acute gynecological findings on ct: expect the unexpected
TRANSCRIPT
Acute Gynecological Findings on CT: Expect
the Unexpected
Neeta Kannan MD1, Liina Poder MD1, Kimberly Maurer1, Michael Ohliger MD PhD1, Jessica
Hayward MD1, and Tara Morgan MD1.
1 University of California San Francisco Department of Radiology and Biomedical Imaging
No Financial Disclosures
Learning Objectives: 1. Review CT cases where the acute pathology was not initially suspected to be
gynecologic.
2. Review imaging features of gynecologic pathology on CT.
3. Illustrate when additional imaging such as with pelvic ultrasound and/or MRI is required to diagnose pathology.
4. Emphasize the importance of careful evaluation of pelvic structures for acute findings on every CT.
Categories of Pathology: Ovarian/Adnexal
Cysts, masses, and/or torsion
Fallopian Tube Salipingitis/Tubo-ovarian abscess
Uterine
Fibroid pathology Perforation/Foreign Device

Hemorrhagic Ovarian Cyst: CT Scan
18 year old with sharp abdominal pain for 3 days.
• Enlarged hypoattenuating cystic structure with mild rim enhancement in the right adnexa
• No free pelvic fluid • HU not reliable to differentiate simple vs hemorrhagic cyst,
however if well circumscribed, <5cm, and premenopausal, ultrasound may not be needed
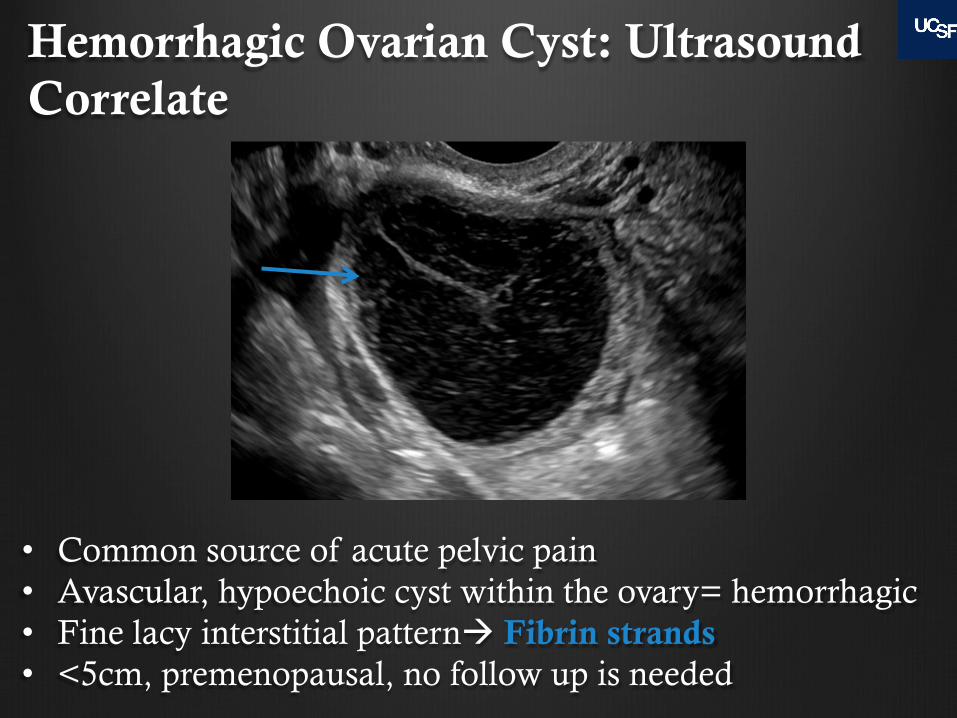
Hemorrhagic Ovarian Cyst: Ultrasound Correlate
