acknowledgements · 4.5 sptool gui ... 4.6 matlab fuzzy logic toolbox ... (limb potential relative...
TRANSCRIPT

2
3
Acknowledgements First and foremost, we would like to thank our Final Year Project (FYP) supervisor, Professor Mohammad Adnan Al‐Alaoui., for his support and assistance in guiding us throughout the project. In addition, we would like to thank Mr. Khaled Joujou for his valuable help in installing and running the database software. We would like to thank the coordinator of the FYPs, Professor Jean Saade, for his time in organizing and coordinating the projects. We are also grateful to the Department of Electrical and Computer Engineering for making this FYP possible.

4
Abstract The Electrocardiogram (ECG) is the most clinically used biological signal and it is the means of detecting several cardiac diseases and abnormalities. Among various abnormalities related with functioning of the human heart, Premature Ventricular Contraction (PVC) is the contraction of the lower chambers of the heart (the ventricles) which occur earlier than usual, because of abnormal electrical activity of the ventricles. The QRS complex detection is a substantial procedure in analyzing the ECG; however, it is not always straightforward. The great variety of QRS detection algorithms reflects the need for a reliable QRS detection in cardiac signal processing, however, the currently achievable detection rates reflect only the overall performance of the detectors which generally hide the problems still present in case of noisy or abnormal ECG signals which indicates that a satisfying solution to these problems is still not found. In our final year project we have designed and implemented an enhanced artificial neural network QRS detection and PVC diagnosis algorithms in MATLAB. In our implementation, the MIT‐BIH Arrhythmia Database, which is the most popular standard database and the most widely used in QRS publications, was used.
5
Contents 1 Introduction Report Structure………………………………………………………2
2 Background The Electrocardiogram (ECG) and its Characteristics…………….3
2.1.1 The Heart and Electrocardiogram………………………….4
2.1.2 ECG characteristics…………………………………………..5
2.2 Premature Ventricular Contraction ………………………………..7
2.3 QRS Detection Approaches …………………………………………8
2.3.1 Artificial Neural Network Approaches……………………8 2.3.5 Hybrid Fuzzy‐Neuro‐Based QRS Detection……………..10
3 Foundation
The ECG Database ………………………………………………….13 ECG Signal Extraction ……………………….……………………..15 Implementation Software…………………………………………..22
Wavelet Toolbox ……………………………………………23 Artificial Neural Network Toolbox .……………………….24 Fuzzy Logic Toolbox ………………………………………..25
6
Preprocessing I ……………………………………………………..26 De‐noising ……………………………………………………...26 Smoothing ……………………………………………………...29 Normalizing ……………………………………………………31
Preprocessing II ……………………………………………………..32 Cutting the Normal and Abnormal Beat ……………………33 Detecting Peaks and Valleys …………………………………35 4 Artificial Neural Network
Design of the Neural Network ……………………………………..37
Implementation of the Neural Network …………………………..39 Simulation of the Neural Network ………………………………...42 5 Fuzzy‐Neural Networks
Design of Fuzzy‐Neuro‐Based Module ……………………………46
The Fuzzy Clustering Algorithm …………………………..48
The Fuzzy‐Neuro MLP Subnetwork Algorithm ………….50
5.2 Implementation of Fuzzy‐Neuro‐Based Module …………………51
5.2.1 The Fuzzy Clustering Algorithm …………………………..51 5.2.2 The Fuzzy‐Neuro MLP Subnetwork Algorithm ………….53
5.3 Results of Fuzzy‐Neuro‐Based Module ……………………...……60
6 Conclusion Bibliography
7
List of Figures
2.1 The objective of electrocardiography ……………………………. 4 2.2 Clinical ECG tracing of patients……………………………………4 2.3 The standard 12‐lead set of ECG…………………………………...5 2.4 The three limb leads…………………………………………………5 2.5 The three augmented leads…………………………………………6 2.6 The six referenced leads …………………………………………..6 2.7 The ECG signal and its different components……………………7 2.8 Normal ECG recording……………………………………………..8 2.9 ECG of an LVH patient……………………………………………11 2.10 Common Structure of the QRS detectors………………………..12 2.11 The relation between the convolution integral of the wavelet function multiplied by a uniform wave and the appearance of a local maxima in the WT…………………………………………..15 2.12 Functional Blocks of a Fuzzy Inference System…………………17 2.13 Block diagram of FIS for ECG interpretation and LVH diagnosis ……………………………………………………………………… 19 2.14 The membership functions of the FIS………………………...….19 2.15 Functional Description of a Single Neuron……………………...21 2.16 A 3‐2‐2 configured multilayer perceptron with direct connection between input and output ………………………………………..21 2.17 A single layer ANN with 202 inputs and 3 outputs employing
the batch mode of the Al‐Alaoui Algorithm, Form I…………...23 2.18 An MLP ANN with 202 inputs and 3 outputs employing the error backpropagation………………………………………….....24 2.19 An MLP ANN structure…………………………………………..26 3.1 The plots in time of the pure surface and the filtrated ECG signals………………………………………………………………33 3.2 The plots of the power spectrum of the pure ECG and the one
8
filtered at 20 Hz……………………………………………………33 3.3 The first module of the ANN MLP Approach 1 for QRS complex detection and beat classification………………………………...34 3.4 The second module of the ANN MLP Approach 1 for LVH diagnosis…………………………………………………………..35 3.5 The structure of a hybrid fuzzy‐neuro‐based network……….37 3.6 The performance of the G‐K algorithm of the self‐organization to the recognition of clusters…………………………………….40 4.1 The MIT‐BIH Arrhythmia Database…………………………....44 4.2 The available ECG files on the database site…………………..45 4.3 Sample Record of the MIT‐BIH Database………………….......46 4.4 MATLAB Signal Processing Toolbox…………………………..47 4.5 SPTool GUI……………………………………………………..…48 4.6 MATLAB Fuzzy Logic Toolbox…………………………….…..48 4.7 ANFIS Editor GUI…………………………………………….….49 4.8 MATLAB Neural Network Toolbox………………………..…..50 4.9 The Neural Network Tool………………………………….……50
9
Chapter 1 Introduction The past few decades have witnessed an outstanding pace of clinical, surgical, and technological developments. Since then great efforts have been made to benefit from the technological advances and use of computers in the medical field. Since the electro cardiogram (ECG) is used for analyzing the clinical conditions of the heart, the most vital organ in the human body, it is of great important to cardiologists to perform ECG analysis with maximum accuracy. Much research has been done in the field of ECG analysis, all aiming at performing automatic signal detection with near perfect detection rates. For thirty years now, efforts have been oriented to the modeling of the expertise of cardiologists and specialists through computers. This issue has been tackled by many researchers who have come up with a variety of different ECG recognition and QRS detection algorithms that have become widely known in the literature. Among the numerous studied and evaluated methods, artificial neural network methods have taken special attention because their properties such as non‐linearity, learning ability, and universal approximation allow them to solve complicated signal processing problems like QRS detection and PVC diagnosis. In this report, we will present our final year project work which consists of designing and implementing enhanced artificial neural and hybrid fuzzy neural networks for QRS detection and PVC diagnosis. In our work, we have used the standard MIT‐BIH Arrhythmia database as our ECG source and MATLAB 7.0.1 as our implementation and testing environment.

10
1.1 Report Structure This final report presents our work throughout the fall and spring semesters of academic year 2005 – 2006 while emphasizing on the work performed during the spring term. The report is divided into six chapters where each chapter covers a substantial portion of the project. In chapter 2, Background, we tackle the basics of this project while elaborating about the heart and electrocardiogram, the Premature Ventricular Contraction abnormality, and an overview of the two QRS detection approaches we have followed in the project, artificial neural networks and hybrid fuzzy‐ neural networks. Chapter 3, Foundation, discusses all what have been done before the actual implementation of the two modules. It involves an explanation about the standard ECG database used in this project and how we managed to extract the signals from it, and then moves to introduce the MATLAB software tools we have used for preprocessing and implementation. Finally, the chapter covers thoroughly each of the preprocessing steps that are divided into two main stages. Chapter 4, Artificial Neural Network, covers the ANN module in details while presenting the design, implementation, and simulation of the module. Similarly, chapter 5 presents the same sections on the second module which is fuzzy‐neural networks. Both chapters 5 and 6 compare the module results with international results from the literature. Finally, we conclude with chapter 6 which wraps up the project and presents a section on ethical considerations.
11
Chapter 2 Background The objective of this chapter is to introduce the ECG signal that is the main subject of the project. The electrocardiogram is very helpful in the diagnosis of cardiac diseases since they often result in ECG abnormalities. To detect such abnormalities as PVC (Premature Ventricular Contraction), a variety of methods have been used in the literature. In this section, we will review the methods that we have implemented in our project, namely artificial neural networks and hybrid fuzzy‐neuro networks. 2.1 The Electrocardiogram and Its
Characteristics
The heart is the most vital organ of the human body since it acts as a pump that pushes oxygen‐rich blood to the organs, cells, and tissues of the body. Every heart beat is caused by electrical impulses from the heart muscle that cause the atria and then the ventricles to contract and consequently pump blood to the lungs and the rest of the body. This electrical activity of the heart is measured by the electrocardiogram which serves as a means to detect for irregular heart conditions and possibly heart diseases. Electrocardiography has evolved over time and is becoming more accurate as it is being automated by making use of the several software QRS detection techniques available.

12
2.1.1 The Heart and Electrocardiogram
The electrical signal that stimulates the heart beat starts from the sinoatrial‐node (SA) which is known as the heart’s “natural pacemaker” and is located at the top of the right chamber or atrium (RA) as shown in Figure 2.1. This signal branches through both atria, causing them to contract and pump blood to the lower chambers, the ventricles, where the signal continues via the atrioventricular node (AV). If the pacemaker is disrupted, the heart may beat at an abnormal rate, impacting the circulation of blood throughout the body. [A,B] Figure 2.1: The conduction System
The electrical signals described above are measured by the electrocardiogram or ECG where each heart beat is displayed as a series of electrical waves characterized by peaks and valleys. Therefore it is important to record the ECG signal since it allows for the detection of abnormalities or diseases in the heart. The recording of the ECG usually takes place by placing electrodes to measure potentials on the surface of specific body parts usually the arms, legs and the chest. Figure 2.2 below shows the typical procedure for clinical ECG tracing of patients.
Figure 2.2: ECG tracing
13
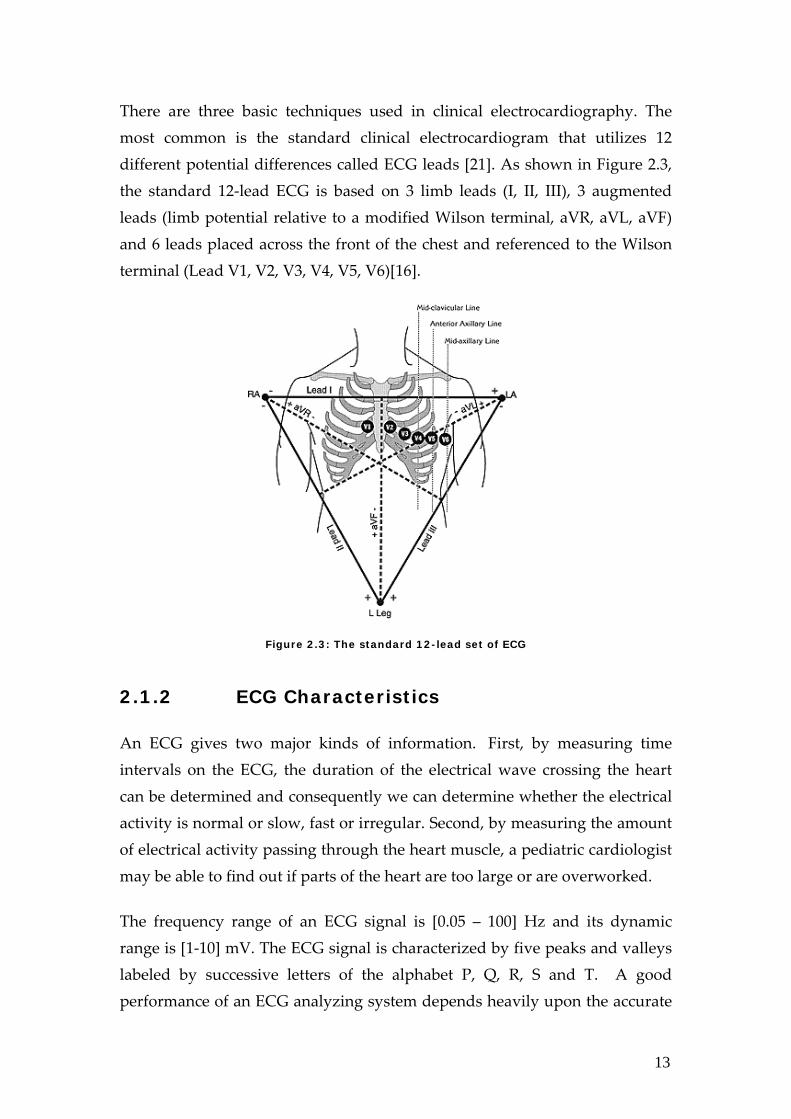
There are three basic techniques used in clinical electrocardiography. The most common is the standard clinical electrocardiogram that utilizes 12 different potential differences called ECG leads [21]. As shown in Figure 2.3, the standard 12‐lead ECG is based on 3 limb leads (I, II, III), 3 augmented leads (limb potential relative to a modified Wilson terminal, aVR, aVL, aVF) and 6 leads placed across the front of the chest and referenced to the Wilson terminal (Lead V1, V2, V3, V4, V5, V6)[16].
Figure 2.3: The standard 12-lead set of ECG
2.1.2 ECG Characteristics
An ECG gives two major kinds of information. First, by measuring time intervals on the ECG, the duration of the electrical wave crossing the heart can be determined and consequently we can determine whether the electrical activity is normal or slow, fast or irregular. Second, by measuring the amount of electrical activity passing through the heart muscle, a pediatric cardiologist may be able to find out if parts of the heart are too large or are overworked.
The frequency range of an ECG signal is [0.05 – 100] Hz and its dynamic range is [1‐10] mV. The ECG signal is characterized by five peaks and valleys labeled by successive letters of the alphabet P, Q, R, S and T. A good performance of an ECG analyzing system depends heavily upon the accurate
14
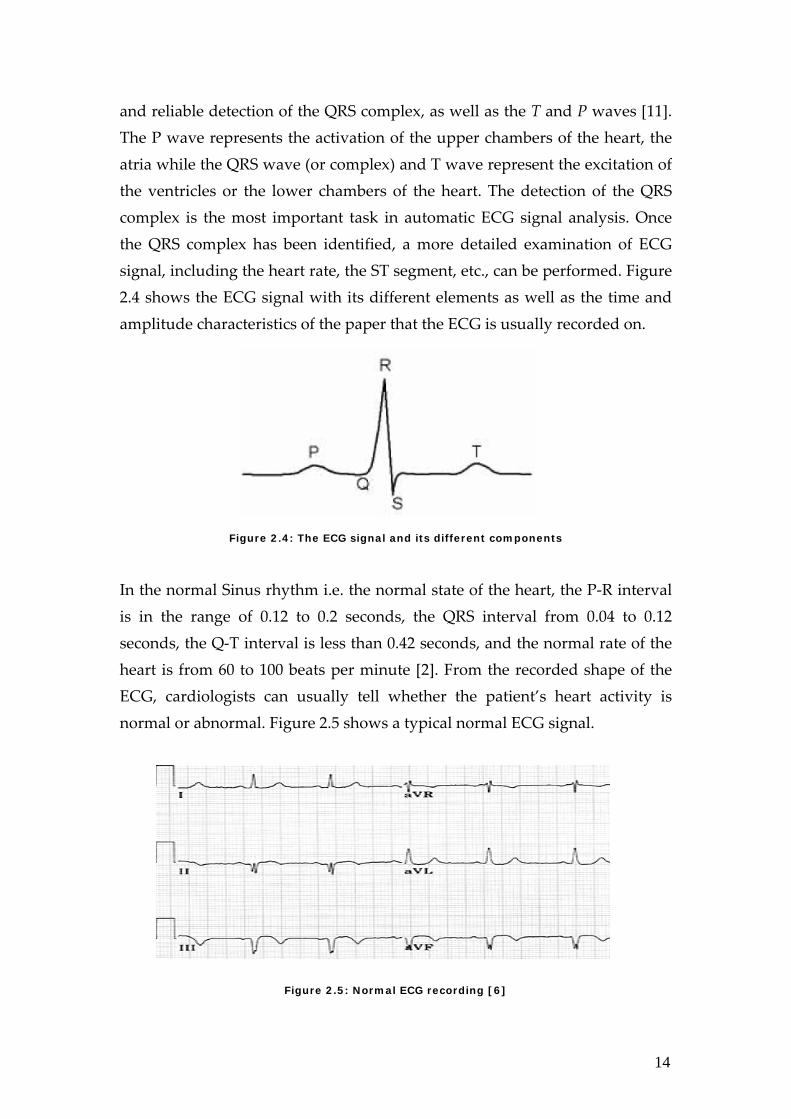
and reliable detection of the QRS complex, as well as the T and P waves [11]. The P wave represents the activation of the upper chambers of the heart, the atria while the QRS wave (or complex) and T wave represent the excitation of the ventricles or the lower chambers of the heart. The detection of the QRS complex is the most important task in automatic ECG signal analysis. Once the QRS complex has been identified, a more detailed examination of ECG signal, including the heart rate, the ST segment, etc., can be performed. Figure 2.4 shows the ECG signal with its different elements as well as the time and amplitude characteristics of the paper that the ECG is usually recorded on.
Figure 2.4: The ECG signal and its different components
In the normal Sinus rhythm i.e. the normal state of the heart, the P‐R interval is in the range of 0.12 to 0.2 seconds, the QRS interval from 0.04 to 0.12 seconds, the Q‐T interval is less than 0.42 seconds, and the normal rate of the heart is from 60 to 100 beats per minute [2]. From the recorded shape of the ECG, cardiologists can usually tell whether the patient’s heart activity is normal or abnormal. Figure 2.5 shows a typical normal ECG signal.
Figure 2.5: Normal ECG recording [6]
15
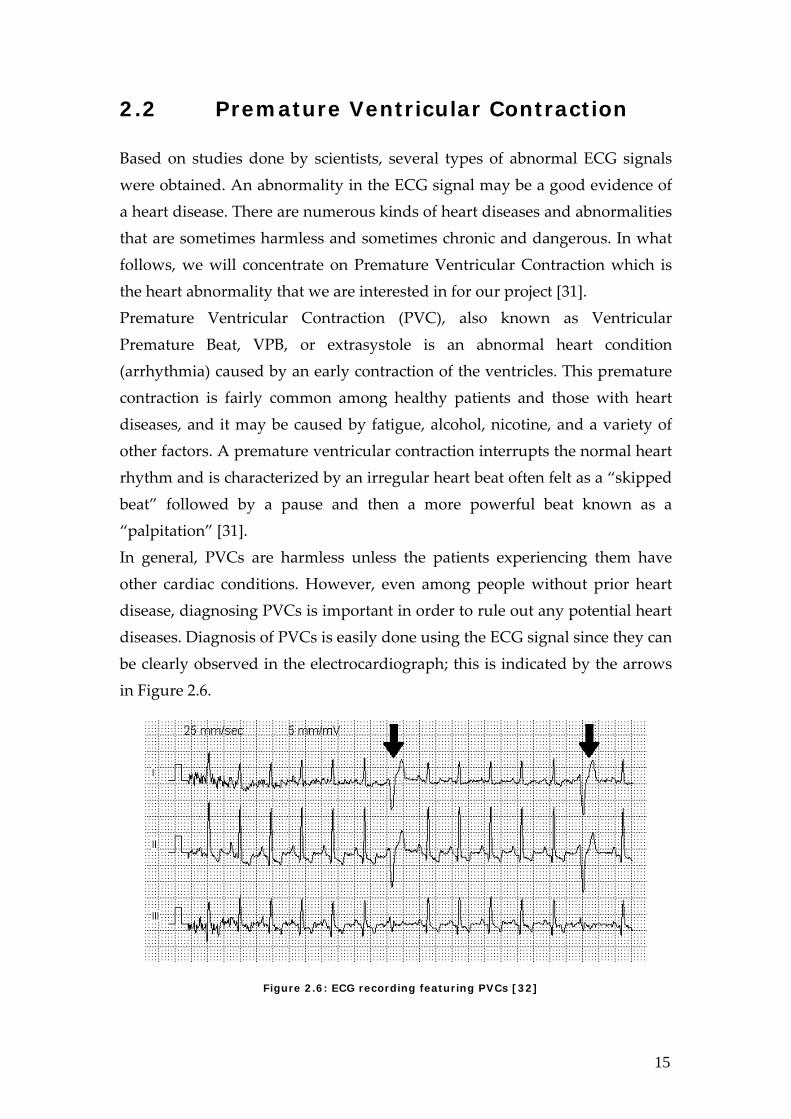
2.2 Premature Ventricular Contraction Based on studies done by scientists, several types of abnormal ECG signals were obtained. An abnormality in the ECG signal may be a good evidence of a heart disease. There are numerous kinds of heart diseases and abnormalities that are sometimes harmless and sometimes chronic and dangerous. In what follows, we will concentrate on Premature Ventricular Contraction which is the heart abnormality that we are interested in for our project [31]. Premature Ventricular Contraction (PVC), also known as Ventricular Premature Beat, VPB, or extrasystole is an abnormal heart condition (arrhythmia) caused by an early contraction of the ventricles. This premature contraction is fairly common among healthy patients and those with heart diseases, and it may be caused by fatigue, alcohol, nicotine, and a variety of other factors. A premature ventricular contraction interrupts the normal heart rhythm and is characterized by an irregular heart beat often felt as a “skipped beat” followed by a pause and then a more powerful beat known as a “palpitation” [31]. In general, PVCs are harmless unless the patients experiencing them have other cardiac conditions. However, even among people without prior heart disease, diagnosing PVCs is important in order to rule out any potential heart diseases. Diagnosis of PVCs is easily done using the ECG signal since they can be clearly observed in the electrocardiograph; this is indicated by the arrows in Figure 2.6.
Figure 2.6: ECG recording featuring PVCs [32]
16
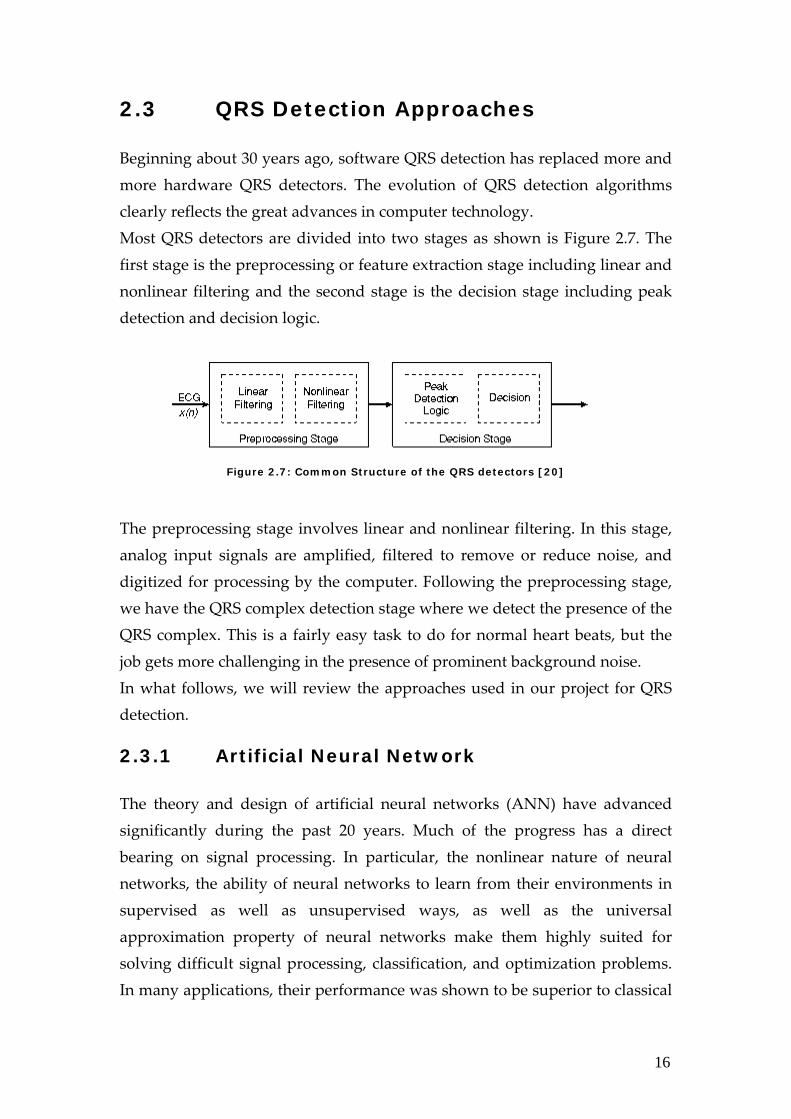
2.3 QRS Detection Approaches Beginning about 30 years ago, software QRS detection has replaced more and more hardware QRS detectors. The evolution of QRS detection algorithms clearly reflects the great advances in computer technology. Most QRS detectors are divided into two stages as shown is Figure 2.7. The first stage is the preprocessing or feature extraction stage including linear and nonlinear filtering and the second stage is the decision stage including peak detection and decision logic.
Figure 2.7: Common Structure of the QRS detectors [20]
The preprocessing stage involves linear and nonlinear filtering. In this stage, analog input signals are amplified, filtered to remove or reduce noise, and digitized for processing by the computer. Following the preprocessing stage, we have the QRS complex detection stage where we detect the presence of the QRS complex. This is a fairly easy task to do for normal heart beats, but the job gets more challenging in the presence of prominent background noise. In what follows, we will review the approaches used in our project for QRS detection. 2.3.1 Artificial Neural Network The theory and design of artificial neural networks (ANN) have advanced significantly during the past 20 years. Much of the progress has a direct bearing on signal processing. In particular, the nonlinear nature of neural networks, the ability of neural networks to learn from their environments in supervised as well as unsupervised ways, as well as the universal approximation property of neural networks make them highly suited for solving difficult signal processing, classification, and optimization problems. In many applications, their performance was shown to be superior to classical
17
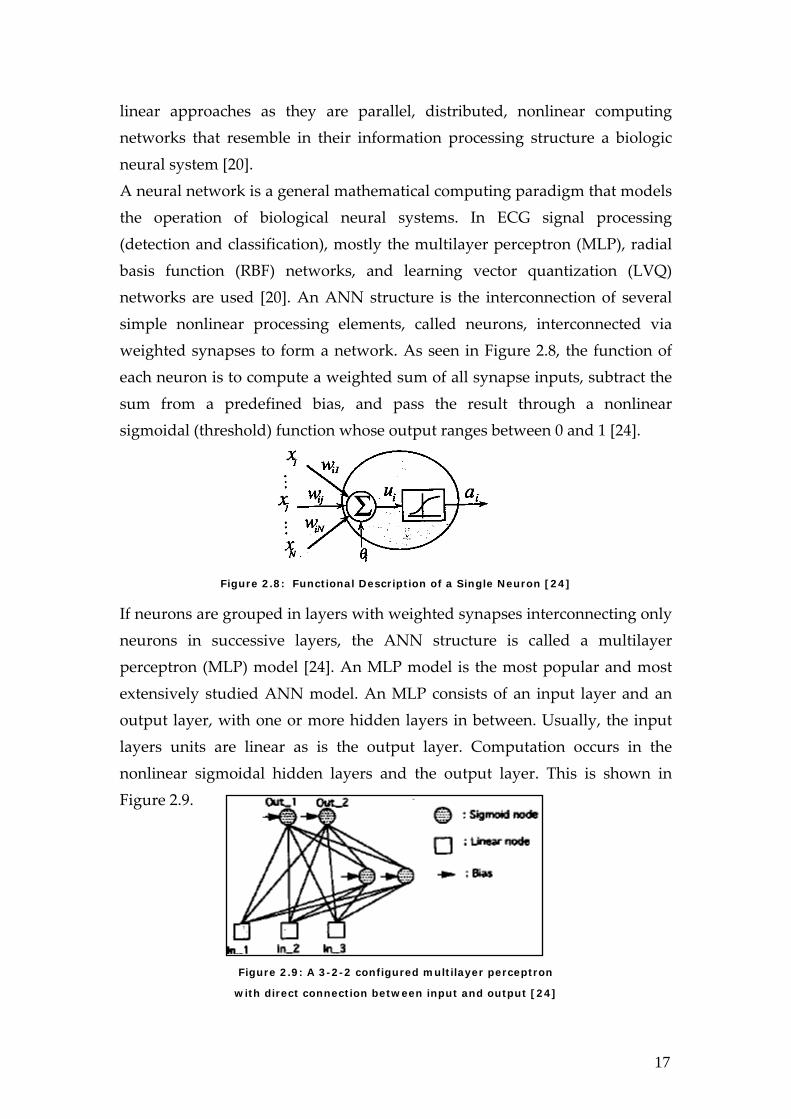
linear approaches as they are parallel, distributed, nonlinear computing networks that resemble in their information processing structure a biologic neural system [20]. A neural network is a general mathematical computing paradigm that models the operation of biological neural systems. In ECG signal processing (detection and classification), mostly the multilayer perceptron (MLP), radial basis function (RBF) networks, and learning vector quantization (LVQ) networks are used [20]. An ANN structure is the interconnection of several simple nonlinear processing elements, called neurons, interconnected via weighted synapses to form a network. As seen in Figure 2.8, the function of each neuron is to compute a weighted sum of all synapse inputs, subtract the sum from a predefined bias, and pass the result through a nonlinear sigmoidal (threshold) function whose output ranges between 0 and 1 [24].
Figure 2.8: Functional Description of a Single Neuron [24]
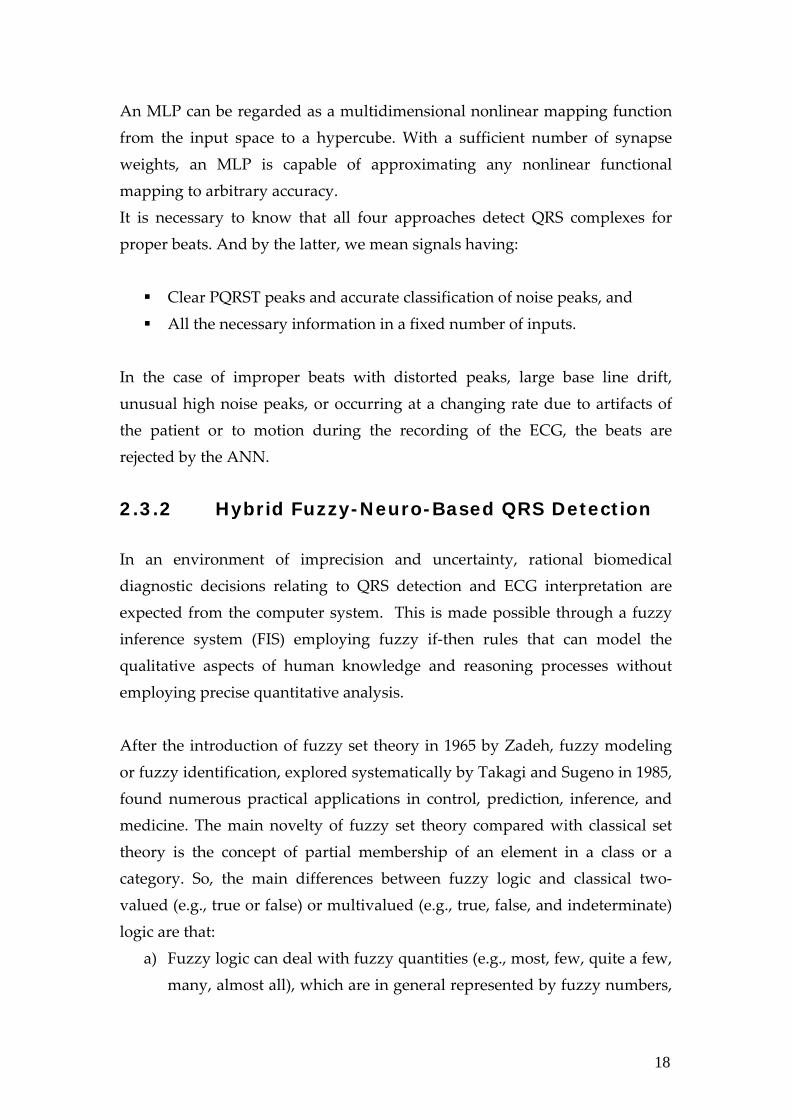
If neurons are grouped in layers with weighted synapses interconnecting only neurons in successive layers, the ANN structure is called a multilayer perceptron (MLP) model [24]. An MLP model is the most popular and most extensively studied ANN model. An MLP consists of an input layer and an output layer, with one or more hidden layers in between. Usually, the input layers units are linear as is the output layer. Computation occurs in the nonlinear sigmoidal hidden layers and the output layer. This is shown in Figure 2.9.
Figure 2.9: A 3-2-2 configured multilayer perceptron
with direct connection between input and output [24]
18
An MLP can be regarded as a multidimensional nonlinear mapping function from the input space to a hypercube. With a sufficient number of synapse weights, an MLP is capable of approximating any nonlinear functional mapping to arbitrary accuracy. It is necessary to know that all four approaches detect QRS complexes for proper beats. And by the latter, we mean signals having:
Clear PQRST peaks and accurate classification of noise peaks, and All the necessary information in a fixed number of inputs.
In the case of improper beats with distorted peaks, large base line drift, unusual high noise peaks, or occurring at a changing rate due to artifacts of the patient or to motion during the recording of the ECG, the beats are rejected by the ANN.
2.3.2 Hybrid Fuzzy-Neuro-Based QRS Detection In an environment of imprecision and uncertainty, rational biomedical diagnostic decisions relating to QRS detection and ECG interpretation are expected from the computer system. This is made possible through a fuzzy inference system (FIS) employing fuzzy if‐then rules that can model the qualitative aspects of human knowledge and reasoning processes without employing precise quantitative analysis. After the introduction of fuzzy set theory in 1965 by Zadeh, fuzzy modeling or fuzzy identification, explored systematically by Takagi and Sugeno in 1985, found numerous practical applications in control, prediction, inference, and medicine. The main novelty of fuzzy set theory compared with classical set theory is the concept of partial membership of an element in a class or a category. So, the main differences between fuzzy logic and classical two‐valued (e.g., true or false) or multivalued (e.g., true, false, and indeterminate) logic are that:
a) Fuzzy logic can deal with fuzzy quantities (e.g., most, few, quite a few, many, almost all), which are in general represented by fuzzy numbers,
19
fuzzy predicates (e.g., expensive, rare), and fuzzy modifiers (e.g., extremely, unlikely).
b) The notions of truth and false are both allowed to be fuzzy using fuzzy true/false values (e.g., very true, mostly false). Then, the ultimate goal of fuzzy logic is to provide foundations for approximate reasoning.
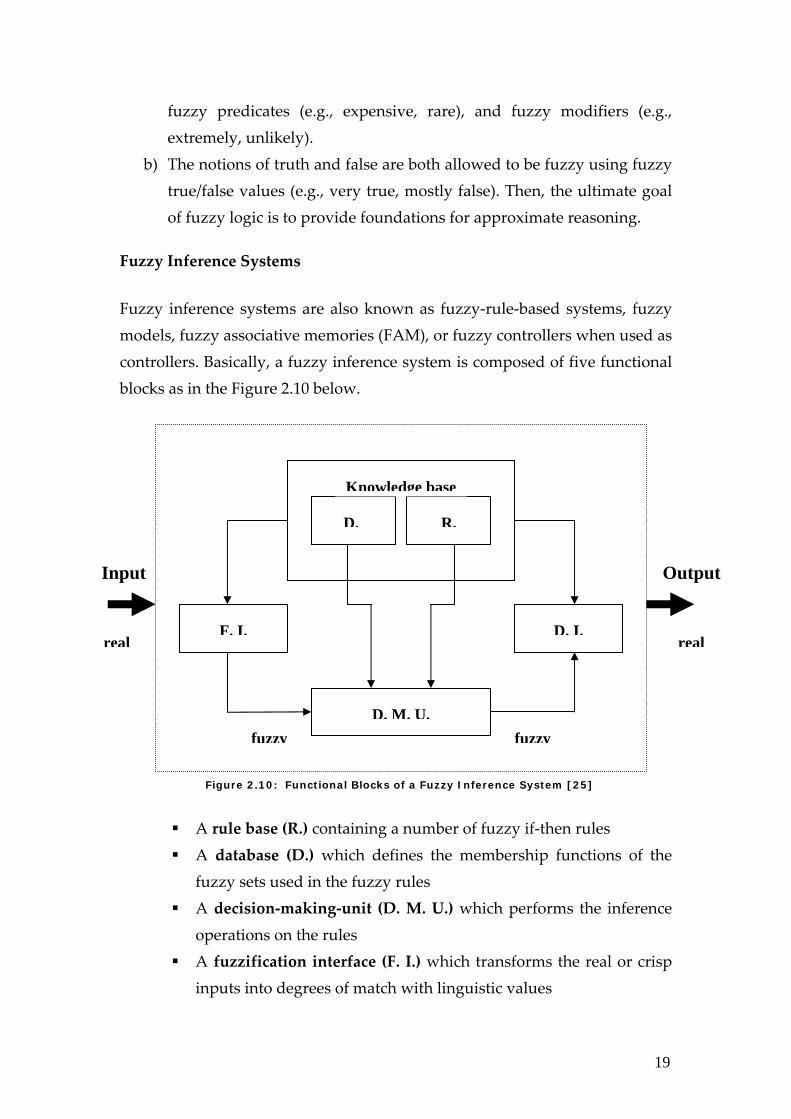
Fuzzy Inference Systems Fuzzy inference systems are also known as fuzzy‐rule‐based systems, fuzzy models, fuzzy associative memories (FAM), or fuzzy controllers when used as controllers. Basically, a fuzzy inference system is composed of five functional blocks as in the Figure 2.10 below.
Figure 2.10: Functional Blocks of a Fuzzy Inference System [25]
A rule base (R.) containing a number of fuzzy if‐then rules A database (D.) which defines the membership functions of the fuzzy sets used in the fuzzy rules
A decision‐making‐unit (D. M. U.) which performs the inference operations on the rules
A fuzzification interface (F. I.) which transforms the real or crisp inputs into degrees of match with linguistic values
F. I. D. I.
D. M. U.
D. R.
Knowledge base
fuzzyfuzzy
Input Output
real real

20
A Defuzzification interface (D. I.) which transforms the fuzzy results of the inference into a crisp output
Usually the rule base and the database are jointly referred to as the knowledge base.
In Figure 2.11 below, we present the structure of a hybrid fuzzy‐neuro‐based network.
Figure 2.11: The structure of a hybrid fuzzy-neuro-based network [18]
This structure is a generalization of the so‐called Hecht‐Nielsen counterpropagation network with the fuzzy self‐organizing layer replacing the Kohonen layer and the MLP subnetwork in place of the Grossberg layer. Figure 2.12 below reveals the task that the self‐organizing fuzzy clustering
algorithm performs.
Figure 2.12 The performance of the G-K algorithm of the self organization to the recognition of clusters
(a) Original Data, (b) Recognized transformed classes [18]
21
Chapter 3 Foundation In this chapter we cover all the steps that preceded project implementation. A major element of the foundation stage was the extraction of ECG signals from the standard database that we have chosen for our project. After extraction, the signals were subject to preprocessing using several tools available by the MATLAB software, the primary implementation software of our final year project. 3.1 The ECG Database
The role of a standard database is very important in evaluating the performance of QRS detection algorithms. A standard or a benchmark database is a well annotated and validated database that is made available for academic and industrial groups for testing and result‐comparison in different applications. ECG databases have been present for a long time now and because they contain a large number of signals that are representative of the large variety of ECGs as well as the rarely observed but clinically important signals, they have been used throughout the literature of QRS detection algorithms in producing and comparing results. It is easy to obtain and make use of ECG data from local hospitals to base work on them; however any results obtained using such data can not be evaluated fairly because of the lack of approved works that use the same data. This is why it is very important to us to select a standard ECG database to base our work on. For a number of years, researchers worldwide have been investigating methods for real‐time ECG rhythm analysis and for that sake standard
22
databases and especially the MIT‐BIH Arrhythmia Database have been an enormous help for the development and evaluation of ECG classification and detection algorithms. We have selected the MIT‐BIH database to base our work on because it is available online where the ECG files are easily accessible and because many important works in the literature have based their work on this database and have reported their results and findings in published and widely acknowledged papers.
Figure 3.1: The MIT-BIH Arrhythmia Database [1]
The MIT‐BIH database is a very popular database that is provided by MIT and Boston’s Beth Israel Hospital. It consists of ten databases that serve different test purposes and the most frequently used database among the others is the Arrhythmia Database that contains 48 half‐hour recordings of two‐channel ambulatory ECG [20]. These recordings were obtained from 47 subjects studied between 1975 and 1979 by the BIH Arrhythmia Laboratory. Out of the 48 recordings, 25 were chosen from numerous ambulatory ECG recordings whereas the rest was randomly selected from a mixed population of patients varying between inpatients (60%) and outpatients (40%) [1]. There are more than a hundred thousand QRS complexes in this database and the detection of these complexes varies from straight‐forward to difficult according to the different levels of abnormality, noise and artifacts. The data of the
23
database consists of annotated ECG sampled at a rate of 360 Hz with 11‐bit resolution over a 10 mV range [1]. Included with the database is the annotations reference which explains approximately 110,000 annotations [1,20].
The data gathering of the MIT‐BIH Arrhythmia Database has started since 1975 but the first distribution has taken place only in 1980. Only recently, February 2005, the full data became available online on PhysioNet’s webpage www.physionet.org as one of physiobank’s databases. 3.2 ECG Signal Extraction
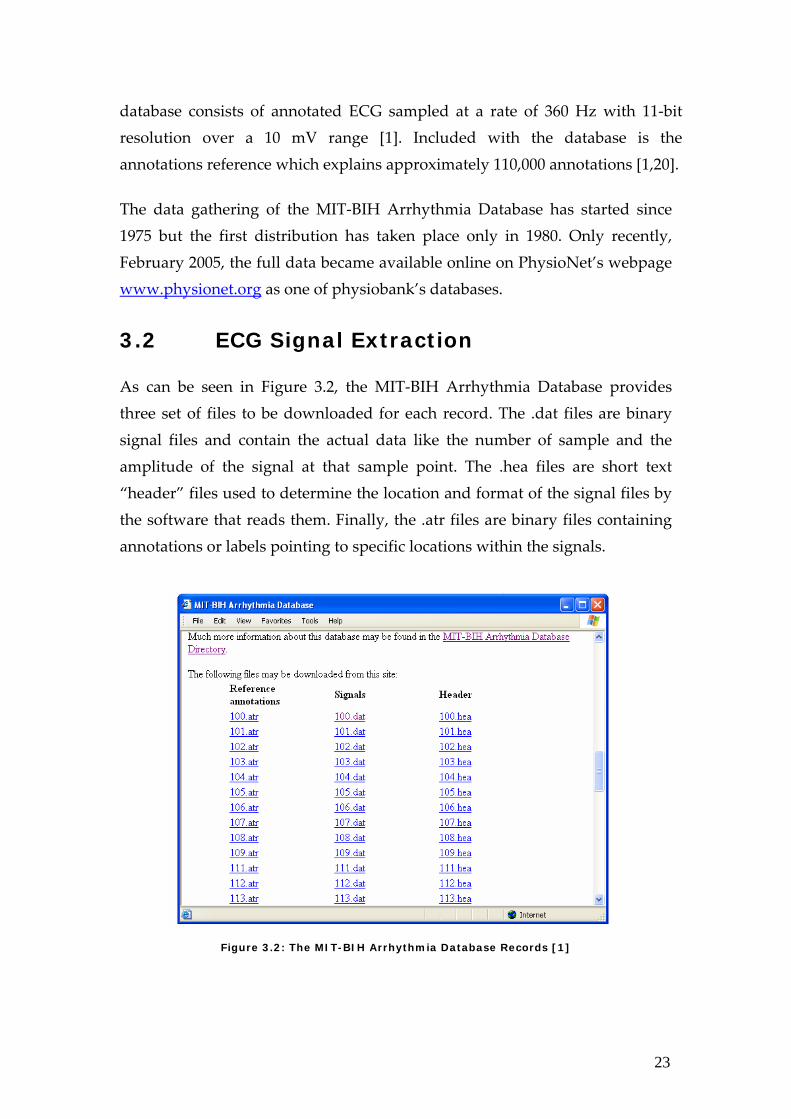
As can be seen in Figure 3.2, the MIT‐BIH Arrhythmia Database provides three set of files to be downloaded for each record. The .dat files are binary signal files and contain the actual data like the number of sample and the amplitude of the signal at that sample point. The .hea files are short text “header” files used to determine the location and format of the signal files by the software that reads them. Finally, the .atr files are binary files containing annotations or labels pointing to specific locations within the signals.
Figure 3.2: The MIT-BIH Arrhythmia Database Records [1]
24
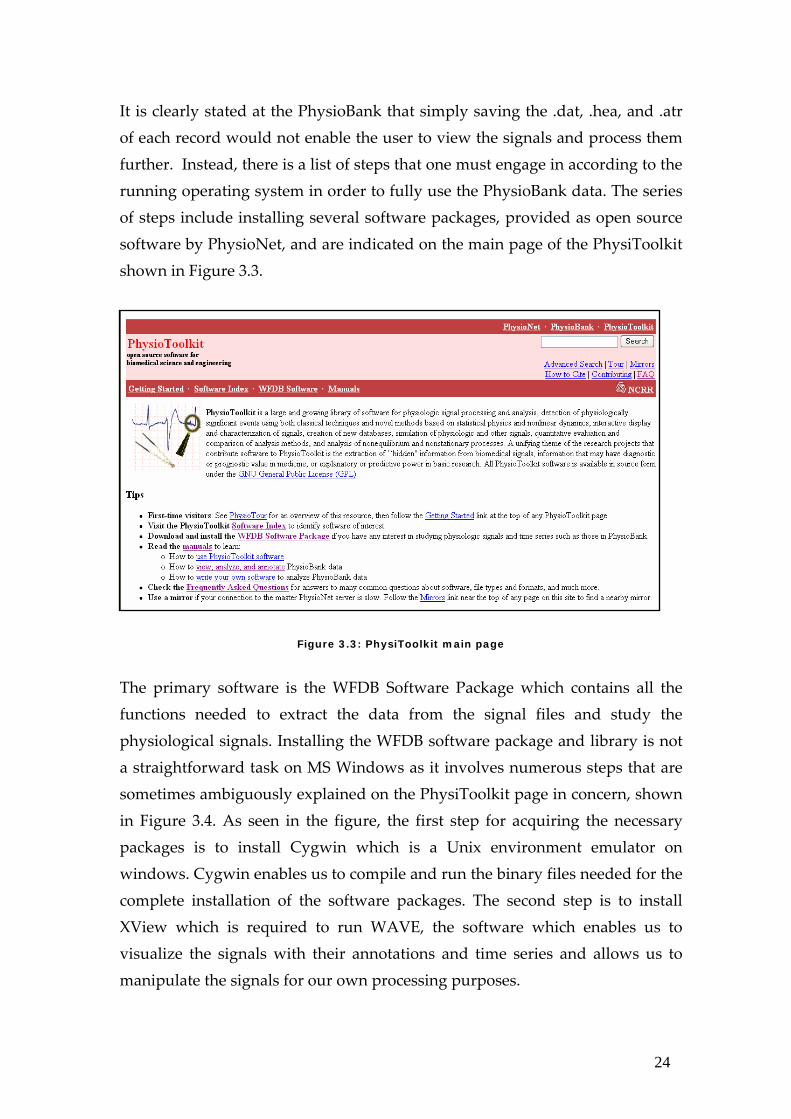
It is clearly stated at the PhysioBank that simply saving the .dat, .hea, and .atr of each record would not enable the user to view the signals and process them further. Instead, there is a list of steps that one must engage in according to the running operating system in order to fully use the PhysioBank data. The series of steps include installing several software packages, provided as open source software by PhysioNet, and are indicated on the main page of the PhysiToolkit shown in Figure 3.3.
Figure 3.3: PhysiToolkit main page
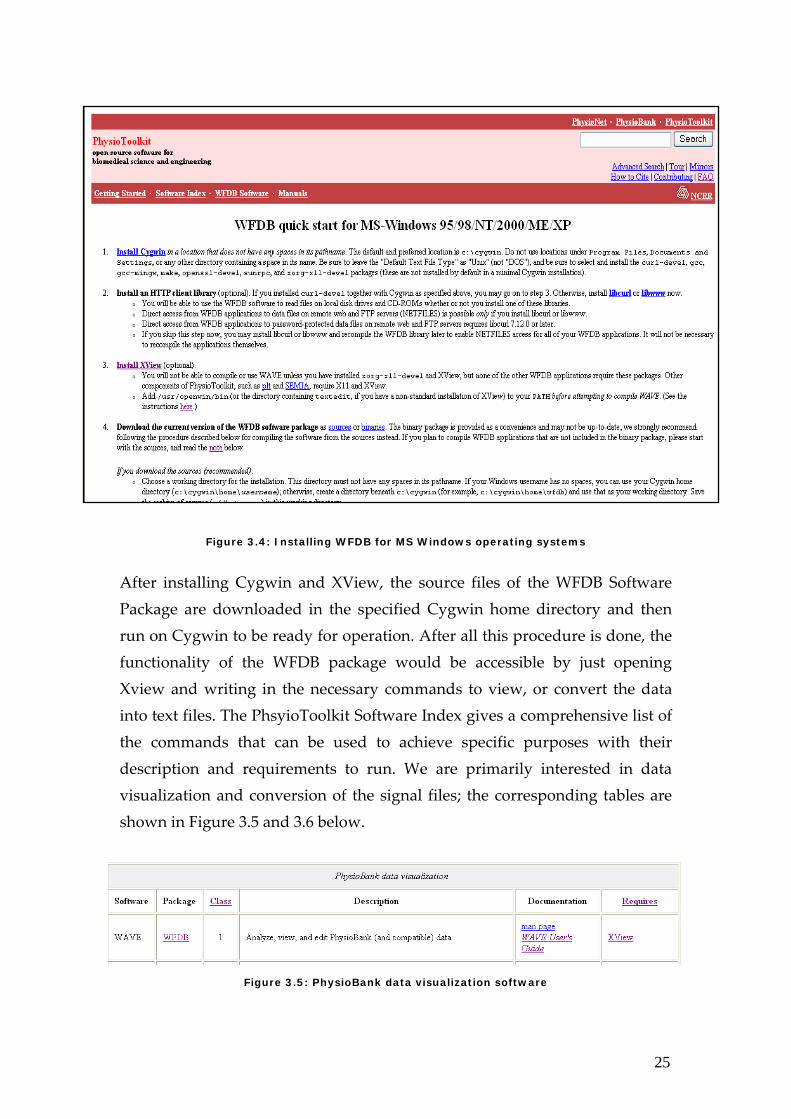
The primary software is the WFDB Software Package which contains all the functions needed to extract the data from the signal files and study the physiological signals. Installing the WFDB software package and library is not a straightforward task on MS Windows as it involves numerous steps that are sometimes ambiguously explained on the PhysiToolkit page in concern, shown in Figure 3.4. As seen in the figure, the first step for acquiring the necessary packages is to install Cygwin which is a Unix environment emulator on windows. Cygwin enables us to compile and run the binary files needed for the complete installation of the software packages. The second step is to install XView which is required to run WAVE, the software which enables us to visualize the signals with their annotations and time series and allows us to manipulate the signals for our own processing purposes.
25
Figure 3.4: Installing WFDB for MS Windows operating systems
After installing Cygwin and XView, the source files of the WFDB Software Package are downloaded in the specified Cygwin home directory and then run on Cygwin to be ready for operation. After all this procedure is done, the functionality of the WFDB package would be accessible by just opening Xview and writing in the necessary commands to view, or convert the data into text files. The PhsyioToolkit Software Index gives a comprehensive list of the commands that can be used to achieve specific purposes with their description and requirements to run. We are primarily interested in data visualization and conversion of the signal files; the corresponding tables are shown in Figure 3.5 and 3.6 below.
Figure 3.5: PhysioBank data visualization software
26
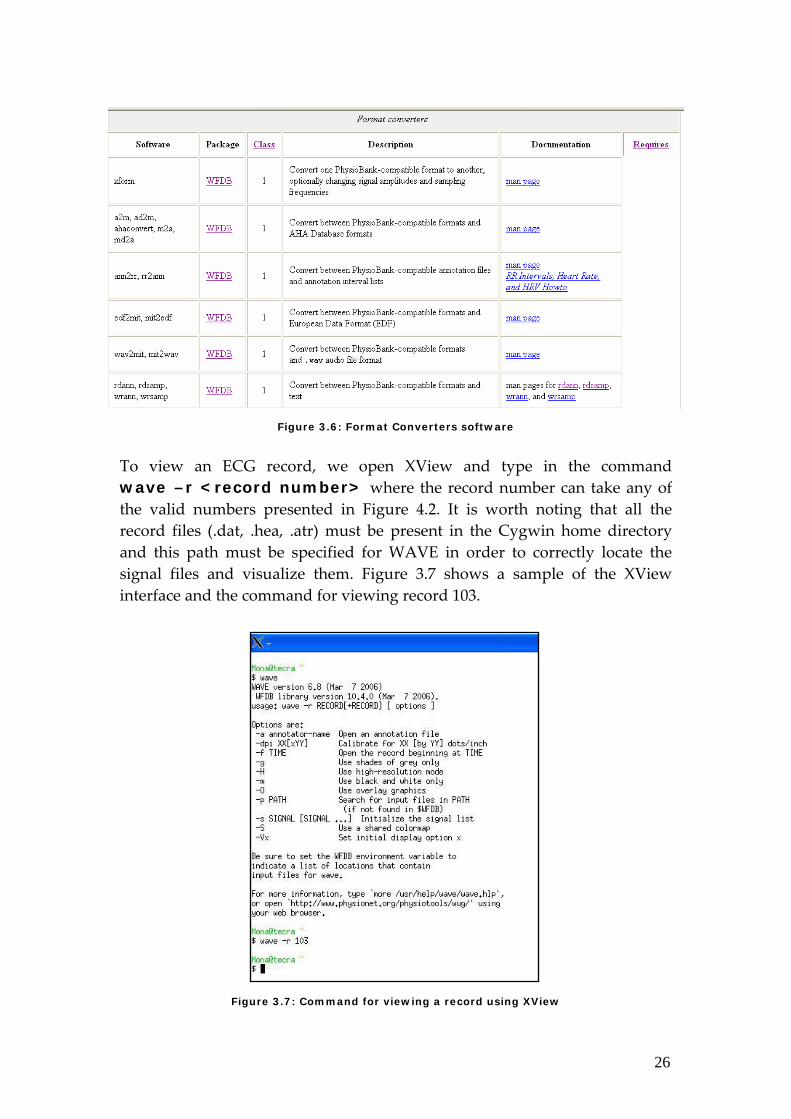
Figure 3.6: Format Converters software
To view an ECG record, we open XView and type in the command wave –r <record number> where the record number can take any of the valid numbers presented in Figure 4.2. It is worth noting that all the record files (.dat, .hea, .atr) must be present in the Cygwin home directory and this path must be specified for WAVE in order to correctly locate the signal files and visualize them. Figure 3.7 shows a sample of the XView interface and the command for viewing record 103.
Figure 3.7: Command for viewing a record using XView
27
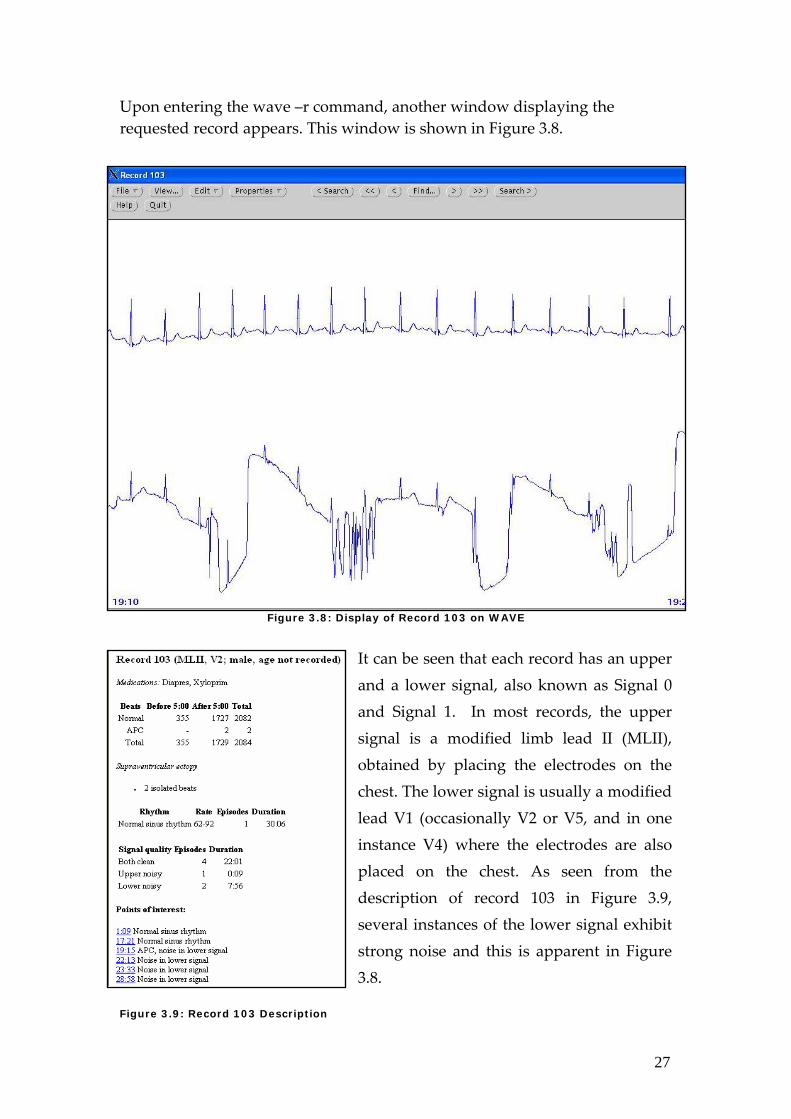
Upon entering the wave –r command, another window displaying the requested record appears. This window is shown in Figure 3.8.
Figure 3.8: Display of Record 103 on WAVE
It can be seen that each record has an upper and a lower signal, also known as Signal 0 and Signal 1. In most records, the upper signal is a modified limb lead II (MLII), obtained by placing the electrodes on the chest. The lower signal is usually a modified lead V1 (occasionally V2 or V5, and in one instance V4) where the electrodes are also placed on the chest. As seen from the description of record 103 in Figure 3.9, several instances of the lower signal exhibit strong noise and this is apparent in Figure 3.8.
Figure 3.9: Record 103 Description
28
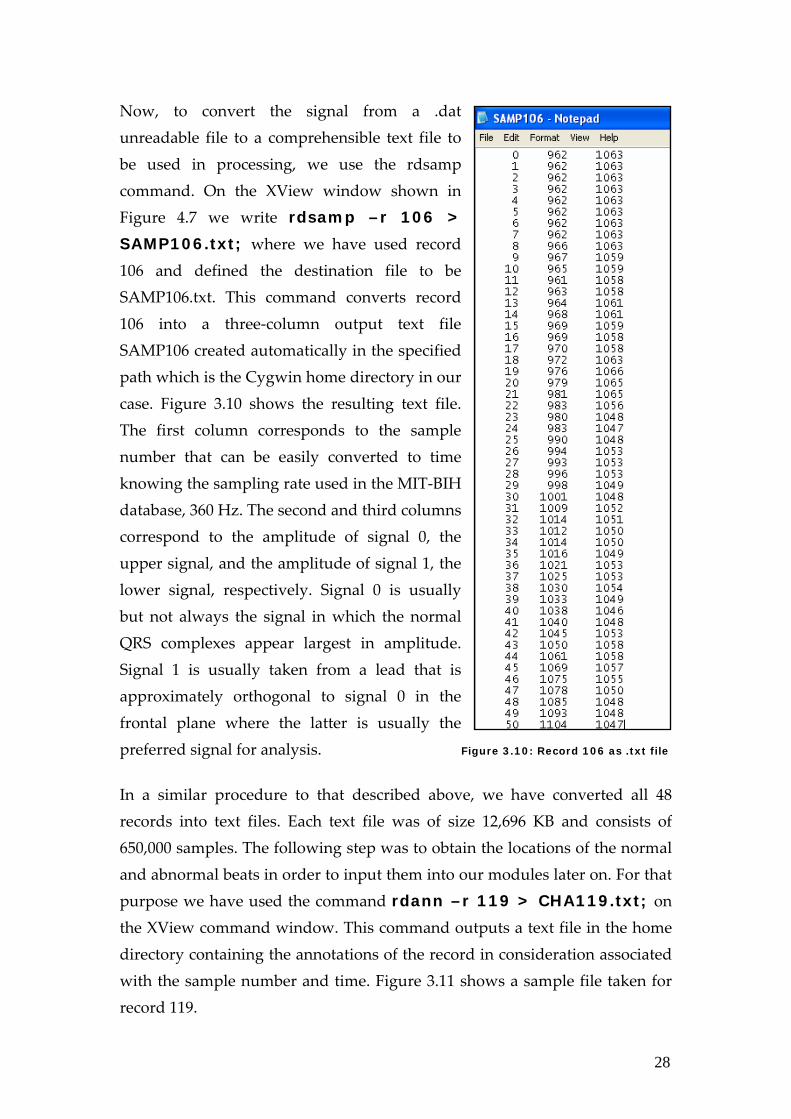
Now, to convert the signal from a .dat unreadable file to a comprehensible text file to be used in processing, we use the rdsamp command. On the XView window shown in Figure 4.7 we write rdsamp –r 106 >
SAMP106.txt; where we have used record 106 and defined the destination file to be SAMP106.txt. This command converts record 106 into a three‐column output text file SAMP106 created automatically in the specified path which is the Cygwin home directory in our case. Figure 3.10 shows the resulting text file. The first column corresponds to the sample number that can be easily converted to time knowing the sampling rate used in the MIT‐BIH database, 360 Hz. The second and third columns correspond to the amplitude of signal 0, the upper signal, and the amplitude of signal 1, the lower signal, respectively. Signal 0 is usually but not always the signal in which the normal QRS complexes appear largest in amplitude. Signal 1 is usually taken from a lead that is approximately orthogonal to signal 0 in the frontal plane where the latter is usually the preferred signal for analysis. Figure 3.10: Record 106 as .txt file
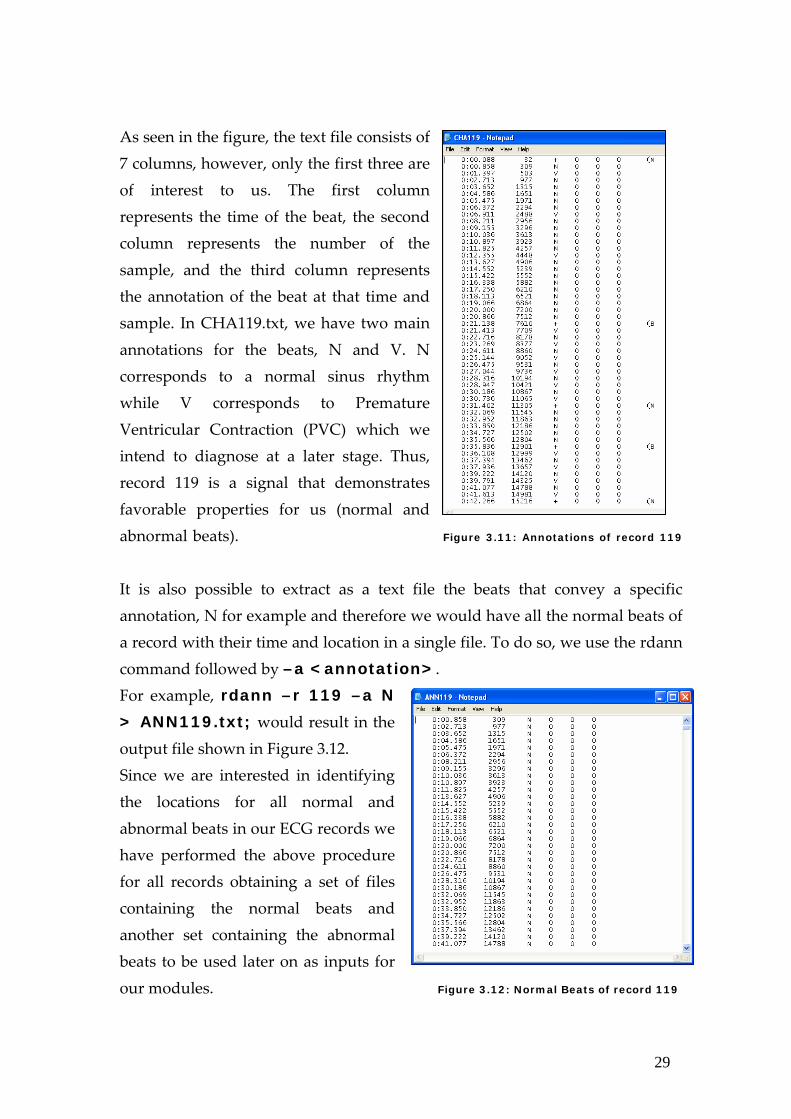
In a similar procedure to that described above, we have converted all 48 records into text files. Each text file was of size 12,696 KB and consists of 650,000 samples. The following step was to obtain the locations of the normal and abnormal beats in order to input them into our modules later on. For that purpose we have used the command rdann –r 119 > CHA119.txt; on the XView command window. This command outputs a text file in the home directory containing the annotations of the record in consideration associated with the sample number and time. Figure 3.11 shows a sample file taken for record 119.
29
As seen in the figure, the text file consists of 7 columns, however, only the first three are of interest to us. The first column represents the time of the beat, the second column represents the number of the sample, and the third column represents the annotation of the beat at that time and sample. In CHA119.txt, we have two main annotations for the beats, N and V. N corresponds to a normal sinus rhythm while V corresponds to Premature Ventricular Contraction (PVC) which we intend to diagnose at a later stage. Thus, record 119 is a signal that demonstrates favorable properties for us (normal and abnormal beats). Figure 3.11: Annotations of record 119
It is also possible to extract as a text file the beats that convey a specific annotation, N for example and therefore we would have all the normal beats of a record with their time and location in a single file. To do so, we use the rdann command followed by –a <annotation>. For example, rdann –r 119 –a N
> ANN119.txt; would result in the output file shown in Figure 3.12. Since we are interested in identifying the locations for all normal and abnormal beats in our ECG records we have performed the above procedure for all records obtaining a set of files containing the normal beats and another set containing the abnormal beats to be used later on as inputs for our modules. Figure 3.12: Normal Beats of record 119
30
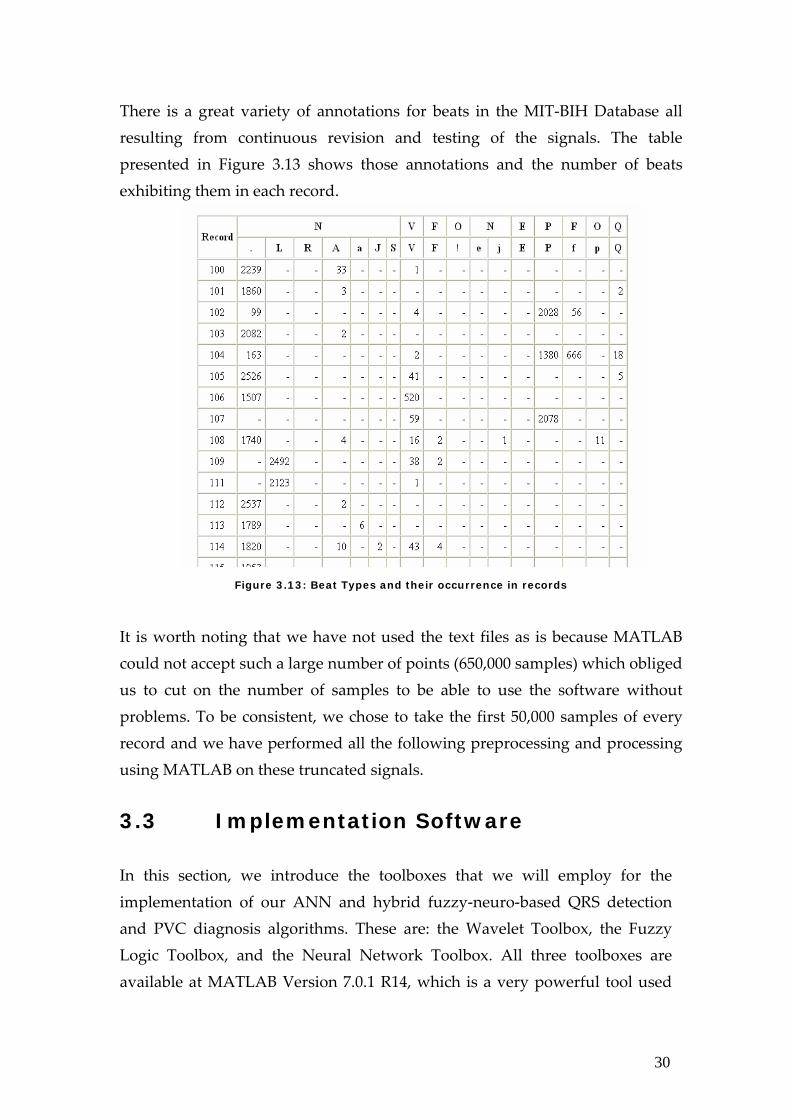
There is a great variety of annotations for beats in the MIT‐BIH Database all resulting from continuous revision and testing of the signals. The table presented in Figure 3.13 shows those annotations and the number of beats exhibiting them in each record.
Figure 3.13: Beat Types and their occurrence in records
It is worth noting that we have not used the text files as is because MATLAB could not accept such a large number of points (650,000 samples) which obliged us to cut on the number of samples to be able to use the software without problems. To be consistent, we chose to take the first 50,000 samples of every record and we have performed all the following preprocessing and processing using MATLAB on these truncated signals. 3.3 Implementation Software In this section, we introduce the toolboxes that we will employ for the implementation of our ANN and hybrid fuzzy‐neuro‐based QRS detection and PVC diagnosis algorithms. These are: the Wavelet Toolbox, the Fuzzy Logic Toolbox, and the Neural Network Toolbox. All three toolboxes are available at MATLAB Version 7.0.1 R14, which is a very powerful tool used
31
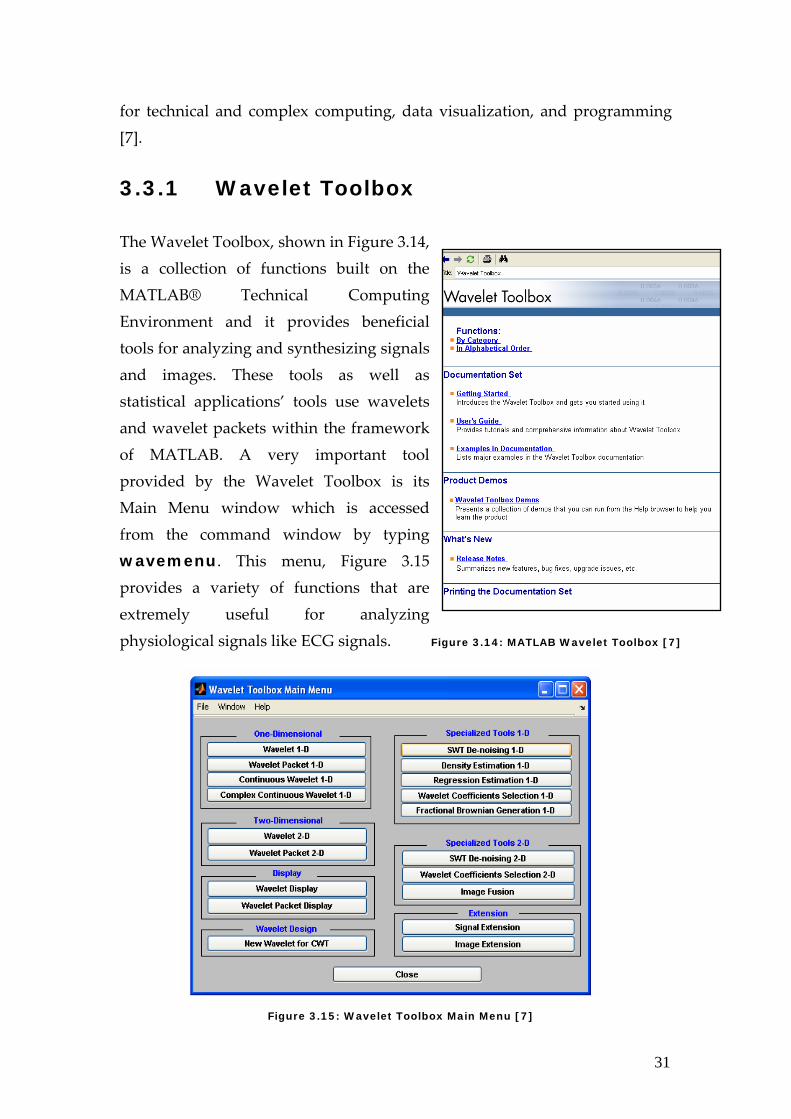
for technical and complex computing, data visualization, and programming [7]. 3.3.1 Wavelet Toolbox The Wavelet Toolbox, shown in Figure 3.14, is a collection of functions built on the MATLAB® Technical Computing Environment and it provides beneficial tools for analyzing and synthesizing signals and images. These tools as well as statistical applications’ tools use wavelets and wavelet packets within the framework of MATLAB. A very important tool provided by the Wavelet Toolbox is its Main Menu window which is accessed from the command window by typing wavemenu. This menu, Figure 3.15 provides a variety of functions that are extremely useful for analyzing physiological signals like ECG signals. Figure 3.14: MATLAB Wavelet Toolbox [7]
Figure 3.15: Wavelet Toolbox Main Menu [7]
32
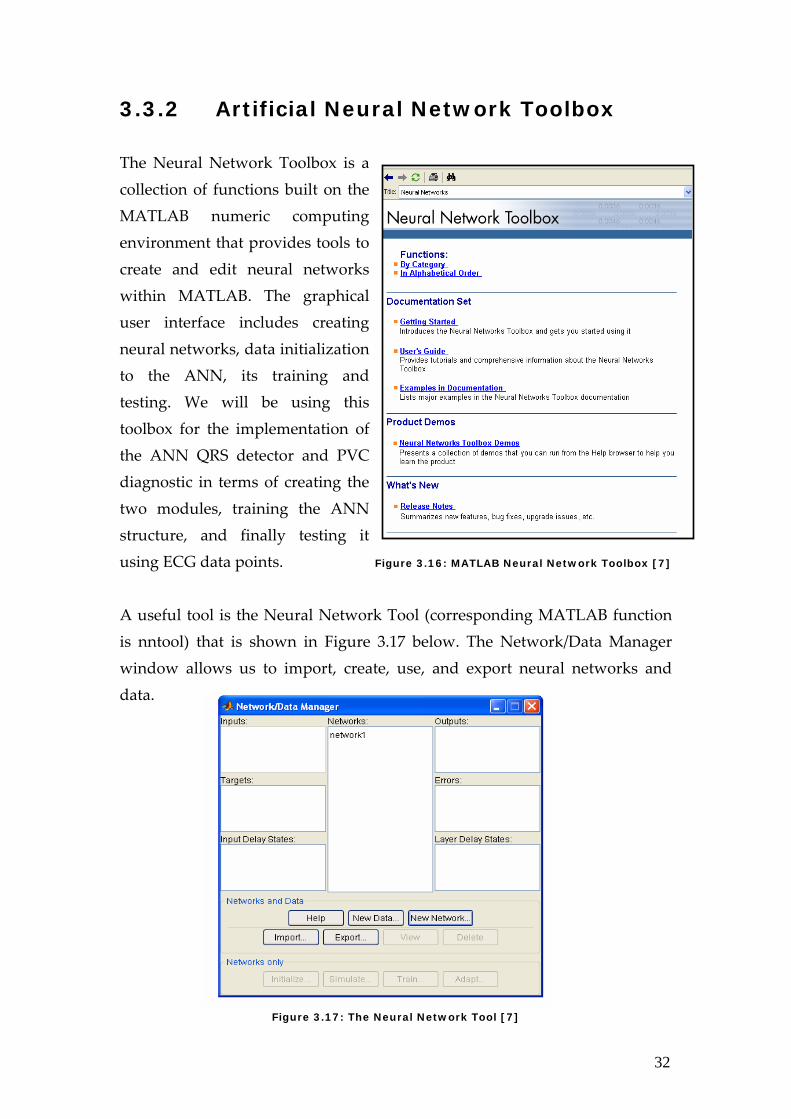
3.3.2 Artificial Neural Network Toolbox The Neural Network Toolbox is a collection of functions built on the MATLAB numeric computing environment that provides tools to create and edit neural networks within MATLAB. The graphical user interface includes creating neural networks, data initialization to the ANN, its training and testing. We will be using this toolbox for the implementation of the ANN QRS detector and PVC diagnostic in terms of creating the two modules, training the ANN structure, and finally testing it using ECG data points. Figure 3.16: MATLAB Neural Network Toolbox [7]
A useful tool is the Neural Network Tool (corresponding MATLAB function is nntool) that is shown in Figure 3.17 below. The Network/Data Manager window allows us to import, create, use, and export neural networks and data.
Figure 3.17: The Neural Network Tool [7]
33
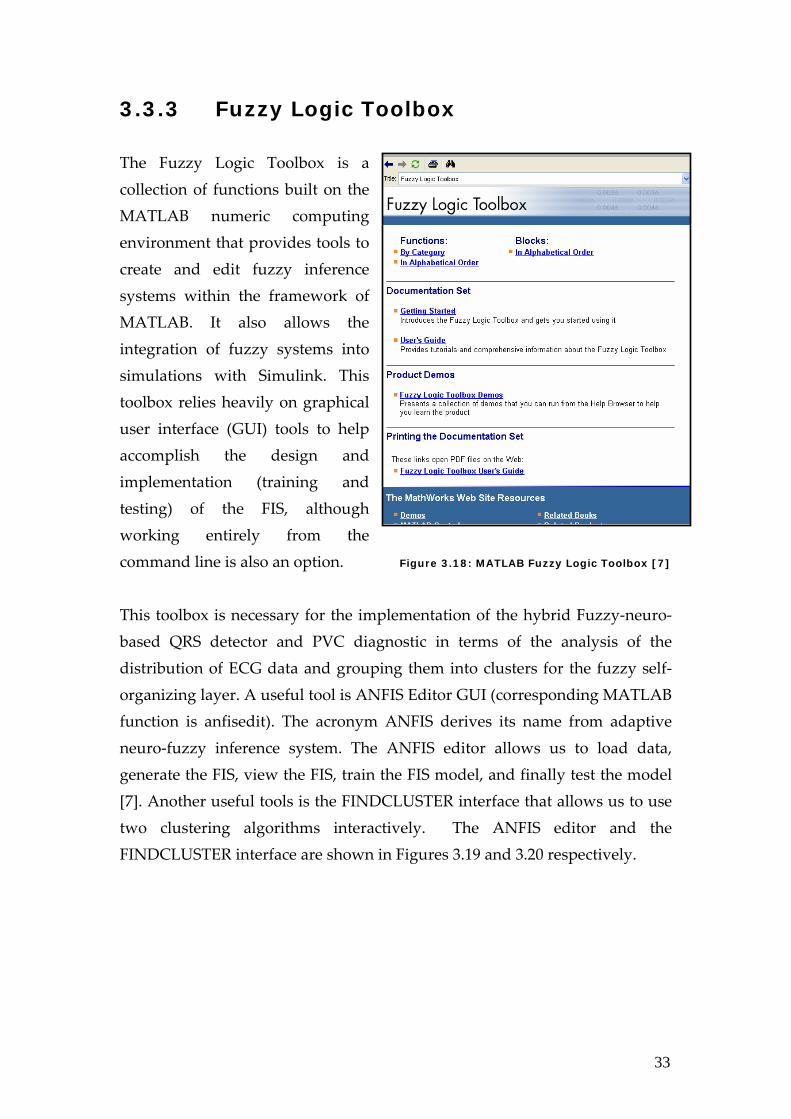
3.3.3 Fuzzy Logic Toolbox The Fuzzy Logic Toolbox is a collection of functions built on the MATLAB numeric computing environment that provides tools to create and edit fuzzy inference systems within the framework of MATLAB. It also allows the integration of fuzzy systems into simulations with Simulink. This toolbox relies heavily on graphical user interface (GUI) tools to help accomplish the design and implementation (training and testing) of the FIS, although working entirely from the command line is also an option. Figure 3.18: MATLAB Fuzzy Logic Toolbox [7]
This toolbox is necessary for the implementation of the hybrid Fuzzy‐neuro‐based QRS detector and PVC diagnostic in terms of the analysis of the distribution of ECG data and grouping them into clusters for the fuzzy self‐organizing layer. A useful tool is ANFIS Editor GUI (corresponding MATLAB function is anfisedit). The acronym ANFIS derives its name from adaptive neuro‐fuzzy inference system. The ANFIS editor allows us to load data, generate the FIS, view the FIS, train the FIS model, and finally test the model [7]. Another useful tools is the FINDCLUSTER interface that allows us to use two clustering algorithms interactively. The ANFIS editor and the FINDCLUSTER interface are shown in Figures 3.19 and 3.20 respectively.
34
Figure 3.19: ANFIS Editor GUI [7] Figure 3.20: FINDCLUSTER Interface [7]
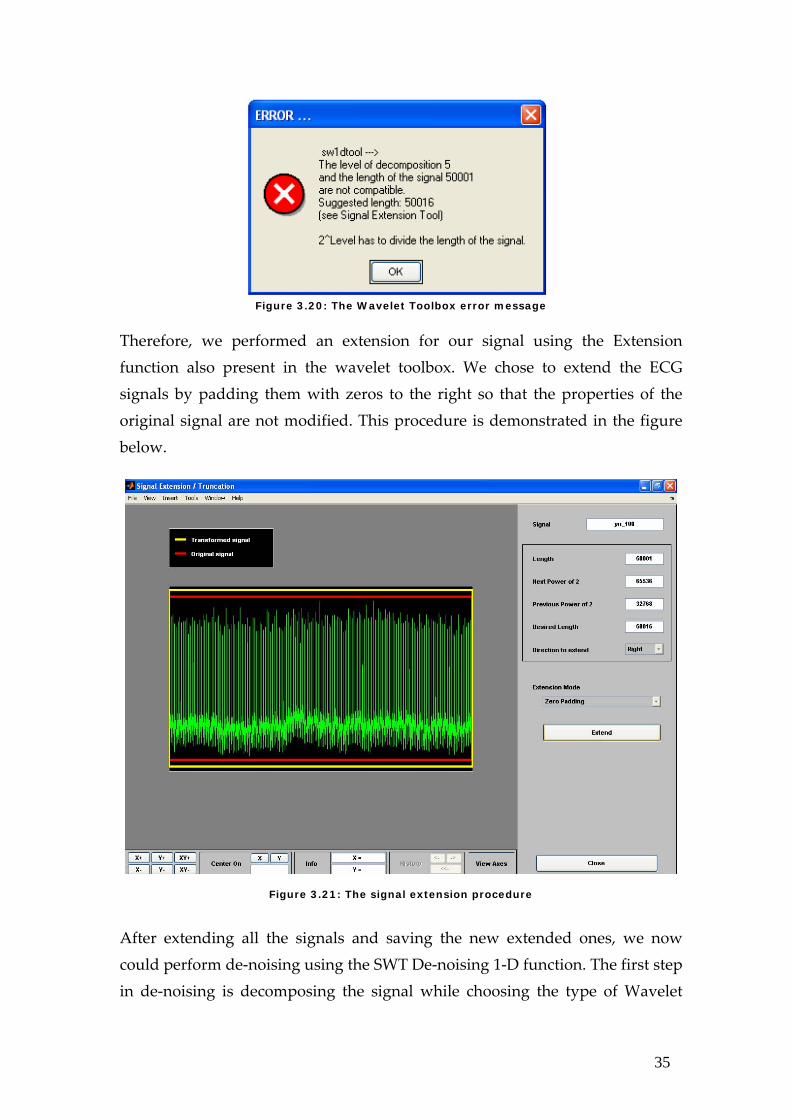
3.4 Preprocessing I In this section we cover the first preprocessing stage of our ECG signals. This stage includes de‐noising, smoothing, and normalization. To perform the following operations, we have used different tools on MATLAB. De‐noising was performed using the Wavelet toolbox, precisely the Stationary Wavelet Transform one‐dimensional de‐noising tool. Smoothing and normalizing was performed using functions that take parameters directly from the command window. 3.4.1 De-noising Since the extracted signals are noisy in many cases, de‐noising was an essential step before further processing of the signals. After searching for and trying several methods, we chose to perform our de‐noising using the Wavelet Toolbox that provides the necessary function for de‐noising signals that convey properties similar to our ECG signals and that is the SWT (Stationary Wavelet Transform) De‐noising 1‐D. Since we have reduced the number of samples to 50000 so that they can run without problems on MATLAB, we had to extend the signals by 16 samples before we could de‐noise them because the Wavelet toolbox gave an error shown in Figure 3.20 below.
35
Figure 3.20: The Wavelet Toolbox error message
Therefore, we performed an extension for our signal using the Extension function also present in the wavelet toolbox. We chose to extend the ECG signals by padding them with zeros to the right so that the properties of the original signal are not modified. This procedure is demonstrated in the figure below.
Figure 3.21: The signal extension procedure
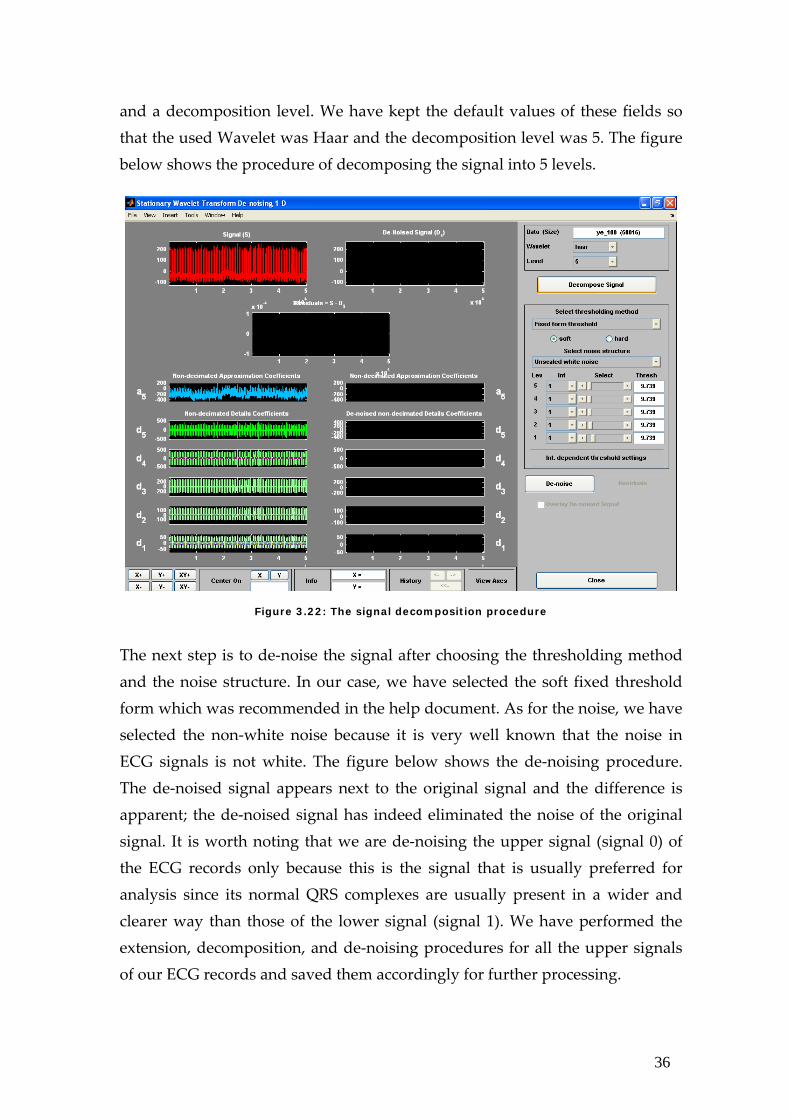
After extending all the signals and saving the new extended ones, we now could perform de‐noising using the SWT De‐noising 1‐D function. The first step in de‐noising is decomposing the signal while choosing the type of Wavelet
36
and a decomposition level. We have kept the default values of these fields so that the used Wavelet was Haar and the decomposition level was 5. The figure below shows the procedure of decomposing the signal into 5 levels.
Figure 3.22: The signal decomposition procedure
The next step is to de‐noise the signal after choosing the thresholding method and the noise structure. In our case, we have selected the soft fixed threshold form which was recommended in the help document. As for the noise, we have selected the non‐white noise because it is very well known that the noise in ECG signals is not white. The figure below shows the de‐noising procedure. The de‐noised signal appears next to the original signal and the difference is apparent; the de‐noised signal has indeed eliminated the noise of the original signal. It is worth noting that we are de‐noising the upper signal (signal 0) of the ECG records only because this is the signal that is usually preferred for analysis since its normal QRS complexes are usually present in a wider and clearer way than those of the lower signal (signal 1). We have performed the extension, decomposition, and de‐noising procedures for all the upper signals of our ECG records and saved them accordingly for further processing.

37
Figure 3.23: The signal de-noising procedure
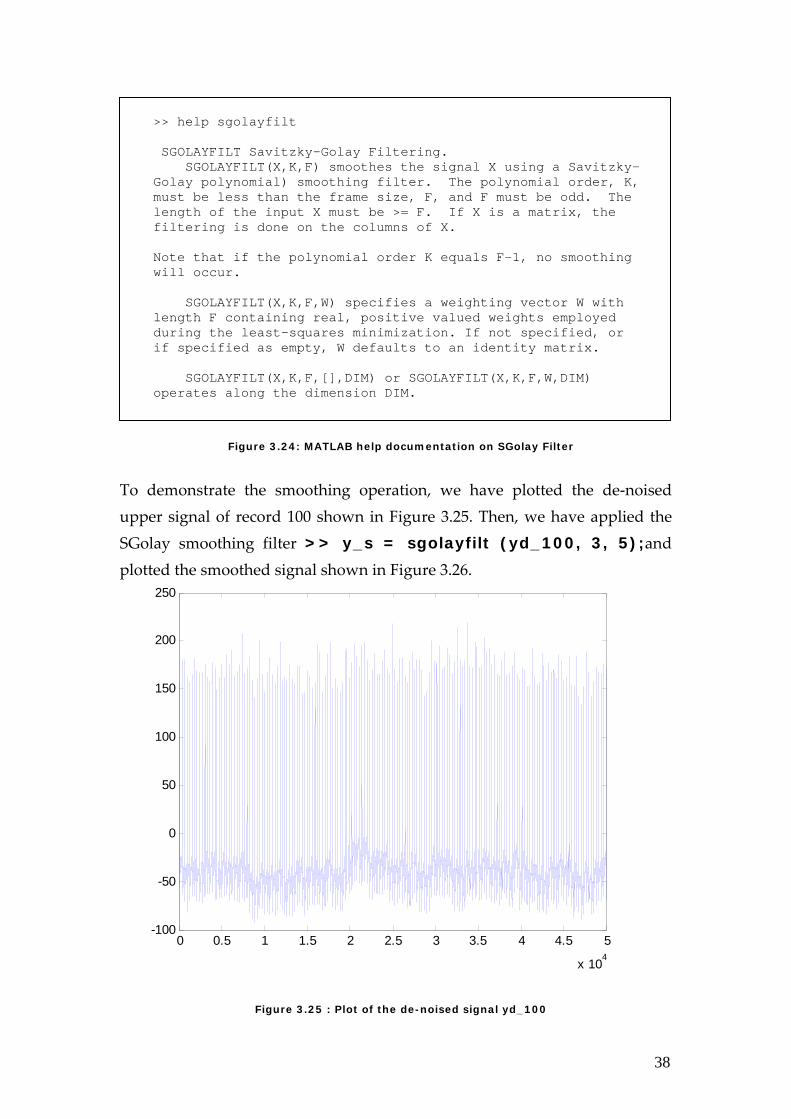
3.4.2 Smoothing To smooth the signals we have also searched for and tested a variety of ways on MATLAB until we discovered an easy and efficient way for smoothing the ECG signals. This method is called Savitsky‐Golay filtering and the command it takes is sgolayfilt which takes two variables in addition to the signal in consideration. The two other variables are the polynomial order, K, and the frame size, F, which must be odd. By trial and error, we have chosen K to be 3 and F to be 5, knowing that K must be less than F. The signals that we have used for smoothing were the de‐noised signals, i.e. of length 50016 samples. Figure 3.24 shows some of the MATLAB help documentation regarding the SGolay filter used for smoothing. We next show in figures 3.25 and 3.26 the shape of the de‐noised signal (record 100) before and after smoothing. After accurate observation, we see a slight difference in the shape of the smoothed signal. The amount of change depends on the record in that some signals vary in shape after smoothing more than others.
38
Figure 3.24: MATLAB help documentation on SGolay Filter
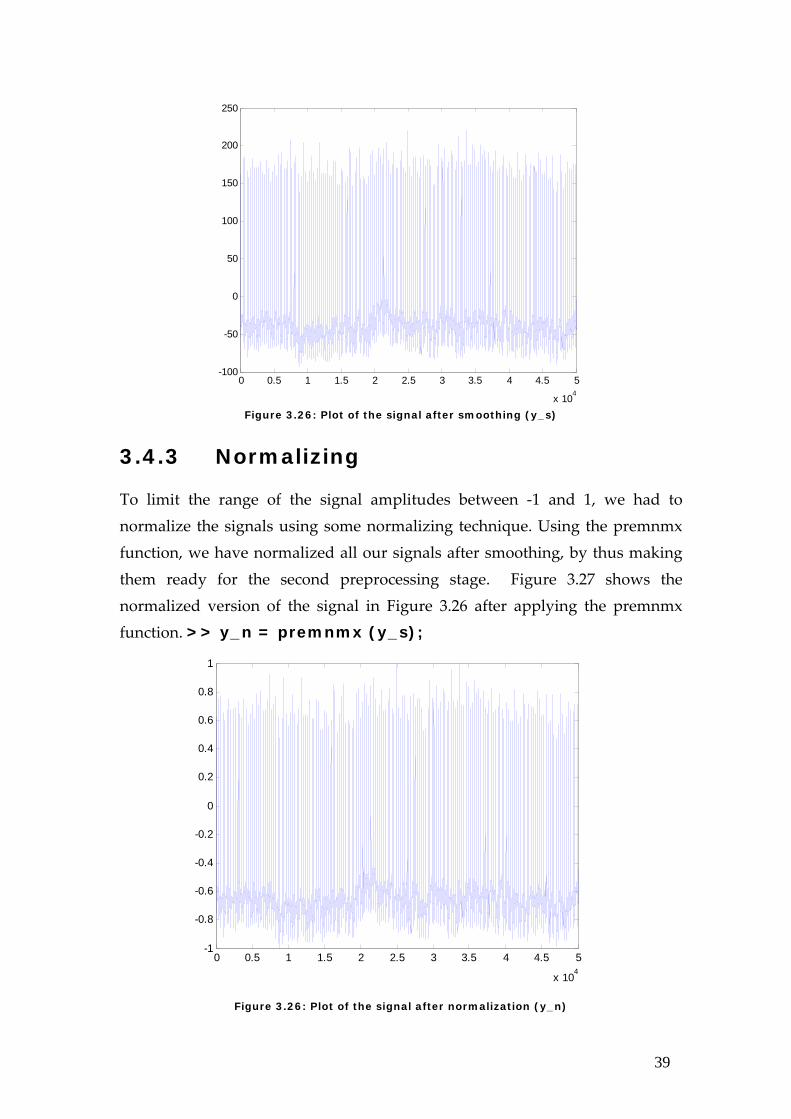
To demonstrate the smoothing operation, we have plotted the de‐noised upper signal of record 100 shown in Figure 3.25. Then, we have applied the SGolay smoothing filter >> y_s = sgolayfilt (yd_100, 3, 5);and plotted the smoothed signal shown in Figure 3.26.
Figure 3.25 : Plot of the de-noised signal yd_100
>> help sgolayfilt SGOLAYFILT Savitzky-Golay Filtering. SGOLAYFILT(X,K,F) smoothes the signal X using a Savitzky-Golay polynomial) smoothing filter. The polynomial order, K, must be less than the frame size, F, and F must be odd. The length of the input X must be >= F. If X is a matrix, the filtering is done on the columns of X. Note that if the polynomial order K equals F-1, no smoothing will occur. SGOLAYFILT(X,K,F,W) specifies a weighting vector W with length F containing real, positive valued weights employed during the least-squares minimization. If not specified, or if specified as empty, W defaults to an identity matrix. SGOLAYFILT(X,K,F,[],DIM) or SGOLAYFILT(X,K,F,W,DIM) operates along the dimension DIM.
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
x 104
-100
-50
0
50
100
150
200
250
39
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
x 104
-100
-50
0
50
100
150
200
250
Figure 3.26: Plot of the signal after smoothing (y_s)
3.4.3 Normalizing
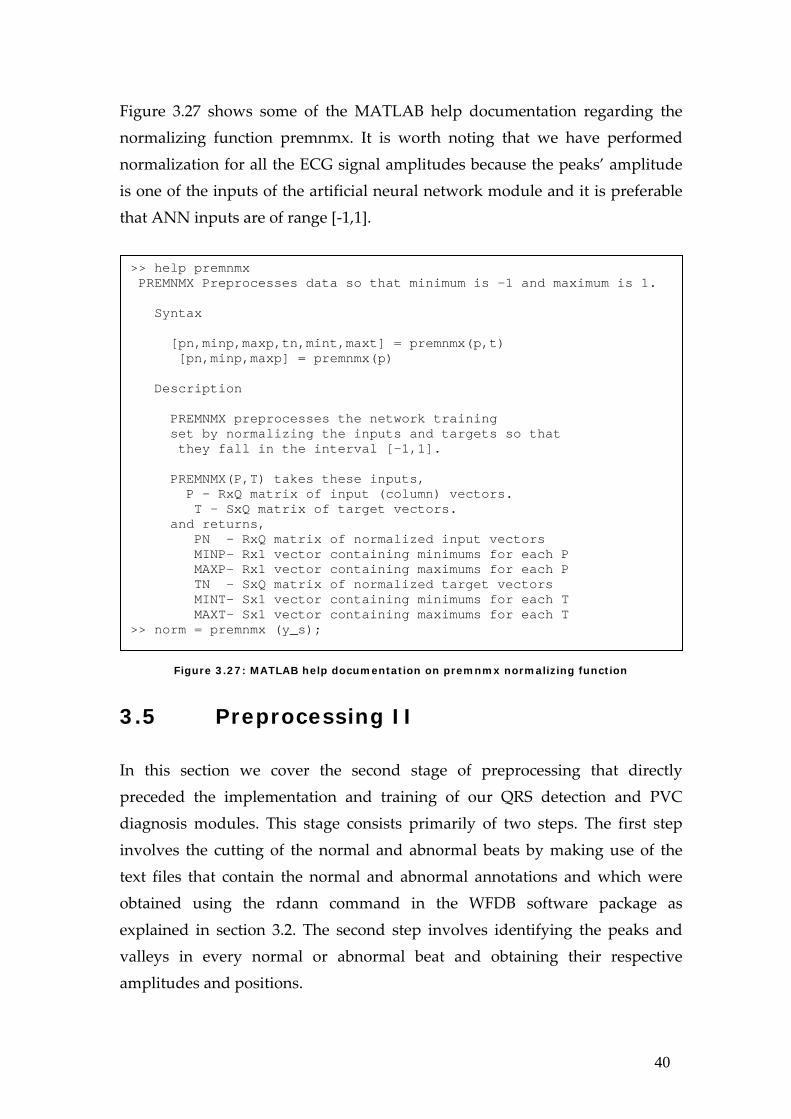
To limit the range of the signal amplitudes between ‐1 and 1, we had to normalize the signals using some normalizing technique. Using the premnmx function, we have normalized all our signals after smoothing, by thus making them ready for the second preprocessing stage. Figure 3.27 shows the normalized version of the signal in Figure 3.26 after applying the premnmx function. >> y_n = premnmx (y_s);
Figure 3.26: Plot of the signal after normalization (y_n)
0 0.5 1 1.5 2 2.5 3 3.5 4 4.5 5
x 104
-1
-0.8
-0.6
-0.4
-0.2
0
0.2
0.4
0.6
0.8
1
40
Figure 3.27 shows some of the MATLAB help documentation regarding the normalizing function premnmx. It is worth noting that we have performed normalization for all the ECG signal amplitudes because the peaks’ amplitude is one of the inputs of the artificial neural network module and it is preferable that ANN inputs are of range [‐1,1].
Figure 3.27: MATLAB help documentation on premnmx normalizing function
3.5 Preprocessing II In this section we cover the second stage of preprocessing that directly preceded the implementation and training of our QRS detection and PVC diagnosis modules. This stage consists primarily of two steps. The first step involves the cutting of the normal and abnormal beats by making use of the text files that contain the normal and abnormal annotations and which were obtained using the rdann command in the WFDB software package as explained in section 3.2. The second step involves identifying the peaks and valleys in every normal or abnormal beat and obtaining their respective amplitudes and positions.
>> help premnmx PREMNMX Preprocesses data so that minimum is -1 and maximum is 1. Syntax [pn,minp,maxp,tn,mint,maxt] = premnmx(p,t) [pn,minp,maxp] = premnmx(p) Description PREMNMX preprocesses the network training set by normalizing the inputs and targets so that they fall in the interval [-1,1]. PREMNMX(P,T) takes these inputs, P - RxQ matrix of input (column) vectors. T - SxQ matrix of target vectors. and returns, PN - RxQ matrix of normalized input vectors MINP- Rx1 vector containing minimums for each P MAXP- Rx1 vector containing maximums for each P TN - SxQ matrix of normalized target vectors MINT- Sx1 vector containing minimums for each T MAXT- Sx1 vector containing maximums for each T >> norm = premnmx (y_s);
41
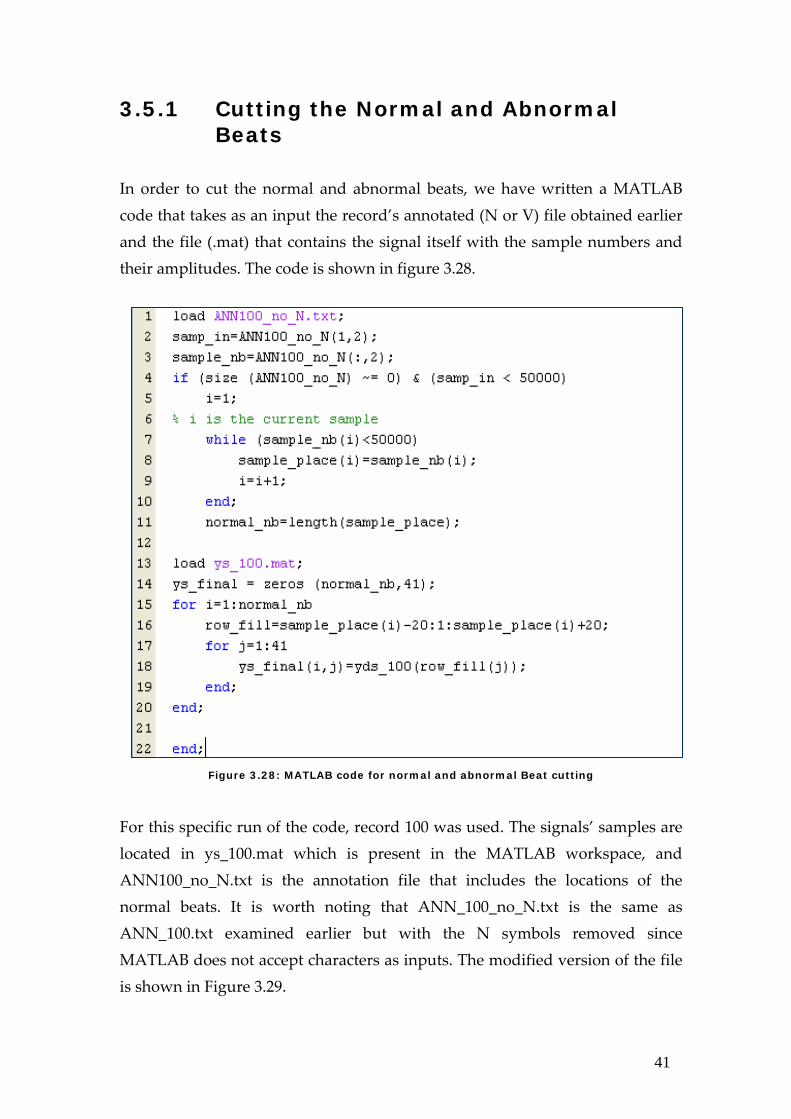
3.5.1 Cutting the Normal and Abnormal Beats
In order to cut the normal and abnormal beats, we have written a MATLAB code that takes as an input the record’s annotated (N or V) file obtained earlier and the file (.mat) that contains the signal itself with the sample numbers and their amplitudes. The code is shown in figure 3.28.
Figure 3.28: MATLAB code for normal and abnormal Beat cutting
For this specific run of the code, record 100 was used. The signals’ samples are located in ys_100.mat which is present in the MATLAB workspace, and ANN100_no_N.txt is the annotation file that includes the locations of the normal beats. It is worth noting that ANN_100_no_N.txt is the same as ANN_100.txt examined earlier but with the N symbols removed since MATLAB does not accept characters as inputs. The modified version of the file is shown in Figure 3.29.
42
The code examines the second row of the annotation file which corresponds to the sample number of the normal beat. Since our signals were cut up‐to 50,000 beats only, the code checks for annotation files with sample numbers greater than 50,000 in order to ignore the samples. The code then creates a matrix with number of rows equals the number of normal beats.
Figure 3.29: Input annotated text file
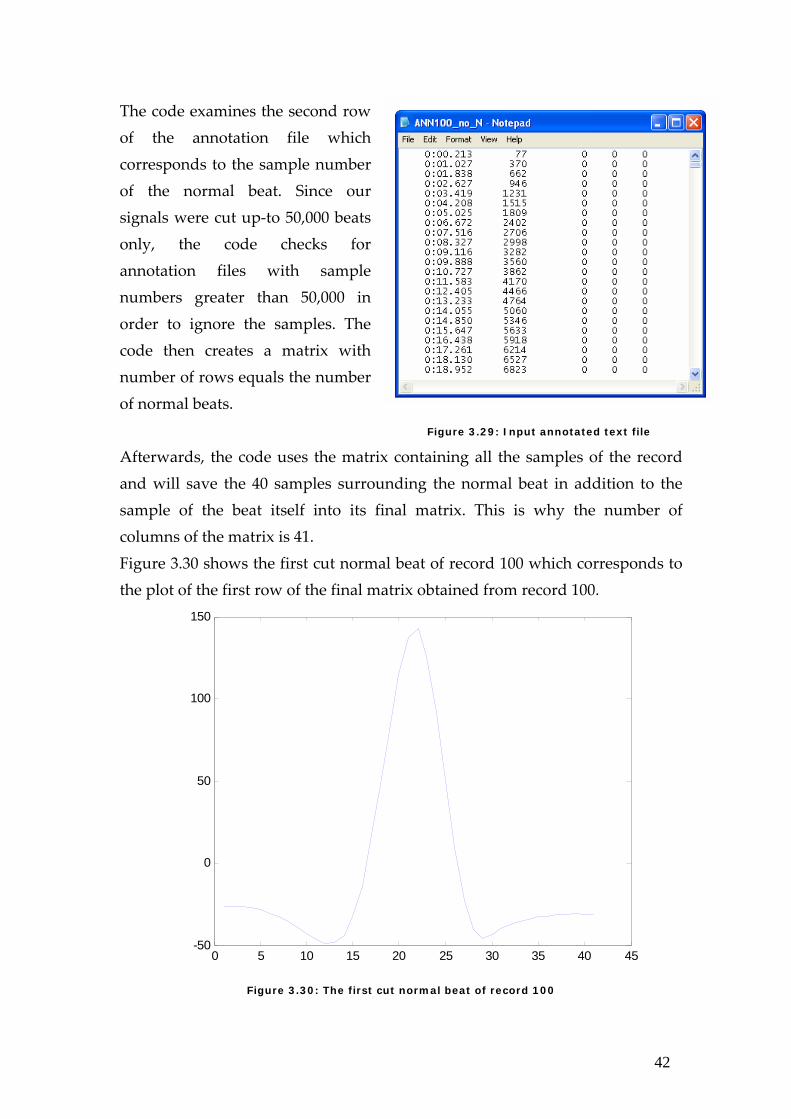
Afterwards, the code uses the matrix containing all the samples of the record and will save the 40 samples surrounding the normal beat in addition to the sample of the beat itself into its final matrix. This is why the number of columns of the matrix is 41. Figure 3.30 shows the first cut normal beat of record 100 which corresponds to the plot of the first row of the final matrix obtained from record 100.
Figure 3.30: The first cut normal beat of record 100
0 5 10 15 20 25 30 35 40 45-50
0
50
100
150
43
Similarly, we cut the normal beats of all signals. We cut the abnormal beats too in the same fashion and with the same code using the PVC annotated files.
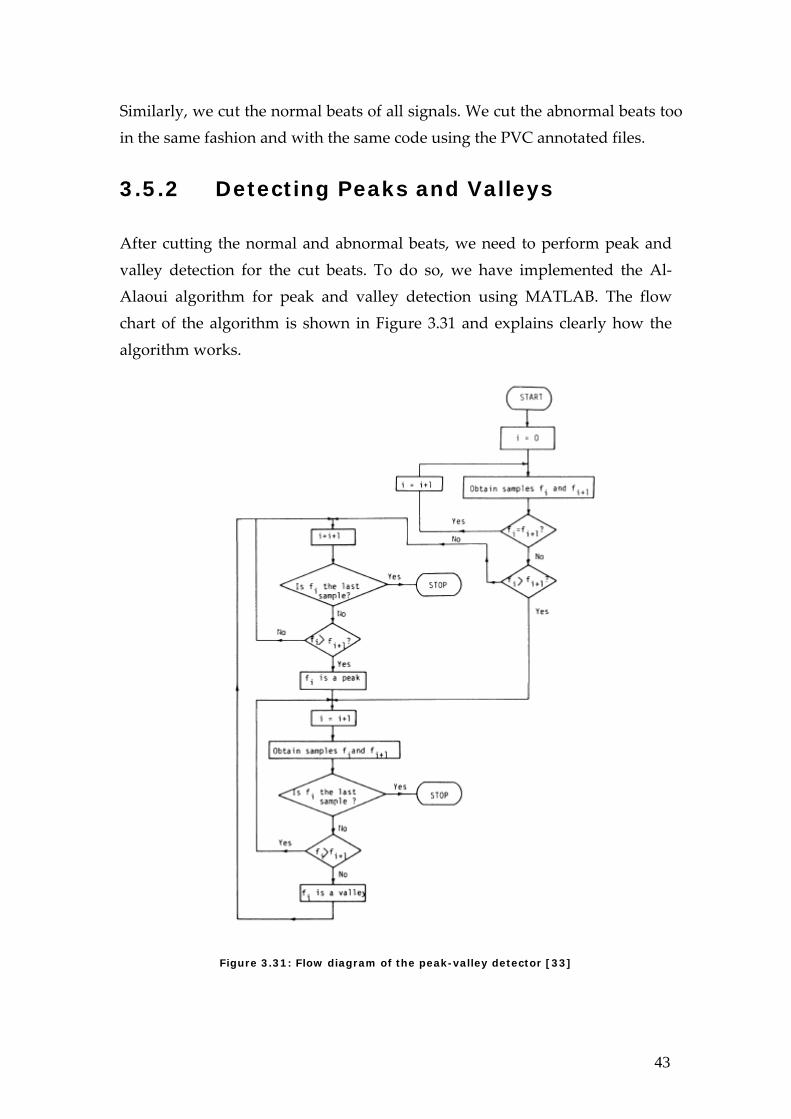
3.5.2 Detecting Peaks and Valleys After cutting the normal and abnormal beats, we need to perform peak and valley detection for the cut beats. To do so, we have implemented the Al‐Alaoui algorithm for peak and valley detection using MATLAB. The flow chart of the algorithm is shown in Figure 3.31 and explains clearly how the algorithm works.
Figure 3.31: Flow diagram of the peak-valley detector [33]

44
The peak and valley detector correctly detects the P, Q, R, S, and T waves. Our code also identifies whether one of these waves is missing by replacing it by a zero ‘0’ since not all beats, especially abnormal ones, are characterized by the standard PQRST waves. Therefore, at this stage we performed the peak and valley detection and consequently QRS detection since we could determine the position and amplitudes of the Q, R, and S waves. The code used at this stage results in five outputs which are the amplitude and position of each of the P, Q, R, S, and T waves. These 10 outputs are used in the processing stage as inputs for the ANN module and the hybrid fuzzy‐neuro module.
45
Chapter 4 Artificial Neural Network A neural network is a connection of parallel operating simple elements that are inspired by biological nervous systems. The neural network can be trained to perform a particular function by adjusting the values of the connections (or weights) between these elements. In this chapter, we will start by introducing the design method of the neural network. We will then move on to the implementation stages involving both the training and testing parts; the latter also known as the simulation. Finally, we will tabulate the computed results and compare those to others achieved by systems in the literature.
4.1 Design of the Neural Network
The Neural Network Toolbox is a useful tool for industry, education and research. It explains procedures, applies them, and shows their successes and failures; thus, helping in the development of neural networks. The NNtool in the Neural Network Toolbox was previously shown in Figure 3.17 Within the Network/Data Manager in the NNTool window, the New Network button is used for creating a neural network which can also be imported from the Matlab workspace. Once we choose creating a new network, a window illustrating the network’s desired characteristics pops up as given by Figure 4.1.
46
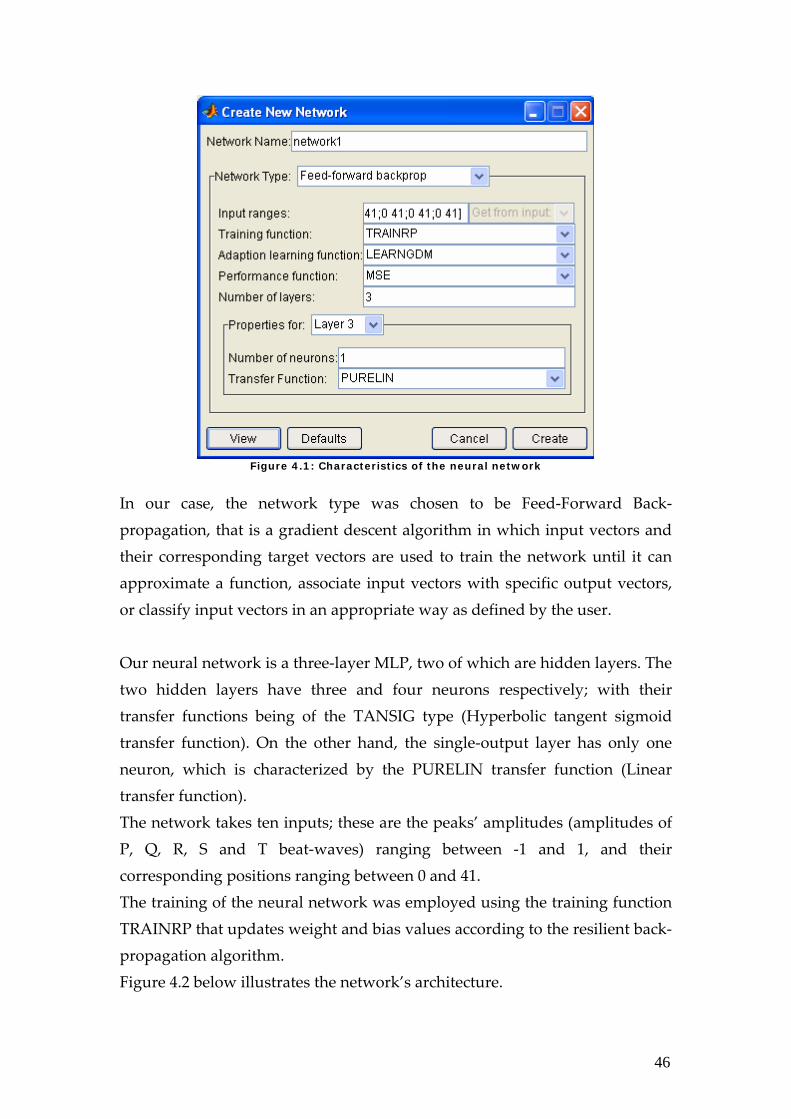
Figure 4.1: Characteristics of the neural network
In our case, the network type was chosen to be Feed‐Forward Back‐propagation, that is a gradient descent algorithm in which input vectors and their corresponding target vectors are used to train the network until it can approximate a function, associate input vectors with specific output vectors, or classify input vectors in an appropriate way as defined by the user. Our neural network is a three‐layer MLP, two of which are hidden layers. The two hidden layers have three and four neurons respectively; with their transfer functions being of the TANSIG type (Hyperbolic tangent sigmoid transfer function). On the other hand, the single‐output layer has only one neuron, which is characterized by the PURELIN transfer function (Linear transfer function). The network takes ten inputs; these are the peaks’ amplitudes (amplitudes of P, Q, R, S and T beat‐waves) ranging between ‐1 and 1, and their corresponding positions ranging between 0 and 41. The training of the neural network was employed using the training function TRAINRP that updates weight and bias values according to the resilient back‐propagation algorithm. Figure 4.2 below illustrates the network’s architecture.
47
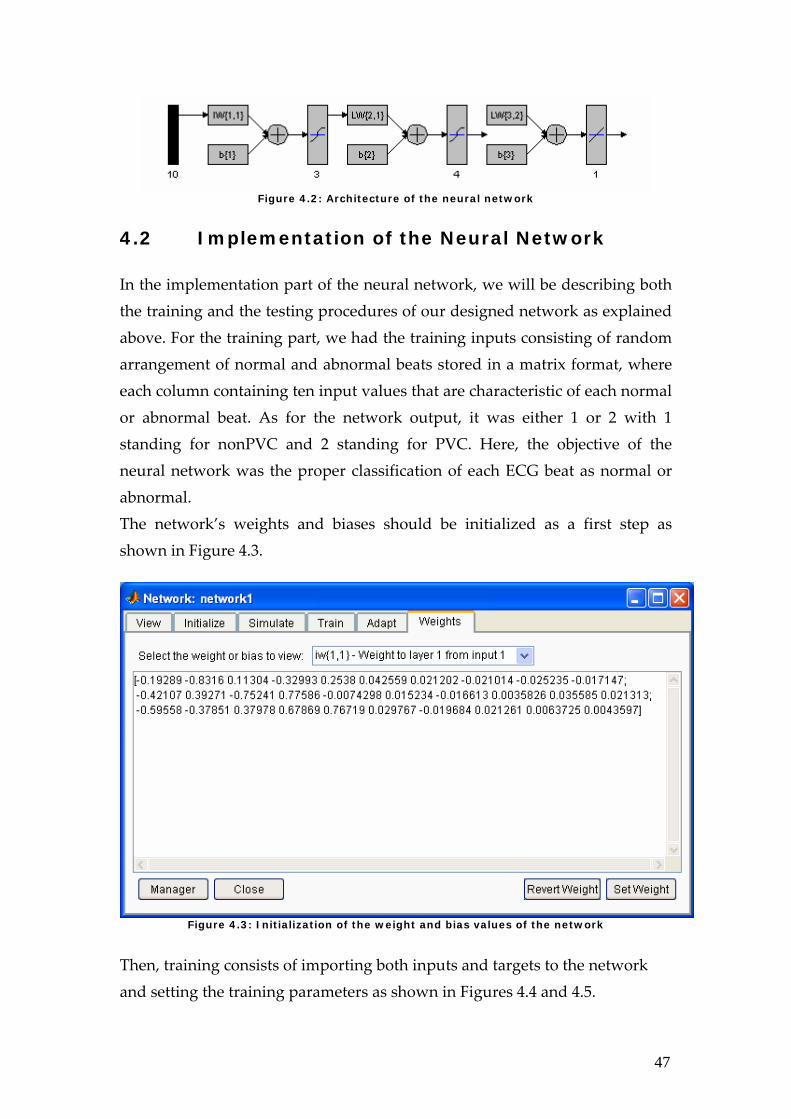
Figure 4.2: Architecture of the neural network
4.2 Implementation of the Neural Network
In the implementation part of the neural network, we will be describing both the training and the testing procedures of our designed network as explained above. For the training part, we had the training inputs consisting of random arrangement of normal and abnormal beats stored in a matrix format, where each column containing ten input values that are characteristic of each normal or abnormal beat. As for the network output, it was either 1 or 2 with 1 standing for nonPVC and 2 standing for PVC. Here, the objective of the neural network was the proper classification of each ECG beat as normal or abnormal. The network’s weights and biases should be initialized as a first step as shown in Figure 4.3.
Figure 4.3: Initialization of the weight and bias values of the network
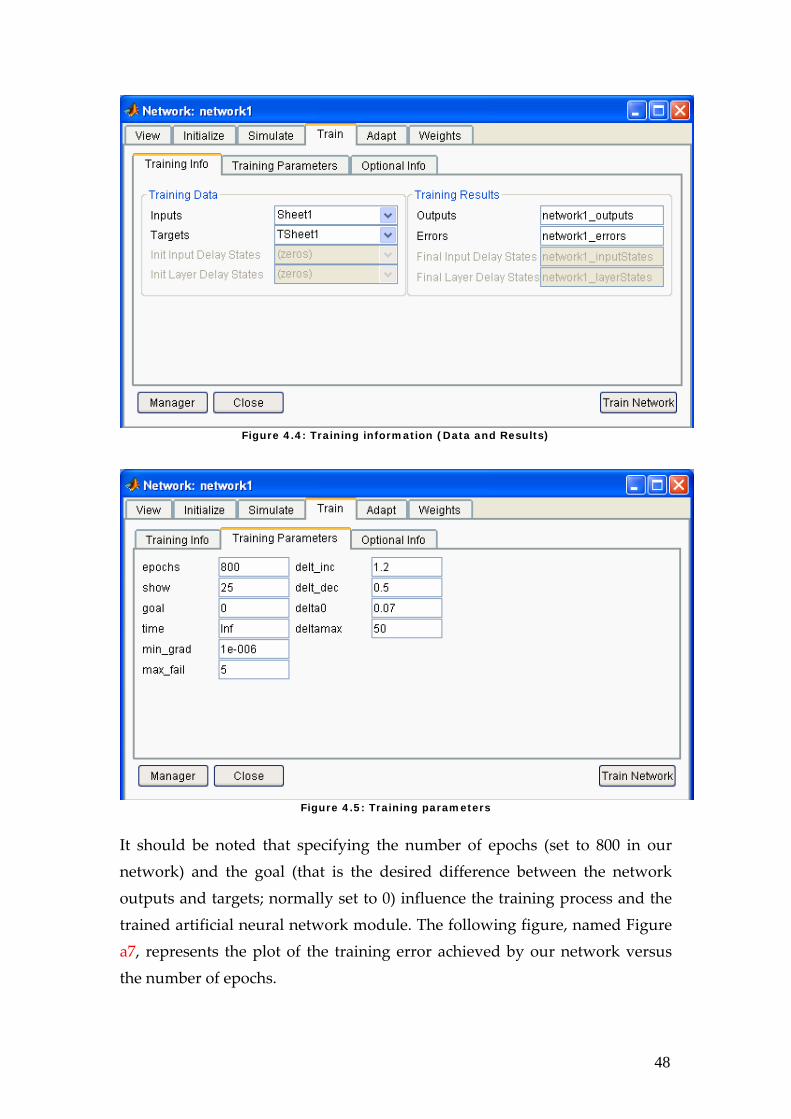
Then, training consists of importing both inputs and targets to the network and setting the training parameters as shown in Figures 4.4 and 4.5.
48
Figure 4.4: Training information (Data and Results)
Figure 4.5: Training parameters
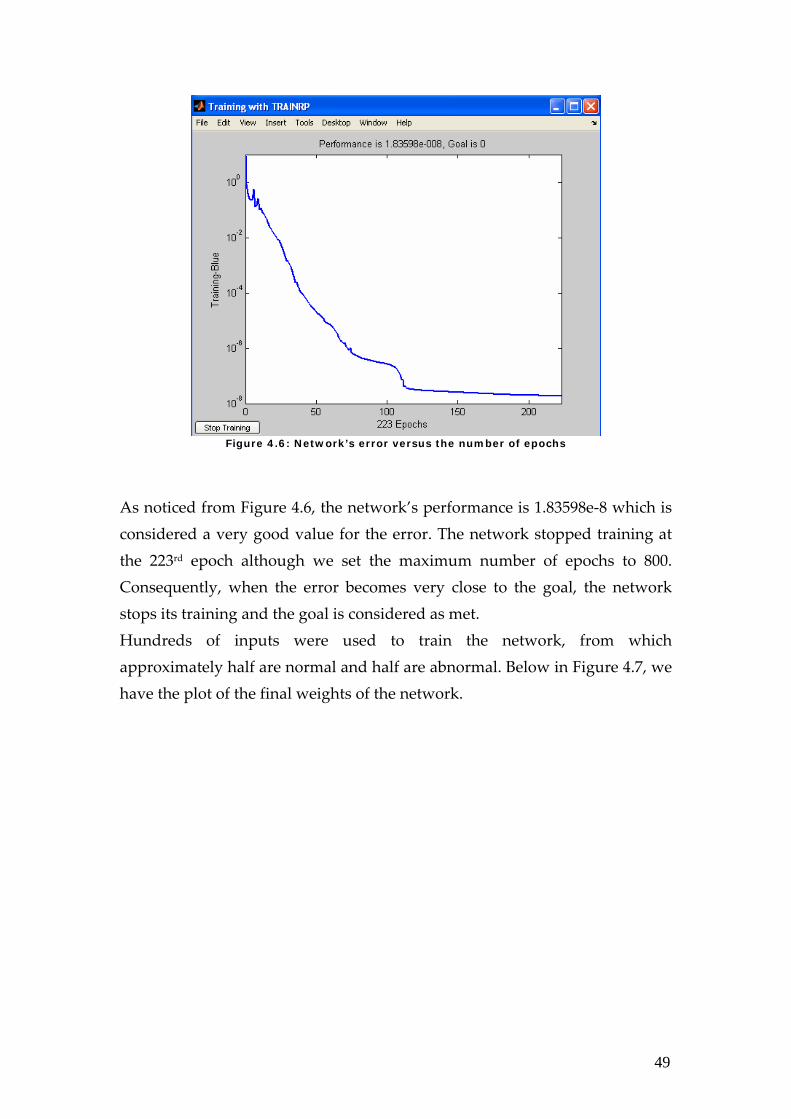
It should be noted that specifying the number of epochs (set to 800 in our network) and the goal (that is the desired difference between the network outputs and targets; normally set to 0) influence the training process and the trained artificial neural network module. The following figure, named Figure a7, represents the plot of the training error achieved by our network versus the number of epochs.
49
Figure 4.6: Network’s error versus the number of epochs
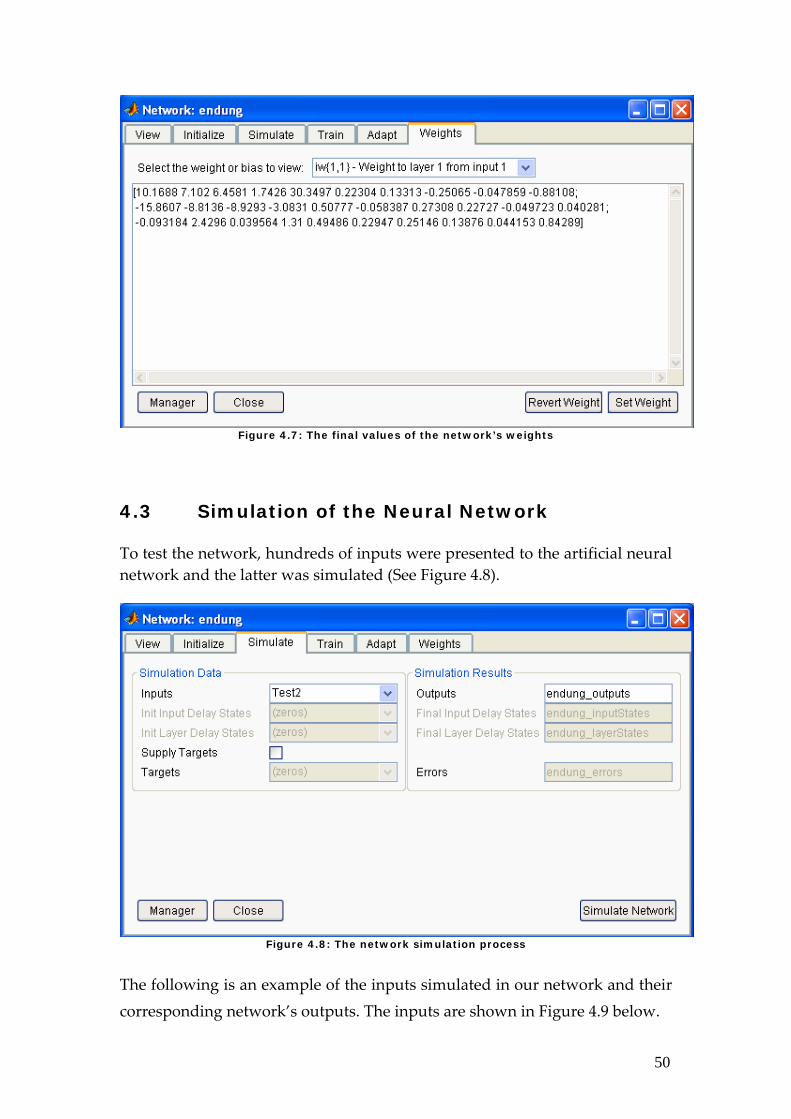
As noticed from Figure 4.6, the network’s performance is 1.83598e‐8 which is considered a very good value for the error. The network stopped training at the 223rd epoch although we set the maximum number of epochs to 800. Consequently, when the error becomes very close to the goal, the network stops its training and the goal is considered as met. Hundreds of inputs were used to train the network, from which approximately half are normal and half are abnormal. Below in Figure 4.7, we have the plot of the final weights of the network.
50
Figure 4.7: The final values of the network’s weights
4.3 Simulation of the Neural Network
To test the network, hundreds of inputs were presented to the artificial neural network and the latter was simulated (See Figure 4.8).
Figure 4.8: The network simulation process
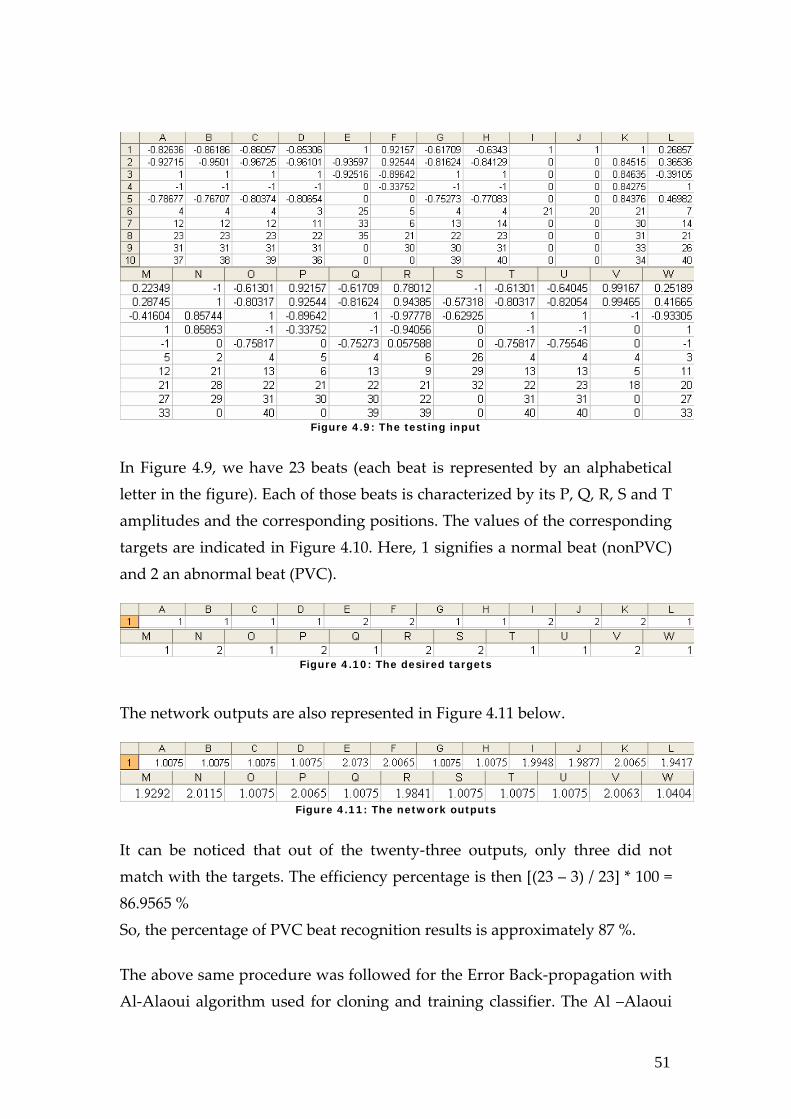
The following is an example of the inputs simulated in our network and their corresponding network’s outputs. The inputs are shown in Figure 4.9 below.
51
Figure 4.9: The testing input
In Figure 4.9, we have 23 beats (each beat is represented by an alphabetical letter in the figure). Each of those beats is characterized by its P, Q, R, S and T amplitudes and the corresponding positions. The values of the corresponding targets are indicated in Figure 4.10. Here, 1 signifies a normal beat (nonPVC) and 2 an abnormal beat (PVC).
Figure 4.10: The desired targets
The network outputs are also represented in Figure 4.11 below.
Figure 4.11: The network outputs
It can be noticed that out of the twenty‐three outputs, only three did not match with the targets. The efficiency percentage is then [(23 – 3) / 23] * 100 = 86.9565 % So, the percentage of PVC beat recognition results is approximately 87 %. The above same procedure was followed for the Error Back‐propagation with Al‐Alaoui algorithm used for cloning and training classifier. The Al –Alaoui
52
0 5 10 15 20 251
1.2
1.4
1.6
1.8
2
2.2
2.4
0 5 10 15 20 250.8
1
1.2
1.4
1.6
1.8
2
2.2
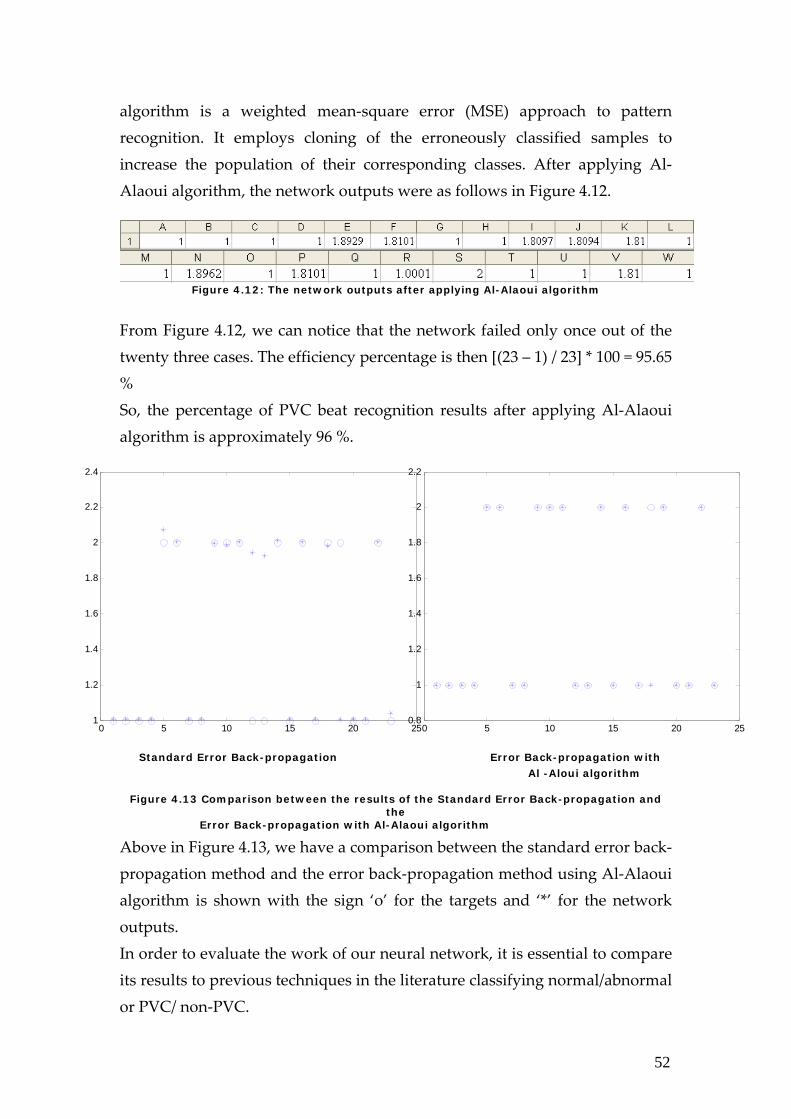
algorithm is a weighted mean‐square error (MSE) approach to pattern recognition. It employs cloning of the erroneously classified samples to increase the population of their corresponding classes. After applying Al‐Alaoui algorithm, the network outputs were as follows in Figure 4.12.
Figure 4.12: The network outputs after applying Al-Alaoui algorithm
From Figure 4.12, we can notice that the network failed only once out of the twenty three cases. The efficiency percentage is then [(23 – 1) / 23] * 100 = 95.65 % So, the percentage of PVC beat recognition results after applying Al‐Alaoui algorithm is approximately 96 %.
Standard Error Back-propagation Error Back-propagation with Al -Aloui algorithm
Figure 4.13 Comparison between the results of the Standard Error Back-propagation and the
Error Back-propagation with Al-Alaoui algorithm
Above in Figure 4.13, we have a comparison between the standard error back‐propagation method and the error back‐propagation method using Al‐Alaoui algorithm is shown with the sign ‘o’ for the targets and ‘*’ for the network outputs. In order to evaluate the work of our neural network, it is essential to compare its results to previous techniques in the literature classifying normal/abnormal or PVC/ non‐PVC.
53
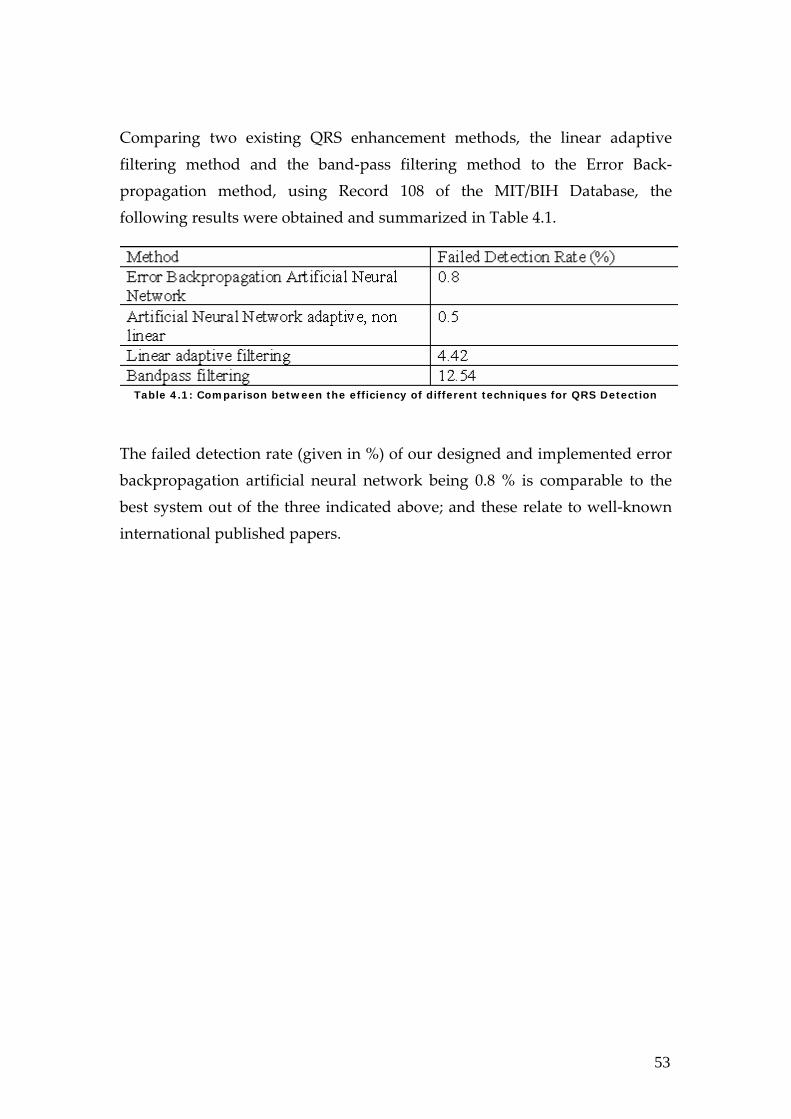
Comparing two existing QRS enhancement methods, the linear adaptive filtering method and the band‐pass filtering method to the Error Back‐propagation method, using Record 108 of the MIT/BIH Database, the following results were obtained and summarized in Table 4.1.
Table 4.1: Comparison between the efficiency of different techniques for QRS Detection
The failed detection rate (given in %) of our designed and implemented error backpropagation artificial neural network being 0.8 % is comparable to the best system out of the three indicated above; and these relate to well‐known international published papers.
54
Chapter 5 Fuzzy-Neural Networks We have presented in Chapter 4 the first module for QRS detection and PVC diagnosis, using the Artificial Neural Networks Method. We have described the design steps and the implementation stages of this method from the creation of the artificial neural network system to its training and finally the testing with standard database records. In addition, we have provided an improvement to this method using the Al‐Alaoui Algorithm and compared both techniques in neural networks in terms of rate of misclassification to other well‐published and recognized systems in the literature. This section will be discussing the second module dedicated for QRS detection and PVC diagnosis, which is the Fuzzy‐Neuro‐Based Module, from the design process to the implementation stages and the results obtained. 5.1 Design of Fuzzy-Neuro-Based Module Design Criteria:
QRS detection and PVC diagnosis Real‐time implementation
Proposed Solution: ANFIS system that can be trained using desired input‐output (amplitude/position‐class) ECG signals and is able to adapt to any patientʹs cardiac signal generating its proper diagnosis, either PVC or nonPVC.
55
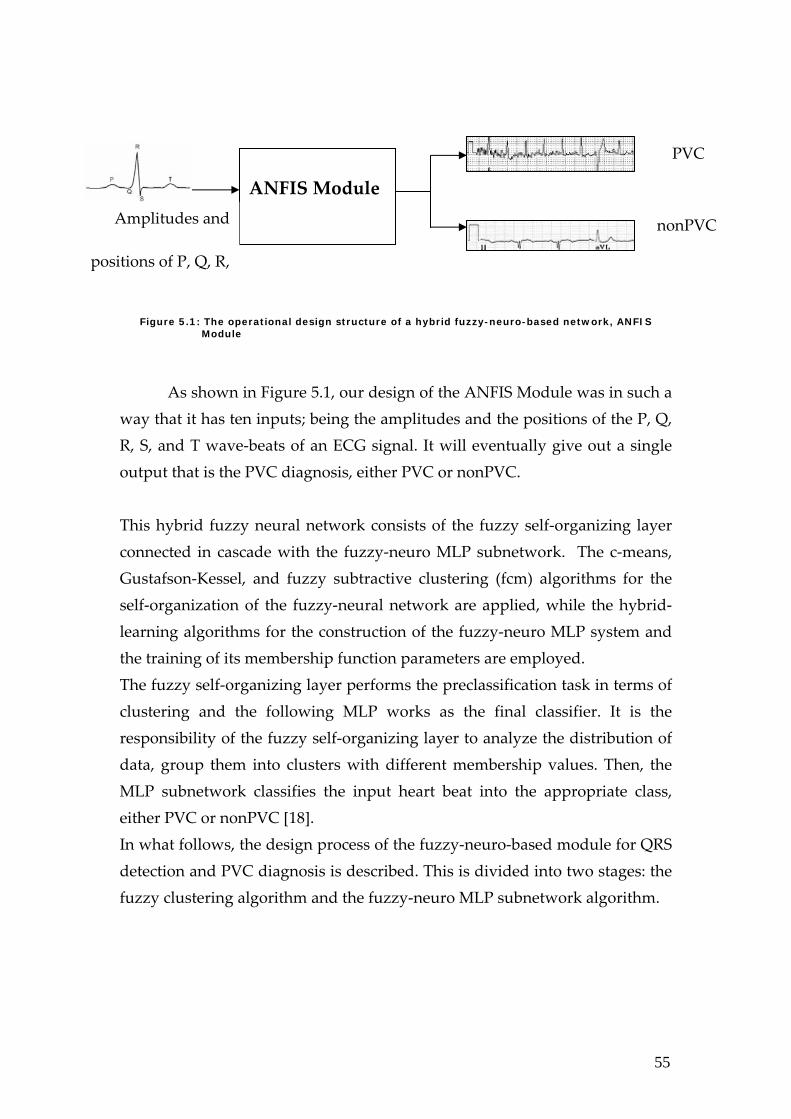
Figure 5.1: The operational design structure of a hybrid fuzzy-neuro-based network, ANFIS Module
As shown in Figure 5.1, our design of the ANFIS Module was in such a way that it has ten inputs; being the amplitudes and the positions of the P, Q, R, S, and T wave‐beats of an ECG signal. It will eventually give out a single output that is the PVC diagnosis, either PVC or nonPVC. This hybrid fuzzy neural network consists of the fuzzy self‐organizing layer connected in cascade with the fuzzy‐neuro MLP subnetwork. The c‐means, Gustafson‐Kessel, and fuzzy subtractive clustering (fcm) algorithms for the self‐organization of the fuzzy‐neural network are applied, while the hybrid‐learning algorithms for the construction of the fuzzy‐neuro MLP system and the training of its membership function parameters are employed. The fuzzy self‐organizing layer performs the preclassification task in terms of clustering and the following MLP works as the final classifier. It is the responsibility of the fuzzy self‐organizing layer to analyze the distribution of data, group them into clusters with different membership values. Then, the MLP subnetwork classifies the input heart beat into the appropriate class, either PVC or nonPVC [18]. In what follows, the design process of the fuzzy‐neuro‐based module for QRS detection and PVC diagnosis is described. This is divided into two stages: the fuzzy clustering algorithm and the fuzzy‐neuro MLP subnetwork algorithm.
ANFIS Module
PVC
nonPVC Amplitudes and
positions of P, Q, R,

56
5.1.1 The Fuzzy Clustering Algorithm This algorithm is a data clustering technique where each data point belongs to a cluster to some degree that is specified by a membership grade. It shows how to group data points that populate some multidimensional space into a specific number of different clusters. The inputs to this fuzzy clustering algorithm are the ten values corresponding to the amplitudes and the positions of the P, Q, R, S, and T beats in the processed ECG signal recording under classification denoted by vectors xk = [xk1 , xk2 , …, xkN]T for k = 1, 2,…p. The classification of these vectors xk into c clusters, with each cluster having a center vector ci = [ci1, ci2, …, ciN]T for i = 1, 2,…c, results in the partitioning of the inputs in the data space according to given membership functions. The fuzzy clustering algorithms search for the partition matrix and cluster centers such that the objective function E is minimized.
1
),(
1
1 1
2
=
=
∑
∑∑
=
= =
c
i
mji
c
i
p
jij
mji
u
cxduE
where the parameter m controls the fuzziness of the clusters; its typical value is 2, the function ),( ij cxd measures the distance between the input vector
jx and the center ic , and the partition matrix U of the elements jiu represents the membership function degrees of the data vector jx . The distance ),( ij cxd of the G‐K algorithm uses the scaled metric norm having
)()(),(2iji
Tijij cxMcxcxd −−=
with iM being a positive definite matrix adjusted to the actual shape of the cluster and it is defined as follows
1)det( −= iN
ii FFM

57
And
∑
∑
=
=
−−= p
j
mji
p
jij
Tij
mji
i
u
cxcxuF
1
1)()(
being the cluster covariance matrix. The training of the fuzzy clustering self‐organizing layer is done using the fuzzy competition. It searches for the cluster centers and the partition matrix elements. And its objective is to find the optimal number of cluster centers needed for the input‐output data‐pair modeling as well as the optimal influence ranges of each of these cluster centers defined by the cluster center radius. Below, we have the different steps in the design process of the fuzzy subtractive algorithm; these are:
1. Choose the number of clusters c and the weighting coefficients m. 2. Initialize the termination tolerance ε and the partition matrix U such
that 11
=∑=
c
i
mjiu .
3. Start iterating. Determine the clusters ci = [ci1, ci2, …, ciN]T for i = 1, 2,…c,where
∑
∑
=
== p
j
mji
p
jj
mji
i
u
xuc
1
1
4. Calculate the matrices iF ( i =1, 2,.. c) 5. Compute the distances cid ji ...,,2,1(2 = and )...,,2,1 pj = between the
input vector and the cluster centers. 6. Update the partition matrix jiu entries ci ...,,2,1( = and )...,,2,1 pj =
∑=
−
=c
k
m
jk
jiji
dd
u
1
)1/(2)(
1
If 0=jid for some i = I, take =jIu 1 and =jiu 0 for i ≠ I. Iterate until
ε≤− − |||| 1ll UU for two succeeding iterations [18].
58
It should be noted that the most important stage of the design is the choice of the number of clusters and the cluster radius centers (the influence range of each cluster center on the data samples nearby belonging to a given cluster by a specified grade of membership); as this will affect the complexity of the whole system in terms of its set of rules as well as the number of membership function for each of the ten inputs and single output when the fuzzy‐neuro system is generated after the second algorithm described later on. It would also affect the reduction rate of the error function and the generalization ability of the network. This can be recognized by the following: If the number of clusters chosen is too small, i.e. the values of the cluster radius centers are too large with respect to the training data samples, then, the number of membership function for the inputs and the output will be low yielding lower complexity of the whole fuzzy‐neuro system. Nevertheless, this will prevent the reduction of the error function from reaching a very low level. From a different perspective, if it is too high, this will destroy the generalization ability of the network. 5.1.2 The Fuzzy-Neuro MLP Subnetwork
Algorithm The fuzzy‐neuro MLP subnetwork classifies the applied input vector, representing the heart beat to the appropriate class, PVC or nonPVC. This is attained by applying the output of the self‐organizing fuzzy clustering layer to the input layer of the MLP subnetwork structure. Now for the generation of the fuzzy‐neuro system, we will create a Sugeno‐type ANFIS, the fuzzy‐neuro system, with a knowledge of the training data pairs composed of the ten inputs and the desired class output as well as the optimal cluster radius center. This is achieved by extracting the set of rules that model the data behaviour by first determining the number of rules and antecedent membership functions and then using linear least‐squares estimation to determine each ruleʹs consequent equations. As for the further learning of the fuzzy‐neuro MLP subnetwork, we will use a hybrid‐learning algorithm to identify the membership function parameters of the single‐output ANFIS. It will adapt the membership function parameters of
59
the ANFIS using a combination of the least‐squares and backpropagation gradient descent methods. After the training procedure is over, the cluster centers and the scaling matrices of the self‐organizing layer as well as the generated adaptive membership function parameters of the fuzzy‐neuro MLP subnetwork are frozen and ready for use in the retrieval mode, when the hybrid fuzzy‐neuro‐based QRS detector and PVC diagnostic approach is tested with ECG signals.
5.3 Implementation of Fuzzy-Neuro-Based Module The ANFIS Module or the Hybrid Fuzzy‐Neuro Module was implemented using the Graphical Interfaces ANFIS Editor GUI and the FINDCLUSTER GUI of the Fuzzy Logic Toolbox of MATLAB Version 7.0 R14. The basic structure of our Sugeno‐type inference system is a model that maps input characteristics to input membership functions, input membership functions to rules, rules to a set of output characteristics, output characteristics to output membership functions, and the output membership functions to a single‐valued output or a decision associated with the output. Let us start by giving the whole picture of the ANFIS module implementation divided into the two basic algorithms implemented and described previously.
5.2.1 The Fuzzy Clustering Algorithm This algorithm estimates the number of clusters and cluster centers in a set of data. So, it starts with an initial guess of the cluster centers, which are intended to spot the mean location of each cluster. In most cases, these initial estimates or guesses are incorrect. It also assigns every data sample point a membership grade for each cluster; i.e. a measure to how much the specific data point follows or agrees with the property described by each cluster defined by the cluster center. By iteratively updating the values of these cluster centers and the membership grades, also known as the partition matrix elements, for each data sample of the training data, the cluster centers
60
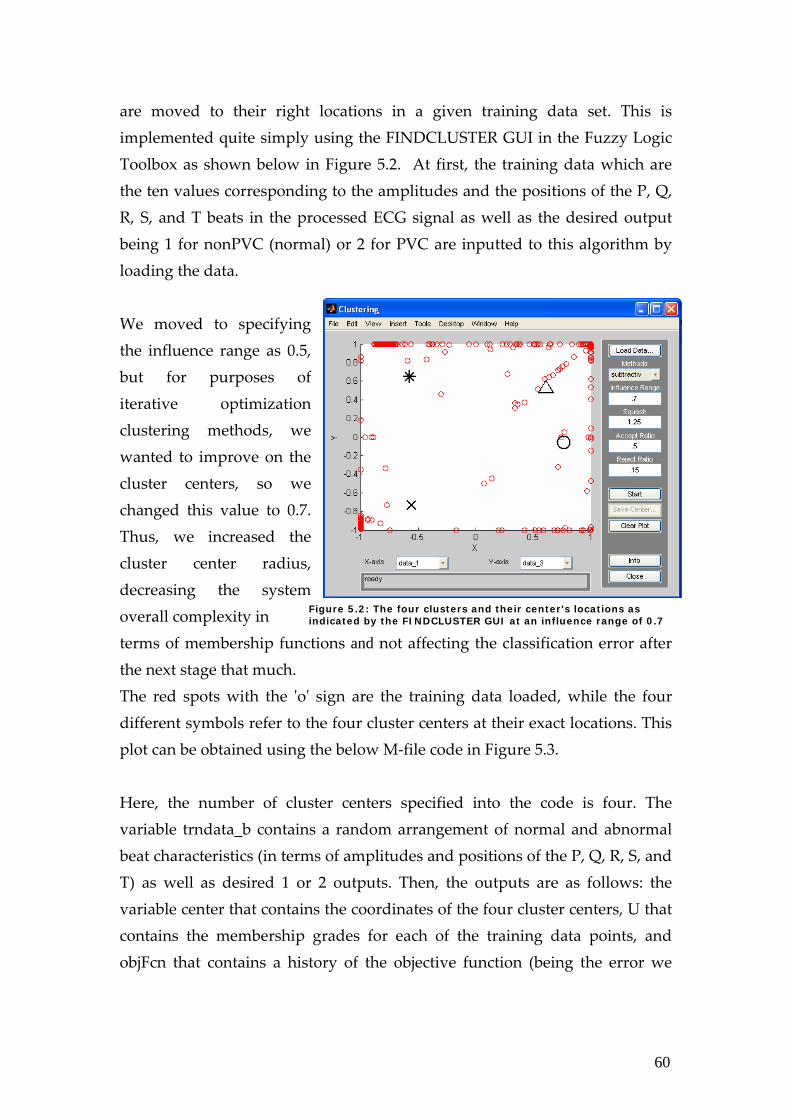
are moved to their right locations in a given training data set. This is implemented quite simply using the FINDCLUSTER GUI in the Fuzzy Logic Toolbox as shown below in Figure 5.2. At first, the training data which are the ten values corresponding to the amplitudes and the positions of the P, Q, R, S, and T beats in the processed ECG signal as well as the desired output being 1 for nonPVC (normal) or 2 for PVC are inputted to this algorithm by loading the data.
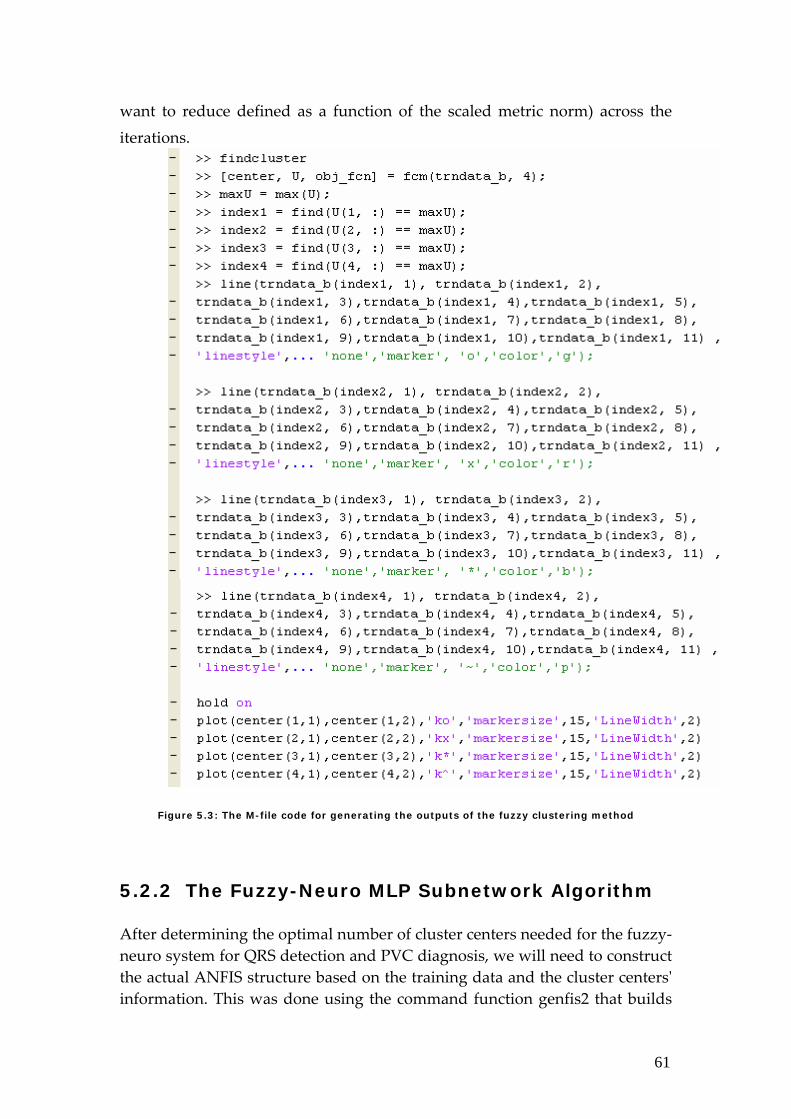
We moved to specifying the influence range as 0.5, but for purposes of iterative optimization clustering methods, we wanted to improve on the cluster centers, so we changed this value to 0.7. Thus, we increased the cluster center radius, decreasing the system overall complexity in terms of membership functions and not affecting the classification error after the next stage that much. The red spots with the ʹoʹ sign are the training data loaded, while the four different symbols refer to the four cluster centers at their exact locations. This plot can be obtained using the below M‐file code in Figure 5.3. Here, the number of cluster centers specified into the code is four. The variable trndata_b contains a random arrangement of normal and abnormal beat characteristics (in terms of amplitudes and positions of the P, Q, R, S, and T) as well as desired 1 or 2 outputs. Then, the outputs are as follows: the variable center that contains the coordinates of the four cluster centers, U that contains the membership grades for each of the training data points, and objFcn that contains a history of the objective function (being the error we
Figure 5.2: The four clusters and their center's locations as indicated by the FINDCLUSTER GUI at an influence range of 0.7
61
want to reduce defined as a function of the scaled metric norm) across the iterations.
S
H
e
Figure 5.3: The M-file code for generating the outputs of the fuzzy clustering method
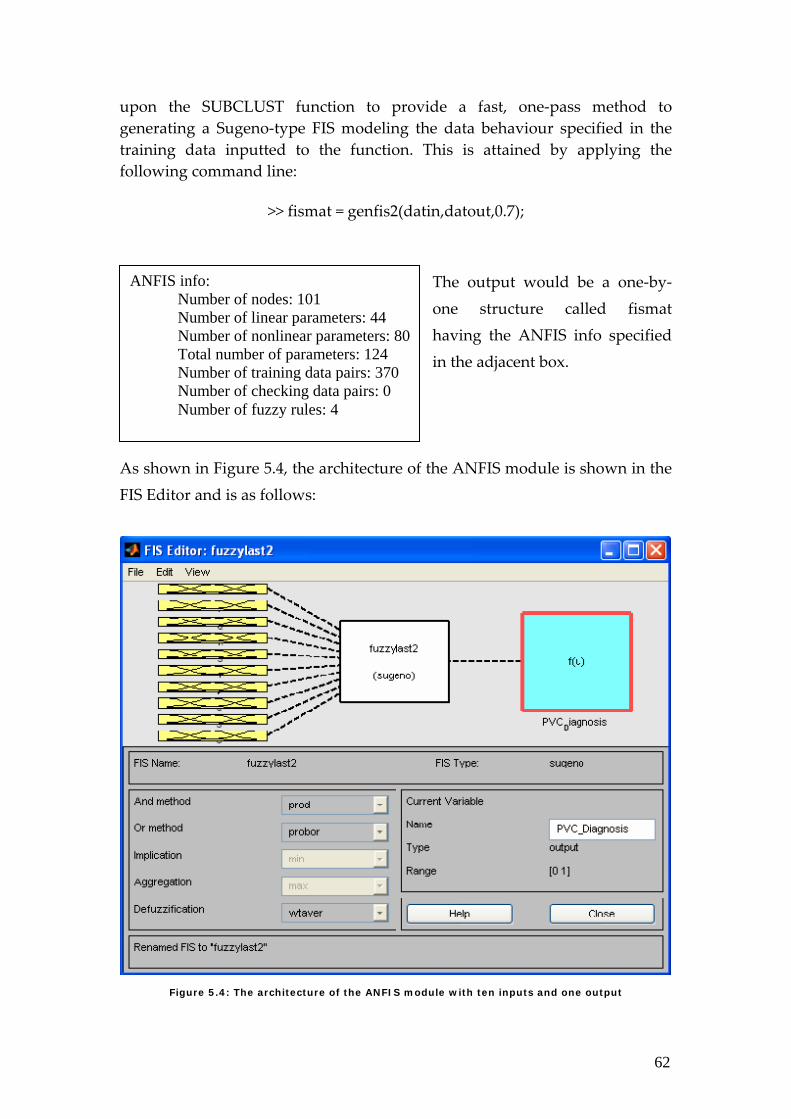
5.2.2 The Fuzzy-Neuro MLP Subnetwork Algorithm After determining the optimal number of cluster centers needed for the fuzzy‐neuro system for QRS detection and PVC diagnosis, we will need to construct the actual ANFIS structure based on the training data and the cluster centersʹ information. This was done using the command function genfis2 that builds
62
upon the SUBCLUST function to provide a fast, one‐pass method to generating a Sugeno‐type FIS modeling the data behaviour specified in the training data inputted to the function. This is attained by applying the following command line:
>> fismat = genfis2(datin,datout,0.7);
The output would be a one‐by‐one structure called fismat having the ANFIS info specified in the adjacent box.
As shown in Figure 5.4, the architecture of the ANFIS module is shown in the FIS Editor and is as follows:
Figure 5.4: The architecture of the ANFIS module with ten inputs and one output
ANFIS info: Number of nodes: 101 Number of linear parameters: 44 Number of nonlinear parameters: 80 Total number of parameters: 124 Number of training data pairs: 370 Number of checking data pairs: 0 Number of fuzzy rules: 4
63
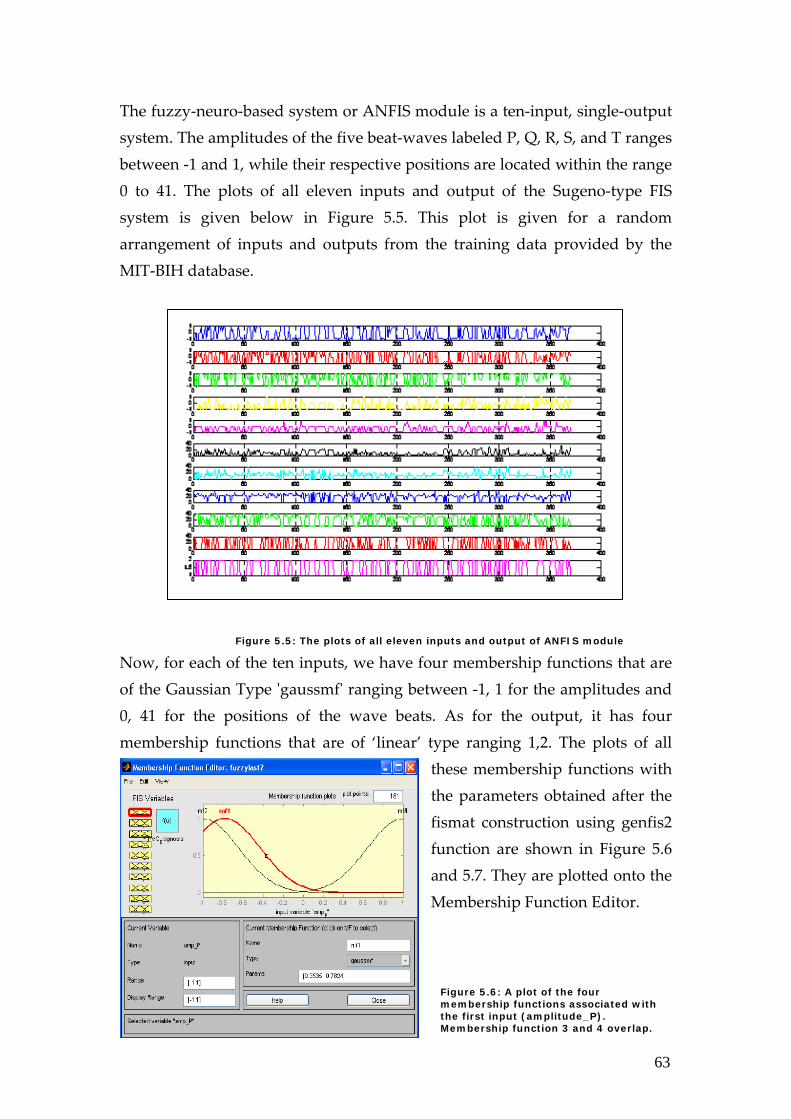
The fuzzy‐neuro‐based system or ANFIS module is a ten‐input, single‐output system. The amplitudes of the five beat‐waves labeled P, Q, R, S, and T ranges between ‐1 and 1, while their respective positions are located within the range 0 to 41. The plots of all eleven inputs and output of the Sugeno‐type FIS system is given below in Figure 5.5. This plot is given for a random arrangement of inputs and outputs from the training data provided by the MIT‐BIH database.
Figure 5.5: The plots of all eleven inputs and output of ANFIS module
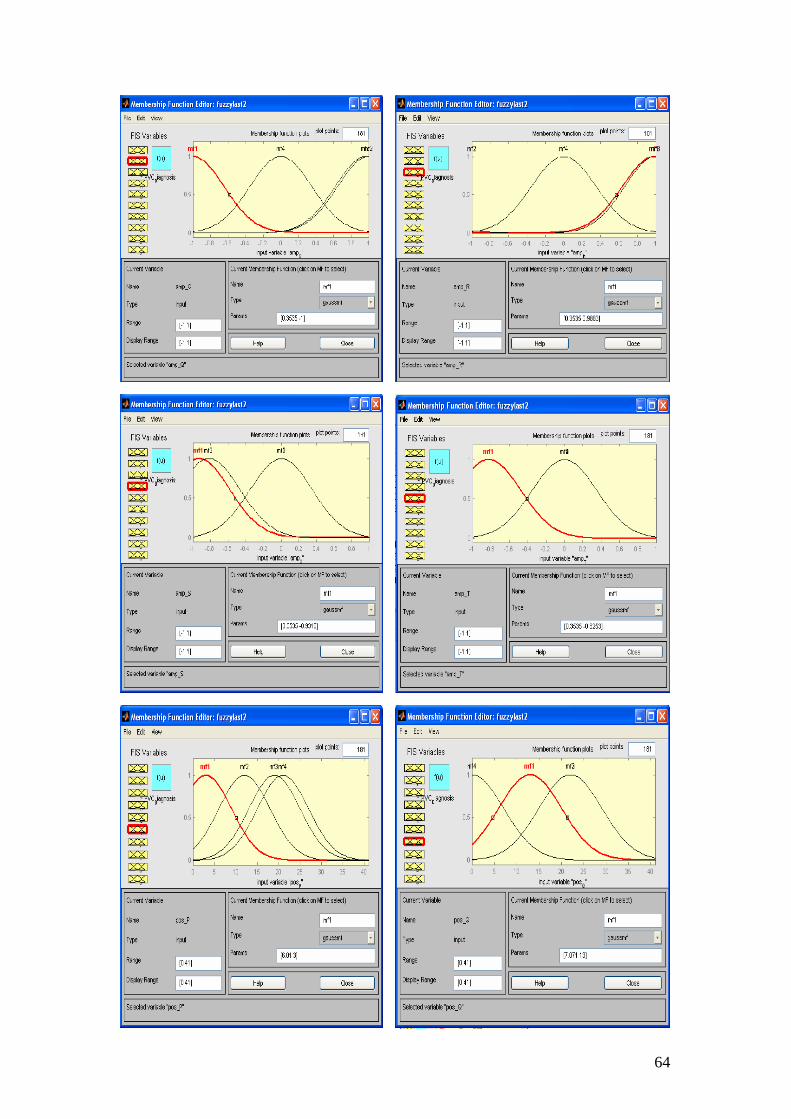
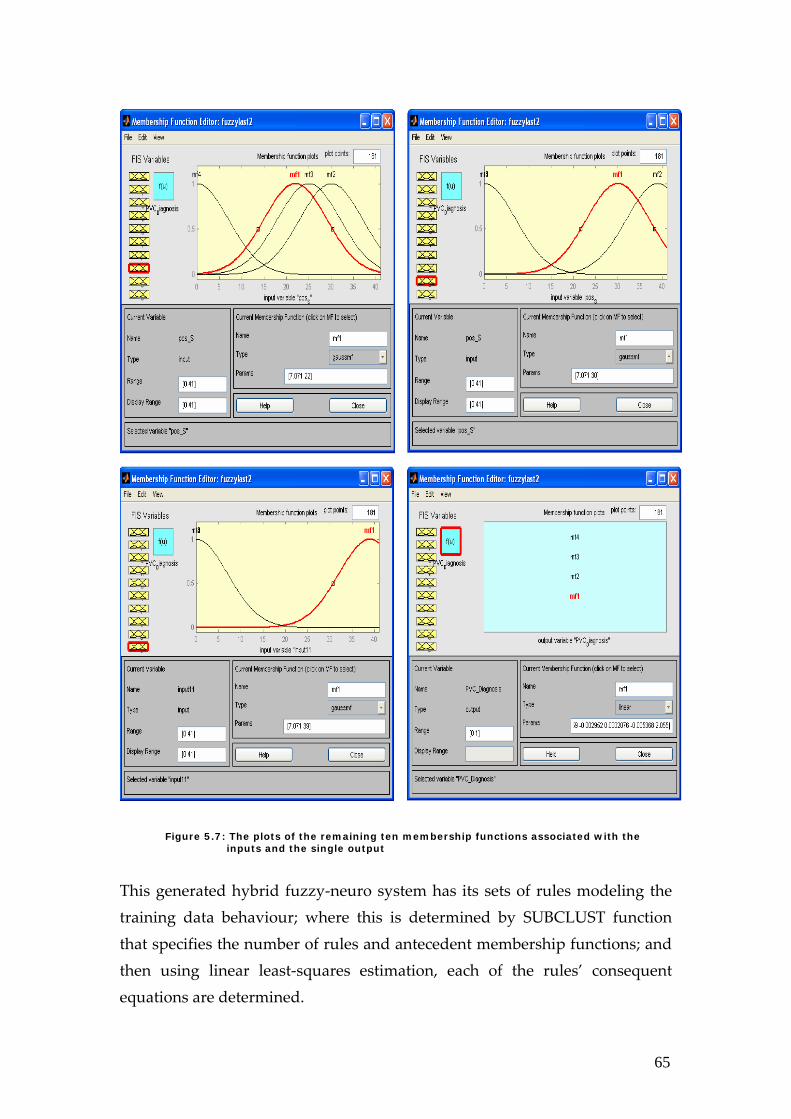
Now, for each of the ten inputs, we have four membership functions that are of the Gaussian Type ʹgaussmfʹ ranging between ‐1, 1 for the amplitudes and 0, 41 for the positions of the wave beats. As for the output, it has four membership functions that are of ‘linear’ type ranging 1,2. The plots of all
these membership functions with the parameters obtained after the fismat construction using genfis2 function are shown in Figure 5.6 and 5.7. They are plotted onto the Membership Function Editor.
Figure 5.6: A plot of the four membership functions associated with the first input (amplitude_P). Membership function 3 and 4 overlap.
64
65
This generated hybrid fuzzy‐neuro system has its sets of rules modeling the training data behaviour; where this is determined by SUBCLUST function that specifies the number of rules and antecedent membership functions; and then using linear least‐squares estimation, each of the rules’ consequent equations are determined.
Figure 5.7: The plots of the remaining ten membership functions associated with the inputs and the single output
66
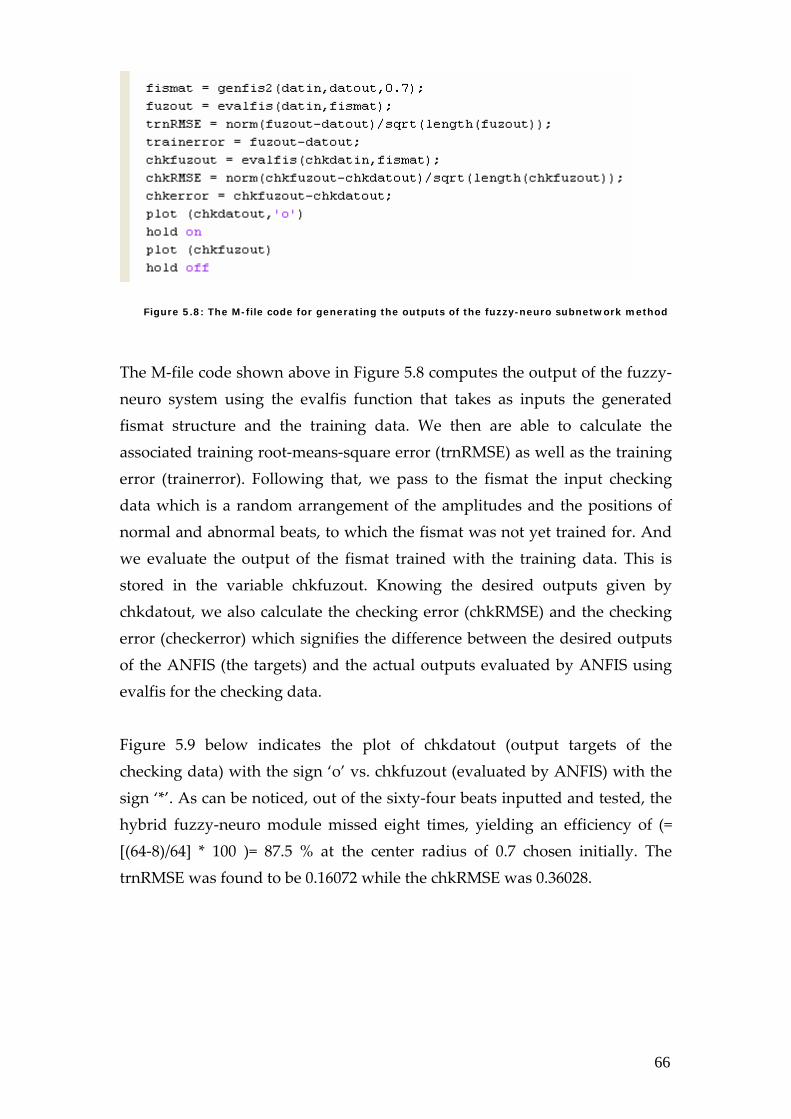
Figure 5.8: The M-file code for generating the outputs of the fuzzy-neuro subnetwork method
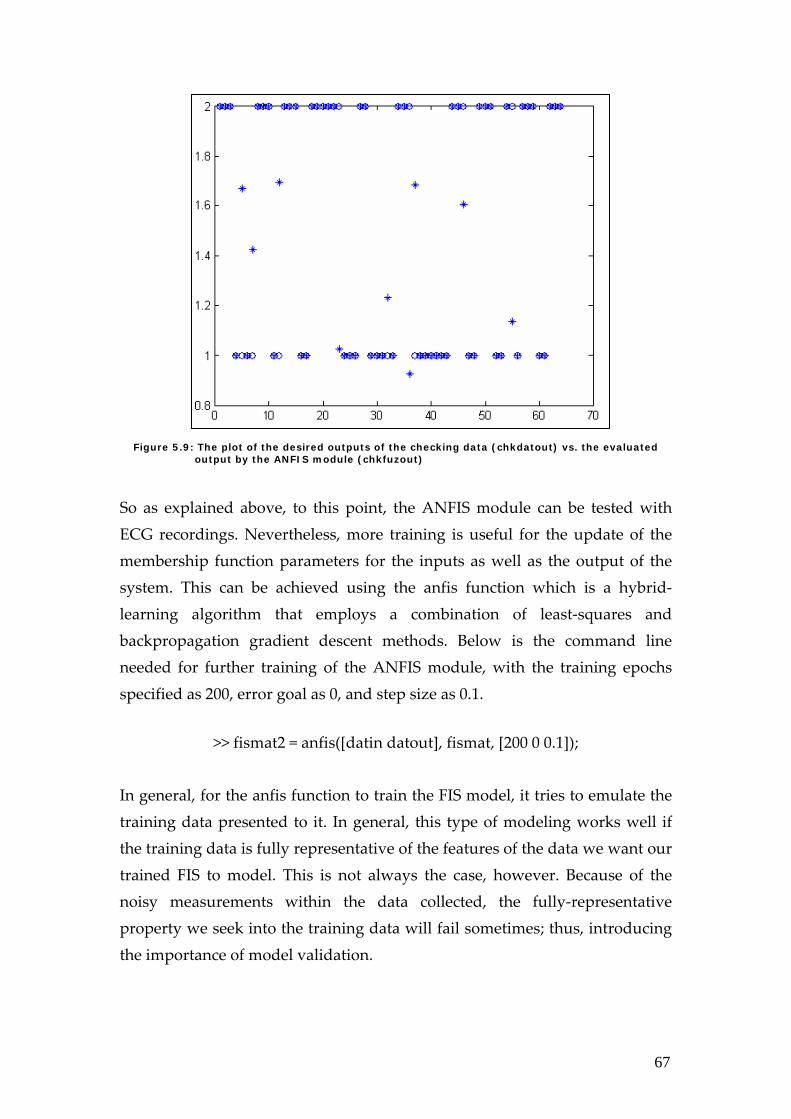
The M‐file code shown above in Figure 5.8 computes the output of the fuzzy‐neuro system using the evalfis function that takes as inputs the generated fismat structure and the training data. We then are able to calculate the associated training root‐means‐square error (trnRMSE) as well as the training error (trainerror). Following that, we pass to the fismat the input checking data which is a random arrangement of the amplitudes and the positions of normal and abnormal beats, to which the fismat was not yet trained for. And we evaluate the output of the fismat trained with the training data. This is stored in the variable chkfuzout. Knowing the desired outputs given by chkdatout, we also calculate the checking error (chkRMSE) and the checking error (checkerror) which signifies the difference between the desired outputs of the ANFIS (the targets) and the actual outputs evaluated by ANFIS using evalfis for the checking data. Figure 5.9 below indicates the plot of chkdatout (output targets of the checking data) with the sign ‘o’ vs. chkfuzout (evaluated by ANFIS) with the sign ‘*’. As can be noticed, out of the sixty‐four beats inputted and tested, the hybrid fuzzy‐neuro module missed eight times, yielding an efficiency of (= [(64‐8)/64] * 100 )= 87.5 % at the center radius of 0.7 chosen initially. The trnRMSE was found to be 0.16072 while the chkRMSE was 0.36028.
67
Figure 5.9: The plot of the desired outputs of the checking data (chkdatout) vs. the evaluated output by the ANFIS module (chkfuzout) So as explained above, to this point, the ANFIS module can be tested with ECG recordings. Nevertheless, more training is useful for the update of the membership function parameters for the inputs as well as the output of the system. This can be achieved using the anfis function which is a hybrid‐learning algorithm that employs a combination of least‐squares and backpropagation gradient descent methods. Below is the command line needed for further training of the ANFIS module, with the training epochs specified as 200, error goal as 0, and step size as 0.1.
>> fismat2 = anfis([datin datout], fismat, [200 0 0.1]); In general, for the anfis function to train the FIS model, it tries to emulate the training data presented to it. In general, this type of modeling works well if the training data is fully representative of the features of the data we want our trained FIS to model. This is not always the case, however. Because of the noisy measurements within the data collected, the fully‐representative property we seek into the training data will fail sometimes; thus, introducing the importance of model validation.
68
Model Validation is the process of presenting input/output data pairs to which the ANFIS module was not trained for, and realizing how well is the ANFIS model predicting the corresponding data set output values. Here, it should be noted that increasing the number of epochs to which the ANFIS module is trained for can be troublesome in the sense that it can create a problem of the system overfitting the data to which it is being trained for. So, we need to be very careful in choosing the number of training epochs, and it is significant for the model validation not becoming trivial to have a large set of data from which we are choosing randomly our training and checking data.
It should be mentioned that the implementation was carried out on an IBM‐PC (Intel/3.2 GHz with 2 GB of RAM), using MATLAB (Mathworks Inc., Natick, Massachusetts).
5.4 Results of Fuzzy-Neuro-Based Module
To compare our hybrid fuzzy‐neuro module with other approaches used for QRS detection and ECG beat recognition, specifically for the PVC diagnosis, we have used the record 108 out of the MIT‐BIH standard database. The comparison was made to the following beat recognition systems, reported in the international journals: hybrid fuzzy neural network (FHyb‐HOSA)[18], multistage systems using MLP (MLP1) [24]; multistage systems using MLP (MLP2) [28]; expert system using Kohonen and SVD (SOM‐SVD) [29]; LVQ and autoregression AR MLP (MLP‐LVQ) [30]; and Fourier and MLP (MLP‐Fourier) [31]. The tables Table 5.1 and Table 5.2 shown below summarize respectively the comparative results of the rate of misclassification (given in %) and the efficiency (given in % as well) of premature ventricular contraction beats, labeled as ‘V’ in the database, using the systems presented above.
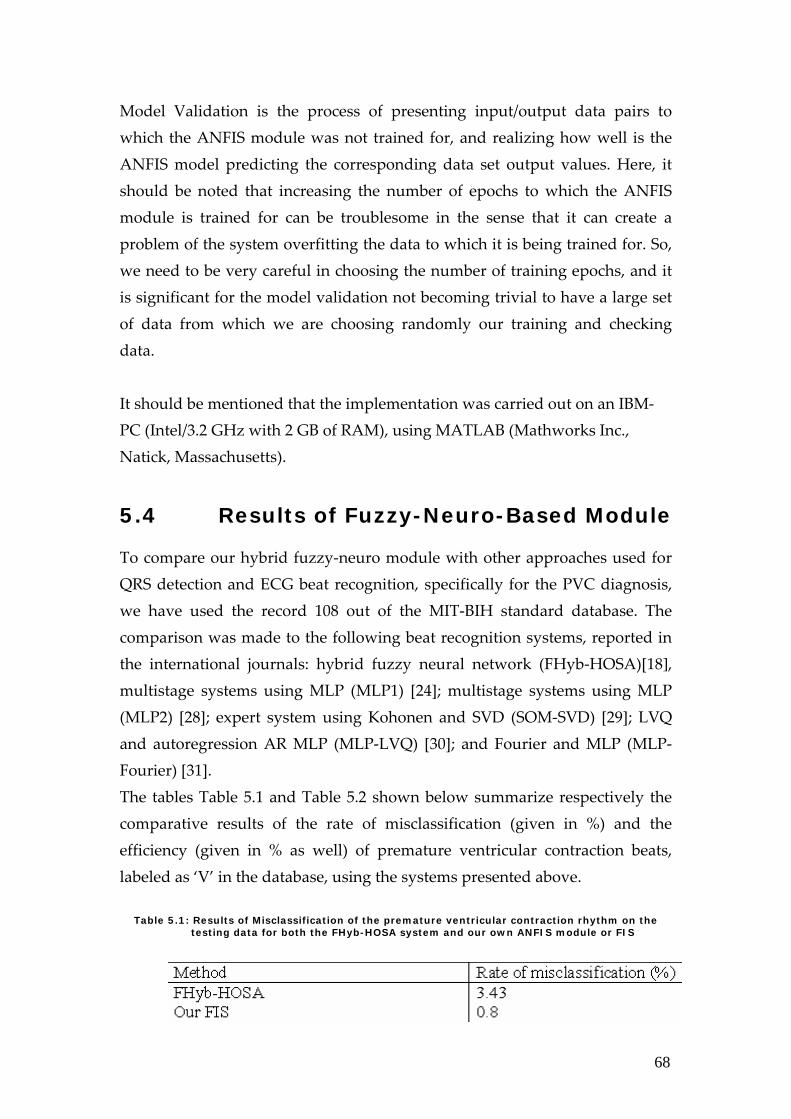
Table 5.1: Results of Misclassification of the premature ventricular contraction rhythm on the testing data for both the FHyb-HOSA system and our own ANFIS module or FIS
69
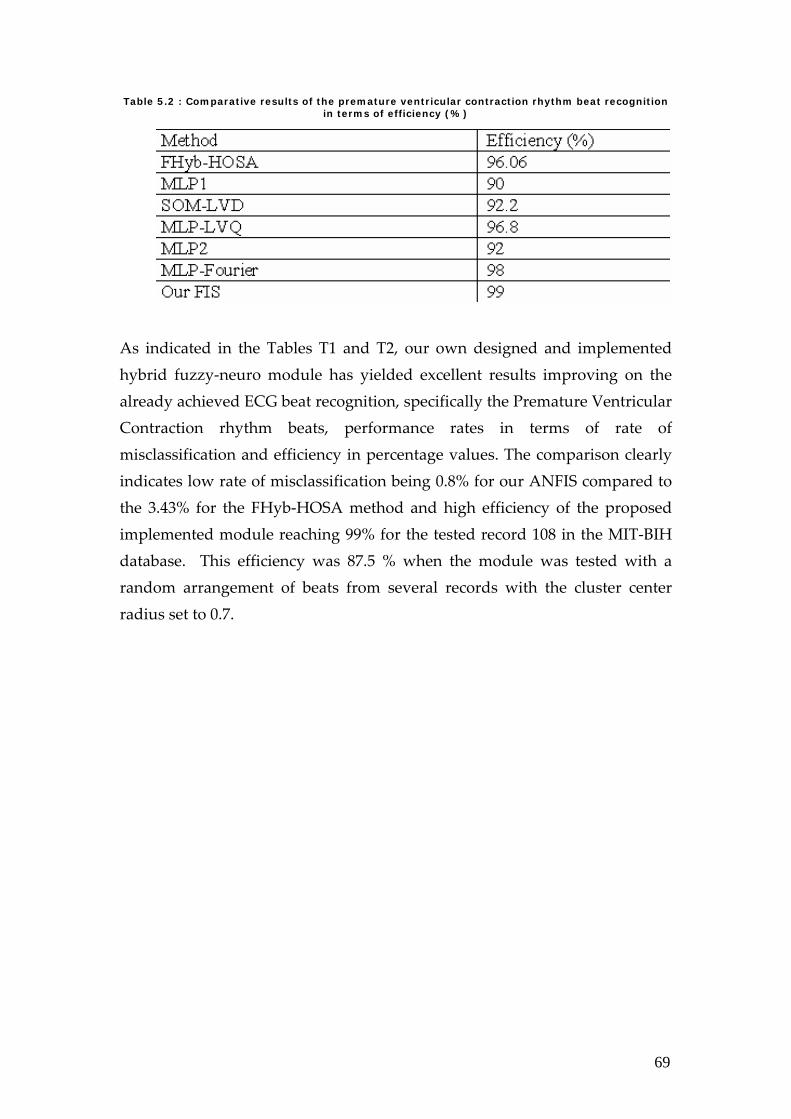
Table 5.2 : Comparative results of the premature ventricular contraction rhythm beat recognition in terms of efficiency (%)
As indicated in the Tables T1 and T2, our own designed and implemented hybrid fuzzy‐neuro module has yielded excellent results improving on the already achieved ECG beat recognition, specifically the Premature Ventricular Contraction rhythm beats, performance rates in terms of rate of misclassification and efficiency in percentage values. The comparison clearly indicates low rate of misclassification being 0.8% for our ANFIS compared to the 3.43% for the FHyb‐HOSA method and high efficiency of the proposed implemented module reaching 99% for the tested record 108 in the MIT‐BIH database. This efficiency was 87.5 % when the module was tested with a random arrangement of beats from several records with the cluster center radius set to 0.7.
70
Chapter 6 Conclusion The great variety of QRS detection and PVC diagnostic algorithms reflect the need for a reliable method for QRS detection and PVC diagnosis in cardiac signal processing. The currently achievable detection rates reflect only the overall performance of the detectors. These numbers hide the problems that are still present in case of noisy or abnormal ECG signals. A satisfying solution to these problems is still not found. In our final year project, we have chosen to design and implement two techniques by which QRS detection and PVC diagnosis are achieved. These are:
1. Artificial Neural Network 2. Hybrid Fuzzy‐neuro Network
We have implemented both techniques in MATLAB using three specialized toolboxes that we have described in the report. The modules implemented aim at performing two tasks: QRS complex detection and PVC diagnosis. These modules managed to perform reliable QRS complex detection and PVC diagnosis in an enhanced and efficient manner. At the end of our fyp work, it is notable to state that our work exhibited good results as we have aspired and hopefully we have made a valuable contribution to the field of cardiac signal processing.
71
6.1 ABET Considerations In the process of design and implementation of any system or process, there are in fact several issues that we need to take into consideration in terms of realistic constraints or boundaries imposed. These can be economic, environmental, social, political, ethical, health and safety, manufacturability and sustainability issues. In our case, we have implemented two modules, the Artificial Neural Network Module and the Hybrid Fuzzy‐Neuro Module in MATLAB using three specialized toolboxes. The two modules aim at performing two tasks: QRS complex detection and PVC diagnosis. In what follows, we will be discussing how the above constraints can be related or realized in our two modules or systems. 1. Economic: In terms of economy, our two systems are software‐integrated implemented on MATLAB. So, in terms of actual cost or budget constraints set by us, there was none due to the lack of the need. Nevertheless, for our systems to be later used in hospitals and clinics, both private and public, for real‐time QRS detection and PVC diagnosis, there will be this economical consideration in terms of the need for the hospital or the clinic to acquire MATLAB and buy its license. This can be avoided if we later on consider writing the two systems, starting from the MATLAB work we have done, in another language that can be less expensive to the hospital or the clinic making use of the systems. 2. Environmental: As for the environmental considerations, these are significant for any responsible person let alone an engineer involved in providing practical solutions to real‐life problems. In our case, given that we have designed two modules but our implementation was software‐oriented, we did not have that concern much. It would have been the case if we had considered actual hardware implementation or even FPGA realization.

72
3. Social: Given that the ultimate goal of our final year project is to be allocated into health services and used among cardiologists and doctors in hospitals or clinics, there exist some social issues here. We need to make the simulation of the two implemented modules, the artificial neural network one and the hybrid fuzzy‐neuro one, as user‐friendly as possible, because software manipulation may not be the expertise of the one handling the simulation run. So, in this case, we need to set out a clear set of instructions or module tutorial which we somehow did in the implementation section in Chapters 4 and 5 in our report. This will really facilitate the job of the person using our systems. Other issues in question can be both socially and economically realized. They have economic roots or origins but they appear more socially related. These are the issues on how to make these services accessible to all classes in the society, especially keeping in mind that this is a new technology employed and not available at all hospitals and clinics. In that case, as hospitals or clinics will be charged for buying the modules first from us and then getting MATLAB, the running software for now, as well as its license, this will incur high charges on people in need of ECG beat interpretation. And here we need to address these issues with scrutiny and delicate care. 4. Political: This does not quite fit our final year project because it is simply not related in any way. 5. Ethical: In terms of ethics and morality, these are of high significance of course because in the end we are aiming onto providing systems handling the health benefit of people, which is quite a responsibility. So, we need to be as responsible and humanistic in terms of incorporating all ethical worries in our handling of all stages of the work: design, implementation,
73
development and marketing later on. We have always taken seriously the honesty factor in all of these stages, especially when it comes to result reporting and work documentation. We have also worked hard to obtain the best possible results for the modules we have designed and implemented, comparing our results at every step of the way to other systemsʹ results provided in the literature. 6. Health and Safety: When it comes to health and safety, a flag is raised. This is one of the priorities that we have set in handling issues related to the final year project. Our fyp, being of a biomedical application, it serves a health‐related purpose. And to this, we have performed reliable QRS detection and PVC diagnosis in an enhanced and highly‐efficient way in an attempt to make ECG abnormalitiesʹ diagnosis stretch to a larger dimension from the smaller one, which is the need of expertise of cardiologists, which can be complementary and informative to our workʹs diagnosis. 7. Manufacturability and Sustainability: Speaking of any system or process implies having manufacturability and sustainability concerns. As for the first, this is conceivable in our implementation later on when we make it integrated into hardware; for instance as part or option of an existing ECG machine in a hospital or even a separate QRS detection and PVC diagnostic machine. And here comes the issues we have spoken earlier on in the economic, social and ethical points stated above. When it comes to the second concern, the sustainability issue, we need to thoroughly examine the proper time schedule for software maintenance and later hardware check. This should be made with cooperation of the modulesʹ acquiring party (hospital, clinics, private ownership by individual, etc…), the MATLAB or any other language if the work were to be revised later on programmers and software specialists, and the Ministry of Health Services if seen needed.
74
The above stated seven points are to be considered realistically when dealing with any system or process. This is why we have taken what is related in them and incorporated that into the considerations of our final year project.
75
Bibliography
1. “PhysioBank MIT‐BIH Database”, http://www.physionet.org/physiobank/database. 2. Bin Ramli, and P. Aidawati Ahmad, « Correlation analysis for
abnormal ECG signal features extraction, » Proceedings of the 4th National Conference on Telecommunication Technology Proceedings, IEEE, pp. 232‐237, 2003.
3. E. J. Berbari, Bioelectric Phenomena: Principles of Electrocardiography. Chap. 13: CRC Press LLC, 1995.
4. E. Karam and G. M. Drzewiecki, « Modeling of hypertension‐induced Left Ventricular Hypertrophy, » Proceedings of the 7th Annual Northeast Bioengineering Conference, 1991.
5. F. U. Humez and P. W. Macfarlane, « Assessment of selected ECG voltage criteria for abnormality in eccentric and concentric Left Ventricular Hypertrophy, » Computers in Cardiology, vol. 30, pp. 57‐59, 2003.
6. F.G, Yanowitz, M.D., The Alan E. Lindsay ECG Learning Center in Cyberspace, University of Utah School of Medicine. Online: http://medstat.med.utah.edu/kw/ecg/index.html.
7. Full Help of Fuzzy Logic Tool Box of MATLAB Version 7.0.1 R14. 8. G. McDarby, B.G. Celler, N. H. Lovell, Characterising the Discrete Wavelet Transform of an ECG Signal with Simple Parameters for use in Automated Diagnosis, 2nd International Conference on Bioelectromagnetism, February 1998, Melbourne Australia.
9. K. Englehart, P. Parker, B. Hudgins, Chapter eight: Wavelet methods in biomedical signal processing, Handbook of Neuroprosthetic Methods (Biomedical Engineering), Book, CRC Press LLC, 2003. Available Online: http://www.neurosciencenetbase.com/ejournals/books.
10. K.Wachtell, J. N. Bella, P. R. Liebson, E. Gerdts, B. Dahlöf, T. Aalto, M.
76
J. Roman, V. Papademetriou, H. Ibsen, J. Rokkedal, and R. B. Devereux, « Impact of different partition values on prevalences of Left Ventricular Hypertrophy and concentric geometry in a large hypertensive population, » The American Heart Association, Inc. , vol. 35, no. 6 , 2000.
11. Li, C. Zheng, C. Tai, Detection of ECG Characteristic Points Using Wavelet Transforms, IEEE Transactions on Biomedical Engineering, Vol. 42 No. 1, January 1995.
12. M. A. Al‐Alaoui, « A unified analog and digital design to peak and valley detector, window peak and valley detectors, and zero crossing detectors, » IEEE Trans. on Instrumentation and Measurement, vol. 35, pp. 304‐307, 1986.
13. M. A. Al‐Alaoui, J. El Achkar, M. Hijazi, T. Zeineddine, and M. Khuri, «Application of artificial neural networks to QRS detection and LVH diagnosis,» Proceedings of ICECSʹ 95, December 1995.
14. M. Kundu, M. Nasipuri, and D. K. Basu, «A knowledge‐based approach to ECG interpretation using fuzzy logic, » IEEE Trans. on Syst., Man, and Cybern., vol. 28, no. 2, pp. 237‐243, April 1998.
15. M.J. Vaessen, A QRS detection method using analog wavelet transform in ECG analysis, June 20, 2005. Available: Online http://www.fdaw.unimaas.nl/education/bachelor/conference/7.pdf.
16. N.A. Mark Estes III, M. S. Link, M. Homoud, and P. J. Wang, « ECG findings in active patients, » The Physician and Sportsmedicine, vol. 29, no. 3, March 2001.
17. P. M. Okin, M. J. Roman, R. B. Devereux, and P. Kligfield, « Time‐voltage area of the QRS for the identification of Left Ventricular Hypertrophy, » The American Heart Association, Inc. , vol. 27, pp. 251‐258, 1996.
18. S. Osowski, and Tran Hoai Linh, «ECG beat recognition using fuzzy hybrid neural network, » IEEE Trans. Biomed. Eng., vol. 48, no. 11, pp. 1265‐1271, November 2001.
19. S.M. Szilagi, Comparison of The Neural_network‐based Adaptive Filtering and Wavelet Transform for R, T and P Waves Detection, Technical University of Budapest, 1997.
20. U. Köhler, C. Hennig, and R. Orglmeister, « The principles of software
77
QRS detection, » IEEE Trans. Biomed. Eng., vol. 2, pp. 42‐57, January 2002.
21. W.J. Tompkins, Biomedical Digital Signal Processing, Prentice Hall, New Jersey, 1993.
22. Y. Deng, W. Wolf, R. Schnell and U. Appel, « New aspects to event‐synchronous cancellation of ECG interference: an application of the method in diaphragmatic EMG signals, » IEEE Trans. Biomed. Eng., vol. 47, no. 9, pp. 1177‐1184, September 2000.
23. Y. Hen Hu, and J. N. Hwang, Neural Networks HandBook: Introduction to Neural Networks for Signal Processing. Chap. 1: CRC Press LLC, 2002.
24. Y. Hen Hu, W. J. Tompkins, J. L. Urrusti, and V. X. Afonso, «Applications of artificial neural networks for ECG signal detection and classification, » Journal of Electrocardiography, vol. 26 supplement, pp. 66‐73, 1993.
25. N. Shublaq, «A fuzzy rule‐based system for real‐time filtration of contaminated EMGdi signals, » Summer Training Report at Ecole Polytechnique de Montreal, 2005.
26. PhysioBank Fantasia Database”, http://www.physionet.org/physiobank/database/fantasia/ 27. N. Izeboudjen, and A. Farah, «A new neural network system for
arrhythmiaʹs classification, » Proc. Neural Networks Conference, Vienna, Austria, pp. 208‐216, 1998.
28. Y. Hen Hu, S. Palreddy, and W. J. Tompkins, «A patient adaptable ECG beat classifier using a mixture of experts approach, » IEEE Trans. Biomed. Eng., vol. 44, pp. 891‐900, September 1997.
29. G. E. Oien, N. A. Bertelsen, T. Eftestol, and J. H. Husoy, «ECG rhythm classification using artificial neural networks, » Proc. 1996 IEEE Digital Signal Processing Workshop, pp. 514‐517, 1996.
30. K. Minami, H. Nakajima, and T. Toyoshima, «Real‐time discrimination of ventricular tachyarrhythmia with Fourier‐transform neural network, IEEE Trans. Biomed. Eng., vol. 46, pp. 179‐185, February 1999.
31.Premature Ventricular Contractions, Available Online: http://heart.healthcentersonline.com/arrhythmia/pvc.cfm
32. “Premature Ventricular Contraction”, Wikepedia the Free Encyclopedia, Available Online:
http://en.wikipedia.org/wiki/Premature_ventricular_contraction
78
33. M. A. Al‐Alaoui, « A unified analog and digital design to peak and valley detector, window peak and valley detectors, and zero crossing detectors, » IEEE Trans. on Instrumentation and Measurement, vol. 35, pp. 304‐307, 1986.