academic medicine, multi-specialty medicine and office - mckesson
TRANSCRIPT
1
CPT® Code Changes for 2014
Academic Medicine, Multi-Specialty Medicine
and Office-Based Practices
Presented by: Lisa Schroeder, CHC, CCS-P, CPC Compliance Program Director – Enterprise & Strategic Services
2
This commentary is a summary prepared by McKesson’s Business Performance Services division which highlights certain changes, not all changes, in 2014 CPT® codes relating to all specialties excluding Pathology/Laboratory, Radiology, Emergency Medicine and Anesthesia. This commentary does not supplant the American Medical Association’s (AMA) current listing of CPT® codes, its documentation in the annual CPT® Changes publications, and other related publications from the AMA, which are the authoritative source for information about CPT® codes. Please refer to your 2014 CPT® Code Book, annual CPT® Changes publication, HCPCS Book and Payer Bulletins for additional information, including additions, deletions, changes and interpretations that may not be reflected in this document. CPT® is a registered trademark of the AMA. The AMA is the owner of all copyright, trademark and other rights to CPT® and its updates. CPT® codes, descriptions and other data are copyright 1966, 1970, 1973, 1977, 1981, 1983-2014 American Medical Association. All rights reserved. Overview To provide you with details on the 2014 CPT® changes McKesson (BPS) has prepared this summary of new, deleted and revised codes for all specialties excluding Pathology/Laboratory, Radiology, Emergency Medicine and Anesthesia issued by the AMA. Any updated HCPCS codes by CMS not currently published will come at a later date when CMS has published those, if any, for 2014. 2014 CHANGES TO EVALUATION AND MANAGEMENT (E/M) SERVICES In the Evaluation and Management section, four new codes have been added for reporting interprofessional telephone/Internet consultations. In addition, a new subsection and guidelines have also been added. Two new codes have been added which were converted from Category III codes. There have also been revisions to the Complex Chronic Care Coordination Services guidelines and Transitional Care Management Services guidelines. Interprofessional Telephone/Internet Consultations The four new codes below are for reporting interprofessional telephone/Internet consultation, which is defined in the guidelines as an assessment and management service in which the patient’s treating physician requests the opinion and/or treatment advice of a physician with specific specialty expertise to assist in the diagnosis and/or management of the patient’s problem without the need for the patient’s face-to-face contact with the consulting physician. It should be noted that CMS has not assigned an RVU value for these services and they will not be reimbursable for 2014.
New
Codes
Description
99446 Interprofessional telephone/Internet assessment and management service provided by a consultative physician including a verbal and written report to the patient’s treating/requesting physician or other qualified health care professional; 5-10 minutes of medical consultative discussion and review
99447 11-20 minutes of medical consultative discussion and review 99448 21-30 minutes of medical consultative discussion and review 99449 31 minutes or more of medical consultative discussion and review
Subsequent Hospital Care – Hospital Discharge Services To conform to the CPT® Nomenclature Reporting Neutrality initiative, the parenthetical note following code 99239 was revised to adhere to the policy of neutrality in identifying who may perform a procedure or a service. In addition, the parenthetical note was further clarified to address concurrent care services.
Revised Code
Parenthetical note only
Description
99239 Hospital discharge day management; more than 30 minutes

3
Pediatric Critical Care Patient Transport The Pediatric Critical Care Patient Transport guidelines have been revised to clarify the types of services performed during a pediatric patient transport. Services not listed in the new guidelines should be reported separately.
Revised Codes
Guidelines Only
Description
99466 Critical care face-to-face services, during an interfacility transport of critically ill or critically injured pediatric patient, 24 months of age or younger; first 30-74 minutes of hands-on care during transport
+99467 each additional 30 minutes (List separately in addition to code for primary service) Inpatient Neonatal and Pediatric Critical Care Codes 99481 and 99482 have been added and now replace the previous Category III codes 0260T and 0261T. The new codes describe total body and selective head hypothermia procedures provided to neonates shortly after birth, who present with moderate to severe utero hypoxia and ischemia (e.g., hypoxic-ischemic encephalopathy). Critical care codes do not include hypothermia. Therefore, codes 99482 and 99482 should be reported in addition to the critical care codes when the service is provided.
New Codes
Description
+99481 Total body systemic hypothermia in a critically ill neonate per day (List separately in addition to code for primary procedure)
+99482 Selective head hypothermia in a critically ill neonate per day (List separately in addition to code for primary procedure)
Complex Chronic Care Coordination Services The Complex Chronic Care Coordination Services guidelines were editorially revised to bring clarity to the appropriate use of these services by clearly defining patient population, practice capabilities, the care plan, and reporting requirements. It is important to note that CMS is still considering the services for these new CPT® codes as bundled services. CMS will continue to explore payment approaches and is developing proposals to promote primary care within a fee-for-service payment structure. Revised Codes
Guidelines Only
Description
99487 Complex chronic care coordination services; first hour of clinical staff time directed by a physician or other qualified health care professional with no face-to-face visit, per calendar month
99488 first hour of clinical staff time directed by a physician or other qualified health care professional with one face-to-face visit, per calendar month
+99489 each additional 30 minutes of clinical staff time directed by a physician or other qualified health care professional, per calendar month (List separately in addition to code for primary procedure)

4
Transitional Care Management Services The use of the transitional care management (TCM) codes has been expanded. The TCM services are now applicable to new patients. Other revisions to the TCM guidelines provide further clarification of the use of these services. Revised Code
Guidelines Only
Description
99495 Transitional Care Management Services with the following required elements: • Communication (direct contact, telephone, electronic) with the patient and/or caregiver
within 2business days of discharge • Medical decision making of at least moderate complexity during the service period • Face-to-face visit, within 14 calendar days of discharge
Quick Reference - E&M Changes
CPT® CODE
ADDED
DELETED
REVISED
99466 X 99447 X 99448 X 99499 X 99481 X 99482 X
2014 Changes to Surgery There have been several changes made to the Surgery section of the 2014 CPT® book which include the addition of 72 new codes, the revision of 79 codes, and the deletion of 37 codes. In the Integumentary section new codes have been added for breast biopsy with imaging guidance, and breast localization device placement with imaging guidance. There have been revisions made to the Musculoskeletal section which include editorial changes to several of the radical resection codes. In the Cardiovascular and the Digestive sections, there have been a number of changes. New procedure codes have been added which include radiological supervision and interpretation. The addition of these new codes has resulted in the deletion of codes in the Surgery and Radiology sections. In the Digestive section, the entire Esophagus/Endoscopy section has changed. The section is now divided into three subsections: Esophagoscopy, Esophagogastroduodenoscopy (EGD), and Endoscopic Retrograde Cholangiopancreatography (ERCP). There are also guideline revisions and new parentheticals in this section. In the Nervous System section there are eight new chemodenervation codes to allow for more specificity for these procedures. There are also changes in the Urinary, Female Genital, Eye, and Auditory sections.

5
Integumentary System Code 10030 has been added to report the bundled service of image-guided fluid collection drainage by catheter. In addition, three parenthetical notes were added to clarify the reporting of the service. Moderate sedation is included in this new code and is not separately reportable.
New Code
Description
10030 Image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst),soft tissue (eg, extremity, abdominal wall, neck), percutaneous
In the integumentary section, the breast codes 19102, 19103, 19290, 19291, and 19295 and the imaging guidance codes 77031 and 77032 have been deleted from the 2014 CPT® book. The services previously reported with codes 19102, 19103, 19290, 19291, and 19295 and components of 77031 and 77032 are now combined and reported with new bundled breast biopsy codes 19081-19086 and new bundled breast localization device codes 19281-19288. To accommodate these changes, six new CPT® codes 19281-19288 have been added to report breast biopsy with imaging guidance and eight new bundled codes 19281-19288 have been added to report placement of breast localization device with imaging guidance. In addition, new and revised introductory guidelines have been added to explain the intent and appropriate use of these new codes.
New Codes
Description
19081 Placement of breast localization device(s) (eg, clip, metallic pellet, wire/needle, radioactive seeds), percutaneous; first lesion, including mammographic guidance
+19082 each additional lesion, including stereotactic guidance (List separately in addition to code for primary procedure)
19083 Biopsy, breast, with placement of breast localization device(s) (eg, clip, metallic pellet), when performed, and imaging of the biopsy specimen, when performed, percutaneous; first lesion, including ultrasound guidance
+19084 each additional lesion, including ultrasound guidance (List separately in addition to code for primary procedure)
19085 Biopsy, breast, with placement of breast localization device(s) (eg, clip, metallic pellet), when performed, and imaging of the biopsy specimen, when performed, percutaneous; first lesion, including magnetic resonance guidance
+19086 each additional lesion, including magnetic resonance guidance (List separately in addition to code for primary procedure)
New Codes
Description
19281 Placement of breast localization device(s) (eg, clip, metallic pellet, wire/needle, radioactive seeds), percutaneous; first lesion, including mammographic guidance
+19282 each additional lesion, including mammographic guidance (List separately in addition to code for primary procedure)
19283 Placement of breast localization device(s) (eg, clip, metallic pellet, wire/needle, radioactive seeds),

6
percutaneous; first lesion, including stereotactic guidance +19284 each additional lesion, including stereotactic guidance (List separately in addition to code for
primary procedure) 19285 Placement of breast localization device(s) (eg, clip, metallic pellet, wire/needle, radioactive seeds),
percutaneous; first lesion, including ultrasound guidance +19286 each additional lesion, including ultrasound guidance (List separately in addition to code for
primary procedure) 19287 Placement of breast localization device(s) (eg clip, metallic pellet, wire/needle, radioactive seeds),
percutaneous; first lesion, including magnetic resonance guidance +19288 each additional lesion, including magnetic resonance guidance (List separately in addition to
code for primary procedure)
Musculoskeletal System Head In an effort to provide greater clarity to a number of codes within the musculoskeletal section of the 2014 CPT® book, the “eg” within the parenthetical for codes 21015 and 21016 has been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
21015 Radical resection of tumor (eg, sarcoma), soft tissue of face or scalp; less than 2 cm 21016 2 cm or greater
Neck (Soft Tissues) and Thorax In an effort to provide greater clarity to codes 21557 and 21558, the “eg” within the parenthetical for codes 21557 and 21558 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
21557 Radical resection of tumor (eg, sarcoma), soft tissue of neck or anterior thorax; less than 5 cm 21558 5 cm or greater
Back and Flank In an effort to provide greater clarity to codes 21935 and 21936, the “eg” within the parenthetical for codes 21935 and 21936 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
21935 Radical resection of tumor (eg, sarcoma), soft tissue of back or flank; less than 5 cm 21936 5 cm or greater
Abdomen In an effort to provide greater clarity to codes 22904 and 22905, the “eg” within the parenthetical for codes 22904 and 22905 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.”

