acknowledgements foreword to the 4th edition resident...1 the resident handbook department of...
TRANSCRIPT

1
The Resident Handbook Department of Anesthesiology
Queen’s University
4th Edition 2008
Dr. Melanie Jaeger Program Director
Department of Anesthesiology Faculty of Medicine Queen’s University
January 2008
ACKNOWLEDGEMENTS Dr. Andrew Klahsen, a resident in the program, started this handbook in the early 1990's. Dr. Steve Shelley, the Program Director, assisted him at that time. Dr. Ted Ashbury produced the 2nd edition in 2000, during his term as Program Director. I revised it again in July 2004 when I took over the role of Program Director. Kim Asselstine, the Postgraduate Program coordinator in Anesthesiology has provided many important contributions since this manual originated in 1999. Their efforts are gratefully acknowledged.
FOREWORD to the 4th Edition
This handbook is intended to provide practical information for residents about the Postgraduate Royal College Program in Anesthesiology, Queen's University, Kingston, Ontario. The information in this book has been compiled over many years and is continually being updated.
All residents have certain expectations about the academic structure of a postgraduate training program. This handbook will help to outline the structure and organization of the academic program in Anesthesiology here at Queen's University. As well, every postgraduate program has a certain service component. It is through meeting the service requirements that residents learn to take responsibility for their actions and develop their skills. This handbook provides a general outline of the expected service commitment.
All components of this handbook will be revised to better reflect the educational experience for residents in the program. Thus, this document is a dynamic one, and always focused on making the Anesthesiology residency the best that it can be.
The Anesthesiology Residency Program at Queen's University complies with the PAIRO contract. The content of this document is subject to this contract and any disagreement between the two should be drawn to the attention of the Chief Resident and the Program Director without delay.

2
Chairman’s Introduction
Welcome to the Residency Program in Anesthesiology here at Queen’s University. The Postgraduate Training Program in Anesthesiology at Queen’s University is a vital component of a dynamic department. Our Department is committed to the goals of providing excellent patient care as well as providing excellent teaching and research activity. The residency program in the Royal College of Physicians and Surgeons (RCPS) training program is designed to achieve these goals. This handbook is a guide to the residents to help them successfully complete the program. The residents initiated the production of this book in the early 1990’s. The success of any academic program is assured when the students take an active role in promoting the learning goals. Residents are encouraged to continue with their constructive input towards making the Queen’s postgraduate Anesthesiology Program the best that it can be. This program will continue to strive to graduate residents who are informed, confident, self-reliant, and competent.
John Cain MD, FRCPC
Head, Department of Anesthesiology Queen’s University
June 2004

3
Short Summary of the Expectations of the Residents in the Postgraduate Anesthesiology Program
at Queen’s University Expectations of the Residents: The academic and service components of the job are intimately intertwined. There are barely 500 days of actual anaesthesia exposure in your PGY2 to PGY5 years when one subtracts holidays, educational leave days as well as the days in medicine and the ICU rotations. Further lessening the experience are the days off before and after call. In Kingston, call is currently only 1:6 to 1:9. It is expected that the residents will quickly demonstrate that they have the attitude and professional sense of responsibility to be capable of becoming the responsible person giving the anesthetic. To this end, the resident will:
see the inpatients or the charts for the next day on the day before surgery – this includes Sundays, so if the resident is unable to see their patients or their charts, they are to make arrangements with the resident on call.
discuss the perceived problems with the staff person if necessary arrive at the OR having read about the case, prepared to discuss the relevant problems recognize that there are patient problems + surgical concerns + anesthesia needs for every case arrive early enough to completely set up (‘early enough’ is 1 hour before “hearts” and big cases, ½ hour before the smaller cases) think about how you want to do the case; confirm with staff person what you want to do, other ideas stay until the case is done (or at least to a reasonable hour); follow cases up, see them the next day see consults promptly answer your pages promptly prepare the anesthesia machines on C5 daily keep the anesthesia emergency pack fully stocked let the staff individual to whom you are responsible know where you are when your time is unstructured.
It is expected that the residents will supplement their practical clinical education by reading all through their training. Residents are expected to be self-directed learners. Residents are expected to read before Core program sessions, and to come to these sessions prepared to discuss cases and ask and answer questions. Attendance at Core is mandatory and expected even when one is pre- or post-call. Residents are expected to attend:
All rounds (Grand Rounds, Case Management rounds, Visiting Professor Rounds) All CME events, even the ones on the weekends!
It is expected that residents will arrange to be ready for the OR at the designated time, even if this means arriving a ½ hour ahead of rounds in order to set up the anesthesia equipment for the day. Residents are expected to ask the staff to fill in their daily evaluations. It is expected that all residents will teach people with less experience (medical students, clinical clerks, junior residents). Daily tracking: residents are to record all cases done in the resident log book. This must be done. Residents are expected to fill in all quarterly evaluation forms, Medicine rotation evaluations, and Program evaluations. Residents are expected to evaluate the staff on a daily basis and in a timely manner. Residents will always ensure that the department has their most up-to-date Email address. This is the most important form of communication.

4
All residents will participate in a research project. These research projects will be presented at the Resident Research Day each spring. Encourage us to teach you and to ask you questions, so we can develop the best program possible. The more questions you ask the more answers you’ll get!
5
TABLE OF CONTENTS
(The page numbers refer to the pages in the paper copy of this handbook.)
ACKNOWLEDGEMENTS………………………………………………………………………. 1 FORWARD………………………………………………….…..……………….………………. 1 CHAIRMAN’S INTRODUCTION……………………………………………..……..…………. 2 SUMMARY OF EXPECTATIONS FOR THE RESIDENTS…………………………………… 3 I. DEPARTMENT OF ANESTHESIOLOGY - QUEEN'S UNIVERSITY
A. Queen's University…………………………………………………………………... 7 B. Health Care Facilities Serviced by Anesthesia………………………………….…… 7
1. Kingston General Hospital…………………………………………….…… 7 2. Hotel Dieu Hospital………………………………………………………… 7
C. Department of Anesthesiology………………………………………………………. 7 1. Department Structure………………………………………………………. 7 2. Anesthetic Services…………………………………………………………. 8
a) Operating Rooms/PAR……………………………………………. 8 b) Pre-Anesthetic Assessment Clinics……………………………….. 8 c) Obstetrical Service………………………………………………… 8 d) Acute Pain Service………………………………………………… 8 e) Chronic Pain Service……………………………………………… 8 f) Arrest & Trauma Service………………………………………….. 8 g) ICU………………………………………………………………… 8
II. RESIDENCY TRAINING PROGRAM
Philosophy & Goals of the Program…………………………………………………. 8 Program Structure
1. Post Graduate Education Committee……………………………………… 8 2. Program Director……………………………………………………….…. 9 3. Residency Positions & Funding…………………………………………... 9 4. Chief Resident…………………………………………………………….. 9 5. Resident Manager…………………………………………………………. 9 6. Resident Mentor…………………………………………………………… 9
Royal College of Physicians and Surgeons of Canada Objectives of Training………………………………………………………….. 10 Specialty Training Requirements………………………………………………. 13 Fellowship Examinations and Preparation……………………………………… 15 Organization of the Educational Program
1. Clinical Training……………………………………………………………. 15 2. Academic Program…………………………………….….……………….. 16
(i) Core Content Sessions…………………………………………….. 16 (ii) Educational Rounds………………………………………………. 19
Weekly Academic Schedule…………………………….…… 19 Grand Rounds………………………………………………… 19 Case Management Rounds…………………………………… 19 Journal Club…………………………………………………. 19
(iii)Resident Research…………………………………………………. 19 Evaluation
1. Evaluations of Resident Performance a) Daily OR Evaluation Criteria and Forms…………….…………… 21 b) Tri-annual Review ………………………………………………… 21 c) Written Examinations …………………………………………….. 21 d) Oral Examinations ……………………………………..…………. 21 e) Case log Review ………………………………………………….. 21 f) Certificate of Completion of Training & FITER …………………. 21 g) Professional Development Assessment Form …………………….. 22
2. Resident Evaluation of Academic Program ………………………………… 22 3. Resident/Staff Liaison Committee Meeting ………………………………… 22

6
Educational Resources 1. Clinical
a) Kingston …………………………………………………………… 23 b) Children's Hospital of Eastern Ontario, Ottawa ………………….. 23 c) Electives ………………………………………………………… 23
2. Research Unit.……………………………………………………………… 23 3. Libraries ……………………………………………………………………… 23 4. Literature Searches ………………………………………………………… 24 5. Computers …………………………………………………………………. 24 6. Presentation Material …………………………………………………………
24 7. Annual Conference Leave …………………………………………………….24
Resident Responsibilities 1. Patient Care ………………………………………………………………………… 24
a) Clinical Competence……………………………………………………….. 24 b) Operating Room Assignments & Responsibilities ………………………… 24 c) Preoperative & Postoperative Assessments…………………………………. 25 d) Patient Care Outside of the Operating Rooms……………………………… 25 e) On Call Coverage & Pagers KGH………………………………………….. 26
i General Comments ii Obstetrical Service iii Trauma Service iv Arrest Service v Acute Pain Service vi Weekend Call vii Assignment of Pagers
f) Consults …………………………………………………………………….. 28 2. Resident Log Book……. …………………………………………………….. 28 3. Scheduling
a) Call Schedule………………………………………………………………. 28 b) Vacations & Statutory Holidays……………………………………………. 28 Vacations Statutory Holidays Christmas & New Years Holidays c) Conference Leave…………………………………………………………… 29 d) Sick Leave………………………………………………………………….. 29
III. QUEEN'S UNIVERSITY POSTGRADUATE EDUCATION POLICIES ………………….. 31 1. Evaluation and Promotion and Appeals 2. Moonlighting Policy 3. Transfers/Crossovers within Postgraduate Medical Education Program 4. Policy on Resident Intimidation and Harassment IV. APPENDIX
Resident Conference Support Resident Block Evaluation Form (completed for some rotations) Resident Evaluation of Program (completed quarterly) Internal Medicine Rotation Evaluation Forms (Cardiology, Respirology, Nephrology) Core Program Evaluation (completed for each seminar)
Resident Daily Evaluation Form Staff Daily Evaluation Form

7
I. DEPARTMENT OF ANESTHESIOLOGY - QUEEN'S UNIVERSITY
A. Queen's University Queen's University is one of the oldest universities in Ontario. An excellent description of the size
of the University, the age of the medical school, and the area serviced by the hospitals can all be found under the Queen's University website. The Queen's University website is http://www.queensu.ca/. For a description of the history of Queen's University this can be found at the following website http://advancement.queensu.ca/html/q_history.
B. Health Care Facilities Serviced by Anesthesiology
1) Kingston General Hospital: The Kingston General Hospital is a multi-programmed hospital consisting of over 300 beds.
Specific surgical services include: thoracic surgery, vascular surgery, cardiac surgery, general surgery, gynecologic surgery, orthopedics, pediatric general surgery, ophthalmologic and ENT surgery, and urology. The hospital also provides a complete tertiary care service in the various medical specialties. There is also a full range of obstetrical services, catering to a wide geographic area. Our residents are members of the trauma team and are therefore commonly called to the Emergency Room to help to manage trauma victims and other patients in whom our expertise at airway management and hemodynamic stabilization are of benefit. Kingston General Hospital is a regional trauma centre and thus a great deal of trauma from the region comes to KGH. The description of Kingston General Hospital on the website can be seen at http://www.kgh.on.ca.
2) Hotel Dieu Hospital: The Hotel Dieu Hospital is an ambulatory care facility. Four to five operating rooms are run daily.
In addition, there is an active Pre-Anesthetic Consult Clinic four days per week and Chronic Pain clinics. A description of the Hotel Dieu Hospital and its mission statement and activities can be found at http://www.hoteldieu.com.
C. Department of Anesthesiology The Department of Anesthesiology has its own web site at www.anesthesia.ca.
1) Department Structure Department Head
Dr. John Cain MD, FRCPC Deputy Chief Academic
Dr. Brian Milne MD, FRCPC Deputy Chief and Clinical Coordinator Dr. Janet VanVlymen, FRCPC Program Director
Dr. Melanie Jaeger MD, FRCPC Family Medicine/Anesthesia Program Director Dr. Brian Mahoney, MD, CCFP Undergraduate Education Coordinator
Dr. Lindsey Patterson MD, FRCPC Continuing Medical Education Coordinator Dr. Kim Turner MD, FRCPC

