acute care refresher - medednhsl.com
TRANSCRIPT

Acute Care
Refresher
pathways for clinical learning

Key Points
• We are going to cover:
– COVID-19 clinical presentation
– Respiratory assessment
– A-E assessment and NEWS
– Escalation of care and SBAR
– DNACPR / TELP
– ILS
– PPE
– Practical procedures including cannulation and
venepuncture
pathways for clinical learning

Learning Outcomes
• Revise taking a focused history of the respiratory
system in an acute setting
• Review performing a respiratory examination in an
acute setting
• Identify the investigations to carry out in a patient
suspected of having COVID-19
• Refresh A-E assessment of an unwell patient
• Consider appropriateness of escalation and
HACP/DNACPR
pathways for clinical learning

COVID-19Consider COVID-19 for current inpatients or patients who require admission who fit the
following criteria:
• requiring admission to hospital
and
• have either clinical or radiological evidence of pneumonia
or
• acute respiratory distress syndrome (ARDS)
or
• influenza like illness (fever ≥37.8°C and at least one of the following
respiratory symptoms, which must be of acute onset: persistent cough (with
or without sputum), hoarseness, nasal discharge or congestion, shortness
of breath, sore throat, wheezing, sneezing)
pathways for clinical learning

PPEFor all patients meeting the case definition the following minimum
PPE should be worn:
• Surgical mask (fluid resistant) with eye protection (visor or safety
glasses)
• Apron
• Disposable gloves
Patient should also be wearing a disposable mask during
assessment
For aerosol generating procedures (eg NIV, intubation/extubation,
suction, CPR) require full PPE (see later slides)
pathways for clinical learning

Respiratory History
• Dyspnoea
– Exertional vs resting
– Severity
• Cough
– Dry / productive
• Wheeze
• Haemoptysis
• Chest pain
– Site / Radiation / Character
pathways for clinical learning
• Systemic symptoms
– Fever (>37.8oC)
– Myalgia
– Rhinorrhoea
– Sore Throat

Respiratory History
• Dyspnoea
– Exertional vs resting
– Severity
• Cough
– Dry / productive
• Wheeze
• Haemoptysis
• Chest pain
– Site / Radiation / Character
pathways for clinical learning
• Systemic symptoms
– Fever (>37.8oC)
– Myalgia
– Rhinorrhoea
– Sore Throat

Further questions
• History of respiratory co-
morbidities
• General medical history
– Is the patient
immunocompromised?
• Onset
• Duration
• Severity
• Course
– Improving? Deteriorating?
• Aggravating/Relieving
factors
• Associated features
• Drug history & allergies
– Immunosuppressive
agents
pathways for clinical learning
REMEMBER: IMMUNOCOMPROMISED PATIENTS MAY NOT PRESENT WITH
TYPICAL HISTORY OR SYMPTOMS

Physical examination General inspection
• Foot of the bed inspection
– Respiratory rate
– Oxygen requirement
– Tripod position
– Use of accessory muscles
• Can the patient speak in full sentences?
• Evidence of central/peripheral cyanosis
pathways for clinical learning

Physical ExaminationChest Examination
• General Inspection
– Work of breathing / signs of respiratory distress
– Symmetry of chest wall movement
– Tracheal deviation
– Scars / evidence of previous thoracic surgery
– Assess for asterixis / flapping tremor (Evidence
of CO2 retention)
pathways for clinical learning