• Common source of acute pelvic pain • Avascular, hypoechoic cyst within the ovary= hemorrhagic • Fine lacy interstitial patternà Fibrin strands • <5cm, premenopausal, no follow up is needed
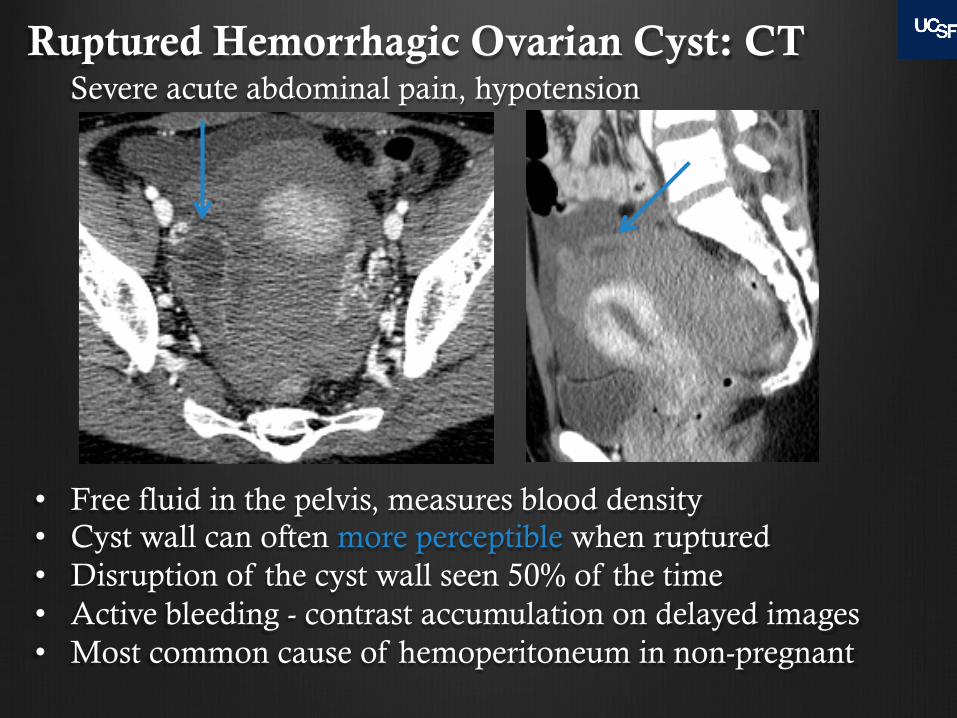
Ruptured Hemorrhagic Ovarian Cyst: CT
• Free fluid in the pelvis, measures blood density • Cyst wall can often more perceptible when ruptured • Disruption of the cyst wall seen 50% of the time • Active bleeding - contrast accumulation on delayed images • Most common cause of hemoperitoneum in non-pregnant
Severe acute abdominal pain, hypotension
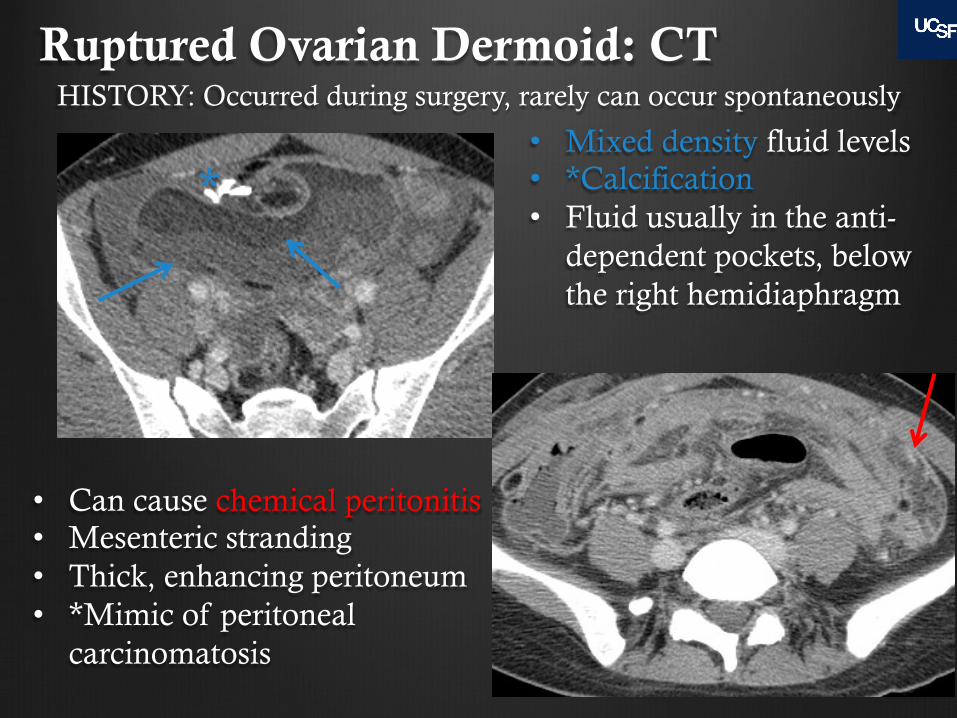
Ruptured Ovarian Dermoid: CT
• Can cause chemical peritonitis • Mesenteric stranding • Thick, enhancing peritoneum • *Mimic of peritoneal
carcinomatosis
• Mixed density fluid levels • *Calcification • Fluid usually in the anti-
dependent pockets, below the right hemidiaphragm
HISTORY: Occurred during surgery, rarely can occur spontaneously
*
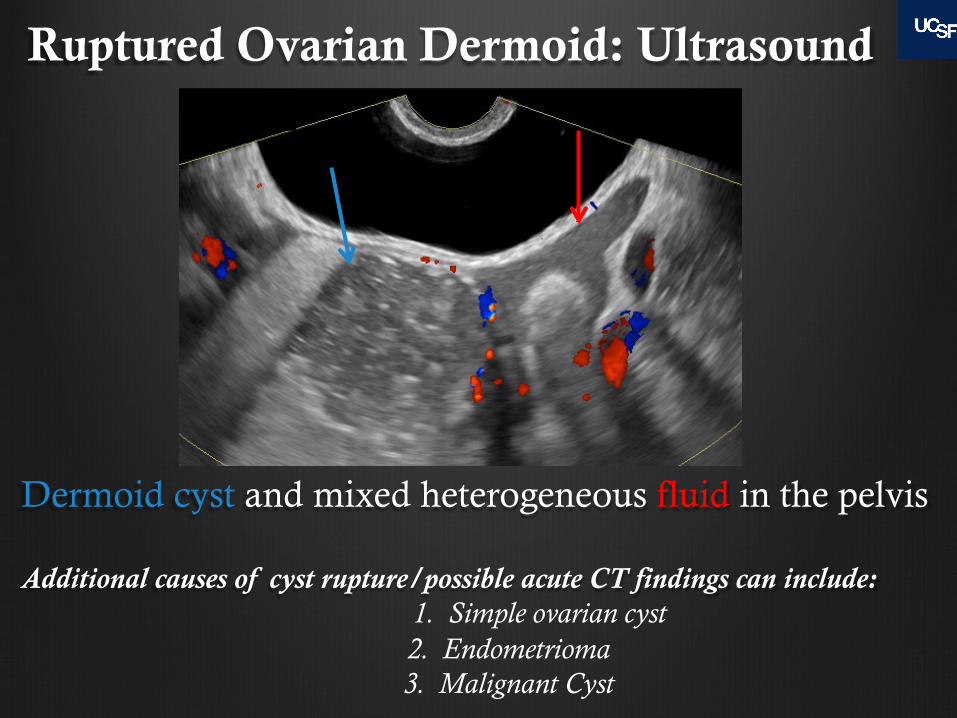
Ruptured Ovarian Dermoid: Ultrasound
Dermoid cyst and mixed heterogeneous fluid in the pelvis Additional causes of cyst rupture/possible acute CT findings can include:
1. Simple ovarian cyst 2. Endometrioma 3. Malignant Cyst
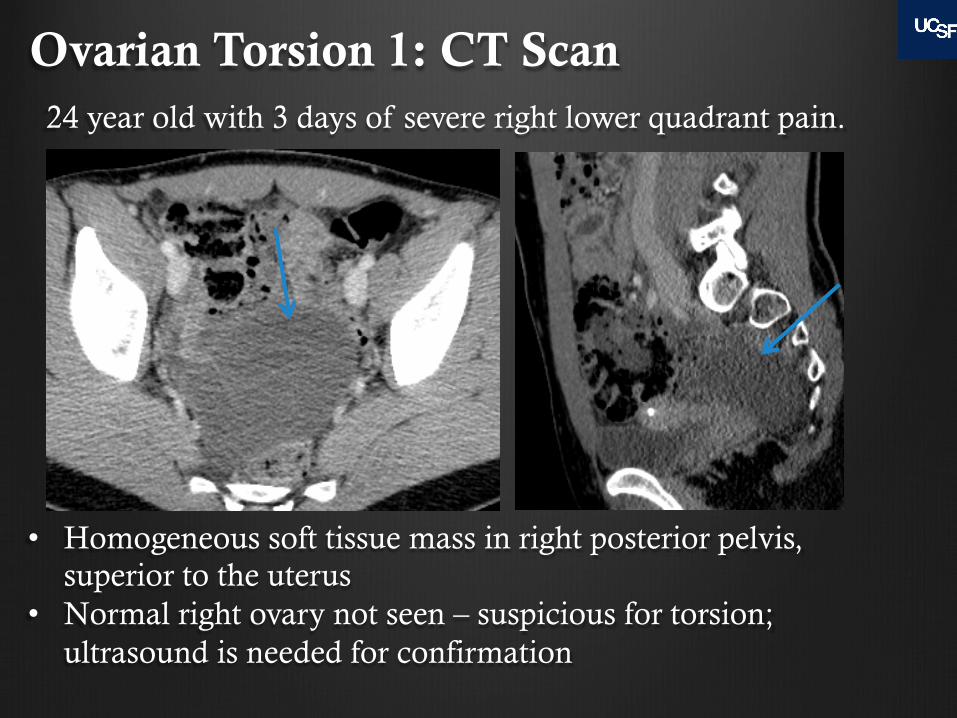
Ovarian Torsion 1: CT Scan
• Homogeneous soft tissue mass in right posterior pelvis, superior to the uterus
• Normal right ovary not seen – suspicious for torsion; ultrasound is needed for confirmation
24 year old with 3 days of severe right lower quadrant pain.
