activation of endothelial and coagulation systems in left
TRANSCRIPT

AiRADM
tmdtutsi
doleflrac
eaig
LhtLpesppfros[t
A
AUM
©P
CA
RD
IAC
ctivation of Endothelial and Coagulation Systemsn Left Ventricular Assist Device Recipientsanjit John, MD, Sandhya Panch, MBBS, Jennifer Hrabe, BS, Peng Wei, MPH,nna Solovey, PhD, Lyle Joyce, MD, PhD, and Robert Hebbel, MD
ivision of Cardiothoracic Surgery, Department of Surgery and Division of Hematology, University of Minnesota, Minneapolis,
innesotafemmspacmbb
eapiaebFi
AD
ULT
Background. The paucity of organ donors has necessi-ated redirecting research toward finding alternative
eans to a heart transplant, such as left ventricular assistevices (LVADs) that will serve not merely as bridge-to-
ransplant but also as destination therapy. To betternderstand hemorrhagic and thromboembolic complica-
ions that currently limit the use of such devices, wetudied the endothelial and coagulation system changesn LVAD recipients with time.
Methods. We studied these markers of endothelialysfunction: circulating endothelial cells and expressionf E-selectin, vascular cell adhesion molecule, intercellu-ar adhesion molecule, and tissue factor on circulatingndothelial cells, thrombin generation (prothrombinragments 1,2 and thrombin/antithrombin), and fibrino-ysis (D-dimer). Our study group consisted of 21 LVADecipients (on day 0 and on postoperative days 1, 7, 30, 90,nd 180) and 7 control patients undergoing non-LVADardiac surgery.
Results. Baseline values of intercellular adhesion mol-cule, E-selectin, tissue factor, thrombin/antithrombin,nd D-dimer were significantly higher in LVAD rec-pients than the normal range. Markers of thrombin
eneration (thrombin/antithrombin and prothrombinic
nsewoatc
tsptbsdwt
niversity of Minnesota, 420 Delaware St SE, MMC 207, Minneapolis,N 55455; e-mail: [email protected].
2009 by The Society of Thoracic Surgeonsublished by Elsevier Inc
ragments 1,2) and fibrinolysis (D-dimer) peaked postop-ratively and declined to baseline levels or below by 3onths. But the expression of inducible endothelialarkers (intercellular adhesion molecule, E-selectin, tis-
ue factor) on circulating endothelial cells increasedostoperatively, then decreased but remained elevatedbove preoperative levels for up to 6 months. In ourontrol patients, baseline levels of intercellular adhesionolecule, E-selectin, tissue factor, D-dimer, and throm-
in/antithrombin were lower and decreased significantlyy day 7, as compared with LVAD recipients (p < 0.05).Conclusions. Left ventricular assist device recipients
xperienced significant baseline activation of endothelialnd coagulation systems, further accentuated in the earlyostoperative period. Left ventricular assist device recip-
ents also had prolonged activation of the endothelialnd coagulation systems, suggesting activation of thextrinsic (tissue factor) pathway of thrombosis mediatedy sustained endothelial dysfunction in these patients.urther studies are needed to determine the clinicalnfluence of such changes in LVAD recipients.
(Ann Thorac Surg 2009;88:1171–9)
© 2009 by The Society of Thoracic Surgeonseft ventricular assist device (LVAD) placement is anestablished therapy for patients with end-stage
eart failure both as bridge-to-transplant and destinationherapy [1, 2]. In the last several years, the application ofVADs has markedly increased, with significantly im-roved results. Nonetheless, hemorrhagic and thrombo-mbolic complications still have a major impact on theuccess of LVAD therapy [3, 4]. The intraoperative andostoperative requirements for (often extensive) bloodroduct usage can lead to decreased right ventricular
unction [5]. Further, the use of blood products may beelated to the development of sensitization, which notnly affects survival in heart transplant patients but alsoignificantly increases the waiting time for a transplant6]. Improvements in surgical technique, patient selec-ion, and recipient care have improved outcomes, yet the
ccepted for publication June 25, 2009.
ddress correspondence to Dr John, Division of Cardiothoracic Surgery,
ncidence of hemorrhagic and thromboembolic compli-ations has recently been reported to be as high as 30%.
Moreover, the requirement of anticoagulation for theewer LVAD rotary pumps has added a different dimen-ion to the hemorrhagic and thromboembolic risks inher-nt with LVAD recipients. The need for anticoagulationith the newer devices imposes a bleeding risk through-ut LVAD support and does increase the risk of bleedingt the time of the cardiac transplant. However, discon-inuation of anticoagulation (for a variety of reasons)ould potentially increase the thromboembolic risks.
