acute&diagnosis&and&treatment … kappa... · ib& lidocaine,&mexili9ne,&...
TRANSCRIPT

Acute Diagnosis and Treatment of Common Dysrhythmias
ACNP/PA Cri9cal Care Boot Camp Vanderbilt University Medical Center
September 9, 2014
Ariel Kappa RN, MSN, ACNP-‐BC
Objec9ves • Review
– Cardiac conduc9on cycle – EKG
• Dysrhythmia Diagnosis and Treatment – Characteris9cs – E9ology – Pharmacological Management
• Case Studies

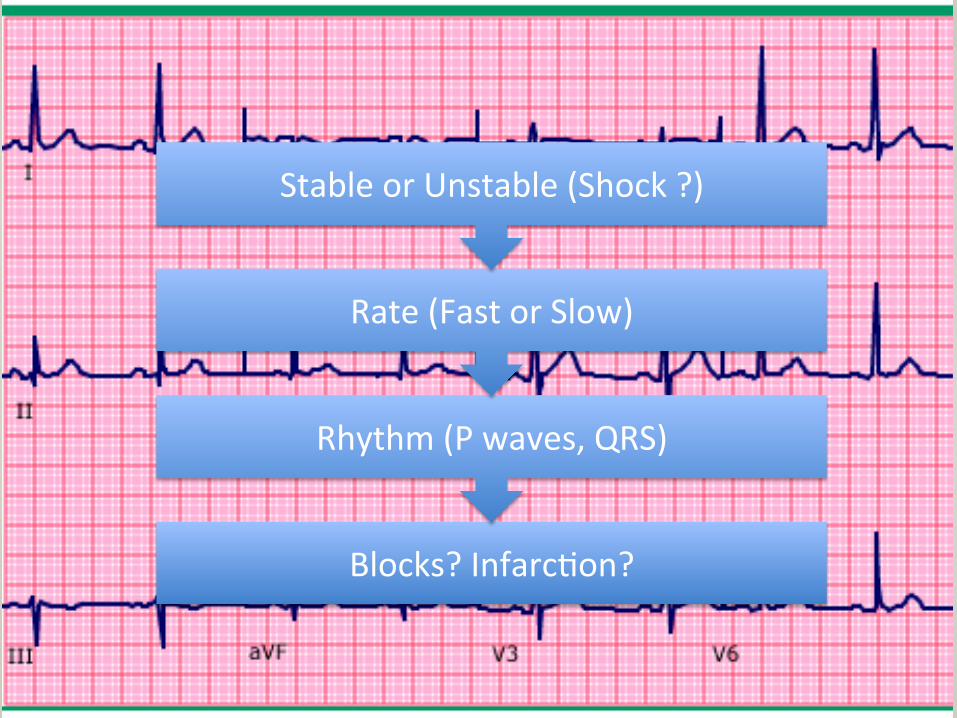
Blocks? Infarc9on?
Rhythm (P waves, QRS)
Rate (Fast or Slow)
Stable or Unstable (Shock ?)
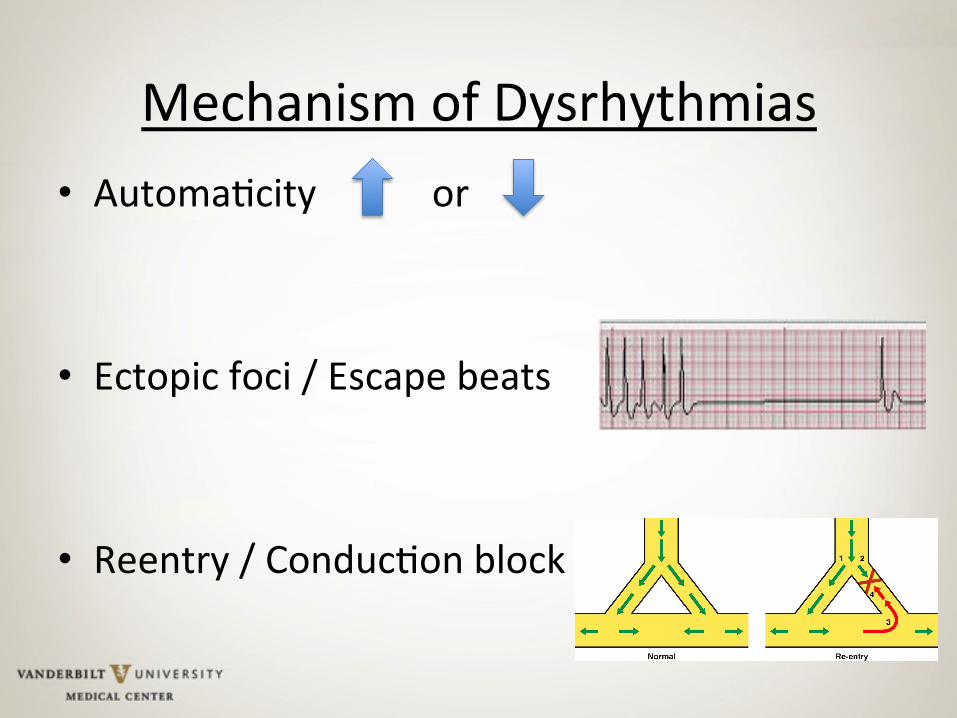
Mechanism of Dysrhythmias • Automa9city or
• Ectopic foci / Escape beats • Reentry / Conduc9on block
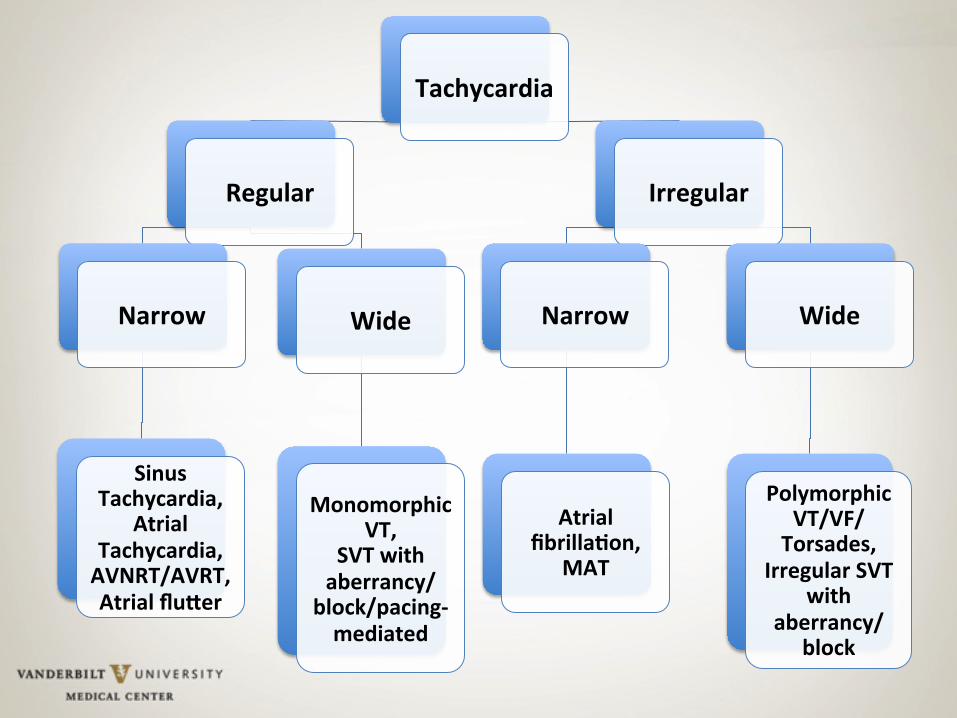
Tachycardia
Regular
Narrow
Sinus Tachycardia,
Atrial Tachycardia, AVNRT/AVRT, Atrial flu;er
Wide
Monomorphic VT,
SVT with aberrancy/
block/pacing-‐mediated
Irregular
Narrow
Atrial fibrillaEon,
MAT
Wide
Polymorphic VT/VF/ Torsades,
Irregular SVT with
aberrancy/block