7
Revised Codes Parenthetical
note only
Description
22904 Radical resection of tumor (eg, sarcoma), soft tissue of abdominal wall; less than 5 cm 22905 5 cm or greater
Shoulder In an effort to provide greater clarity to codes 23077 and 23078, the “eg” within the parenthetical for codes 23077 and 23077 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
23077 Radical resection of tumor (eg, sarcoma), soft tissue of shoulder area; less than 5 cm 23078 5 cm or greater
For 2014, codes 23331 and 23332 have been deleted, and three new codes have been added 23333, 23334, and 23335. The new codes now distinguish between the removal of foreign body and the removal of prosthesis of the shoulder. Code 23333 has been added and specifies the removal of foreign body of the shoulder for deep, subfascial or intramuscular tissue. And codes 23334 and 23335 have been added to specify the removal of prosthesis, including debridement and synovectomy when performed of the humeral and/or glenoid component, for total shoulder.
New Codes
Description
23333 Removal of foreign body, shoulder; subcutaneous deep (subfascial or intramuscular) 23334 Removal of prosthesis, includes debridement and synovectomy when performed; humeral or
glenoid component 23335 humeral and glenoid components (eg, total shoulder)
Humerus (Upper Arm) and Elbow In an effort to provide greater clarity to codes 24077 and 24079, the “eg” within the parenthetical for codes 24077 and 24079 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.”
Revised Codes
Parenthetical note only
Description
24077 Radical resection of tumor (eg, sarcoma), soft tissue of upper arm or elbow area; less than 5 cm 24079 5 cm or greater
For 2014, codes 24160 and 24164 have been revised to now specify the removal of prosthesis, including debridement and synovectomy when performed, for humeral and ulnar components and radial head. In addition, a number of instructional parenthetical notes have been added clarifying when to report the removal of foreign body codes versus the hardware removal codes.

8
Revised Codes
Description
24160 Removal of prosthesis, includes debridement and synovectomy when performed; humeral and ulnar components
24164 radial head
Forearm and Wrist In an effort to provide greater clarity to codes 25077 and 25078, the “eg” within the parenthetical for codes 25077 and 25078 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
25077 Radical resection of tumor (eg, sarcoma), soft tissue of forearm and/or wrist area; less than 3 cm 25078 3 cm or greater
Hand and Fingers In an effort to provide greater clarity to codes 26117 and 26118, the “eg” within the parenthetical for codes 26117 and 26118 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
26117 Radical resection of tumor (eg, sarcoma), soft tissue of hand or finger; less than 3 cm 26118 3 cm or greater
Pelvis and Hip Joint In an effort to provide greater clarity to codes 27049 and 27059, the “eg” within the parenthetical for codes 27049 and 27059 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
27049 Radical resection of tumor (eg, sarcoma), soft tissue of pelvis and hip area; less than 5 cm 27059 5 cm or greater
Femur (Thigh Region) and Knee Joint In an effort to provide greater clarity to codes 27329 and 27364, the “eg” within the parenthetical for codes 27329 and 27364 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
27329 Radical resection of tumor (eg, sarcoma), soft tissue of thigh or knee area; less than 5 cm 27364 5 cm or greater

9
Leg (Tibia and Fibula) and Ankle Joint In an effort to provide greater clarity to codes 27615 and 27616, the “eg” within the parenthetical for codes 27615 and 27616 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
27615 Radical resection of tumor (eg, sarcoma), soft tissue of leg or ankle area; less than 5 cm 27616 5 cm or greater
Foot and Toes In an effort to provide greater clarity to codes 28046 and 28047, the “eg” within the parenthetical for codes 28046 and 28047 have been editorially revised. The reference to “malignant neoplasm” has been replaced with “sarcoma.” Revised Codes Parenthetical
note only
Description
28046 Radical resection of tumor (eg, sarcoma), soft tissue of foot or toe; less than 3 cm 28047 3 cm or greater
Respiratory System Lungs and Pleura Parenthetical notes have been placed following code 32200 to identify the deletion of code 32201 and to direct users to report code 49405. In addition, code 32200 is now considered a stand-alone code.
Revised Code Parenthetical
note only Description
32200 Pneumonostomy, with open drainage of abscess or cyst For codes 32550 and 32557, the exclusionary parentheticals have been revised to clarify that the procedures listed should not be reported together when performed on the same side of the chest. Revised Codes Parenthetical
note only
Description
32550 Insertion of indwelling tunneled pleural catheter with cuff 32557 Pleural drainage, percutaneous, with insertion of indwelling catheter; with imaging guidance
Additional codes have been included within a parenthetical note that follows add on code 32674. The additional codes were added to identify the parent procedures with which this add-on code may be reported. This includes an extensive listing of varied procedures

10
Revised Code Parenthetical
note only
Description
+32674 with mediastinal and regional lymphadenectomy (List separately in addition to code for primary procedure)
Cardiovascular System Heart and Pericardium For 2014, codes 33222 and 33223 have been revised to describe a skin pocket relocation rather than revision. Prior to 2014, code 33222 described revision or relocation of a skin pocket for a pacemaker and code 33223 described revision of a skin pocket for a cardioverterdefibrillator. The two new revised codes now only describe relocation of the skin pocket.
Revised Codes
Description
33222 Relocation of skin pocket for pacemaker 33223 Relocation of skin pocket for cardioverter-defibrillator
The moderate sedation symbol has been added to codes 33282 and 33284 and therefore is not separately reportable for 2014.
New Code
Description
33282 Implantation of patient-activated cardiac event recorder 33284 Removal of an implantable, patient-activated cardiac event recorder
Cardiac Valves For 2014, code 33366 has been added and Code 0318T has been deleted. Code 33366 is used to report transcatheter aortic valve replacement via transapical exposure (such as left thoracotomy). In addition, numerous guideline and parenthetical note revisions and additions have been made to clarify the intended use of these codes.
New Code
Description
33366 Transcatheter aortic valve replacement (TAVR/TAVI) with prosthetic valve; percutaneous transapical exposure (eg, left thoracotomy)
Arteries and Veins For code 34800, a parenthetical note was added prior to the code instructing users to use codes 34841-34844f for fenestrated endovascular repair of the visceral aorta and to report fenestrated endovascular repair of the visceral aorta and concomitant infrarenal abdominal aorta using codes 34845-34848.

11
Revised Code Parenthetical
note only
Description
34800 Endovascular repair of infrarenal abdominal aortic aneurysm or dissection; using aorto-aortic tube prosthesis
Fenestrated Endovascular Repair of the Visceral and Infarenal Aorta For 2014, there is the addition of eight new codes 34841-34848 which delete Category III codes 0078T, 0079T, 0080T, 0081T. In addition to the new codes, a new subsection and guidelines have been added to provide instructions for the appropriate reporting of these codes Codes 34841-34848 are used to report placement of a fenestrated endovascular graft in the visceral aorta, either alone or in combination with the infrarenal aorta for aneurysm, pseudoaneurysm, dissection, penetrating ulcer, intramural hematoma, or traumatic disruption. Codes 34841-34844 describe repair using proximal endoprostheses that span from the visceral aortic component to one, two, three, or four visceral artery origins and distal extent limited to the infrarenal aorta. Codes 34845-34848 are used to report deployment of a fenestrated endoprosthesis that spans from the visceral aorta (including one, two, three, or four visceralartery origins) through the infrarenal aorta into the common iliac arteries. In addition Radiological Supervision and Interpretation procedures are not separately reportable and the new coding structure now bundles these services together.
New Codes
Description
34841 Endovascular repair of visceral aorta (eg, aneurysm, pseudoaneurysm, dissection, penetrating ulcer, intramural hematoma, or traumatic disruption) by deployment of a fenestrated visceral aortic endograft and all associated radiological supervision and interpretation, including target zone angioplasty, when performed; including one visceral artery endoprosthesis (superior mesenteric, celiac or renal artery)
34842 including two visceral artery endoprostheses (superior mesenteric, celiac and/or renal artery[s]) 34843 including three visceral artery endoprostheses (superior mesenteric, celiac and/or renal artery[s]) 34844 including four or more visceral artery endoprostheses (superior mesenteric, celiac and/or renal
artery[s]) 34845 Endovascular repair of visceral aorta and infrarenal abdominal aorta (eg, aneurysm,
pseudoaneurysm, dissection, penetrating ulcer, intramural hematoma, or traumatic disruption) with a fenestrated visceral aortic endograft and concomitant unibody or modular infrarenal aortic endograft and all associated radiological supervision and interpretation, including target zone angioplasty, when performed; including one visceral artery endoprosthesis (superior mesenteric, celiac or renal artery)
34846 including two visceral artery endoprostheses (superior mesenteric, celiac and/or renal artery[s]) 34847 including three visceral artery endoprostheses (superior mesenteric, celiac and/or renal artery[s]) 34848 including four or more visceral artery endoprostheses (superior mesenteric, celiac and/or renal
artery[s])

