acute renal failure in the icu - ucsf cme · acute renal failure in the icu ... ct, arteriography...
TRANSCRIPT
Acute Renal Failure Acute Renal Failure in the ICUin the ICU
Kathleen D. Liu, MD, PhDKathleen D. Liu, MD, PhDJune 2008June 2008
Acute Renal FailureAcute Renal Failure
Scope of the problemScope of the problemPrevention strategiesPrevention strategiesPrevention strategies: contrastPrevention strategies: contrastTreatmentTreatment
Role of diureticsRole of diureticsDialysis modalitiesDialysis modalities

Acute renal failure is a Acute renal failure is a spectrum of diseasespectrum of disease
Increased serum Cr DialysisVolume overloadAcidosis

Acute renal failure is a Acute renal failure is a spectrum of diseasespectrum of disease
Increased serum Cr DialysisVolume overloadAcidosis
Metnitz et al, Crit Care Med 2002

Patients with ARF are at a Patients with ARF are at a higher risk for deathhigher risk for death
ARF is COMMON: 31% had an increase in Cr of ARF is COMMON: 31% had an increase in Cr of 0.3 0.3 mg/dL mg/dL or greater, 13% had an increase of or greater, 13% had an increase of 0.5 0.5 mg/dL mg/dL or greateror greaterEven small changes are associated with an Even small changes are associated with an increased risk of death: OR for death of 1.7 for increased risk of death: OR for death of 1.7 for those with an increase in Cr of 0.3those with an increase in Cr of 0.3--0.4 0.4 mg/dLmg/dLARF is associated with increasedARF is associated with increased length of stay:length of stay:those with an increase inthose with an increase in Cr of 0.5 Cr of 0.5 mg/dL mg/dL or or greater had a 3.5 day increase in LOS greater had a 3.5 day increase in LOS (p<0.0001)(p<0.0001)
Chertow et al, JASN 2005

What is acute renal What is acute renal failure?failure?

Acute Tubular Necrosis is the Most Acute Tubular Necrosis is the Most Common Cause of HospitalCommon Cause of Hospital
Acquired ARFAcquired ARF
PRERENAL
Vascular Glomerulonephritis
IschemicHypotension
SepsisProlonged prerenal state
NephrotoxicAminoglycosides
ContrastMyoglobin
Acute TubularNecrosis
Acute InterstitialNephritis
INTRINSIC RENAL POSTRENAL
ACUTE RENAL FAILURE

NewNew terminology for ARF: terminology for ARF: Acute Kidney InjuryAcute Kidney Injury
Bellomo et al, Crit Care
8(2004): R204-212

NewNew terminology for ARF: terminology for ARF: Acute Kidney InjuryAcute Kidney Injury
Mehta et al, Crit Care
11(2007): R31
Prevention of ARFPrevention of ARF
EarlyEarly recognition is keyrecognition is keyChanges in Changes in creatinine creatinine reflect changes in reflect changes in GFR, which is probably a late GFR, which is probably a late manifestation of renal injurymanifestation of renal injuryA A ““normalnormal”” serum serum creatinine creatinine may reflect may reflect significant renal insufficiency, in significant renal insufficiency, in particularly in the elderlyparticularly in the elderly
Prevention of ARFPrevention of ARFAvoid Avoid nephrotoxic nephrotoxic medications:medications:
NSAIDsNSAIDsRadiocontrastRadiocontrastAminoglycosidesAminoglycosidesAmphotericinAmphotericinACE ACE inhibitors/Angiotensin inhibitors/Angiotensin receptor blockersreceptor blockers
Avoid Avoid hypoperfusion hypoperfusion Volume depletionVolume depletionHHypotensionypotension

Prevention of complicationsPrevention of complications
Nephrogenic Nephrogenic systemic fibrosissystemic fibrosis

Prevention of complicationsPrevention of complicationsNephrogenic Nephrogenic systemic fibrosissystemic fibrosis
Associated with use of gadoliniumAssociated with use of gadolinium--based MRI based MRI contrast agentscontrast agentsHas been observed in patients with chronic Has been observed in patients with chronic kidney disease and acute renal failurekidney disease and acute renal failureIncidence unknown for either CKD/ESRD or Incidence unknown for either CKD/ESRD or ARF (butARF (but rare)rare)Must weigh risks/benefits of study (andMust weigh risks/benefits of study (andpotential risk of contrast nephropathy with potential risk of contrast nephropathy with alternative imaging modalities)alternative imaging modalities)

