academy healthcare news - handinscan healthcare news ... mitsuo kaku, hiroyuki kunishima, bijie hu,...
TRANSCRIPT

HEALTHCARE NEWSAcademyInfection Control Specialist
A Half Century of Success
Every day, SARAYA helps keep millions of hands clean all over the world. Since 1952, our pioneering vision and sense of social responsibility have earned us the respect of businesses, schools, the government and households all over Japan.Sanitation continues to be a primary focus for SARAYA. Every year, millions of people fall ill needlessly due to unsafe food and lack of sanitation. We strive to make hand washing easier because it is the number one defense against the spread of illness.
With nature as our inspiration, we find new uses for natural substances to develop unique sanitation and health products. We are committed to improving health by developing technology, educating the public and protecting the environment. Environmentalism has been our mandate since the beginning, long before "eco-friendly" became a buzzword. We are ISO 9001 and ISO 14001 certified for quality control and environmental manage-ment systems.
By responding to changes in society and encouraging dialogue, we develop value-added products that go beyond the conventional. This customer-oriented approach lets us meet the ever-evolving needs of our clients. Besides offering a wide range of biodegradable, natural products, we also invest in green technologies, conservation initiatives and waste reduction programs in our opera-tions. Of course, our largest asset is our dedicated staff. Employing over 1500 people worldwide, SARAYA encourages equity and teamwork in a supportive workplace.
An Introduction of Saraya
Welcome to HYGIENE ACADEMYThe specialists in healthcare hygiene, safety and quality management
There are many excellent products for medical hygiene, but without proper education to develop a consciousness on the importance of medical hygiene, the effectiveness of these products cannot be realized and a facility's safety and compliance may suffer. HYGIENE Academy is a major contributor to hospital sanitation education and research publications, and our R&D department and education specialists have created innovative tools to teach staff and the public about proper and effective hand hygiene methods. Education is an important tool in fighting healthcare related infections, which is why we support the health of patients by backing up our products with our own research.
The HYGIENE Academy with headquarters in Japan, near Osaka, was incorporated as a subsidiary of the established global company "Saraya Co Ltd". HYGIENE Academy has over 10 years of experience nationwide and has established branches throughout Japan. The employees possess qualifications of specialist nurse / nurses for hospital hygiene and infection control. The HYGIENE Academy acts as the consulting and training arm for hygiene and specialized relevant cross-cutting issues. We see our responsibilities as our customers in an economical and medical related need in preventing infection as the view of the topic of hygiene prevention optimally. Hygiene Professional is used to prevent infection and our services will help these hazards off switch and give you legal security to authorities. We want to partner and have project-related support to our customers needs as a satisfied and repeat customer’s supplier’s win-win situation.
Saraya Co., Ltd2-2-8 Yuzato, Higashisumiyoshi-ku, Osaka 546-0013 JapanPhone: +81-6-6703-6556E-mail: [email protected]: http://worldwide.saraya.com
Academy
Healthcare News no.1 August 2011

HEALTHCARE NEWSAcademyInfection Control Specialist
SARAYA is at the forefront of research, development and education of healthcare sanitation, infection control and hand hygiene in Japan. For 60 years, SARAYA has been dedicated to preventing infection through high level disinfectants, hand hygiene solutions and unique dispenser technology. In addition, SARAYA is involved in preventing food borne illness and the protection of public and household health throughout the world. Biodiversity and the environment are central to SARAYA’s corporate culture, and actively educate consumers on global issues regarding sustainability and health. Proceeds are used to help fund many projects such as biodiversity conservation in the Borneo rainforest as well as improving hand hygiene for children in Uganda.
SARAYA operates in 5 continents with the vision of improving the sanitation, environ-ment and health around the world.
Healthcare Hygiene services include:
• Education and practice in Hygiene Management• Hand washing and disinfection• High level disinfection• Instrument reprocessing• Surface disinfection• No-touch dispensing • Personal protection equipment
To all contributors of the newsletter without your support and effort we would not be able to publish this news well. We dedicate this news to all healthcare workers that work hard in commanding patient safety throughout the world.
Creative: Jaisone & Mark James.
Photographs: Yusuke Saraya, Etsu Noguchi, Alexander Dorofeev, Ittoku Saraya, Ekaterina Povod & MCI Geneva.
To all contributors of the newsletter for ICPIC: Hillard Witt, Marlon Marmaril, Takeo Hojo, Adam Klimkowski, Ekaterina Povod, Alexander Dorofeev, Nicole van Hall, Yuko Higashino, Kazumasa Miyamoto, Christophe Catanzano, Etsu Noguchi, Hidekazu Tanaka, Yoko Yoshida, Ween Muskay & Lee seulbee for sharing their experience.
WHO CCiSC team, ICPIC Conference, RIPAQS AFRICA, MCI Geneva, Ô les mains Dancers & HUG Novae Restaurant.
Sir Liam Donaldson, Didier Pittet, Andreas Voss, Wing-Hong Seto, Stephan Harbarth, Tim Walsh, Hugo Sax, Manfred Rotter, Stephanie Dancer, John Boyce, Ziad Memish, Helen Oh, Mitsuo Kaku, Hiroyuki Kunishima, Bijie Hu, Nordiah Jalil, Nazri Aziz, Patricia Ching, & Tamas Haidegger.
Changi General Hospital, Tottori University Hospital, SARAYA Biochemical Laboratory and Budapest University of Technology and Economics.
Special Thanks & Acknowledgment
SARAYA Healthcare Hygiene Department

HEALTHCARE NEWSAcademyInfection Control Specialist
Message from the presidentOne of the most dynamic and followed topics concerning current medical practices is infection control and prevention. However, with so much research being conducted every year by professionals and students, how can ICPIC find its place among an already matured field with many congresses meeting around the world every year?
The defining feature of ICPIC lay in its international participation. Being an "International Congress" we witnessed participants, research and presentations from a diverse and fresh dicotomy of the world. Poster presentations, abstracts, and lectures from members of 84 different countries made this global congress represent the real state of the infection control and prevention field. The opportunity to hear experts from leading universities or infection control nurses from rural Africa, and from keynote to closing, the speaking roster at ICPIC contained the greatest contributors to patient safety and infection prevention in the world today.
We cannot talk about ICPIC without giving a nod to Professor Didier Pittet, ICPIC chair and creater. Professor Pittet has dedicated much of his recent career to expanding knowledge on hand hygiene, infection prevention and patient safety to every corner of the world. Through the WHO's World Alliance on Patient Safety, Professor Pittet has gained the support of many governments around the world, representing over 87% of the world's popula-tion, to address healthcare associated infections. It is likely that most participants came to ICPIC through their familarity with Professor Pittet's projects with the WHO and the WHO Guideline on Hand Hygiene.
The importance of preventing HAI's is globally recognized as an urgent issue that affects patients from every level of society, in every country. It is all too well known that infections caused in the hospital can lead to serious health complications and financial turmoil. Fortunately this urgency is being undestood on a global level, inspiring better practices and more research. With this global awakening, we can expect the International Congress on Prevention and Infection Control to continue on for many years.
Yusuke Saraya
HEALTHCARE NEWSAcademyInfection Control Specialist
Foreword"We look for medicine to be an orderly field of knowledge and procedure. But it is not. It is an imperfect science, an enterprise of constantly changing knowledge, uncertain information, fallible individuals, and at the same time lives on the line. There is science in what we do, yes, but also habit, intuition, and sometimes plain old guessing. The gap between what we know and what we aim for persists. And this gap complicates everything we do." — Atul Gawande (Complications: A Surgeon's Notes on an Imperfect Science)
We live in an imperfect world: as human beings we all make mistakes and no system is perfect. However, all of us are working towards the delivery of patient safety that we owe it to all patients and to ourselves to do all that we can to minimize errors and maximize quality.
From the beginning of their education, healthcare professionals are taught that errors are intolerable: no diagnosis, allergic reaction or past medical difficulty can be missed, every check must be tracked down, and every medication dose must be precise. In spite of this, in every healthcare system errors do occur, occasionally with severe or even fatal consequences for patients and their families. When such adverse events occur there must be a system in place that ensures that there is investigation and learning from
the error to try to prevent the recurrence of such an event. The distribution of learning throughout the system is vital to minimizing mistake and protecting future patients.
For the last three decades, benchmarking of surveillance data for health-care-associated infection (HCAI) has been practice to share information on prevention strategies and improve patient safety. Lately, reporting of HCAI indicators has been mandated in many countries due to the increasing demand for transparency in the healthcare settings. With this effort, and exercise, for a direct public reporting of incidence of HCAIs, it has contributed to a substantial organizational change in the field of patient safety around the world. An opportunity now exists to learn from the different strategies that have been adopted and we at SARAYA are proud to share in our HYGIENE newsletter with the public of what we know, learn and understand through our network.
“We're all going to make mistakes; it's just a question of choosing how we move toward them. Are we going to blame on others or pretend it never happen? Or are we going to take accountability for it, and try to learn from it and forgive ourselves and others? We all have the choice. The only option we don't have is perfection.”
We hope you enjoy this edition of HEALTHCARE news and once again, it is your feedback which makes the newsletter what it is so please e-mail with any comments, thoughts or contributions you wish to make to future editions to [email protected]
““If you were admitted to hospital tomorrow in any country… your chances of being subjected to an error in your care would be something like 1 in 10. Your chances of dying due to an error in health care would be 1 in 300,”
Sir Liam Donaldson.
Harvey YeapChairman, Global Healthcare Department