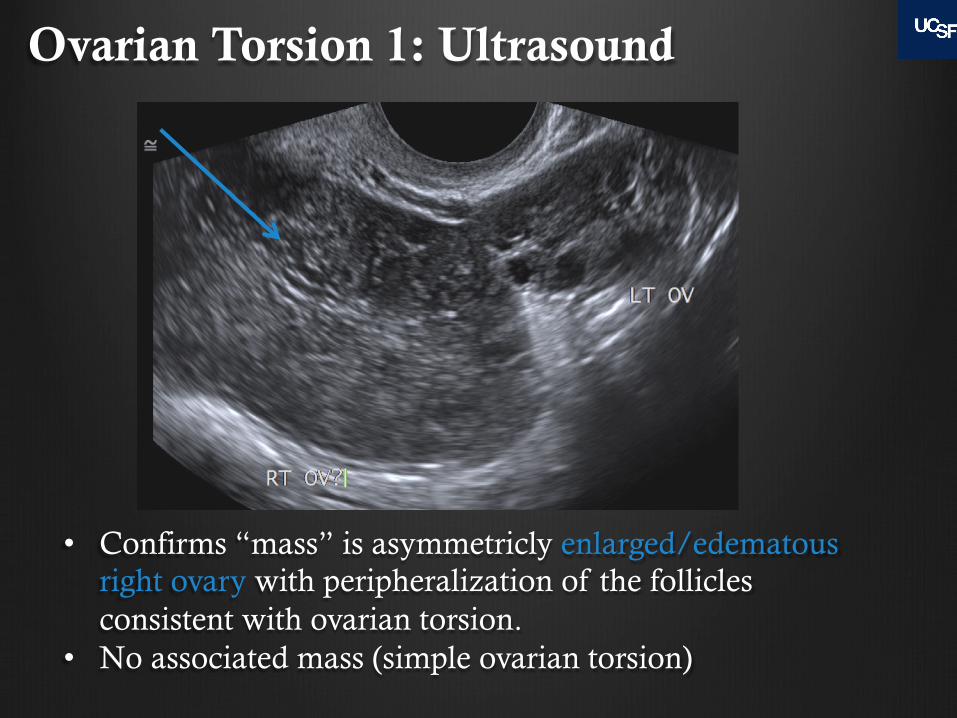
Ovarian Torsion 1: Ultrasound
• Confirms “mass” is asymmetricly enlarged/edematous right ovary with peripheralization of the follicles consistent with ovarian torsion.
• No associated mass (simple ovarian torsion)
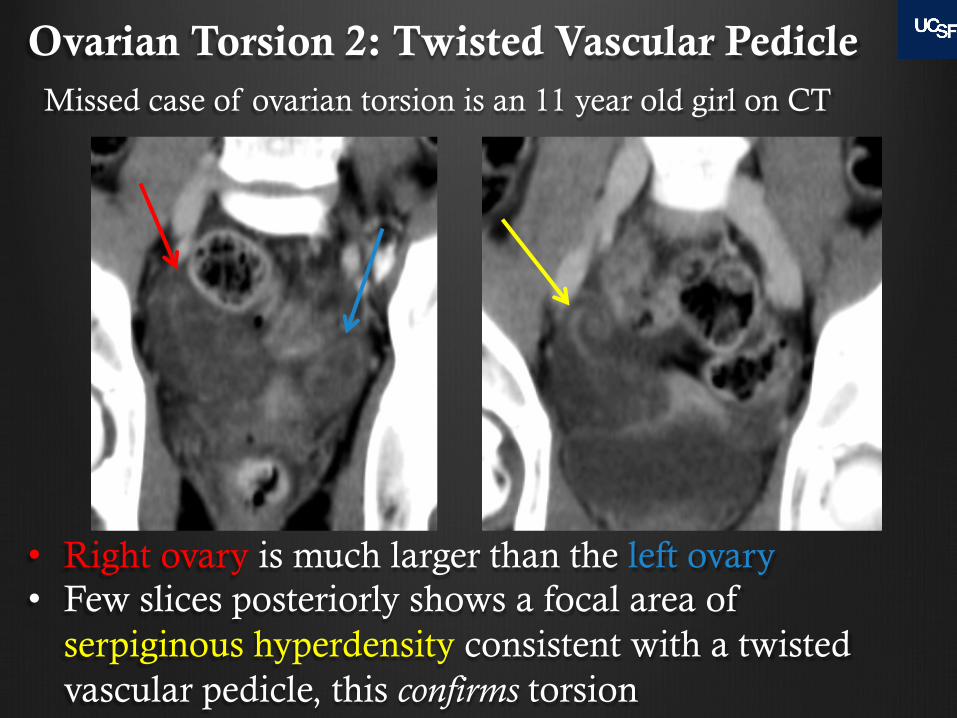
Ovarian Torsion 2: Twisted Vascular Pedicle
• Right ovary is much larger than the left ovary • Few slices posteriorly shows a focal area of
serpiginous hyperdensity consistent with a twisted vascular pedicle, this confirms torsion
Missed case of ovarian torsion is an 11 year old girl on CT

Ovarian Torsion 3: Right Dermoid, Left Ovarian Torsion, CT
• Fat-fluid level compatible with a right ovarian dermoid • BEWARE: satisfaction of search!! • Left ovary is too large, and correlates with pain, highly
concerning for ovarian torsion– ultrasound to confirm
31 year old woman with 1 day left sided abdominal pain

Ovarian Torsion 3: Dermoid and Contralateral Torsion on Ultrasound Left Ovary
• Asymmetrically enlarged left ovary with dermoid, peripheralization of the follicles confirms torsion
• Right ovarian dermoid cyst • Correlate findings with history and search thoroughly!