12
Vascular Injection Procedures The parenthetical note following code 36218 was revised to reflect the deletion of codes 37205-37208 and replacement with codes 37211, 37213, 37214, 37236-37239, and 37241-37244.
Revised Code Parenthetical
note only
Description
+36218 additional second order, third order, and beyond, thoracic or brachiocephalic branch, within a vascular family (List in addition to code for initial second or third order vessel as appropriate)
Transcatheter Procedures A new code has been added to report a retrograde treatment through an open cervical carotid artery exposure which is significantly different than a percutaneous or open approach through brachial or femoral access. Previous to the addition of the new code 37217, the procedure was previously reported using an unlisted vascular procedure code 37799.
New Code Description
37217 Transcatheter placement of an intravascular stent(s), intrathoracic common carotid artery or innominate artery by retrograde treatment, via open ipsilateral cervical carotid artery exposure, including angioplasty, when performed, and radiological supervision and interpretation
Endovascular Revascularization (Open or Percutaneous, Transcatheter) Codes 37221 and 37223 have revised parenthetical notes to clarify that codes 37220, 37221, 37222, and 37223 should be reported in conjunction with codes 34802-34805, 34825, 34826, 34845-34848, 34900, and 0254T only when codes 37220, 37221, 37222, and 37223 are performed outside the target treatment zone of the endoprosthesis. Revised Codes Parenthetical
note only
Description
37221 Revascularization, endovascular, open or percutaneous, iliac artery, each additional ipsilateral iliac vessel; with transluminal angioplasty (List separately in addition to code for primary procedure)
37223 with transluminal stent placement(s), includes angioplasty within the same vessel, when performed (List separately in addition to code for primary procedure)
liac and Lower Extremity Arterial Anatomy Territory Due to the fact that codes 37205-37208 and the radiological supervision and interpretation code (75960) have been identified as being reported together 75% of the time or more, the intravascular stent placement codes (37205-37208) and the radiological supervision and interpretation code (75960) have been deleted. To accommodate the deletion of the codes, new guidelines and new codes 37236-37239 have been created to report open or percutaneous transcatheter placement of an intravascular stent(s) including radiological supervision and interpretation directly related to the intervention(s). Codes 37236 and 37237 describe transluminal intravascular stent insertion in an artery while codes 37238 and 37239 describe transluminal intravascular stent insertion in a vein. Both sets of codes include moderate sedation which is not separately reportable.

13
New Codes
Description
37236 Transcatheter placement of an intravascular stent(s) (except lower extremity, cervical carotid, extracranial vertebral or intrathoracic carotid, intracranial, or coronary), open or percutaneous, including radiological supervision and interpretation and including all angioplasty within the same vessel, when performed; initial artery
+37237 each additional artery (List separately in addition to code for primary procedure) 37238 Transcatheter placement of an intravascular stent(s), open or percutaneous, including radiological
supervision and interpretation and including angioplasty within the same vessel, when performed; initial vein
+37239 each additional vein (List separately in addition to code for primary procedure) Vascular Embolization and Occlusion Due to the fact that code 37204 and the radiological supervision and interpretation codes 75894 and 75898 have been identified as being reported together 75% of the time or more, four new bundled codes 37241-37244 have been added and a new subsection and instructional guidelines have been added to clarify the reporting of these services. In addition, the instructional guidelines clarify that these new codes include all associated radiological supervision and interpretation services. Codes 37204 and 37210 have been deleted due to the fact that the services would be reported with codes in the new family of embolization codes. Code 37241 is used to report vascular embolization and occlusion procedures for venous conditions other than hemorrhage; code 37242 is used to report vascular embolization or occlusion for arterial conditions other than hemorrhage; code 37243 is used to report embolization for tumors, organ infarction, or ischemia; and 37244 is used to report embolization for treatment of hemorrhage or lymphatic extravasation.
New Codes
Description
37241 Vascular embolization or occlusion, inclusive of all radiological supervision and interpretation, intraprocedural roadmapping, and imaging guidance necessary to complete the intervention; venous, other than hemorrhage (eg, congenital or acquired venous malformations, venous and capillary hemangiomas, varices, varicoceles)
37242 arterial, other than hemorrhage or tumor (eg, congenital or acquired arterial malformations, arteriovenous malformations, arteriovenous fistulas, aneurysms, pseudoaneurysms)
37243 for tumors, organ ischemia, or infarction 37244 for arterial or venous hemorrhage or lymphatic extravasation
Digestive System Esophagus/Endoscopy The Esophagus/Endoscopy section of the new 2014 CPT® book includes substantial changes. New Endoscopy guidelines states that control of bleeding that occurs as a result of the endoscopic procedure is not separately reported during the same operative session. In addition, the anatomic structures that are included in an esophagoscopy are now listed in the Endoscopy guidelines.
14
The Esophagus/Endoscopy section is now divided into three subsections: Esophagoscopy, Esophagogastroduodenoscopy (EGD), and Endoscopic Retrograde Cholangiopancreatography (ERCP). All three subsections now include guidelines. Parenthetical notes have also been added throughout the new sections. The Esophagoscopy subsection includes two new flexible transnasal esophagoscopy (TNE) codes (43197 and 43198).
New Codes
Description
43917 Esophagoscopy, flexible, transnasal; diagnostic, includes collection of specimen(s) by brushing or washing when performed (separate procedure)
43198 with biopsy, single or multiple Codes 43200-43232 have been revised to describe procedures using a flexible scope, and six new codes 43191-43196 have been added to describe transoral esophagoscopy using a rigid scope. The change occurred due to the need for distinction between rigid and flexible and transnasal and transoral esophagoscopy. Different means of sedation are used for each. Moderate sedation is included with codes 43200-43232 and should not be reported separately.
Revised Codes
Description
43200 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)
43201 with directed submucosal injection(s), any substance 43202 with biopsy, single or multiple 43204 with injection sclerosis of esophageal varices 43205 with band ligation of esophageal varices 43206 with optical endomicroscopy 43215 with removal of foreign body 43216 with removal of tumor(s), polyp(s), or other lesion(s) by hot biopsy forceps or bipolar cautery 43220 with transendoscopic balloon dilation (less than 30 mm diameter) 43226 with insertion of guide wire followed by passage of dilator(s) over guide wire 43227 with control of bleeding, any method 43231 with endoscopic ultrasound examination 43232 with transendoscopic ultrasound-guided intramural or transmural fine needle aspiration/biopsy(s)
New Codes
Description
43191 Esophagoscopy, rigid, transoral; diagnostic, including collection of specimen(s) by brushing or washing when performed (separate procedure)
43192 with directed submucosal injection(s), any substance 43193 with biopsy, single or multiple 43194 with removal of foreign body 43195 with balloon dilation (less than 30 mm diameter) 43196 with insertion of guide wire followed by dilation over guide wire
15
Two new codes have added for endoscopic mucosal resection (EMR). New code 43211 describes the esophagoscopy procedure, and new code 43254 describes the EGD procedure. Both new codes include moderate sedation and should not be reported separately.
New Codes
Description
43211 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with endoscopic mucosal resection
43254 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with endoscopic mucosal resection
CPT® codes 43219, 43256, 43267, and 43268 have been deleted and replaced with new codes with descriptors that specify the inclusion of pre- and postdilation and guide wire passage when performed. The new codes that were added are 43212, 43266, and 43274. Codes 43212, 43266, and 43274 all include moderate sedation and should not be reported separately.
New Codes
Description
43212 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with placement of endoscopic stent (includes pre- and post-dilation and guide wire passage, when performed)
43266 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)with placement of endoscopic stent (includes pre- and post-dilation and guide wire passage, when performed)
43274 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)with placement of endoscopic stent into biliary or pancreatic duct, including pre- and postdilation and guide wire passage, when performed, including sphincterotomy, when performed, each stent
The dilation procedure codes have been added, revised, and deleted to better describe current practice. CPT® codes 43220 and 43249 have been revised to specify transendoscopic balloon dilation of less than 30 mm in diameter. A new esophagoscopy code 43213 has been added to report retrograde dilation of the esophagus with a balloon or dilator. Esophagoscopy code 43214 and EGD code 43233 have been added to report balloon dilation of 30 mm in diameter or larger. CPT® codes 43213, 43214, and 43233 include fluoroscopic guidance when used and therefore not separately reportable. CPT® code 43245 has been revised to describe dilation of gastric/duodenal stricture(s). All of the following CPT® codes include moderate sedation and is not separately reportable: 43213, 43214, 43220, 43233, 43245, and 43249.
Revised Codes
Description
43220 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic balloon dilation (less than 30 mm diameter)
43249 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic balloon dilation of esophagus (less than 30 mm diameter)

16
43245 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with dilation of gastric/duodenal stricture(s) (eg, balloon, bougie)
New Codes
Description
43213 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)
43214 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with dilation of esophagus with balloon (30 mm diameter or larger) (includes fluoroscopic guidance, when performed)
43233 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic balloon dilation of esophagus (less than 30 mm diameter)
A new Esophagogastroduodenoscopy code, 43253, has been added to describe ultrasound-guided transmural injection of substances or fiducial markers. This code includes endoscopic ultrasound (EUS) of the esophagus, stomach, and either the duodenum or a surgically altered stomach where the jejunum is examined distal to the anastomosis. The new code also includes moderate sedation and therefore should not be reported separately.
New Code
Description
43253 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic ultrasound-guided transmural injection of diagnostic or therapeutic substance(s) (eg, anesthetic, neurolytic agent) or fiducial marker(s) (includes endoscopic ultrasound examination of the esophagus, stomach, and either the duodenum or a surgically altered stomach where the jejunum is examined distal to the anastomosis)
CPT® code 43260 has been revised to make the descriptor language consistent with CPT® convention. CPT® code 43271 has been deleted and code 43277 has been added for ERCP with balloon dilation of biliary/pancreatic duct or of ampulla. CPT® code 43277 includes moderate sedation and therefore should not be reported separately.
Revised Code
Description
43260 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)
New Code
Description
43277 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)with trans-endoscopic balloon dilation of biliary/pancreatic duct(s) or of ampulla (sphincteroplasty), including

17
sphincterotomy, when performed, each duct CPT® codes 43226 and 43248 have been revised to describe passage of dilator(s) over a guide wire rather than dilation.
Revised Codes
Description
43226 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with insertion of guide wire followed by passage of dilator(s) over guide wire
43248 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with insertion of guide wire followed by passage of dilator(s) through esophagus over guide wire
CPT® code 43227, esophagoscopy with control of bleeding, has been revised to specify “any method” for consistency with EGD with control of bleeding code 43255.
Revised Code
Description
43227 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with control of bleeding, any method
CPT® codes 43228, 43258, and 43272 have been deleted and new codes have been added for ablation of tumors with esophagoscopy (43229), EGD (43270), and ERCP (43278). The new codes include pre- and postdilation and guide wire passage when performed. Moderate sedation is also included and therefore is not separately reportable.
New Codes
Description
43229 Esophagoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure)with ablation of tumor(s), polyp(s), or other lesion(s) (includes pre- and post-dilation and guide wire passage, when performed)
43270 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with ablation of tumor(s), polyp(s), or other lesion(s) (includes pre- and post-dilation and guide wire passage, when performed)
43278 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with ablation of tumor(s), polyp(s), or other lesion(s), including pre- and post-dilation and guide wire passage, when performed
CPT® codes 43237 and 43238 have been revised to describe EUS limited to the esophagus, stomach, or duodenum and adjacent structures and CPT® codes 43242 and 43259 have been revised to include examination of a surgically altered stomach where the jejunum is examined distal to the anastomosis.