Physical ExaminationChest Examination
• Chest expansion– Front and back
– Asymmetrical or reduced- signs of pathology on that side
pathways for clinical learning
Physical ExaminationChest Examination
• Percussion– Supra and infraclavicular, throughout chest, axillae
– Resonant- normal
– Dull- consolidation/fluid/tumour/collapse
– Stony dullness- effusion
– Hyper-resonant- pneumothorax
pathways for clinical learning
Physical ExaminationChest Examination
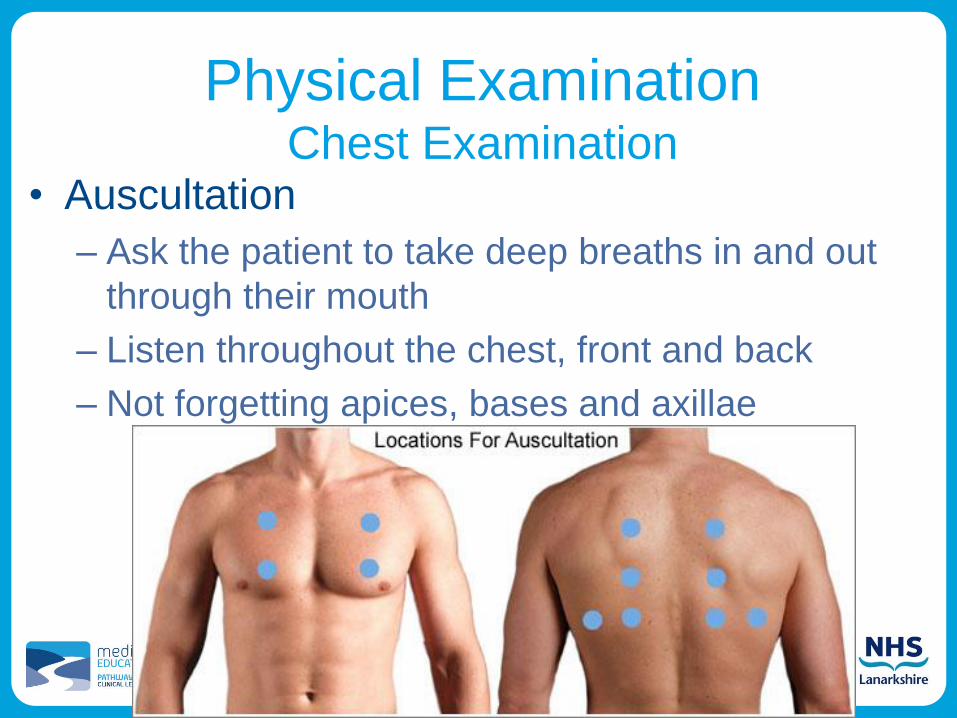
• Auscultation
– Ask the patient to take deep breaths in and out
through their mouth
– Listen throughout the chest, front and back
– Not forgetting apices, bases and axillae
pathways for clinical learning
Physical ExaminationChest Examination
• Auscultation
– Coarse crackles/crepitations
• Infection, cardiac overload (if bilateral)
– Reduced air entry
• Consolidation/lobar collapse/pleural effusion
– Wheeze
• Asthma/COPD
• Stethoscope should remain with the patient or
be cleaned appropriately after use
pathways for clinical learning

Investigations
• Observations/NEWS
• Bloods
– FBC, U&E, CRP, LFT,
lactate
– Other bloods guided
by clinical assessment
• Blood cultures
– Performed as per usual
indications
• Chest X-ray- portable if
suspected COVID
• ABG- see local protocol
• COVID:
– WCC often normal
– Lymphopenia common
– CRP ↑
– Nasal & throat swab for
PCR
pathways for clinical learning

pathways for clinical learning
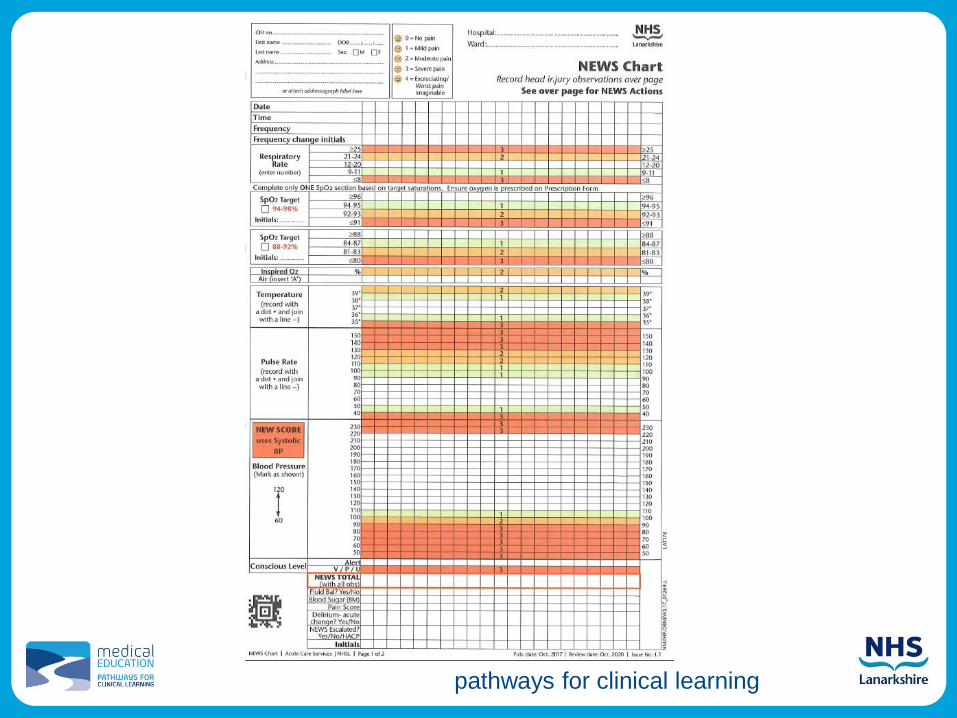
NEWS
• ‘National Early Warning Score’
– Standardised tool to recognise deteriorating
patients
– Scoring system based upon physiological
measurements:
• Higher number indicates a sicker patient
• Trends help indicate whether patients improving
or deteriorating
• Score corresponds to appropriate escalation plan

