1155
2.5 •
- 2 .5 •
-5-1
Amplitude difference (R minus L)
RPD
Control B.A.K. L.U.T. M.A.R. P.J.C. R.K.
• 0 25 Hz• 0.33 HzW 0.50 Hz
LPD
Control A.D.L. L.H. Q.L.D. S.E.V.
FIG. 5. Difference of amplitude between right and left saccades during predictive tracking al different target frequencies(0.25, 0.33, 0.50, 1 Hz). The mean values are represented for the control group (with standard deviation) and for eachindividual of the patient groups. Negative bars indicate hypometria of rightwards saccades.
[direction factor effect: F(l,225) = 2.2, P = 0.13]. This result was confirmed bycomputing a / test on the difference of the mean amplitude between right and left saccadesin each patient group (RPD: t = 1.2, P = 0.28; LPD: t = - 0 . 1 1 , P = 0.92).
The amplitude of the non-anticipatory saccades during predictive tracking was slightlydecreased only in the LPD patients [group effect: F(2,221) = 9.5, P = 0.0001]. Thenon-anticipatory saccade amplitude was independent of the stimulus frequency (Fig. 8).Both ANOVA and a t test showed significant asymmetry in the amplitude of non-anticipatory saccades due to a decrease in the amplitude for rightward saccades in patientsgroups (RPD, / = -3 .6 , P = 0.02; LPD, t = - 1 6 , P = 0.00008; Student's / test)(Fig. 8).

1156 J. VENTRE AND OTHERS
"5 4
E 3 •
Q 2
1 •
• Control• RPD• LPD
1 0.75 0.5 0.33 0.25 0.25 0.33 0.5 0.75 1
Left RightTarget frequency (Hz)
Fie. 6. Standard deviation (SD) of saccade amplitude during predictive tracking at the different target frequenciesfor the control, RPD and LPD groups. *P < 0.05; **P < 0.01; ***P < 0.001 (Student's Itest).
100-,
80 -
oa 40
c
o
-0 50 -0 25 0 0.25
Target frequency (Hz)
050 0.75 1 00
FIG. 7. Percentage of anticipatory saccadcs as a function of the target frequency, for the control ( • ) , RPD (O)and LPD ( • ) groups. Each point represents the mean of the percentage values of all the subjects in each group.
To summarize: the decrease of saccade amplitude was mainly apparent in theanticipatory responses in both hemi-PD groups; this amplitude defect depended uponfrequency and was more marked in LPD patients, but it did not correlate with responsedirection.
Latency-amplitude correlationBy a linear regression analysis, we found a significant positive correlation between
saccade latency and amplitude at low frequencies, in both patient groups (P < 0.0001

PREDICTIVE SACCADES IN H EMI PARKINSON S DISEASE
A
2 5 1
20.
15.
10.
5.
1157
\ * If
25 -
20
•o 15
8W
10"
25
2 0 .
15.
10.
5 .
\ \
-100 0.7S 0 5 0 - 0 25 0 0 2S 0 50 0 75 100
Target frequency (Hz)
FIG. 8. Mean amplitude of the non-anticipatory (filled symbols) and of the anticipatory (open symbols) saccade asfunction of the target frequency, A, the control group; B, the RPD group; and c, the LPD group.
at 0.33 and 0.25 Hz, P < 0.05 at 0.5 Hz) but not in controls. At high frequencies(1 Hz), a significant latency-amplitude correlation was found mainly for leftwardssaccades in both patient groups.

1158 J. VENTRE AND OTHERS
DISCUSSION
The main finding of this study is that patients with mild hemi-PD show abnormalitiesof saccades during tracking of targets jumping with predictable timing and location,but not to targets jumping to random locations at unpredictable times. This effect wasindependent of the side affected. The patients demonstrated hypometria of saccades andincreased variability in the pattern of tracking. The deficits, usually greatest at lowfrequencies of target motion, were largely bilateral in both RPD and LPD. However,in patients with LPD, overall saccadic hypometria (for saccades in both directions) wasgreater and saccade latency was asymmetric (left latency greater than right latency).On the other hand, in patients with RPD, the pattern of timing during prediction wasmore variable.