8
2) Anesthesiology Services
There are a number of services that are provided by the Department of Anesthesiology throughout the hospital. As time goes by, and as the nature of medicine and healthcare changes, different services are added to the spectrum of perioperative care.
a) Operating Rooms/PACU KGH usually has 11 Operating Rooms working on weekdays. Hotel Dieu Hospital has 4-6
Operating Rooms running for outpatient services. During holidays and at times of major anesthesia conferences, the number of operating rooms decreases accordingly. Each operating room is staffed by a member of the faculty of the Queen's University, Department of Anesthesiology. b) Preoperative Assessment Clinics
This is a growing function of the Anesthesiology Department. Currently there are preassessment clinics for orthopedic, vascular, thoracic, and cardiac patients, which are scheduled Monday, Tuesday and Wednesday. Thursdays we have a consultation clinic for a variety of medical problems where Anesthesiology can be consulted prior to their surgery. Residents spend a number of days throughout their training period in these clinics where they learn to assess complicated medical conditions, optimize patients and address anesthetic concerns.
c) Obstetrical Service The Anesthesiology services for the Department of Obstetrics are available 24 hours a day. The
majority of patients receive epidural analgesia during their labour. A consult service is available for complicated obstetrical problems.
d) Acute Pain Management Service Dr. David Goldstein is the medical director of the Acute Pain Management Service. With the
assistance of Rosemary Wilson, our nurse practitioner, we have a very active service. The majority of patients have continuous epidural analgesia or PCEA as well as continuous peripheral nerve catheters. Patients with IVPCA pumps are also followed and monitored on a daily basis. This service is continually expanding as we use newer techniques to achieve better analgesia in the perioperative period.
Coupled with the acute pain service is the regional block experience in which the residents have an opportunity to practice various regional techniques for both pain management as well as the intraoperative management of patients.
e) Chronic Pain Program Dr. Richard Henry coordinates the anesthesia component of this program service along with other
specialists who practice chronic pain and all work together in a multidisciplinary fashion. Residents on this service will experience the opportunity of placing blocks and following patients who have chronic pain problems. This service involves both block and clinic time.
f) Arrest & Trauma Service The Department of Anesthesiology is always on call for cardiac arrests and all traumas. The resident is the focal point of this service and all arrest calls and stat trauma calls are paged directly to the resident on call.
g) ICU There is always at least one resident who is on the ICU rotation. As well, Anesthesiology is on stand by for helping people in the intensive care unit manage difficult airway related problems.
II. RESIDENCY TRAINING PROGRAM Philosophy & Goals of the Program
The primary goal of the training program is to train and prepare residents to become successful consultants and professionals, whether they choose an academic, administrative or community environment. In doing so, we inevitably focus on meeting the requirements of the Royal College Specialty Program in Anesthesiology (see the booklet Goals and Objectives of the Program) and success at the specialty examinations.
Program Structure 1) Residency Training Committee Members of this committee include; Dr. Melanie Jaeger (Program Director), Dr. John Cain (Head),
Dr. Alison Froese, Dr. Ted Ashbury, Dr. Melinda Fleming, Dr. Lindsey Patterson, Dr. Mike Cummings,

9
Dr. Brian Milne, Dr. Susan Haley, and the Chief Resident and a Junior Resident elected by peers. Dr. Brian Mahoney, Dr. Bob Heid (Peterborough) and Dr. Abu Shawan (CHEO) are corresponding members.
2) Program Director
Dr. Melanie Jaeger has been the Program Director since 2003. With the help of the RTC, her function is to oversee the day-to-day operation of the educational component of the residency program. In effect, she is the liaison between the Royal College of Physicians and Surgeons and the residents in the training program. As well, from a departmental point of view, she functions as the resident advocate in all matters relating to maintaining the balance between the service component and the educational component of the program. It is the Program Director's responsibility to ensure that the program meets the standards of the Royal College of Physicians and Surgeons with respect to all of the educational components. This includes setting goal-oriented objectives and setting realistic evaluative techniques to see that residents are meeting those objectives. In order to meet the educational objectives of the program, specific components of the program must be in place. These components include the establishment of educational rounds, such as Core Program, Grand Rounds, and Case Management Rounds. As well Journal Clubs are a part of the educational program. The program is structured around the various objectives of each subspecialty area of anesthesia, which are clearly outlined in the goals and objectives booklet.
The Head of the Department appoints the Program Director to the position. The appointment of the Program Director must be ratified by the Associate Dean of Postgraduate Medical Education at Queen's University. As well the Program Director must be a member in good standing of the Royal College of Physicians and Surgeons of Canada.
3) Residency Positions and Funding Each year the anesthesia residency program will have four PGY 1 positions available. All residents
come to Queen's based on the CaRMS match. The residency training in Anesthesia is a five-year program. In addition, a position may be available yearly via the IMG CaRMS match.
As well there is a Family Practice/Anesthesia program into which two residents per year are accepted. This program has its own program director, separate goals and objectives and evaluative process. It will not be discussed further in this manual.
4) Chief Resident The Postgraduate Education Committee on the recommendation of the Program Director appoints
the Chief Resident. The Chief Resident usually has a six-month to one-year appointment. No more than two Chief Residents are appointed per year, each for six-month terms. There is a stipend that accompanies the appointment of Chief and senior residents for the extra administrative tasks that they must undertake in order to do their job. The Chief Resident is the liaison between the Residency Staff and the Program Director and the Residency Training Committee (RTC). It is the Chief Resident's responsibility to design a working call schedule for the residents. As well, the Chief Resident is responsible for relaying any concerns from the residents to the Program Director and vice versa. In instances where there are conflicts, in call schedule and/or service duties for residents who are off service (e.g. Medicine) rotations, it is expected that the Chief Resident will be able to deal with these situations in the first instance.
5) Resident Manager Each month, a senior resident will be designated as resident manager. It is his/her duty to assign the
residents and medical students to appropriate operating rooms and other anesthetizing locations. Rooms will be allocated based on seniority and educational need. Residents can request certain room allocations if they feel they need more experience in a particular area. Likewise, the resident manager will attempt to ensure that difficult, complicated or rare cases are covered by an appropriate resident. If disagreements regarding room allocations cannot be sorted out between the involved parties, the Program Director will get involved. If the resident manager is unable to assign the rooms due to vacation or leave, he/she must delegate the task to an appropriate resident colleague.
6) Resident Mentors Each resident will be assigned a faculty mentor at the start of their PGY 1 year. This faculty
member is there to guide and support the resident throughout their training. The hope is that each resident feels that they have someone who is there to help them if they need it.

10
The Royal College of Physicians and Surgeons of Canada
OBJECTIVES OF TRAINING AND SPECIALTY TRAINING REQUIREMENTS IN ANESTHESIA
Approved by Education Committee, 2008 (Please see also the green "General Information" booklet.) DEFINITION
Anesthesia is a medical specialty which includes patient assessment and provision of life support, amnesia, and analgesia for both surgical procedures and childbirth; assessment and management of critically ill patients; and the assessment and management of patients with acute and chronic pain.
Contents
GENERAL OBJECTIVES
Upon completion of training, a resident is expected to be a competent specialist anesthesiologist, capable of assuming a consultant's role in the specialty. The resident must acquire a working knowledge of the theoretical basis of the specialty, including its foundations in the basic medical sciences and research. Training must also encompass the provision of anesthesia services for all age groups in varied clinical situations. Performance must, therefore, reflect the anesthesiologist's knowledge of surgery, intensive care and resuscitation, the management of acute and chronic pain and includes assessment and provision of appropriate care of the mother and neonate in obstetrics. The resident must demonstrate a thorough knowledge of how perioperative management should be modified in the presence of concurrent medical problems.
The resident must also demonstrate the knowledge, skills and attitudes relating to gender, culture and ethnicity pertinent to Anesthesia. In addition, all residents must demonstrate an ability to incorporate gender, cultural and ethnic perspectives in research methodology, data presentation and analysis.
Contents
CanMeds Competencies --LINK to http://rcpsc.medical.org/canmeds/bestpractices/framework_e.pdf
2005
Specifically for Anesthesiology, at the completion of training, the resident will have acquired the following competencies and will function effectively as:
Medical Expert
General Requirements
o Demonstrate diagnostic and therapeutic skills for ethical and effective patient care.
o Access and apply relevant information to clinical practice.
o Demonstrate effective consultation services with respect to patient care, education and legal opinions.
Specific Requirements
o Demonstrate knowledge of the basic sciences as applicable to anesthesia, including anatomy, physiology, pharmacology, biochemistry and physics.
o Demonstrate knowledge of general internal medicine with particular reference to the cardiovascular, respiratory, renal, hepatic, endocrine, hematologic and neurologic systems.

11
o Demonstrate knowledge of age related variables in medicine as they apply to neonatal, pediatric, adult and geriatric patient care.
o Demonstrate knowledge of the principles and practice of anesthesia as they apply to patient support during surgery or obstetrics.
o Demonstrate clinical skills necessary for basic resuscitation and life support as practiced in critical care facilities.
o Demonstrate knowledge of the principles of management of patients with acute and chronic pain.
o Demonstrate knowledge of the role of the consultant anesthesiologist in the provision of safe anesthetic services within both community and teaching facilities.
o Demonstrate clinical skills necessary for the independent practice of anesthesia, including preoperative assessment, intraoperative support and postoperative management of patients of any physical status, all ages and for all commonly performed surgical and obstetrical procedures.
o Demonstrate clinical skills necessary to general internal medicine and intensive care including the ability to investigate, diagnose, and manage appropriately factors that influence a patient's medical and surgical care.
o Recognize that prior to provision of anesthetic care specific medical intervention and modification of risk factors may be required.
o Demonstrate competence in all technical procedures commonly employed in anesthetic practice, including airway management, cardiovascular resuscitation, patient monitoring and life support, general, and regional anesthetic and analgesic techniques and postoperative care.
o Demonstrate knowledge of basic legal and bioethical issues encountered in anesthetic practice including informed consent.
Communicator General Requirements
o Establish a professional relationship with patients and families.
o Obtain and collate relevant history from patients, and families.
o Listen effectively.
o Discuss appropriate information with patients and families and other members of the health care team.
Specific Requirements
o Demonstrate consideration and compassion in communicating with patients and families.
o Provide accurate information appropriate to the clinical situation.
o Communicate effectively with medical colleagues, nurses, and paramedical personnel in inpatient, outpatient, and operating room environments.
o Demonstrate appropriate oral and written communication skills.
o Ensure adequate information has been provided to the patient prior to undertaking invasive procedures.
Collaborator General Requirements
o Consult effectively with other physicians and health care professionals.

12
o Contribute effectively to other interdisciplinary team activities.
Specific Requirements
o Demonstrate ability to function in the clinical environment using the full abilities of all team members.
Manager General Requirements
o Utilize personal resources effectively in order to balance patient care, continuing education, and personal activities.
o Allocate finite health care resources wisely.
o Work effectively and efficiently in a health care organization.
o Utilize information technology to optimize patient care, and life long learning.
Specific Requirements
o Demonstrate knowledge of the management of operating rooms.
o Demonstrate knowledge of the contributors to anesthetic expenditures.
o Demonstrate knowledge of the guidelines concerning anesthetic practice and equipment in Canada.
o Record appropriate information for anesthetics and consultations provided.
o Demonstrate principles of quality assurance, and be able to conduct morbidity and mortality reviews.
Health Advocate General Requirements
o Identify the important determinants of health affecting patients.
o Contribute effectively to improved health of patients and communities.
o Recognize and respond to those issues where advocacy is appropriate.
Specific Requirements
o Provide direction to hospital administrators regarding compliance with national practice guidelines and equipment standards for anesthesia.
o Recognize the opportunities for anesthesiologists to advocate for resources for chronic pain management, emerging medical technologies and new health care practices in general.
Scholar General Requirements
o Develop, implement, and monitor a personal continuing education strategy.
o Critically appraise sources of medical information.
o Facilitate learning of patients, students, and other health professionals.
o Contribute to the development of new knowledge.
Specific Requirements
o Develop criteria for evaluating the anesthetic literature.
o Critically assess the literature using these criteria.
o Describe the principles of good research.
o Using these principles, judge whether a research project is properly designed.

