acute tonsillitis with concurrent kikuchi’s disease as a...
TRANSCRIPT
MJMS 16(4): 73
CASE REPORT
Acute Tonsillitis With Concurrent Kikuchi’s Disease as a Causeof Persistent Lymphadenopathy
Halimuddin Sawali1, Primuharsa Putra Sabir HuSin atHar2, Mazita ami1, Nor Hasni SHamSudin3, Gopalan nair4
1 Department of Otorhinolaryngology - Head & Neck Surgery, Universiti Kebangsaan Malaysia Medical Centre, Jalan Yaakob Latif, Bandar Tun Razak, 56000 Kuala Lumpur, Malaysia
2 Ear, Nose and Throat-Head and Neck Consultant Clinic, KPJ Seremban Specialist Hospital, 70200 Seremban, Negeri Sembilan, Malaysia
3 Department of Pathology, Tuanku Jaafar Hospital, Jalan Rasah, 70300 Seremban, Negeri Sembilan, Malaysia4 Ear, Nose,Throat-Head and Neck Consultant Clinic, Lam Wah Ee Hospital, 141 Jalan Tan Sri Teh Ewe Lim, 11600 Penang,
Malaysia
Submitted: 18 Feb 2009 Accepted: 30 Aug 2009
Abstract
We present a young adult female with symptoms of acute tonsillitis and tender cervicallymphadenopathy. Despite a full course of oral antibiotics, she had persistent left lower cervicallymphadenopathy measuring 2.0 x 1.5 cm at 2 weeks post-treatment. Rigid and flexible scopeexaminations did not reveal any abnormalities in the nasopharynx, oropharynx or hypopharynx.Tuberculosistestswerenegativeandbloodindexresultswerenormal.Fineneedleaspirationcytologyrevealed a non-specific granulomatous inflammatory process. Excisional lymph node biopsy wasperformed,andthepatientwasdiagnosedashavingKikuchi’sDisease(KD).WewouldliketohighlightthediagnosticchallengesindetectingthisconditionandtheimportanceofdifferentiatingKDfromtuberculosisandmalignantlymphoma,thelatterofwhichrequiresaggressivetreatment.
Keywords:histiocytic necrotizing lymphadenitis, Kikuchi disease, Kikuchi-Fujimoto disease, medical sciences
Introduction
Kikuchi-Fujimoto disease (histiocyticnecrotizinglymphadenitis)isabenign,self-limiteddisease of unknown cause that often manifestswith persistently enlarged cervical lymph nodesthat are unresponsive to antibiotic therapy (1).The disease was first identified by Kikuchi in1972; this condition is primarily seen in youngadult women, frequently of Asian origin, and isbecoming increasingly recognized worldwide (2).The incidence of Kikuchi’s disease (KD) rangesfrom3% to9%of allbiopsy casesofneck lymphnodes(3).Approximately30%ofKDpatientsaremistakenlythoughttohavemalignantlymphoma.Therefore, it is important for clinicians andpathologiststobeawareofthisbenign,self-limitingentity and to differentiate it fromnon-Hodgkin’slymphoma, systemic lupus erythematosus (SLE),andcarcinoma.