Ini9al considera9ons • Stable?
– Hypotension, AMS, signs of shock, CP – 12-‐lead EKG
• Pharmacological management • Non-‐Pharmacological management
– Synchronized cardioversion (50-‐200 J) • Oxygen, airway, monitor, seda9on
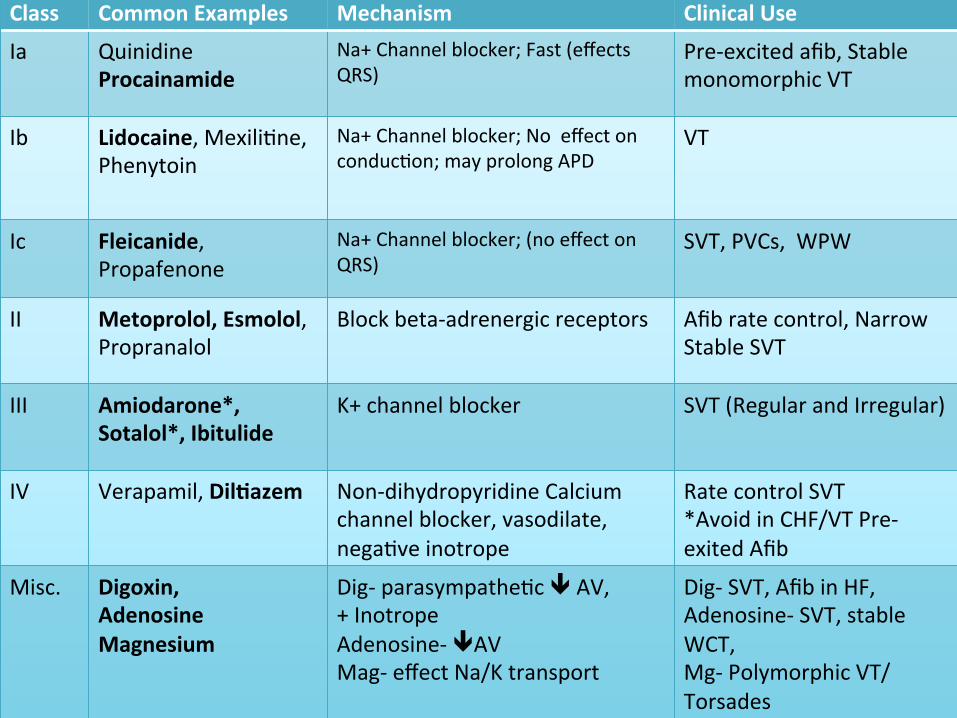
Pharmacology Class Common Examples Mechanism Clinical Use
Ia Quinidine Procainamide
Na+ Channel blocker; Fast (effects QRS)
Pre-‐excited afib, Stable monomorphic VT
Ib Lidocaine, Mexili9ne, Phenytoin
Na+ Channel blocker; No effect on conduc9on; may prolong APD
VT
Ic Fleicanide, Propafenone
Na+ Channel blocker; (no effect on QRS)
SVT, PVCs, WPW
II Metoprolol, Esmolol, Propranalol
Block beta-‐adrenergic receptors Afib rate control, Narrow Stable SVT
III Amiodarone*, Sotalol*, Ibitulide
K+ channel blocker SVT (Regular and Irregular)
IV Verapamil, DilEazem Non-‐dihydropyridine Calcium channel blocker, vasodilate, nega9ve inotrope
Rate control SVT *Avoid in CHF/VT Pre-‐exited Afib
Misc. Digoxin, Adenosine Magnesium
Dig-‐ parasympathe9c ê AV, + Inotrope Adenosine-‐ êAV Mag-‐ effect Na/K transport
Dig-‐ SVT, Afib in HF, Adenosine-‐ SVT, stable WCT, Mg-‐ Polymorphic VT/Torsades