13
Professional General Requirements
o Deliver highest quality care with integrity, honesty and compassion.
o Exhibit appropriate personal and interpersonal professional behaviours.
o Practice medicine ethically consistent with the obligations of a physician.
Specific Requirements
o Periodically review his/her own personal and professional performance against national standards.
o Include the patient in discussions concerning appropriate diagnostic and management procedures.
o Respect the opinions of fellow consultants and referring physicians in the management of patient problems and be willing to provide means whereby differences of opinion can be discussed and resolved.
o Show recognition of limits of personal skill and knowledge by appropriately consulting other physicians and paramedical personnel when caring for the patient.
o Establish a pattern of continuing development of personal clinical skills and knowledge through medical education.
Specialty Training Requirements
The purpose of the training required under Section 1 of the training requirements is to introduce and expose the resident to independent responsibility for decisions involving clinical judgment skills; the further development of an effective and mature physician-patient relationship; and the achievement of competence in primary technical skills across a broad range of medical practice, and an understanding of the nature of the relationships between a referring physician and consultant clinical anesthesiologist. Five years of approved residency training. This period must include:
1. One year of basic clinical training, which must be completed before Section 2 training begins. Training done during this year can be credited only under Section 1.
2. Four years of approved training. This period must include:
a. two and a half years (30 months) of approved resident training in anesthesia. This period is designated as the primary training for the science and clinical practice of anesthesia; required elements of the training must therefore reflect the need to diversify the experience to enable the resident to fulfill the consultant role. The following minimum required elements of training may be undertaken as separate rotations, or interspersed with one another, provided that it can be demonstrated that experience fulfilling the minimum requirements has been obtained:
i. adult anesthesia (12 months minimum) - including experience in out-patient surgical management, recognized general and subspecialty surgical procedures, and associated emergency conditions; an appropriate combination of general and regional anesthetic experience must be demonstrable;
ii. pediatric anesthesia (3 months minimum);
iii. obstetrical anesthesia (2 months minimum);
iv. chronic pain management (1 month minimum) incorporating experience in long-term care.
b. one year of approved resident training in general internal medicine, to be undertaken preferably after a year of clinical training in anesthesia. This year, in conjunction with the basic clinical training, is designed to allow the resident to achieve primary skills across a broad range of medical practice; to develop a mature and effective physician-patient

14
relationship; to acquire the general medical knowledge necessary to function as a competent consultant in anesthesia. Therefore, this year must include:
i. at east six months of approved resident training in adult internal medicine. Rotations eligible for credit include general internal medicine and/or any combination of experience in at least two of the following subspecialties: cardiology, coronary care, respirology, neurology, hematology, nephrology, endocrinology, and infectious diseases;
ii. at least three months of approved resident training in adult intensive care. In addition, it is strongly recommended that the acute care experience include broader elements, such as neonatal/pediatric ICU, coronary care and emergency medicine. A maximum of six months I.C.U. experience is allowed under this section;
iii. up to six months of research done in an approved centre may also be acceptable for credit in this section, where special arrangements have been made to include intensive care training under Section 2(a). [Please see NOTE on Research or Clinical Pharmacology after Section 2(c)iii.];
iv. up to six months of training in an accredited clinical pharmacology program during the final residency year may be credited under this section, when special arrangements have been made to include intensive care training under Section 2(a) [Please see Note under 2(c).].
c. six months of training that may include:
i. further training in an approved anesthesia program;
ii. research experience in a clinical or basic science department approved by the Royal College;
iii. six months training in clinical pharmacology undertaken in an accredited program during the final residency year.
Research or Clinical Pharmacology In appropriate circumstances and upon the recommendation of the program director, to facilitate a one-year commitment to either an approved research program or an accredited Clinical Pharmacology program, three months of ICU training may be taken under 2(a) of the above requirements. The six months of research or clinical pharmacology training permitted under sections 2(b)iii, and 2(c)ii for research, and 2(b)iv and 2(c)iii for clinical pharmacology allows the option of a full year of research or clinical pharmacology within the limitations of the training requirements.
iv. any other course of study and training relevant to the objectives of anesthesia and acceptable to the director of the training program and the Royal College.
The purpose of this period is to develop subspecialty interests, diversify the resident's experience, or address deficiencies in earlier training.
NOTE: Those who have completed four years residency in Anesthesia in a non RCPSC program within a system that has been deemed acceptable to the RCPSC and within acceptable time frames and have:
i. been in a continuous practice of Anesthesia for one or more years post certification and
ii. maintained continuous enrolment with their certifying authority may fulfill the requirements for Section 2 (b) with one of the following options:
1. additional critical care training, to a maximum of 12 months,
2. acceptable training in Pediatrics at a senior level to a maximum of six months credit,

15
3. one year of other post graduate clinical training (as outlined in the Policies and Procedures for Certification and Fellowship under Section IV, Part 1.2.2) in Anesthesia,
4. an additional year of acceptable Anesthesia specialty practice.
Editorial revision May 2003 Contents RCPS Examination preparation: Preparation for taking the RCPS examinations in the PGY5 year begins in the PGY1 year. Residents are encouraged to study consistently throughout the residency program. Such consistent reading in preparation for cases, as well as preparation for core program, grand rounds, and case management rounds generally ensures that residents will acquire the knowledge necessary to write the RCPS exams. Further preparation and evaluation occurs during oral exams conducted three times per year plus substantially more practice oral exams in the PGY5 year, particularly in the last 6 months prior to the oral exam. The written exam consists of multiple choice and short answer questions. Residents prepare for these exams by reading from the 11 or 12 approved textbooks from which all exam questions are taken. The oral exams are based on questions that come from 12 domains in Anesthesiology. These domains are well known, however the format of the questions continues to evolve over the years. Residents have all felt well prepared to take the oral exams in the past several years.
Organization of the Educational Program
The residency program in Anesthesia can be divided into clinical and academic streams. The academic stream consists of Core Content Sessions, Grand Rounds, Case Management Rounds, Resident Research Day and Journal Club. The Clinical Training is scheduled throughout the entire year.
1) Clinical Training The practical clinical experience for residents within the Department of Anesthesiology in the
PGY2-5 years occurs on daily basis in the OR, the obstetrical unit or the consult clinic. Some subspecialty areas are structured as a block rotation (cardiac, obstetrics, chronic pain), while others occur throughout the training in a less structured format that more reflects actual practice. Each subspecialty area has an assigned coordinator who is responsible to oversee the experience, whether or not it is accomplished in a block rotation or in a more continuous horizontal fashion. These coordinators are responsible for developing appropriate objectives and evaluation. The following table contains a summary of the subspecialty areas and the clinical block in which they occur. Objectives for each subspecialty area are located in the Goals and Objectives book.
The required off-service rotations are scheduled in throughout the PGY3-5 years. This consists of a total of 6 months of internal medicine and 6 months of ICU (5 adult and 1 neonatal). There is also 6 months of elective time during which the resident can arrange to work in other centers and in various subspecialties.

16
Clinical Anesthesia Subspecialty Coordinators
Code Subspecialty Coordinator Block Duration/yr
Cardiac Dr. M. Cummings CARDIAC 1 month PGY2/3, 1month PGY 4/5
Vascular Dr. R. Allard KGH PGY3-5 Thoracic Dr. M. Fleming KGH PGY3-5 Neurosurgery Dr. B. Simchison KGH PGY3-5 Obstetrics Dr. S. Haley OB 1 month
PGY2, 1month PGY5
Orthopaedics, Trauma, Burns, Plastic Surgery
Dr. Melanie Jaeger Dr. M. McMullin
KGH PGY2/3
Chronic Pain Dr. R. Henry CHRONIC PAIN
1-2 months PGY3-5
General Surgery Dr. D. Engen KGH PGY2/3 Urology Dr. A. Froese KGH PGY2/3 Acute Pain/ Regional Dr. D. Goldstein APS PGY 2-5 Preassessment Clinics Dr. J. vanVlymen PAC PGY2-5 Gynecology Dr. S. Duggan KGH PGY 2-4 Elective Various KGH 1-4 months HDH Ambulatory,
ENT, Ophthalmology Dr. L. Patterson HDH 1-2 months
CHEO* Paediatrics Dr. Ibrahim Said CHEO 3 months AIRWAY
Dr. R. Zamora
KGH
1 month PGY2
* Children's Hospital of Eastern Ontario, Ottawa, Ontario
2) Academic Program (i)Core Content Sessions
The academic content of the program is to be covered by a series of weekly teaching sessions from September through June of each year. The sessions are presented in a two-year cycle. The sessions are currently scheduled to be held every Wednesday afternoon from 1230h till 1530h. Staff are assigned to present specific topics during these sessions. They are to provide and distribute objectives and a detailed reading list for each session at least one week prior to the assigned date. There may also be a resident assigned to research and present a particular topic related to the session; resident participation varies depending on the session. Residents are expected to prepare for the sessions in advance. The teaching style in the individual sessions will vary depending on the staff person involved. A mechanism of resident feedback will be provided to assist staff presenters in maximizing the effectiveness of their sessions. (see Appendix iv)
Resident attendance at Core Program Seminars is expected unless the resident is on vacation, conference leave or sick leave. Internal medicine rotations should allow the resident to attend
these seminars
17
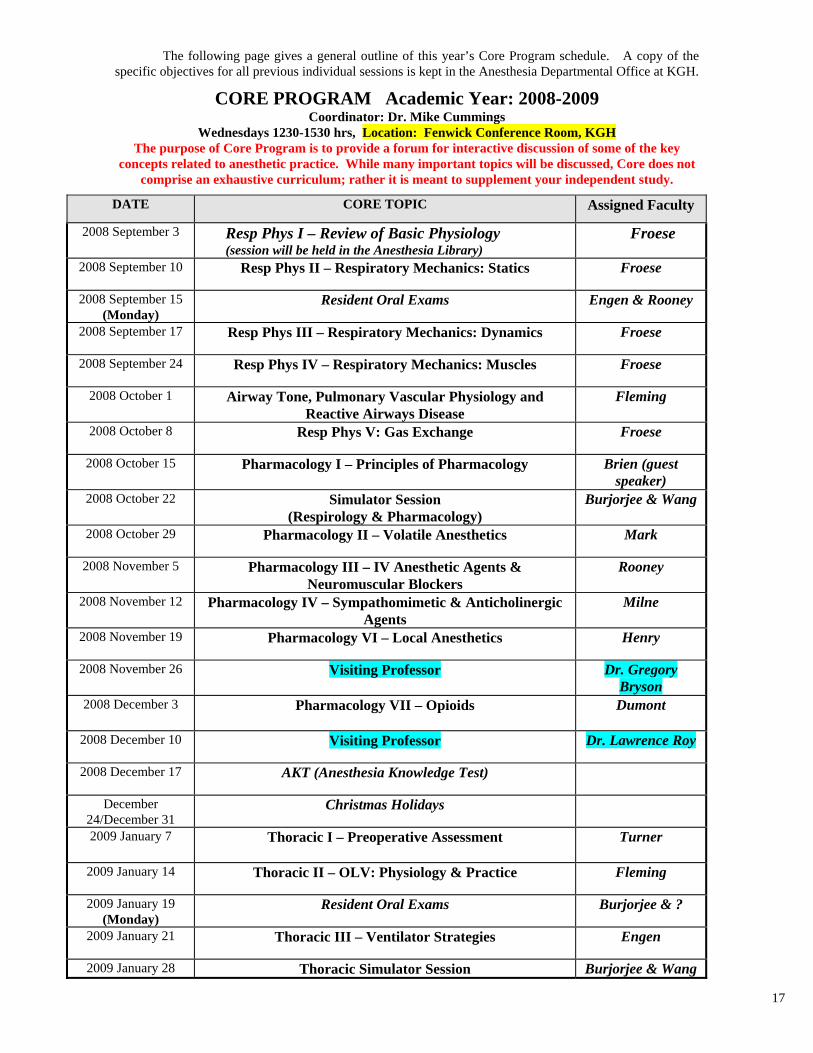
The following page gives a general outline of this year’s Core Program schedule. A copy of the specific objectives for all previous individual sessions is kept in the Anesthesia Departmental Office at KGH.
CORE PROGRAM Academic Year: 2008-2009 Coordinator: Dr. Mike Cummings
Wednesdays 1230-1530 hrs, Location: Fenwick Conference Room, KGH The purpose of Core Program is to provide a forum for interactive discussion of some of the key
concepts related to anesthetic practice. While many important topics will be discussed, Core does not comprise an exhaustive curriculum; rather it is meant to supplement your independent study.
DATE CORE TOPIC Assigned Faculty
2008 September 3
Resp Phys I – Review of Basic Physiology (session will be held in the Anesthesia Library)
Froese
2008 September 10
Resp Phys II – Respiratory Mechanics: Statics Froese
2008 September 15 (Monday)
Resident Oral Exams Engen & Rooney
2008 September 17
Resp Phys III – Respiratory Mechanics: Dynamics Froese
2008 September 24
Resp Phys IV – Respiratory Mechanics: Muscles Froese
2008 October 1
Airway Tone, Pulmonary Vascular Physiology and Reactive Airways Disease
Fleming
2008 October 8
Resp Phys V: Gas Exchange Froese
2008 October 15 Pharmacology I – Principles of Pharmacology
Brien (guest speaker)
2008 October 22
Simulator Session (Respirology & Pharmacology)
Burjorjee & Wang
2008 October 29
Pharmacology II – Volatile Anesthetics Mark
2008 November 5
Pharmacology III – IV Anesthetic Agents & Neuromuscular Blockers
Rooney
2008 November 12
Pharmacology IV – Sympathomimetic & Anticholinergic Agents
Milne
2008 November 19
Pharmacology VI – Local Anesthetics Henry
2008 November 26
Visiting Professor
Dr. Gregory Bryson
2008 December 3 Pharmacology VII – Opioids
Dumont
2008 December 10
Visiting Professor Dr. Lawrence Roy
2008 December 17
AKT (Anesthesia Knowledge Test)
December 24/December 31
Christmas Holidays
2009 January 7
Thoracic I – Preoperative Assessment
Turner
2009 January 14
Thoracic II – OLV: Physiology & Practice Fleming
2009 January 19 (Monday)
Resident Oral Exams Burjorjee & ?
2009 January 21
Thoracic III – Ventilator Strategies Engen
2009 January 28 Thoracic Simulator Session Burjorjee & Wang

