acetylcholine kevin k. caldwell, ph.d. - university of …neurohsc/532/ppt_ach for neurochem...
TRANSCRIPT

Acetylcholine
Kevin K. Caldwell, Ph.D.
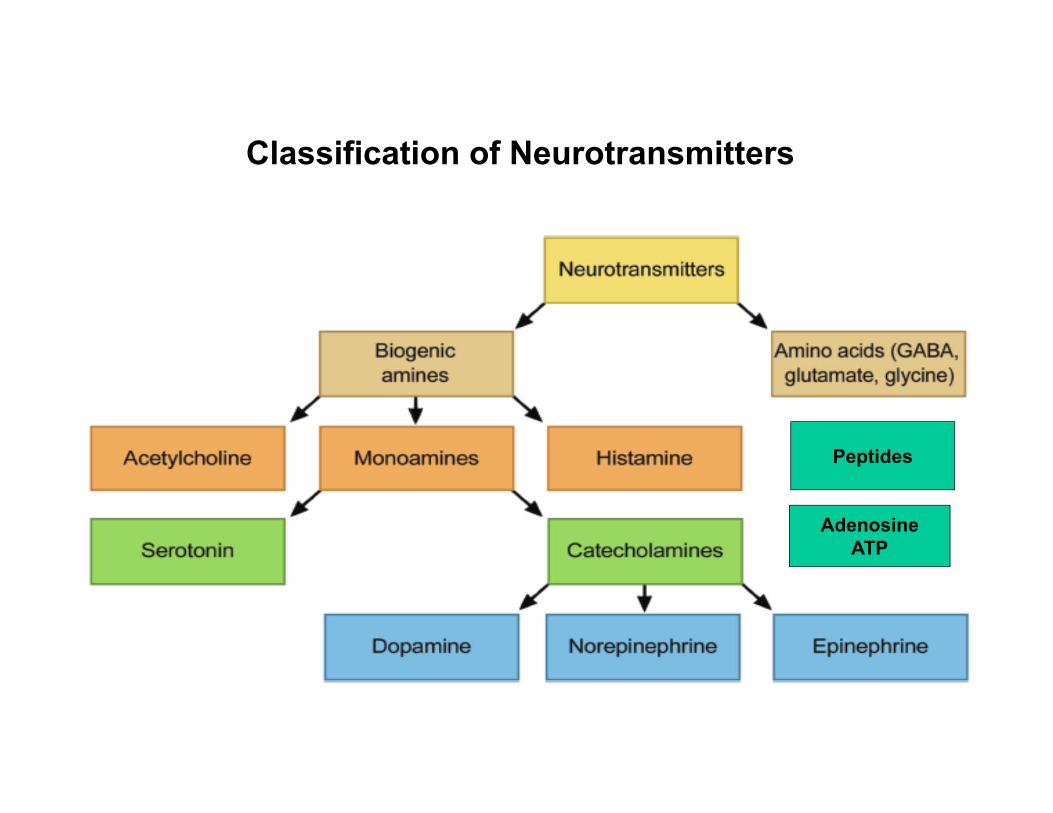
Peptides
AdenosineATP
Classification of Neurotransmitters

Criteria for defining a neurotransmitter
Purves, D. et al. Neuroscience, 4th edition, 2007

Synaptic vesicle release and recycling
ATP
ATP

ACETYLCHOLINE
Biochemistry
Anatomy
Physiology
Pharmacology
Pathology

Acetylcholine Synthesis
Acetyl-CoA + Choline Acetylcholine (ACh)ChAT
choline acetyltransferase
Acetylcholine = CH3-C=O-O-CH2-CH2-N(CH3)3
+
Mitochondria Diet
PC
Re-uptake
PC PLD PA + Choline

HO-CH2-CH2-N(CH3)3
CH3-C=O-O-CH2-CH2-N(CH3)3
AChE-OH
AChE-O-C=OCH3H2O
AChE-OH + HO-C=OCH3
Acetylcholine Degradation: acetytlcholiesterase+
+
Acetylated enzyme intermediary
H2O
AChE turnover number: 25,000 molecules/second
Nerve gases, pesticides, and therapeutic drugs

