acute situation in anticoagulated patients: what are the ... · acute situation in anticoagulated...
TRANSCRIPT

Acute Situation in
Anticoagulated patients:
What are the options?
Peter VerhammeVascular Medicine and Haemostasis
Dept. of Cardiovascular Medicine
University of Leuven

77y old man
Afib – NOAC
e-BIKE trauma
Expanding subdural hematoma
How would you manage?
76y old woman
Afib - NOAC
Cholangitis – Choledocholithiasis
Acute renal insufficiency
How would you manage?

• Clinical benefit in trials and real world
NOACs
RR(95% CI)
p-value
Efficacy
Ischaemic stroke 0.92 (0.83–1.02) 0.10
Haemorrhagic stroke 0.49 (0.38–0.64) <0.0001
Myocardial infarction 0.97 (0.78–1.20) 0.77
All-cause mortality 0.90 (0.85–0.95) 0.0003
Safety
Intracranial haemorrhage 0.48 (0.39–0.59) <0.0001
210.50.2
Favours
NOAC
Favours
warfarinRuff CT et al, Lancet 2014

• Clinical benefit in trials and real world
But
• Emergencies can occur
– Urgent Surgery
– Bleeding
NOACs
• Is anticoagulant present?
» Recent intake – tincture of time
• Can we rely on lab tests?
• Is the surgery/intervention critical?
• Is bleeding uncontrollable / life-
threatening?
Key questions in case of emergency

• Is common
– Major bleeding 1-5% per year in AF
– Intracranial bleeding 0.5-1.2% per year in AF
• Is an independent predictor of subsequent
cardiovascular events
– 3 to 5-fold increase in thrombotic events &
death
Bleeding in anticoagulated patients

• Less critical bleeding with NOACs
• Different bleeding pattern with NOACs
• Patient characteristics drive bleeding
Bleeding in anticoagulated patients

• Supportive care to stabilize patient
• Identify and control source of bleeding
• Assess (anti-)coagulation
Initial Management of Serious
Bleeding Events
Heidbuchel H et al, Europace 2015;17:1467–1507; Weitz JI et al, Circulation 2012;126:2428–2432

How to counteract NOAC?

• Non-specific support of haemostasis
Procoagulants (PCCs, aPCC, FVIIa)
Antifibrinolytics
• Reverse anticoagulation
Idarucizumab
Andexanet
How to counteract NOAC?

Honickel et al. Anesthesiology 2015
In dabigatran-treated pigs, PCC at ≥50 IU/kg
associated with improved outcomes after trauma
PCC 50 or 100 IU/kg: significant
reduction in blood loss
PCC 50 and 100 IU/kg: all animals
survived to the end of the study
Blo
od loss (
mL)
0
2500
5000
PCC 25Control PCC 100PCC 50
Sham
**
Su
rviv
al (%
)
0
50
100
0 60
Control
120 180 240 300
Time (min)
PCC 25 PCC 50 + PCC 100
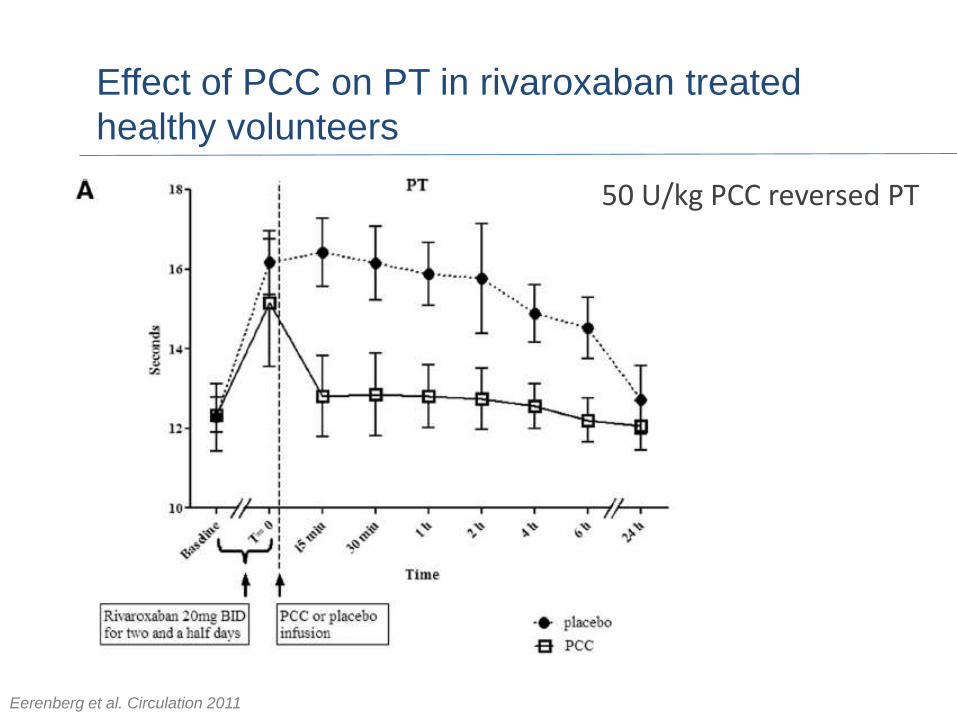
Effect of PCC on PT in rivaroxaban treated
healthy volunteers
Eerenberg et al. Circulation 2011
50 U/kg PCC reversed PT

