acknowledgements - indiana university …mri/seminars/slides/spring 2014/neurovascular mra...anatomy...
TRANSCRIPT
4/17/2014
1
E. Michael Harned, M.D. Assistant Professor of Clinical Radiology Indiana University School of Medicine
I have nothing to disclose
Neurovascular Magnetic Resonance Angiography And Magnetic Resonance Venography
ACKNOWLEDGEMENTS
1. Daroff RB, Fenichel GM, Jankovic J, Mazziotta JC: Bradley’s Neurology in Clinical Practice, 6th ed. Saunders
2. Anderson CM, Edelman RR, Turski PA: Clinical Magnetic Resonance Angiography. Raven Press
For neurovascular imaging, MRA has largely been replaced by CTA due to its higher spatial resolution and relatively fewer artifacts.
However, MRA may still be desired in certain situations:
Patients with a contraindication to iodinated contrast administration: history of anaphylactoid reaction, severe asthma, renal insufficiency, multiple myeloma
Lack of venous access
Patients having an MRI of the brain, neck, or cervical spine where it is desired to get vascular imaging done at the same time- “killing 2 birds with 1 stone”
NEUROVASCULAR ANATOMY

4/17/2014
2
Int . carot·id Ant. communicat ing
Ant . cerebral ·
ATterial eircle
Posttrior ·inferihr cc1·ehellar
Occtprtal vein - •
- Factal vein
Internal jugular vein (IJV )I
Extemal acoustic meatus
Superior bulb of IJV
Inferior petrosal smus
- Lingual vein
mal jugular vein (EJV) - . Inferior bulb and valve of IJV
\ - Ant erior jugular vetn
- Sternoclavtcular JOint
Right brachrocephahc vem .....;.,. Superior vena cava
•
4/17/2014
3
_,jll 1 e I " ' " h,....ton• II · wpt!- t lo t \ ._.
I'
I "
.,..
C'l •liJ I liu • I 0 • C :n«fn iOIB
' " . .
0 h : • , . , . ..'N i l " O>'t
ELSEV IER. INC - NETIERIMAGES.COM
MRA TECHNIQUES
Time-Of-Flight (TOF)
Relies on repeated saturation pulses to a slice or volume so that background tissue is suppressed and only new spins (flow) are able to generate signal
May be performed as a 2D or 3D technique
2D examines a single slice at a time and then stacks them
3D examines a slab and uses phase-encoding along the Z-axis
3D TOF allows better spatial resolution but is more
susceptible to signal loss due to in-slab flow
RF Pulse
,,-, ., '', '' ,,'
Z Gradient I \ ,I \ C J \._.
Y Gradient 0
Gradient r '
SATURATION INCREASES WITH:
Shorter TR
Larger flip angle
Multiple repetitions
Longer T1
c

4/17/2014
4
Inflow of Magnetized Blood into 3D Slab
Projected Plane
·------tu _ tion 18 nd
Acquir d Slice
a a/sine
I I I I
4/17/2014
5
Phase-Contrast
Relies on bipolar gradient pulse which causes phase shift for flowing spins but no phase shift for stationary spins
Excellent background suppression
No need for saturation band
Also provides information on flow direction
May be performed as a 2D or 3D technique
3D Phase-Contrast allows better spatial resolution and provides flow direction information along all 3 axes
I
I
I
I
I
time
Statiollary a p l • aeaamulale pit••....... lobe and tileD wrap l t d arauad _ . . . _ IMIJ M •
I .aamuladoa durln1111e •LDMI loiJe . , . . _ • • r
I
I
Contrast-Enhanced MRA
Really a form of 3D TOF MRA but uses gadolinium to increase intravascular signal and overcome problem of signal loss due to in-slab flow
Images acquired quickly while a bolus of gadolinium is in the vessels of interest
Different physics- uses elliptical-centric k-space filling:
Central (most important) points of k-space are filled first, at time of greatest intravascular gadolinium concentration
May acquire preinjection source images as mask for subtraction- “Digital Subtraction MRA”
4/17/2014
6
ATHEROSCLEROTIC STENOTIC DISEASE
WHY IT MATTERS (all numbers approximate and for United States)
795,000 people suffer new or recurrent stroke each year
1 stroke every 40 seconds
Stroke kills more than 137,000 people per year.
1 stroke death every 4 minutes
#4 cause of death
1 in every 18 deaths
Stroke death rates per year per 100,000 population: 41.7 for white males 41.1 for white females 67.7 for black males 57.0 for black females
Americans pay about $73.7 billion per year for stroke-related medical costs and disability
Likely Histories/Indications:
Stroke, CVA, or TIA
Specific neurologic deficit- hemiparesis, aphasia, facial numbness, etc.