Previous studies have demonstrated various coagula-ion and hemostatic abnormalities in LVAD recipients,uch as hypercoagulation, fibrinolysis, and increasedlatelet activation [7–11]. Abnormalities in the coagula-
ion, inflammatory, and complement systems have alsoeen clearly recognized in patients undergoing cardiacurgery [12]. However, very little research on endothelialysfunction has been done in LVAD recipients. It isidely established that significant endothelial dysfunc-
ion exists in patients with heart failure. Prolonged or
0003-4975/09/$36.00doi:10.1016/j.athoracsur.2009.06.095

rphtdecdaAem
mlatatcrttwLscwn
M
PWroDURtwLrhbsu
f
pp
TAttptirεALpLttwd
Fbstmp2
Fct
1172 JOHN ET AL Ann Thorac SurgHEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS 2009;88:1171–9
AD
ULT
CA
RD
IAC
epeated exposure to cardiovascular risk factors or theresence of cardiovascular disease can ultimately ex-aust the protective effect of endogenous antiinflamma-
ory systems within endothelial cells. As a result, not onlyoes the endothelium become dysfunctional but alsondothelial cells can lose integrity and detach into theirculation. Circulating markers of such endothelial cellamage include endothelial microparticles (derived fromctivated or apoptotic cells) and whole endothelial cells.
broader appreciation of the numerous functions of thendothelium can be obtained by studying the levels ofolecules of endothelial origin in circulating blood [13].As one of the fundamental homeostatic mechanisms ofammalian biology, the blood coagulation system estab-
ishes a delicate balance between the procoagulant andnticoagulant functions of blood and of the vessel wall,hereby guarding against excesses in either directionnd, normally, preventing unwanted hemorrhage orhrombosis. The vascular endothelium and its variousomponents, such as tissue factor (TF), play an integralole in this homeostasis. We herein report our study ofhe alterations in the endothelial and coagulation sys-ems in LVAD recipients. The objectives of our studyere to (1) identify changes in the endothelial system inVAD recipients, (2) identify changes in their coagulationystem, (3) determine trends in such changes during theourse of LVAD support, and (4) compare such changesith those occurring in control patients who underwenton-LVAD cardiac surgery.
aterial and Methods
atientse performed a prospective study of 21 unselected
ecipients undergoing LVAD placement at the Universityf Minnesota Medical Center, from July 1, 2006, throughecember 30, 2007. The study was approved by theniversity of Minnesota Institutional Review Board foresearch on Human Subjects and conducted according
o the Declaration of Helsinki. All patients providedritten informed consent. Our exclusion criteria for theVAD study recipients were a history of renal failureequiring dialysis, a requirement for ventilatory support,epatic dysfunction resulting in coagulopathy, andiventricular failure requiring biventricular assist deviceupport. We also studied a control group of 7 patientsndergoing non-LVAD cardiac surgery.In the LVAD recipients, we measured all markers as
ig 1. Circulating endothelial cells (CECs) inlood enumerated by immunohistochemicaltaining of buffy-coat smears. Surface pheno-ype was evaluated by immunofluorescenceicroscopy of circulating endothelial cell
reparations. (DAPI � 4’,6-diamidino--phenylindole.)
ollows: on day 0 (preoperative or baseline levels) and on v
ostoperative days 1, 7, 30, 90, and 180; in the controlatients, on day 0, and on postoperative days 1, 7, and 30.
reatmentnesthetic and surgical care was given per our institu-
ional protocols. Monitoring included standard modali-ies (electrocardiogram, temperature, invasive bloodressure, pulse oximetry, and gas monitoring) plus cen-
ral venous pressure or pulmonary artery catheter mon-toring and transesophageal echocardiography. Ap-otinin was used for repeat sternotomy procedures;-aminocaproic acid, for first-time sternotomy procedures.nticoagulation for non-LVAD cardiac surgery andVAD placement consisted of 400 U/kg unfractionatedorcine heparin. Standard techniques were used both forVAD placement and for non-LVAD cardiac surgery. At
he conclusion of cardiopulmonary bypass, anticoagula-ion was reversed with protamine. All 28 study patientsere monitored with continuous telemetry until theirischarge from the hospital.
ig 2. Measured study markers in relation to the coagulation cas-ade. (ICAM � intercellular adhesion molecule; PF 1�2 � pro-hrombin fragments 1,2; TAT � thrombin/antithrombin III; VCAM �
ascular cell adhesion molecule; vWA � von Willebrand antigen.)
LH
IbpTuTaaepdcV
(
ttwsapfit
DPuLlo
Fi
T
V
NASDBB
E
1173Ann Thorac Surg JOHN ET AL2009;88:1171–9 HEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS
AD
ULT
CA
RD
IAC
eft Ventricular Assist DevicesEARTMATE II LEFT VENTRICULAR ASSIST DEVICE. The HeartMate
I (Thoratec Corp, Pleasanton, CA) consists of an internallood pump with a percutaneous lead that connects theump to an external system driver and power source.he pump has an implant volume of 63 mL and generatesp to 10 L/min of flow at a mean pressure of 100 mm Hg.he inflow cannula is connected to the left ventricularpex; the outflow graft is connected to the ascendingorta. The pump has a rotor that is mobilized by anlectromotive force generated by the motor. Pump out-ut depends on the speed of the rotor and on theifference in pressures between the inflow and outflowannulas.ENTRASSIST LEFT VENTRICULAR ASSIST DEVICE. The VentrAssistVentracor, Sydney, Australia) is a third-generation cen-
ig 3. Baseline hematologic data between the two types of left ventric
able 1. Patient Demographics
ariable Total
umber 21ge (y) 55.9 � 13.5ex Males: 81% (17/21)iagnosis Ischemic cardiomyopathy (86aseline EF 0.206 � 0.0883aseline creatinine (mg/dL) 1.46 � 0.57
F � ejection fraction; HM � HeartMate.
zed ratio.)