We will discuss these results first by reviewing some aspects of the normal physiologyof the basal ganglia relevant to saccadic eye movements. Secondly, we will considerthe nature of the deficits of prediction in PD. Finally, we will speculate upon therelationship between the ocular motor findings and the asymmetry of the somato-motordeficits in our patients.
Saccade abnormalities in basal ganglia diseaseNormal ocular motor physiology of the basal ganglia. The superior colliculus (SC)
appears to participate in the generation of all types of saccades. The basal ganglia maygate activity in the SC, to facilitate more volitional types of saccades and to suppress,when necessary, more reflexive types of saccades. By virtue of successive inhibitorypathways from the caudate nucleus (CN), to the substantia nigra pars reticulata (SNPR),and then from the SNPR to the SC, the basal ganglia can modulate activity within theSC (Hikosaka and Wurtz, \9S3a,b,c,d, 1985a,*; Hikosaka et al., 1989aAc). The frontaland parietal lobes may also modulate activity in the SC by direct projections as wellas through projections to the CN (Petras, 1971; Fries 1984, 1985; Komatsu and Suzuki,1985; Lynch et al., 1985; Selemon and Golman-Rakic, 1985; Huerta et al., 1986;Updyke, 1986; Segraves and Goldberg, 1987; Selemon and Goldman-Rakic, 1988;Stanton et al., 1988).
Pathophysiology of basal ganglia disturbances of eye movements. In HD, there arepathological changes in the CN and probably also in the SNPR (Albin et al., 1989;Oyanagi et al., 1989). Patients with HD show defects in initiating more voluntary saccades(including those in predictive tracking paradigms) and in suppressing, uncalled-for,reflexive saccades (Lasker et al., 1987; 1988; Tian et al., 1991).
In PD, the main pathologic effect is seen in the SNPC. Although the SNPC has noknown ocular motor function, it could influence activity in the CN, or even the SNPR,by virtue of its direct projections to both structures (Hikosaka and Wurtz, 1989). Likepatients with HD, patients with PD have difficulty initiating voluntary saccades (Bronsteinand Kennard, 1985; Crawford et al., 1989a; Lueck et al., 1990).
However, the saccadic eye-movement defects in PD differ in some respects from thosein HD. A loss in the ability to suppress uncalled-for reflexive saccades, the oculomotorsine qua non for HD (Lasker et al., 1987), has not been observed in PD (Crawfordet al., 19896). Although patients with either PD or HD have difficulty generating predictivesaccades, abnormalities of latencies are more prominent in HD and abnormalities ofaccuracy more prominent in PD (Crawford et al., 1989*; Tian et al., 1991).

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE 1159
The reasons for the differences in eye movements between HD and PD are not clear.Dysmetric and delayed saccades are produced by acute pharmacological lesions of theSC (Hikosaka and Wurtz, 1985a, 1986; Lee et al., 1988). It is possible that both thelevel of tonic activity in the SNPR, and the level of phasic activity that occurs in relationto saccades (either in the CN or in the SNPR), determine whether or not there willbe hypometria and/or delay in initiating saccades. Which abnormality predominates inpatients with HD or PD might depend upon the relative differences between alterationsin phasic and in tonic activity emanating from the basal ganglia.
On the other hand, it is difficult to attribute specific ocular motor defects to malfunctionin a single structure or in a particular population of neurons, since defects in one structureoften lead to changes in distant ones. For instance, in PD, metabolic changes affectnot only the substantia nigra and striatum but also the thalamus and the frontal lobes(Wolfson et al., 1985; Ho et al., 1988; Mitchell et al., 1989; Palombo et al., 1990).