HEALTHCARE NEWSAcademyInfection Control Specialist
4 Days & 6 Highlights Of the Event
1. The opening ceremony (29 July), with Ian Smith, Councilor Mrs Margaret Chan, WHO Director-General, and Ms. Nora Berra, Secretary of State for Health to the French government.
2. Two lectures: "Shock" (29 July) of the Bacterium Escherichia Coli made in Germany and the History of the Bacteria NDM-1 Discovery in India, narrated by the authors and the publisher of the scientific article published in The Lancet
3. The Innovations Academy sponsored by SARAYA, ranging from the processing of bank notes against viruses and bacteria to a new intelligent anti-bacterial hand wipes (Thursday 30 to 5:15 p.m.): 55 applica-tions received, 14 selected projects, five projects selected to compete in an Award ( 2 July)
4. The European project MOSAR (Mastering Hospital Antimicrobial Resistance) (1'350'000 euros, 10 hospitals involved, including HUG responsible for coordination), with the presentation of initial results on the control of antibiotic resistant bacteria in surgical (2 July)
5. "Semmelweiss" Day (first Friday, at 9) celebration, 150 years after the thesis-and revealing-professor Ignaz Philipp Semmelweis published ("The Etiology, Concept and Prevention of Childbed Fever "), the progress in hand hygiene. 10 global experts present their 10 commandments of hand hygiene! 6. The Special Session of the International Network for Planning and Quality Improvement in Health Systems in Africa (1 July), with Micheline Calmy-Rey, President of the Confederation and Head of Federal Department of Foreign Affairs and Ms. Theresa A. N'dri-Yoman, Minister of Health and the fight against AIDS in Côte d'Ivoire.
GENEVA, SWITZERLAND – The first International Conference on Prevention & Infection Control was heavily participated from countries all around the world. Each year, hundreds of millions of patients worldwide become infected during hospital care leading to significant mortality and financial losses for the health systems. This incident affects more with developing countries; and it does not give any exception to developed country too.In Switzerland, some 70 000 patients are affected with HAI each year’s during their course of hospitalization. Hence the essential role of infection controls an area which is the expertise of University Hospitals of Geneva is recognized for worldwide and WHO has organized this great event, in Uni Mail last June 29th - July 2nd addressing the major concern of HAI.
The topic of HAI is regularly discussed at major conferences around the world, but this is the first time an international conference took the initiatives to look in an international dimension in addressing this issue related also to developing countries.A real solidarity movement & effort of the conference has allowed nationalities from 84 countries participated in the event, which bring together to a number total of 1300 participants from around the world. The President of the Confederation of Switzerland, Micheline Calmy-Rey also participated in this important event and showed her support to the conference in the solidarity of addressing the issue of HAI together with participants from developing countries during the Special Session of International Network for planning and improving Quality & Security in Health System in Africa.On the main agenda of the conference was to stress the importance of good hand hygiene, which is the primary measure of prevention but also to addressed the wake of recent major infections with new elements, the E. coli breakout in Germany and an NDM1 outbreak in India.
Finally, this conference has shown that infection control issues are not limited just to hospital but also in the community in the fight against HAI.
With this for the first time, SARAYA is proud to have been part of the event and showcase our Healthcare Hygiene contribution alongside with the world's leading experts of infections and antibiotic resistance in the first International Conference on the Prevention and Control of Infections.
“I was interested with the conference topic related to the hand washing compliance systems and learning about training techniques to improve hand hygiene programs....”
Hillard Witt

HEALTHCARE NEWSAcademyInfection Control Specialist
AcademicsKeynotePatient Safety: International PerspectivesSir Liam Donaldson (WHO and UK)
Professor Sir Liam Donaldson as WHO Envoy for Patient Safety. Sir Liam, who served as England's Chief Medical Officer between 1998 and 2010, will support the Organization promote patient safety as a global public health priority. Specifically, Sir Liam will mobilize political support for WHO Patient Safety with health leaders around the world and with major donors, philanthropic organizations and governments for priority activities addressing patient
safety issues at national and international levels. He will also advise the WHO Director-General on strategic issues in patient safety and propose strategic actions and collaborations at global level.
Sir Liam Donaldson, presenting on “Patient Safety International Perspectives”, a major program on scientific efforts that have grown on to global recognition. In his presentation, Sir Donaldson covers 5 simple observations about the world that put the patient at risk. Safety from infection through these perspec-tives should be recognized and comply with global standards.
• Accidents are largely systems failures • Simple errors cost lives• Safe teamwork is not just about doctors and nurses• Systems are important but so are well trained, safety-oriented staff• Other industries have a lot to teach healthcare about risk management
Infection Control: From Local to Global… Fostering Partnership and Rock’n’RollDidier Pittet (CH)
Didier Pittet, MD, MS is the Hospital Epidemiologist and Director of the Infection Control Program at the University of Geneva Hospitals and Faculty of Medicine, Geneva, Switzer-land; Professor of Medicine and Hospital Epidemiology at the Univer-sity of Geneva; and Attending
Physician in Adult and Paediatric Infectious Diseases, University of Geneva Hospitals.
He holds Honorary Professorships at Imperial College London, UK, the Faculty of Health and Social Sciences, Hong Kong Polytechnic University School of Health Science, and the First Medical School of the Fu, Shang-hai, China.
Professor Pittet spoke about his experience with the WHO, HUG, and around the world to achieve the World Health Organization First Global Patient Safety Challenge, “Clean Care is Safe Care”. This is perhaps a truly international and mind-challenging event, dedicated to the fight against HAI. He also showed the new HH video by HUG WHO to everyone.
Special Lectures: The New Gram-Negative Challenges NDM-1: A Threat to Patients (And the Author)Tim Walsh (UK)
English born Professor Tim Walsh was raised in Australia and completed his tertiary studies in the UK. Focused on the unusual mechanisms of antimicrobial resistance and how they are mobilized into the clinical sector and spread once established, Prof Walsh has published over 160 papers, in particular on the characterization of unusual b-lactamases within Gram-negative bacteria. Prof Walsh speaks about NDM-1, a new antibiotic resistant gene discovered in UK patients by a leading team of scientist for the first time. He first identified the NDM-1 gene in Klebsiella pneumoniae and Escherichia coli. bacteria taken from a Swedish patient admitted to hospital in India in 2009. The new NDM-1-producing bacteria are resistant to many antibiotics including carbapenems, a group of antibiotics generally reserved for use in emergencies and the treatment of infections caused by multi-resistant bacteria. In his presentation, it was mention that the emergence of NDM-1 positive bacteria is potentially a serious
global public health risk as there are few new anti-Gram-negative antibiotics in development and none that are effective against NDM-1.
Goals of the conference “Goals of the conference is to export the principles of infection outside the hospital and generalized to all health care facilities to ensure patient safety; & to mobilize as many (patients, professionals, authorities, etc..) For the challenge against antibiotic resistance.”
“I found the topics of patient safety and improvements in hand hygiene compliance interesting. I'm glad to have the chance at ICPIC to introduce SARAYA to people who dedicate their lives and careers to patient care and safety.”
Adam Klimkowski

