acute hip fracture rehabilitation - noca · pdf fileacute hip fracture rehabilitation ... the...
TRANSCRIPT

Acute Hip Fracture
Rehabilitation
Michelle Fitzgerald BSc, MSc, MISCP
Senior Physiotherapist, Tallaght Hospital, Dublin
4th National Irish Hip Fracture Conference
RCSI 18th November 2015

“Mobilise with
physio”

Overview
1. Why mobility is important
2. The evidence base
3. Research study
4. The plan for 2016

Background
• Senior Physiotherapist, Tallaght Hospital
• MSc Neuromusculoskeletal Physiotherapy UCD
• Hip fracture research, audit & quality improvement
• National hip fracture steering group member
• Irish National Orthopaedic Register
• Global Fragility Fracture Network
• Clinical interest group orthopaedics (CPO, IPONG)

Hip Fractures
10%
Die within a month
33%
Die within a year
50%
Unable to walk
unaided
25%
Long Term Care
Stretch Health System
(British Orthopaedic Association 2007, Cummings and Melton., 2002,
Department of Health 2013, Hall et al., 2000, Keen, 2003, McGowan et al., 2013)
The “Hip Attack”

What predicts mortality ?

What predicts hip fracture mortality?
Age
Gender
Medical fitness
Comorbidities
Cognition
Etc
Etc

Anything else?

What else predicts mortality ?
Early
mobility

Early Mobility is Important
(Boonen et al., 2004, Dubljanin-Raspopovic et al., 2013, Hirose et al., 2010)
Post-Op Long-Term
Mobility
Survival
+
Function

Active Acute Rehabilitation
• Maximises recovery
• Successful discharge home
• Decreases length of stay
• Reduce overall cost
(Laflamme et al 2012, Kristenson et al 2007, NICE 2010, Beaupre et al 2013, BOA 2010)

“Rehabilitation of hip
fractures is the central
challenge for trauma
services”
(British Orthopaedic Association 2007)

Review of Rehabilitation
• Amount of rehab varies widely in acute hospitals
• Confidence in rehabilitation progression
• More intense post-operative physio
• Barriers identified
• No data in Ireland
• Time for change
(British Orthopaedic Association 2015, Health Service Executive, 2012, National Institute for Health
and Clinical Excellence, 2011, Ranhoff et al., 2010, Svensson et al., 1996, Thomas et al., 2007)

Time for Change in Ireland
• In order to get better we need to measure what
we are currently doing.
• First step in effecting change:
• Add function specific data-fields to the IHFD
– Functional progress
– Rehabilitation service provision
– Effect of hospital approaches

Irish Hip Fracture Physio Working Group
• Irish Physiotherapy Hip Fracture Working Group
– Edel Callanan (Orthopaedic QCCD therapy lead)
– Dr C Blake & Dr C Cunningham (UCD)
– Michelle Fitzgerald (Senior Physiotherapist)
• ADPATE framework for guideline adaptation

Databases
Direct Communication
International Guidelines

Care Standard Guideline Synopsis
Physio assessment First postoperative day
Frequency of mobilisation Daily (7days)
Rehabilitation Early, MDT
Discharge planning Early, MDT, individualised
Type of physiotherapy Multidimensional
(ANZHFR 2014, NICE 2011, Waddell 2011, SIGN 2009, BOA 2007)

Standardised Outcome Measures
• Hip fracture mobility measures vary widely
• Feasible in clinical practice
• Valid and reliable
• Hip fracture population
• Predict outcome
• Comparison and research
(Foss et al., 2006, Farag et al., 2012, Hollman et al., 2008,
Laflamme et al., 2012, Kristensen et al., 2009b, Kristensen et al., 2007)

New Mobility Score
NMS Category Score Functional ability
0 Not at all
1 Assistance of one person
2 With an aid
3 No difficulty/no aid
Indoor walking, outdoor walking, shopping

New Mobility Score
NMS Category Score Functional ability
0 Not at all
1 Assistance of one person
2 With an aid
3 No difficulty/no aid
Overall Score: 0-9