Predictive tracking in normal subjects and in patientsAccurate predictive saccadic tracking requires that the temporal (timing) and the spatial
(location) components of the motion of the target are correctly stored in memory andthen used, in lieu of direct visual information, to trigger a saccade of the right amplitudeat the right time. In normal subjects, the ability to anticipate the motion of the targetin a predictive tracking task is best at a target frequency of about 0.5 Hz. At lowerand higher frequencies the degree of anticipation is less though accuracy is relativelymaintained.
Only a few studies have reported the effects of focal structural lesion on predictivetracking capabilities. Lesions of both frontal and parietal structures have been implicatedin predictive tracking deficits but specific details of how the lesions affected amplitudeversus timing are scanty (Pyykko et al., 1984; Bruce and Borden, 1986; Sharpe, 1986;MacAvoy and Bruce, 1989; Ron et al., 1989). In patients with HD, the predominantdefect in predictive tracking is an increase in latency; the degree of anticipation isconsiderably less than that of normal subjects (Tian et al., 1991).
Abnormalities of predictive tracking in PDPatients with PD also show abnormalities during predictive tracking but the degree
of defect is subject to the specific nature of the instructions and of the task (Bronsteinand Kennard, 1985; Crawford et al., 19896). Performance was relatively worse if thepatient was informed of the predictive nature of the task and relatively better when anauditory cue was substituted for a visual one.
Amplitude disorders. The most striking defect of prediction in PD is hypometria ofsaccades (Bronstein and Kennard, 1985; Crawford et al., 19896). Our patients, too,showed a decrease in amplitude of predictive saccades and we also found that the degreeof hypometria was closely related to the latency; saccades made at lower latencies weresmaller. Moreover, the amplitude of saccades during a period of tracking was morevariable than in normal subjects. During predictive tracking, as expected, hypometriawas present mainly for the anticipatory saccades (latency < 100 ms) since hypometriawas not present for saccades made in the reflexive paradigm. Presumably during thepredictive paradigm, all saccades made within 100 ms of the target jump had no immediatevisual information available to assist in programming saccade amplitude while saccades

1160 J. VENTRE AND OTHERS
made well after the target jumped (e.g. >250 ms) had visual information available toadjust saccade size. Non-anticipatory saccades made with latencies between these extremesprobably reflect a mixture of internally generated and visually guided movements. Hence,they would be expected to, and did, show intermediate values of saccade amplitude.
The explanation for the hypometria of anticipatory saccades in PD does not appearto be one of an inaccurate memory of the spatial location of the target, since patientswith PD have been reported to make corrective saccades to the actual target location,even without new visual information (Crawford et al., 19896). Thus, during predictivetracking in PD, the problem is not an inability to register accurately the location ofthe targets in memory; rather it is an inability to generate an initial saccade of a largeenough amplitude.
Timing disorders. The abnormality of predictive timing in our patients was not simplya global decrease in the ability to anticipate the position of the target; the mean latenciesof the patient groups were not significantly different from those of normal subjects.Rather, the pattern of tracking was less consistent, as reflected in more fluctuation ofthe mean values of latency throughout each period of tracking at a given stimulusfrequency. Whether this defect is part of a generalized loss of fidelity of performance,as is suggested from the increase in the overall variability of saccade latency, or reflectsa specific defect in the ability to store and to use timing information during predictivetracking, is not known.
Frequency dependency of predictive deficits. In our patients, the defects in timingand amplitude were more prominent at lower frequencies. Occasionally, defects werealso seen at higher frequencies. Furthermore, the effect of frequency, per se, was greaterin patients than in normal subjects. At low frequencies, prediction may be more impairedbecause of an inability to sustain the memory trace of target timing, while at 1 Hz,PD patients may falter in prediction in a similar way to that described by Dejong andJones (1971) for eye movements and by Flowers (1978) and Bloxham et al. (1984) formanual tracking. Whether these effects of frequency are specific to patients with PDor also occur in patients with other conditions in which predictive behaviour is impaired,remains to be determined.