HEALTHCARE NEWSAcademyInfection Control Specialist
AcademicsHuman Factors Design Hugo Sax (CH)
Hugo Sax was born in Zurich (Switzerland) in 1956. After training in anesthesia and internal medicine (Cantonal Hospital Winterthur then Chur, Switzerland), as well as training in Infectious Diseases (University Hospital Basel, Zurich and Geneva, Switzerland), he took his current position. In the University Hospital of Zurich, Hugo Sax has conducted clinical research in the field of hepatitis C and HIV, and was an outpatient consultant for adult patients with HIV and infectious diseases. Hugo Sax is a member of the Swiss Society of Internal Medicine, the Swiss Society of Infectious Disease (as a member of the Committee) and the Swiss Society of Hospital Hygiene. He co-authored over 20 publications and numerous textbook chapters. He also serves on the editorial board of Swiss-NOSO. His current research focuses on the epidemiology and prevention of nosocomial infections (especially Staphylococcus aureus resistant to methicillin), the impact and cost of infections in patients who are in critical condition and use of information technology in the prediction and prevention of nosocomial infections. His
interests also cover the major methods for studying infection and adjustment of controls between various health institutions, particularly in regard to prevalence studies multi-centric, and the impact and cost of methods to promote a wider use of isolation precautions and hand hygiene practices. In his presentation he elaborates of wide range of topics, from human ergonomics to psychology, and their application to hand hygiene and hand washing compliance in the field of Human Factor from applications method, to principles.
Testing of the World Health Organization recommended formulations for surgical hand preparation and proposals for increased efficacyManfred Rotter (AT)
Professor M. Rotter is Head of the Department of Clinical Microbiology of the Hygiene-Institute of the Medical School of the University at the General Hospital, Vienna. He published about 400 scientific publications including areas of clinical microbiology, hospital epidemiology, and disinfection. Prof. Rotter was awarded the Unilever Award 1975, the Austrian Hygiene-Award 1976, the Rudolf Schülke Award 1982, and the Düsseldorf Hygiene Award 1984. He is temporary adviser to the WHO and previously he was President of the Austrian Society of Hygiene, Microbiology and Preventive Medicine, President of the Austrian Society for Chemo-therapy, and Vice president of the Paul-Ehrlich Society for Chemotherapy. In his presentation, the main message to the audience was that 1) the WHO-recommended formulations do not meet the efficacy requirements of the European norm 12791 (surgical hand rub), but 2) could do so if the alcohol concentrations were increased by approximately 5%, which
can easily be done by exchanging the prescribed % volume concentrations (v/v) to % weight concentrations (w/w) AND by decreasing the glycerol concentration from 1,45% to 0,725%. Which regards to this matter it was discussed during the congress by the expert group with WHO-representatives. Probably, the formulations will have to be changed according to his proposals.
Novel strategies for cleansing and monitoring: the effectiveness of environmental cleaningStephanie Dancer (UK)
Stephanie works in NHS Lanarkshire (Consultant in Microbiology and Infection Control) and was the editor-in-chief of the Journal of Hospital Infection for the past five years. She recently presented at the International Hospital Infection Society and Lancet Infectious Diseases conferences on issues related to environmental cleanliness and HAIs. At present she balances clinical and editorial duties with various research projects on MRSA.
In her presentation on environmental cleaning in the UK, Dr. Dancer discussed the importance of hospital cleaning in relation to the increasing numbers of patients acquiring meticillin-resistant Staphylococcus aureus (MRSA). However, there
is little direct evidence on the effectiveness of cleaning because it has never been afforded scientific status. Hospital hygiene is usually assessed visually, but this does not necessarily correlate with microbiological risk. A more robust case for hospital cleaningcan be presented by considering the evidence for all the stages of the staphylococcal transmission cycle between human beings and their environment. Cleaning has already been accepted as an important factor in the control of other hardy environmental pathogens, such as Clostridium difficile, vancomycin-resistant enterococci, norovirus, and Acinetobacter spp. In her presenatation it also shows why the removal of dirt might have more impact on the control of MRSA than previously thought. Concentration of available cleaning resources on high-risk hand-touch sites may be the most cost-effective cleaning strategy.
“ The trip to Geneva was worthwhile as there were many interesting oral and poster presenta-tions. I would like to know Professor Hugo Sax more - he covers a wide range of topics, from human ergonomics to psychology, and their application to hand hygiene and hand washing compliance, this is interesting! ”
Marlon Marmaril

HEALTHCARE NEWSAcademyInfection Control Specialist
AcademicsStrategies for Improving Cleaning and Disinfection of Environmental Surfaces in Healthcare SettingsJohn Boyce (US)
Dr. Boyce is currently Chief of the Section of Infectious Diseases and Hospital Epidemiolo-gist at the Hospital of Saint Raphael in New Haven, CT, and is Clinical Professor of Medicine at the Yale University School of Medicine. He is a past president of the Society for Healthcare Epidemiology of America (SHEA). He was the lead co-author on the 2002 CDC Hand Hygiene Guideline for Healthcare Settings. Since 2004, he has served as a temporary consultant to the World Health Organization, where he is a member of a core group who developed the WHO
Guideline for Hand Hygiene. He is Director of the Hand Hygiene Resources Center. He has served as a member of the Institute for Healthcare Improvement (IHI) expert panels on improving hand hygiene and on reducing transmission of methicillin-resistant Staphylo-coccus aureus (MRSA), and on the Joint Commission’s Consensus Measurement in Hand Hygiene Expert Advisory Panel. He also served on a CDC expert panel on the role of decolonization therapy in prevention of staphylococcal infections. He is an internationally recognized expert on the epidemiology and prevention of healthcare-associated MRSA infections. He has published articles on the potential role of environmental contamination in transmission of healthcare-associated pathogens, and was principal investigator for the first trial in the United States to evaluate hydrogen peroxide vapor technology for terminal decontamination of patient rooms in a hospital setting. He received his MD degree from the University of Washington in Seattle, Washington, and completed his infectious diseases fellowship training at Hermann Hospital in Houston, TX.
Dr Boyce presented 3 topics in ICPIC, Cleaning and disinfection of environmental surface, how important is the environment in the transmission of epidemiologically important pathogens? And Measuring hand hygiene improvement: Compliance observation or alcohol-based handrub consumption?
In his presentation which regards to cleaning and disinfection of environmental surface, he shares strategy in Improving cleaning/disinfection practices in hospitals, by having different methods of monitoring the adequacy of cleaning, concerns of new liquid disinfectants which warrants further evaluation. He also share checklist of Issues to consider when evaluating liquid disinfectants or area decontamination systems which regards to its effectiveness against bacteria, including C. difficile spores, viruses, including non-enveloped viruses like Norovirus, ease of application, speed of action or room turn-around time, materials compatibility, adverse effects on house-keepers, patients, environment, impact on pathogen transmission and lastly cost required for any new technology.
He also presented on Hand Hygiene improvement by having a multi- modal campaign that is an important element of a successful program, with administrative support, providing HCWs with a well-tolerated alcohol-based hand rub near points of patient care, consistent new educational and motivational materials are also needed. Besides the effort listed, a successful hand hygiene program would be providing monitoring of hand hygiene compliance and updating HCWs with periodic feedback regarding their performance.
Religion and infection control Ziad Memish (SA)
Ziad Memish is currently Assistant Deputy Minister of Health for Preventive Medicine in Saudi Arabia. He is a senior consultant in adult infectious diseases at King Fahad Medical City, a professor of medicine at the college of medicine at Alfaisal University in Riyadh, KSA, President of the Saudi Association of Public Health, an adjunct professor in the department of medicine at the University of Ottawa, Canada, and an adjunct professor in the Hubert department of public health at the Rollins School of Public Health, Emory
University. International committee memberships include the Council of the International Society of Infectious Diseases, the International Infection Control Informal Network at WHO, and the Core WHO Hand Hygiene Guidelines Committee in Geneva. On a regional level he is a member of the WHO EMRO Research Advisory Group and Regional Expanded Program for Immunization Advisory Group. In November 2007, he was awarded by the Custodian of the Two Holy Mosques King Abdullah Bin Abdulaziz Al Saud, the King Abdulaziz Medal from the First Degree for achievements in the field of infectious diseases and infection control.
Dr. Ziad’s presentation, Religion & Infection Control, discusses his efforts to understand the differences in culture in the world that can affect hand hygiene in healthcare facilities around the world. An extensive survey of literature was conducted in addition to interviews with experts and religious authorities to investigate religious and cultural factors that may potentially influence hand hygiene promo-tion. He offers possible solutions and suggests areas for future research. Dr. Ziad’s research shows that religious faith and culture can strongly influence hand hygiene behavior in health care workers and potentially affect compliance with best practices. Interesting data were retrieved on specific indications for hand cleansing according to the seven main religions worldwide, interpretation of hand gestures, the concept of “visibly dirty” hands, and the use of alcohol-based hand rubs and prohibition of alcohol use by some religions were share and presented. He concludes that, as medicine advances faster than we can assimilate required changes in attitudes and ethical beliefs, we will see an increasing number of interfaces between science and belief—interfaces that may take time to resolve. Today’s health-care delivery systems must be sensitive to a range of personal religious and cultural beliefs and take these into consideration.
“I attended the conference to learn more about new disinfectants entities in the markets and updates of any new information which regards to novel products and technologies knowledge to bring back and share in Russia. We sponsored several KOLs from Russia and they had a chance to get acquainted with Mr. President Saraya which is very good for our business.”
Alexander Dorofeev