Right Ovary
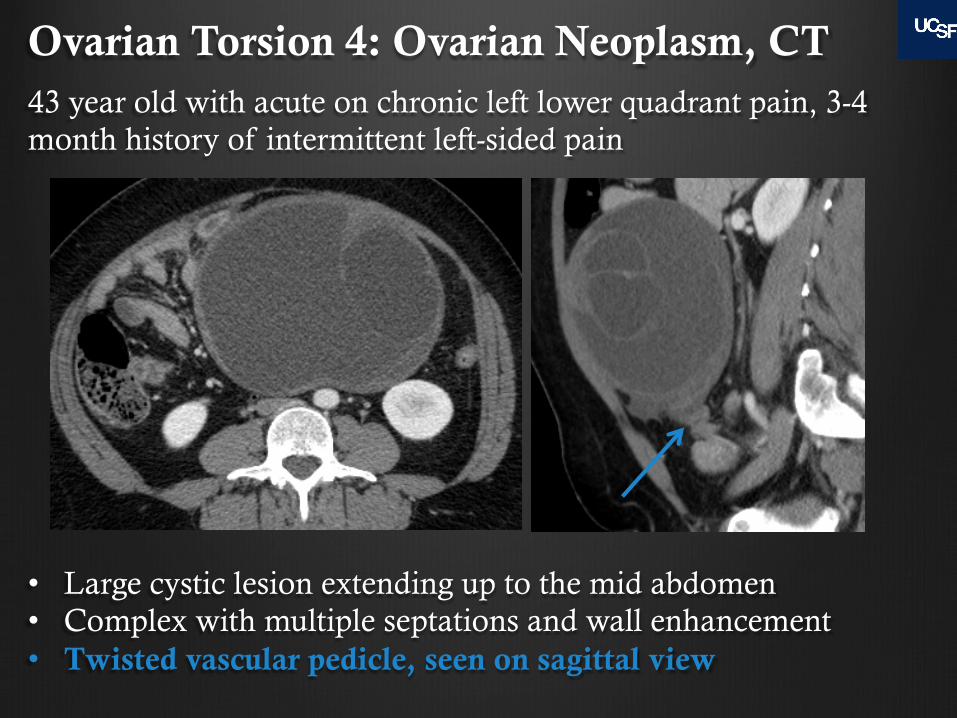
Ovarian Torsion 4: Ovarian Neoplasm, CT 43 year old with acute on chronic left lower quadrant pain, 3-4 month history of intermittent left-sided pain
• Large cystic lesion extending up to the mid abdomen • Complex with multiple septations and wall enhancement • Twisted vascular pedicle, seen on sagittal view
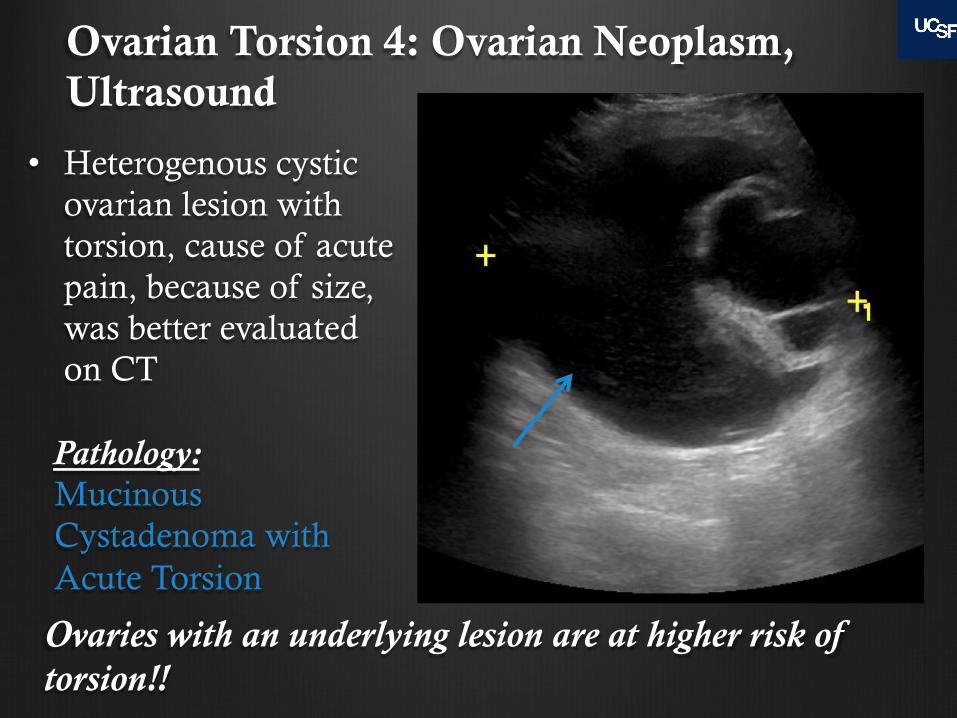
Ovarian Torsion 4: Ovarian Neoplasm, Ultrasound
• Heterogenous cystic ovarian lesion with torsion, cause of acute pain, because of size, was better evaluated on CT
Pathology: Mucinous Cystadenoma with Acute Torsion
Ovaries with an underlying lesion are at higher risk of torsion!!