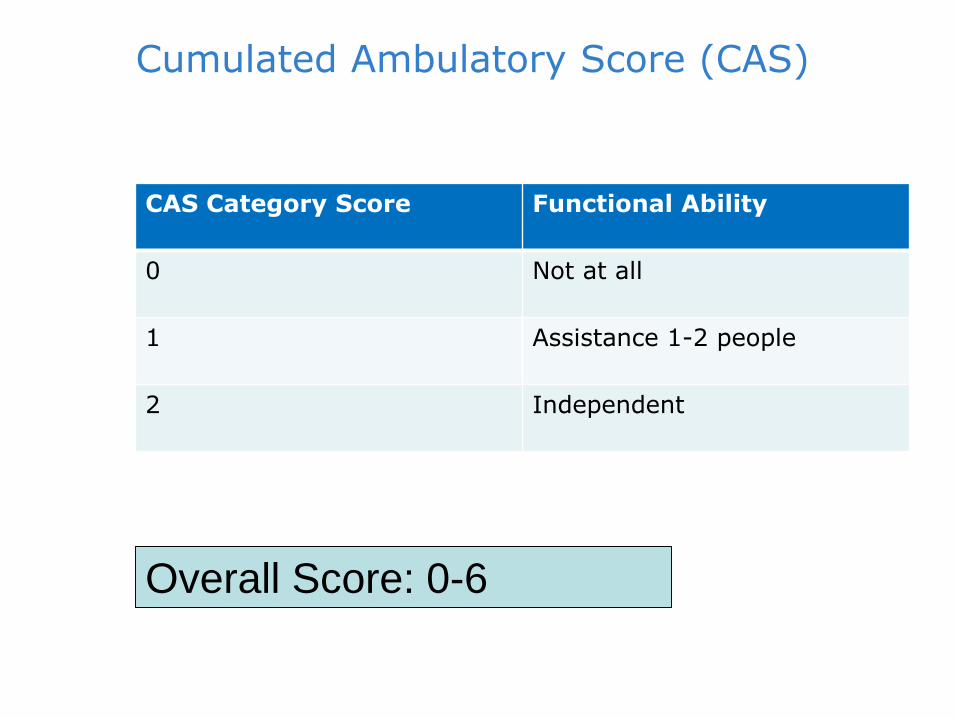
Cumulated Ambulatory Score (CAS)
CAS Category Score Functional Ability
0 Not at all
1 Assistance 1-2 people
2 Independent
Bed mobility, STS, mobilisation
Cumulated Ambulatory Score (CAS)
CAS Category Score Functional Ability
0 Not at all
1 Assistance 1-2 people
2 Independent
Overall Score: 0-6

Predictors of Mobility Outcome at
One Week Post Hip Fracture
Surgery
Michelle Fitzgerald1, Blake, C2. Askin, D3. Coughlan, T3.
Quinlan, J3. Cunningham, C2.
1 Physiotherapy Department & Bone and Joint Unit2, Tallaght Hospital
3 School Of Public Health, Physiotherapy & Population Science, UCD

What should we do?
Rehabilitation Planning
Influencing factors
Optimise early
mobility
(Health Service Executive, 2012, National Institute for Health and Clinical Excellence, 2011,
Ranhoff et al., 2010, Svensson et al., 1996, Thomas et al., 2007)

Study Aim
Identify independent predictors of
mobility at one week post hip fracture
surgery

Methods
• 6 month study period
• Prospective observational cohort study
• 77 patients included (age 77.4±10.2 years)
• Low trauma hip fractures
• Routine physiotherapy
• Chi-square, fischer exact, regression analysis

Day 1
• Patient Demographics
• Fracture-Specific Characteristics
Day 7
• Mobility Outcome MeasuresCumulated Ambulatory Score (CAS) Timed up and Go (TUG)
Discharge• Discharge Details
Data Collection Time-Points

Demographics
Age
Premorbid place of
residence
New Mobility Score
Fall location
Sex

Fracture-Specific
ASA
Fracture Type
Operation Time to Surgery
Ability to stand day
one