HEALTHCARE NEWSAcademyInfection Control Specialist
Sponsorships
Innovation AcademyThe Innovation Academy at ICPIC 2011
In line with our company goal and direction of providing know-how and creativity targeted towards real world applications and our customers' needs is the basis for developing SARAYA’s innovative products, we are very proud to be a sponsor of the Innovation Academy.
What is the Innovation Academy?
The Innovation Academy is a unique opportunity to allow researchers and participants at ICPIC 2011 to partici-pate in a forum which brings the spotlight to new and upcoming innovations in the field of infection control and prevention of antimicrobial resistance. As the first of its class at an Infection Prevention and Control Meeting the Innovation Academy was an exciting opportunity for all attendees. The Innovation Academy brought together experts from many diverse fields allowing for great interaction during the event. In the end, three “Innovation Awards of Excellence” were presented after the Expert International Jury of the Academy reviewed the presenta-tions.
The first Innovation Academy competition was organized on the final day of ICPIC 2011. A world of ideas and businesses were presented with their both lifesaving and commercial designs. In the end, Budapest University of Technology and Economics Hand-In- Scan Out received first place. Their invention allows instructors to give an objective evaluation of surgical hand disinfec-tion practice and review.
The first Innovation Academy of its kind was organized in cooperation with the Hospital University of Geneva (HUG) representing 1,300 people from around the world in every major infection control and hospital hygiene company. The conference accepted 600 applications and 54 were selected for the Innovation Academy finalists. The remaining 14 were given the opportunity to proceed to the semi-final first poster presentation. It was then a short 3-minute presentation to present the innovation idea to the international jury and the hundreds of interested parties about their project.
Five finalists were selected from the poster presentation on the last day of the event , and each gave a 15 minutes presentation to the judgesand audience. The finalists included contestants from Ireland, Spain, Canada, the USA, and Hungary. The contestants from Hungary were awarded the trophy and 10,000CF for their innovative hand hygiene scanner. The Innovation Academy was sponsored by SARAYA, and we are excited to support new technology and research around the world.
The Hand-in-Scan team (Melinda Nagy, Ákos Lehotsky, Dr. Szilagyi Laszlo and Dr. Thomas Haidegger) invented a compact device for the objective verification of hand disinfection quality. After the regular hand washing procedure using a marked soap (alcohol-based disinfectant mixed with UV-reflective powder), the hands are inserted under the device, one side at a time. Surfaces treated sufficiently appear brighter. Digital images are taken in the UV-lighted area with a camera mounted on the case. The images are processed by specific software (using artificial intelligence methods), running on a connected laptop, which performs automated evaluation providing visual feedback on the screen. It highlights disinfected versus untreated areas, and indicates an overall score of the hand washing that is displayed on the computer screen.
This innovation results also show that the world increasingly has begun to take hand hygiene in health care seriously because ofimproper and inadequate hand washing practices is risking the human life. The system is able to teach the techniques required, and then check for accuracy as well.
“If at first, the idea is not absurd, then there is no hope for it. Innovation is not the product of logical thought, although the result is tied to logical structure.”
Albert Einstein, Physicist and Nobel Laureate, who spoke often of innovation and creativity.
“It was interesting to listen to presentations regarding hand hygiene and learn about the research and tests in this field. Most of all, I appreciated the presentations regarding the surface disinfection and cleaning, because SARAYA Europe are starting with surface disinfection product line”
Nicole van Hall

T. Haidegger 1,2, M. Nagy 1, Á. Lehotsky 1, L. Szilágyi 3
Hospital acquired infection (HAI) in hospitals:
• Average HAI ratio: 7.1% for the Western world (1996–2007)• [SENIC study, Am J Epidem 2005; Annual Epidemiological Report 2008]
•HAI causes 15,000 deaths in Europe; 90,000 in the USA annually • [Pollack 2010; Korniewicz 2007]
• Nosocomial infections can triple hospitalization time and costs• [Plowman et al. 1999]
• $0.7–1.4M annual cost/US hospital, $4–8B total direct cost/year• [Pollack 2010; Korniewicz 2007; CDC Annual Report 2010]
Regular use of the system
hand washing with the UV-reflective soap
hands are inserted into the box
digital imaging (remote controlled)
image processing on a laptop
software performs image processing
automated segmentation and clustering
artificial intelligence method
hand contour from intensity image
objective evaluation and feedback
reporting towards the Hospital IT System
creating large case studies/user databases
Clinical need
The fight against HAI begins at the hands
Stery-Hand: a compact device for objective verification and control
Surgical hand disinfection—hand rubbing
• 15–30% of HAI could be prevented through better hand hygiene• [Plowman et al. 1997; Pittet 2000; Graves et al. 2002]
• 40% further reduction through other solutions• [Plowman et al. 1997]
European norms for hygienic care
• EN 1499 – hygienic hand wash
• EN 1500 – hand disinfection
• Most frequently omitted parts• [CDC 2009]
• Medical staff’s hand washing
compliance must be improved
Digitalcamera .
Case withUV lighting .
UV-reflective antiseptic . Raw image
Imageprocessing
Tamás HAIDEGGER, [email protected] Website: https://sites.google.com/site/steryhandbme
An Innovative Device for Objective Hand Disinfection Control
• Stery-Hand is a pilot project of the BME Technology and Knowledge Transfer Office • It is supported by ACMIT and formerly by Contact Singapore• Strategic partner of the project is the National University Hospital, Singapore• Graduate of the Semmelweis Innovation’s SIBE business development course• Special thanks to Erik-Artur Csonka
World Health Organization (WHO) major efforts:
• World-wide hand washing campaign
• Hand Washing Day (May 5th) since 2009
• Over 13,000 medical institutions in 2011
• 5 moments for hand hygiene
• 8 steps of hand rubbing
• 8 steps of hand washing
• US FDA norms
• US CDC recommendations
• Similar standards in Singapore
Additional steps
Washing the lower arm
Washing up to the elbow
1 Budapest University of Technology and Economics, Dept. of Control Engineering and Information Technology2 ACMIT – Austrian Center for Medical Innovation and Technology
3 Sapientia – Hungarian Science University of Transylvania, Faculty of Technical and Human Sciences
No.O39c
Stery-Hand prototype Software-based evaluation
Application and validation
Primary applications of the Stery-Hand
• Education of medical students
• Medical institution staff training
• Public health awareness raising
• Tight control over the hospital staff compliance
• requires further H&S development
• Food industry
• Electronics manufacturing
Clinical tests at
• Semmelweis University, Budapest
• 25 medical students
• Korányi National Pulmonology Institute, Budapest
• 50 staff members
• Targu-Mures County Hospital, Romania
• 15 staff members
• Singapore National University Hospital
• 4700 people (under evaluation)
• Non-medical deployment in Hungary, Austria and France
Acknowledgment
Ro
man
iaH
un
gary
Hu
nga
ry
Contact