18
DATE CORE TOPIC Assigned Faculty
2009 February 4
Cardiac I – Review of Cardiovascular Physiology Parlow
2009 February 9 (Monday)
Cardiac II – Cardiopulmonary Bypass & Hypothermia Saha
CaRMS Interviews: February 10 – 13, 2009
2009 February 18
Cardiac III – Intraoperative Monitoring Cummings
2009 February 25 Cardiac IV - Cardiomyopathies
Mark
2009 March 4
Cardiac V – Valvular Heart Arellano
2009 March 11
Cardiac VI – EP, Arrhythmias & Devices Simpson
2009 March 18 March Break - cancelled 2009 March 25 Cardiac VII – Circulatory Failure & Shock Arellano
2009 March 27 (Friday)
Resident Research Day
2009 April 1
Cardiac VIII – Preoperative Assessment and Management of Patients with Cardiac Disease
Tanzola
2009 April 8
Cardiac IX – CVICU: The Postop Heart Allard
2009 April 15
Simulator Session (Cardiac)
Burjorjee & Wang
2009 April 22
Obs I – Physiology and Pharmacology of the Pregnant Patient
Haley
2009 April 29
Obs II – Obstetrical Anesthesia & Analgesia Cummings
2009 May 6 Obs III – Maternal Disease and Pregnancy Patterson
2009 May 13 Resident Oral Exams (Guest Oral Examiner)
?
2009 May 20
Obs IV – Labour Issues Turner
2009 May 25 (Monday)
Simulator Session (Obstetrics)
Burjorjee & Wang
2009 May 27
Obs V – Obstetrical Complications Murdoch
2009 June 3
Patient Safety: Complications of Anesthesia Goldstein
2009 June 10
Legal Aspects of Anesthesia CMPA Guest
2009 June 17 Biostatistics & Critical Appraisal
VanDenKerkhof
2009 June 24 REVISED – 2008 Nov 20
19
Anesthesiology Residency Simulation Program
Overview: The simulation program for anesthesia residents at Queen’s University has been up and running with regular sessions occurring since May 2006. We are committed to using this new technology to provide excellent educational sessions for our residents in a fun, safe & protected learning environment. Sessions are designed specifically for our residents to practice identifying and responding to crises, to develop team and communication skills, and to handle challenging scenarios and practice decision making. Each simulation is followed by a group debriefing to maximize the learning from each session. It is in this way that the simulation program offers the residents a unique opportunity to apply & practice implementing their knowledge in a safe environment without compromising patient care. Introduction to the HDH Simulation Lab: The high fidelity simulator is located at the HDH just across from the surgical suites. The mannequin is set up on an OR table in the renovated OR suite with a functioning anesthesia machine including ventilator and monitoring capabilities. With the drapes up and the monitor beeping in the background we have had many people believing that a real patient was in the room. There is a separate small room for the operator of the computer that runs the simulator as well as for the video equipment. Another room just down the hall allows students to watch and hear what is happening in the simulator room in real time or to review the session for debriefing purposes from multiple different camera angles. Our anesthesia supplies are accumulating and include a difficult airway equipment and a resuscitation cart. Our simulator is a state of the art high fidelity simulator (Human Patient Simulator model) made by the company METI specifically for the purpose of medical education. The simulator is driven by sophisticated models of human physiology and pharmacology that automatically determine the ‘patient’s’ response to the students’ actions and interventions. We have an adult and a pediatric mannequin that can be used at the site and may also have access to an infant in the future. The clinical features of the mannequins include heart and breath sounds, palpable pulses and chest excursion with generated end tidal CO2, cardiac rhythm & oxygen saturation; all of which correlate with the clinical conditions of the patient. Invasive and non-invasive monitoring is possible. The airway is anatomically realistic and allows for various methods of intubation, as well as simulation of the difficult airway through tongue swelling, airway swelling and laryngospasm. A simulated cricothyroid membrane can allow for emergency surgical airway access. The pulmonary system allows for spontaneous or mechanical ventilation and multiple physiologic parameters can be altered to reproduce the patient with atelectasis, pneumothorax, asthma or COPD. Similarly the cardiac system generates appropriate heart sounds, an appropriate ECG for the scenario as well abnormalities such as ischemia or arrhythmias. Trauma features include the ability to do pericardiocentesis and decompression of a tension pneumothorax via needle or chest tube. The drug recognition system identifies drugs given by the students through a barcode reader and has pharmacokinetic and dynamic modeling for 50 intravenous drugs.
Although the mannequin for our simulator often looks the same, the simulator can act like almost any patient; from the frail elderly hypovolemic granny to the robust healthy teenager. Almost any scenario can occur from common problems such as hypotension from hypovolemia or sympathectomy, high airway pressures and desaturation to full blown anaphylaxis and MH. There is the potential for designing a scenario to meet almost any educational goals that you may have.
We welcome you to the anesthesia simulator program and look forward to your participation.
Dr. Jessica E. Burjorjee Dr. Louie Wang
20
(ii) Educational Rounds Resident attendance at the following rounds is mandatory unless the resident is on vacation, conference leave, sick leave, or off service. Residents are expected to attend rounds on time. Those who are off service are encouraged to attend if time permits. Weekly Academic Schedule: Monday: Wednesday: 0700-0750 Grand Rounds 1230-1530 Core Program Thursday: 1800-1900 Journal Club (6 times per year) Friday: 0700-0745 Case Management Rounds
Grand Rounds Grand Rounds for the Department of Anesthesiology are held every Wednesday morning at 0700
for the months of September through June in the Richardson Amphitheatre. These rounds will be presented by residents, staff and visiting professors. Each resident will be expected to present on a yearly basis. In addition, residents may be asked to present at Morbidity and Mortality Rounds. There are 3-4 spots reserved for Morbidity/Mortality or Trauma Rounds. (Trauma Rounds are held in Etherington Hall at KGH starting at 0730).
Case Management Rounds Case Management Rounds (formerly known as “Problem Rounds”) are held once per week
throughout the entire year. These are rounds that involve case presentations by a resident, but the exact format may vary over the years. Staff attendance is encouraged to provide feedback on the problem presented. Cases presented will be of general interest and posted a few days prior to the Friday.
Journal Club This is held approximately 6 times per year. Two to three articles are chosen by an assigned staff
member and are presented by that staff member and an assigned resident. The articles should be chosen for an interesting and/or controversial viewpoint and be made available to the departmental secretaries at KGH at least two weeks in advance to permit sufficient time for distributing copies. Presentations for each article should be 10-15 min in length and include a brief synopsis of the study, a critical appraisal of the design and a discussion of the issues relevant to the current practice of Anesthesia. An open discussion of the respective article will follow each presentation.
(iii) Resident Research
Dr. Ian Gilron is the coordinator for Resident Research. His wealth of knowledge and expertise in research helps to guide the residents and make research a fulfilling educational experience. All residents are expected to get involved with research at some level. The following is an outline of how research will be conducted by residents…this is an outline only and is meant to guide you. Deviations from this outline will be expected PGY-1 • Residents will be given times/locations of mandatory research course. Until further notice, this will be Dr. Bob Reid's course (http://meds.queensu.ca/medicine/obgyn/research/course2003.htm) • Depending on the 2-year Core Lecture cycle, some years, PGY-1s will also attend Core Lecture on the critical appraisal of research literature. • Residents will be required to critically appraise a published research data article relevant to the specialty of Anesthesiology. • There will be a PGY-1 award for "Best Critical Appraisal Essay" which will be published in the Resident Research Day syllabus

21
PGY-2 • Resident to submit to Residency Program Director (RPD) 2 one-page preliminary proposal summaries for two possible research projects (with the heading format: clinical need, knowledge gap, hypothesis, study design, pitfalls/feasibility/project timeline). These proposals will be reviewed by the RRC and only one will be approved (by October 15) for the Resident to write a full proposal on. • For the proposed project, the research area is flexible (could be laboratory, clinical, survey, epidemiological etc.) but the research question should be relevant to anesthesia, critical care and/or pain management. PGY-2, February 1: • submit full research proposal to RPD (for review by the RRC) and present this proposal as an oral communication at Grand Rounds in the month of February • incorporate feedback from RRC (and from Departmental comments at rounds) in order to improve their proposal for Resident Research Day PGY-2, March: • present research proposal at Resident Research Day. One Resident will be awarded prize for best research proposal. PGY-2, April 1: •start to carry out research plan, e.g. Ethics submission, data recording instruments, patient recruitment etc. with the help from staff advisor PGY-3/4 • abstract submission to CAS Meeting resident competition PGY-3/4, March: • project presentation at Resident Research Day; Gold, Silver and Bronze medals for top 3 project presentations PGY-4, June • research manuscript is submitted to peer-reviewed journal. If the manuscript is not appropriate for a peer-reviewed journal, hopefully it could be published in some other venue (e.g. "NARQ", Queen's Health Sciences Journal etc.) PGY-5: • research is forbidden, must study for FRCPC exams!!!
Annual Resident Research Day A resident research day is held every spring. As outlined above, residents will present a research proposal in PGY2 and ideally a finished product in PGY3 or 4.