NEWS
How it works:
– Based on an aggregate scoring system in
which a score is allocated to physiological
measurements– respiration rate
– oxygen saturation
– systolic blood pressure
– pulse rate
– level of consciousness or new confusion
– temperature
– inspired oxygen
pathways for clinical learning

pathways for clinical learning
pathways for clinical learning

pathways for clinical learning
NEWS Escalation

A-E Assessment
• This is a very quick assessment (5-10
minutes) of an unwell patient.
• Address problems as you find them and
reassess regularly and after interventions
pathways for clinical learning

Airway
• Assessment:
– Is the patient talking / obtunded / evidence of airway
obstruction (snoring, gurgling, stridor)
• When to seek help:
– If concerns with airway, seek help immediately (anaesthetics/
arrest team)
• Interventions:
– Whilst awaiting perform basic airway manoeuvres
• Head tilt, chin lift
• Jaw thrust
• Use of airway adjuncts (Oropharyngeal airway, nasopharyngeal
airway)
pathways for clinical learning

Breathing• Assessment:
– Respiratory rate
– Oxygen saturations
– Percussion & Auscultation
• Interventions:
– Supplemental oxygen to achieve oxygen saturations (94-98%)
• If risk of type 2 respiratory failure (i.e. COPD), consider aiming for SpO2
of 88-92%
– Consider nebulised salbutamol to treat wheeze
• When to seek help:
– If unable to achieve target saturations despite high flow
oxygen (6-8L via any oxygen delivery) escalate to senior
decision maker
pathways for clinical learning
Circulation• Assessment:
– Heart rate
– Blood pressure
– Warmth of extremities and presence of peripheral pulses
– Consider ECG / telemetry
• Interventions:
– Establish IV access (large bore cannula, consider 2)
– Take appropriate bloods
– If evidence of shock, consider a bolus of IV fluids (i.e. 500ml
Plasmolyte)
• When to seek help:
– If no/inadequate/transient response to fluid resuscitation,
escalate care to senior decision maker
pathways for clinical learning

Disability
• Assessment:
– AVPU/GCS
– Pupillary response
– Blood glucose
• Interventions:
– Treat hypoglycaemia if present
– Consider causes of impaired consciousness and treat
appropriately
• When to seek help:
– Concerns about consciousness level always warrant senior
input. Re-assess and maintain the airway.
pathways for clinical learning
Exposure
• Assessment:
– Temperature
– Top to toe examination including abdomen
– Look for evidence of:
• Rashes
• Injury
• Bleeding
• Interventions:
– Respond and treat based upon clinical findings
• When to seek help:
– Escalate care if any findings that cause concern.
pathways for clinical learning
Reassessment
• Reassess patient following each
intervention.
• Escalate patient care at any time that
you have concerns
• Use ‘SBAR’ handover format when
discussing or escalating a patient
pathways for clinical learning
SBARSituation
• Introduce self, check you are speaking to the right person
• Who and where (Identify patient and where you are calling from)
• What the current problem appears to be and why your calling them
Background
• Background information about patient
• Reason/date of admission
• Relevant past medical/surgical/social history
Assessment
• Include specific observations and ABCDE assessment findings
Recommendation
• State specifically what you want the person your calling to do
• What and when? (e.g. I’m going to start the following treatment, would you suggest anything else? I think the patient needs reviewed urgently)
pathways for clinical learning