Case Report
A 22-year-old female presented with a five-dayhistoryofsorethroatandfeverwithbilateralcervical lymph lymphadenopathy. Examinationrevealed a high fever of 38.5 °C,mildly enlargedinflamed tonsils and bilateral tender cervicallymphadenopathy.Shewastreatedwithacourseofantibioticsforaweek.Sherecoveredwellexceptforapersistentmobileleftlowercervicallymphnodemeasuring2.0x1.5cm,whichdidnotregressevenat2weekspost-treatment.Therewereneitherotherlymphadenopathiesnorhepatosplenomegaly. Investigations for tuberculosis (TB) werenegative. White cell counts were normal. Fineneedle aspiration cytology (FNAC) of the lymphnode was suggestive of an acute granulomatousinflammatory process. Rigid nasal endoscopyand flexible nasopharyngolaryngoscopy did notreveal any abnormality in the nasopharynx or
CASE REPORT - Kikuchi’s disease Malaysian Journal of Medical Sciences, Vol. 16, No. 4, Pg 73-76, October - December 2009

MJMS 16(4): 74
Malaysian Journal of Medical Sciences, Vol. 16, No. 4, October - December 2009
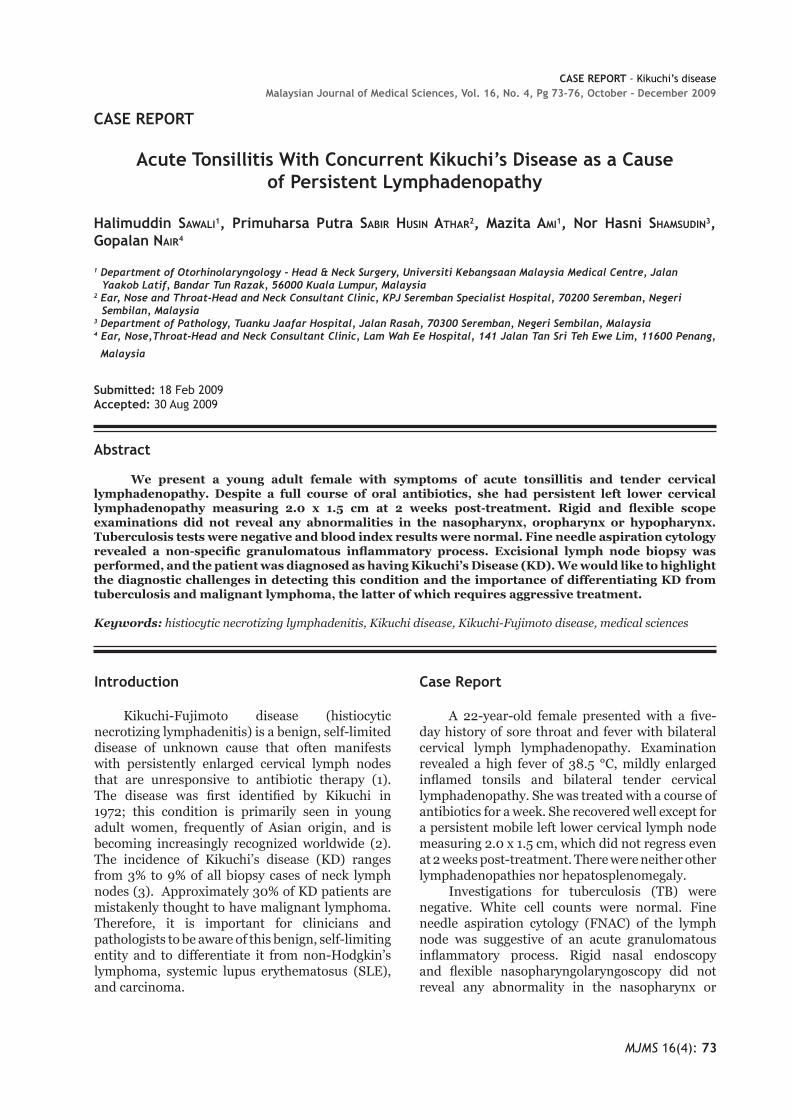
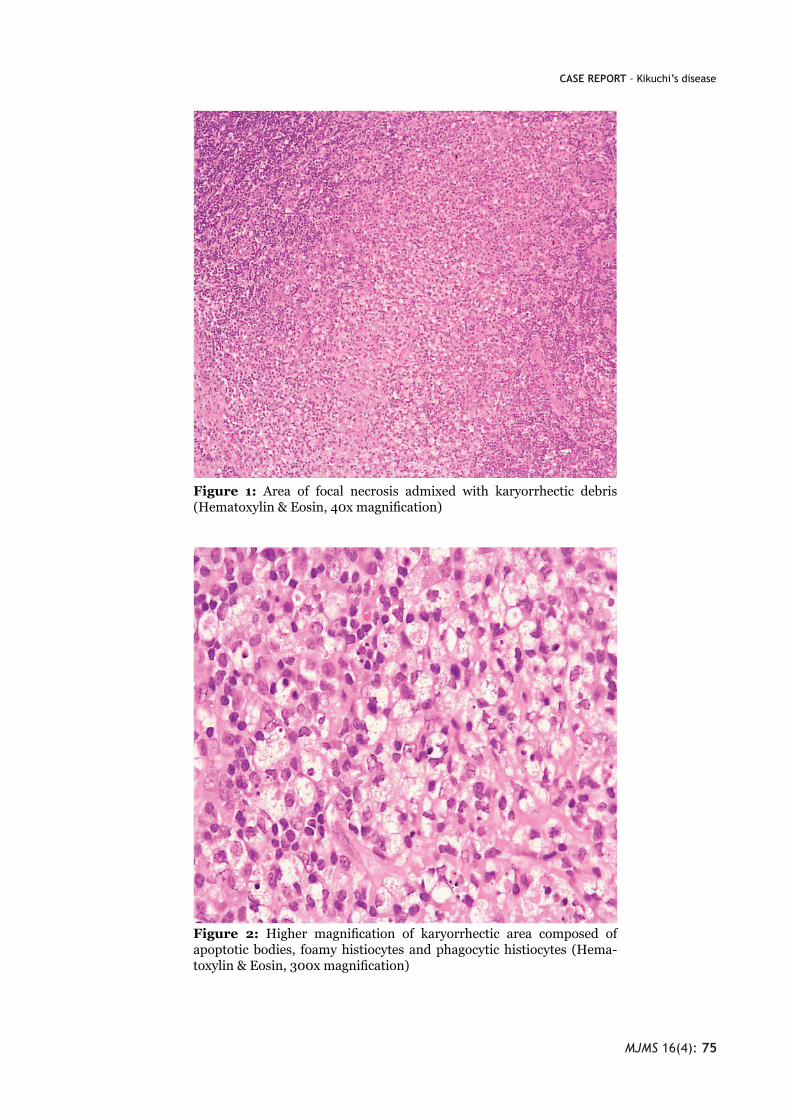
hypopharynx. An excisional lymph node biopsywasperformedandhistopathologicalexaminationreportedKD(Figure1andFigure2).Furtherbloodinvestigations for connective tissue screening(antinuclear antibody, rheumatoid factor) werenegative.Levelsof complementsC3andC4werealso normal. The patient recovered well afterexcisional biopsy of the lymph node. It has been8monthssincethesurgeryandtherehasbeennorecurrence.
Discussion