rifugal pump with hydrodynamic bearings and an elec-romagnetically driven impeller. The pump is treatedith a diamond-like carbon coating on blood-contacting
urfaces to enhance neointimalization. The pump is smallnd measures 67 mm in diameter and 298 grams; it canrovide flows from 2 to 10 L/min with average pressure
rom 50 to 160 mm Hg. Similar to the HeartMate II, thenflow cannula is connected to the left ventricular apex;he outflow graft is connected to the ascending aorta.
evice Managementer our local practice at the University of Minnesota, wesually adjust the fixed-rate speed of the continuous-flowVADs (both HeartMate II and VentrAssist) to maximize
eft ventricular decompression and to improve cardiacutput, simultaneously allowing for at least a 1:3 ratio of
ssist devices. (HM II � HeartMate II; INR � international normal-
HM II VentrAssist p Value
11 1056.2 � 14.9 55.6 � 12.7 0.92
Males: 82% (9/11) Males: 80% (8/10) 0.31100% 70% 0.05
0.227 � 0.109 0.186 � 0.060 0.341.5 � 0.6 1.4 � 0.6 0.62
ular a
%)

amgpss
aptd
BB(doiLat
eeaoiCpMmscazrLfl
Faaaa
ble
2.M
ean
Val
ues
ofTe
sts
for
Cas
esa
stN
orm
alV
alu
esD
ay0
(pre
op)
Day
1(p
osto
p)
Day
7(p
osto
p)
Day
30D
ay90
Day
180
Mix
edM
odel
Tim
eT
ren
ds
sma
Hb
(mg/
dL
)�
157.
5�
1.6
3.7
�0.
93.
0�
0.7
7.6
�0.
912
�4.
67.
9�
0.6
No
chan
gete
lets
(�10
6 /L)
150–
450
223.
7�
26.7
142
�13
b26
7.4
�27
318.
5�
26.1
b26
7.6
�13
.423
1.8
�18
Cu
bic
R0.
8–1.
21.
3�
0.06
1.4
�0.
031.
9�
0.1b
2.0
�0.
16b
2.0
�0.
17b
2.0
�0.
12b
Lin
ear
TT
(s)
25–3
539
.5�
2.5
38.3
5�
1.0
...
42.6
�1.
939
.7�
1.9
39.1
�1.
3Q
uad
rati
cC
s(c
ells
/mL
)2.
6�
1.6
(0–5
)3.
7�
0.91
5.37
�1.
66.
12�
1.46
5.76
�1.
413.
72�
1.99
2.8
�0.
97N
och
ange
AM
-1(%
)13
�3
49.8
9�
3.24
56.5
2�
4.86
73.3
�4.
79b
54.3
�4.
2348
.2�
6.43
53.3
8�
5.53
Cu
bic
elec
tin
(%)
2�
553
.36
�4.
565
.42
�4.
59b
73.7
8�
3.01
b58
.33
�5.
252
.5�
7.1
65.6
2�
5.19
Cu
bic
M(%
)25
�15
55.3
�4.
555
�4.
769
.9�
4.33
62.5
�4.
6663
.68
�4.
9262
.75
�6.
56N
och
ange
(%)
10�
1357
.06
�4.
6870
.52
�4.
0578
.5�
3.66
b54
.75
�4.
9550
.25
�4.
5876
�7.
79C
ubi
cT
(�g/
L)
1–4.
110
.3�
2.04
18.5
�2.
3b11
.2�
1.12
7.32
�1.
065.
55�
0.58
8.1
�2.
25C
ubi
c1�
2(n
mol
/L)
0–0.
220.
3�
0.03
0.48
�0.
06b
0.5
�0.
08b
0.3
�0.
030.
2�
0.02
0.24
�0.
05C
ubi
cA
(%)
55–1
6018
3.09
�8.
9421
6.8
�10
.79b
267.
87�
10.2
9b17
0.7
�10
.316
8.2
�11
.414
6.8
�16
.4C
ubi
cd
imer
(FE
U/m
L)
�0.
52.
1�
0.45
1.77
�0.
245.
94�
0.71
b4.
27�
0.61
b1.
9�
0.22
1.89
�0.
42Q
uad
rati
c
alu
esar
em
ean
�st
and
ard
erro
rof
the
mea
n.
bSi
gnifi
can
tly
diff
eren
tfr
omba
selin
eva
lues
(p�
0.01
).
TT
�ac
tiva
ted
par
tial
thro
mbo
pla
stin
tim
e;C
EC
s�
circ
ula
tin
gen
dot
hel
ialc
ells
;FE
U�
fibr
inog
eneq
uiv
alen
tu
nit
s;H
b�
hem
oglo
bin
;IC
AM
�in
terc
ellu
lar
adhe
sion
mol
ecul
e;IN
R�
rnat
ion
aln
orm
aliz
edra
tio;
PF
1�2
�p
roth
rom
bin
frag
men
ts1,
2;p
osto
p�
pos
top
erat
ive;
pre
op�
pre
oper
ativ
e;T
AT
�th
rom
bin/
antit
hrom
bin
III;
TF�
tissu
efa
ctor
;V
CA
M�
cula
rce
llad
hes
ion
mol
ecu
le;
VW
A�
von
Will
ebra
nd
anti
gen
.
1174 JOHN ET AL Ann Thorac SurgHEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS 2009;88:1171–9
AD
ULT
CA
RD
IAC
ortic valve opening. We optimize the revolutions perinute speed, both hemodynamically and echocardio-
raphically, at the time of LVAD placement, before theatient is discharged from the hospital (ie, after admis-ion for LVAD placement), and if clinical events (eg, newymptoms or suction events) warrant further adjustment.