Carotid bruit
ICA stenosis on carotid ultrasound
WHAT THE RADIOLOGIST NEEDS FROM YOU
3D TOF MRA of the circle of Willis
Contrast-enhanced MRA of the arteries of the neck (Often a good idea to do a 2D TOF MRA of the neck first in case there is a problem with the gadolinium bolus- There is no going back and doing this once contrast has been injected)
Please send both sets of source images as well as rotating segmented MIPs of right carotid, left carotid, and vertebrobasilar for circle of Willis and for neck
3D TOF MRA circle of Willis- source images

4/17/2014
7
3D TOF MRA circle of Willis- MIPs Contrast-enhanced MRA neck- source images Contrast-Enhanced MRA neck- MIPs
2D TOF MRA neck- source images 2D TOF MRA neck- MIPs
Carotid stenosis%= (1 • Nto) x 100
4/17/2014
8
B
I
Figure 1. A 58-year-old man with truncus bicaroticus as normal variant that is displayed both on
MRA and DSA (a and b; arrow heads), and 90% diameter stenosis of the right ICA diagnosed on
MRA (c; bold arrow) and confirmed by DSA (d; bold arrow).
Willinek W A et al. Stroke. 2005;36:38-43
Copyright © American Heart Association, Inc. All rights reserved.
4/17/2014
9
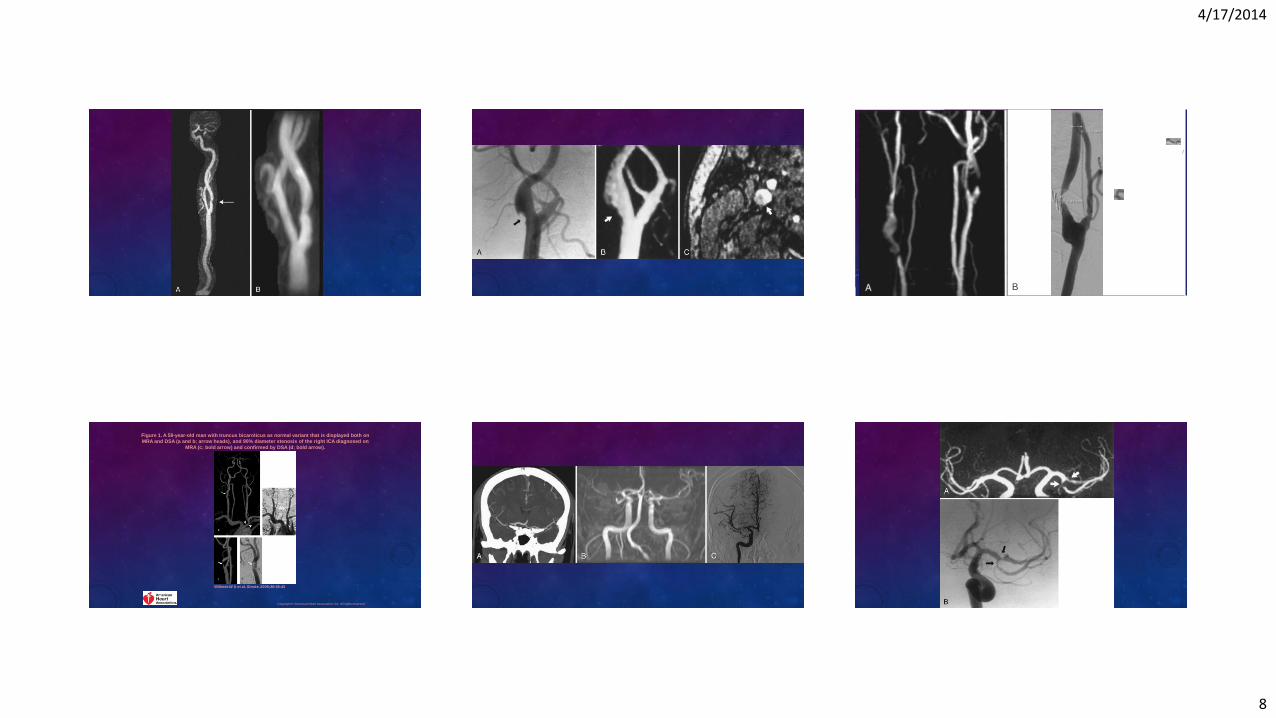
Figure 2. Enlarged MIP image from CE MRA (a) and DSA image (b) of the circle of Willis of a 44-
year-old man: 50% stenosis in the M1 segment (arrow heads) of the right MCA was concordantly
diagnosed on MRA and DSA.