DiagnosisofKD iseasilymissedandreadilyunderdiagnosed. It is more common thanpreviouslythought(4).Menasceetal.(5)performedastudyinUKthatreportedthatKDisstillapoorlyrecognizedentityand is frequentlyconfusedwithmalignantlymphoma.Theyre-examined27lymphnodebiopsiesfrom25patientswhowerediagnosedwithKD.Only threecasesshowedthat the initialpathological diagnosis was Kikuchi disease; themost common suggested diagnosis was non-Hodgkin’slymphoma(5).DiagnosisofKDisrarelymade as a provisional diagnosis until all otherpossiblecausesofcervicallymphadenopathyhavebeenruledout,especiallyinSouthEastAsiaregion,where tuberculosis is endemic. In most cases,persistenceof lymphadenopathyaftercompletionof antibiotics will raise suspicion of this disease,whichcanonlybeconfirmedbyhistopathologicalexamination. In this case report, KD is an incidentalfinding. Even though both acute tonsillitis andKD can present with cervical lymphadenitis, thepresence of sore throat with inflamed tonsilsfavourthediagnosisofacutetonsillitisduringtheinitialpresentation.Acutetonsillitiswouldusuallyrespondtoacourseofantibiotics,whichisnotthecase forKD.Therefore, in this case,wepostulatethatKDoccurredconcurrentlywithtonsillitis. Histologically,KDmustbedifferentiatedfromnon-Hodgkin’slymphoma,SLEandcarcinoma.Itis very important to differentiate between thesediseases because the treatment regimen andprognosisarespecifictoeachcondition.BasedonthehistologyofKikuchidisease, itcanbe furtherdivided into four subtypes: lymphohistiocytictype, phagocytic type, necrotic type and foamycell type. Kikuchi et al. (2004) reported thatlymphohistiocytic and phagocytic are the morecommon types, which constitutemore than 80%of cases; the other two types are occasionallyencountered. The symptom of high-grade fevergreaterthan39oCiscommonlyseenincasesofthenecrotictype(6).