Prevention of complicationsPrevention of complicationsNephrogenic Nephrogenic systemic fibrosissystemic fibrosis
We do not empirically dialyze patients to We do not empirically dialyze patients to remove gadolinium, nor do we perform remove gadolinium, nor do we perform hemodialysis hemodialysis on PD patients (half life is on PD patients (half life is markedly prolonged with markedly prolonged with hemodialysishemodialysis, and is , and is even longer with peritoneal dialysis)even longer with peritoneal dialysis)For dialysis patients, we do try to dialyze them For dialysis patients, we do try to dialyze them as soon as possible after the imaging study as soon as possible after the imaging study (so requires some coordination with radiology)(so requires some coordination with radiology)

Contrast NephropathyContrast NephropathyContrastContrast--induced nephropathy accounts induced nephropathy accounts for approximately 10% of hospitalfor approximately 10% of hospital--acquired acquired ARFARFThe incidence of ARF and ARF requiring The incidence of ARF and ARF requiring dialysis was 144.6/1000 and 7.7/1000 dialysis was 144.6/1000 and 7.7/1000 cases respectively (N=1826)cases respectively (N=1826)The inThe in--hospital mortality rate for those who hospital mortality rate for those who required dialysis was 35.7%required dialysis was 35.7%
Briguiori et al, Prog Cardivasc Dis 45(2003): 493-503McCullough et al, Am J Med 103(1997): 368-75
PathophysiologyPathophysiologyContrast induced nephropathy is thought to be Contrast induced nephropathy is thought to be the result of free radical generation the result of free radical generation Hyperosmolar stress (contrast) prompts the Hyperosmolar stress (contrast) prompts the generation of reactive O2 speciesgeneration of reactive O2 speciesFreeFree--radical generation is further promoted by radical generation is further promoted by an acidic environment typical of tubular urinean acidic environment typical of tubular urineRadiocontrast causes vasoconstriction and a Radiocontrast causes vasoconstriction and a decrease in RBF, leading to worsening decrease in RBF, leading to worsening medullary hypoxiamedullary hypoxia
Risk factors for contrast Risk factors for contrast nephropathynephropathy
Chronic kidney diseaseChronic kidney diseaseDiabetes mellitusDiabetes mellitusAgeAgeHypotensionHypotensionHeart failureHeart failureIntraaortic ballon Intraaortic ballon pumppumpContrast propertiesContrast propertiesContrast volumeContrast volume
Pannu et al, JAMA 295(2006): 2765-79

What is the role of NAC in What is the role of NAC in contrast nephropathy?contrast nephropathy?
Tepel Tepel et al reported a 90% risk reduction et al reported a 90% risk reduction in the risk of contrast nephropathy with Nin the risk of contrast nephropathy with N--acetylcysteine (22% vs 2%)acetylcysteine (22% vs 2%)Many small studies have since been Many small studies have since been published with variable effects published with variable effects There have now beenThere have now been numerous metanumerous meta--analyses on this subject showinganalyses on this subject showing little to little to no benefitno benefit (but no(but no harm)harm)
Tepel et al, NEJM 343(2000):180-4

What is the role of NAC in What is the role of NAC in contrast nephropathy?contrast nephropathy?
Marenzi Marenzi et al, NEJM 354(2006): 2773et al, NEJM 354(2006): 2773RCT ofRCT of 354 patients undergoing primary 354 patients undergoing primary angioplasty for STEMIangioplasty for STEMI1:1:1 allocation of placebo/standard dose/ 1:1:1 allocation of placebo/standard dose/ high dose NAChigh dose NACRegimen: IV bolus of 600(1200) mg, Regimen: IV bolus of 600(1200) mg, followed by PO dosingfollowed by PO dosing x 48hx 48h