18
Revised Codes
Description
43237 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with endoscopic ultrasound examination limited to the esophagus, stomach or duodenum, and adjacent structures
43238 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic ultrasound-guided intramural or transmural fine needle aspiration/ biopsy(s), esophagus (includes endoscopic ultrasound examination limited to the esophagus, stomach or duodenum, and adjacent structures)
43242 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transendoscopic ultrasound-guided intramural or transmural fine needle aspiration/ biopsy(s) (includes endoscopic ultrasound examination of the esophagus, stomach, and either the duodenum or a surgically altered stomach where the jejunum is examined distal to theanastomosis)
43259 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with endoscopic ultrasound examination, including the esophagus, stomach, and either the duodenum or a surgically altered stomach where the jejunum is examined distal to the anastomosis
CPT® code 43240 has been revised to specify that it includes placement of transmural drainage catheters/stents and EUS when performed.
Revised Code
Description
43240 Esophagogastroduodenoscopy, flexible, transoral; diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with transmural drainage of pseudocyst (includes placement of transmural drainage catheter[s]/stent[s], when performed, and endoscopic ultrasound, when performed)
CPT® code 43263 has been revised with the removal of the reference to pancreatic duct or common bile duct and CPT® codes 43264 and 43265 have been revised to more accurately describe the procedures.
Revised Codes
Description
43263 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with pressure measurement of sphincter of Oddi
43264 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with removal of calculi/debris from biliary/pancreatic duct(s)
43265 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with destruction of calculi, any method (eg, mechanical, electrohydraulic, lithotripsy)

19
CPT® 43269 has been deleted and replaced with two new ERCP codes. CPT® code 43275 describes removal of foreign body(s) or stent(s) from the biliary/pancreatic duct(s) and CPT® code 43276 describes removal and exchange of stent(s) of the biliary or pancreatic duct and includes pre- and postdilation and guide wire passage and sphincterotomy when performed. Moderate sedation is included in codes 43275 and 43276 and therefore should not be reported separately.
New Codes
Description
43275 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with removal of foreign body(s) or stent(s) from biliary/pancreatic duct(s)
43276 Endoscopic retrograde cholangiopancreatography (ERCP); diagnostic, including collection of specimen(s) by brushing or washing, when performed (separate procedure) with removal and exchange of stent(s), biliary or pancreatic duct, including pre- and post-dilation and guide wire passage, when performed, including sphincterotomy, when performed, each stent exchanged
Appendix In support of the establishment of CPT® codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), parenthetical notes have been added following CPT® code 44900 that identify deletion of code 44901 and also direct users to report code 49406 to identify percutaneous image-guided fluid collection drainage by catheter of peritoneal or retroperitoneal cysts, abscesses, hematomas, seromas, etc.
Revised Codes Parenthetical
note only
Description
44900 Incision and drainage of appendiceal abscess, open Rectum In support of the establishment of CPT® codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), a parenthetical note has been placed following code 45000 that directs users to report code 49407 to identify transrectal image-guided fluid collection drainage by catheter of pelvic abscesses, hematomas, seromas, etc.
Revised Code Parenthetical
note only
Description
45000 Transrectal drainage of pelvic abscess Liver In support of the establishment of CPT® codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), parenthetical notes have been placed following code 47010 that identify deletion of code 47011 and direct users to report code 49405 to identify percutaneous image-guided fluid collection drainage by catheter of hepatic cysts or abscesses.

20
Revised Code Parenthetical
note only
Description
47010 Hepatotomy, for open drainage of abscess or cyst, 1 or 2 stages Biliary Tract CPT® code 47552 has been revised to make the descriptor language consistent with CPT® convention. Specifically, the language has been changed by removing the language referencing “with or without” within the code descriptor and inserting the term “when performed” to note that collection of specimen(s) by brushing and/ or washing is inherently included as part of the procedure when these services are done with the endoscopy.
Revised Code
Description
47552 Biliary endoscopy, percutaneous via T-tube or other tract; diagnostic, with collection of specimen(s) by brushing and/or washing, when performed (separate procedure)
Pancreas In support of the establishment of codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), parenthetical notes have been placed following code 48510 that identify the deletion of code 48511 and direct users to report code 49405 to identify percutaneous image-guided fluid collection drainage by catheter of a pancreatic pseudocyst.
Revised Code Parenthetical
note only
Description
48510 External drainage, pseudocyst of pancreas, open Abdomen, Peritoneum and Omentum In support of the establishment of codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), CPT® codes 49021, 49041, and 49061 have been deleted. As a result, codes 49020, 49040, and 49060 are now considered stand-alone codes. In addition, parenthetical notes have been placed to identify the deleted codes, and three parenthetical notes have been added following codes 49020, 49040, and 49060 to specify the appropriate codes to use to report these services. Revised Codes Parenthetical
note only
Description
49020 Drainage of peritoneal abscess or localized peritonitis, exclusive of appendiceal abscess, open 49040 Drainage of subdiaphragmatic or subphrenic abscess, open 49060 Drainage of retroperitoneal abscess, open
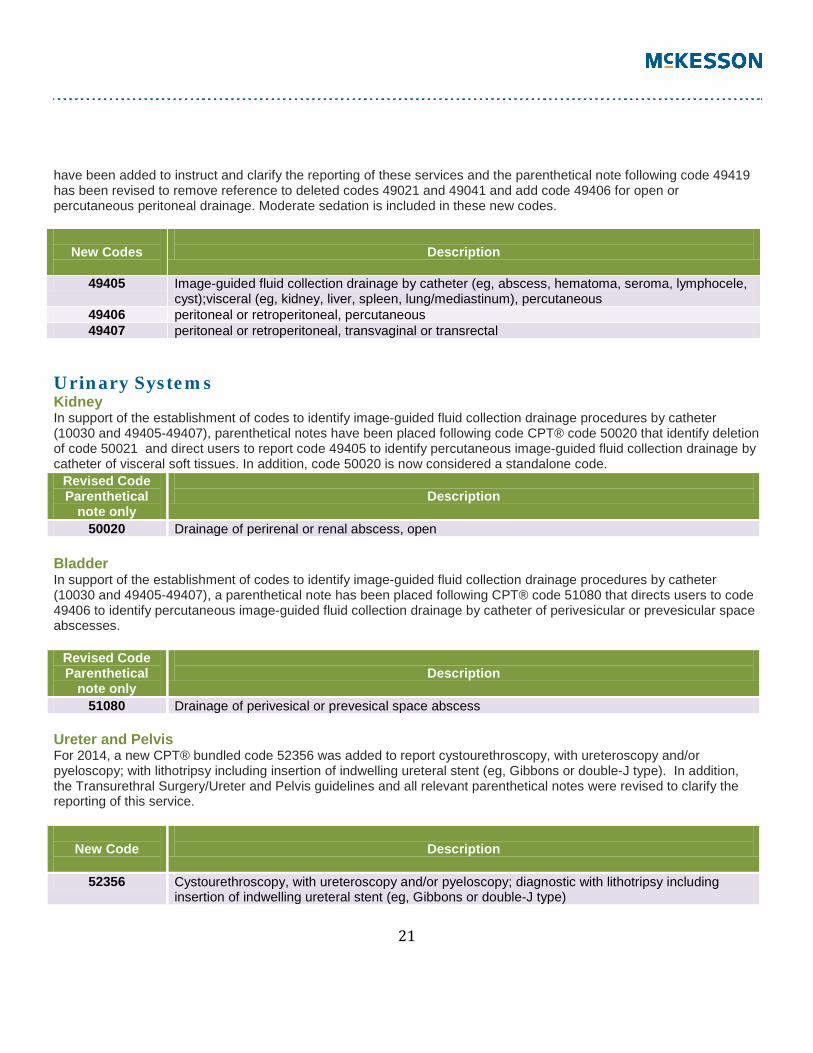
For 2014, three new bundled codes have been established in the Abdomen, Peritoneum, and Omentum/Laparoscopy subsection to identify image-guided fluid collection drainage procedures by catheter (49405-49407).The addition of these new CPT® codes is intended to clarify reporting of soft-tissue fluid drainage procedures performed at different anatomical sites and according to the type of approach used for the procedure. In addition, new cross-reference notes
21
have been added to instruct and clarify the reporting of these services and the parenthetical note following code 49419 has been revised to remove reference to deleted codes 49021 and 49041 and add code 49406 for open or percutaneous peritoneal drainage. Moderate sedation is included in these new codes.
New Codes
Description
49405 Image-guided fluid collection drainage by catheter (eg, abscess, hematoma, seroma, lymphocele, cyst);visceral (eg, kidney, liver, spleen, lung/mediastinum), percutaneous
49406 peritoneal or retroperitoneal, percutaneous 49407 peritoneal or retroperitoneal, transvaginal or transrectal
Urinary Systems Kidney In support of the establishment of codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), parenthetical notes have been placed following code CPT® code 50020 that identify deletion of code 50021 and direct users to report code 49405 to identify percutaneous image-guided fluid collection drainage by catheter of visceral soft tissues. In addition, code 50020 is now considered a standalone code.
Revised Code Parenthetical
note only
Description
50020 Drainage of perirenal or renal abscess, open Bladder In support of the establishment of codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), a parenthetical note has been placed following CPT® code 51080 that directs users to code 49406 to identify percutaneous image-guided fluid collection drainage by catheter of perivesicular or prevesicular space abscesses.
Revised Code Parenthetical
note only
Description
51080 Drainage of perivesical or prevesical space abscess Ureter and Pelvis For 2014, a new CPT® bundled code 52356 was added to report cystourethroscopy, with ureteroscopy and/or pyeloscopy; with lithotripsy including insertion of indwelling ureteral stent (eg, Gibbons or double-J type). In addition, the Transurethral Surgery/Ureter and Pelvis guidelines and all relevant parenthetical notes were revised to clarify the reporting of this service.
New Code
Description
52356 Cystourethroscopy, with ureteroscopy and/or pyeloscopy; diagnostic with lithotripsy including insertion of indwelling ureteral stent (eg, Gibbons or double-J type)