22
Evaluation 1) Evaluation of Resident Performance
a) Daily OR Evaluation Criteria and Forms Staff persons should complete individual resident evaluations on a daily basis. It is expected that
the resident will encourage the staff person to fill out the evaluation form each day. The results of this will be compiled by the Program Director and discussed with the resident during the review of the resident’s performance every three or four months (see “b”, page 26, below). The form that is filled out by the faculty member is confidential. It is the means of communication that the faculty member uses to inform the Program Director about the resident’s performance on that day.
The most important part of the daily evaluations is the feedback that the staff individual gives to the resident at the end of the day. This feedback should give the resident basically the same information that is communicated to the Program Director on the daily evaluation form. Residents should seek out this feedback. Faculty members know that part of their daily responsibility is to give this feedback.
b) Tri-annual Review
Residents will meet with the Program Director three to four times per year. This will provide opportunity to review the resident's performance based on written and oral examinations, individual staff evaluations and the resident's Log Book (see below). It should also be used to confirm that the resident is meeting his or her educational goals, both personal and departmental (i.e. Resident Research Day). Either party may initiate additional meetings if specific concerns are identified which require more frequent review. Residents are encouraged to seek out the Program Director as soon as possible when issues arise to allow timely intervention. The benefits of having a small program include an “open door” policy between staff/PD and residents.
c) Written Examinations
AKT
Residents are required to write the Anesthesia Knowledge Test (AKT) at 4 points throughout their training; on day 1 and 30 of their first month, after 6 months, and in PGY4/5. This exam will be evaluated and results will be normalized against many other US and Canadian residents.
d) Oral Examinations
An oral examination in September, February and May will be given to each resident. It will be in the same format as the FRCP oral examinations. The exam will be graded in the same fashion as the RCPC oral examinations. There will be an external examiner for the oral examinations in the spring. All residents are expected to take the oral examination. All residents will receive oral and written feedback on their performance.
e) Resident Log Book
It is mandatory that each resident maintain a current log of all of the anesthetic interventions which he or she has performed.
Residents will keep a record of all the cases in which they have significant involvement. They will record these cases on the web. Instructions for how to access the Resident Log Book (RLB) Program will be given to each resident during their first rotation in Anesthesiology during the PGY1 year. The use of this RLB program is required for every Anesthesiology resident in the country and allows cross program comparisons.
f) Certificate of Completion of Training & FITER
A Certificate of Completion of Training and a Final In-Training Evaluation Report (FITER) will be completed near the end of the residency program by the Program Director. The Royal College of Physicians

23
and Surgeons requires these before the resident will be allowed the opportunity to take the College examinations. A copy of the FITER can be obtained from Kim Asselstine.
g) Deadlines for Applications for Royal College Exams
It is very important that you are aware of the Royal College application deadlines for your exams. It is the resident’s responsibility to contact the Royal College in their PGY4 year in order to meet any necessary deadlines for the resident Royal College exams in PGY5 year. You are encouraged to submit your application early. You will need to determine the following:
- deadline for notifying the Royal College that you will be sitting the Royal College exams - deadline for fee and submitting a request for a preliminary assessment of training - deadline for submitting examination application and fees There is a penalty fee for late applications and there is no guarantee that you will be able to sit the exams if you submit your application late. For further details, the Royal College website is: www.rcpsc.medical.org.
2) Resident Evaluation of the Academic Program Residents are encouraged to provide feedback to the Program Director and the Postgraduate Education
Committee about all aspects of the training program. Various forms have been developed to facilitate this feedback. Residents are encouraged to provide thoughtful, constructively critical feedback about the program at any time. Evaluations will be done in the following areas. (see appendices for forms)
Clinical Block Evaluation Form – for certain rotations (Community Anesthesia, Peterborough) Program Evaluation Form (completed quarterly) Core Program Evaluation Form - used to evaluate each seminar Internal Medicine Rotation Evaluation Forms (Cardiology, Respirology, Nephrology) Faculty Teaching Evaluation Form
Residents are expected to evaluate the staff on a daily basis just as they are evaluated. This is done on a web-based program and can be done at the same time one is entering their data on the RLB. This will provide specific feedback on the role of each staff person and their effectiveness as a clinical teacher. The information obtained from this form will be compiled with no reference to any resident and is completely confidential. The Department Head will review a graphical printout summary for each staff. The evaluation will become a permanent part of the staff person's record at Queen's University.
Annual Award for "Teacher of the Year"
At the end of each academic year, residents will vote for the staff person that has been the best overall teacher for the past year. The Chief Resident will make a formal acknowledgment to the winner of the award at the annual Resident Research Day.
3) Resident/Staff Liaison Committee Meeting Resident attendance at this meeting is mandatory unless the resident is on vacation, conference leave, sick leave, or off service.
Meetings between the residents, the Program Director and the Department Head are to be scheduled by the Chief Resident. These meetings should be held at least every three to six months. These meetings are to provide both parties with the opportunity to raise concerns and issues regarding the residency program in an open forum. An itinerary of topics to be discussed is to be distributed at least one week in advance by the Chief Resident.

24
Educational Resources
1) Clinical a) Kingston The clinical experience in anesthesia at Queen's University is provided at both the Kingston General
Hospital and the Hotel Dieu Hospital. See section on "Department of Anesthesiology, Queen's University-Health Care Facilities Serviced by Anesthesia" for more detail.
b) Children's Hospital of Eastern Ontario, Ottawa Residents in the Queen's University Residency training program in Anesthesia must spend three months
in an accredited Pediatric Hospital for pediatric anesthesia. Queen's has a formal arrangement with the Children's Hospital of Eastern Ontario (CHEO) http://www.cheo.on.ca such that residents have accommodation provided in CHEO House while doing their pediatric anesthesia rotation in Ottawa. Residents may choose to do their 3-month pediatric anesthesia elective in another location (eg. Hospital for Sick Children in Toronto). Arrangements for alternate rotations must be made by the resident and approved by the Program Director.
c) Peterborough Residents have a one month rotation in Peterborough to give them an opportunity to work in a
community setting. Accommodations are provided. b) Electives
Up to six months of anesthesia related elective time may be set aside for straight FRCP residents if their clinical performance is considered adequate. An application may be made to use any allotted elective time outside of Queen's University in an approved setting. Electives can be arranged in third world settings with Dr. Alison Froese. She has years of experience providing developing areas with anesthetic services and can take interested residents on certain missions. Any such requests should be made to the Program Director by April for the upcoming academic year beginning in July.
2) Research Unit
Queen’s University has a Clinical Research Unit at KGH. The Clinical Research Center (CRC) is available to assist residents with the design, conduct and analysis of their clinical research. They offer a wide range of:
a)biostatistical services – correct inference requires that results are produced by a valid data analysis, but a valid data analysis may not be possible for data collected from a poor study design. - they can ensure that your study is designed soundly and analyzed appropriately so that its conclusions are reliable b)data management – by explicitly defining the data base elements and data management procedures at the beginning of the study you can avoid unexpected problems that lead to cost overruns, delays and poor quality data c)technical writing services – assistance with proposal development, ethics review, results of analysis, manuscript preparation and submissions to peer-reviewed journals
3) Libraries
Bracken Library - The main medical library located beside KGH in Botterell Hall is available to all residents. Hospital Libraries - Both HDH and KGH have medical libraries available to all house staff.
Department of Anesthesia Library - This is located in the department at KGH. Books and journals should only be removed for photocopying purposes and returned immediately thereafter. Stolen and lost items will not be replaced. "This is your library, but the books are not yours."

25
4) Literature Searches Access to Medline in a CD-ROM format is available at Bracken Library and both hospital libraries and
through the resident's computer. The hospital libraries provide the service free of charge on a "first come, first serve basis."
Librarians at Bracken Library and the hospitals are available to run literature searches when more sophisticated searching is necessary. The cost of literature searches used for rounds and which have been approved by the departmental secretary at HDH may be billed to the department directly.
Residents can access the departmental homepage at www.anesthesia.ca
5) Computers Residents have access to 4 IBM clone computers, printer, scanner and multimedia machine in the
department library at KGH. Database, spreadsheet and word processing programs are installed, as well s educational programs such as the Anesthesia Simulator Consultant. 6) Presentation Material
Photocopying for official departmental rounds, presentations and academic requirements is available. A data projector for connection to a lap top computer is available. 7) Annual Conference Leave
Residents in the PGY2 to PGY5 years are encouraged to attend at least one major conference during their training. The faculty has donated some money to the residents which can be used specifically for the purpose of attending a conference (See Appendix). Currently, each resident is entitled to $3000 which they can use over the course of their residency towards covering the travel, accommodation and registration costs of attending a conference. Requests for use of this money must be made in advance and residents will be reimbursed from original receipts. A maximum of $2000 can be used in any single year.
Resident Responsibilities 1) Patient Care
a) Clinical Competence Residents are required to acquire and maintain certification in ACLS, ATLS, and NRP throughout their residency. The department will cover the cost of these courses. Please contact the Program Director for further details.
b) Operating Room Assignments & Responsibilities Residents at KGH will be assigned to an operating list for the next day by 1400h by the resident manager. Every effort will be made to assign residents to a list which is appropriate for their level of training. Concurrent coverage rooms may occur up to 2 times per month per resident in PGY 3-5. This will consist of having two residents covered by one staff person. It is the resident's responsibility to confirm the exact list that they are assigned to for the following day.
The Deputy Clinical Head does the list assignments at KGH for staff. If there are any concerns regarding the assignment of resident lists which cannot be resolved by the involved parties, then they should be taken up with the Program Director or his delegate, the Deputy Clinical Head or the Chief Resident.
At HDH resident lists are assigned in the same manner as KGH. Concerns regarding appropriateness of the assigned lists should be directed to the Program Director, the Deputy Chief of Anesthesia at HDH, or the most senior resident assigned to HDH at the time.
Operating rooms at both hospitals are currently scheduled to start at 08:00 daily, except for Wednesdays when it is delayed to 08:30 because of departmental Grand Rounds. This means that the rooms must be ready to begin by 07:45 (08:15 on Wednesdays). Earlier starts may be required if one plans to place a block prior to the anesthetic. Residents are reminded that any early morning Rounds do not change the need to have rooms ready by the above times. If a resident is unable to have the assigned room ready on time, it is his or her responsibility to inform the staff person assigned to the list as soon as possible. On weekends, residents should arrive in the OR at 0730h to ensure an 0800h start.

26
It is expected that the resident will set up the machine and prepare the appropriate monitors and drugs for each case on his/her assigned list. Staff anesthetists should ask residents about their plans for the anesthetic, and make suggestions for changes in the plan to illustrate new ideas or correct problems. It is expected that the staff anesthetist to which a resident is assigned is aware of the activities of the resident in regards to patient care. Cases should not be started without the staff anesthetist aware of the situation, and he or she should be immediately informed of any significant change in the status or treatment of a patient with which a resident is involved.
KGH has an Acute Pain Management Service which is covered by a staff on a daily or weekly basis. It is assumed that residents will setup and initiate the epidural/nerve block infusions or the PCA on any of their own patients who require it, as well as enter them on the computer. Failure to enter a patient on to the Acute Pain Management Service means that the resident is responsible for that patient until the APMS is notified.
c) Preoperative & Postoperative Assessments Residents are expected to preoperatively assess all inpatients and all Same Day Admission (SDA)
patient charts assigned to their lists for the following day. This includes Sunday evenings before a Monday list. If they are unable to see their patient/charts then they must make arrangements with the resident on call. This does not, however, relieve the resident of the expectation that he/she is aware of and prepared for their day. It is advised that all patients on a list be assessed even if the resident plans to be away from the OR for a set period of time (i.e. Core Content Sessions). Lists are often rearranged at the last minute and one cannot guarantee that the resident will only see the cases originally assigned during his or her scheduled OR time. Residents are encouraged to freely discuss patient management with staff and any concerns regarding the patient's care should be conveyed to the staff person in a timely manner. This may mean contacting the staff person at home during the evening if the issue cannot be dealt with on the day of the surgery.
It should be noted that a documented postoperative follow-up of all inpatients with which the resident is involved is now expected within 24 hours of any anesthetic intervention.
Any complication resulting from a resident's intervention should be referred back to that specific resident for follow-up. (eg. an inadvertent spinal tap done during call should be followed by the resident and staff person responsible at the time of the epidural insertion, not the resident assigned to the Obstetrical Block for the following day)
d) Patient Care Outside of the Operating Rooms Residents are required to inform, in a timely manner, the appropriate staff person of any clinical
intervention done outside the operating environment. This is necessary to ensure complete patient care, as well as to provide a certain degree of protection for the resident should any complication arise from his or her involvement.
The appropriate staff person will be defined in the following order:
1. Between the hours of 0800-1530 the obstetrics/consults anesthetist is responsible for coverage of Connell 5, as well as all emergency interventions and all consultations (unless preceded by the situation described in #2).
2. The staff person assigned to a case regardless of the call schedule. Examples include coverage of emergency C-sections by the first available staff anesthetist, or if a consult is directed to a specific staff person.
3. Between the hours of 1800-0730 the first on call anesthetist is responsible for coverage (unless preceded by situation described in #2.)
4. Between the hours of 1530 and 1800 the 2nd call anesthetist is responsible.
5. The Acute Pain Management Service is covered by an assigned staff person with or without a resident.