*1°
*
*

NAC NAC -- words of caution?words of caution?Acute renal failure in these studies is typically Acute renal failure in these studies is typically defined as a 0.5 mg/dL increase in serum defined as a 0.5 mg/dL increase in serum creatininecreatinineThese studies typically enroll patients These studies typically enroll patients undergoing elective/emergent CT or cardiac undergoing elective/emergent CT or cardiac catheterization but who are not critically illcatheterization but who are not critically illNACNAC may directly affect serum Cr levels may directly affect serum Cr levels (Hoffman (Hoffman et al, JASN, 2005)et al, JASN, 2005)
What are the effects on other disease states,What are the effects on other disease states, eg eg sepsis? sepsis? ((Spapen Spapen et al, Chest, 2005)et al, Chest, 2005)

What is the IVF of choice prior What is the IVF of choice prior to contrast administration?to contrast administration?IV hydration is beneficialIV hydration is beneficialBecause free radicals are postulated to Because free radicals are postulated to mediate contrast nephropathy, alkalinizing mediate contrast nephropathy, alkalinizing the urine with bicarbonate may reduce the urine with bicarbonate may reduce injuryinjuryHypothesis: Using IVF that contain Hypothesis: Using IVF that contain bicarbonate for prebicarbonate for pre--contrast hydration may contrast hydration may have benefit over NaClhave benefit over NaCl--containing fluidscontaining fluids

Bicarbonate Hydration for the Prevention Bicarbonate Hydration for the Prevention of Contrast Nephropathyof Contrast Nephropathy
Single center, randomized control trialSingle center, randomized control trialPatients with Cr Patients with Cr ≥≥ 1.1 mg/dL scheduled to 1.1 mg/dL scheduled to undergo cardiac cath, CT, arteriography or TIPS undergo cardiac cath, CT, arteriography or TIPS (emergent cases were excluded)(emergent cases were excluded)Study terminated early because of increased Study terminated early because of increased incidence of contrast nephropathyincidence of contrast nephropathy with NS with NS hydration (8/59hydration (8/59 vs vs 1/60)1/60)Bicarbonate should be used with caution in Bicarbonate should be used with caution in those with a respiratory or metabolic alkalosis,those with a respiratory or metabolic alkalosis,and those at risk forand those at risk for hypokalemiahypokalemia
Merten, et al. JAMA
291(2004): 2328-34

Bicarbonate 2008 Update: Bicarbonate 2008 Update: REMEDIALREMEDIAL
Briguori et al, Circulation 115(2007): 1211-7

Bicarbonate 2008 Update: Bicarbonate 2008 Update: REMEDIALREMEDIAL
No
untreated control group!

Bicarbonate 2008 Update:Bicarbonate 2008 Update: RENORENO
RCT of anRCT of an
““activeactive””
treatment strategy treatment strategy vs vs ““standardstandard”” care in patientscare in patients
undergoing emergent PCIundergoing emergent PCI
ActiveActive StandardStandard
BolusBolusYes:Yes:
5 ml/kg D5W+154meQ 5 ml/kg D5W+154meQ NaHCO3 x 1hNaHCO3 x 1h
NoNo
IVFIVF 1.5 ml/kg D5W+154meQ 1.5 ml/kg D5W+154meQ NaHCO3 x 12hNaHCO3 x 12h 1 ml/kg1 ml/kg
NS x 12hNS x 12h
NACNAC2400 mg2400 mg
with bolus with bolus fluids, then 2 x 600 fluids, then 2 x 600 mg PO the next daymg PO the next day
2 x 600 mg PO the 2 x 600 mg PO the next daynext day