Regular Narrow Complex
• Sinus Tachycardia • Atrial Tachycardia • Atrioventricular Nodal Tachycardia (AVNRT) • Atrioventricular Tachycardia (AVRT, Orthodromic)
• Atrial flueer
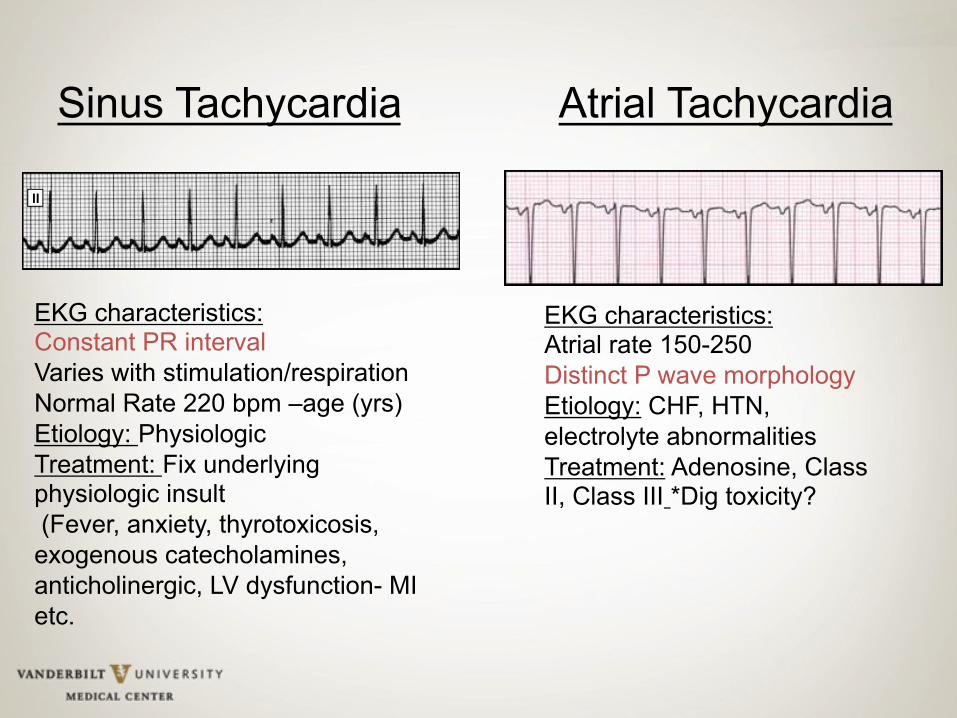
Sinus Tachycardia Atrial Tachycardia
EKG characteristics: Constant PR interval Varies with stimulation/respiration Normal Rate 220 bpm –age (yrs) Etiology: Physiologic Treatment: Fix underlying physiologic insult (Fever, anxiety, thyrotoxicosis, exogenous catecholamines, anticholinergic, LV dysfunction- MI etc.
EKG characteristics: Atrial rate 150-250 Distinct P wave morphology Etiology: CHF, HTN, electrolyte abnormalities Treatment: Adenosine, Class II, Class III *Dig toxicity?
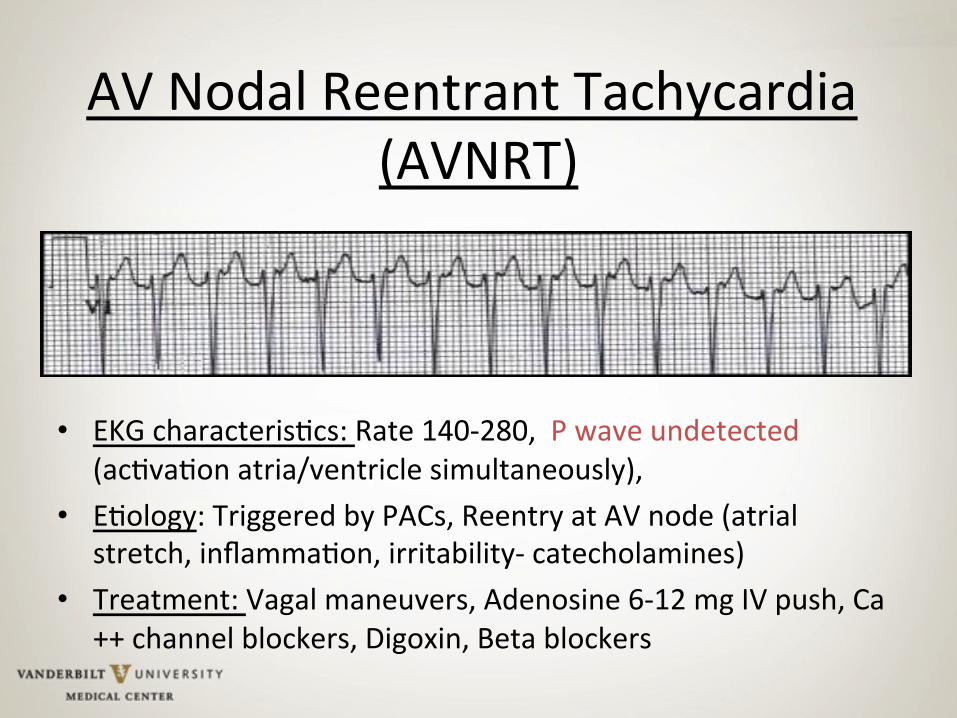
AV Nodal Reentrant Tachycardia (AVNRT)
• EKG characteris9cs: Rate 140-‐280, P wave undetected (ac9va9on atria/ventricle simultaneously),
• E9ology: Triggered by PACs, Reentry at AV node (atrial stretch, inflamma9on, irritability-‐ catecholamines)
• Treatment: Vagal maneuvers, Adenosine 6-‐12 mg IV push, Ca++ channel blockers, Digoxin, Beta blockers