22
Female Genital System Ovary In support of the establishment of codes to identify image-guided fluid collection drainage procedures by catheter (10030 and 49405-49407), code 58823 has been deleted. In addition, a parenthetical note has been added following code 58822 to instruct the user to report 49407 for transrectal image-guided fluid collection drainage by catheter of pelvic abscess procedure.
Revised Code Parenthetical
note only
Description
58822 Drainage of ovarian abscess; vaginal approach, open abdominal approach Nervous System Extracranial Nerves, Peripheral Nerves and Autonomic Nervous System For 2014, CPT® code 64613 has been deleted and two new codes, 64616 and 64617, have been added to allow more specificity and to capture the intensity of each service. In addition, a parenthetical note was also added to direct the user to report codes 95873 and 95874 for guidance and to clarify that it is not appropriate to report more than one guidance code for 64615.
New Codes
Description
64616 Chemodenervation of muscle(s); muscle(s) innervated by facial nerve, unilateral (eg, for blepharospasm, hemifacial spasm) neck muscle(s), excluding muscles of the larynx, unilateral (eg, for cervical dystonia, spasmodictorticollis)
64617 Chemodenervation of muscle(s); muscle(s) innervated by facial nerve, unilateral (eg, for blepharospasm, hemifacial spasm) larynx, unilateral, percutaneous (eg, for spasmodic dysphonia), includes guidance by needle electromyography, when performed
CPT® code 64614 has been deleted for 2014 and six new codes, 64642-64647, have been added to allow more specificity and report chemodenervation of extremity and trunk muscles. Codes 64642-64645 are specifically intended to report chemodenervation of extremity, 1-4 muscles and 5 or more muscles. Codes 64646 and 64647 are specifically intended to report chemodenervation of trunk, 1-5 muscles and 6 or more muscles.
New Codes
Description
64642 Chemodenervation of one extremity; 1-4 muscle(s) +64643 each additional extremity, 1-4 muscle(s) (List separately in addition to code for primary
procedure) 67644 Chemodenervation of one extremity; 5 or more muscle(s)
+64645 each additional extremity, 5 or more muscle(s) (List separately in addition to code for primary procedure)
64646 Chemodenervation of trunk muscle(s); 1-5 muscle(s) 64647 6 or more muscle(s)

23
Eye and Ocular Adnexa CPT® codes 65778 and 65779 were editorially revised to omit the phrase “for wound healing” and to substitute the term “self-retaining” with “without sutures” in the code language and cross-reference note following 65780. The use of the term “without sutures” in code 65778 serves to clarify and better distinguish between the two different techniques, non-sutured or sutured or self-retaining. Revised Codes Parenthetical
note only
Description
65778 Placement of amniotic membrane on the ocular surface; without sutures 65779 single layer, sutured
A new code, 66183, has been added to report the insertion of an anterior segment drainage device for the management of glaucoma utilizing an external surgical approach and replaces Category III code 0192T.
New Code
Description
66183 Insertion of anterior segment aqueous drainage device, without extraocular reservoir, external approach
Auditory System CPT® code 69210 has been revised to clarify that this code should be used to report unilateral removal of impacted cerumen. The descriptor was further revised to clarify that 69210 should only be used when removal of impacted cerumen requires use of instrumentation. In addition, a parenthetical note has been added to direct users to report bilateral procedures with modifier 50.
Revised Code
Description
69210 Removal impacted cerumen requiring instrumentation, unilateral The parenthetical note following 69320 addressing other reconstructive procedures with grafts has been revised to reflect the deletion of code 13150.
Revised Code Parenthetical
note only
Description
69320 Reconstruction external auditory canal for congenital atresia, single stage

24
Quick Reference - Surgery Changes
CPT® CODE
ADDED
DELETED
REVISED
10030 X 13150 X 13151 X 13152 X 13153 X 15777 X 19081 X 19082 X 19083 X 19084 X 19085 X 19086 X 19102 X 19103 X 19281 X 19282 X 19283 X 19284 X 19285 X 19286 X 19287 X 19288 X 19280 X 19281 X 19295 X 21015 X 21016 X 21557 X 21558 X 21935 X 21936 X 22094 X 22905 X 23077 X 23078 X

25
23331 X 23332 X 23333 X 23334 X 23335 X 24077 X 24079 X 24160 X 24164 X 25077 X 25078 X 26117 X 26118 X 27049 X 27059 X 27329 X 27364 X 27615 X 27616 X 28046 X 28047 X 32201 X 33222 X 33223 X 33282 X 33284 X 33366 X 34841 X 34842 X 34843 X 34844 X 34845 X 34846 X 34847 X 34848 X 37204 X 37205 X 37206 X 37207 X 37208 X

26
37210 X 37217 X 37236 X 37237 X 37238 X 37239 X 37241 X 37242 X 37243 X 37244 X 42802 X 43191 X 43192 X 43193 X 43194 X 43195 X 43196 X 43197 X 43198 X 43200 X 43201 X 43202 X 43204 X 43205 X 43206 X 43211 X 43212 X 43213 X 43214 X 43215 X 43216 X 46317 X 43219 X 43220 X 43226 X 43227 X 43228 X 43229 X 43231 X 43232 X

27
43233 X 43235 X 43236 X 43237 X 43238 X 43239 X 43240 X 43241 X 43242 X 43243 X 43244 X 43245 X 43246 X 43247 X 43249 X 43250 X 43251 X 43252 X 43253 X 43254 X 43255 X 43256 X 43257 X 43258 X 43259 X 43260 X 43263 X 43264 X 43265 X 43266 X 43267 X 43268 X 43269 X 43270 X 43271 X 43272 X 43273 X 43274 X 43275 X 43276 X

28
43277 X 43278 X 43456 X 43458 X 44901 X 47011 X 47552 X 48511 X 49021 X 49041 X 49061 X 49405 X 49406 X 49407 X 50021 X 52356 X 58823 X 64613 X 64614 X 64616 X 64617 X 64642 X 64643 X 64644 X 64645 X 64646 X 64647 X 65778 X 65779 X 66183 X 69210 X

29
2014 CHANGES TO MEDICINE There have been several changes made to the Medicine section of the 2014 CPT® book which include the addition of 13 new codes, the revision of five codes and one deleted code. The Vaccine, Toxoids subsection includes the addition of four new influenza virus codes. In addition Otorhinolaryngologic Services subsection contains new guidelines and four new codes. The new codes describe the evaluation of speech production, receptive language, and expressive language abilities. For 2014, the Cardiovascular subsection has new codes and changes to the parenthetical notes in the Cardiac Catheterization section. Pulmonary, Neurology, and Physical Medicine also contain changes for 2014. Vaccines, Toxoids For 2014, a new vaccine product code 90673 has been added. The new vaccine product received FDA approval in January of 2013. In addition, influenza virus product codes 90685, 90686, 90687, and 90688 have been included in the published edition of the CPT® 2014® code set.
New Codes
Description
90673 Influenza virus vaccine, trivalent, derived from recombinant DNA (RIV3), hemagglutinin (HA) proteinonly, preservative and antibiotic free, for intramuscular use
90685 Influenza virus vaccine, quadrivalent, split virus, preservative free, when administered to children 6-35 months of age, for intramuscular use
90686 Influenza virus vaccine, quadrivalent, split virus, preservative free, when administered to individuals 3 years of age and older, for intramuscular use
90687 Influenza virus vaccine, quadrivalent, split virus, when administered to children 6-35 months of age, for intramuscular use
90688 Influenza virus vaccine, quadrivalent, split virus, when administered to individuals 3 years of age and older, for intramuscular use
Psychiatry For Medicine code 30937, an instructional parenthetical note has been added to reference a 90-minute threshold requirement for reporting prolonged services codes 99354-99357 with psychotherapy services. To coincide with the deletion, the second parenthetical note following 90838 referencing 68 minutes has been deleted.
Revised Code Parenthetical
note only
Description
90837 Psychotherapy, 60 minutes with patient and/or family member

30
Ophthalmology To support the addition of a new Category III code 0329T for 24-hour intraocular pressure monitoring, a parenthetical note has been added after code 92100 to instruct the use of code 0329T when a monitoring device is fitted to the patient for continuous monitoring during a 24-hour period.
Revised Code Parenthetical
note only
Description
92100 Serial tonometry (separate procedure) with multiple measurements of intraocular pressure over an extended time period with interpretation and report, same day (eg, diurnal curve or medical treatment of acute elevation of intraocular pressure)
For codes 92132 and 92136, there has been the addition of parenthetical notes instructing users to use code 0330T for tear film imaging. Revised Codes Parenthetical
note only
Description
92132 Scanning computerized ophthalmic diagnostic imaging, anterior segment, with interpretation and report, unilateral or bilateral
92136 Ophthalmic biometry by partial coherence interferometry with intraocular lens power calculation
For code 92285, a parenthetical note has been added to support the addition of a new Category III code 0330T for digital interferometry of the lipid layer of the tear film of the eye.
Revised Code
Parenthetical note only
Description
92285 External ocular photography with interpretation and report for documentation of medical progress (eg, close-up photography, slit lamp photography, goniophotography, stereo-photography)
Special Otorhinolaryngologic Services For 2014, four new codes have been added which clearly define and describe the wide range of services that were included in code 92506 which has been deleted. In addition, the guidelines have been revised by removing deleted code 92506 and replacing it with new codes 92521-92524.
New Codes
Description
92521 Evaluation of speech fluency (eg, stuttering, cluttering) 92522 Evaluation of speech sound production (eg, articulation, phonological process, apraxia, dysarthria) 92523 with evaluation of language comprehension and expression (eg, receptive and expressive
language) 92534 Behavioral and qualitative analysis of voice and resonance