The typical pathology of KD permitsdifferentiationfromlymphoma,SLE,andinfectivelymphadenopathies (7). The classic morphologyof KD includes patchy lymph node involvementcentred in paracortical areas, extensive fibrinoidnecrosis, absenceofgranulomatous reaction,andfoamy histiocytes at the margins of the necroticareas.Plasmacellsarerarelynotedandabundantpredominantly extracellular apoptosis debris ispresent (8). Typical features of infiltration byblasts and histiocytes with extensive necrosis orkaryorrhexis are shared with other conditions,such as malignant lymphoma, tuberculosis, andSLE(9). The features that distinguish lymphomafrom KD include the presence of cytologicallyblandhistiocytes,absenceofaprominent“starry-sky” appearance, presence of predominantlyextracellular“nucleardust,”absenceofneutrophils,eosinophils,andplasmacells inareasofnecrosisand a predominance of T immunoblasts. Reed-Stenberg cells are also not a feature of KD.Pertainingtoimmunohistochemicalstudies,CD68highlightscrescentichistiocytesandplasmacytoidmonocytes, unlike non-Hodgkin lymphoma,in which it shows sheets of B or T cells. In KD,immunoblastsarenegative forCD15andpositiveforLCA(CD45)(8). Histologic featuresofSLElymphadenopathymay not be distinguishable on a morphologicor immunophenotypic basis alone. Presence ofnumerousplasmacells,DNAdepositiononvesselwalls and extensive areas of acellular coagulativenecrosis devoid of karyorrhectic material wouldfavour thediagnosisofSLE(8).EventhoughKDisrarelyassociatedwithSLE,butitsdiagnosiscanprecede, postdate or coincide with SLE becauselymphadenopathy is a common presentationin both conditions and histologically may beindistinguishablebetweenthem(10). Although the aetiology of KD is unknownat present, it has long been speculated to be ofautoimmuneorinfectiousorigin(2).PossiblelinksbetweenKDandsystemiclupuserythematosusanda nonspecific hyperimmune reaction to a varietyof infections, chemical, physical, and neoplasticagentshasalsobeenproposedforitspathogenesis.As in this case, the young female patient hadpresented with typical symptoms of an upperrespiratory tract infection that resolvedwith oralantibiotics;however,theleftlowercervicallymphnode remainedpersistent.Further investigations,which included FNAC of the node, TB work-upandflexiblescopeexaminationofthenasopharynxandhypopharynxdidnot lead toany conclusion.Excisionbiopsyofthenodehadtobecarriedoutto
MJMS 16(4): 75
CASE REPORT - Kikuchi’s disease
Figure 1: Area of focal necrosis admixed with karyorrhectic debris(Hematoxylin&Eosin,40xmagnification)
Figure 2: Higher magnification of karyorrhectic area composed ofapoptoticbodies, foamyhistiocytes andphagocytichistiocytes (Hema-toxylin&Eosin,300xmagnification)
MJMS 16(4): 76
Malaysian Journal of Medical Sciences, Vol. 16, No. 4, October - December 2009
establishaKDdiagnosisforthispatient. KD is a self-limiting disease; thelymphadenopathy slowly resolves after a fewmonths. Prognosis is excellent, but about 3% ofpatients show recurrence of the disease withinseveral years; one study reports this number tobe2%to5%ofcases (3).Someauthorsadvocatethe use of corticosteroids and reported fasterhealing responses in terms of lymphadenopathydisappearance. Meanwhile, other conditionsthat share similar clinical presentations, such asmalignantlymphoma,SLEandtuberculosis,havespecific,aggressiveandprolongedtreatments.