Reversal Effects of 4F-PCC on Edoxaban after
punch biopsy
Dose-dependent effect of PCC on bleeding
duration (BD), bleeding volume (BV),
Endogenous Thrombin Potential (ETP) and PT
Zahir H, et al. Circulation. 2015

What do the guidelines recommend?
• In case of life-threatening bleeding:
– PCC (50 U/kg)
– aPCC (50–100 U/kg)
– rFVIIa (90 µg/kg)No data about additional benefit
Heidbuchel et al. Europace 2015

How do (a)PCCs support coagulation?
Tissue factor
Xa
Thrombin
Contact
Clot formation
Dabigatran
Rivaroxaban
Apixaban
Edoxaban
PCC or
aPCC
IX
X
II
VII VIIaIXarVIIa
NOAC reversal agents
Andexanet alpha is an investigational compound under development and has not been approved for use
1. Adapted from Greinacher A et al. Thromb Haemost 2015;113:931–42;
2. Clinicaltrials.gov: NCT02104947; 3. Pollack CV et al. Thromb Haemost. 2015;114:198–205;
4. ClinicalTrials.gov Identifier: NCT02329327; 5. ClinicalTrials.gov Identifier: NCT02207257

NOAC reversal agents
Approved by
EMA/FDA
Widely
available
Phase IIIPatients requiring urgent
surgery/with major
bleeding; started
May 20142,3
Phase IIIPatients with
major bleeding;
started Jan 20154
Phase II
Phase II
Phase I
Phase I
Idarucizumab1
Target: dabigatran
Andexanet alfa(PRT064445)1
Target: FXa inhibitors
Andexanet alpha is an investigational compound under development and has not been approved for use
1. Adapted from Greinacher A et al. Thromb Haemost 2015;113:931–42;
2. Clinicaltrials.gov: NCT02104947; 3. Pollack CV et al. Thromb Haemost. 2015;114:198–205;
4. ClinicalTrials.gov Identifier: NCT02329327; 5. ClinicalTrials.gov Identifier: NCT02207257
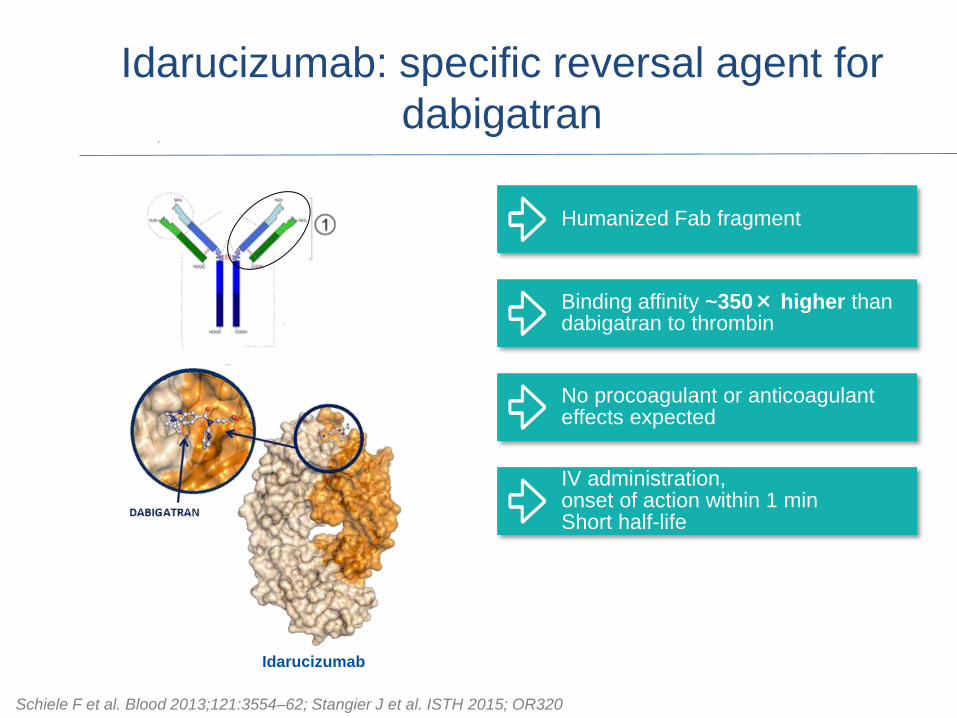
Schiele F et al. Blood 2013;121:3554–62; Stangier J et al. ISTH 2015; OR320
Idarucizumab: specific reversal agent for
dabigatran
Idarucizumab
Humanized Fab fragment