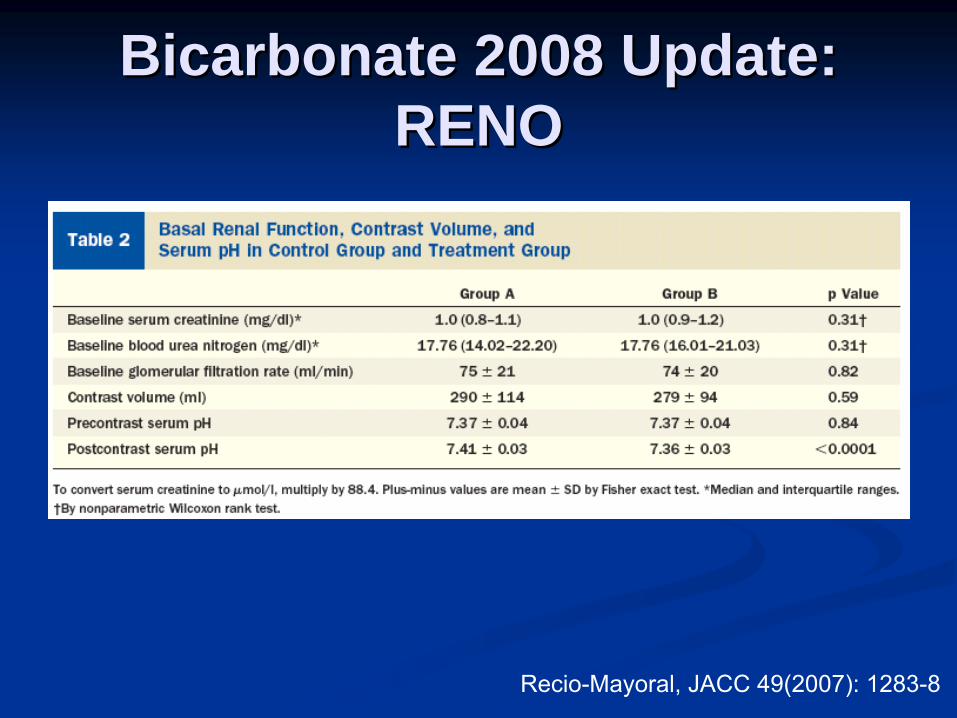
Bicarbonate 2008 Update:Bicarbonate 2008 Update: RENORENO
Recio-Mayoral, JACC 49(2007): 1283-8
Bicarbonate 2008 Update:Bicarbonate 2008 Update: RENORENO
Recio-Mayoral, JACC 49(2007): 1283-8

Bicarbonate 2008 Update:Bicarbonate 2008 Update: RENORENO
Multipledifferencesbetweentreatmentstrategies!

Bicarbonate 2008 Update:Bicarbonate 2008 Update: Mayo ExperienceMayo Experience
Retrospective cohort study of 7977 Retrospective cohort study of 7977 patientspatients with 11516 contrast exposureswith 11516 contrast exposures
From
et al, CJASN 3(2008): 10-18

Bicarbonate 2008 Update:Bicarbonate 2008 Update: Mayo ExperienceMayo Experience
From
et al, CJASN 3(2008): 10-18

Does your patient Does your patient ““needneed””dialysis?dialysis?
Classic indications can be divided into:Classic indications can be divided into:A A cidosiscidosisE E lectrolyteslectrolytesI I ngestionsngestionsOO verload verload (volume)(volume)U U remia remia
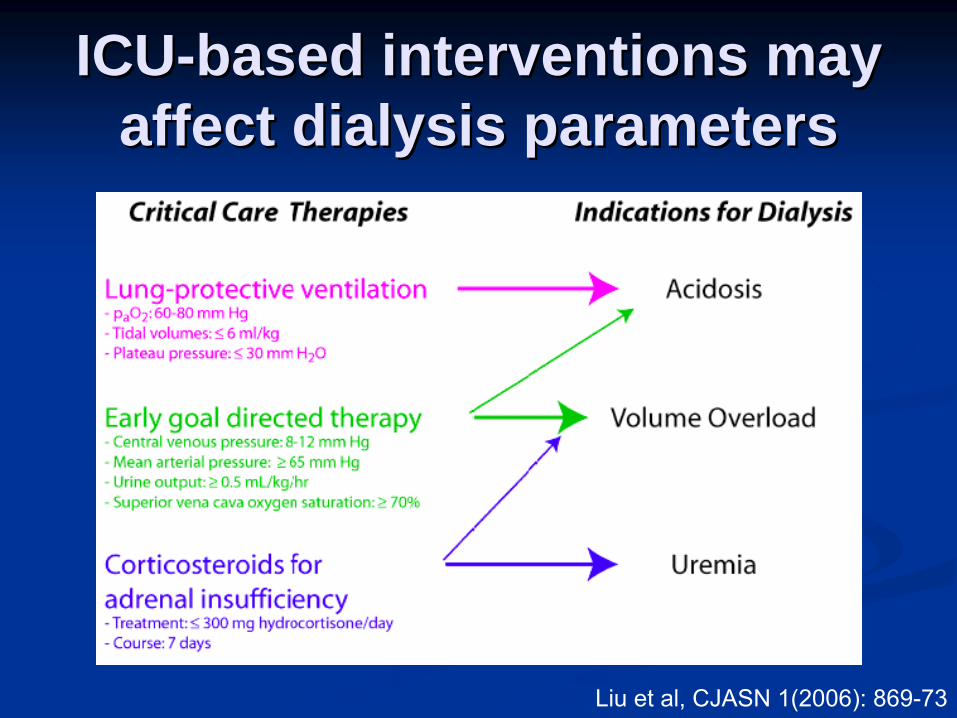
ICUICU--based interventions may based interventions may affect dialysis parametersaffect dialysis parameters
Liu et al,
CJASN 1(2006): 869-73
If your patient If your patient ““needsneeds”” dialysis,dialysis, what is the data what is the data in support of continuous in support of continuous
versus intermittent versus intermittent dialysis?dialysis?