27
e) On Call Coverage & Pagers Residents on ‘first call’ will be assigned to no more than 16 hours of Anesthetic coverage per shift. This does not include educational responsibilities (i.e. educational rounds, core content sessions).
i) General Comments
The Department of Anesthesiology provides 24 hour in-house coverage of services at KGH. The resident carrying beeper #100 is expected to respond to all calls within at least 10 minutes in a professional manner. Two "on call" rooms are available for anesthesia residents on Connell 6
pager 100 - Anesthesia services (OR, obstetrics, PACU, cardiac & respiratory arrests, etc.) and Trauma pager
The resident carrying the pager at any time is responsible to:
1. Ensure that the Connell 5 Case Room is always ready for emergency C-sections. This means a full machine check out and fresh medications drawn up, dated and signed daily (including STP, Sux, Ephedrine and Oxytocin). This should be completed as soon as possible in the morning.
2. Ensure that the emergency Anesthesia Pack located in the pharmacy room is fully stockedand includes fresh medications which are drawn up, dated, and signed on a daily basis.This should be completed as soon as possible in the morning.
ii) Obstetrical Service The resident carrying the pagers has a primary responsibility to ensure that Connell 5 is ready as
soon as is practical. The "Board" on Connell 5 should be checked to ascertain how many patients are on the floor and what stages they are at in their labors and deliveries. It is also appropriate to talk to the Obstetrical house staff about potential problems that might be brewing at that time. The resident should report to the staff anesthetist covering Connell 5 and should keep him/her aware of any potential or developing problems throughout the day. Booked C/S are to start at 0800h. There are usually 2-3 elective C/S per day.
Residents must respond to requests for epidurals or deliveries as soon as possible, if not in person then by phone to confirm the estimated time of their arrival on the floor.
Epidurals
Calls for epidurals on Connell 5 are understood to be requests on the part of the Department of Obstetrics for an anesthetic assessment to determine if a specific patient is a suitable candidate for an epidural. The resident is not a technician arriving to do another service's bidding. At that time it is appropriate to:
-review the patient's chart and old records -review the patient's medical history with her -do a complete anesthetic assessment to determine the patient's candidacy for spinal or epidural techniques -review risks, complications, expectations and alternatives to epidural anesthesia -provide opportunity for patient questions involving epidural anesthesia -specifically ask the patient if she wants to have an epidural -assess the degree of block post insertion, complete charting and orders
Deliveries
Residents may be called to any delivery for a patient with an epidural, as well as any high-risk deliveries. At the delivery:
-The resident is responsible for the management of the epidural as well as general patient monitoring. -The resident should check the neonatal resuscitation equipment immediately upon arrival. -If the neonatal team is present, the resident should introduce him/herself. The most senior person from either team (anesthesia and neonatology) will be in charge of the resuscitation.

28
iii) Trauma Service
KGH is the Trauma Centre for the Kingston area and Anesthesia will be routinely called for any incoming trauma. Residents must make every effort to respond immediately and documentation of all assessments and services provided is required for every call, including appropriate completion of the "Trauma Team Anesthesia Sheet" available in the Emergency Department. The Trauma Team is run by a Trauma Team Leader (an assigned staff person), and his/her assigned delegate, usually one of the emergency residents. The role of the anesthesia resident is to assist with the care of the patient under direction of the Team Leader in whatever way possible, with specific emphasis on managing the airway. This may include patient transport to and from radiology, the ICU or the OR. The resident must inform the appropriate staff person (see above) as soon as possible so that the necessary staff coverage can be provided for any resident interventions.
iv) Arrest Service
Arrests are identified as either cardiac arrests (code blue) or otherwise (code 99). Residents must make every effort to respond immediately and documented follow-up is required for every call. Arrests are run by a Team Leader, usually the medical resident, however if the anesthesia resident is the first on the scene then he or she should assume this role until the appropriate person arrives. The role of the resident is to assist with the arrest in whatever way possible, with specific emphasis on managing the airway. The resident must inform the appropriate staff person (see above) as soon as possible so that the necessary staff coverage can be provided for any resident interventions.
v) Acute Pain Service
The Acute Pain Service is run by staff persons who are assigned on a daily or weekly basis. Patients utilizing PCEA, continuous epidural analgesia or continuous peripheral nerve blocks are assessed twice daily by the staff person and the resident on the service. Patients on IV PCA are usually assessed daily unless they have complications. Residents are often called to trouble shoot problems regarding these patients or to see new consultations. The resident must respond to the calls promptly and appropriately, which involves patient assessment. It is assumed that residents or staff will setup and initiate the appropriate post operative analgesia regime on any of their own patients who require it. The staff person should be informed of any new pain consults. It is not the responsibility of the resident to make rounds of patients on the Acute Pain Service on behalf of the staff person unless the resident is assigned to the Acute Pain Service block rotation.
vi) Weekend Call
The first case on Saturday, Sunday or holiday mornings should be ready to begin at 0800 hours. Connell 5 should be checked and new drugs made ready (see above) and the emergency room machine should be checked and ready for the first patient by 0800 hours. APMS rounds begin at 0800h until all patients are seen. A separate staff and resident are assigned to APMS weekend rounds.
vii) Assignment of Pagers
The pagers are carried during the hours of 08:30 and 16:00 by the resident doing the Connell 5 Obstetrical block. After 16:00 they are carried by the resident on call for the day. In the event that there is no resident assigned to the Obstetrical block (i.e. post call, vacation, sick leave) the pagers are carried from 08:30 by the resident on call for the day.
*Protected time is provided for core sessions on Wednesday afternoons
f) Consults Consults are covered by anesthetic residents on the C5/consult rotation. At KGH consults are
transmitted to the resident by the Anesthesia secretaries as soon as they become available. The resident assigned to consults should check with the secretaries on a regular basis and respond in a timely manner.
All consults should be reviewed with the assigned staff person. (See section "Resident Responsibilities - Patient Care - Patient Care Outside of the Operating Rooms" for the appropriate staff person)

29
2) Resident Log Book It is mandatory that each resident maintain a current log of all of the anesthetic interventions which he or
she has performed via the web, www.residentlogbook.com.
3) Scheduling Scheduling is the responsibility of the department to ensure adequate patient coverage and that the
PAIRO contract is followed. All scheduling will be done by the Chief Resident or his/her delegate. Any concerns regarding this process which cannot be resolved between the resident and the Chief Resident should be directed to the Program Director.
All requests for time off for any reason will be considered on a "first come first serve" basis. This includes time for conference leave, vacation & lieu days. Requests should be submitted in writing to the postgraduate secretary at KGH where they will be dated upon receipt.
a) Call Schedule
The call schedule is made up on a monthly basis, 14 days prior to the first day of the month. Any requests for time off must be made by the 10th of the previous month for it to be included on the printed "Resident Duty Schedule." Changes to this schedule after the 10th of the month are possible. Residents may switch "on call duties" without confirmation with the Chief Resident. Any additional time off which has not already been allotted to the schedule must be confirmed by the Chief Resident. It is the responsibility of the resident initiating the scheduling changes to inform the following locations at the respective hospitals of any changes to the "Resident Duty Schedule."
1. Kim Asselstine, Program Secretary
2. Anesthesia Duty Room
3. Operating Room
4. Connell 5
5. Switchboard
6. Emergency Department
b) Vacations & Statutory Holidays
1. Vacations Vacations will be allotted as per PAIRO negotiations. It is recommended that any requests be made
in seven-day blocks with the preferred weekend off specified (i.e. Monday - Sunday or Saturday - Friday). Every effort will be made to provide both weekends off for each block requested (i.e. Saturday through the following Sunday), however this may not always be guaranteed. If specific requests are made that do not conform to this format they should be followed up directly with the Chief Resident to confirm if they can be accommodated.
When vacations are requested/taken during off service rotations, you must also inform the postgraduate secretary in writing of these, so that an up-to-date record of your vacation can be recorded.
2. Statutory Holidays Residents scheduled to work on statutory holidays (except for Christmas Day, Boxing Day & New
Years Day) will be permitted to take a lieu day. This includes both the resident who was on call during the holiday, as well as the resident on call for the night prior to the holiday. Scheduling of the lieu day should be done at least one week in advance, confirmed by the Chief Resident, and recorded by the postgraduate secretary at KGH.
Differences in OR scheduling for statutory holidays occur between KGH & HDH (i.e. both hospitals do not always recognize the same holidays). Under the PAIRO contract, residents are allotted 11 statutory holidays. If a resident works at an institution that recognizes a statutory holiday which is not listed in the PAIRO agreement, it shall be considered as one of the resident's floating holidays. Over the course of the year, each resident will be entitled to a maximum of 11 statutory holidays. Floating holidays may be taken as lieu days and applied for as described above.

30
Holiday PAIRO KGH HDH
New Years Day X X X
Family Day X X X
Easter Friday X X X
Easter Monday X
Victoria Day X X X
Dominion Day X X X
August Civic Holiday X X X
Labour Day X X X
Thanksgiving Day X X X
Remembrance Day
Christmas Day X X X
Boxing Day X X X
Floating Days 1
3. Christmas & New Years Holidays Scheduling for Christmas and New Years will be done on a separate basis. Each hospital will have
unique requirements during this period depending on the number of lists assigned for each specific day. Difference in the annual timing of each holiday will also vary the requirements for each year. The PAIRO clause requiring each resident to have at least 5 consecutive days off over either Christmas or New Years will be respected (Christmas Day, Boxing Day, New Years Day, & one weekend). In addition, the following guidelines will be used by the Chief Resident in making the schedule for this time period. The holiday period will be divided into two equal length blocks, one for Christmas and one for New Years.
The number of residents required to provide daily service during these time periods will be established between the Chief Resident and the Deputy Chief of Anesthesia of each hospital and will reflect the changes in the staff anesthetists' list for the time period. This may mean that the number of residents off during each block is not equal.
Requests to be off for either Christmas or New Years will ordinarily be filled on a "first come first serve" basis, unless extenuating circumstances exist. More than 5 days off at Christmas will count as holiday time.
c) Conference Leave Residents may apply for up to 7 days of paid conference leave per year as outlined above. See
section on Organization of Educational Program - Conference Leave for more detail. d) Sick Leave Residents who are unable to work due to illness must contact the following: the departmental
secretaries, the staff person you were scheduled to work with for the day, and the OR early in the morning so that appropriate coverage can be arranged. If a room is to be setup by 08:00 (08:30 on Wednesdays) for invasive monitoring, or if there are any specific concerns regarding the cases to be done, the assigned staff person should be contacted as soon as possible. This may mean calling the staff person directly at home. Any information regarding the estimated duration of the sick leave would be appreciated to assist in scheduling for the next day.
The Program Director or his/her delegate (O.R. Manager) must be notified to ensure coverage of the preoperative assessments which would otherwise be assigned to the resident for the following day.