Treatment Excalation/
Limitation Plan(TELP)
pathways for clinical learning
• Should be put in place at admission
(ED or ECU)
• Should be done for EVERY patient
admitted, regardless of
age/functionality/fitness
• Should be discussed with patient,
(and family if appropriate) but
ultimately, it is a MEDICAL decision

pathways for clinical learning

DNACPR
• “The decision to use any treatment
should be based on the balance of
burdens, risks and benefits to the
individual receiving the treatment,
and that principle applies as much
to CPR as to any other treatment.”
• Treatment is justified only if there
is expected benefit to the patient,
i.e. we must justify attempting
CPR, as opposed to justifying not
attempting it.
pathways for clinical learning

Immediate Life Support
Refresher Training
COVID-19
Version: Jan
2016

This session should enable you to:
• Safely deliver standardised CPR in adults
with or without suspected/confirmed
COVID-19
• Deliver safe defibrillation (AED only)
Learning outcomes

Chain of survival
Chain of
Survival

Life Support Algorithm

To confirm cardiac
arrest in non-COVID-19
patients…• Patient response?
• Call for help early
• Open airway
• Check for signs of life
• Feel carotid pulse (if trained)
• Check for normal breathing
10 seconds
• caution agonal breathing
Unresponsive and not
breathing normally

Emergency red buzzer

Head tilt chin lift

Check pulse ONLY if trained to
check for carotid pulse.
Look, listen and feel for breath
sounds for 10 seconds
Look, listen and feel
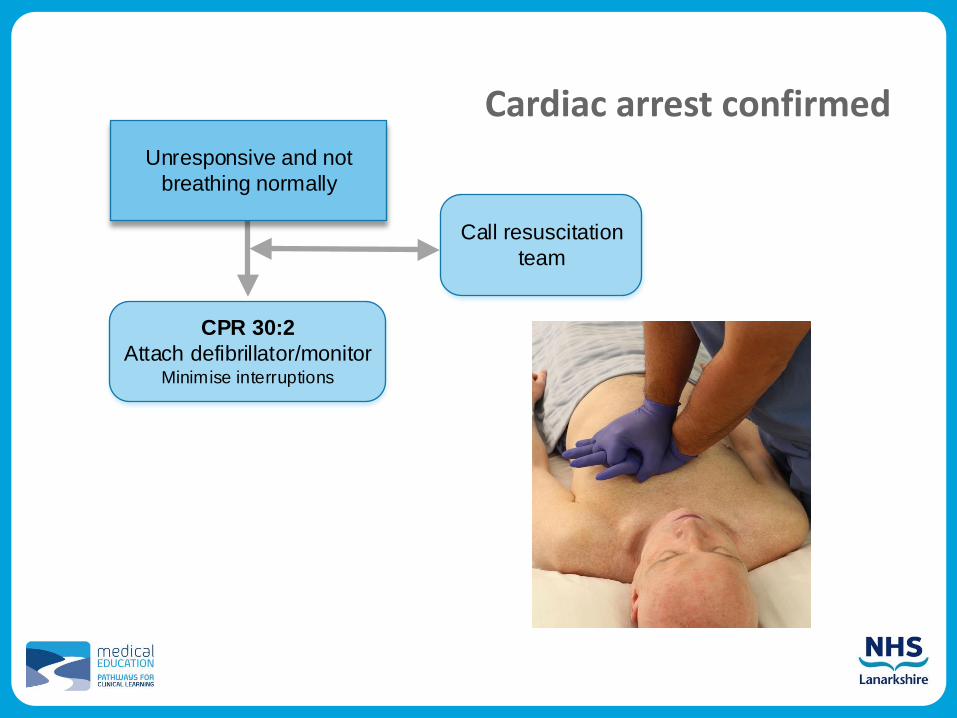
Cardiac arrest confirmedUnresponsive and not
breathing normally
Call resuscitation
team
CPR 30:2
Attach defibrillator/monitorMinimise interruptions