Asymmetrical ocular motor junction in hemi-PDDirectional asymmetry in hemi-PD patients. Why did our patients with hemi-PD not
show more directional asymmetry of their saccades abnormalities, considering theremarkable asymmetry of their somato-motor syndrome? Prior studies in hemi-PD haveshown minimal or no directional asymmetries in saccades to randomly appearing targets(Carl and Wurtz, 1985; Rascol et al., 1989). Only in memory-guided saccades has aclear-cut asymmetry, in peak velocity (slower to the side of the somato-motor deficit)but not in amplitude or latency, been reported.
In interpreting results in hemi-PD one must keep in mind several caveats. First, itmay be that the ocular motor abnormalities correlate with only one aspect of the somato-motor syndrome, for example the rigidity, the bradykinesia or the tremor. Our patientswere heterogeneous with respect to somato-motor abnormalities though there was noobvious correlation between the predominant somato-motor finding and the ocular motordeficit. Secondly, it had been shown with positron emission tomography in patients withhemi-PD that asymmetrical activity in the putamen was correlated with the somato-

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE 1161
motor syndrome, while the decrease of activity with the CN was not (Leenders et al,1990). Since the latter structure is more likely to be related to the control of eyemovements, a large asymmetry in saccade performance might not be expected. Thirdly,predictive tracking in either direction may be behaviour that can be relatively wellelaborated by either cerebral hemisphere. With respect to this last point there are bilateralcortical-striatal projections and considerable interhemispheric connections between thefrontal lobes (Selemon and Goldman-Rakic, 1985, 1988; Stanton et al, 1988). Theseanatomical interconnections might account for the largely bidirectional nature of theocular motor deficits in prediction in hemi-PD.
Directional asymmetries in experimental hemi-PD. In contrast, experimental studiesin monkeys made acutely hemi-parkinsonian with l-methyl-4-phenyl-1,2,3,6-tetrahydro-pyridine, have shown marked asymmetry of saccade function. Saccades were delayed,hypometric and slowed when directed toward the side of the affected limb (Miyashitaet al., 1990; Usui et al., 1990). These deficits were greatest for memory-guided saccades;predictive capabilities were not examined. Furthermore, these experimental studies arenot directly comparable to our results since, in patients there is often subtle involvementof the non-affected side of the body even when the somato-motor syndrome ispredominantly unilateral. Likewise, since the pace of damage in human subjects withhemi-PD is much slower, more compensation would be possible than in the relativelyacute animal models of hemi-PD.
Cerebral hemispheral specialization and PDThere is some evidence that the right and left cerebral hemispheres contribute to overall
motor control in slightly different ways. The right hemisphere is thought to be moreinvolved in the integration for spatial localization of the position of the target and theleft hemisphere in programming and learning bilateral motor sequencing (Kimura andArchibald, 1974; Jason, 1983a,6; Haaland et al, 1987; Fisk and Goodale, 1988;Harrington and Haaland, 1991). Although the ocular motor deficits in our patients werelargely bidirectional, our patients with hemi-PD did show several side-to-side differencesin predictive tracking.
For LPD patients, predictive latencies were greater for leftward saccades. This findingis consonant with the idea that the right cerebrum, including the basal ganglia, maybe relatively more important for triggering leftward than rightward saccades, whereasthe left cerebral hemisphere may be relatively equi-potent for triggering saccades ineither direction. Perhaps related is the finding that hemi-neglect in human patients isusually more prominent with right cerebral lesions. Furthermore, neuropsychologicaltests have shown a mild left hemispatial neglect in patients with LPD (Starkstein, 1987;Levin et al, 1991). This asymmetric defect in attention may account for the asymmetryin predictive latency in our patients with LPD. It is interesting that there was no asymmetryin latency for more reflexive, visually guided saccades, which suggests the idea thatour patients could have neglect that is specific for internally generated, rather than forexternally triggering behaviour.