Anticoagulation involved a combination of warfarinnd aspirin for the continuous-flow groups. After LVADlacement, we did not change defibrillator and biven-
ricular pacing settings. All patients underwent a stan-ard postoperative rehabilitation program.
lood Sampling and Biochemical Assayslood samples were drawn from patients on day 0
baseline or preoperative levels) and on postoperativeays 1, 7, 30, 90, and 180. After discarding the initial bloodbtained from venipuncture, venous blood was collected
n Vacutainer tubes (BD Vacutainer Systems, Franklinakes, NJ) containing EDTA (for endothelial cell analysis)nd sodium citrate (for serum markers). We processedhe blood samples immediately for study.
For endothelial studies, we used immunohistochemicalxamination of buffy-coat smears to enumerate circulatingndothelial cells, and evaluated the surface phenotype bypplying immunofluorescence microscopy to preparationsf circulating endothelial cells. The panel of antibodies used
ncluded a specific anti–endothelial cell antibody (detectingD-148), P1H12, polyclonal blocking antibody to TF (Fig 1;rovided by Dr. Ron Bach, Veterans Affairs Administrationedical Center, Minneapolis, MN), fluorochrome-labeledurine monoclonal antibodies against intercellular adhe-
ion molecule 1 (ICAM-1) or vascular-cell adhesion mole-ule 1 (VCAM-1; South Biotechnology, Birmingham, AL);nd murine monoclonal antibodies against E-selectin (Gen-yme, Cambridge, MA) We used secondary antibodies asequired: goat antimouse immunoglobulin conjugated toissamine rhodamine (Jackson IRL, Westgrove, PA) or
ig 4. Levels of circulating endothelial cells in 21 left ventricularssist device recipients (day 0 and postoperative days 1, 7, 30, 90,nd 180) and in 7 control patients undergoing non–left ventricularssist device cardiac surgery (day 0 and postoperative days 1, 7,nd 30).
uorescein isothiocyanate (Sigma Chemical Co, St. Louis,
Ta TePla
Pla
IN AP
CE
VC
E-s
ICA
TF
TA
PF
VW
D-
aV
AP
inte
vas

Muat
mfDa
alF
l
STs
Ffn
T
T
CVEITTPVD
a
Cfc
1175Ann Thorac Surg JOHN ET AL2009;88:1171–9 HEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS
AD
ULT
CA
RD
IAC
O); rhodamine-conjugated goat anti-rabbit immunoglob-lin (Jackson IRL); and alkaline phosphatase–conjugatedntimouse immunoglobulin (Sigma or Chemicon Interna-ional, Temecula, CA).
The serum markers measured included prothrombin frag-ent 1.2 monoclonal antibody (Behring kit); von Willebrand
actor (BCS VWA LIA ASSAY; using STAGO KIT:LIATEST);-dimers, (Diagnostica Stago STA-R); and thrombin/
ntithrombin III complexes (enzyme-linked immunosorbent
ig 5. Markers of endothelial activation (intercellular adhesion molecactor) in 21 left ventricular assist device recipients (day 0 and postop
able 3. Mean Values for Control Subjectsa
est Normal Values Day 0 (preop)
ECs (cells/mL) 2.6 � 1.6 (0–5) 0.5 � 0.29CAM-1 (%) 13 � 3 48.25 � 1.75-selectin (%) 2 � 5 30 � 10.64
CAM (%) 25 � 15 39.33 � 3.18F (%) 10 � 13 36.67 � 5.24AT (�g/L) 1–4.1 9.88 � 2.32F 1�2 (nmol/L) 0–0.22 0.26 � 0.04WA (%) 55–160 134.67 � 12.6-dimer (FEU/mL) �0.5 0.78 � 0.48
Values are mean � standard error of the mean. b Significantly diffe
ECs � circulating endothelial cells; FEU � fibrinogen equivalent uragments 1,2; postop � postoperative; preop � preoperative; Tell adhesion molecule; VWA � von Willebrand antigen.
on–left ventricular assist device cardiac surgery (day 0 and postoperative
ssay test). These four tests were performed at the clinicalaboratory of the University of Minnesota Medical Center,airview, MN, according to standard methods.The measured study markers in relation to the coagu-
ation cascade have been depicted in Figure 2.
tatistical Analysishe changes in the biomarker levels with time weretudied by using a linear mixed model with random
CAM], vascular cell adhesion molecule [VCAM], E-selectin, tissuee days 1, 7, 30, 90, and 180) and in 7 control patients undergoing
Day 1 (postop) Day 7 (postop) Day 30 (postop)
2.25 � 0.75 3 � 1.73 . . .45.25 � 3.35 51.5 � 4.11 0
45 � 3.32 41.5 � 4.35 4846.33 � 8.67 49.67 � 4.33 33.232.67 � 2.03 63.67 � 5.21 2316.63 � 3b 6.28 � 1.08 3.80.35 � 0.08 0.34 � 0.04 0.24
206.87 � 18.2b 227.67 � 33.96b 1600.57 � 0.11 0.22 � 0.34b 0.4
rom baseline values (p � 0.01).