31
III. Queen’s University Postgraduate Education Policies
Many of the policies of the Postgraduate Education Office, Faculty of Medicine, at Queen’s University can be found at their web site: http://meds.queensu.ca/postgrad/
The following policies are not reproduced here. The web address is noted here for easy access.
1. Evaluation, Promotion and Appeals: http://meds.queensu.ca/postgrad/policies/evaluation_promotion_appeals
2. Moonlighting Policy: http://meds.queensu.ca/postgrad/policies/moonlighting_policy
3. Transfers/Cross-overs within Postgraduate Medical Education Program: http://meds.queensu.ca/postgrad/policies/transfers_and_crossovers
4. Policy on Resident Intimidation and Harassment: http://meds.queensu.ca/postgrad/policies/intimidation_and_harrassment_policy

32
Appendix l
Guidelines for Conference Support
for Residents 1. Residents shall receive a general allowance of $3000 towards travel, accommodation, and registration
expenses during their PGY2 to PGY5 residency years. A maximum of $3000 can be used in any one fiscal year. (The fiscal year begins May 1st and extends to April 30th.) All conferences chosen by the residents should be approved by the Program Director prior to attendance to qualify for expense coverage.
2. No more than $10000 total will be available in any one year for resident conferences. This includes
money for general use (#1 above) and money for those presenting at a conference (#7 below). Thus, residents should notify the Program Director of their desire to use some of their conference money and the estimated amount as soon as they have decided to go to a meeting. (Request forms for Conference money can be obtained from the Kim Asselstine, Residency Program Administrative Secretary.)
3. Residents are expected to make their own travel, accommodation and registration arrangements. 4. Residents must submit the original receipts to the Departmental Academic Secretary to qualify for
reimbursement. 5. Unused portions of the $3000 conference money will be used at the discretion of the Departmental
Chairman and Program Director for resident related activity. 6. Use of funding for educational activities other than attendance at conferences must have the approval in
advance from the Program Director. 7. Residents who have abstracts accepted for presentation, or who are invited to present at a major
conference will receive support for travel and accommodation expenses subject to #2 and #3 above. This money would be available in addition to the general allowance money described in #1 above.
8. Residents will be supported for only one conference per year per original abstract (i.e. the resident will
not be supported for presenting the same abstract at more than one conference per year). The resident may qualify for special allowance money for more than one conference per year if the Departmental Research Coordinator and the Program Director agree that the abstract to be presented at the second conference is sufficiently different to be considered another original work.
9. Should there be a disagreement about any aspect of a particular request for Conference money support,
the resident will present his/her case to the Residency Training Committee of the department. The RTC will make the final decision about the eligibility of the resident’s request. Should the request be seen to be one that meets the criteria for support but is beyond the funding allowance of any given year, a special request for funding may be made to the department for support over and above the $10000 limit.
Revised Jan 2008

33
Appendix II
Queen’s University Department of Anesthesiology
Resident Evaluation of Clinical Block
Resident:____________________________________Block:__________________________________ No. of days on assigned block: ______ No. of cases specific for block: ________ I was aware of the learning objectives for this block Yes:______ No:______ Strongly disagree Strongly agree These objectives enhanced my learning during this block 1 2 3 4 5 These objectives were appropriate for my level of training 1 2 3 4 5 My evaluation was consistent with these objectives 1 2 3 4 5 Comments The knowledge component was well covered as far as: The basic sciences 1 2 3 4 5 The clinical sciences 1 2 3 4 5 Comments: Specific Clinical Skills obtained during this rotation (eg. Double lumen tube placement, central line placement, etc.): 1. ____________________________ No. of opportunities: _____________ 2. ____________________________ No. of opportunities: _____________ 3. ____________________________ No. of opportunities: _____________ I received appropriate opportunities to acquire clinical skills: 1 2 3 4 5 Comments: I received appropriate instruction in clinical skills 1 2 3 4 5
Comments:
I received enough feedback daily on how I was progressing 1 2 3 4 5 Comments: The feedback that I received from the faculty was valuable 1 2 3 4 5 Comments: I especially valued the feedback that I receive from the following faculty:
1. __________________ 2. __________________ 3. __________________

34
I received the appropriate amount of clinical supervision: 1 2 3 4 5 Comments: The quality of the reference material suggested was excellent 1 2 3 4 5 Comments: Aspects of this block that I would like to see improved at this time are:
1. ______________________________________________________________________ 2. ______________________________________________________________________ 3. ______________________________________________________________________
Aspects of this block that are particularly good at this time are:
1. ______________________________________________________________________
2. ______________________________________________________________________
3. ______________________________________________________________________ Other Comments: Strongly disagree Strongly agree Overall, this block met my expectations 1 2 3 4 5 Comments
PLEASE RETURN TO KIM ASSELSTINE IN THE DEPARTMENT OF ANESTHESIOLOGY OFFICE

35
Appendix III
Department of Anesthesiology Resident Evaluation of the Program
Strongly disagree Strongly agree Overall, the program is meeting my expectations 1 2 3 4 5 Comments: The knowledge component is well covered as far as: The basic sciences 1 2 3 4 5 The clinical sciences 1 2 3 4 5 Comments: I receive appropriate opportunities to acquire clinical skills: 1 2 3 4 5 Comments: I receive appropriate instruction in clinical skills 1 2 3 4 5
Comments:
I receive enough feedback daily on how I am progressing 1 2 3 4 5 Comments: I value the feedback that I receive from all the faculty: 1 2 3 4 5 Comments: I especially value the feedback that I receive from the following faculty:
1. __________________ 2. __________________ 3. __________________
I receive the appropriate amount of clinical supervision: 1 2 3 4 5
Comments: Aspects of the residency program that I would like to see improved at this time are:
1. ______________________________________________________________________ 2. ______________________________________________________________________ 3. ______________________________________________________________________
Aspects of the residency program that are particularly good at this time are:
4. ______________________________________________________________________ 5. ______________________________________________________________________ 6. ______________________________________________________________________
If you have important concerns that are not covered in the above questionnaire, please speak to Dr. Melanie Jaeger.
Please complete and return to Kim Asselstine
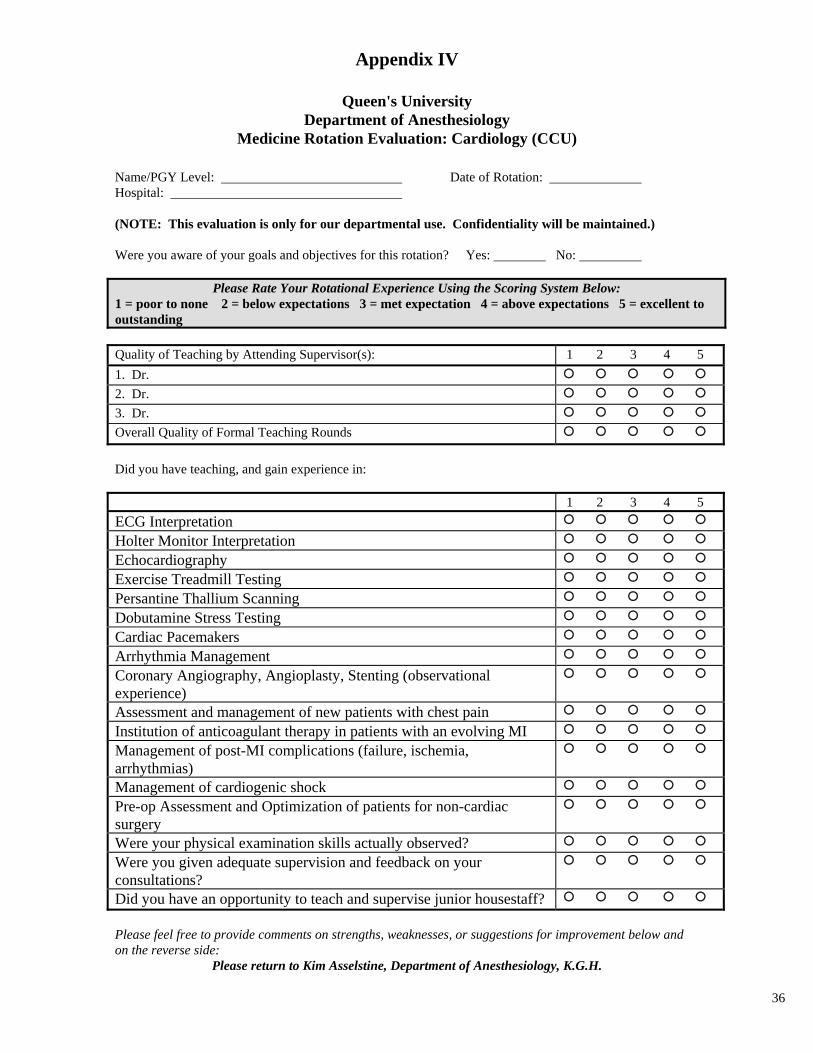
36
Appendix IV
Queen's University Department of Anesthesiology
Medicine Rotation Evaluation: Cardiology (CCU)
Name/PGY Level: Date of Rotation: Hospital: (NOTE: This evaluation is only for our departmental use. Confidentiality will be maintained.) Were you aware of your goals and objectives for this rotation? Yes: No:
Please Rate Your Rotational Experience Using the Scoring System Below: 1 = poor to none 2 = below expectations 3 = met expectation 4 = above expectations 5 = excellent to outstanding Quality of Teaching by Attending Supervisor(s): 1 2 3 4 5
1. Dr.
2. Dr.
3. Dr.
Overall Quality of Formal Teaching Rounds
Did you have teaching, and gain experience in: 1 2 3 4 5
ECG Interpretation
Holter Monitor Interpretation
Echocardiography
Exercise Treadmill Testing
Persantine Thallium Scanning
Dobutamine Stress Testing
Cardiac Pacemakers
Arrhythmia Management
Coronary Angiography, Angioplasty, Stenting (observational experience)
Assessment and management of new patients with chest pain
Institution of anticoagulant therapy in patients with an evolving MI
Management of post-MI complications (failure, ischemia, arrhythmias)
Management of cardiogenic shock
Pre-op Assessment and Optimization of patients for non-cardiac surgery
Were your physical examination skills actually observed?
Were you given adequate supervision and feedback on your consultations?
Did you have an opportunity to teach and supervise junior housestaff?
Please feel free to provide comments on strengths, weaknesses, or suggestions for improvement below and on the reverse side:
Please return to Kim Asselstine, Department of Anesthesiology, K.G.H.
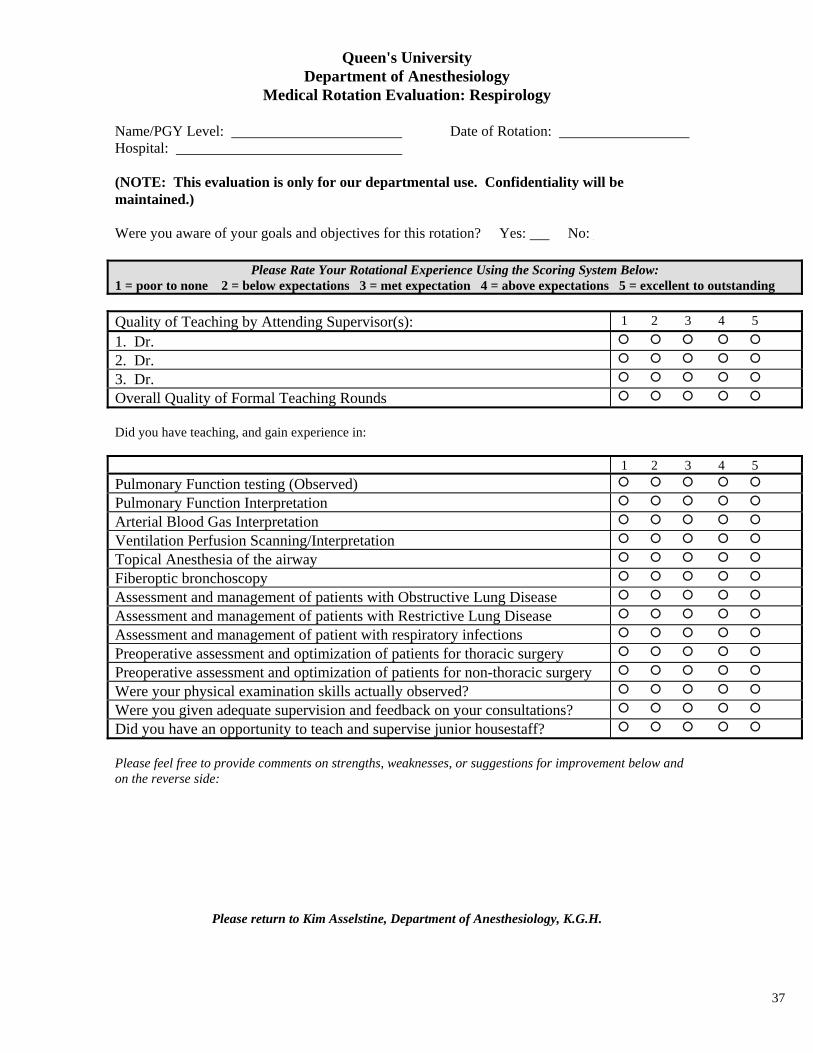
37
Queen's University Department of Anesthesiology
Medical Rotation Evaluation: Respirology
Name/PGY Level: Date of Rotation: Hospital: (NOTE: This evaluation is only for our departmental use. Confidentiality will be maintained.) Were you aware of your goals and objectives for this rotation? Yes: No:
Please Rate Your Rotational Experience Using the Scoring System Below: 1 = poor to none 2 = below expectations 3 = met expectation 4 = above expectations 5 = excellent to outstanding
Quality of Teaching by Attending Supervisor(s): 1 2 3 4 5
1. Dr.
2. Dr.
3. Dr.
Overall Quality of Formal Teaching Rounds
Did you have teaching, and gain experience in: 1 2 3 4 5
Pulmonary Function testing (Observed)
Pulmonary Function Interpretation
Arterial Blood Gas Interpretation
Ventilation Perfusion Scanning/Interpretation
Topical Anesthesia of the airway
Fiberoptic bronchoscopy
Assessment and management of patients with Obstructive Lung Disease
Assessment and management of patients with Restrictive Lung Disease
Assessment and management of patient with respiratory infections
Preoperative assessment and optimization of patients for thoracic surgery
Preoperative assessment and optimization of patients for non-thoracic surgery
Were your physical examination skills actually observed?
Were you given adequate supervision and feedback on your consultations?
Did you have an opportunity to teach and supervise junior housestaff?
Please feel free to provide comments on strengths, weaknesses, or suggestions for improvement below and on the reverse side:
Please return to Kim Asselstine, Department of Anesthesiology, K.G.H.