Day 1
• Patient Demographics
• Fracture-Specific Characteristics
Day 7
• Mobility Outcome MeasuresCumulated Ambulatory Score (CAS) Timed up and Go (TUG)
Discharge• Discharge Details
Data Collection Time-Points
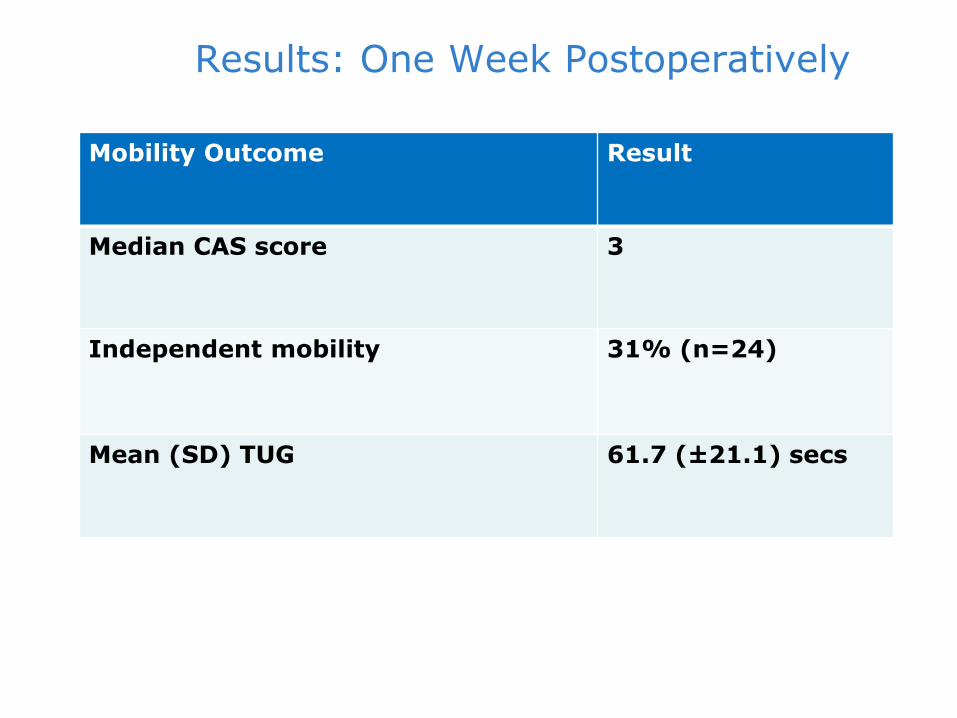
Results: One Week Postoperatively
Mobility Outcome Result
Median CAS score 3
Independent mobility 31% (n=24)
Mean (SD) TUG 61.7 (±21.1) secs

Rehabilitation Needs
• Low functional ability
• Rehabilitation to achieve pre-morbid function
Early stratification for rehabilitation pathways
(Laflamme et al 2012, Kristenson et al 2007, NICE 2010, Beaupre et al 2013, BOA 2010)

Predictor variable Univariate analysis OR (CI)
Multivariate analysis OR (CI)
Fall Location OutdoorIndoorp value
0.180 (0.58-0.557)Reference
p=0.003
3.848 (1.053 – 14.061)Reference
p=0.042
ASA ≤ 2≥ 3p value
3.014 (1.060 – 8.569)Reference
p=0.039
Time to Surgery <36hours≥36hours
p value
8.625 (1.827 – 40.707)Reference
p=0.006
5.472 (1.073-27.907)Reference
p=0.041
NMS 0-67-9
p value
Reference0.304 (0.111-0.833)
p=0.021
Reference 3.366 (1.042 – 10.879)
p=0.043

Predictor variable Univariate analysis OR (CI)
Multivariate analysis OR (CI)
Fall Location OutdoorIndoorp value
0.180 (0.58-0.557)Reference
p=0.003
3.848 (1.053 – 14.061)Reference
p=0.042
ASA ≤ 2≥ 3p value
3.014 (1.060 – 8.569)Reference
p=0.039
Time to Surgery <36hours≥36hours
p value
8.625 (1.827 – 40.707)Reference
p=0.006
5.472 (1.073-27.907)Reference
p=0.041
NMS 0-67-9
p value
Reference0.304 (0.111-0.833)
p=0.021
Reference 3.366 (1.042 – 10.879)
p=0.043