ICAM � intercellular adhesion molecule; PF 1�2 � prothrombinthrombin/antithrombin III; TF � tissue factor; VCAM � vascular
ule [Ierativ
rent f
nits;AT �
days 1, 7, and 30).
edct(LPIccsczsaws
almwwci0
R
POa5r5poBfp
CAWceresirfs
Fad
1176 JOHN ET AL Ann Thorac SurgHEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS 2009;88:1171–9
AD
ULT
CA
RD
IAC
ffects. The advantage of the mixed model over stan-ard analysis of variance is to take into account theorrelations between repeated measurements withinhe same subject and estimate the effects of covariatescases versus controls, device) using all available data.inear mixed model analysis was carried out by usingROC MIXED procedures of SAS software V8.0 (SAS
nstitute, Inc, Cary, NC). Linear, quadratic, and cubicurves were fitted to the biomarker levels to model thehanges with time. F tests were used to determine thepecific parametric forms (horizontal line indicatingonstant with time, linear line with slope not equal toero, and quadratic or cubic curves) as well as theignificance of covariate effects (cases versus controlnd device difference among cases). Statistical testsith probability values less than 0.05 were considered
ignificant.Paired Student’s t test was used to compare postoper-
tive levels in cases with their baseline (preoperative)evels. Because there were five postoperative measure-
ents (days 1, 7, 30, 90, 180), five paired Student’s t testsere conducted for each marker. Bonferroni procedureas used to adjust for multiple hypothesis testing. Spe-
ifically, a paired Student’s t test was considered signif-cant only if its probability value was less than 0.05/5, or.01.
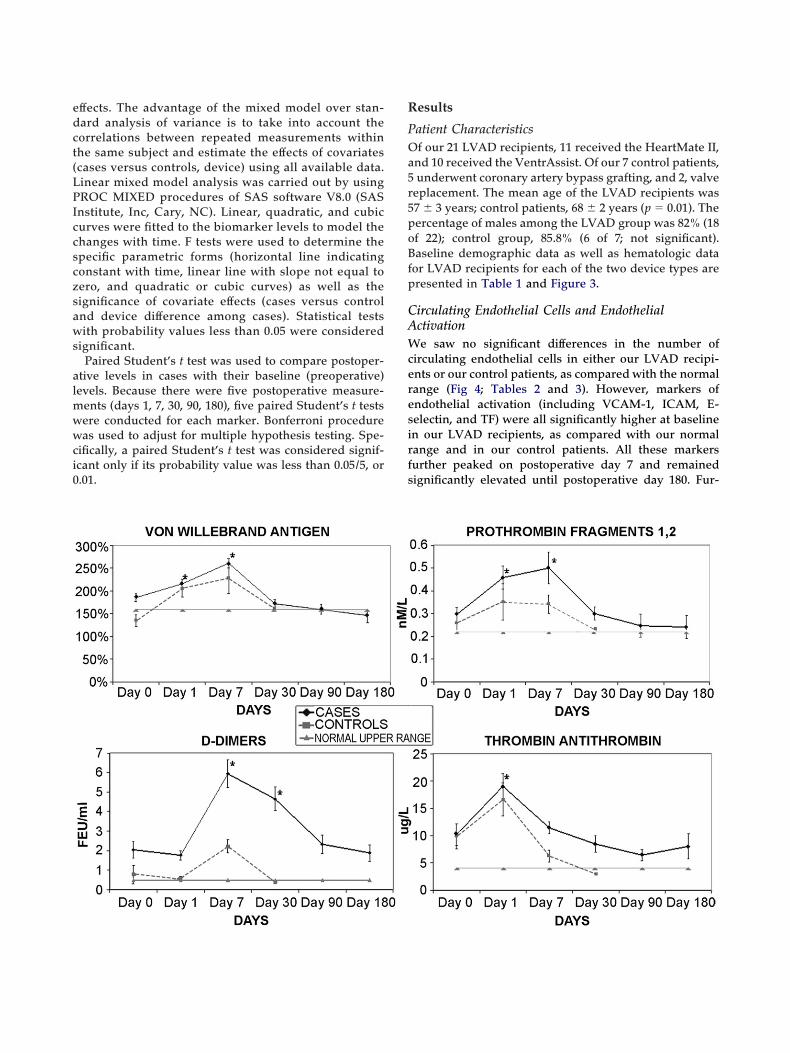
ig 6. Serum markers (von Willebrand antigen, prothrombin fragmenssist device recipients (day 0 and postoperative days 1, 7, 30, 90, an
evice cardiac surgery (day 0 and postoperative days 1, 7, and 30).esults
atient Characteristicsf our 21 LVAD recipients, 11 received the HeartMate II,
nd 10 received the VentrAssist. Of our 7 control patients,underwent coronary artery bypass grafting, and 2, valve
eplacement. The mean age of the LVAD recipients was7 � 3 years; control patients, 68 � 2 years (p � 0.01). Theercentage of males among the LVAD group was 82% (18f 22); control group, 85.8% (6 of 7; not significant).aseline demographic data as well as hematologic data
or LVAD recipients for each of the two device types areresented in Table 1 and Figure 3.