AV Nodal Tachycardia (AVRT) or Orthodromic
• E9ology: Macroreentry through normal conduc9on system with accessory AV pathway; Delayed ac9va9on of atria = visible P wave
• Treatment: Similar to treatment of AVNRT, AV nodal blockers, eventual abla9on

Atrial Flueer
EKG Characteris9cs: ‘Sawtooth’ paeern: atrial rate ~300, ventricular rate 75-‐150 bpm (unless irregular). Usually with 2:1/4:1block at AV node. Rhythm constant amplitude, morphology, dura9on. **May be variable and irregular
E9ology: Reentrant circuit in the wall of the atrium
Treatment: Class III (Ibu9lide, sotalol, amiodarone): prolong refractory period (not slowing conduc9on) *Small risk for torsades. Ventricular rate control can be difficult, AV nodal blockers prevent 1:1 conduc9on. Unmasking of flueer waves with adenosine.
*Nonpharmacological : Rapid pacing or low voltage DC cardioversion is effec9ve.
Regular Wide Complex
• Ventricular Tachycardia (VT) • Wide complex SVT
– Bundle branch block – An9dromic-‐ Wolf-‐Parkinson-‐White (WPW) – Pacemaker-‐mediated

Monomorphic VT
EKG characteris9cs: 3 consecu9ve beats >100 bpm, QRS >120ms Brugada criteria: Precordial leads-‐ No RS complex or RS >100ms, AV dissocia9on, QRS morphology E9ology: CAD, CM, Ischemia Treatment: Correct aggrava9ng condi9ons (hypokalemia, ischemia) *Wide QRS presumed VT if unclear (LOE: C). *DCCV unstable (LOE: C). Class Ia: Procainamide-‐ careful in LV dysfunc9on, CHF, hypotension-‐ prolong QT. Class III-‐ Sotalol, Amiodarone (benefit IV to PO). Class IIb-‐ IV lidocaine ini9al treatment associated with MI (LOE: C).
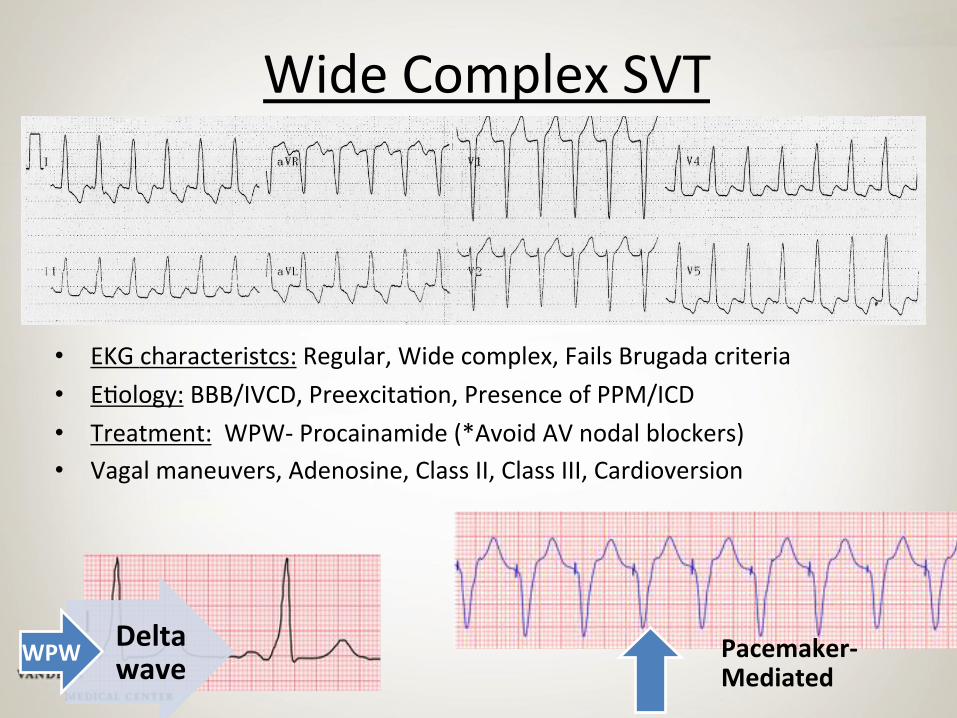
Wide Complex SVT
• EKG characteristcs: Regular, Wide complex, Fails Brugada criteria • E9ology: BBB/IVCD, Preexcita9on, Presence of PPM/ICD • Treatment: WPW-‐ Procainamide (*Avoid AV nodal blockers) • Vagal maneuvers, Adenosine, Class II, Class III, Cardioversion
Delta wave WPW Pacemaker-‐
Mediated
Irregular Narrow Complex
• Atrial fibrilla9on • MAT
• Sinus Tachycardia w/ Premature atrial contrac9ons (PACs)
• SVT with block