Predictor variable Univariate analysis OR (CI)
Multivariate analysis OR (CI)
Fall Location OutdoorIndoorp value
0.180 (0.58-0.557)Reference
p=0.003
3.848 (1.053 – 14.061)Reference
p=0.042
ASA ≤ 2≥ 3p value
3.014 (1.060 – 8.569)Reference
p=0.039
Time to Surgery <36hours≥36hours
p value
8.625 (1.827 – 40.707)Reference
p=0.006
5.472 (1.073-27.907)Reference
p=0.041
NMS 0-67-9
p value
Reference0.304 (0.111-0.833)
p=0.021
Reference 3.366 (1.042 – 10.879)
p=0.043

Predictor variable Univariate analysis OR (CI)
Multivariate analysis OR (CI)
Fall Location OutdoorIndoorp value
0.180 (0.58-0.557)Reference
p=0.003
3.848 (1.053 – 14.061)Reference
p=0.042
ASA ≤ 2≥ 3p value
3.014 (1.060 – 8.569)Reference
p=0.039
Time to Surgery <36hours≥36hours
p value
8.625 (1.827 – 40.707)Reference
p=0.006
5.472 (1.073-27.907)Reference
p=0.041
NMS 0-67-9
p value
Reference0.304 (0.111-0.833)
p=0.021
Reference 3.366 (1.042 – 10.879)
p=0.043

Total CAS Score at Day 7
• Ability to stand day 1 (p=0.018)
• Age (p=0.018)
• Fall location (p=0.005)
• Premorbid place of residence (p=0.014)
• ASA (p=0.005)
• Time to surgery (p=0.002)
• NMS (p=0.002)

Clinical Implications
3 Predictors
Mobility Measures
Modifiable variables
Pre-fracture function

CAS & NMS
Feasible clinical indicators
for early rehabilitation planning

IHFD Rehabilitation Data-fields 2016
First postoperative
day
DischargeLonger term
Baseline function

Baseline
• New Mobility Score (0-9 + individual sections)
1st post-op Day
• Physio assessment (Yes/No)
• Mobilisation (Yes physio/Yes other/No)
• Cumulated Ambulatory Score (0-6)
Discharge
• Cumulated Ambulatory Score (0-6)
30day
& 120 day
• New Mobility Score (0-9 + individual sections)
Guideline adherence
Service provision
No extra work
Ideal outcome measures
Leading hip
fracture care
Irish data

Guideline adherence
Service provision
No extra work
Ideal outcome measures
Leading hip
fracture care
Irish data

Exciting Times Ahead !!
Advocate
Encourage
Site visits
AHP reps
Future data-fields

Acknowledgements
• National hip fracture steering group
• Physiotherapy hip fracture working group
• Integrated care pathway work to date by physios/OTs

Thank You !

References (1)
• Australian and New Zealand Hip Fracture Registry (ANZHFR) Steering Group.
Australian and New Zealand Guideline for Hip Fracture Care: Improving
Outcomes in Hip Fracture Management of Adults 2014. Sydney
• British Orthopaedic Association (2007) ‘The Care of Patients with Fragility
Fractures’. London, United Kingdom
• British Orthopaedic Association (2015) Getting it Right First Time Report: A
national review of adult elective orthopaedic services in England. London,
United Kingdom.
• Boonen, S. Autier, P. Barette, M. Vanderschueren, D. Lips, P. and Haentjens,
P. (2004) 'Functional outcome and quality of life following hip fracture in
elderly women: a prospective controlled study'. Osteoporos International,
15(2): 87-94.
• Cummings, S. R. and Melton, L. J. (2002) 'Epidemiology and outcomes of
osteoporotic fractures'. The Lancet, 359: 1761-1767.
• Department of Health (2013) health Care Quality Indicators in the Irish Health
System; Examining the Potential of Hospital Discharge Data using the Hospital
Inpaitent Enquiry System. Available at
http://www.dohc.ie/publications/pdf/HCQI.pdf (accessed on 21/04/2014)