Willinek W A et al. Stroke. 2005;36:38-43
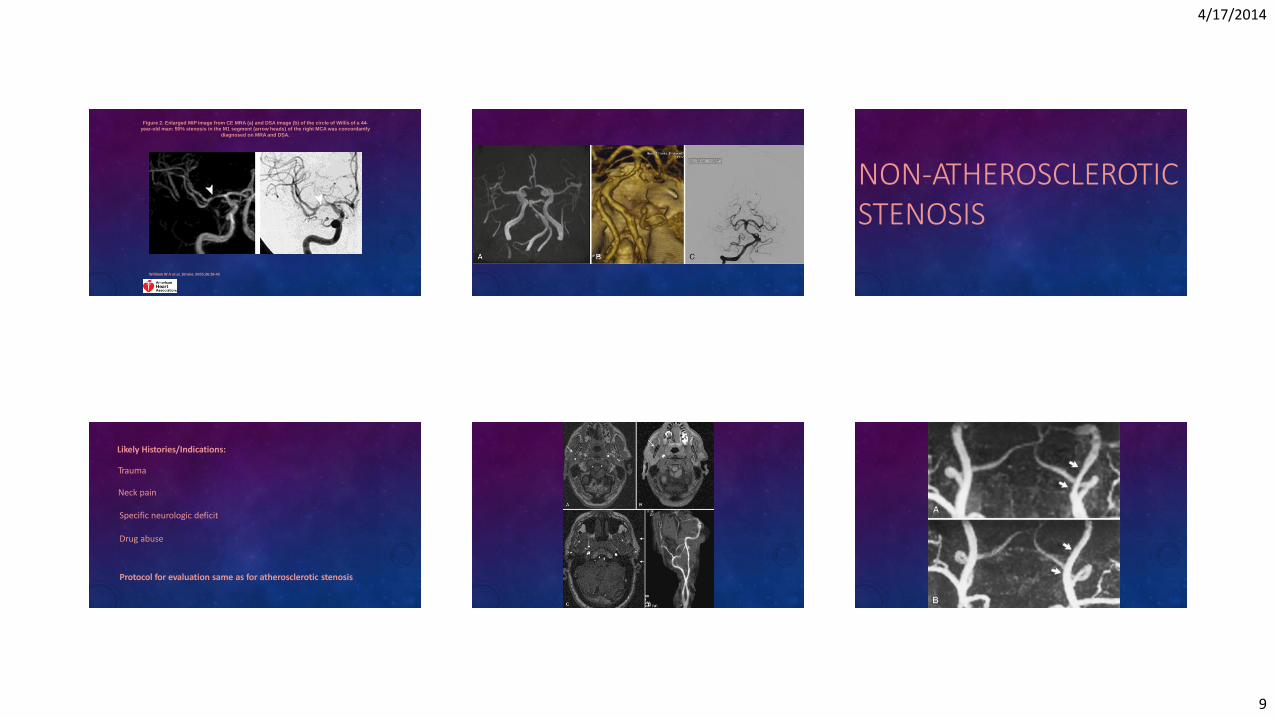
NON-ATHEROSCLEROTIC STENOSIS
Likely Histories/Indications:
Trauma
Neck pain
Specific neurologic deficit
Drug abuse
Protocol for evaluation same as for atherosclerotic stenosis

4/17/2014
10
Figure 4. A 61-year-old man patient with subacute right MCA territory infarction. 75% stenosis of
right ICA was diagnosed on CE MRA (a; arrow), but DSA revealed a thrombus causing a 55%
diameter stenosis (b; arrow).
Willinek W A et al. Stroke. 2005;36:38-43
Copyright © American Heart Association, Inc. All rights reserved.
Date of download: 12/22/2013 Copyright © 2012 American Medical
Association. All rights reserved.
From: Cocaine-Induced Cerebral Vasoconstriction Detected in Humans With Magnetic Resonance Angiography
JAMA. 1998;279(5):376-380. doi:10.1001/jama.279.5.376
Figure Legend:
Axial maximum intensity projection images at baseline (left) and20 minutes following intravenous cocaine (0.4 mg/kg) administration
(right).Cocaine induced a signal loss at distal segments of the middle cerebral arteries(upper arrowheads) and in the posterior
cerebral arteries (lower arrowheads),indicative of vasoconstriction. A indicates anterior; P, posterior; L, left;and R, right. Scale bar =
1 cm.
Moyamoya Disease
Disease where vessels at the base of the brain become constricted- Most commonly distal internal carotid arteries but may also involve proximal middle and anterior cerebral arteries
Collateral circulation develops around the blocked vessels, but the collateral vessels are small, weak, and prone to hemorrhage
On angiography, the collateral vessels resemble a “puff of smoke”- “Moyamoya” in Japanese
Patients present with TIAs, strokes, headaches, and seizures
Most common in women in their 20s and 30s
Association with Down’s syndrome, neurofibromatosis type 1, sickle cell disease, prior brain radiation
Figure 3. A 45-year-old woman with Moyamoya disease.