There are two types of cholinesterasesAcetylcholinesterase ( (AChE), also known as RBC cholinesterase, erythrocyte cholinesterase, or (most formally) acetylcholinesterase. It is found primarily in the blood and neural synapses. Acetylcholinesteraseexists in multiple molecular forms. In the mammalian brain the majority of AChE occurs as a tetrameric, G4 form with much smaller amounts of a monomeric G1 (4S) form
Pseudocholinesterase ( (BChE or BuChE), also known as plasma cholinesterase, butyrylcholinesterase, or (most formally) acylcholine acylhydrolase, found primarily in the liver
butyrylcholinesterase
Butyrylcholinesterases are important for the degradation of succinylcholine, a short-acting depolarizing neuromuscular blocking agent used as a muscle relaxant.
AChE

Localization of Acetylcholine in the CNS, PNS, and ANS
Acetylcholine is also present in the autonomic ganglia: pre-ganglionic neurons in sympathetic
ganglia and pre- and post- ganglionic neurons in the parasympathetic system
Acetylcholine is the neurotransmitter in the neuromuscular junction
Central cholinergic neurons are localized in the basal forebrain cholinergic complex, septal nuclei, striatum
and in the dorsal tegmental area (DTA)

Physiology of Cholinergic Transmission

Physiology of Cholinergic Transmission
Acetylcholine receptors (AChRs)
• 2 types:– Nicotinic (nAChR):
1. Agonist: nicotine2. Antagonist: d-tubocurarine
– Muscarinic (mAChR):1. Agonist: muscarine, pilocarpine2. Antagonist: atropine

Nicotinic Receptors• nicotinic receptors are classified as:
– muscle– neuronal
• ligand-gated ion channels: permeable to Na+, K+ and sometimes Ca2+ ions.• pentameric structures that are homomeric or heteromeric combinations of
seventeen (α1-α10, β1-β4, γ, δ,ε) similar, but genetically distinct, subunits.• α4 and β2 are the most abundant nAChR subunits in the brain• nAChRs containing α4β2 subunits are the most abundant high affinity nicotine-
binding nAChRs in the brain and mediate the rewarding and reinforcing effects of nicotine
• neuronal nAChRs are localized both presynaptically (where they regulate the release of several neurotransmitters) and postsynaptically (where they reside extrasynaptically and influence cell excitability)
• The α-subunit constitutes the principal component of the binding site, whereas the adjacent subunit provides the complementary site.
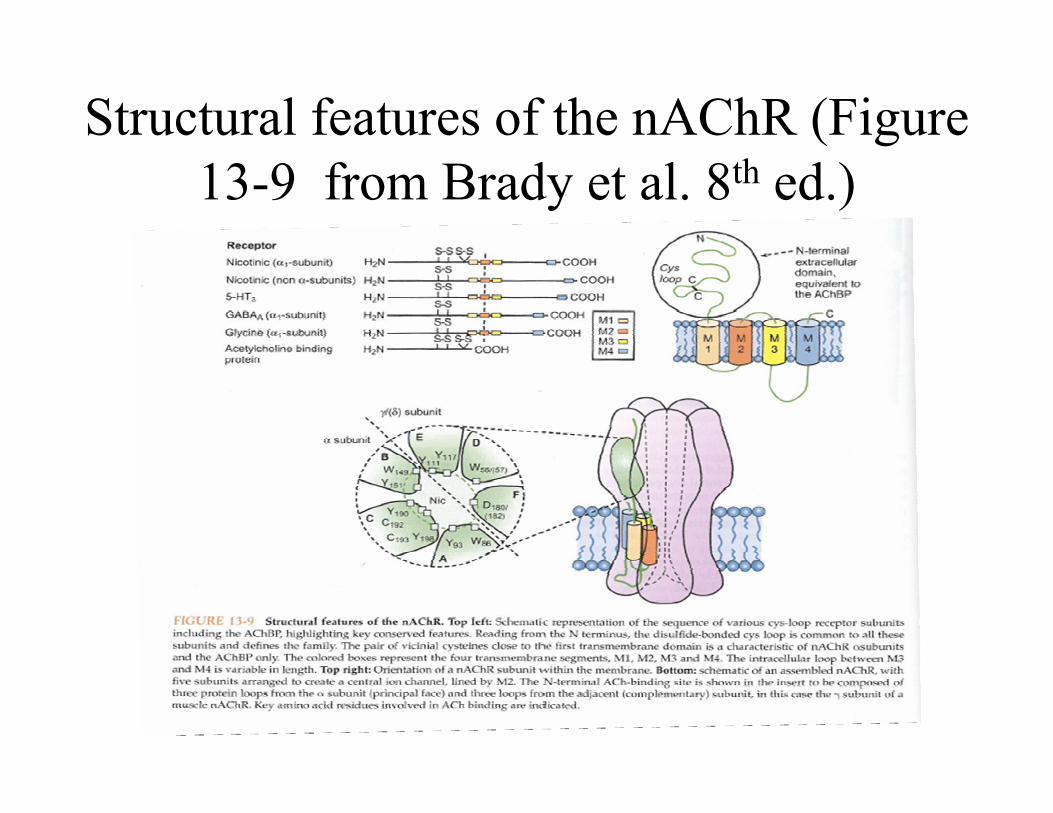
Structural features of the nAChR (Figure 13-9 from Brady et al. 8th ed.)