IV administration,onset of action within 1 minShort half-life
Binding affinity ~350× higher than dabigatran to thrombin
No procoagulant or anticoagulant effects expected

‘Normal upper reference limit’ refers to (mean+2 SD) of 86 predose measurements from a total of 51 subjects; AE, adverse event; dTT, diluted thrombin timeGlund et al. Lancet 2015
Idarucizumab showed immediate, complete, and
sustained reversal of dabigatran anticoagulation in a
healthy volunteer study
20
End of idarucizumab injection (5-min infusion)
Dabigatran etexilate
+ placebo
dT
T (
s)
70
65
60
55
50
45
40
35
30
Dabigatran Idarucizumab or placebo
Time after end of infusion (hrs)Minutes
72–2 0 120906030 36241264 8 10 48 60
Dabigatran etexilate plus:
Placebo (n=9)
Internal use only – strictly confidential
2 g idarucizumab (day 4) (n=9)
4 g idarucizumab (day 4) (n=8)

RE-VERSE AD: multicentre, open-label,
single-arm Phase III study
dTT, diluted thrombin time; ECT, ecarin clotting time
Pollack CV et al. Thromb Haemost 2015;114:198–205
Group A:
Uncontrolled bleeding
+ dabigatran-treated
Group B: Emergency
surgery or procedure*
+ dabigatran-treated
N=500
0–15 minutes 90 days follow-up
0–24 hours
Hospital
arrival
5 g idarucizumab
(two infusions of 2.5 g)
Pre-2nd vial 2 h 4 h 12 h 24 h 30 d 90 d1 h
Blood
samples10–30
min
Primary endpoint: dabigatran reversal within 4 hours
(dTT or ECT)
7 d
Reverses up to the
99th percentile of
dabigatran levels
measured in RE-LY

RE-VERSE AD interim results:
primary endpoint by dTT reversal
Assay
upper limit
of normal
Idarucizumab
2x 2.5 g
dT
T (
s)
130
110
70
60
50
40
30
20
120
100
90
80
1h 2h 4h 12h 24hBaseline Between
vials
10–30
min
Time post idarucizumab
Uncontrolled
bleeding
Interim analysis includes data for the first 90 patients.
Pollack CV et al. N Engl J Med 2015:373:511–20