irculating Endothelial Cells and Endothelialctivatione saw no significant differences in the number of
irculating endothelial cells in either our LVAD recipi-nts or our control patients, as compared with the normalange (Fig 4; Tables 2 and 3). However, markers ofndothelial activation (including VCAM-1, ICAM, E-electin, and TF) were all significantly higher at baselinen our LVAD recipients, as compared with our normalange and in our control patients. All these markersurther peaked on postoperative day 7 and remainedignificantly elevated until postoperative day 180. Fur-
, D-dimers, and thrombin/antithrombin III) in 21 left ventricular) and in 7 control patients undergoing non–left ventricular assist
ts 1,2d 180

tabdr0sd
SStairmb1tpdte
C
Tnw[lwscr
smCsmi
dcfitmc(ihmtHpeat
spb[
twIotLsbto
vTitscbatatvetccstwtmasfittt[dtt
sticmcIqifc
1177Ann Thorac Surg JOHN ET AL2009;88:1171–9 HEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS
AD
ULT
CA
RD
IAC
her, there appeared to be a secondary rise in E-selectinnd TF in LVAD recipients (p � 0.05), suggesting aiphasic response (Fig 5; Tables 2 and 3). All endothelialysfunction markers were significantly higher in LVADecipients than in control patients at each time point (p �.05). In our control patients, all markers except E-electin returned to the normal range by postoperativeay 30 (Fig 5).
erum Markerserum markers (including von Willebrand antigen, pro-hrombin fragment 1.2, D-dimers, and thrombin/ntithrombin III) were all significantly higher at baselinen our LVAD recipients, as compared with the normalange and our control patients (p � 0.05). All thesearkers peaked on postoperative day 7 (except throm-
in/antithrombin III, which peaked on postoperative day) and remained significantly elevated until postopera-ive day 90 (Fig 6; Tables 2 and 3). Similarly, in our controlatients, all these markers peaked between postoperativeays 1 and 7; however, unlike in our LVAD recipients, all
hese markers returned to the normal range by postop-rative day 30 (Fig 6).
omment
he discrepancy between the limited availability of do-or organs and the ever-increasing number of patientsith heart failure has led to the increasing use of LVADs
1]. The excellent medium-term results with LVADs haveed to the use of permanent LVAD placement for patientsith end-stage heart failure [2]. Nevertheless, the clinical
uccess of LVADs has been accompanied by significantomplications, including thromboembolic and hemor-hagic events in as many as 30% of recipients.
The development of novel materials used for implanturgery and the increasing use of implanted devices hasade it evident that no material is biologically inert.ommonly used biomaterials, so-called inert compounds
uch as titanium, polytetrafluoroethylene, and acrylics,ay trigger an array of iatrogenic effects, including
nflammation, fibrosis, coagulation, and infection.In the case of LVADs, in which the biomaterial is in
irect contact with the blood circulation, significanthanges in systemic immunologic and thrombostaticunctions have been well documented. Like most othermplanted devices, LVADs activate the coagulation sys-em, resulting in device-related thrombus [7, 14]. The
ajor reasons for this are (1) the contact between bloodomponents and the foreign surfaces of the LVADs and2) the altered rheologic conditions with different veloc-ties of blood flow and blood stasis in the LVAD recipienteart. Spanier and associates [15] described a pheno-enon of a “compensated coagulopathy” underlying
he apparent autoanticoagulation in textured-surfaceeartMate XVE recipients, attributing this finding torocoagulant stimuli elicited from the LVAD cell-surfacenvironment. Some investigators suggested that suchctivation of anticoagulation was attributable largely to
he continuous contact of blood with the foreign LVAD burface; however, others showed that specific cells thatrogressively adhere to the textured LVAD surface andecome activated may also contribute to the coagulopathy
16, 17].Our study demonstrated significant activation of both
he endothelial and the coagulation systems in patientsith end-stage heart failure requiring LVAD placement.
n addition, the findings from our current study extendthers’ previous observations of significant activation ofhe procoagulant as well as fibrinolytic pathways inVAD recipients. We clearly demonstrated that theseerum procoagulant and fibrinolytic markers returned toaseline levels by postoperative days 30 to 90. In contrast
o the coagulation system, we found persistent activationf the endothelial system up to postoperative day 180.Hebbel and colleagues [18] found activation of the
ascular endothelium in patients with sickle cell disease.hey also showed that an increased number of circulat-
ng endothelial cells expressed TF in sickle cell patients;his expression was further increased during vasoocclu-ive episodes. The TF expressed on the antigen-positiveirculating endothelial cell is functional, as demonstratedy a binding assay for factor VIIa and a chromogenicssay sensitive to generation of factor Xa [19, 20]. Beforehis latter study, the role of the vascular endothelium inctivating the coagulation system was uncertain becausehere is little evidence indicating that endothelial cells inivo express TF, the system’s triggering mechanism. Bystablishing that endothelial cells in vivo can express TF,he study demonstrated that the vast endothelial surfacean provide an important pathophysiologic trigger foroagulation activation. Until now, studies of the hemo-tatic alterations associated with LVADs showed elevatedhrombin generation in the early postoperative period,ith increased thrombin activity and fibrinolysis
hroughout the course of LVAD support. Those abnor-alities were attributed to plasma protein adsorption
nd intrinsic pathway activation. Our current studyhowed a late secondary rise in TF, demonstrating for therst time that activation of the extrinsic (TF) pathway of
hrombosis mediated by sustained endothelial dysfunc-ion in LVAD recipients may be equally responsible forhe coagulation abnormalities. Wilhelm and coworkers21] previously suggested a role for complement in me-iating formation of leukocyte-platelet aggregates,
hereby indirectly contributing to thrombin generationhrough monocyte TF expression.