Ovarian Torsion 5: CT 69 year old with few weeks of left pelvic pain, concern for diverticulitis
• Torsion can present at any age! • Large left adnexal lesion with hetereogenous enhancement • Twisted vascular pedicle • Left ovarian torsion with large ovarian mass • MRI was performed
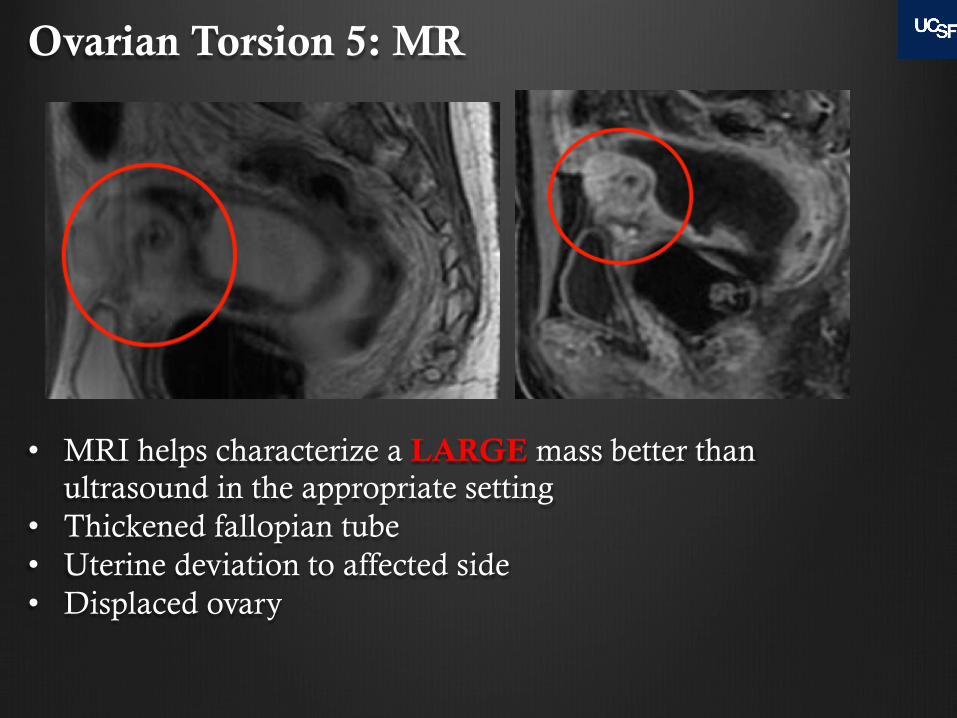
Ovarian Torsion 5: MR
• MRI helps characterize a LARGE mass better than ultrasound in the appropriate setting
• Thickened fallopian tube • Uterine deviation to affected side • Displaced ovary
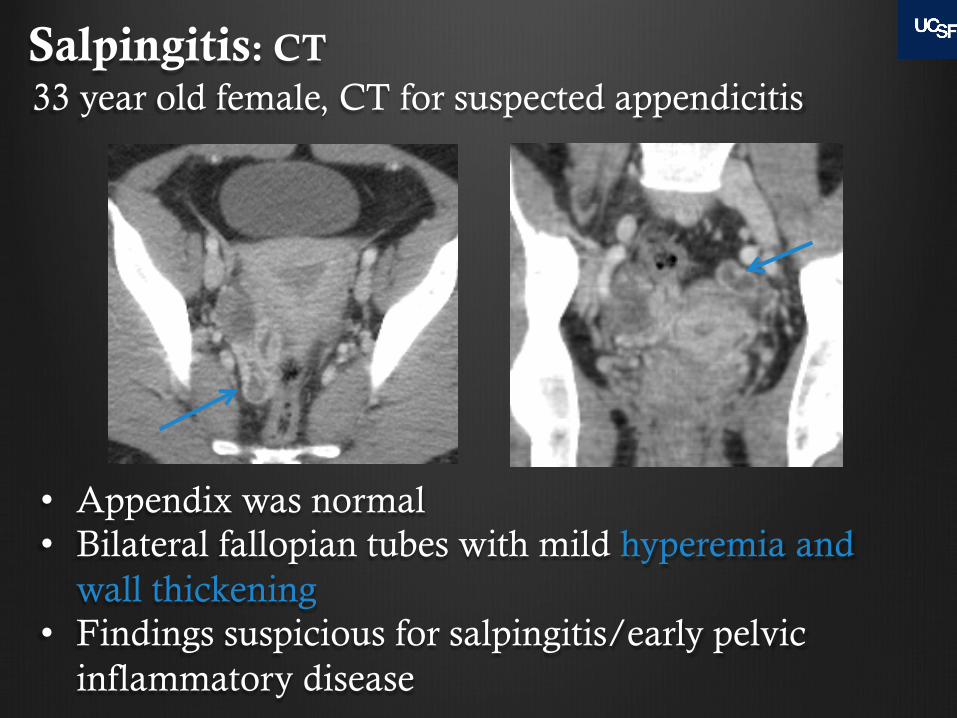
Salpingitis: CT 33 year old female, CT for suspected appendicitis
• Appendix was normal • Bilateral fallopian tubes with mild hyperemia and
wall thickening • Findings suspicious for salpingitis/early pelvic
inflammatory disease
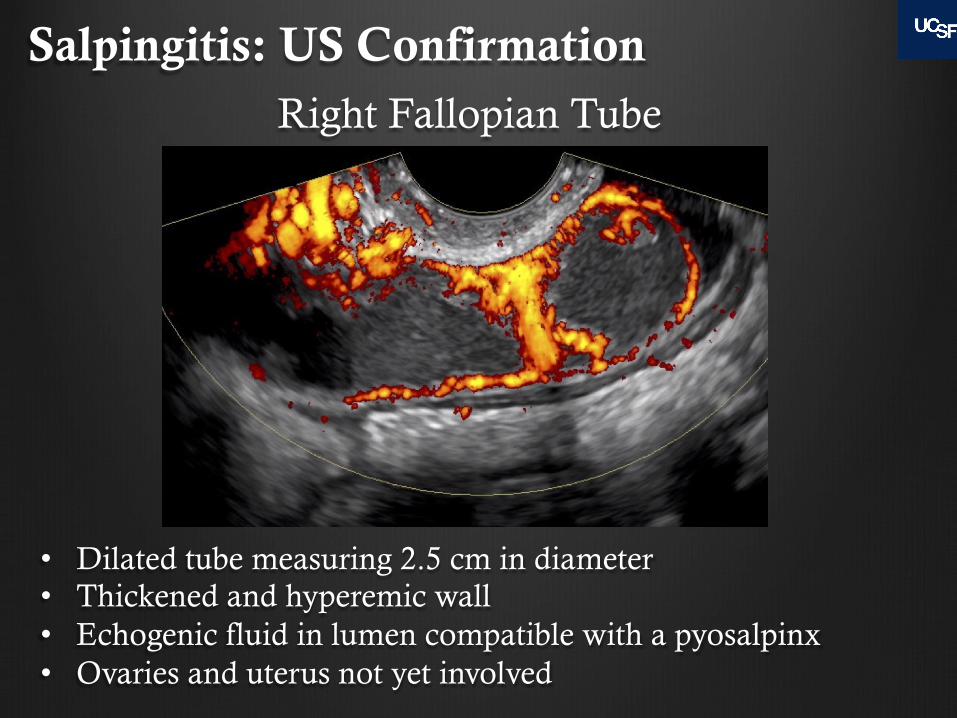
Salpingitis: US Confirmation Right Fallopian Tube
• Dilated tube measuring 2.5 cm in diameter • Thickened and hyperemic wall • Echogenic fluid in lumen compatible with a pyosalpinx • Ovaries and uterus not yet involved
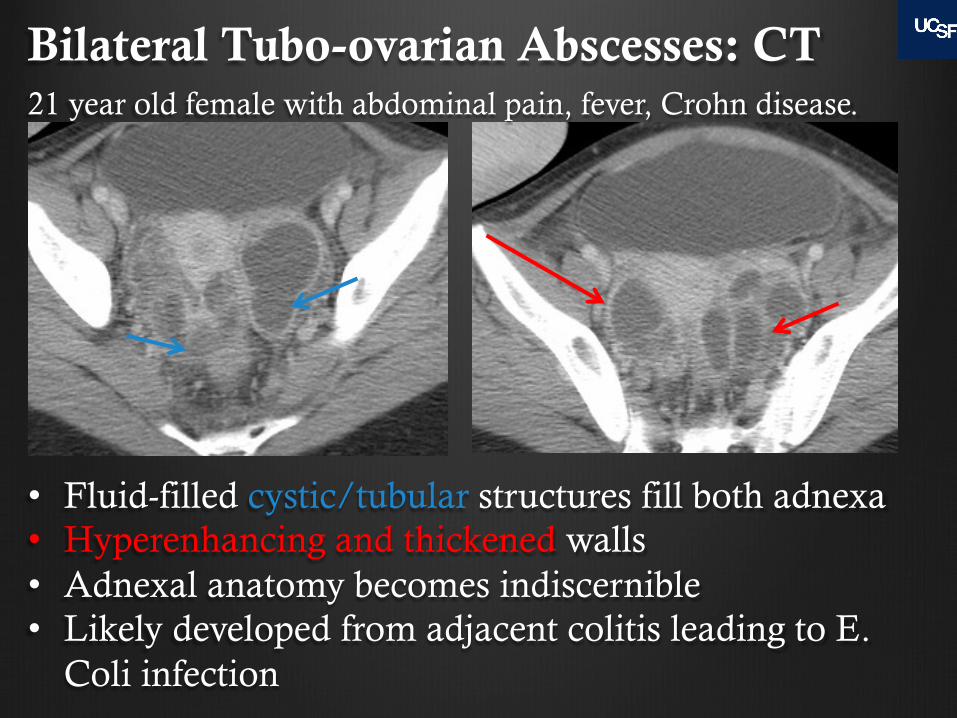
Bilateral Tubo-ovarian Abscesses: CT