31
Cardiovascular For 2014, two new codes have been added to the Cardiovascular section. Code 93582 is used to report percutaneous transcatheter closure of patent ductus arteriosus. The new code includes moderation sedation and therefore is not separately reportable. In addition, five parenthetical notes have been added instructing on the appropriate use of code 93582 in relation to other procedures. Code 93583 has been added to report percutaneous transcatheter septal reduction therapy (eg, alcohol septal ablation). Code 93583 also includes moderation sedation and therefore is not separately reportable. In addition, several parenthetical notes have been added to provide instruction on the appropriate use of code 93583.
New Codes
Description
93582 Percutaneous transcatheter closure of patent ductus arteriosus 93583 Percutaneous transcatheter septal reduction therapy (eg, alcohol septal ablation) including
temporary pacemaker insertion when performed Intracardiac Electrophysiological Procedures/Studies For 2014, the intracardiac electrophysiologic procedures/studies guidelines have been revised to allow reporting of code 93622 with 93653 and 93656 and 93623 with 93653- 93656 and removal of the phrase “treatment of atrial fibrillation.” Furthermore, the guidelines were revised to provide further details of the intent of the complex descriptor for codes 93653, 93654, and 93656. In addition, the descriptor for code 93653 was revised to change the phrase “when possible” to “when necessary” and add the term “bundle” within the code descriptor. The descriptor for code 93656 was revised to clarify the intent that if atrial pacing and recording, right ventricular pacing and recording, and His bundle recording cannot be performed, 93656 still may be reported. Additional revisions were made to change “when possible” to “when necessary” and to add “and” before “His bundle” to maintain consistency within the CPT® code set. Several exclusionary parenthetical notes following codes 93600-93623 and 93653, 93654 have been added, and existing parenthetical notes following codes 93609, 93612, 93619, 93620, 93621, and 93654 were revised to provide additional instructions for the appropriate reporting of these codes. Noninvasive Vascular Diagnostic Studies For 2014, Parenthetical notes have been added following codes 93922 and 93923 that exclude use of these codes in conjunction with code 0337T.
Revised Codes
Parenthetical note only
Description
93922 Limited bilateral noninvasive physiologic studies of upper or lower extremity arteries, (eg, for lower extremity: ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus bidirectional, Doppler waveform recording and analysis at 1-2 levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus volume plethysmography at 1-2 levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries
32
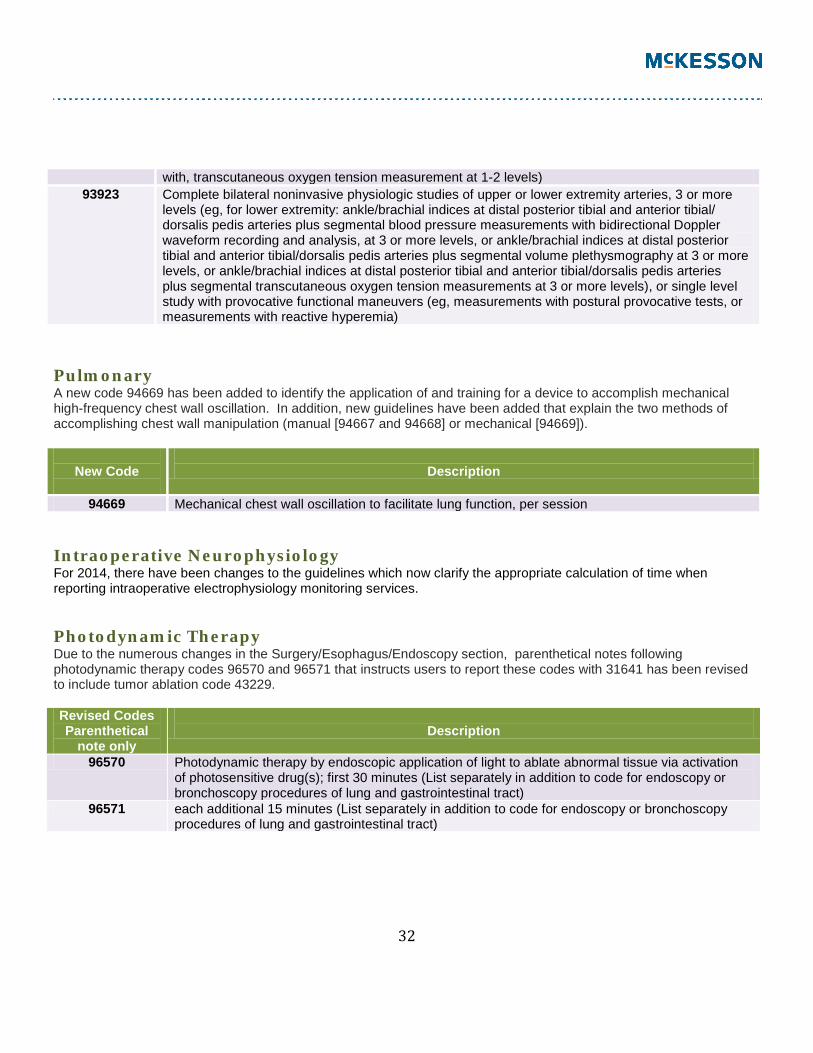
with, transcutaneous oxygen tension measurement at 1-2 levels) 93923 Complete bilateral noninvasive physiologic studies of upper or lower extremity arteries, 3 or more
levels (eg, for lower extremity: ankle/brachial indices at distal posterior tibial and anterior tibial/ dorsalis pedis arteries plus segmental blood pressure measurements with bidirectional Doppler waveform recording and analysis, at 3 or more levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus segmental volume plethysmography at 3 or more levels, or ankle/brachial indices at distal posterior tibial and anterior tibial/dorsalis pedis arteries plus segmental transcutaneous oxygen tension measurements at 3 or more levels), or single level study with provocative functional maneuvers (eg, measurements with postural provocative tests, or measurements with reactive hyperemia)
Pulmonary A new code 94669 has been added to identify the application of and training for a device to accomplish mechanical high-frequency chest wall oscillation. In addition, new guidelines have been added that explain the two methods of accomplishing chest wall manipulation (manual [94667 and 94668] or mechanical [94669]).
New Code
Description
94669 Mechanical chest wall oscillation to facilitate lung function, per session Intraoperative Neurophysiology For 2014, there have been changes to the guidelines which now clarify the appropriate calculation of time when reporting intraoperative electrophysiology monitoring services. Photodynamic Therapy Due to the numerous changes in the Surgery/Esophagus/Endoscopy section, parenthetical notes following photodynamic therapy codes 96570 and 96571 that instructs users to report these codes with 31641 has been revised to include tumor ablation code 43229. Revised Codes Parenthetical
note only
Description
96570 Photodynamic therapy by endoscopic application of light to ablate abnormal tissue via activation of photosensitive drug(s); first 30 minutes (List separately in addition to code for endoscopy or bronchoscopy procedures of lung and gastrointestinal tract)
96571 each additional 15 minutes (List separately in addition to code for endoscopy or bronchoscopy procedures of lung and gastrointestinal tract)

33
Physical Medicine and Rehabilitation For 2014, a new code has been added to report low frequency, non-contact, non-thermal ultrasound treatment of a wound with assessment and instructions for ongoing care which replaces the previous Category III code 0183T. The new code is 97610.
New Code
Description
97610 Low frequency, non-contact, non-thermal ultrasound, including topical application(s), when performed, wound assessment, and instruction(s) for ongoing care, per day
Other Services and Procedures For 2014, a revision has been made to code 99170. The revision was made to reflect current practice for the anogenital examination procedure as well as to reflect capture of digital imaging for legal recording/documentation. In addition, the parenthetical cross reference regarding sedation was also revised, replacing the term “conscious” with the term “moderate” to match CPT® code convention.
Revised Code
Description
99170 Anogenital examination, magnified, in childhood for suspected trauma, including image recording when performed
Quick Reference - Medicine Changes
CPT® CODE
ADDED
DELETED
REVISED
90673 X 90685 X 90686 X 90687 X 90688 X 91065 X 92506 X 92521 X 92522 X 92523 X 92524 X 93582 X 93583 X