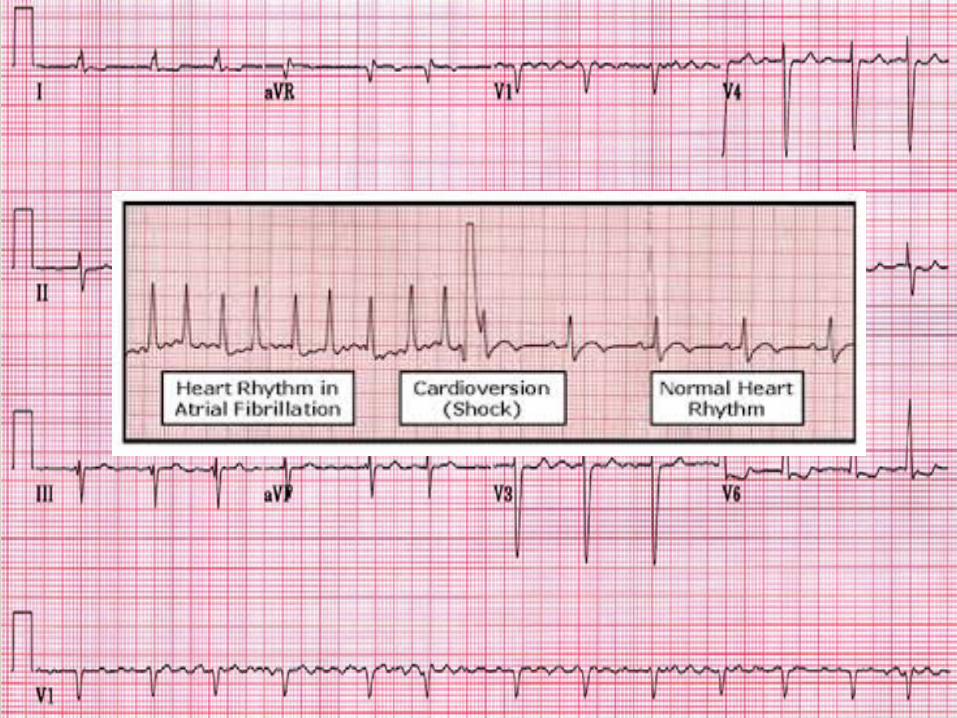
Atrial Fibrilla9on
EKG Characteris9cs: Irregularly Irregular.
E9ology: Numerous waves of depolariza9on spreading throughout the atria, leading to an absence of coordinated atrial contrac9on.
Treatment: Stable: rate control not rhythm control – AFFIRM trial (NEJM 2002). Class II, Class IV, Class III, Digoxin: HF (inotropic support). Unstable: Low voltage DC cardioversion
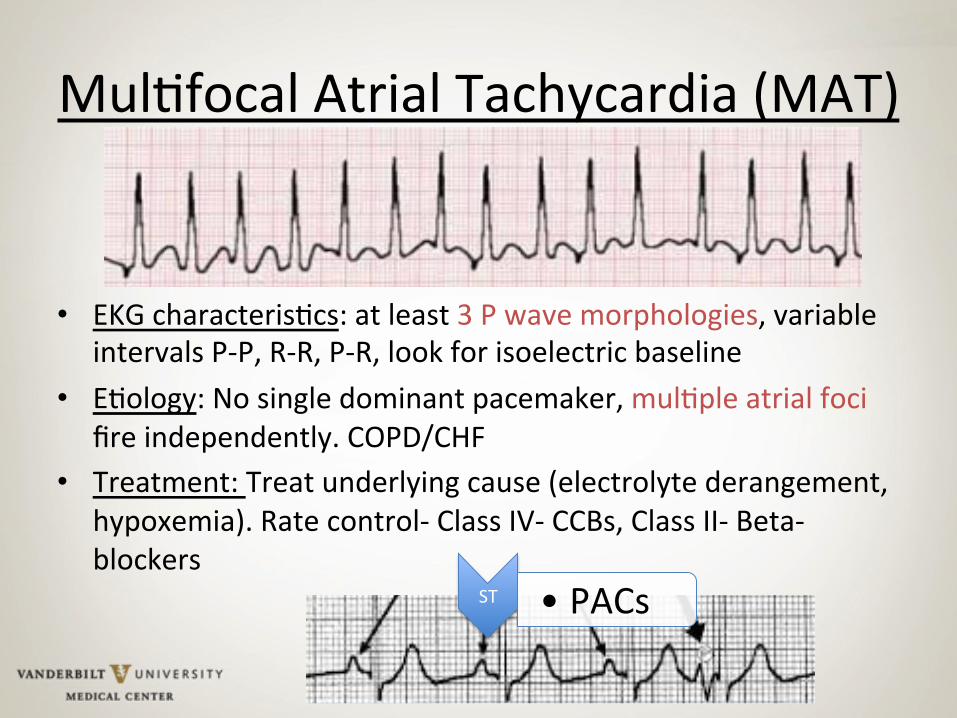
Mul9focal Atrial Tachycardia (MAT)
• EKG characteris9cs: at least 3 P wave morphologies, variable intervals P-‐P, R-‐R, P-‐R, look for isoelectric baseline
• E9ology: No single dominant pacemaker, mul9ple atrial foci fire independently. COPD/CHF
• Treatment: Treat underlying cause (electrolyte derangement, hypoxemia). Rate control-‐ Class IV-‐ CCBs, Class II-‐ Beta-‐blockers
ST • PACs