HEALTHCARE NEWSAcademyInfection Control Specialist
Sponsorships
Travel fellowship
Limited information is available on the endemic burden of HAI in Africa, however it is known that infections occur much more frequently in African hospitals than in developed countries. There is an urgent need to identify and implement feasible and sustainable approaches to strengthen HAI surveillance and control in Africa, including preventive strategies.
In 2008, it was reported that 135 of every 1000 children under the age of 5 was victim to a fatal disease. Most were preventable diseases such as diarrhea or respiratory infections.
At ICPIC the AFRICA RIPAQS ICPIC session was held on "Contribution of quality strategies for the care and patient safety in the fight against infections in maternity services to achieve the health MDGs (Millennium Development Goals) in Africa."
The objective was simple, improving the health of the African population, which has been a major public health initiative since African countries adopted recommendations of the Alma Ata conference in 1978.But for 30 years after Alma Ata, most countries in the African region should further accelerate progress in strengthening health systems through the PHC (Public Health Care) approach by integrating the concepts of quality of care and patients safety to achieve health goals agreed at the national and international, including MDGs.
According to WHO research, the negative factors influencing the safety of patient care is the cause of the high mortality rate with 4 to 16% of all hospital patients becoming the victim of adverse events including life-threatening issues. Over half are associated with surgical care and more than half are preventable.
Nosocomial infections are at the forefront of these adverse events related to care and are now a constant concern in hospital practice in both developing countries and developed countries.
In Africa, the prevalence of nosocomial infections varies from 35 to 60% and they represent the third leading cause of maternal mortality. Infections in the hospital the second leading cause of neonatal mortality and the leading cause of postoperative mortality. The prevalence of these conditions reduces the impact of interventions against HIV, malaria and other diseases (MDG 6).
This prevalence is estimated at 10.9% in Senegal, 12% in Côte d'Ivoire, 10%, Benin and 14% in Mali
So there is a positive and strong relation between patient safety activities and the strategies to improve the critical components of the healthcare system. Strengthening the national health care systems is essential to fight against disease and to achieve the MDGs related to healthcare in Africa.
Nosocomial infections severely affect the quality of care and contribute to increased direct and indirect costs of healthcare. In Quebec, the cost of nosocomial infections in the health care system are estimated at $180 million per year or about 72 billion CFA francs. Therefore improving patient safety is an urgent issue, and realizing better patient safety practices can improve Africa’s healthcare quality drastically.
SARAYA and UNICEF introduced the “Wash A Million Hands Project” to provide hand washing to children and raise hand hygiene awareness in Uganda in 2010. We are very proud to be a sponsor and contributor to ICPIC, sponsoring 9 participants from around the world to Geneva.
All the presentation at the conference related to a hygiene condition of a medical facilities in under developing countries were quite fascinating because those were what exactly I would like to learn and share in Uganda.”
Kazumasa Miyamoto
“The main task for me to attend this event was to increase our brand prestige and recognition amongst French speaking participants. Overall I believe it has been a great success. Many French native speakers came to our booths, and they were amazed with what SARAYA initiatives globally.”
Christophe Catanzano

HEALTHCARE NEWSAcademyInfection Control Specialist
SponsorshipsWine & Cheese reception, Poster presentation.
Hard cheese, soft cheese, cottage cheese, cheese made in mountain chalets, cheese made in valley factories, cheese shaved into rosettes, cheese boxed in red pine, cheese melted in wine to make fondue, hot cheese dribbled over potatoes to make raclette... There's much more to Swiss cheese than making holes!
No-one knows exactly when or where cheese was invented - although it can be said for certain that it was not in Switzer-land. One story has it that a merchant travelling through the desert 5000 years ago made the discovery by accident when the milk he was transporting in a bag made of a sheep's stomach reacted with the natural rennet in the stomach lining and was churned into cheese by constant jogging. Be that as it may, cheese is certainly mentioned in the Old Testament in
texts which may date back 3,500 years.
With the famous proverb “All work and no play makes Jack a dull boy” SARAYA sponsored the Friday evening, POSTER VIEWING, EXHIBITION, WINE & CHEESE reception. This is a session for all to mingle and network between participants, and poster presenters. Some of the posters presented during the event are attached in the following pages.
Topics
1 Health-care associated infection• Bloodstream and intravasculardevice associated infections• Surgical site infections• Ventilator-associated pneumonia• Urinary tract infections• Gastroenteritis (other thanNorovirus and CDAD)• Norovirus1g C.difficile/CDAD• Staphylococcal infections• Bone- and prosthetic jointinfections• Nosocomial viral infections (otherthan norovirus and influenza)• Influenza/lessons learned from H1N11l Yeast and mold infections• Burden of HAI
2 Multi-drug resistant microorganisms• MRSA epidemiology and control• Vancomycin-reistant enterococci• ESBL & Co (Gram-negativeresistance)• Multidrug-resistant pathogens(other than MRSA, VRE and ESBL&Co)
3 Antimicrobials• Antimicrobial-resistance (surveillance)• Antimocrobial-use and stewardship
4 Special issues in infection control• Hand hygiene• Behaviour and infectioncontrol/influencing HCWs• Patient participation• Healthcare worker (HCW)education• Innovative approaches in infectioncontrol• Ergonomics and human factorsdesign in infection control• Epidemiological methods and theirapplication to infection control • Mathematical modelling ininfection control
5 Surveillance of HAI• Surveillance and infection controlindicators• Public reporting / Benchmarking of infection rates OR Public reporting/Benchmarking
6 Special patient populations• Infections & infection preventionin critical care (ICU)• Infections & infection control inneutropenic patients• Transplantation and HAI/HAIprevention• Infections and infection preventionin pediatric populations• Infection control in long-term carefacilities and nursing homes• Infections and infection preventionin the developing world
7 Special settings• Operating room• Dialysis• Endoscopes
8 Disinfection/sterilization• Environmental control• Disinfection – skin (other thanhands)• Sterilization
9 Outbreaks
10 Public-health and patient safety issues
11 Nursing homes
12 Occupational health
13 Submissions in French
14 Innovation in infection control andantimicrobial
resistance prevention
“What interest me most of the whole event was the Innovation academy was the most interesting as it was all about product development even out of my research field. I would like to know Dr Rotter & Dr Andreas Widmer !”
Etsu Noguchi