Diluted Thrombin Time (dTT) – reversal of dabigatran
anticoagulation with idarucizumab
Pollack et al presented at AHA Nov 15, 2016
Similar results were also obtained with Ecarin Clotting Time (ECT)
30
40
50
60
70
80
90
100
110
dT
T(s
)
Baseline Between 10-30 1 h
vials min
2 h 4 h 12 h 24 h
Time post-idarucizumab
Idarucizumab
2 x 2.5 g
Uncontrolled bleeding
N = 298
110
Urgent Surgery
N = 196
Idarucizumab
2 x 2.5 g
30
40
50
60
70
80
90
100
dT
T(s
)
Baseline Between 10-30 1 h
vials min
2 h 4 h 12 h
Time post-idarucizumab
24 h
Assay
ULN
Median and 25th/75th percentiles 10th/90th percentiles 5th/95th percentiles

Urgent surgery: periprocedural haemostasis
• 191 of 196 (97.4%) patients
underwent surgery/procedures
• Median time from
administration to procedure
was 1.6 hours
• Adequacy of hemostasis during
surgery determined locally
Periprocedural haemostasis in 191 patients
Pollack et al presented at AHA Nov 15, 2016
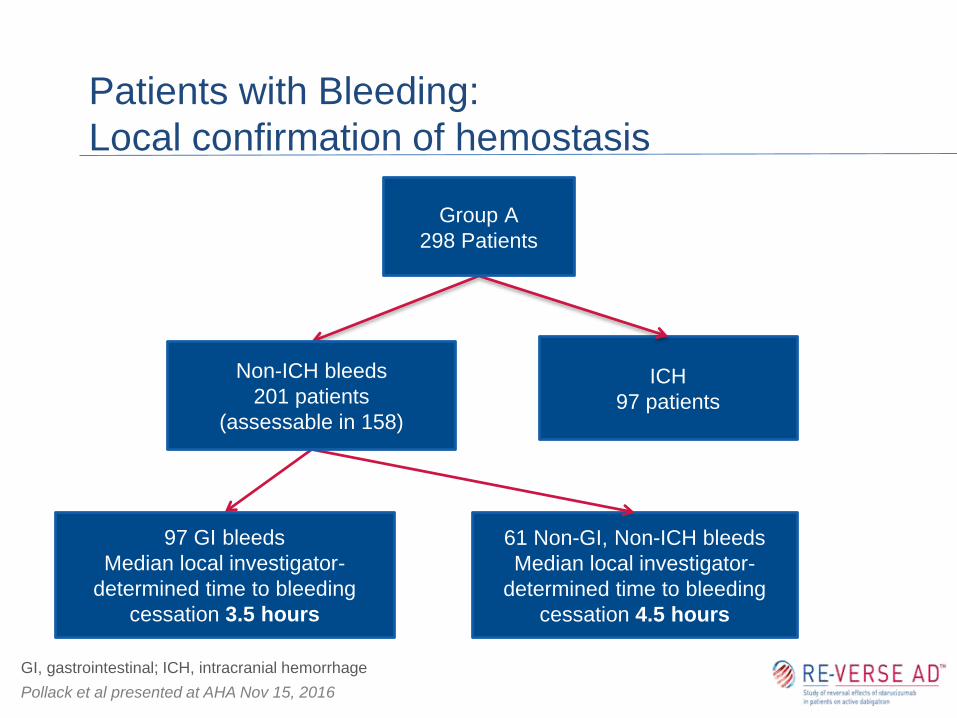
Patients with Bleeding:
Local confirmation of hemostasis
ICH
97 patients
97 GI bleeds
Median local investigator-
determined time to bleeding
cessation 3.5 hours
61 Non-GI, Non-ICH bleeds
Median local investigator-
determined time to bleeding
cessation 4.5 hours
Non-ICH bleeds
201 patients
(assessable in 158)
Group A
298 Patients
GI, gastrointestinal; ICH, intracranial hemorrhage
Pollack et al presented at AHA Nov 15, 2016