Chest compression• 30:2
• compressions
• centre of chest
• 5-6 cm depth
• 2 per second (100-120 min-1)
• maintain high quality
compressions with minimal
interruptions (<5 s)
• continuous compressions
once airway secured
• switch CPR provider every 2
min cycle to avoid fatigue

Bag valve mask technique

Pad positioning

AP pad position

Automated External
Defibrillation• Use an AED
• Start CPR whilst awaiting AED to arrive
• Switch on and follow AED prompts

Local AED

START PAUSE
CPR
MINIMISE INTERRUPTIONS IN CHEST COMPRESSIONS
Assess rhythm
Shockable
(VF/Pulseless VT)
Non-shockable
(PEA/Asystole)

Reversible causes of cardiac
arrest

Vascular access
• Peripheral versus central
veins
• Intraosseous

Assess rhythm
Return of spontaneous
circulation
Immediate post cardiac
arrest treatment Use ABCDE approach
Aim for SpO2 of 94-98%
Aim for normal PaCO2
12-lead ECG
Treat precipitating cause
Targeted temperature
management

Resuscitation team
• Roles planned in advance
• Identify team leader
• Importance of
non-technical skills
• task management
• team working
• situational awareness
• decision making
• Structured communication
• SBAR or RSVP

Non-COVID-19 Summary
• ILS providers should use those skills in which
they are proficient
• If using an AED – switch on and follow the
prompts
• Ensure high quality chest compressions
• Ensure early defibrillation
• Treat any reversible causes
• Ensure expert help is coming

COVID-19(Suspected and confirmed)
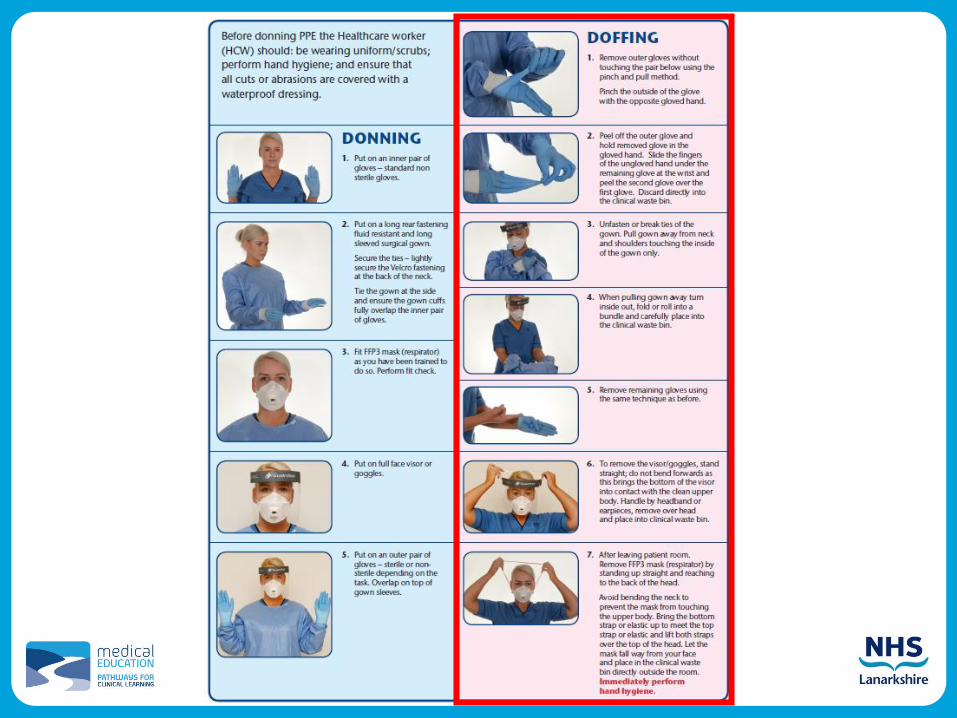
Personal Protective Equipment
Full PPE required to start CPR:
• FFP3 respirator
• Gloves for tight-fitting cuffs
• A single-use, disposable, fluid resistant, full-
sleeve gown
• Eye protection (a full face visor or single use
goggles)
AND patient should be wearing a surgical mask.