Our patients with LPD also showed a greater degree of overall hypometria, and morevariability, than did RPD. Whether or not these findings reflect a specific aspect ofright cerebral hemisphere function related to programming the spatial components ofpredictive tracking remains to be proven.

1162 J. VENTRE AND OTHERS
On the other hand, patients with RPD showed more variability of saccade latency,across a wider range of frequencies, than did LPD patients. This finding suggests thatthe left cerebral hemisphere may play a more critical role in generating a precise estimateof the timing of the target during prediction.
To summarize, our results suggest that the left and the right cerebral hemispheresmake slightly different contributions to the timing and the spatial components thatcomprise optimal predictive saccadic behaviour. Furthermore, this finding is compatiblewith the idea that the functions of the basal ganglia are intimately related to cerebralcortex via reciprocal loops (Alexander et al., 1986; Alexander and Crutcher, 1990).Further studies in patients with focal cerebral (and basal ganglia) lesions may confirmor refute these speculations about hemispheric specialization in predictive ocular motorbehaviour.
A C K N O W L E D G E M E N T S
The authors wish to thank Cheryl Enger and Jean-Louis Martin for their helpful contribution in dataanalysis. This research was supported by NIH grant NS16375.
R E F E R E N C E S
ALBIN RL, YOUNG AB, PENNEY JB (1989) The functional anatomy of basal ganglia disorders. Trendsin Neurosciences, 12, 366—375.
ALEXANDER GE, DELONG MR, STRICK PL (1986) Parallel organization of functionally segregated circuitslinking basal ganglia and cortex. Annual Review of Neuroscience, 9, 357—381.
ALEXANDER GE, CRUTCHER MD (1990) Functional architecture of basal ganglia circuits: neural substratesof parallel processing. Trends in Neurosciences, 13, 266—271.
BLOXHAM CA, MINDEL TA, FRITH CD (1984) Initiation and execution of predictable and unpredictablemovements in Parkinson's disease. Brain, 107, 371—384.
BRONSTEIN AM, KENNARD C (1985) Predictive ocular motor control in Parkinson's disease. Brain, 108,925-940.
BRUCE CJ, BORDEN JA (1986) The primate frontal eye fields are necessary for predictive saccadic tracking.Society for Neuroscience Abstracts, 12, 1086.
BRUCE CJ, GOLDBERG ME (1985) Primate frontal eye fields. I. Single neurons discharging before saccades.Journal of Neurophysiology, 53, 603—635.
CARL JR, WURTZ RH (1985) Asymmetry of saccadic control in patients with hemi-Parkinson's disease.Investigative Ophthalmology and Visual Science, 26, Supplement, 258.
CRAWFORD TJ, HENDERSON L, KENNARD C (1989a) Abnormalities of nonvisually-guided eye movementsin Parkinson's disease. Brain, 112, 1573-1586.
CRAWFORD T, GOODRICH S, HENDERSON L, KENNARD C (19896) Predictive responses in Parkinson's disease:manual keypresses and saccadic eye movements to regular stimulus events. Journal of Neurology,Neurosurgery, and Psychiatry, 52, 1033-1042.
DEJONG JD, JONES GM (1971) Akinesia, hypokinesia, and bradykinesia in the oculomotor system of patientswith Parkinson's disease. Experimental Neurology, 32, 58—68.
DENG SY, GOLDBERG ME, SEGRAVES MA, UNGERLEIDER LG, MISHKIN M (1986) The effect of unilateralablation of the frontal eye fields on saccadic performance in the monkey. In: Adaptive Processes inVisual and Oculomotor Systems. Edited by E. L. Keller and D. S. Zee. Oxford: Pergamon Press,pp. 201-208.
FISK JD, GOODALE MA (1988) The effects of unilateral brain damage on visually guided reaching:hemispheric differences in the nature of the deficit. Experimental Brain Research, 72, 425—435.
FLOWERS K (1978) Some frequency response characteristics of parkinsonism on pursuit tracking. Brain,101, 19-34.