IntroductionInfection and colonization with Methicillin-resistantStaphylococcus aureus (MRSA) is associated with significantmorbidity and mortality. The essential components of recentguidelines to control MRSA in hospital settings are activesurveillance cultures (ASCs) in addition to contact precautionsand isolation.In 2009-2010, there was an increase in the number if MRSAinfected cases in SICU in CGH compared to 2007-2008.
MethodologyThe study was undertaken in the SICU (18 single rooms) inChangi General Hospital. MRSA ASCs were performed from 20Sep 2010 to 28 Feb 2011 on all patients admitted or transferredin and transferred out of SICU. Patients were excluded from exitswabs if they had an ICU stay of less than 24 hours or known tobe previously positive for MRSA.ASC specimens consisted of one swab from the anterior naresand another from the axilla/groin. The swabs were inoculatedonto chromogenic agar selective for MRSA (MRSASelect, Bio-Rad). MRSA positive patients were electronically flagged by theinfection control nurses. Contact precautions (gloves, gowns andstrict hand hygiene) in single room isolation were instituted forthese patients.The five days decolonization regimen consisted of mupirocinnasal ointment tds and daily skin antisepsis with Prontoderm0.1% polyhexanide (B. Braun, Melsungen, Germany). Automatichand sanitizers UD1000 (Saraya, Japan) were installed in SICUto increase hand hygiene compliance. Sureclean, an ionic silverdisinfectant lasting 24 hours, was used for environmentaldisinfection during the study period.
ConclusionOur study demonstrates the usefulness of active surveillancecultures, intensified MRSA control program and environmentalcleaning in significantly reducing MRSA Infections in the SICU.
The Impact of Active Surveillance Cultures in Reducing Methicillin-resistant Staphylococcus aureus Infections in a Surgical Intensive Care Unit in SingaporeHML Oh1, TY Tan2, GH Chua3, J Li3, QS Meng31Medicine, 2Laboratory Medicine, 3Infection Control, Changi General Hospital, Singapore
ObjectiveTo study the impact of ACS, environmental cleaning anddecolonization regimen in reducing MRSA infection in SurgicalIntensive Care Unit (SICU).
ResultsA total of 453 patients were screened on admission/transfer inand 214 patients were screened on transfer out/death. 45patients (9.9%) were MRSA positive on entry and 9 patients(4.2%) acquired MRSA on exit. The compliance rate for entryswabs was 95.4% and for exit swabs was 79.6%.There were 10 skin, 29 nasal and 15 skin/nasal carriers. 7patients received nasal, 17 received skin and 9 received nasaland skin decolonization with 40%, 38% and 27% clearancerespectively.
Characteristics of MRSA-positive and MRSA-negative Patients
MRSA positive MRSA negative P. value
No. of Patients 54 (45 entry, 9 exit) 399 -
Age, years mean (range) 67 (23 – 99) 60 (15 – 97) 0.023
Sex, n (%)MaleFemale
38 (70.4%)16 (29.6%)
249 (62.4%)150 (37.6%)
0.254
Pre ICU L0S, days (range) 12 (1 – 132) 3 (1 – 77) <0.001
Average LOS in SICU days (range)
4 (1 – 29) 4 (1 – 62) 0.591
Discussion
ICUs are high risk units for the importation and acquisition ofMRSA. The primary outcome of this study was the acquisitionrate of MRSA colonization. This study revealed the MRSAcolonization rate on admission to be 9.9% which reflects the highlocal burden of endemic MRSA.
The acquisition rates for SICU was 4.2% (9 patients) whichimplied that the cross transmission was reduced by theenhanced hand hygiene practices. The multiple interventionsused in this study namely active surveillance cultures, intensifiedMRSA control program, decolonization measures andenvironmental cleaning reduced the MRSA infection rates inSICU.
Detection of MRSA on ICU admission or discharge wasassociated with older age (mean age 67 years vs 60 years, p =0.023) and a longer pre-ICU LOS 12 days vs 3 days, p < 0.001)
There was an increase in overall hand hygiene compliance from68.4% in Sep 2010 to 90.9% in Feb 2011. The incidence ofMRSA infection was reduced from 1.7/1000 patient days (Mar-Aug 2010) to 0.9/1000 patient days (Sep 2010-Feb 2011)
MRSA infected cases in SICU from Jan 10 to May 11
1
3
0
1
0
1 1 1
0 0
1 1
0 0
1
0 00
1
2
3
4
Jan-1
0
Feb-10
Mar-10
Apr-10
May-10
Jun-1
0Ju
l-10
Aug-10
Sep-10
Oct-10
Nov-10
Dec-10
Jan-1
1
Feb-11
Mar-11
Apr-11
May-11
no. o
f cas
es
Study Period---------------------------




HEALTHCARE NEWSAcademyInfection Control Specialist
Social time with KOL
On a sunny Tuesday evening we had the privilege of getting together with Dr Ziad of Saudi Arabia for dinner at the French Seafood restaurant, Brasserie Lipp. The dinner reception was well attended and fun, of all most important was the time and precious company of Dr. Ziad, Prof. Helen Oh & Dr. Nazri. The evening ended with the famous French dessert; Crème brûlée.
After the entertaining and informative opening ceremony and keynote lectures by Sir Liam Donaldson and the famous Lancet author on NDM-1, Tim Walsh, we had a great evening dinner at the Les Armures Restaurant. I remember it as a beautiful chill and drizzling evening. The 20 minute walk from ICPIC to the restaurant allowed us to pass through the famous Patek Philippe time piece museum, up the corner of Parc des Bastions to the old town of Geneva. Les Armures, the 13th Century structure serves the best of Swiss specialties and has been host to some very famous clients such as former US President Bill Clinton and his wife Hillary.
We had the privilege of the evening with Dr. Seto, Dr. Bijie, Ms. Patricia Ching, Prof. Nordiah, Prof. Helen Oh, Dr. Kaku and Dr Kunishima
From infection control to the beautiful mountains of Austria and we finish lunch with the famous classic by Mozzart, at the Universal Café. We were much honored to have the company of Prof Rotter. During lunch Yusuke and Rotter met for the first time, and both end up being acquainted by Mozzart pieces.
Because of the quick and delicious food that was served at the Universal Café, we again had lunch with Dr. Boyce there. I must thank this restaurant recommendation to Dr. Harbarth.
Pizza time with Prof Helen and Dr Nazri! Perhaps the best pizza we could agree to have!
Dinner with Prof Nordiah and her team, a wonderful time to get together.
June 28th Evening Dinner
29th Evening Dinner
June 30th Afternoon Lunch
July 1st Afternoon Lunch
July 2nd Evening Dinner
July 4th Afternoon Dinner
“I attended the conference to manage and arrange the booth setup, and to promote SARAYA. I believe overall we did a good job as a first step, since there are more people who got to know us by the end of the conference. I would like to meet Prof Pittet and Prof Lindsay Grayson again!”
Hidekazu Tanaka