Minimum PPE Requirements
For anything NOT involving aerosol:
• Fluid resistant (surgical) facemask
• Eye protection
• Plastic apron
• Gloves
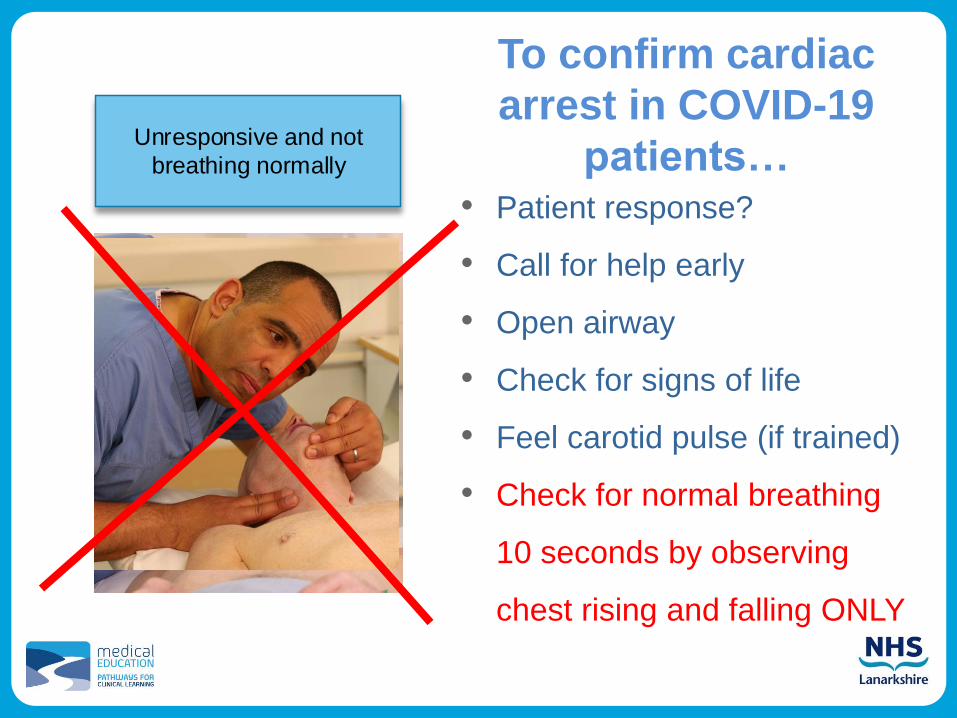
To confirm cardiac
arrest in COVID-19
patients…• Patient response?
• Call for help early
• Open airway
• Check for signs of life
• Feel carotid pulse (if trained)
• Check for normal breathing
10 seconds by observing
chest rising and falling ONLY
Unresponsive and not
breathing normally
Check pulse ONLY if trained to
check for carotid pulse.
Look, listen and feel for breath
sounds for 10 seconds
Look, listen and feel

EVERYTHING ELSE REMAINS THE
SAME

Summary
• ILS providers should use those skills in
which they are proficient
• If COVID-19 suspected/positive: don
PPE before any intervention and do not
listen and feel for breaths

Summary
• If using an AED – switch on and follow
the prompts
• Ensure high quality chest compressions
• Ensure early defibrillation
• Treat any reversible causes
• Ensure expert help is coming

Work within your skillset and escalate
as appropriate.
pathways for clinical learning

Useful links and apps
• GGC Medicines App
– login: ggcstaff
– password: medicines
• BNF App
• Quick Medicine App (GP Notebook content)
• BMJ Best Practice App
– Athens login
• MD Calc
• Antimicrobial Companion (NHSL Antibiotic Guidelines)
• Geeky medics clinical examination app
• NHS Scotland NEWS App
pathways for clinical learning

Online Learning• LearnPro modules
– SIPSEC (infection control)
– Certification of Death
– Antibiotic Prescribing Today's Practitioners
– Intro to Delirium
– AWI
• Resuscitation Council
• ECG revision: LITFL (Life in The Fast Lane) for ECGs
• X-ray interpretation: Radiology Masterclass
• General Revision: GeekyMedics
pathways for clinical learning
Any questions?