Idarucizumab reverses dabigatran in
emergencies
Interim analysis includes data for the first 90 patients.
Pollack CV et al. N Engl J Med 2015:373:511–20
Secondary clinical endpoints • cessation of bleeding *
• intraoperative haemostasis ‘normal’ in evaluable patients
A 5 g dose of idarucizumab resulted in immediate and complete
reversal of dabigatran anticoagulation in almost all patients
No idarucizumab-related safety concerns identified to date
in the interim analysis
27
NEJM, Aug 6th 2015

28
NEJM, Aug 6th 2015 NEJM, Sep 22nd 2016

Designed to Reverse Activity of direct and indirect
Factor Xa Inhibitors
Andexanet
Factor Xa andexanet
Catalytic DomainGla
S S
S419
S S
A419Factor Xa inhibitor Factor Xa inhibitor
• fXa decoy to bind molecules that target and inhibit fXa
• Np catalytic activity
Gla
Lu et al. Nat Med 2013

Andexanet: Reversal of Rivaroxaban
Siegal et al. NEJM 2015

ANNEXA-4: preliminary analysis
Apixaban (n=20) Rivaroxaban (n=26)
Connolly SJ, et al. NEJM 2016

• Be prepared!
Institutional protocols
Patient education
• Reversal agents: rarely needed but impact
on outcome
• Reassurance for patients and physicians
Compliance
Weitz et al. Circulation 2012; Majeed et al. Circulation 2013; Graham et al. Circulation 2015
Conclusions:
Emergencies in anticoagulated patients

What do the guidelines recommend?
• In case of life-threatening bleeding:
– Idarucizumab (dabigatran only)
– PCC (50 U/kg)
– aPCC (50–100 U/kg)
– rFVIIa (90 µg/kg)
No data about additional benefit
• In case of urgent surgery:
– Time
– Idarucizumab (dabigatran)
– PCCs 50 U/kg
Heidbuchel et al. Europace 2015

77y old man
Afib – NOAC
e-BIKE trauma
Expanding subdural hematoma
How would you manage?

76y old women
Afib - NOAC
Cholangitis – Choledocholithiasis
Acute renal insufficiency
How would you manage?

22 patients 9 bleeding / 13 urgent surgery
• ICH (intraparenchymal)
• Intoxication
• Gangrene Fournier
• ICH (subdural 3x)
• Cholangitis
• Acute mesentericischemia (2x)
• Dialysis
• Craniofacial trauma
• Lower GI bleeding
• Abscess drainage
• ‘Fausse route’ after
urinary catheter
• Open Tibial Fracture
• Visible vessel upper GI-
bleeding
• Haematemesis
• Hearttransplant (2x)
• Colon bleeding
• Urgent nephrostomy

• Pollack CV et al. N Engl J Med 2015
Reversal was also evident on aPTT results
Patients with bleeding Patients with urgent procedures
Pollack CV et al. N Engl J Med 2015:373:511–20


25-02-2017 11:42
Protrombinetijd (PT) * 25.3 s 9.4 - 12.5
Protrombinetijd (PT) * 35.0 % 70.0 - 150.0
Protrombinetijd (PT) 2.1 INR
APTT 34.9 s 25.1 - 36.5
25-02-2017 12:17
Rivaroxaban 440 ng/mL



Acute Situation in
Anticoagulated patients:
What are the options?
Peter Verhamme
Vascular Medicine and Haemostasis
Dept. of Cardioascular Medicine
University of Leuven

Evaluation of effect of the anticoagulant
• Routine coagulation assays
• FXa-inhibitors: Prothrombin Time (PT) Prolonged
suggests on-therapy levels (or above)
(riva > edo > apixaban)
Normaldoes not exclude on-therapy levels
high levels unlikely (riva > edo > apixaban)
Cuker, et al. JTT 2016

Evaluation of effect of the anticoagulant
• Routine coagulation assays
• Dabigatran: aPTTProlonged
suggests on-therapy levels (or above)
Normaldoes not exclude on-therapy
high levels unlikely
Cuker, et al. JTT 2016