38
Queen's University Department of Anesthesiology
Medical Rotation Evaluation: Nephrology
Name/PGY Level: Date of Rotation: Hospital: (NOTE: This evaluation is only for our departmental use. Confidentiality will be maintained.) Were you aware of your goals and objectives for this rotation? Yes: No:
Please Rate Your Rotational Experience Using the Scoring System Below: 1 = poor to none 2 = below expectations 3 = met expectation 4 = above expectations 5 = excellent to outstanding
Quality of Teaching by Attending Supervisor(s): 1 2 3 4 5
1. Dr.
2. Dr.
3. Dr.
Overall Quality of Formal Teaching Rounds
Did you have teaching, and gain experience in: 1 2 3 4 5 Understanding normal renal physiology
Methods of evaluation of renal function
How altered renal function affects drug pharmacokinetics
Assessment of the anephric patient
Management of the patient with renal transplant
Management of the patient on hemodialysis
Placement of double lumen central dialysis lines
Understanding the components of writing dialysis orders
Understanding continuous renal replacement therapy
Evaluation of the patient with abnormal electrolytes
Evaluation of the patient with abnormal acid-base status
Were your physical examination skills actually observed?
Were you given adequate supervision and feedback on your consultations?
Did you have an opportunity to teach and supervise junior housestaff?
Please feel free to provide comments on strengths, weaknesses, or suggestions for improvement below and on the reverse side:
Please return to Kim Asselstine, Department of Anesthesiology, K.G.H.
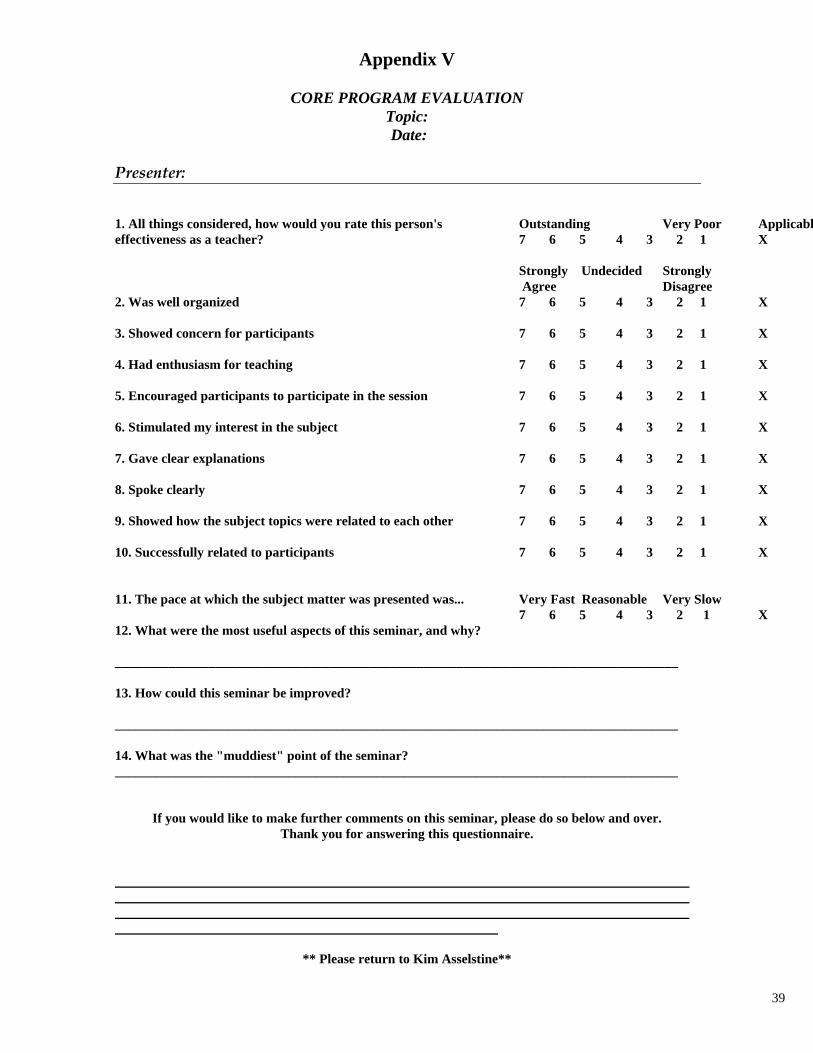
39
Appendix V
CORE PROGRAM EVALUATION Topic: Date:
Presenter: 1. All things considered, how would you rate this person's effectiveness as a teacher? 2. Was well organized 3. Showed concern for participants 4. Had enthusiasm for teaching 5. Encouraged participants to participate in the session 6. Stimulated my interest in the subject 7. Gave clear explanations 8. Spoke clearly 9. Showed how the subject topics were related to each other 10. Successfully related to participants 11. The pace at which the subject matter was presented was...
Outstanding Very Poor Applicabl7 6 5 4 3 2 1 X Strongly Undecided Strongly Agree Disagree 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X 7 6 5 4 3 2 1 X Very Fast Reasonable Very Slow 7 6 5 4 3 2 1 X
12. What were the most useful aspects of this seminar, and why? ____________________________________________________________________________________ 13. How could this seminar be improved? ____________________________________________________________________________________ 14. What was the "muddiest" point of the seminar? ____________________________________________________________________________________
If you would like to make further comments on this seminar, please do so below and over. Thank you for answering this questionnaire.
** Please return to Kim Asselstine**
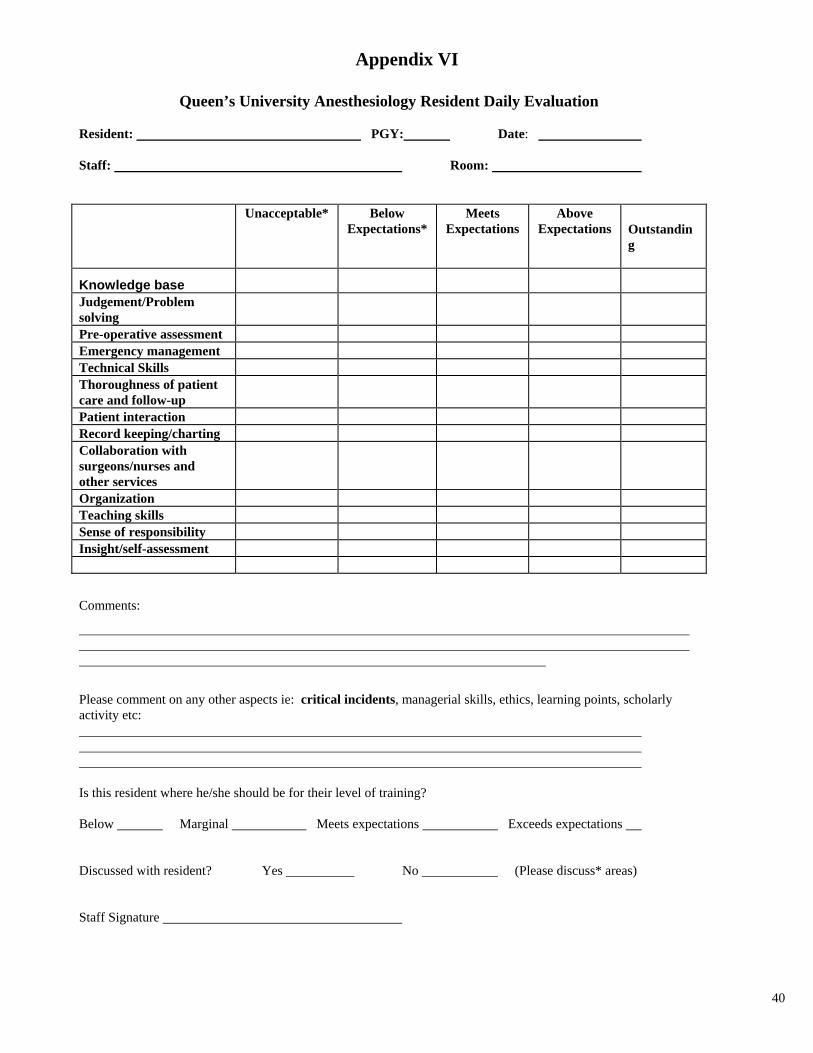
40
Appendix VI
Queen’s University Anesthesiology Resident Daily Evaluation Resident: PGY: Date: Staff: Room:
Unacceptable* Below Expectations*
Meets Expectations
Above Expectations Outstandin
g
Knowledge base
Judgement/Problem solving
Pre-operative assessment Emergency management Technical Skills Thoroughness of patient care and follow-up
Patient interaction Record keeping/charting Collaboration with surgeons/nurses and other services
Organization Teaching skills Sense of responsibility Insight/self-assessment
Comments:
Please comment on any other aspects ie: critical incidents, managerial skills, ethics, learning points, scholarly activity etc: Is this resident where he/she should be for their level of training? Below Marginal Meets expectations Exceeds expectations Discussed with resident? Yes No (Please discuss* areas) Staff Signature
1
Appendix VII
Queen’s University Anesthesiology Staff Daily Evaluation (to be filled out by Resident at the end of the day)
DEPARTMENT OF ANESTHESIOLOGY
PRECEPTOR EVALUATION This evaluation is confidential. Your preceptor will not see this form. The Program Director and/or the Department Head provide feedback on a semi-annual basis to the preceptor. You may request a discussion of this evaluation with the Program Director.
1 2 3 4 5 NA
I do not agree Needs
improvement Satisfactory Good
I definitely agree
Not Assessed
Deficiencies of consequence
Few significant deficiencies
Not great but not bad
Good performance
No deficiencies, exemplary
**COMMENTS ARE REQUIRED FOR MARKS LESS THAN 3**
Feedback 1 The preceptor provided constructive feedback.
1 2 3 4 5 NA
Feedback 2 The preceptor’s feedback contained these elements: timely, specific, non-judgmental manner, in a private setting.
1 2 3 4 5 NA How could the preceptor’s feedback be improved? _______________________________________________________ ________________________________________________________________________________________________
Organization of Teaching The preceptor taught in a clear, organized manner.
1 2 3 4 5 NA
Clinical Supervision 1 The preceptor involved me in patient management at an appropriate level for my level of training and understanding.
1 2 3 4 5 NA
Clinical Supervision 2 The preceptor appropriately demonstrates/critiques clinical procedures.
1 2 3 4 5 NA
Resident Interaction 1
The preceptor treated me in a respectful manner.
1 2 3 4 5 NA
Resident Interaction 2
The preceptor created a positive learning environment.
1 2 3 4 5 NA
How could the preceptor improve the learning environment? ________________________________________________
_________________________________________________________________________________________________

2
Resident Interaction 3
The preceptor was open to discussion of alternative views or approaches to the clinical management of patients.
1 2 3 4 5 NA
Scholarly Influence 1
The preceptor related theories and concepts to clinical practice in a manner that was clear.
1 2 3 4 5 NA
Scholarly Influence 2
The preceptor influenced me to broaden my knowledge of the literature.
1 2 3 4 5 NA
Scholarly Influence 3
The preceptor encouraged me to broaden my problem solving skills.
1 2 3 4 5 NA
Availability
The preceptor was accessible for advice perioperatively.
1 2 3 4 5 NA
Supervision
The preceptor provided effective supervision when necessary.
1 2 3 4 5 NA
OVERALL
The preceptor as a teacher/role model:
1 2 3 4 5 NA
**COMMENTS ARE REQUIRED FOR MARKS LESS THAN 3** COMMENTS
Other Comments: