acnp 2015 pact
TRANSCRIPT
Testing the “PACT” Strategy: Amphetamine Enhances Gains in Auditory Discrimination Training in Adult Schizophrenia Patients Neal R. Swerdlow1, Melissa Tarasenko1,2, Savita G. Bhakta1, Jo Talledo1,Erica L. Hughes1, Alexis I. Alvarez1, Brinda Rana1, Sophia Vinogradov3, Gregory A. Light1,2
1UC San Diego Dept. Psychiatry; 2VISN-22 MIRECC, VA San Diego Healthcare System; 3UC San Francisco Dept. Psychiatry
Abstract
References
DiscussionMethods
Conflicts of Interest
Introduction
Results
Background An intensive program of computerized targeted cognitive training (TCT) of auditory processing and auditory working memory appears to drive improvements in higher-order cognition in schizophrenia (SZ) patients. Potentially, such therapeutic effects might be facilitated pharmacologically, via drugs that enhance attention, sensory processing and/or working memory processes that are taxed by the training. If this “pharmacologically augmented cognitive therapy” (“PACT”) strategy is successful, it might be possible to augment and accelerate the clinical benefits of TCT in SZ patients. Because gains in auditory psychophysical efficiency can be detected after a single one-hour session of training, it is possible to use a placebo (PBO)-controlled single dose cross-over design to assess drug effects on training response. We assessed the effects of the pro-attentional drug, d-amphetamine (AMPH; 10 mg po), on one hour of auditory TCT in SZ patients and healthy subjects (HS). Methods Carefully screened and characterized HS and patients with a diagnosis of SZ participated in this study; this sample included only individuals homozygous (AA or GG) at the rs4680 SNP for COMT. Subjects were tested three times with 1 week between tests: first in a screening session (no pill administered), and next in a double-blind order-balanced crossover design (test days 2 and 3), comparing PBO vs. 10 mg of AMPH. On each test day, 1 hour of Posit Science “Sound Sweeps” training was bracketed by brief (2-4 min) pre- and post-training assessments of auditory processing speed (APS). Training consisted of a speeded auditory time-order judgment task of two successive frequency modulation (FM) sweeps. On test days 2 and 3, pre-training assessments began 210 min post-pill administration, when 10 mg AMPH is known to be bioactive. Autonomic and subjective measures were collected throughout test days 2 and 3. All test days also included measures of neurocognition and sensorimotor gating, reported separately. Results AMPH was bioactive, enhancing autonomic function as well as subjective measures of alertness in HS. Baseline (screening and pre-training) performance (APS, trials completed) was impaired in SZ patients vs. HS (all p’s<0.02–0.0001). Auditory system “learning” (APS post- vs. pre-training) was enhanced by AMPH, and this effect was relatively comparable in HS and patients (main effect of diagnosis: ns; main effect of AMPH: p<0.035; diagnosis x drug interaction: p<0.085; effect of AMPH in patients: d=0.40; main effect of AMPH in HS: d=0.27. Independent of diagnosis, AMPH effects on auditory system “learning” tended to be greater among rs4680 AA vs. GG subjects (p<0.02); learning achieved statistical significance only among AA (p<0.002) but not GG subjects (ns). Conclusions We demonstrate that a low dose of the pro-attentional drug, AMPH, enhances auditory discrimination learning in SZ patients. This effect may not be unique to SZ: a weaker but similar effect in HS supports the notion that AMPH’s benefits in SZ patients reflect an enhancement of intact brain mechanisms, in the service of the attentional demands of training. Identifying patients most sensitive to such drug effects via biomarkers is an important part of the “PACT” strategy, and the present findings provide tentative evidence that AMPH effects on auditory discrimination learning may be most pronounced among individuals homozygous for methionine at the rs4680 SNP. It is important to note that we do not yet know whether the behavioral improvement (i.e. gains in APS) observed in SZ patients after a single session of auditory discrimination training predicts clinical benefits after an entire course of 30-50 hours of auditory system exercises. However, if such benefits are demonstrated, and AMPH can enhance the therapeutic effects of training, then this “PACT” approach could represent a transformative treatment paradigm for SZ.
GAL has served as a consultant for Astellas, Forum Pharmaceuticals, Boehringer Ingelheim and Neuroverse. SV serves as a site PI on an SBIR grant to Positscience.
Neurocognitive deficits contribute strongly to functional disability in chronic psychotic disorders, including schizophrenia (SZ). While antipsychotics can blunt the most severe acute psychotic symptoms, they are generally ineffective in treating negative symptoms or neurocognitive deficits. Efforts at remediating cognitive deficits using computerized targeted cognitive training (TCT) have generally shown a modest degree of efficacy at the group level, yet almost half of all SZ patients demonstrate virtually no cognitive enhancement after undergoing a therapeutic dose (e.g. 40 hours) of TCT. For patients and clinicians, the costs associated with these time- and resource-intensive interventions can be prohibitive. An area of active research – and the topic of a 2012 ACNP Panel - is the development of Pharmacologically Augmented Cognitive Therapies (“PACTs”) for SZ: can drugs with pro-cognitive effects will specifically, and perhaps synergistically, augment the clinical benefits of cognitive therapies such as TCT? A "proof of concept" for this approach is found in the use of pro-extinction drugs to selectively enhance the therapeutic impact of cognitive therapies for anxiety disorders. We hypothesize that in the context of TCT for SZ, pro-cognitive agents will be particularly effective in enhancing function in subgroups of patients with specific neurobiological and/or genetic characteristics. This study tested the hypothesis that the pro-attention drug, d-amphetamine (AMPH), will enhance performance of a TCT task – Posit Science “Sound Sweeps” – which is known to enhance neurocognition in groups of SZ patients. Such an observation would establish a clear rationale for predicting enhanced therapeutic effects of a PACT paradigm in which AMPH is paired with TCT.
Paid participants (N’s: HS = 20; SZ = 15) were carefully screened to establish appropriate diagnoses and rule out potential exclusionary conditions (pregnancy, current substance abuse, significant medical illness, seizure history, open head injury or closed head injury with loss of consciousness >1 min, known hearing or visual impairment). Screening and 2 test sessions were conducted 5-10 days apart. Alleles in rs4680 were identified from saliva prior to screening via a restriction fragment length polymorphism after PCR amplification. All SZ subjects had been maintained on stable AP doses for > 1 month. Testing included measures of acoustic startle and prepulse inhibition, as well as measures of neurocognition (MATRICS Consensus Neurocognitive Battery; MCCB) and TCT performance. Targeted Cognitive Training (TCT) (PositScience; brainhq.com) is a computerized cognitive training program that targets both low-level auditory perceptual processes and higher order attention and working memory operations. The present study utilized one of the most basic training exercises, “Sound Sweeps,” an auditory frequency discrimination time-order judgment task. In this exercise, participants were presented with pairs of frequency-modulated sound “sweeps” and indicated whether they perceived each sweep as becoming higher or lower in pitch. The training is continuously adaptive – sweep duration, frequency range, and interstimulus interval (ISI) become shorter after correct responses, but longer after incorrect responses. Correct responses are rewarded with reinforcing visual and auditory stimuli. Training is divided into stages, with each stage comprised of levels that differ by stimulus frequency and ISI. Baseline auditory processing speed (APS) is calculated for each level based on the shortest duration of stimuli that participants are able to correctly discriminate upon initial exposure to that level. To progress to the next level, participants must either match their baseline APS score (i.e. discriminate stimulus pairs that are equivalent in duration) or surpass their baseline APS score (i.e. discriminate stimulus pairs that are shorter in duration) – this stimulus duration constitutes their “best” APS score for that level. Baseline and best APS scores are calculated for each level, with possible scores ranging from 13-1,000ms and lower scores indicating better APS. On screen and test days, subjects completed 1h of TCT. A practice block of Sound Sweep exercises was administered prior to training to ensure familiarity with computers and comprehension of task instructions. All participants successfully completed the practice block and demonstrated an understanding of the task before beginning the training. Thus, the practice block served to minimize early variability in performance due to factors other than APS. A research assistant monitored the session, which lasted one hour. Analytic software yielded the dependent measures: subjects’ across-session improvement score, processing speed percentile and total number of levels completed.
A low dose of the pro-attentional drug, AMPH, enhanced auditory discrimination learning in SZ patients. This effect may not be unique to SZ: a weaker but similar effect in HS supports the notion that AMPH’s benefits in SZ patients reflect an enhancement of intact brain mechanisms, in the service of the attentional demands of training. Conceivably, by enhancing auditory discrimination learning, AMPH might accelerate or potentiate the neurocognitive and functional gains associated with this form of TCT; if the underlying mechanisms of AMPH effects reflect enhanced attention rather than an auditory-specific process, then such AMPH effects might generalize to other forms of TCT. This hypothesis will be tested next. We detected no adverse consequences of exposure to 10 mg of AMPH among our antipsychotic-treated SZ patients. This is consistent with a substantial literature documenting the safety and neurocognitive benefits of AMPH in AP-mediated SZ patients. Importantly, a therapeutic paradigm in which AMPH (or any other pro-cognitive agent) is used to potentiate the benefits of TCT would involve total drug exposure limited to the mornings prior to TCT training, e.g. 10 mg, three times weekly, for about 10 weeks. Using biomarkers to identify patients most sensitive to such TCT-enhancing drug effects via is an important part of the “PACT” strategy. The present findings suggest that AMPH effects on auditory discrimination learning may be most pronounced among homozygous rs4680 “Met/Met” individuals. A critical next step is to determine whether AMPH-enhanced TCT “learning” (i.e. gains in APS) observed in SZ patients after a single session of TCT predicts clinical benefits after an entire course of 30-50 hours. If so, and it is demonstrated that AMPH can enhance the therapeutic effects of TCT, then this “PACT” approach could represent a transformative treatment paradigm for SZ.
Barch DM, Carter CS. Amphetamine improves cognitive function in medicated individuals with schizophrenia and in healthy volunteers. Schizophr Res 77:43-58, 2005. Fisher M, Holland C, Merzenich MM, Vinogradov S. Using neuroplasticity-based auditory training to improve verbal memory in schizophrenia. Am J Psychiatry 166:805-811, 2009 Fisher M, Holland C, Subramaniam K, Vinogradov S. Neuroplasticity-based cognitive training in schizophrenia: an interim report on the effects 6 months later. Schizophr Bull 36:869-879, 2010. Tarasenko M, Perez VB, Pianka ST, Vinogradov S, Braff DL, Swerdlow NR, Light GA. Measuring the capacity for auditory system plasticity: An examination of performance gains during initial exposure to auditory-targeted cognitive training in schizophrenia. Schiz Res (in press) 2015. Vinogradov S, Fisher M, de Villers-Sidani E. Cognitive training for impaired neural systems in neuropsychiatric illness. Neuropsychopharmacology 37:43-76, 2012
0.25
.5.75
11.25
1.51.75
22.25
Cell
Mea
n
screen stage completed
PTNCS
0.25
.5.75
11.25
1.51.75
22.25
Cell M
ean
screen stage completed
PTNCS0
.25.5
.751
1.251.5
1.752
2.25
Cell
Mea
n
screen stage completed
PTNCSHS SZ
Stag
es C
ompl
eted
*
0
50
100
150
200
250
300
350
400
Cell
Mea
n fo
r sc
reen
tra
inin
g (m
sec)
ave
best
eve
r
ave
base
line
ave
best
PTNCS
0.25
.5.75
11.25
1.51.75
22.25
Cell
Mea
n
screen stage completed
PTNCSHS SZ
Dis
crim
inat
ion
Thre
shol
d (m
s)
Ave. Best3
Ave. Best Ever1
Ave. Baseline2
*
0
.5
1
1.5
2
2.5
3
Cell
Mea
n fo
r sta
ge c
ompl
eted
pbo
v. a
ctiv
e
NCS PT
activepbo
0
.5
1
1.5
2
2.5
3
Cell
Mea
n fo
r sta
ge c
ompl
eted
pbo
v. a
ctiv
e
NCS PT
activepboPBO
AMPH
HS SZ
Stag
es C
ompl
eted
*
-500-400-300-200-100
0100200300400500600
Cell
Mea
n fo
r as
essm
ent
lear
ning
pbo
v. a
ctiv
e
NCS
, AA
NCS
, GG
PT, A
A
PT, G
G
activepbo
0
.5
1
1.5
2
2.5
3
Cell
Mea
n fo
r st
age
com
plet
ed p
bo v
. act
ive
NCS PT
activepboPBO
AMPH
“Lea
rnin
g” (m
s)
HS SZ
rs4680: AA GG AA GG **
-50
0
50
100
150
200
250
Colu
mn
2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250Co
lum
n 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn
2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-50
0
50
100
150
200
250
Colu
mn
3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colum
n 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 2
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
-800
-600
-400
-200
0
200
400
600
800
1000
1200
1400
Colu
mn 3
.98 .985 .99 .995 1 1.005 1.01 1.015 1.02Column 4
Bivariate ScattergramSplit By: Column 1Row exclusion: Untitled Dataset #1
Lear
ning
(ms)
HS SZ
PBO PBO AMPH AMPH
“Lea
rnin
g” (m
s)
-200-150-100
-500
50100150200250300350
Cel
l Mea
n fo
r as
essm
ent
lear
ning
pbo
v. ac
tive
NCS PT
activepbo
0
.5
1
1.5
2
2.5
3
Cel
l Mea
n fo
r st
age
com
plet
ed p
bo v
. ac
tive
NCS PT
activepboPBO
AMPH
HS SZ
“Lea
rnin
g” (m
s) *
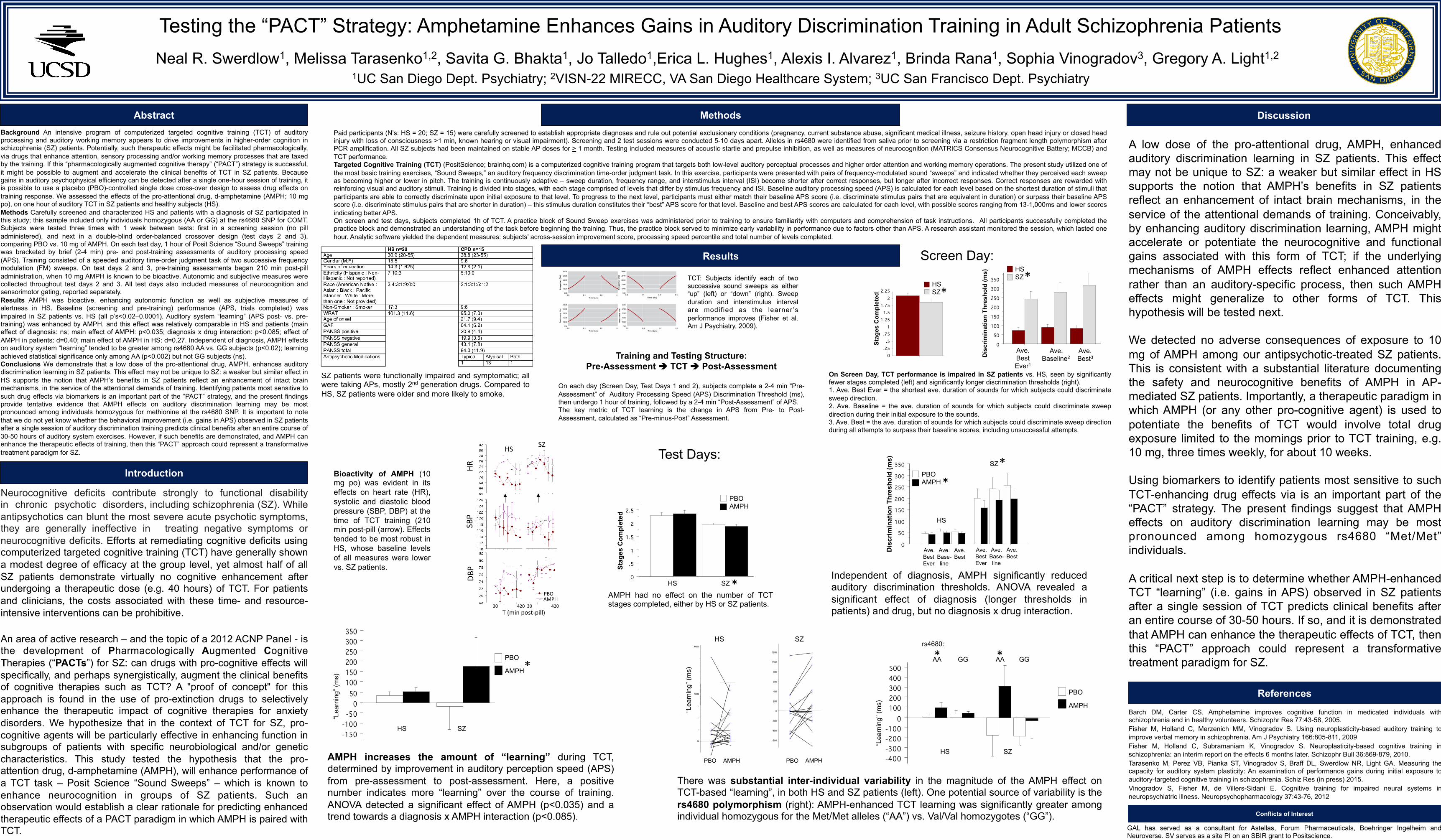
SZ patients were functionally impaired and symptomatic; all were taking APs, mostly 2nd generation drugs. Compared to HS, SZ patients were older and more likely to smoke.
Screen Day:
On Screen Day, TCT performance is impaired in SZ patients vs. HS, seen by significantly fewer stages completed (left) and significantly longer discrimination thresholds (right). 1. Ave. Best Ever = the shortest ave. duration of sounds for which subjects could discriminate sweep direction. 2. Ave. Baseline = the ave. duration of sounds for which subjects could discriminate sweep direction during their initial exposure to the sounds. 3. Ave. Best = the ave. duration of sounds for which subjects could discriminate sweep direction during all attempts to surpass their baseline scores, including unsuccessful attempts.
AMPH had no effect on the number of TCT stages completed, either by HS or SZ patients.
Independent of diagnosis, AMPH significantly reduced auditory discrimination thresholds. ANOVA revealed a significant effect of diagnosis (longer thresholds in patients) and drug, but no diagnosis x drug interaction.
AMPH increases the amount of “learning” during TCT, determined by improvement in auditory perception speed (APS) from pre-assessment to post-assessment. Here, a positive number indicates more “learning” over the course of training. ANOVA detected a significant effect of AMPH (p<0.035) and a trend towards a diagnosis x AMPH interaction (p<0.085).
0
.5
1
1.5
2
2.5
3
Cell
Mea
n fo
r sta
ge c
ompl
eted
pbo
v. a
ctiv
e
NCS PT
activepboPBO
AMPH
HS
SZ
Dis
crim
inat
ion
Thre
shol
d (m
s)
*
Ave. Best
Ave. Best Ever
Ave. Base- line
Ave. Best
Ave. Best Ever
Ave. Base- line
*
0
50100
150200
250300
350
NCS,
ave
best
eve
r
NCS,
ave
base
line
NCS,
ave
best
PT, a
ve b
est e
ver
PT, a
ve b
aseli
ne
PT, a
ve b
est
64666870727476788082
Cell
Mea
n fo
r Hea
rt R
ate
NCS,
pos
t pill
t=30
NCS,
pos
t pill
t=60
NCS,
pos
t MAT
RICS
t=16
5NC
S, p
ost p
ill t=
270
NCS,
pos
t pill
t=32
0NC
S, p
ost p
ill t=
370
NCS,
pos
t pill
t=42
0
PT, p
ost p
ill t=
30PT
, pos
t pill
t=60
PT, p
ost M
ATRI
CS t=
165
PT, p
ost p
ill t=
270
PT, p
ost p
ill t=
320
PT, p
ost p
ill t=
370
PT, p
ost p
ill t=
420
ActivePlacebo
HR
SBP
DBP
T(minpost-pill)3042030420
HS SZ
PBOAMPH
Bioactivity of AMPH (10 mg po) was evident in its effects on heart rate (HR), systolic and diastolic blood pressure (SBP, DBP) at the time of TCT training (210 min post-pill (arrow). Effects tended to be most robust in HS, whose baseline levels of all measures were lower vs. SZ patients.
Training and Testing Structure: Pre-Assessment è TCT è Post-Assessment
On each day (Screen Day, Test Days 1 and 2), subjects complete a 2-4 min “Pre-Assessment” of Auditory Processing Speed (APS) Discrimination Threshold (ms), then undergo 1 hour of training, followed by a 2-4 min “Post-Assessment” of APS. The key metric of TCT learning is the change in APS from Pre- to Post-Assessment, calculated as “Pre-minus-Post” Assessment.
Test Days:
There was substantial inter-individual variability in the magnitude of the AMPH effect on TCT-based “learning”, in both HS and SZ patients (left). One potential source of variability is the rs4680 polymorphism (right): AMPH-enhanced TCT learning was significantly greater among individual homozygous for the Met/Met alleles (“AA”) vs. Val/Val homozygotes (“GG”).
TCT: Subjects identify each of two successive sound sweeps as either “up” (left) or “down” (right). Sweep duration and interstimulus interval are modified as the learner ’s performance improves (Fisher et al. Am J Psychiatry, 2009).