Irregular, Wide Complex • Polymorphic VT
– E9ology: Ischemia, Catecholamines – Treatment: Defibrilla9on
• Ventricular fibrilla9on, Torsades de pointes – E9ology-‐ QT prolonga9on, Class I, III-‐ prolong refractory period

Bradycardia
Regular
Sinus Bradycardia, Junc9onal Bradycardia, Idioventricular
escape rhythm, 1st Degree AV block, 3rd Degree AV
block
Irregular
2nd Degree Type I AV block, 2nd
Degree Type II AV block,

Ini9al considera9ons • Stable?
– Hypotension, AMS, Light-‐headedness,/syncope, angina
• Pharmacologic – Atropine (selec9ve muscarinic antagonist)
– Epinephrine, Dopamine
• Non-‐pharmacologic – Transcutaneous pacing > Transvenous – Expert consulta9on, PPM

Sinus Bradycardia
• EKG Characteris9cs: <60 bpm, normal P wave with PR <.20 prior to every narrow QRS
• E9ology: Normal variant, hypoxemia, Increased ICP, SSS, OSA, hypothermia, MI, Drugs
• Treatment: Symptoma9c? • CCB and Beta-‐blocker overdose-‐ IV calcium, glucagon
with or without insulin
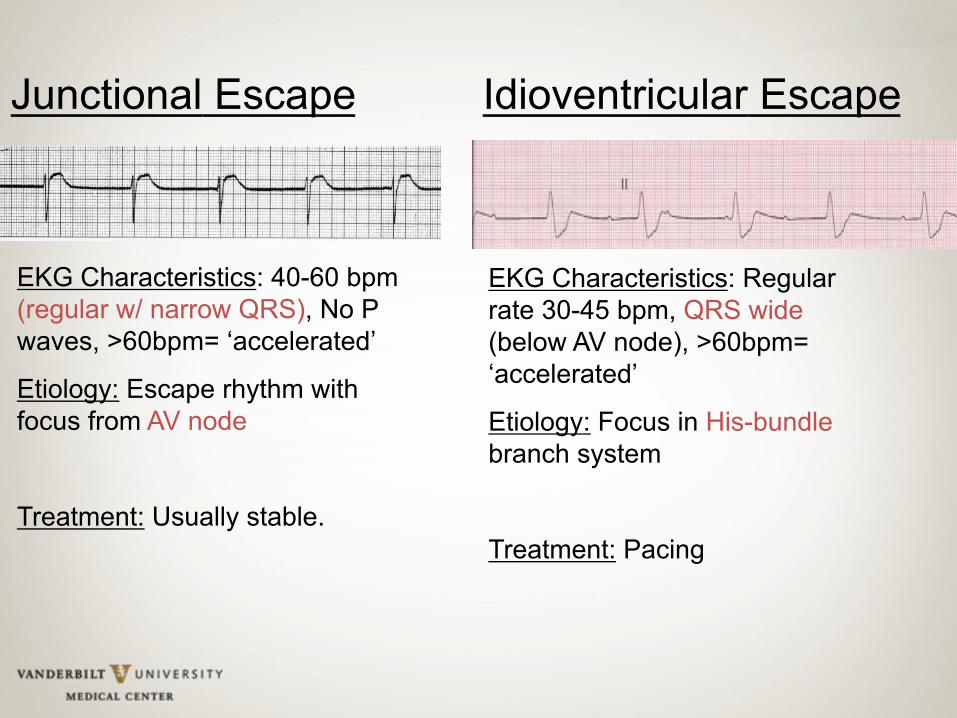
Junctional Escape Idioventricular Escape
EKG Characteristics: 40-60 bpm (regular w/ narrow QRS), No P waves, >60bpm= ‘accelerated’
Etiology: Escape rhythm with focus from AV node
Treatment: Usually stable.
EKG Characteristics: Regular rate 30-45 bpm, QRS wide (below AV node), >60bpm= ‘accelerated’
Etiology: Focus in His-bundle branch system
Treatment: Pacing
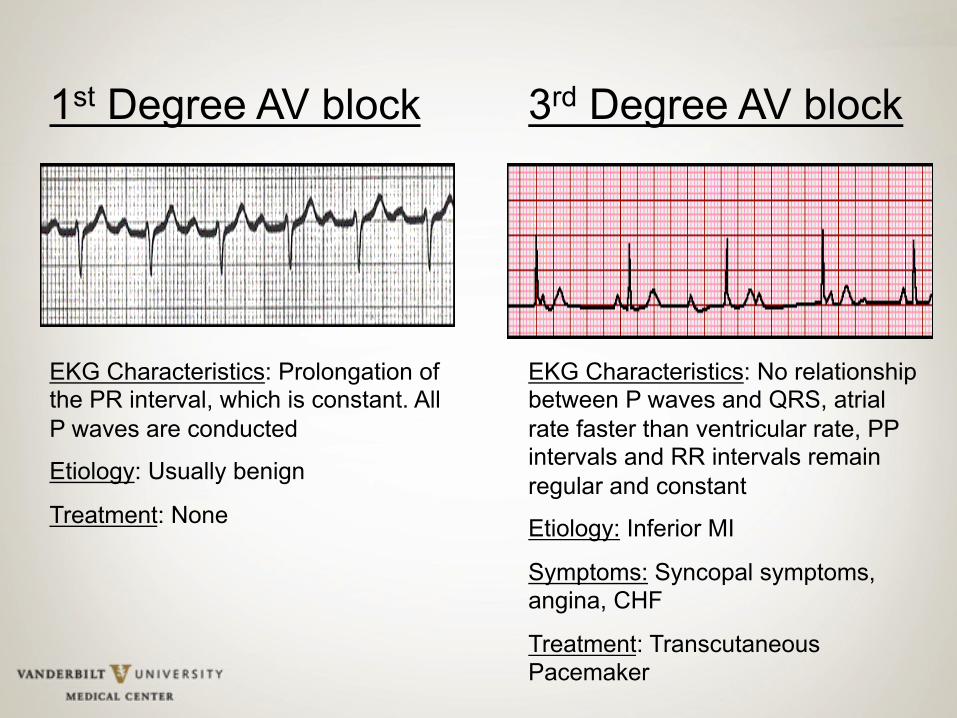
3rd Degree AV block
EKG Characteristics: No relationship between P waves and QRS, atrial rate faster than ventricular rate, PP intervals and RR intervals remain regular and constant
Etiology: Inferior MI
Symptoms: Syncopal symptoms, angina, CHF
Treatment: Transcutaneous Pacemaker
1st Degree AV block
EKG Characteristics: Prolongation of the PR interval, which is constant. All P waves are conducted
Etiology: Usually benign
Treatment: None