• Fluid-filled cystic/tubular structures fill both adnexa • Hyperenhancing and thickened walls • Adnexal anatomy becomes indiscernible • Likely developed from adjacent colitis leading to E.
Coli infection
21 year old female with abdominal pain, fever, Crohn disease.

Acute Fallopian Tube Pathology
" The normal fallopian tube is usually not visualized on CT
" If you see the fallopian tube, suspect pathology, and consider an ultrasound
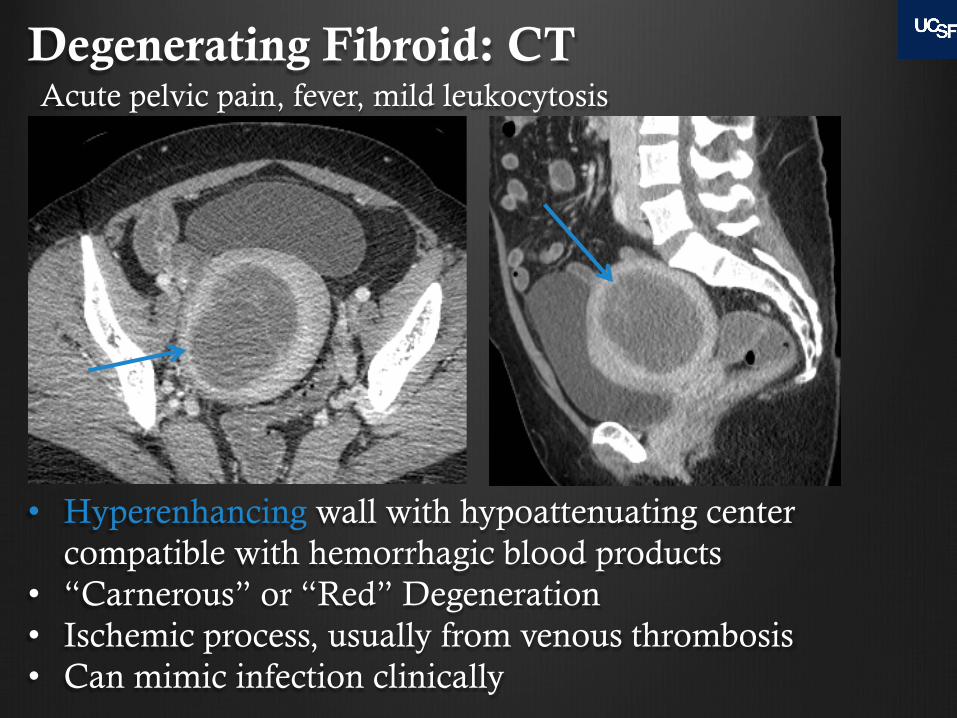
Degenerating Fibroid: CT Acute pelvic pain, fever, mild leukocytosis
• Hyperenhancing wall with hypoattenuating center compatible with hemorrhagic blood products
• “Carnerous” or “Red” Degeneration • Ischemic process, usually from venous thrombosis • Can mimic infection clinically
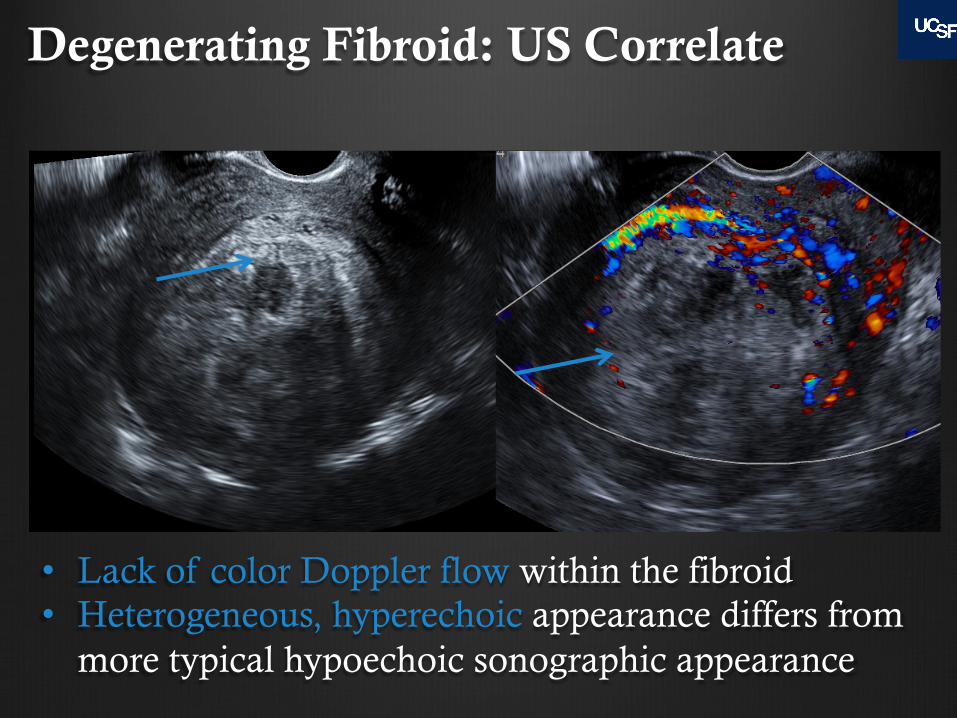
Degenerating Fibroid: US Correlate
• Lack of color Doppler flow within the fibroid • Heterogeneous, hyperechoic appearance differs from
more typical hypoechoic sonographic appearance
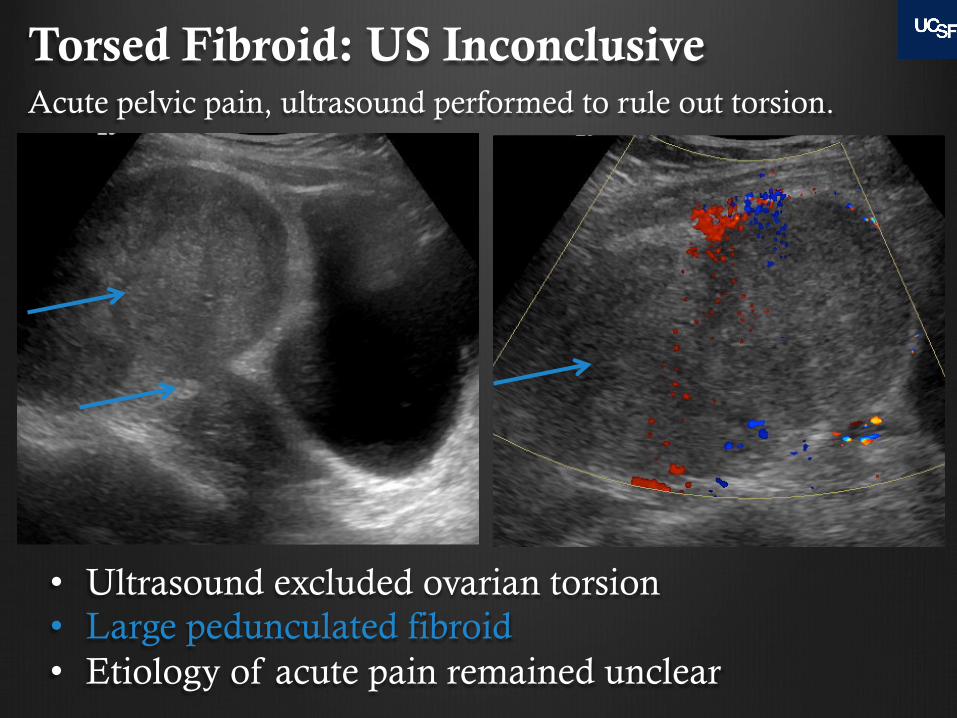
Torsed Fibroid: US Inconclusive
• Ultrasound excluded ovarian torsion • Large pedunculated fibroid • Etiology of acute pain remained unclear
Acute pelvic pain, ultrasound performed to rule out torsion.