References (2)
• Dubljanin-Raspopovic, E. Markovic-Denic, L. Marinkovic, J. Nedeljkovic, U.
Bumbasirevic, M. (2013) Does Early Functional Outcome Predict 1-year
Mortality in Elderly Patients With Hip Fracture? Clin Orthop Relat Res
471:2703–2710
• Foss, N. B. Kristensen, M. T. and Kehlet, H. (2006) 'Prediction of
postoperative morbidity, mortality and rehabilitation in hip fracture patients:
the cumulated ambulation score'. Clinical Rehabilitation, 20(8): 701-708.
• Fervers B, Burgers JS, Haugh MC, Latreille J, Mlika-Cabanne N, Paquet L,
Coulombe M, Poirier M, Burnand B. Adaptation of clinical guidelines: literature
review and proposition for a framework and procedure. Int J Qual Health Care
2006;18(3):167–76.
• Fitzgerald M, Cunningham C. Prediction of mobility outcome at one week post
hip fracture surgery. MSc Thesis 2014, UCD.
• Fitzgerald M, Askin D, Coughlan T, Quinlan J, Blake C, Cunningham C.
Predicting mobility one week after hip fracture surgery: a prospective
observational cohort study. Presented at the 3rd Fragility Fracture Network
Global Congress 2014; Madrid, Spain.
• Freter, SH and Fruchter, N. (2000) ‘Relationship between timed 'up and go'
and gait time in an elderly orthopaedic rehabilitation population’. Clinical
Rehabilitation, 14:96-101.

References (3)
• Green, C. Molony, D. Fitzpatrick, C. and O'Rourke, K. (2010) 'Age-specific
incidence of hip fracture in the elderly: a healthy decline'. The Surgeon,
Journal of the royal Colleges of Surgeons of Edinburgh and Ireland, 8:310-
313
• Guccione, A. A. Fagerson, T. L. and Anderson, J. J. (1996) 'Regaining
functional independence in the acute care setting following hip fracture'.
Physical Therapy, 76(8): 818-26.
• Hall, S. E. Williams, J. A. Senior, J. A. Goldswain, P. R. and Criddle, R. A.
(2000) 'Hip fracture outcomes: quality of life and functional status in older
adults living in the community'. Australian and New Zealand Medical Journal,
30(3):327-32.
• Kristensen M T, Bandholm T, Foss N B, Ekdahl C and Kehlet H. High inter-
tester reliability of the new mobility score in patients with hip fracture. J
Rehabil Med 2008; 40(7): 589-91.
• Handoll, H. H. Cameron, I. D. Mak, J. C. and Finnegan, T. P. (2009)
'Multidisciplinary rehabilitation for older people with hip fractures'. Cochrane
Database Systematic Review, (4):CD007125.
• Health Service Executive (2012) ‘National Service Plan 2013’. Dublin, Ireland.
Available at:
http://www.hse.ie/eng/services/Publications/corporate/NSP2013.pdf
(accessed 03 February 2013).