Endothelial cell activation leads to increased expres-ion of inflammatory cytokines and adhesion moleculeshat trigger leukocyte homing, adhesion, and migrationnto the subendothelial space, processes fundamental toardiovascular disease in general. Well-characterizedolecules that can be measured in the circulation with
ommercial microassays include E-selectin, VCAM,CAM, and P-selectin. Similarly, the procoagulant conse-uences of endothelial activation can be measured and
nclude tissue plasminogen activator and von Willebrandactor. Circulating endothelial cells that detach in theontext of endothelial activation and loss of integrity can
e measured in the circulation by flow cytometry. Cur-
ricerbtpusrecpcnosetu
sfHanlmLrttakarfi
owwbeblTbosctwtmicsap
mta
RAS
R
1
1
1
1
1
1
1
1178 JOHN ET AL Ann Thorac SurgHEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS 2009;88:1171–9
AD
ULT
CA
RD
IAC
ent evidence suggests that endothelial function is anntegrative marker of the net effects of damage on theardiovascular system. Importantly, strategies to reversendothelial function have now been examined in a wideange of patients with cardiovascular disease. Benefit haseen shown with a number of pharmacologic interven-
ions, which include drugs that lower lipids and bloodressure, as well as with novel therapies based on newnderstanding of endothelial biology. These have mostlyhown that recovery of endothelial function occurs inesponse to strategies known to reduce cardiovascularvents [22–26]. More recently, it has been shown thatlopidogrel may improve endothelial dysfunction inatients with coronary artery disease independent ofhanges in platelet oxidative stress and platelet-deriveditric oxide availability favoring direct stimulating effectsn the endothelium [27]. Combining different agents,uch as statins and clopidogrel, may have synergisticffects on endothelial cell dysfunction [28]. Whetherhese data can be applied to benefit LVAD recipients isnknown.Our single-center study was limited by its relatively
mall number of patients. Also, we were not able toollow up our control patients for more than 1 month.
owever, it should be noted that other than E-selectin,ll other biomarkers tested in control patients returned toormal levels by 1 month. In addition, we did not have a
arge enough sample size to adjust for the effect ofedications (primarily warfarin). However, all of our
VAD recipients underwent LVAD placement during aelatively short period (1 year), so their perioperativereatment protocols were consistent. And, we consis-ently examined the endothelial and coagulation alter-tions in our LVAD recipients with a variety of biomar-ers at different times during a 6-month period. We werelso able to compare these alterations in our LVADecipients with those of our control patients during therst month.The exact clinical implications for LVAD recipients of
ur findings remain uncertain. Certainly, a larger studyould help validate our findings; a sufficient sample sizeould possibly be able to correlate clinical events such asleeding and thromboembolism with changes in thendothelial and coagulation systems. The significantaseline activation that we found suggests a procoagu-
ant tendency in patients even before LVAD placement.he decline of serum prothrombotic markers to or belowaseline levels with time may reflect a lower requirementf anticoagulation in some LVAD recipients. In conclu-ion, although previous reports have shown that theoagulation abnormalities in LVAD recipients were at-ributed to plasma protein adsorption and intrinsic path-ay activation, this current study showed for the first
ime that activation of the extrinsic (TF) pathway of thro-bosis mediated by sustained endothelial dysfunction
n LVAD recipients may be equally responsible for theoagulation abnormalities. Continued and further under-tanding of these abnormalities is essential to reducedverse events after LVAD placement and thereby im-
rove long-term outcomes. An improved understandingay even allow potential therapeutic interventions in aimely fashion so as to decrease the incidence of bleedingnd thromboembolic complications in high-risk patients.
anjit John received funding for the study from the W. Geraldusten Young Investigator Award, Society of Thoracicurgeons.
eferences
1. Frazier OH, Rose EA, Oz MC, et al. Multicenter clinicalevaluation of the HeartMate vented electric left ventricularassist system in patients awaiting heart transplantation.J Thorac Cardiovasc Surg 2001;122:1186–95.
2. Rose EA, Gelijns AC, Moskowitz AJ, et al. Long-term me-chanical left ventricular assistance for end-stage heart fail-ure. N Engl J Med 2001;345:1435–43.
3. Gross DR. Concerning thromboembolism associated withleft ventricular assist devices. Cardiovasc Res 1999;42:45–7.
4. Goldstein DJ, Oz MC, Rose EA. Implantable left ventricularassist devices. N Engl J Med 1998;339:1522–33.
5. Kavarana MN, Pessin-Minsley MS, Urtecho J, et al. Rightventricular dysfunction and organ failure in left-ventricularassist device recipients: a continuing problem. Ann ThoracSurg 2002;73:745–50.
6. John R, Lietz K, Naka Y, et al. Immunologic sensitization inrecipients of left ventricular assist devices. J Thorac Cardio-vasc Surg 2003;125:578–91.
7. Spanier TB, Oz MC, Levin HR, et al. Activation of coagula-tion and fibrinolytic pathways in patients with left ventric-ular assist devices. J Thorac Cardiovasc Surg 1996;112:1090–7.
8. Hampton CR, Verrier ED. Systemic consequences of ventric-ular assist devices: alterations of coagulation, immune func-tion, inflammation, and the neuroendocrine system. ArtifOrgans 2002;26:902–8.