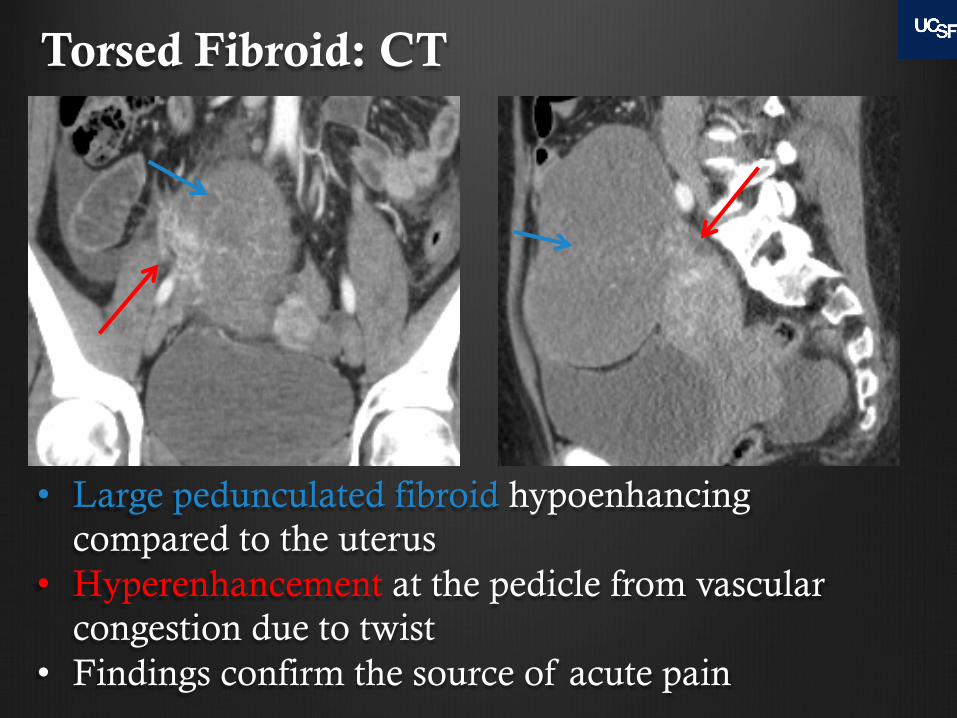
Torsed Fibroid: CT
• Large pedunculated fibroid hypoenhancing compared to the uterus
• Hyperenhancement at the pedicle from vascular congestion due to twist
• Findings confirm the source of acute pain

Torsed Fibroid: CT comparison with prior
• Current CT shows new lack of fibroid enhancement compared to the prior CT
• Torsed fibroid appears has also rotated in position
Prior CT
Current CT
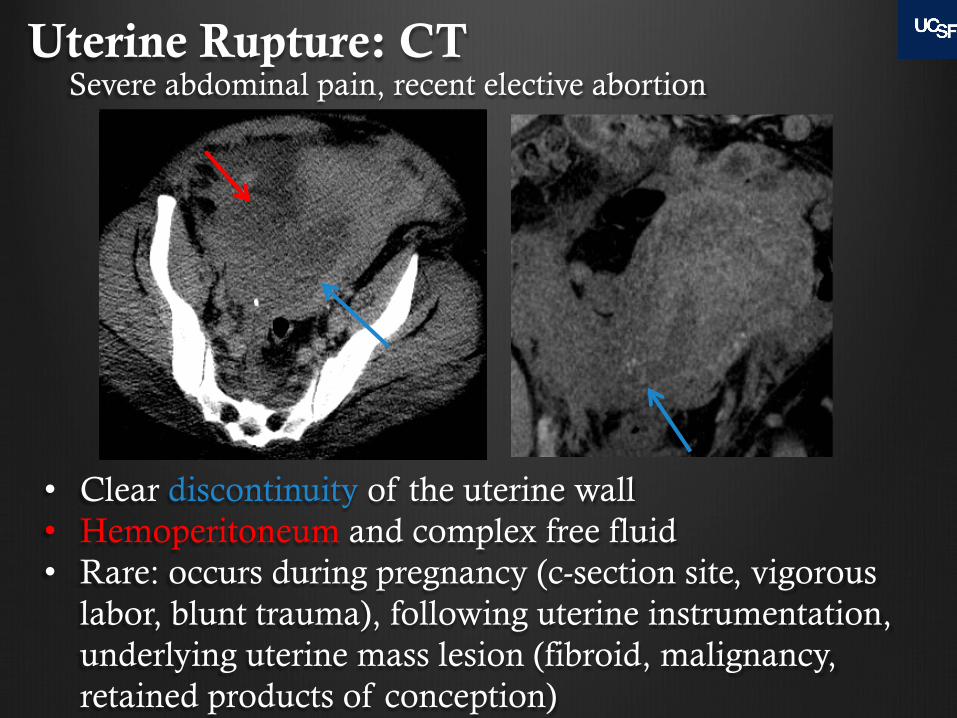
Uterine Rupture: CT Severe abdominal pain, recent elective abortion
• Clear discontinuity of the uterine wall • Hemoperitoneum and complex free fluid • Rare: occurs during pregnancy (c-section site, vigorous
labor, blunt trauma), following uterine instrumentation, underlying uterine mass lesion (fibroid, malignancy, retained products of conception)
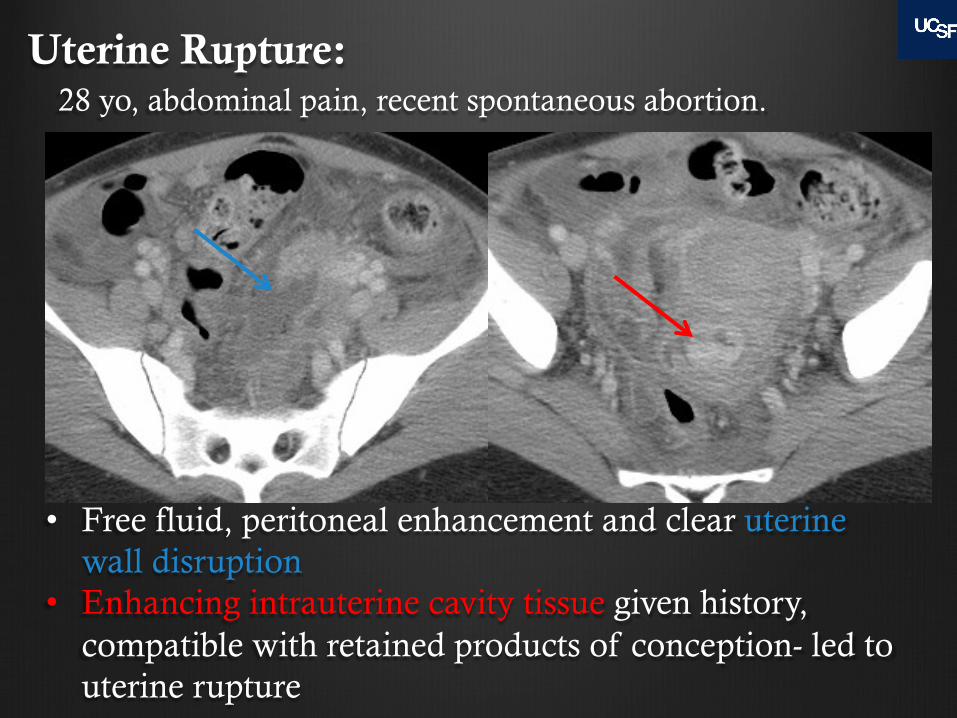
Uterine Rupture:
• Free fluid, peritoneal enhancement and clear uterine
wall disruption • Enhancing intrauterine cavity tissue given history,
compatible with retained products of conception- led to uterine rupture
28 yo, abdominal pain, recent spontaneous abortion.

Misplaced IUD: CT