2nd Degree AV Block (Mobitz I, Wenckebach)
EKG Characteristics: Progressive prolongation of the PR interval until a P wave is not conducted. PR interval prolongs, the RR interval actually shortens, Narrow QRS.
Etiology: High AV nodal block. Usually benign unless associated with underlying pathology, i.e. Inferior MI, Toxicity (beta-blockers, CCBs).
2nd Degree AV Block (Mobitz II)
EKG Characteristics: Constant PR interval with intermittent failure to conduct. Rhythm is dangerous as the block is lower in the conduction system
Etiology: Infranodal His-Purkinje system conduction delay. Inferior/Anterior MI-fibrotic disease of the conduction system

Leu Bundle Branch Block
R-wave (R’) in V1, and a slurred S-wave in V5 - V6.
QS or rS complex in lead V1 and a monophasic or notched R wave in lead V6.
Etiology: CAD, HTN, CM, Aortic valve disease
Etiology: Congenital, MI, PE
Right Bundle Branch Block
Case Study # 1 • 78 yo female POD 3 s/p AVRt.
• Pa9ent c/o palpita9ons.
• Vitals HR: 160s, SBP: 119/65, SPO2: 95% 4 LNC
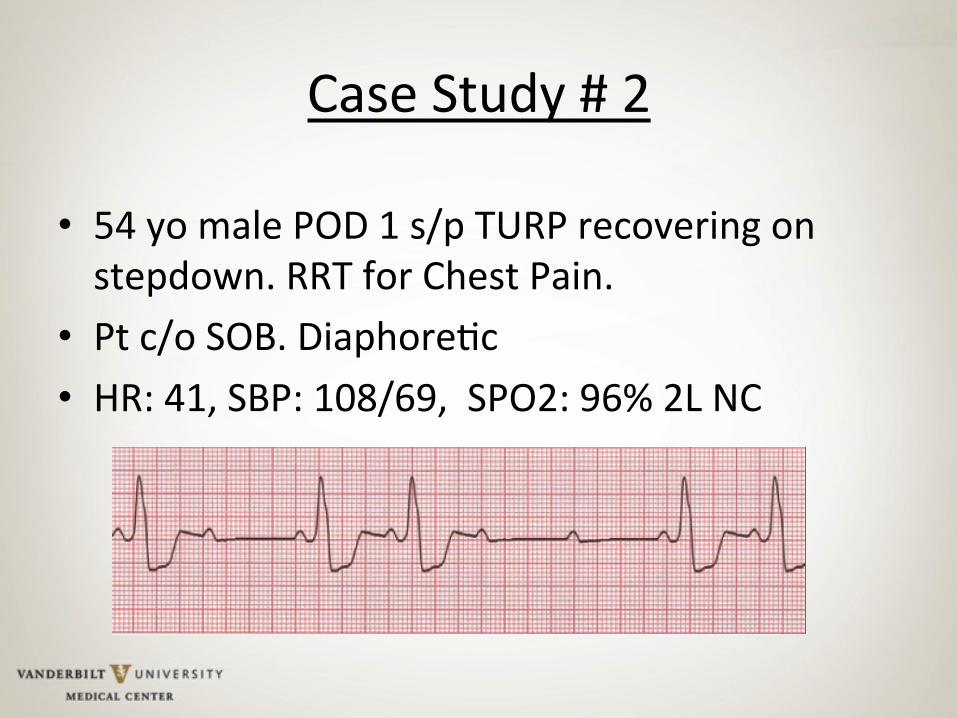
Case Study # 2
• 54 yo male POD 1 s/p TURP recovering on stepdown. RRT for Chest Pain.
• Pt c/o SOB. Diaphore9c • HR: 41, SBP: 108/69, SPO2: 96% 2L NC