Conclusion
KD, although rare, has become a morerecognized condition since it has been reportednot only in Asia, but around the world as well.This diagnosis should be seriously considered,especially in patients presenting with fever andpersistent cervical lymphadenopathy. Includingthis disease as a differential diagnosis whenhistopathological examination is requested willimprove early detection.By identifyingKDearly,expensive and extensive investigations that mayleadtounnecessarytreatmentscanbeavoided.
Author’s contributions
Conceptionanddesign:MAProvisionofstudymaterialsorpatients:GNCollectionandassemblyofdata,draftingofthearticle:HSDataanalysisandinterpretation:NHSCriticalrevisionofthearticle:MA,PPSHAFinalapprovalofthearticle:PPSHA
Correspondence
DrPrimuharsaPutraBinSabirHusinAtharMD(UKM),MSurgORL-HNS(UKM),AM(Mal)ConsultantENT-Head&NeckSurgeonKPJSerembanSpecialistHospitalJalanToman1,KemayanSquareSeremban,NegeriSembilanMalaysiaTel:06-7677800ext139Fax:06-7653406Email:[email protected]
References
1. Norris AH, Krasinskas AM, Salhany KE, GluckmanSJ. Kikuchi-Fujimoto disease: a benign cause of feverand lymphadenopathy. Am J Med. 1996;101:401–405.
2. PileriS,KikuchiM,HelbronD,LennertK.Histiocyticnecrotizing lymphadenitis without granulocyticinfiltration. Virchows Arch A Pathol Anat Histol.1982;395:257–271.
3. Kikuchi M, Takeshita M, Eimoto T, Iwasaki H,Minamishima Y, Maeda Y. Histiocytic necrotizinglymphadenitis: clinicopathologic, immunologic, andHLAtypingstudy.In:HanaokaM,KadinME,MikataA,etal.editors.LymphoidMalignancy:ImmunologyandCytogenetics. New York: Field &Wood; 1990. p.251–257.
4. Ahmad Z. More on diagnosis and management ofKikuchi disease. J Clin Rheumatol. 2006;12(3):158–159.
5. Menasce LP, Benarjee SS, Edmondson D, HarrisM. Histiocytic necrotizing lymphadenitis (Kikuchi-Fujimoto disease): continuing diagnostic difficulties.Histopathology.1998;33(3):248–254.
6. Kikuchi M, Ohshima K. Cervical Lymphadenopathy,Fever and Leukopenia (Histiocytic-NecrotizingLymphadenitis or Kikuchi Disease). Pathol Case Rev.2004;9(5):199–205.
7. KlingerM, Danter J, Siegert R,Moubayed P. Kikuchilymphadenitis. A contribution to the differentialdiagnosisof cervical lymphnode swellingofunknownorigin.HNO.1995;43:253–256.
8. Onciu M, Medeiros LJ. Kikuchi-FujimotoLymphadenitis.Adv Anat Pathol.2003:10(4);204–211.
9. Mahadeva U, Allport T, Bain B, Chan WK.Haemophagocyticsyndromeandhistiocyticnecrotisinglymphadenitis(Kikuchi’sdisease).J Clin Pathol.2000;58(8):636–638.
10. Martinez-Vazquez C, Hughes G, Bordon J, Alonso-Alonso J, Anibarro-Garcia J, Redondo-Martinez E etal. Histiocytic necrotizing lymphadenitis, Kikuchi-Fujimoto’s disease, associated with systemic lupuserythemotosus.QJM.1997;90(8):531–533.