HEALTHCARE NEWSAcademyInfection Control Specialist
Activities at the booth
SARAYA exibition booth Girls in kimono
World of dispensers! Sam’s magic hands! Swiss president
Diverted! Dancers of HH videoThe Hands
KOL
“I attended the conference to support our colleagues and also to appeal Japanese identity at the exhibition with Kimono, and I believe that we have done it well together with our beautiful colleagues.”
Yuko Higashino
“The location of our booth was the best to my opinion as we were placed in front of the main entrance and also the main conference room. I would like to know Prof Pittet more, as he is a professional in Hand Hygiene!”
Lee Seulbee
“I was very pleased to attend the conference and become acquainted with all colleagues from SARAYA. It was also a good opportunity to meet and discuss current healthcare issues and future mutual cooperation with KOL from Russia”
Ekaterina Povod
HEALTHCARE NEWSAcademyInfection Control Specialist
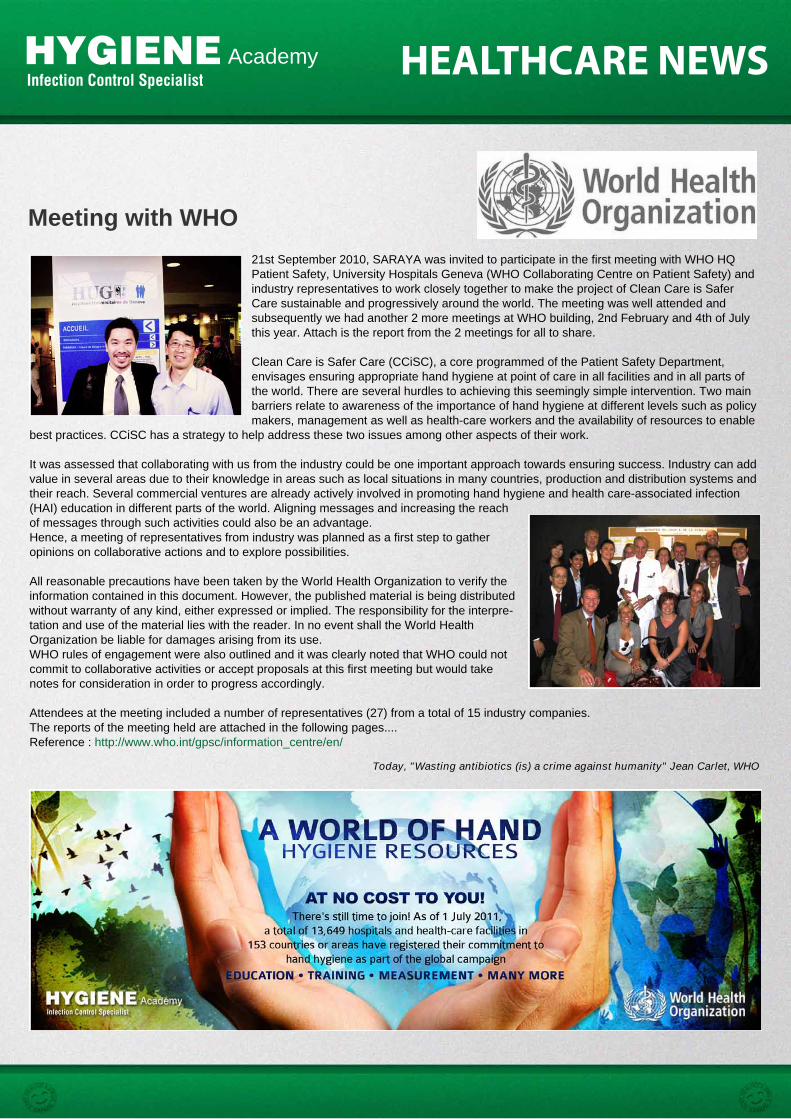
Meeting with WHO21st September 2010, SARAYA was invited to participate in the first meeting with WHO HQ Patient Safety, University Hospitals Geneva (WHO Collaborating Centre on Patient Safety) and industry representatives to work closely together to make the project of Clean Care is Safer Care sustainable and progressively around the world. The meeting was well attended and subsequently we had another 2 more meetings at WHO building, 2nd February and 4th of July this year. Attach is the report from the 2 meetings for all to share.
Clean Care is Safer Care (CCiSC), a core programmed of the Patient Safety Department, envisages ensuring appropriate hand hygiene at point of care in all facilities and in all parts of the world. There are several hurdles to achieving this seemingly simple intervention. Two main barriers relate to awareness of the importance of hand hygiene at different levels such as policy makers, management as well as health-care workers and the availability of resources to enable
best practices. CCiSC has a strategy to help address these two issues among other aspects of their work.
It was assessed that collaborating with us from the industry could be one important approach towards ensuring success. Industry can add value in several areas due to their knowledge in areas such as local situations in many countries, production and distribution systems and their reach. Several commercial ventures are already actively involved in promoting hand hygiene and health care-associated infection (HAI) education in different parts of the world. Aligning messages and increasing the reach of messages through such activities could also be an advantage. Hence, a meeting of representatives from industry was planned as a first step to gather opinions on collaborative actions and to explore possibilities.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpre-tation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. WHO rules of engagement were also outlined and it was clearly noted that WHO could not commit to collaborative activities or accept proposals at this first meeting but would take notes for consideration in order to progress accordingly.
Attendees at the meeting included a number of representatives (27) from a total of 15 industry companies.The reports of the meeting held are attached in the following pages....Reference : http://www.who.int/gpsc/information_centre/en/
Today, "Wasting antibiotics (is) a crime against humanity" Jean Carlet, WHO

1All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Report from the first meeting of WHO HQ Patient Safety, University
Hospitals Geneva (WHO Collaborating Centre on Patient Safety) and industry representatives
21 September 2010, University Hospitals Geneva, Switzerland
Report Issue Date: October 2010
1. Introduction Clean Care is Safer Care (CCiSC), a core programme of the Patient Safety Department, envisages ensuring appropriate hand hygiene at point of care in all facilities and in all parts of the world. There are several hurdles to achieving this seemingly simple intervention. Two main barriers relate to awareness of the importance of hand hygiene at different levels such as policy makers, management as well as health-care workers and the availability of resources to enable best practices. CCiSC has a strategy to help address these two issues among other aspects of their work. It was assessed that collaborating with those in industry could be one important approach towards ensuring success. Industry can add value in several areas due to their knowledge in areas such as local situations in many countries, production and distribution systems and their reach. Several commercial ventures are already actively involved in promoting hand hygiene and health care-associated infection (HAI) education in different parts of the world. Aligning messages and increasing the reach of messages through such activities could also be an advantage. Hence, a meeting of representatives from industry was planned as a first step to gather opinions on collaborative actions and to explore possibilities. Aims of the meeting were presented prior to the meeting as:
• To overview WHO First Global Patient Safety Challenge: Clean Care is Safer Care and WHO Collaborating Centre (University Hospitals Geneva) activities
• To gather input on where the 'private sector' can further the WHO goal of sustainable improvement of hand hygiene in health-care facilities around the globe (to be achieved through active discussion)
• To discuss how to work together to further the WHO agenda, for example supporting the availability of items to improve hand hygiene where there is a need and to contribute to awareness-raising in a manner acceptable to the WHO ethos.

2All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
WHO rules of engagement were also outlined and it was clearly noted that WHO could not commit to collaborative activities or accept proposals at this first meeting but would take notes for consideration in order to progress accordingly. Attendees at the meeting included a number of representatives (27) from a total of 15 industry companies. 2. Summary of meeting proceedings Following introductory presentations from WHO representatives there were a number of questions and points raised, e.g. clarifications on our strategy and recommendations, experiences with implementation, adaptation of WHO hand hygiene tools and permissions for this (as per information available at http://www.who.int/gpsc/copyright/en/index.html) and barriers within countries to implementing the use of alcohol based handrub (ABHR). Structured discussions, which represented the majority of the meeting, followed and focussed on three key areas as had been identified by WHO:
• System change • Education • Research.
Participants deliberated over their role, the role of WHO and the potential benefit to others while considering these three areas. Key points and themes emerged from discussions:
• Firstly there was clear enthusiasm for collaboration • A number of hurdles need to be overcome before this can be a reality
o Key concerns included competitors working together and inherent conflicts of interest between WHO and industry
• Corporate responsibility of industry was highlighted as a possible opportunity for collaboration and action
• Potential action areas were explored and are summarised in Table 1. Table 1: Summary of potential action areas Area Potential benefits for HCFs Suggested actions Education Scale up, better penetration and
wider reach Support for resources (funded by industry)
Individual company or collaborative/group support for awareness raising campaigns in low-resourced countries
System change Advice on regulation and other obstacles to introducing hand hygiene facilities such as ABHR
Exploring possibilities for creating micro-production sites for ABHR

3All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
and provision of water and soap Identification of solutions to obstacles and increased participation in this work
Support governmental and non-governmental agencies involved in providing hand hygiene facilities
Research Identifying avenues for funding for operational research e.g. to understand sustainability and benefits to health-care systems and embedding of hand hygiene in bundles related to care/hygiene
Exploring and offering funding and/or resources for WHO identified priority areas of research aimed at improving hand hygiene at the point of care
3. Next steps Based on discussions and suggested areas for collaboration, WHO has identified the following as next steps:
• Setting up an initiative to allow competitors to work comfortably alongside each other, so that WHO will be transparent about their activities with all industry partners and may solicit their participation in specific projects
• Explore proposals on the practicalities of ABHR micro-production in low resource settings, prior to any further steps.
Should the aforementioned two areas be acceptable to WHO and industry partners, detailed proposals will be necessary, explaining the role of WHO, the role of industry and benefit to the target population, e.g. health-care facilities. Input from industry partners to establish next steps for realistic collaborative working will be sought in a timely manner. Note: Several activities can happen concurrently based on agreed proposals. In order to maintain momentum for collaborative working, all participants agreed that frequent communications and further meetings would be crucial. Based on WHO approval to continue working in this manner, a next meeting early in 2011 will be announced. It is also anticipated that a further meeting will be held in June 2011 during the time of the International Conference on Prevention and Infection Control, Geneva, Switzerland. WHO and the WHO Collaborating Centre would like to thank all of those who participated in this inaugural meeting.