At this point, CRRT and At this point, CRRT and IHDIHD cancan be considered be considered essentially equivalentessentially equivalent

How much dialysis is How much dialysis is enough?enough?
What should our goals be?What should our goals be?Normal electrolytes?Normal electrolytes?Normal BUN/Cr?Normal BUN/Cr?Normal volume status?Normal volume status?Mortality benefit of therapy?Mortality benefit of therapy?

How much dialysis is How much dialysis is enough?enough?
What should our goals be?What should our goals be?Normal electrolytes?Normal electrolytes?Normal BUN/Cr?Normal BUN/Cr?Normal volume status?Normal volume status?Mortality benefit of therapy?Mortality benefit of therapy?
Studies of dose of dialysis in acute renal Studies of dose of dialysis in acute renal failure are extremely limited (one large trial failure are extremely limited (one large trial for CVVH, one large trial for IHD)for CVVH, one large trial for IHD)

Department of Veterans AffairsCOOPERATIVE STUDIES PROGRAM
Intensive vs Conventional Renal Supportin Acute Renal Failure
Overview of Study DesignOverview of Study Design
IntensiveManagement
Strategy
ConventionalManagement
Strategy

Overview of Study DesignOverview of Study Design
Intermittent Hemodialysis(SOFA Cardiovascular Score 0-2)
CVVHDF or SLED/EDD(SOFA Cardiovascular Score 3-4)

Intensive Management Intensive Management StrategyStrategy
Intermittent Hemodialysis 6-times per week(target Kt/V of 1.2/treatment)
CVVHDF with effluent flow of 35 mL/kg/hror
SLED/EDD 6-times per week (target Kt/V of 1.2/treatment)

Conventional Management Conventional Management StrategyStrategy
Intermittent Hemodialysis 3-times per week(target Kt/V of 1.2/treatment)
CVVHDF with effluent flow of 20 mL/kg/hror
SLED/EDD 3-times per week (target Kt/V of 1.2/treatment)


Baseline DemographicsBaseline DemographicsIntensiveIntensive(N=563)(N=563)
LessLess-- IntensiveIntensive(N=561)(N=561)
PP--valuevalue
Age (yr)Age (yr) 59.659.6±±16.316.3 59.759.7±±15.215.2 0.970.97Gender (% male)Gender (% male) 72.672.6 68.668.6 0.130.13Race/ethnicity (%)Race/ethnicity (%)
WhiteWhiteBlackBlackHispanicHispanicOtherOther
73.773.716.216.27.87.82.32.3
75.075.015.715.75.95.93.43.4
0.430.43
Primary treating service (%)Primary treating service (%)MedicalMedicalSurgicalSurgicalOtherOther
48.348.340.740.711.011.0
46.246.241.841.812.012.0
0.760.76
Length of stay preLength of stay pre--randomization randomization (days)(days)
HospitalHospitalICUICU
11.111.1±±13.613.66.96.9±±10.110.1
10.310.3±±14.714.76.46.4±±7.87.8
0.360.360.380.38

