addressing food allergies in schools...managing food allergies shared responsibility among schools,...
TRANSCRIPT
1
ADDRESSING FOOD ALLERGIES
IN SCHOOLS[PRESENTER, TITLE]
[ORGANIZATION]
[DATE]
2
SESSION OBJECTIVES
1.Develop an awareness of food
allergy basics
2.Learn why schools should address
food allergies
3.Understand the components of
food allergy policy
4.Learn about resources for policy
and practice
3
Food allergy is a potentially serious immune
response to eating or otherwise coming into
contact with certain foods or food additives.
A food allergy occurs when the immune system:
1) identifies a food protein as dangerous and
creates antibodies against it; and
2) tries to protect the body against the danger by
releasing substances, such as histamine, tryptase,
and others, into our blood when that food is
eaten.

4
FOOD ALLERGY VS. FOOD INTOLERANCE
Food allergy is a potentially serious immune
response to eating certain foods.
Food Intolerance is an adverse reaction to food
that does not involve the immune system and is
not life-threatening.
Example
Lactose intolerance
Trouble digesting milk sugar (lactose)
Symptoms
Might include abdominal cramps, bloating and
diarrhea
MD13

Slide 4
MD13 This slide should be in the introduction, possibly following slide 3?CDC, 5/17/2011
5
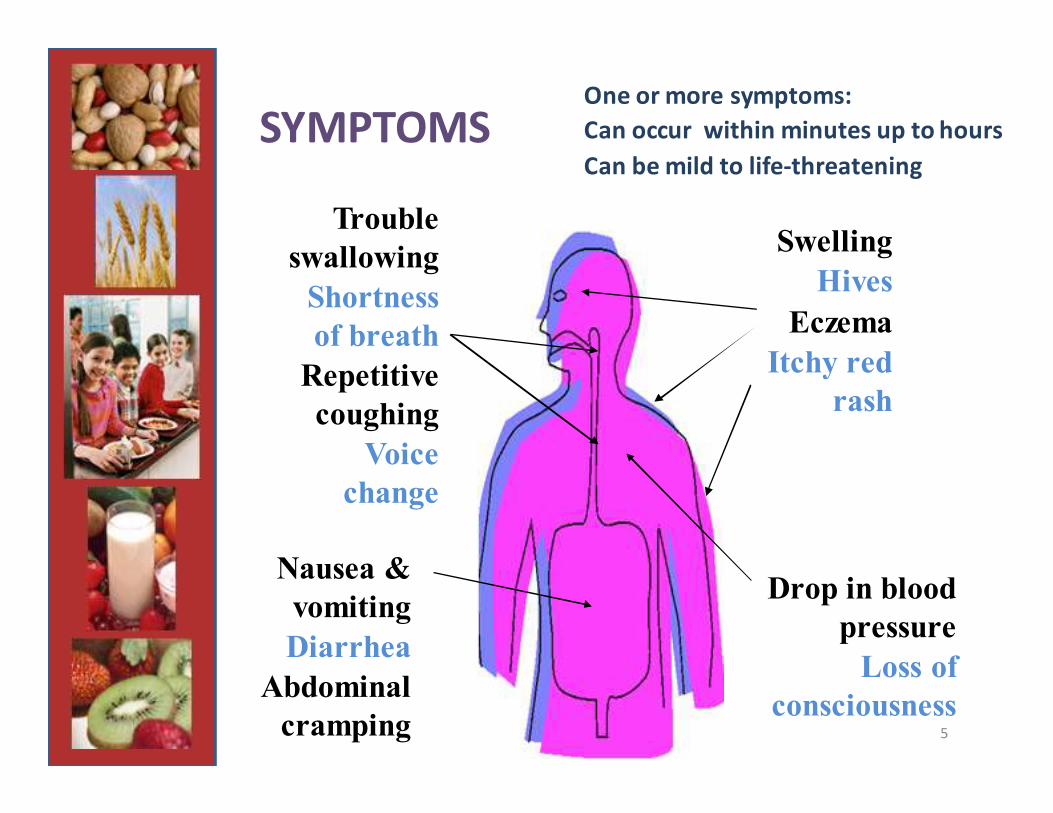
One or more symptoms:
Can occur within minutes up to hours
Can be mild to life-threatening
Trouble
swallowing
Shortness
of breath
Repetitive
coughing
Voice
change
Nausea &
vomiting
Diarrhea
Abdominal
cramping
Drop in blood
pressure
Loss of
consciousness
Swelling
Hives
Eczema
Itchy red
rash
SYMPTOMS

6
LIFE-THREATENING REACTION:
ANAPHYLAXIS
A serious allergic reaction that is rapid in
onset and may cause death
Food Insect Venom Medications Latex

7
TREATMENT OF ANAPHYLAXIS
• Epinephrine by injection is the treatment for a
serious reaction
• Quick administration is key – a delay can be
deadly
• Follow-up care and observation in the
emergency room for 4-6 hours
• Biphasic reactions occur about 20% of the time
(symptoms improve or disappear, then the 2nd
wave can be worse than the first)
8
WHY SHOULD SCHOOLS BE PREPARED
TO ADDRESS FOOD ALLERGIES?
• Responsibility for health and safety of children at
school
• Food allergy is the most common cause of
anaphylaxis.
• Need for immediate response
• Factor when dealing with other chronic conditions.
• Unique social and emotional challenges

9
WHY IS COMPREHENSIVE
FOOD ALLERGY POLICY NEEDED?
• Increased presence of students with food allergy; 18% increase (children under 18) 1997 –2007
• All students need to be safe and ready to learn– Teens are the highest risk group for fatal allergic reactions
• Emergencies are inevitable– Proactive approach rather than reactive
BZG4