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE 1163
FRIES W (1984) Cortical projections to the superior colliculus in the macaque monkey: a retrograde studyusing horseradish peroxidase. Journal of Comparative Neurology, 230, 55-76.
FRIES W (1985) Inputs from motor and premotor cortex to the superior colliculus of the macaque monkey.Behavioural Brain Research, 18, 95-105.
GOLDBERG ME, SEGRAVES MA (1989) The visual and frontal cortices. In: Reviews of Oculomotor Research,Volume 3, The Neurobiology ofSaccadic Eye Movements. Edited by R. H. Wurtz and M. E. Goldberg.Amsterdam: Elsevier, pp. 283-313.
HAALAND KY, HARRINGTON DL, YEO R (1987) The effects of task complexity on motor performancein left and right CVA patients. Neuropsychologia, 25, 783—794.
HARRINGTON DL, HAALAND KY (1991) Hemispheric specialization for motor sequencing: abnormalitiesin levels of programming. Neuropsychologia, 29, 147—163.
HIKOSAKA O, WURTZ RH (1983a) Visual and oculomotor functions of monkey substantia nigra parsreticulata. I. Relation of visual and auditory responses to saccades. Journal of Neurophysiology, 49,1230-1253.
HIKOSAKA O, WURTZ RH (19836) Visual and oculomotor functions of monkey substantia nigra parsreticulata. n. Visual responses related to fixation of gaze. Journal of Neurophysiology, 49, 1254-1267.
HIKOSAKA O, WURTZ RH (1983c) Visual and oculomotor functions of monkey substantia nigra parsreticulata. ID. Memory-contingent visual and saccade responses. Journal of Neurophysiology, 49,1268-1284.
HIKOSAKA O, WURTZ RH (1983d) Visual and oculomotor functions of monkey substantia nigra parsreticulata. IV. Relation of substantia nigra to superior colliculus. Journal of Neurophysiology, 49,1285-1301.
HIKOSAKA O, WURTZ RH (1985a) Modification of saccadic eye movements by GABA-related substances.I. Effect of muscimol and bicuculline in monkey superior colliculus. Journal of Neurophysiology,53, 266-291.
HIKOSAKA O, WURTZ RH (19856) Modification of saccadic eye movements by GABA-related substances.II. Effect of muscimol in monkey substantia nigra pars reticulata. Journal of Neurophysiology, 53,292-308.
HIKOSAKA O, WURTZ RH (1986) Saccadic eye movements following injection of lidocaine into the superiorcolliculus. Experimental Brain Research, 61, 531—539.
HIKOSAKA O, WURTZ RH (1989) The basal ganglia. In: Reviews of Oculomotor Research, Volume 3.The Neurobiology of Saccadic Eye Movements. Edited by R. H. Wurtz and M. E. Goldberg.Amsterdam: Elsevier, pp. 257-281.
HIKOSAKA O, SAKAMOTO M, USUI S (1989a) Functional properties of monkey caudate neurons I. Activitiesrelated to saccadic eye movements. Journal of Neurophysiology, 61, 780—798.
HIKOSAKA O, SAKAMOTO M, USUI S (19896) Functional properties of monkey caudate neurons n . Visualand auditory responses. Journal of Neurophysiology, 61, 799-813.
HIKOSAKA O, SAKAMOTO M, USUI S (1989C) Functional properties of monkey caudate neurons ID. Activitiesrelated to expectation of target and reward. Journal of Neurophysiology, 61, 814-832.
Ho VW, PORRINO LJ, CRANE AM, BURNS RS, KOPIN IJ, SOKOLOFF L (1988) Metabolic mapping of theoculomotor system in MPTP-induced parkinsonian monkeys. Annals of Neurology, 23, 86-89.
HUERTA MF, KRUBITZER LA, KAAS JH (1986) Frontal eye field as defined by intracortical microstimulationin squirrel monkeys, owl monkeys, and macaque monkeys: I. Subcortical connections. Journal ofComparative Neurology, 253, 415—439.