34
93653 X 93654 X 93656 X 94669 X 97610 X 99170 X
2014 CHANGES TO CATEGORY II CODES For 2014, 47 new codes have been added and revisions have been made to the Perioperative Care 2 (Peri 2) measure set. Patient Management Code 0580F has been added to indicate that a multidisciplinary care plan was developed or updated for the patient.
New Code
Description
0580F Multidisciplinary care plan developed or updated (ALS)8 Codes 0581F-0584F have been added to the Perioperative Care 2 (Peri2) measure set.
New Codes
Description
0581F Patient transferred directly from anesthetizing location to critical care unit (Peri2)11 0582F Patient not transferred directly from anesthetizing location to critical care unit (Peri2)11 0583F Transfer of care checklist used (Peri2)11 0584F Transfer of care checklist not used (Peri2)11
Code 1500F has been added to report for the Diagnosis Criteria: DSP Symptoms and Signs8 measure within the Distal Symmetrical Polyneuropathy (DSP) measure set.
New Code
Description
1500F Symptoms and signs of distal symmetric polyneuropathy reviewed and documented (DSP)8 Code 1501F has been added and should be used within three different measures for the Distal Symmetrical Polyneuropathy (DSP) measure set.
New Code Description
1501F Not initial evaluation for condition (DSP)8
35
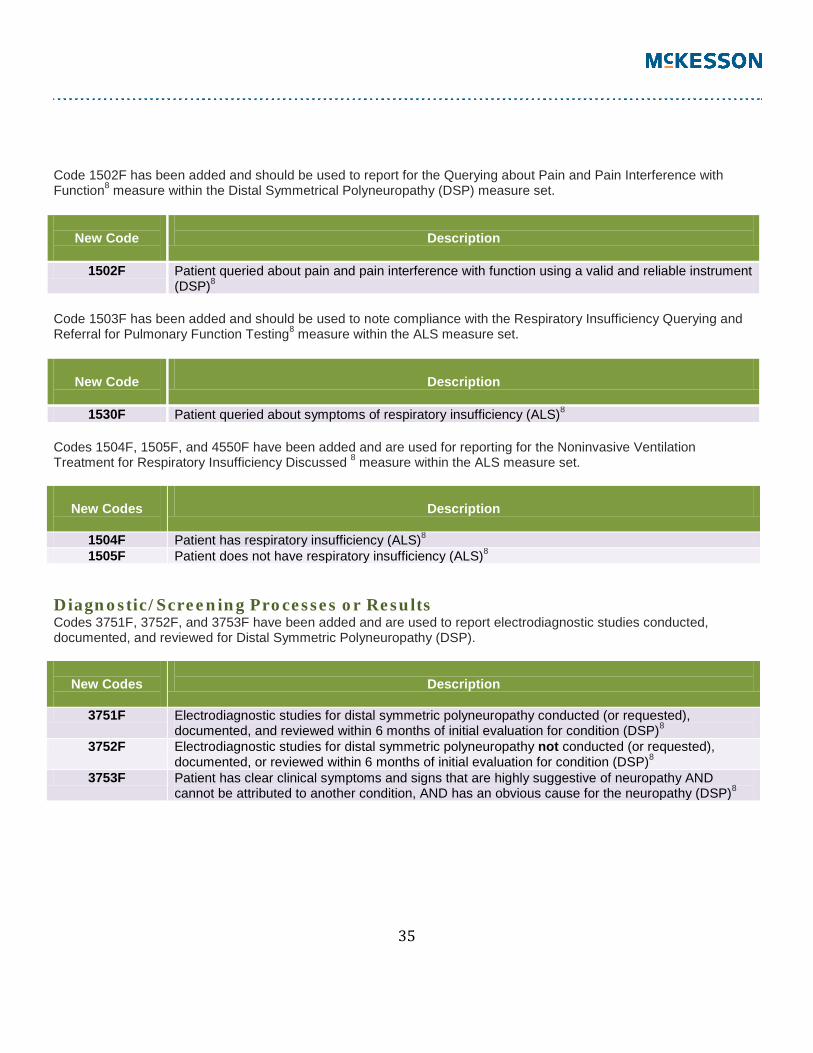
Code 1502F has been added and should be used to report for the Querying about Pain and Pain Interference with Function8 measure within the Distal Symmetrical Polyneuropathy (DSP) measure set.
New Code
Description
1502F Patient queried about pain and pain interference with function using a valid and reliable instrument (DSP)8
Code 1503F has been added and should be used to note compliance with the Respiratory Insufficiency Querying and Referral for Pulmonary Function Testing8 measure within the ALS measure set.
New Code
Description
1530F Patient queried about symptoms of respiratory insufficiency (ALS)8 Codes 1504F, 1505F, and 4550F have been added and are used for reporting for the Noninvasive Ventilation Treatment for Respiratory Insufficiency Discussed 8 measure within the ALS measure set.
New Codes
Description
1504F Patient has respiratory insufficiency (ALS)8 1505F Patient does not have respiratory insufficiency (ALS)8
Diagnostic/Screening Processes or Results Codes 3751F, 3752F, and 3753F have been added and are used to report electrodiagnostic studies conducted, documented, and reviewed for Distal Symmetric Polyneuropathy (DSP).
New Codes
Description
3751F Electrodiagnostic studies for distal symmetric polyneuropathy conducted (or requested), documented, and reviewed within 6 months of initial evaluation for condition (DSP)8
3752F Electrodiagnostic studies for distal symmetric polyneuropathy not conducted (or requested), documented, or reviewed within 6 months of initial evaluation for condition (DSP)8
3753F Patient has clear clinical symptoms and signs that are highly suggestive of neuropathy AND cannot be attributed to another condition, AND has an obvious cause for the neuropathy (DSP)8

36
Code 3754F has been added and is used to report for the Diabetes/Pre-Diabetes Screening for Patients with DSP8
measure within the Distal Symmetrical Polyneuropathy (DSP) measure set.
New Code
Description
3754F Screening tests for diabetes mellitus reviewed, requested, or ordered (DSP)8 Code 3755F has been added and is used to report for the Cognitive Impairment and Behavioral Impairment Screening8 measure for the amyotrophic lateral sclerosis (ALS) measure set.
New Code
3755F Cognitive and behavioral impairment screening performed (ALS)8 Codes 3756F and 3757F have been added and are used to report for the Symptomatic Therapy Treatment Offered8
measure within the amyotrophic lateral sclerosis (ALS) measure set.
New Codes
Description
3756F Patient has pseudobulbar affect, sialorrhea, or ALS-related symptoms (ALS)8 3757F Patient does not have pseudobulbar affect, sialorrhea, or ALS-related symptoms (ALS)8
Code 3758F has been added and is one of two codes used to identify compliance for the Respiratory Insufficiency Querying and Referral for Pulmonary Function Testing8 measure.
New Code
Description
3758F Patient referred for pulmonary function testing or peak cough expiratory flow (ALS)8 Code 3759F has been added is used to report for the Screening for Dysphagia, Weight Loss, or Impaired Nutrition8
measure within the amyotrophic lateral sclerosis (ALS) measure set.
New Code
Description
3759F Patient screened for dysphagia, weight loss, and impaired nutrition, and results documented (ALS)8
Codes 3760F and 3761F have been added and are used to report for the Nutritional Support Offered8 measure within the amyotrophic lateral sclerosis (ALS) measure set.

37
New Codes
Description
3760F Patient exhibits dysphagia, weight loss, or impaired nutrition (ALS)8 3761F Patient does not exhibit dysphagia, weight loss, or impaired nutrition (ALS)8
Codes 3762F and 3763F have been added and are used to report for the Communication Support Referral8 measure within the amyotrophic lateral sclerosis (ALS) measure set.
New Codes
Description
3762F Patient is dysarthric (ALS)8 3763F Patient is not dysarthric (ALS)8
Code 4540F is used to report compliance for the Disease Modifying Pharmacotherapy for ALS Discussed8 measure.
New Code
Description
4540F Disease modifying pharmacotherapy discussed (ALS)8 Code 4541F has been added is used to report compliance for the Symptomatic Therapy Treatment Offered8 measure within the amyotrophic lateral sclerosis (ALS) measure set.
New Code
Description
4541F Patient offered treatment for pseudobulbar affect, sialorrhea, or ALS-related symptoms (ALS)8 Code 4550F has been added and is used for reporting for the Noninvasive Ventilation Treatment for Respiratory Insufficiency Discussed8 measure within the ALS measure set.
New Code
Description
4550F Options for noninvasive respiratory support discussed with patient (ALS)8 Code 4551F has been added is used to note compliance for the Nutritional Support Offered8 measure within the ALS measure set.
New Code
Description
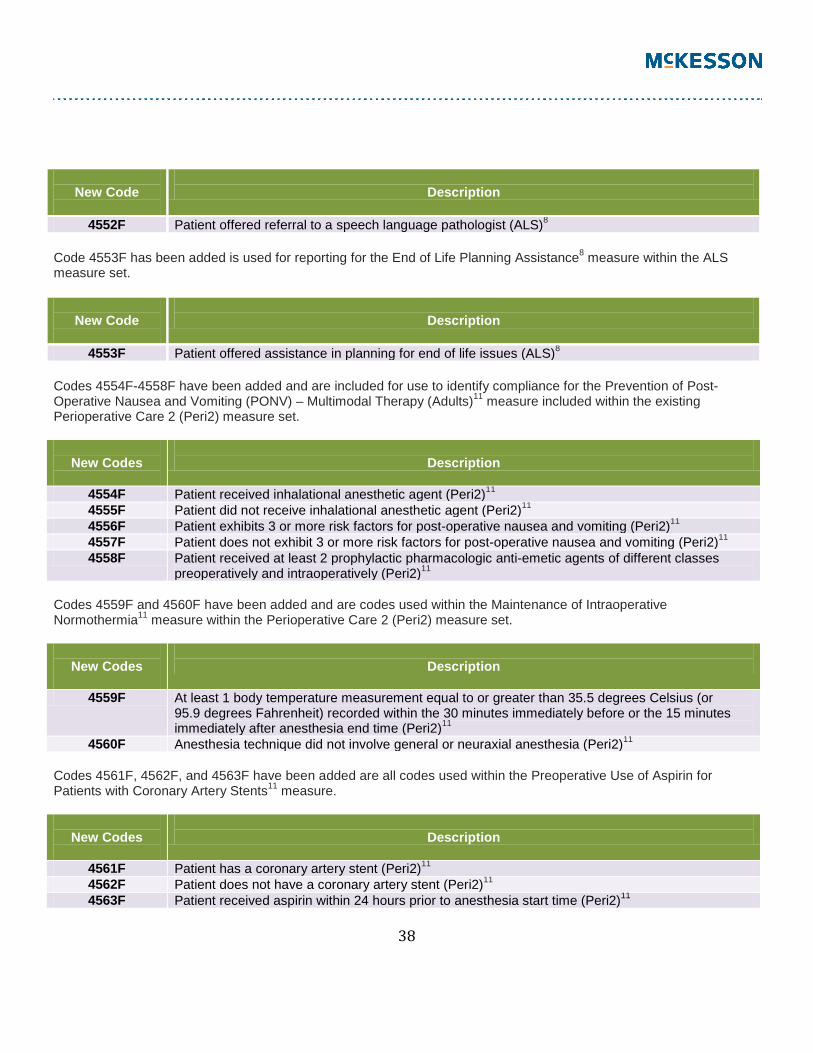
4551F Nutritional support offered (ALS)8 Code 4552F has been added is used to note compliance for the Communication Support Referral8 measure within the ALS measure set.
38
New Code
Description
4552F Patient offered referral to a speech language pathologist (ALS)8 Code 4553F has been added is used for reporting for the End of Life Planning Assistance8 measure within the ALS measure set.
New Code
Description
4553F Patient offered assistance in planning for end of life issues (ALS)8 Codes 4554F-4558F have been added and are included for use to identify compliance for the Prevention of Post-Operative Nausea and Vomiting (PONV) – Multimodal Therapy (Adults)11 measure included within the existing Perioperative Care 2 (Peri2) measure set.
New Codes
Description
4554F Patient received inhalational anesthetic agent (Peri2)11 4555F Patient did not receive inhalational anesthetic agent (Peri2)11 4556F Patient exhibits 3 or more risk factors for post-operative nausea and vomiting (Peri2)11 4557F Patient does not exhibit 3 or more risk factors for post-operative nausea and vomiting (Peri2)11 4558F Patient received at least 2 prophylactic pharmacologic anti-emetic agents of different classes
preoperatively and intraoperatively (Peri2)11 Codes 4559F and 4560F have been added and are codes used within the Maintenance of Intraoperative Normothermia11 measure within the Perioperative Care 2 (Peri2) measure set.
New Codes
Description
4559F At least 1 body temperature measurement equal to or greater than 35.5 degrees Celsius (or 95.9 degrees Fahrenheit) recorded within the 30 minutes immediately before or the 15 minutes immediately after anesthesia end time (Peri2)11
4560F Anesthesia technique did not involve general or neuraxial anesthesia (Peri2)11 Codes 4561F, 4562F, and 4563F have been added are all codes used within the Preoperative Use of Aspirin for Patients with Coronary Artery Stents11 measure.
New Codes
Description
4561F Patient has a coronary artery stent (Peri2)11 4562F Patient does not have a coronary artery stent (Peri2)11 4563F Patient received aspirin within 24 hours prior to anesthesia start time (Peri2)11