1
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either
expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Report from the second meeting of WHO HQ Patient Safety and industry
representatives With invited representative from University Hospitals Geneva (WHO
Collaborating Centre on Patient Safety, Infection Control and Improving Practices)
2 February 2011, World Health Organization (WHO) Geneva, Switzerland
Report Issue Date: March 17 2011
1. Introduction Following discussions and decisions made during the first exploratory meeting on 21 September, 2010 between representatives from private industry and WHO, a second meeting was convened in the World Health Organization Geneva, Switzerland on 2 February 2011. 2. Overall Purpose The overall goal of WHO Clean Care is Safer Care (CCiSC) is to improve hand hygiene in health care facilities. There are several hurdles to achieving this seemingly simple intervention. Two main problems relate to awareness on the importance of hand hygiene at different levels, such as policy makers, management and health-care workers, and the availability of resources to enable best practices. There is a potential for the private sector to significantly contribute to these two main areas and amplify the efforts of CCiSC. They can add value in several areas due to their reach, their knowledge in areas such as local situations in many countries and production and distribution systems for hand hygiene products. Several commercial ventures are already actively involved in promoting hand hygiene and health care-associated infection (HAI) education in different parts of the world. Aligning messages and increasing the reach of messages through such activities could be of great advantage. It could be possible to exploit 'corporate social responsibility' to support health-care system change developments as well as education in resource poor countries. According to recommendations of CCiSC, 'system change' includes primarily making available essential commodities needed for hand hygiene - alcohol-based handrub, water, soap and single use towels - at all times in all health-care facilities. There are also specific recommendations related to numbers, positioning, etc related to these products.

2
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either
expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
Such a collaboration links with the overall WHO Patient Safety Programme draft strategic objectives of making safety issues everyone's business while making more stakeholders taking responsibility for actions. Given the purpose of and potential for collaboration, as has been described, this second meeting was deemed a useful next step. In summary, during the first meeting, two potential areas for action were identified:
1. developing a coherent and lucid collaboration where industry representatives can sign up and thus commit to the regulations and overall work of the collaboration
2. developing a model for micro-production of alcohol-based handrub (ABHR) in resource poor areas, to enable access to products
For full details refer to the report of the first meeting (http://www.who.int/gpsc/information_centre/gpsc_slcyh_meetingreport_oct2010_en.pdf). 3. Summary of second meeting proceedings The aims of this second meeting were:
1. to keep the momentum generated during the first meeting; 2. to take forward discussions on modalities of working together.
The meeting was chaired by Dr Edward Kelley and Professor Didier Pittet. Welcome, introductions by all (including descriptions from industry representatives on their areas of work and geographical coverage) and preliminary remarks by the Chairs were delivered. Following this, the purpose of the meeting, the current status of the work towards building collaboration modalities and outputs expected from small group discussions during this meeting were explained by Dr Elizabeth Mathai. Small group discussions followed, featuring the majority of the meeting with feedback subsequently provided. To close the meeting, Ms Claire Kilpatrick provided an update of the CCiSC current activities and the activities proposed for the global call for action on May 5 2011 as part of the WHO SAVE LIVES: Clean Your Hands campaign, before final discussions led by the Chairs. The agenda, attendee list and slides presented by WHO staff can be found in the appendix.

3
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either
expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
4. Summary of group discussions on the three potential areas for collaboration The topics addressed by the groups were the same as that of first meeting namely: education (raising awareness and sharing knowledge), system change (enabling access to essential commodities for hand hygiene) and research (product merits, evidence for impact of hand hygiene and implementation research). The groups focussed on WHO role, collaborator role and benefits as a result of collaboration in these areas. In summary, the outputs from the group discussions were significant. All groups acknowledged that working on the points outlined with WHO leadership would be acceptable to them. They also expressed willingness to actively participate (success depends on this) in the collaboration and to sign up to some form of 'code of conduct'. Summary of group discussion on 'Education': WHO's role is to provide direction and develop educational materials. Industry can further the reach by using the materials in a responsible manner as will be outlined in a 'code of conduct' to be developed. It was further expressed that: • This work needs to have defined outcomes and a produce a 'legacy'; • Support for the 5 components of WHO's multimodal improvement strategy
promoted by CCiSC is essential, for this to be disseminated through education;
• A working group on education with definite terms of reference needs to be established.
Summary of group discussion on 'System change': WHO's role is to convene and to facilitate communications between industry (participants in the collaboration) and beneficiaries, i.e. to provide information on needs known to WHO, related to system change, to the participants of the network and then take part in initial actions to facilitate contact between industry and the beneficiary and any other participant such as an Non Governmental Organisation (NGO) interested in this area. Participants inform WHO of their interest and interact directly with the beneficiary after initial interactions involving WHO. Participants could also inform WHO about needs in health-care facilities or countries they they identify and would like to provide assistance. The group further expressed the need for: • Developing a 'code of conduct' clearly addressing conflict of interest,
competitive behaviour etc. This should be signed and posted on the 'collaborative working platform';
• Maintaining two way communication respecting requirements of both parties; • Maintaining confidentiality. This should be stated and details clarified in the
'code of conduct'.

4
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either
expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
(Micro-production of ABHR was discussed briefly, but felt that plans would be country specific and hence some kind of gap analyses is the first step.) Summary of small group discussion on 'Research': Areas requiring research were identified by this group. These included improving the evidence base to justify hand hygiene promotion and identifying customer needs. The actionable areas suggested were customized messaging, innovation and education tools to drive change, compliance measurements, impact of work flow on compliance, prevalence of adverse events and cost benefit studies. More details are needed to conceptualise the roles of WHO and industry on this area of collaboration. 5. Mechanism for collaboration proposed In the first instant, the plan is to develop a web-based platform which will enable WHO to be transparent and provide equal opportunity to all participants. This would also allow for confidentiality of the information shared by participants with WHO.
• The idea was accepted by those present, who also welcomed progressing this as a next step;
• Criteria for participation in the collaboration should be developed; • Sub-groups or working groups, such as the one suggested for education,
should be hosted on the platform; • That other NGOs, i.e. those involved in improving water supplies, as well
participants of WHO CleanHandsNet (the WHO network of coordinators of countries with coordinated hand hygiene promoting campaigns) could be other potential participants;
• At a later stage, it could be used for sharing information between WHO and participants, for announcements and for calling for action on specific proposals.
Specific requests related to May 5 2011 were made and agreed upon. These were:
• Key messages for May 5 to be continually shared through our web pages; • To include those present in the email list for disseminating information.
It was also proposed and agreed that: - Representatives who had not yet attended CCiSC sessions could request training on WHO strategies and models of promoting hand hygiene in health care; - Participants would share with WHO their available data on sales of ABHR, to do a global mapping and gap analyses exercise. This could be done as one of the initial activities via the platform. While the information may not be complete and represent the total ABHR sales in the world, this will provide WHO with useful information.

5
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this document. However, the published material is being distributed without warranty of any kind, either
expressed or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use.
6. Next steps The participants were informed of the potential for a next meeting to coincide with the International Conference on Prevention and Infection Control (ICPIC) meeting to be held in the University of Geneva from June 29 to July 2 2011. It was agreed that participants would submit two slides on their main areas of work and geographical coverage to WHO and that WHO would circulate the WHO slides presented and the meetings notes subsequent to necessary approvals.

HEALTHCARE NEWSAcademyInfection Control Specialist
SARAYA Worldwide
Today, "Wasting antibiotics (is) a crime against humanity" Jean Carlet, WHOSaraya Australia Pty Ltd
Saraya Taiwan Co., Ltd.
Best Sanitizers, Inc.
Saraya International (Thailand) Co., Ltd.Saraya MFG (Thailand) Co., Ltd.
OOO Best Sanitizers CIS
Saraya Canada Co., Ltd.
Saraya Malaysia
Saraya (Shanghai) Biotech Co., Ltd.
Saraya HongKong Co., Limited
Saraya Korea Co., Ltd.
Saraya Co., Ltd.
Best Sanitizers Inc. Kentucky Factory
Saraya Co., Ltd. Europe