• Right limb of an IUD grossly penetrates the myometrium
• Ultrasound is not needed to confirm if clearly malpositioned
29 year old with right lower quadrant pain x 4 days.
Conclusions " Acute gynecologic pathology is commonly seen
on CT which may have been performed for other suspected pathology
" CT can be diagnostic in certain cases without additional imaging
" Make the correct diagnosis by: " Include gynecologic organs in CT search pattern
" Recognizing normal and abnormal findings and using secondary signs of acute disease
" If CT is non-confirmatory, correlate with pelvic ultrasound

Sources Choi HJ, Kim SH, Kim SH et al. “Ruptured Corpus Luteal Cyst: CT Findings” Korean J Radiology 2003 Jan-Mar; 4(1): 42-45
Hiller N, Appelbaum L, Simanovsky N, et al. CT Features of Adnexal Torsion. AJR 2007 July; 189(1) 124-129.
Murase E, Siegelman E, Outwater EK, et al. Uterine Leiomyomas: Histopathologic features, MR imaging findings, differential diagnosis, and treatment. Radiographics. 1999 Sep-Oct; 19(5): 1179-97.
Patel MD, Feldstein VA, Lipson SD et-al. Cystic teratomas of the ovary: diagnostic value of sonography. AJR Am J Roentgenol. 1998;171 (4): 1061-5.