JASON GW (1983a) Hemispheric asymmetries in motor function: I. Left-hemisphere specialization formemory but not performance. Neuropsychologia, 21, 35—45.
JASON GW (19836) Hemispheric asymmetries in motor function: n. Ordering does not contribute to left-hemisphere specialization. Neuropsychologia, 21, 47—58.
JOSEPH JP, BARONE P (1987) Prefrontal unit activity during a delayed oculomotor task in the monkey.Experimental Brain Research, 67, 460—468.
KENNARD C, LUECK CJ (1989) Oculomotor abnormalities in diseases of the basal ganglia. RevueNeurologique, 145, 587-595.
KIMURA D, ARCHIBALD Y (1974) Motor functions of the left hemisphere. Brain, 97, 337—350.KOMATSU H, SUZUKI H (1985) Projections from the functional subdivisions of the frontal eye field to
the superior colliculus in the monkey. Brain Research, Amsterdam, 327, 324—327.

1164 J. VENTRE AND OTHERS
LASKER AG, ZEE DS, HAIN TC, FOLSTEIN SE, SINGER HS (1987) Saccades in Huntington's disease: initiationdefects and distractibility. Neurology, Cleveland, 37, 364-370.
LASKER AG, ZEE DS, HAIN TC, FOLSTEIN SE, SINGER HS (1988) Saccades in Huntington's disease: slowingand dysmetria. Neurology, Cleveland, 38, 427-431.
LEE C, ROHRER WH, SPARKS DL (1988) Population coding of saccadic eye movements by neurons inthe superior colliculus. Nature, London, 332, 357—360.
LEENDERS KL, SALMON EP, TYRRELL P, PERANI D, BROOKS DJ, SAGER H et al. (1990) The nigrostriatal
dopaminergic system assessed in vivo by positron emission tomography in healthy volunteer subjectsand patients with Parkinson's disease. Archives of Neurology, Chicago, 47, 1290-1298.
LEIGH RJ, ZEE DS (1991) The Neurology of Eye Movements. Second edition. Philadelphia: F. A. Davis.LEVIN BE, LLABRE MM, REISMAN S, WEINER WJ, SANCHEZ-RAMOS J, SINGER Cet al. (1991) Visuospatial
impairment in Parkinson's disease. Neurology, Cleveland, 41, 365—369.LIEBERMAN AN (1974) Parkinson's disease: a clinical review. American Journal of the Medical Sciences,
267, 66-80 .LUECK CJ, TANYERI S, CRAWFORD TJ, HENDERSON L, KENNARD C (1990) Antisaccades and remembered
saccades in Parkinson's disease. Journal of Neurology, Neurosurgery, and Psychiatry, 53, 284—288.LYNCH JC, GRAYBIEL AM, LOBECK LJ (1985) The differential projection of two cytoarchitectonk subregions
of the inferior parietal lobule in macaque upon the deep layers of the superior colliculus. Journalof Comparative Neurology, 235, 241—254.
MACAVOY MG, BRUCE CJ (1989) Oculomotor deficits associated with lesions of the frontal eye field areain macaque monkeys. Society for Neuroscience Abstracts, 15, 1203.
MITCHELL IJ, CLARKE CE, BOYCE S, ROBERTSON RG, PEGGS D, SAMBROOK MA et al. (1989) Neural
mechanisms underlying parkinsonian symptoms based upon regional uptake of 2-deoxyglucose inmonkeys exposed to l-methyl-4-phenyl-l,2,3,6-tetrahydropyridine. Neuroscience, 32, 213—226.
MIYASHITA N, MATSUMURA M, USUI S, KATO M, KORJ A, GARDINER TW et al. (1990) Deficits in task-related eye movements induced by unilateral infusion of MPTP in the monkey caudate nucleus. Societyfor Neuroscience Abstracts, 16, 235.
NOMURA Y, SEGAWA M, SODA M, HIKOSAKA O (1986) Voluntary saccadic eye movements in basal gangliadisorders. In: Proceedings of the Sixth Meeting of the International Society, Hakone, Japan. Amsterdam:Aeolus Press, pp. 139-145.