Cholinergic Receptors

Figure 13-11 from Brady textbook

Nicotinic (ligand-gated channel)
Ach- -ACh
In the neuromuscular junction, the embryonic form of nicotinic receptors is composed of α1, β1, δ, and γ subunits in a 2:1:1:1 ratio, or the adult form composed of α1, β1, δ, and ε subunits in a 2:1:1:1

Toxins affecting Nicotinic receptors

2. Diseases Affecting Transmission at the NMJ
A. Autoimmune Disorders
Myasthenia gravis (MG)
(Ag: nAChR)

Muscarinic (G-protein coupled)

GPCRs• GPCRs all posses a common structure:
1. an extracellular amino terminus2. seven hydrophobic transmembrane (TM) segments3. an intracellular carboxyl terminus.
• The GPCRs can be divided into five families based on sequence similarity within the 7 TM segments:1. the rhodopsin family (~80-90% of all GPCRs, inlcuding the
mAChRs)2. the adhesion family3. the frizzled/taste family4. the glutamate family5. the secretin family
mAChRs in brain• M1 is the predominant form of the mAChR in the CNS; it is found
postsynaptically (principally on dendrites) in the cerebral cortex, hippocampal formation, striatum and thalamus.
• M2 receptors are enriched in the brainstem and thalamus, but are also found in the cerebral cortex, hippocampal formation and striatum. Many M2 are presynaptic- on cholinergic terminals- serve as autoreceptors.
• M3 and M5 are expressed at much lower levels than M1 and M2.• M4 are widely disributed throughout the brain; highest expression in
the striatum, where they regulate DA release.

mAChR antagonists in the treatment of Parkinson’s Disease
• PD is characterized by reduced number of dopaminergic neurons in the substantia nigra.
• This leads to an imbalance in striatal dopaminergic and choliergic NT, which is required for coordinated locomotor control.
• The cholinergic “dominance” is treated using an mAChR antagonist, such as bentropine or trihexyphenidyl.