Baseline Severity of IllnessBaseline Severity of Illness
IntensiveIntensive(N=563)(N=563)
LessLess-- IntensiveIntensive(N=561)(N=561)
PP--valuevalue
Charlson coCharlson co--morbidity indexmorbidity index 4.34.3±±3.03.0 4.24.2±±2.82.8 0.660.66Mechanically ventilated (%)Mechanically ventilated (%) 80.580.5 80.780.7 0.910.91Sepsis (%)Sepsis (%) 63.663.6 62.462.4 0.680.68APACHE II scoreAPACHE II score 26.626.6±±7.27.2 26.126.1±±7.57.5 0.290.29SOFA scoreSOFA score
RespiratoryRespiratoryCoagulationCoagulationLiverLiverCardiovascularCardiovascularCNSCNS
14.714.7±±3.73.72.42.4±±1.11.11.41.4±±1.21.21.51.5±±1.31.32.32.3±±1.71.72.52.5±±1.41.4
14.414.4±±3.73.72.32.3±±1.11.11.31.3±±1.21.21.41.4±±1.31.32.22.2±±1.71.72.52.5±±1.41.4
0.210.210.100.100.490.490.290.290.230.230.690.69
Cleveland Clinic ICUCleveland Clinic ICU--ARF scoreARF score 12.312.3±±3.33.3 12.012.0±±3.43.4 0.110.11

Management of IHD: Management of IHD: Delivered Kt/VDelivered Kt/Vureaurea

Management of CVVHDF: Management of CVVHDF: Effluent Flow by TreatmentEffluent Flow by Treatment
Prescribed Dose of CVVHDF
Delivered Dose of CVVHDF
perc
ent o
f pat
ient
spe
rcen
t of p
atie
nts

6060--Day All Cause MortalityDay All Cause Mortality
Odds Ratio: 1.0995% CI: 0.86-1.40P=0.47

6060--Day All Cause Mortality: Day All Cause Mortality: Subgroup AnalysisSubgroup Analysis
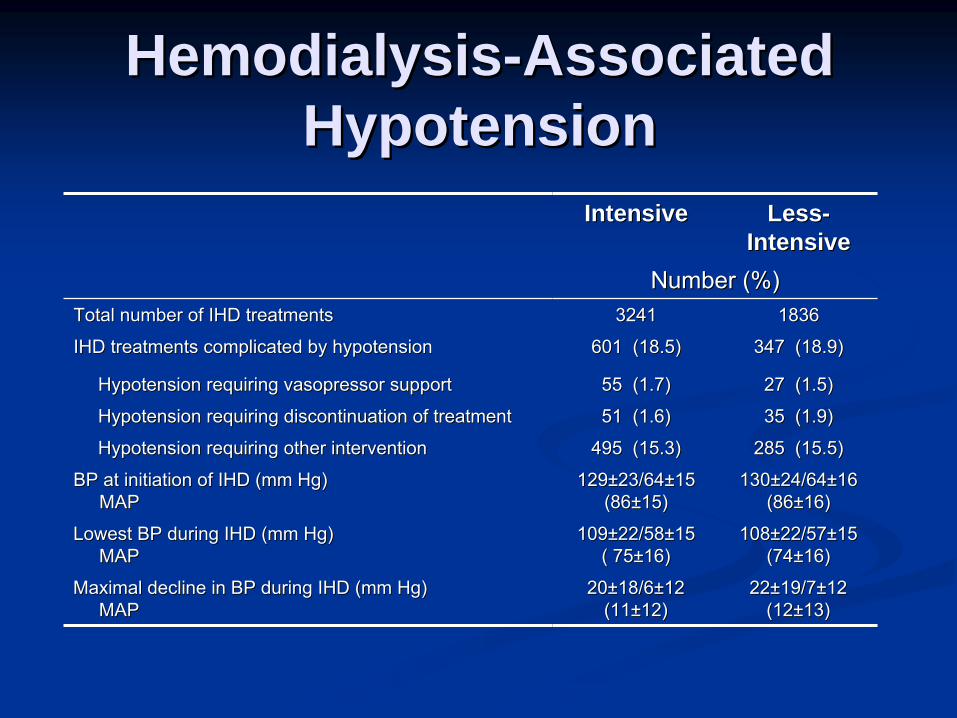
HemodialysisHemodialysis--Associated Associated HypotensionHypotension
IntensiveIntensive LessLess-- IntensiveIntensive
Number (%)Number (%)Total number of IHD treatmentsTotal number of IHD treatments 32413241 18361836
IHD treatments complicated by hypotensionIHD treatments complicated by hypotension 601 (18.5) 601 (18.5) 347 (18.9)347 (18.9)
Hypotension requiring vasopressor supportHypotension requiring vasopressor support 55 (1.7)55 (1.7) 27 (1.5)27 (1.5)
Hypotension requiring discontinuation of treatmentHypotension requiring discontinuation of treatment 51 (1.6)51 (1.6) 35 (1.9)35 (1.9)
Hypotension requiring other interventionHypotension requiring other intervention 495 (15.3)495 (15.3) 285 (15.5)285 (15.5)
BP at initiation of IHD (mm Hg) BP at initiation of IHD (mm Hg) MAPMAP
129129±±23/6423/64±±1515(86(86±±15)15)
130130±±24/6424/64±±1616(86(86±±16)16)
Lowest BP during IHD (mm Hg) Lowest BP during IHD (mm Hg) MAPMAP
109109±±22/5822/58±±1515( 75( 75±±16)16)
108108±±22/5722/57±±1515(74(74±±16)16)
Maximal decline in BP during IHD (mm Hg) Maximal decline in BP during IHD (mm Hg) MAPMAP
2020±±18/618/6±±1212(11(11±±12)12)
2222±±19/719/7±±1212(12(12±±13)13)