Willinek W A et al. Stroke. 2005;36:38-43
Copyright © American Heart Association, Inc. All rights reserved.
INTRACRANIAL ANEURYSMS
4/17/2014
11
Likely Histories/Indications:
Subarachnoid hemorrhage
Headaches
Family history of intracranial aneurysms
Autosomal dominant polycystic kidney disease
WHAT THE RADIOLOGIST NEEDS FROM YOU
3D TOF MRA of the circle of Willis
No need for gadolinium
No need to image the neck
0 lrehiJiiun ttl t:111• ( t•IW
c 1nh•:al n " on
hrltttcq '"·•l :.l r
l' u 'lrt IN
t,i-i;,.I. II 0 0
lll'lltttl ''f'rlm In 101 t r r htll.u
ELSEVIER. INC - NETIERIMAGES.COM
4/17/2014
12
VENOUS PATHOLOGY
Likely Histories/Indications:
Possible venous sinus thrombosis- pregnancy, oral contraceptives, cancer, other hypercoagulable states
Cavernous sinus syndrome
Hyperdense dural venous sinus or intracranial vein on CT
Venous infarct on CT or MRI
4/17/2014
13
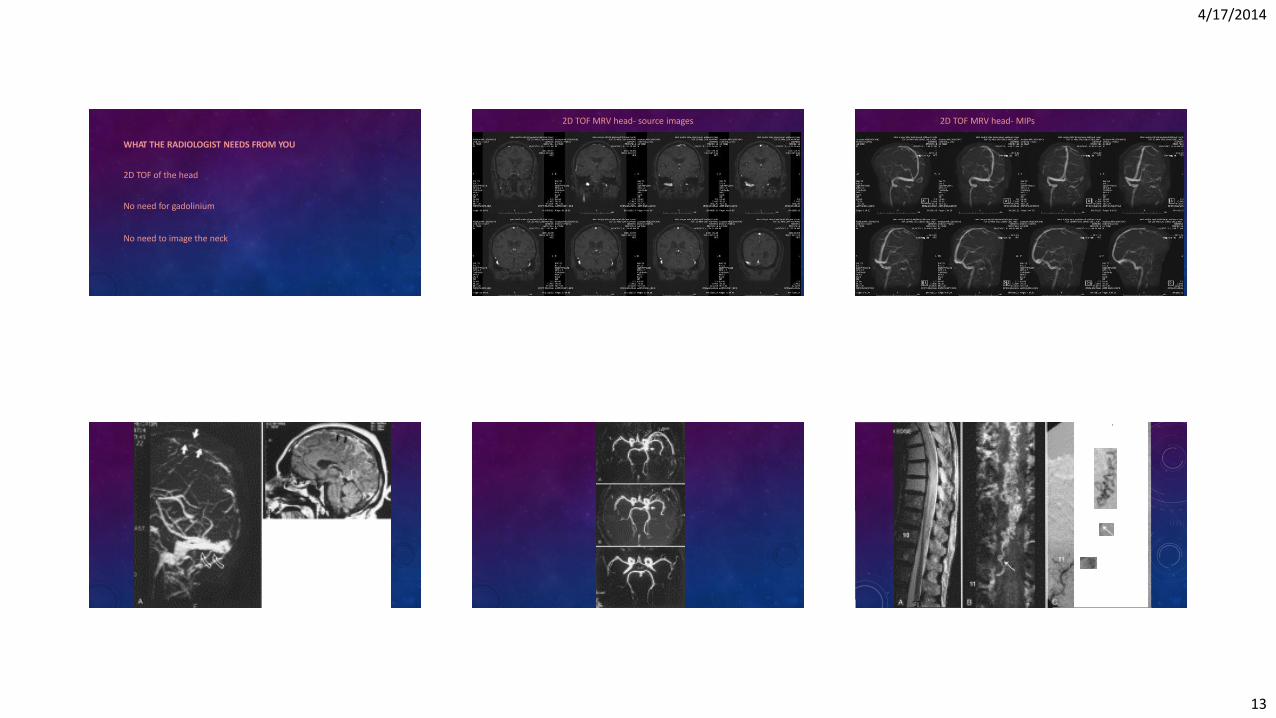
WHAT THE RADIOLOGIST NEEDS FROM YOU
2D TOF of the head
No need for gadolinium
No need to image the neck
2D TOF MRV head- source images 2D TOF MRV head- MIPs
•
4/17/2014
14
Thanks!
Questions?