References (4)
• Hirose, J. Ide, J. Yakushiji, T. Abe, Y. Nishida, K. Maeda, S. Anraku, Y. Usuku,
K. and Mizuta, H. (2010) 'Prediction of postoperative ambulatory status 1 year
after hip fracture surgery'. Archives of Physical Medical Rehabilitation, 91:67-
72.
• Hollman, J. H., Beckman, B. A., et al. (2008). "Minimum detectable change in
gait velocity during acute rehabilitation following hip fracture." J Geriatr Phys
Ther 31(2): 53-56
• Keen, R. W. (2003) 'Burden of osteoporosis and fractures', Current
Osteoporosis Reports. 1(2): 66-70.
• Kristensen, M. T. Bandholm, T. Bencke, J. Ekdahl, C. and Kehlet, H. (2009a)
'Knee-extension strength, postural control and function are related to fracture
type and thigh edema in patients with hip fracture'. Clinical Biomechanics,
218-224.
• Kristensen M T, Foss N B, Ekdahl C and Kehlet H. Prefracture functional level
evaluated by the New Mobility Score predicts in-hospital outcome after hip
fracture surgery. Acta Orthop 2010; 81(3): 296-302.
• Kristensen M T, Bandholm T, Foss N B, Ekdahl C and Kehlet H. High inter-
tester reliability of the new mobility score in patients with hip fracture. J
Rehabil Med 2008; 40(7): 589-91.
References (5)
• Kristensen, M. T. Foss, N. B. and Kehlet, H. (2007) 'Timed "up & go" test as a
predictor of falls within 6 months after hip fracture surgery'. Physical Therapy,
24-30.
• Kristensen, M. T. Foss, N. B. and Kehlet, H. (2009b) 'Factors with
independent influence on the 'timed up and go' test in patients with hip
fracture', Physiotherapy Research International.14(1):30-41.
• Kristensen, M. T. Jakobsen, T. L. Nielsen, J. W. Jorgensen, L. M. Nienhuis, R.
J. and Jonsson, L. R. (2012) 'Cumulated Ambulation Score to evaluate
mobility is feasible in geriatric patients and in patients with hip fracture'.
Danish Medical Bulletin,July:1-5.
• Laflamme, G. Y. Rouleau, D. M. Leduc, S. Roy, L. and Beaumont, E. (2012)
'The Timed Up and Go test is an early predictor of functional outcome after
hemiarthroplasty for femoral neck fracture' Journal of Bone and Joint Surgery
America, 1175-9.
• Latham, N., Mehta, V., et al. (2008). "Performance-based or self-report
measures of physical function: which should be used in clinical trials of hip
fracture patients?" Archives of physical medicine and rehabilitation 89(11):
2146-2155.
• McGowan, B. Casey, M. C. Silke, C. Whelan, B. and Bennett, K. (2013)
'Hospitalisations for fracture and associated costs between 2000 and 2009 in
Ireland: a trend analysis'. Osteoporosis International, 24(3): 849-57.

References (6)
• Michel, J. P. Klopfenstein, C. Hoffmeyer, P. Stern, R. and Grab, B. (2002) 'Hip
fracture surgery: is the pre-operative American Society of Anesthesiologists
(ASA) score a predictor of functional outcome?', Ageing Clincial and
Experimental Research. 14(5): 389-94.
• National Institute for Health and Clinical Excellence (2011) ‘The management
of hip fractures in adults’ [CG124]. London.
• National Office of Clincial Audit (NOCA). Irish Hip Fractre Database
Preliminary Report 2013; Dublin, Ireland. Accessed
http://www.noca.ie/files/NOCA/20140304103916_IHFD_Preliminary_Report_
%202013..pdf on 2nd October 2014.
• Parker M J and Palmer C R. A new mobility score for predicting mortality after
hip fracture. J Bone Joint Surg Br 1993; 75(5): 797-8.
• Parker, M. J. and Palmer, C. R. (1995) 'Prediction of rehabilitation after hip
fracture', Age and Ageing, 24(2): 96-8.
• Podsiadlo, D. and Richardson, S. (1991)’ The Timed Up & Go: A test of basic
functional mobility for frail elderly persons’. Journal of the American Geriatrics
Society. 39:142-148.

References (7)
• Ranhoff, A. H. Holvik, K. Martinsen, M. I. Domaas, K. and Solheim, L. F.
(2010) 'Older hip fracture patients: three groups with different needs'. BMC
Geriatrics, 10(65):1-7
• Scottish Intercollegiate Guidelines Network (SIGN). Management of hip
fracture in older people: a natioanl clinical guidline 2009. Edinburgh
• Svensson, O. Stromberg, L. Ohlen, G. and Lindgren, U. (1996) 'Prediction of
the outcome after hip fracture in elderly patients', Journal of Bone and Joint
Surgery Britian, 78(1): 115-8.
• Thomas, S. Mackintosh, S. and Halbert, J. (2011) 'Determining current
physical therapist management of hip fracture in an acute care hospital and
physical therapists' rationale for this management'. Physical Therapy, 91(10):
1490-502.
• Waddell J. National Hip Fracture Toolkit 2011; accessed
http://boneandjointcanada.com/wp-content/uploads/2014/05/National-hip-
fracture-toolkit-June-2011.pdf on 24 November 2014