OYANAGI K, TAKEDA S, TAKAHASHI H, OHAMA E, IKUTA F (1989) A quantitative investigation of thesubstantia nigra in Huntington's disease. Annals of Neurology, 26, 13 — 19.
PALOMBO E, PORRJNO LJ, BANKIEWICZ KS, CRANE AM, SOKOLOFF L, KOPIN LI (1990) Local cerebral
glucose utilization in monkeys with hemiparkinsonism induced by intracarotid infusion of the neurotoxinMPTP. Journal of Neuroscience, 10, 860-869.
PETRAS JM (1971) Connections of the parietal lobe. Journal of Psychiatric Research, 8, 189-201.PYYKK6 I, DAHLEN Al, SCHALEN L, HINDFELT B (1984) Eye movements in patients with speech dyspraxia.
Acta Otolaryngologica, 98, 481-489.RASCOL O, CLANET M, MONTASTRUC JL, SIMONETTA M, SOUUER-ESTEVE MJ, DOYON B et al. (1989)
Abnormal ocular movements in Parkinson's disease: evidence for involvement of dopaminergic systems.Brain, 112, 1193-1214.
RON S, SCHMID R, ORPAZ D (1989) Applying a model of saccadic prediction to patients' saccadic eyemovements. Brain, Behavior and Evolution, 33, 179—182.
SEGRAVES MA, GOLDBERG ME (1987) Functional properties of corticotectal neurons in the monkey's frontaleye field. Journal of Neurophysiology, 58, 1387 — 1419.
SELEMON LD, GOLDMAN-RAKIC PS (1985) Longitudinal topography and interdigitation of corticostriatalprojections in the rhesus monkey. Journal of Neuroscience, 5, 776—794.
SELEMON LD, GOLDMAN-RAKIC PS (1988) Common cortical and subcortical targets of the dorsolateralprefrontal and posterior parietal cortices in the rhesus monkey: evidence for a distributed neural networksubserving spatially guided behavior. Journal of Neuroscience, 8, 4049—4068.
SHARPE JA (1986) Adaptation to frontal lobe lesions. In: Adaptive Processes in Visual and OculomotorSystems. Edited by E. L. Keller and D. S. Zee. Oxford: Pergamon Press, pp. 239-246.
STANTON GB, GOLDBERG ME, BRUCE CJ (1988) Frontal eye field efferents in the macaque monkey: I.Subcortical pathways and topography of striatal and thalamic terminal fields. Journal of ComparativeNeurology, 271,473-492.

PREDICTIVE SACCADES IN HEMI-PARKINSON'S DISEASE 1165
STARKSTEIN S, LEIGUARDA R, GERSHANIK O, BERTHIER M (1987) Neuropsychological disturbances inhemiparkinson's disease. Neurology, Cleveland, 37, 1762—1764.
TIAN JR., ZEE DS, LASKER AG, FOLSTEIN SE (1991) Saccades in Huntington's disease: predictive trackingand interaction between release of fixation and initiation of saccades. Neurology, Cleveland, 41,875-881.
UPDYKE BV (1986) Cortical and thalamic extrastriate visual afferents to cat striatum: putative visuomotorcircuits. Society for Neuroscience Abstracts, 12, 1540.
Usui S, KATO M, KORJ A, MATSUMURA M, MIYASHITA N, HIKOSAKA O (1990) Deficits in spontaneouseye movements induced by unilateral infusion of MPTP in the monkey caudate nucleus. Society forNeuroscience Abstracts, 16, 235.
WOLFSON LI, LEENDERS KL, BROWN LL, JONES T (1985) Alterations of regional cerebral blood flowand oxygen metabolism in Parkinson's disease. Neurology, Cleveland, 35, 1399—1405.
(Received November 7, 1991. Revised February 26, 1992. Accepted March 23, 1992)