39
Nonmeasure Based Reporting For 2014, a new section has been added to the Category II code set—the Nonmeasure Based Reporting listing. These codes differ from all other Category II codes because none of these codes are or have been associated with any existing measure.
New Codes
Description
9001F Aortic aneurysm less than 5.0 cm maximum diameter on centerline formatted CT or minor diameter on axial formatted CT (NMA–No Measure Associated)
9002F Aortic aneurysm 5.0 - 5.4 cm maximum diameter on centerline formatted CT or minor diameter on axial formatted CT (NMA–No Measure Associated)
9003F Aortic aneurysm 5.5 - 5.9 cm maximum diameter on centerline formatted CT or minor diameter on axial formatted CT (NMA–No Measure Associated)
9004F Aortic aneurysm 6.0 cm or greater maximum diameter on centerline formatted CT or minor diameter on axial formatted CT (NMA–No Measure Associated)
9005F Asymptomatic carotid stenosis: No history of any transient ischemic attack or stroke in any carotid or vertebrobasilar territory (NMA–No Measure Associated)
9006F Symptomatic carotid stenosis: Ipsilateral carotid territory TIA or stroke less than 120 days prior to procedure (NMA–No Measure Associated)
9007F Other carotid stenosis: Ipsilateral TIA or stroke 120 days or greater prior to procedure or any prior contralateral carotid territory or vertebrobasilar TIA or stroke (NMA–No Measure Associated)
Quick Reference – Category II Changes
CPT® CODE
ADDED
DELETED
REVISED
0580F X 0581F X 0582F X 0583F X 0584F X 1040F X 1500F X 1501F X 1502F X 1503F X 1504F X 1505F X 3751F X

40
3752F X 3753F X 3754F X 3755F X 3756F X 3758F X 3759F X 3760F X 3761F X 3762F X 3763F X 4540F X 4541F X 4550F X 4551F X 4552F X 4553F X 4554F X 4555F X 4556F X 4557F X 4558F X 4559F X 4560F X 4561F X 4562F X 4563F X 9001F X 9002F X 9003F X 9004F X 9005F X 9006F X 9007F X

41
2014 CHANGES TO CATEGORY III CODES For 2014, there are 21 new codes and 12 deleted Category III codes. Nine of the deleted Category III codes have been converted to Category I codes. In addition, there is a new subsection, guidelines, and 10 codes for Subcutaneous Implantable Defibrillator System. Subcutaneous Implantable Defibrillator System Ten Category III codes (0319T-0328T) have been established for reporting insertion, removal, replacement, and repositioning of a subcutaneous cardioverter-defibrillator pulse generator, subcutaneous electrode (lead), electrophysiologic evaluation, programming device evaluation, and interrogation device evaluation.
New Codes
Description
0319T Insertion or replacement of subcutaneous implantable defibrillator system with subcutaneous electrode
0320T Insertion of subcutaneous defibrillator electrode 0321T Insertion of subcutaneous implantable defibrillator pulse generator only with existing
subcutaneous electrode 0322T Removal of subcutaneous implantable defibrillator pulse generator only 0323T Removal of subcutaneous implantable defibrillator pulse generator with replacement of
subcutaneous implantable defibrillator pulse generator only 0324T Removal of subcutaneous defibrillator electrode 0325T Repositioning of subcutaneous implantable defibrillator electrode and/or pulse generator 0326T Electrophysiologic evaluation of subcutaneous implantable defibrillator (includes defibrillation
threshold evaluation, induction of arrhythmia, evaluation of sensing for arrhythmia termination, and programming or reprogramming of sensing or therapeutic parameters)
0327T Interrogation device evaluation (in person) with analysis, review and report, includes connection, recording and disconnection per patient encounter, implantable subcutaneous lead defibrillator system
0328T Programming device evaluation (in person) with iterative adjustment of the implantable device to test the function of the device and select optimal permanent programmed values with analysis, implantable subcutaneous lead defibrillator system
A new Category III code (0329T) has been added for reporting monitoring of intraocular pressure for 24 hours or longer with interpretation and report.
New Code
Description
0329T Monitoring of intraocular pressure for 24 hours or longer, unilateral or bilateral, with interpretation and report

42
Category III code 0330T has been added report digital interferometry to access the quality and thickness of the lipid layer of the tear film of the eye with interpretation and report.
New Code
Description
0330T Tear film imaging, unilateral or bilateral, with interpretation and report Category III codes 0331T and 0332T have been added to report myocardial sympathetic innervation imaging.
New Codes
Description
0331T Myocardial sympathetic innervation imaging, planar qualitative and quantitative assessment; 0332T with tomographic SPECT
Category III code 0333T has been added to report a limited screening of visual acuity using an automated visual evoked potential instrument-based algorithm with a pass/fail result.
New Code
Description
0333T Visual evoked potential, screening of visual acuity, automated Category III code 0334T has been added to report sacroiliac joint stabilization for arthrodesis using a percutaneous or minimally invasive (indirect visualization) approach.
New Code
Description
0334T Sacroiliac joint stabilization for arthrodesis, percutaneous or minimally invasive (indirect visualization),includes obtaining and applying autograft or allograft (structural or morselized), when performed,includes image guidance when performed (eg, CT or fluoroscopic)
Category III code 0335T has been added to report insertion of a subtalar joint implant for joint stabilization.
New Code
Description
0335T Extra-osseous subtalar joint implant for talotarsal stabilization

43
Category III code 0336T has been added to report laparoscopic surgical ablation of uterine fibroids including intraoperative ultrasound guidance and monitoring using radiofrequency.
New Code
Description
0336T Laparoscopy, surgical, ablation of uterine fibroid(s), including intraoperative ultrasound guidance and monitoring, radiofrequency
Category III code 0337T has been added and is used to report endothelial function assessment using the peripheral vascular response to hyperemia.
New Code
Description
0337T Endothelial function assessment, using peripheral vascular response to reactive hyperemia, noninvasive (eg, brachial artery ultrasound, peripheral artery tonometry), unilateral or bilateral
Category III codes 0338T and 0339T have been added to report renal denervation from a percutaneous transcatheter approach, unilateral and bilateral.
New Codes
Description
0338T Transcatheter renal sympathetic denervation, percutaneous approach including arterial puncture, selective catheter placement(s) renal artery(ies), fluoroscopy, contrast injection(s), intraprocedural roadmapping and radiological supervision and interpretation, including pressure gradient measurements, flush aortogram and diagnostic renal angiography when performed; unilateral
0339T bilateral Quick Reference – Category III Changes
CPT® CODE
ADDED
DELETED
REVISED
0078T X 0079T X 0080T X 0081T X 0124T X 0183T X 0185T X 0186T X 0192T X

44
0260T X 0261T X 0318T X 0329T X 0330T X 0331T X 0332T X 0333T X 0334T X 0335T X 0336T X 0337T X 0338T X 0339T X 0319T X 0320T X 0321T X 0322T X 0323T X 0324T X 0325T X 0326T X 0327T X 0328T X
Footnotes ___________________________________________________________________________________________ 8American Academy of Neurology, www.aan.com/go/praactice/quality/measurements or [email protected] 11American Society of Anesthesiologists (ASA), www.asahq.org DISCLAIMER: This is an overview of the 2014 CPT®/Modifier changes affecting the academic medicine and multi-specialties. Please refer to your 2014 CPT® Book, HCPCS Book and Payer Bulletins for additional information; HCPCS additions, deletions and changes are not reflected in this document. The Business Performance Services business unit is one of several business units within McKesson Technology Solutions. We refer to ourselves as “BPS” or “Business Performance Services” for internal communications and certain external communication, such as media releases. PST Services, Inc. is the legal entity BPS uses with contracts with its clients or third-party vendors. Copyright © 2014 PST, Inc. and/or one of its subsidiaries. All rights reserved. All other product or company names mentioned may be trademarks, service marks or registered trademarks of their respective companies. This publication is not intended to constitute legal, accounting, financial, investment or other professional advice. Any business decisions should be made in consultation with your personal legal, professional and accounting advisors. Current Procedural Terminology (CPT®) copyright: 2014 American Medical Association