Case Study # 3
44 yo male admieed to observa9on unit for SOB, dyspnea... HR 174, SBP 92/60, SPO2 94% NRB

References • The Atrial Fibrilla9on Follow-‐up Inves9ga9on of Rhythm Management (AFFIRM) Inves9gators . A comparison of
rate control and rhythm control in pa9ents with atrial fibrilla9on. New England Journal of Medicine. 2002, 347, 1825-‐1833.
• Carina Blomström-‐Lundqvist, Melvin M. Scheinman, E9enne M. Aliot, Joseph S. Alpert, Hugh Calkins, A. John
Camm…Hans-‐Joachim Trappe. CC/AHA/ESC Guidelines for the Management of Pa9ents With Supraventricular Arrhythmias−−Execu9ve Summary: A Report of the American College of Cardiology/American Heart Associa9on Task Force on Prac9ce Guidelines and the European Society of Cardiology Commieee for Prac9ce Guidelines (Wri9ng Commieee to Develop Guidelines for the Management of Pa9ents With Supraventricular Arrhythmias). Circula5on, 2003, 108:1871-‐1909. doi: 10.1161/01.CIR.0000091380.04100.84.
• Douglas P. Zipes, A. John Camm, Mar9n Borggrefe, Alfred E. Buxton, Bernard Chaitman, Mar9n Fromer…Cynthia Tracy. CC/AHA/ESC 2006 Guidelines for Management of Pa9ents With Ventricular Arrhythmias and the Preven9on of Sudden Cardiac Death: A Report of the American College of Cardiology/American Heart Associa9on Task Force and the European Society of Cardiology Commieee for Prac9ce Guidelines (Wri9ng Commieee to Develop Guidelines for Management of Pa9ents With Ventricular Arrhythmias and the Preven9on of Sudden Cardiac Death): Developed in Collabora9on With the European Heart Rhythm Associa9on and the Heart Rhythm Society. Circula5on, 2006, 114, e385-‐e484. doi: 10.1161/CIRCULATIONAHA.106.178233.
• Dubin, Dale. (2000). Rapid Interpreta9on of EKGs: Dr. Dubin’s classic simplified methodology for understanding EKGs, 6th Ed. Loca9on. C.o.v.e.r.
• ECC Guidelines. Part 6: Advanced Cardiovascular Life Support: Sec9on 5: Pharmacology I: Agents for Arrhythmias. Circula5on. 2000, 102, I-‐112-‐I-‐128. doi: 10.1161/01.CIR.102.suppl_1.I-‐112.
References Cont. • Fuster V, Ryden LE, Cannom DS, et al. 2011 ACCF/AHA/HRS focused updates incorporated into the ACC/AHA/ESC
2006 guidelines for the management of pa9ents with atrial fibrilla9on: a report of the American College of Cardiology Founda9on/ American Heart Associa9on Task Force on Prac9ce Guidelines. Circula5on. 2011, 123, e269-‐e367.
• Goodman S, Shiov T, Weissman C. Supraventricular arrhythmias in intensive care unit pa9ents: short and long-‐term consequences. Anesth Analg. 2007, 104:880-‐886.
• January CT, Wann LS, Alpert JS, Calkins H, Cleveland JC, Cigarroa JE, Con9 JB, Ellinor PT, Ezekowitz MD, Field ME, Murray KT, Sacco RL, Stevenson WG, Tchou PJ, Tracy CM, Yancy CW. 2014 AHA/ACC/HRS guideline for the management of pa9ents with atrial fibrilla9on: a report of the American College of Cardiology/American Heart Associa9on Task Force on Prac9ce Guidelines and the Heart Rhythm Society. Circula5on. 2014, 129, 1-‐56. DOI: 10.1161/CIR.0000000000000040.
• Delle Karth G, Geppert A, Neunteufl T , et al. Amiodarone versus dil9azem for rate control in cri9cally ill pa9ents with atrial tachyarrhythmias. Cri5cal Care Medicine. 2001, 29, 1149-‐1153.
• Robert W. Neumar, Chair; Charles W. Oeo; Mark S. Link; Steven L. Kronick; Michael Shuster; Cliuon W. Callaway…Laurie J. Morrison. Part 8: Adult Advanced Cardiovascular Life Support 2010 American Heart Associa9on Guidelines for Cardiopulmonary Resuscita9on and Emergency Cardiovascular Care. Circula5on 2010, 122, S729-‐S767. DOI: 10.1161/CIR.0b013e31820ff511.