ANZICS RENAL StudyANZICS RENAL Study““ClosedClosed”” ICU model where ICU model where intensivistsintensivistsprescribe RRTprescribe RRTRCT of 2 doses of CVVHDF: 25 RCT of 2 doses of CVVHDF: 25 vsvs 40 40 ml/kg/hour of effluentml/kg/hour of effluentTargeted enrollment of 1500 patients: Targeted enrollment of 1500 patients: power calculations based on mortality rate power calculations based on mortality rate of 60% in control arm, 51.5% in of 60% in control arm, 51.5% in intervention armintervention arm
SummarySummaryIntensive renal support did not:Intensive renal support did not:
decrease mortality, decrease mortality, accelerate recovery of kidney function, or accelerate recovery of kidney function, or alter the rate of nonalter the rate of non--renal organ failurerenal organ failure
The intensive management strategy was The intensive management strategy was associated with:associated with:
A greater percentage of patients with treatment A greater percentage of patients with treatment associated hypotensionassociated hypotensionMore hypokalemia and More hypokalemia and hypophosphatemiahypophosphatemia

SummarySummary
The lessThe less--intensive treatment strategy intensive treatment strategy provided a dose of RRT that may have provided a dose of RRT that may have exceeded customary care, particularly for exceeded customary care, particularly for intermittent hemodialysisintermittent hemodialysis

ConclusionsConclusions
Providing more intensive renal Providing more intensive renal replacement therapy than intermittent replacement therapy than intermittent hemodialysis: 3x/week with a target hemodialysis: 3x/week with a target achieved Kt/Vachieved Kt/Vureaurea of 1.2of 1.2--1.4 per treatment 1.4 per treatment or CRRT with an effluent flow of 20 or CRRT with an effluent flow of 20 mL/kg/hr is not associated with improved mL/kg/hr is not associated with improved outcomes. outcomes.

ConclusionsConclusions
Acute renal failure remains associated with Acute renal failure remains associated with high morbidity and mortalityhigh morbidity and mortalityInterventions to prevent acute renal failure Interventions to prevent acute renal failure remain limited (remain limited (““best standard carebest standard care””))NAC and bicarbonate may have benefit for NAC and bicarbonate may have benefit for contrast nephropathycontrast nephropathy
Role in emergency setting less clearRole in emergency setting less clearRRelatively safeelatively safe

ConclusionsConclusionsDiuretics may be used to manage volume Diuretics may be used to manage volume overload in patients with acute renal overload in patients with acute renal failure, but consider dialysis sooner rather failure, but consider dialysis sooner rather than later for volume overloadthan later for volume overloadCRRT has not been shown to be superior CRRT has not been shown to be superior to intermittent to intermittent hemodialysishemodialysis