TABLE 11-2. EFFECTS OF ACETYLCHOLINE (ACh) STIMULATION ON PERIPHERAL TISSUESMediated primarily by Muscarinic receptors
Tissue Effects of AChVasculature (endothelial cells) Release of endothelium-derived relaxing factor
(nitric oxide) and vasodilationEye iris (pupillae sphincter muscle) Contraction and miosisCiliary muscle Contraction and accommodation of lens to near visionSalivary glands and lacrimal glands Secretion—thin and wateryBronchi Constriction, increased secretionsHeart Bradycardia, decreased conduction (atrioventricular block
at high doses), small negative inotropic actionGastrointestinal tract Increased tone, increased gastrointestinal secretions,
relaxation at sphinctersUrinary bladder Contraction of detrusor muscle, relaxation of the sphincterSweat glands Diaphoresis (excessive sweating)Reproductive tract, male ErectionUterus Variable, dependent on hormone influence
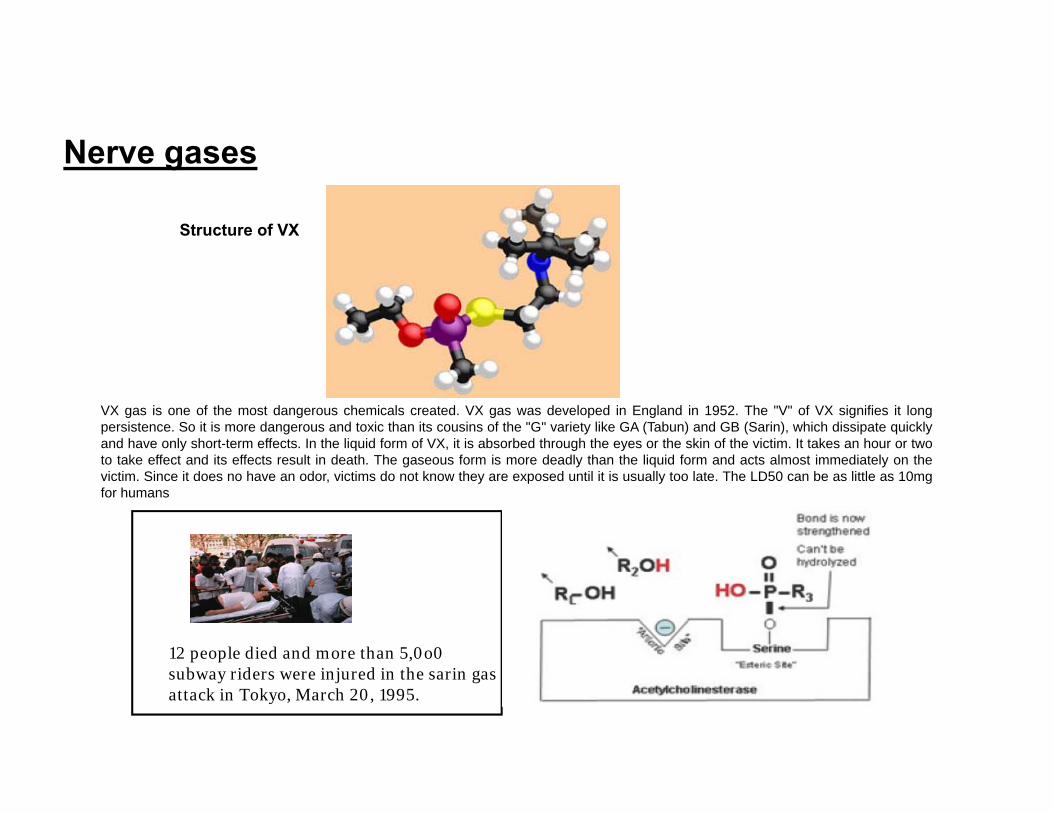
VX gas is one of the most dangerous chemicals created. VX gas was developed in England in 1952. The "V" of VX signifies it longpersistence. So it is more dangerous and toxic than its cousins of the "G" variety like GA (Tabun) and GB (Sarin), which dissipate quicklyand have only short-term effects. In the liquid form of VX, it is absorbed through the eyes or the skin of the victim. It takes an hour or twoto take effect and its effects result in death. The gaseous form is more deadly than the liquid form and acts almost immediately on thevictim. Since it does no have an odor, victims do not know they are exposed until it is usually too late. The LD50 can be as little as 10mgfor humans
Structure of VX
Nerve gases
12 people died and more than 5,0o0 subway riders were injured in the sarin gas attack in Tokyo, March 20, 1995.

Clinical Signs of a Cholinergic Crisis resulting from nerve gas exposure
NMJ (Nicotinic)• Fasciculations, Flaccid paralysis (NMJ)
Parasympathetic NS (Muscarinic AChR)• Bronchospasm• Nausea, vomiting, diarrhea• Miosis, blurring of vision • Hypersecretions of nasopharynx,
trachea, conjunctivae and GI tract • Bradycardia

Mild
People exposed to a low or moderate dose of VX by inhalation, ingestion (swallowing), or skin absorption may experience some or all of the following symptoms within seconds to hours of exposure: Runny nose Watery eyes Small, pinpoint pupils Eye pain Blurred vision Drooling and excessive sweating Cough Chest tightness Rapid breathing Diarrhea Increased urination Confusion Drowsiness Weakness Headache Nausea, vomiting, and/or abdominal pain Slow or fast heart rate Abnormally low or high blood pressure
Moderate• Respiratory distress,wheezing
• Muscle fasciculations• Urinary incontinence• Fecal Incontinence
Treatment of Mild to Moderate Exposure: Atropine
A reversible AChE inhibitor Pyridostigme was also given as protective a agent during First Gulf war

Treatment• 6 mg of atropine by autoinjector• 2 ampules of 600 mg of 2-PAM Cl *
by autoinjector• Diazepam 10 mg IM
*2-Pyridine Aldoxime Methylchloride (Pralidoxime)
Exposure to a large dose of VX by any route may result in these additional health effects: Loss of consciousness Convulsions Paralysis Respiratory failure possibly leading to death
Treatment of Severe Exposure to Nerve gases
Oximes remove agent from enzyme unless aging has occurred
• Aging: agent-enzyme complex changes• T ½ Aging times: Soman 2 minutes, Sarin3-4 hours, others longer

Therapeutic agents affecting ACh function
AChE inhibitors Myasthenia gravis
(reversible) (Pyridostigmine)
Alzheimer’s Disease
(Donezepil and Galantamine)
Pyrid
ostig
min
eG
alan
tam
ine