9. Koster A, Loebe M, Hansen R, et al. Alterations in coagula-tion after implantation of a pulsatile Novacor LVAD and theaxial flow MicroMed DeBakey LVAD. Ann Thorac Surg2000;70:533–7.
0. Livingston ER, Fisher CA, Bibidakis EJ, et al. Increasedactivation of the coagulation and fibrinolytic pathways leadsto hemorrhagic complications during left ventricular assistimplantation. Circulation 1996;94(Suppl2):II-227–34.
1. Himmelreich G, Ullmann H, Riess H, et al. Pathophysiologicrole of contact activation in bleeding followed by thrombo-embolic complications after implantation of a ventricularassist device. ASAIO J 1995;41:M790–4.
2. Edmunds LH Jr. Blood-surface interactions during cardio-pulmonary bypass. J Card Surg 1993;8:404–10.
3. Deanfield JE, Halcox JP, Rabelink TJ. Endothelial functionand dysfunction. Testing and clinical relevance. Circulation2007;115:1285–95.
4. Menconi MJ, Prockwinse S, Owen TA, Dasse KA, Stein GS,Lian GB. Properties of blood contacting surfaces of clinicallyimplanted cardiac assist devices: gene expression, matrixcomposition, and ultra structural characterization of cellularlinings. J Cell Biochem 1995;57:557–73.
5. Spanier TB, Chen JM, Oz MC, Stern DM, Rose EA, SchmidtAM. Time-dependent cellular population of textured-surface left ventricular assist devices contributes to thedevelopment of a biphasic systemic procoagulant response.J Thorac Cardiovasc Surg 1999;118:404–13.
6. Rose EA, Levin HR, Oz MC, et al. Artificial circulatorysupport with textured interior surfaces: a counterintuitiveapproach to minimize thromboembolism. Circulation 1994;
90(5 pt 2):II-87–91.
1
1
1
2
2
2
2
2
2
2
2
2
N
TMetdbw
c(
1179Ann Thorac Surg JOHN ET AL2009;88:1171–9 HEMATOLOGIC COMPLICATIONS IN LVAD PATIENTS
©P
AD
ULT
CA
RD
IAC
7. Graham TR, Dasse K, Coumbe A, et al. Neointimal devel-opment on textured biomaterial surfaces during clinical useof an implantable left ventricular assist device. Eur J Cardio-thoracic Surg 1990;4:182–90.
8. Solovey A, Lin Y, Browne P, Choong S, Wayner E, HebbelRP. Circulating activated endothelial cells in sickle cellanemia. N Engl J Med 1997;337:1584–90.
9. Solovey A, Gui L, Key N, Hebbel RP. Tissue factor expres-sion by endothelial cells in sickle cell anemia. J Clin Invest1998;101:1899–904.
0. Hebbel RP. Adhesive interactions of sickle erythrocytes withendothelium. J Clin Invest 1997;99:2561–4.
1. Wilhelm CR, Ristich J, Kormos RL, Wagner WR. Monocytetissue factor expression and ongoing complement genera-tion in ventricular assist device patients. Ann Thorac Surg1998;65:1071–6.
2. Blann AD, Woywodt A, Bertolini F, et al. Circulating endo-thelial cells. Biomarkers of vascular disease. Thromb Hae-
otice From the American Boa
written) examination.
ei
BC2
2009 by The Society of Thoracic Surgeonsublished by Elsevier Inc
3. Boldt J, Kumle B, Papsdorf M, Hempelmann G. Are circu-lating adhesion molecules specifically changed in cardiacsurgical patients? Ann Thorac Surg 1998;65:608–14.
4. Gearing AJH, Newman W. Circulating adhesion moleculesin disease. Immunol Today 1993;14:506–12.
5. Boos CJ, Lip GYH, Blann AD. Circulating endothelial cells incardiovascular disease. J Am Coll Cardiol 2006;48:1538–47.
6. Hill JM, Zalos G, Halcox JP, et al. Circulating endothelialprogenitor cells, vascular function and cardiovascular risk.N Engl J Med 2003;348:593–600.
7. Warnholtz A, Ostad MA, Velich N, et al. A single loadingdose of clopidogrel causes dose-dependent improvement ofendothelial dysfunction in patients with stable coronaryartery disease: Results of a double-blind, randomized study.Atherosclerosis 2008;196:689–95.
8. Bledsoe SL, Barr JC, Fitzgerald RT, et al. Pravastatin andclopidogrel combined inhibit intimal hyperplasia in a ratcarotid endarterectomy model. Vasc Endovascular Surg
most 2005;93:228–35. 2006;40:49–57.
rd of Thoracic Surgery
he 2009 Part I (written) examination will be held ononday, November 30, 2009. It is planned that the
xamination will be given at multiple sites throughouthe United States using an electronic format. The closingate for registration was August 1, 2009. Those wishing toe considered for examination must apply online atww.abts.org.To be admissible to the Part II (oral) examination, a
andidate must have successfully completed the Part I
A candidate applying for admission to the certifyingxamination must fulfill all the requirements of the Boardn force at the time the application is received.
Please address all communications to the Americanoard of Thoracic Surgery, 6333 N St. Clair St, Suite 2320,hicago, IL 60611; telephone: (312) 202-5900; fax: (312)02-5960; e-mail: [email protected].
Ann Thorac Surg 2009;88:1179 • 0003-4975/09/$36.00