Slide 9
BZG4 What is a digestive allergy? I don't think I've heard that term before.BZG, 4/25/2011
10
LAWS AND LIABILITY
• A life-threatening food allergy can be considered a disability under federal laws
– Rehabilitation Act of 1973, Section 504
– The Individuals with Disabilities Education Act (IDEA)
– The Americans with Disabilities Act (ADA), along with the ADA Amendments of 2008 (ADAA)
• Assure compliance for privacy and confidentiality
– Family Educational Rights and Privacy Act (FERPA) and
– Health Insurance Portability and Accountability Act of 1996 (HIPAA)
• Civil rights claim on behalf of student
– Follow the laws or parents/caregivers can file a claim
11
MANAGING FOOD ALLERGIES
Shared responsibility among schools, students,
families, and healthcare providers
Avoidance of food allergens
Being prepared in case of a reaction
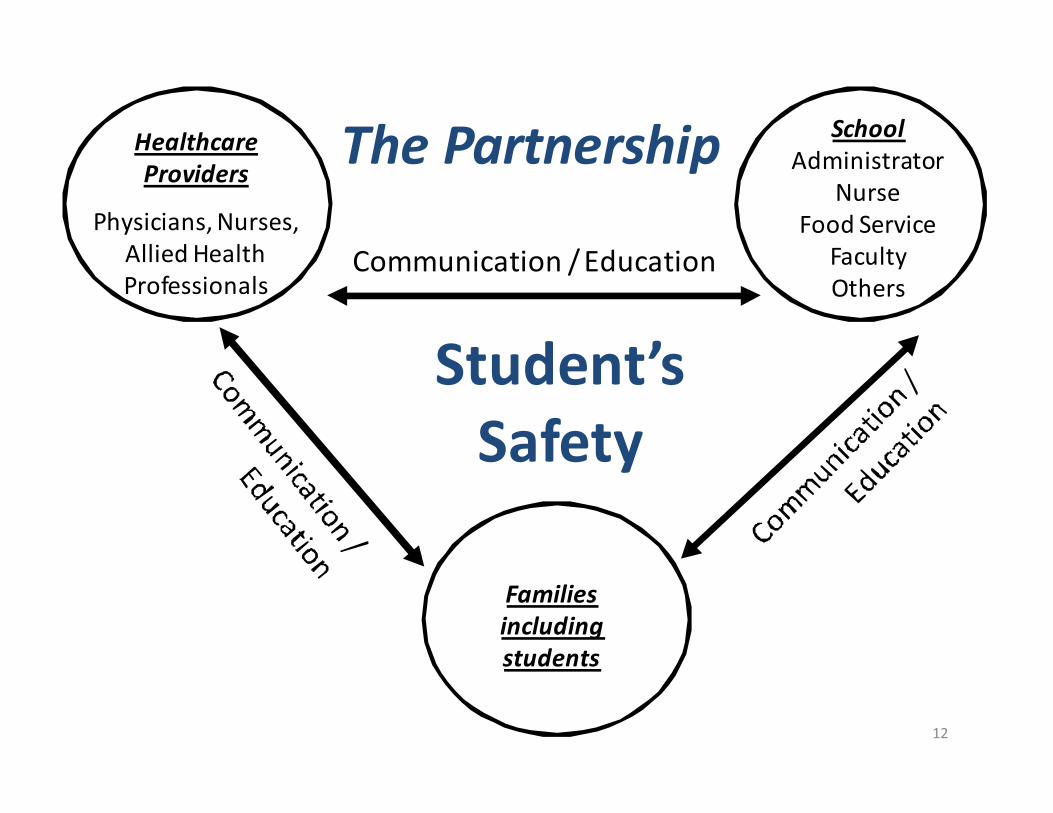
12
Student’s
Safety
Healthcare
Providers
Physicians, Nurses,
Allied Health
Professionals
School
Administrator
Nurse
Food Service
Faculty
Others
Families
including
students
The Partnership
Communication / Education
13
AVOIDANCE OF KNOWN
FOOD ALLERGENS
Eight (8) foods cause ninety (90) percent
of the food allergic reactions in the United
States:
Milk Peanuts
Eggs Tree Nuts
Wheat Fish
Soy Shellfish
14
REVIEW
What Questions
Come to Mind?
15
Comprehensive Policy Guidance:
Management of Life-Threatening Food
Allergies in Schools

SAFE AT SCHOOL AND READY TO LEARN:
10 POLICY COMPONENTS
1. Identification of students with food allergies and provision of
school health services
2. Individual written management plans
3. Medication protocols: storage, access, and administration
4. Healthy school environments: comprehensive and coordinated
approach
5. Communication and confidentiality
6. Emergency response
7. Professional development and training for school personnel
8. Awareness education for students
9. Awareness education and resources for parents/caregivers
10. Monitoring and evaluation
16

17
IDENTIFICATION OF STUDENTS WITH FOOD
ALLERGIES AND PROVISION OF SCHOOL
HEALTH SERVICES
• Identify students with food allergies
• Provisions of appropriate school health
services, including medication
administration
• Follow state and federal privacy and
confidentiality laws
18
INDIVIDUAL WRITTEN MANAGEMENT PLANS
• Individual Healthcare Plan (IHP or IHCP)
• Emergency Care Plan (ECP)
• Develop in collaboration with others
MD12
Slide 18
MD12 Last sentence in the notes section should read ..." A 504 plan is needed or required." CDC, 5/24/2011
19
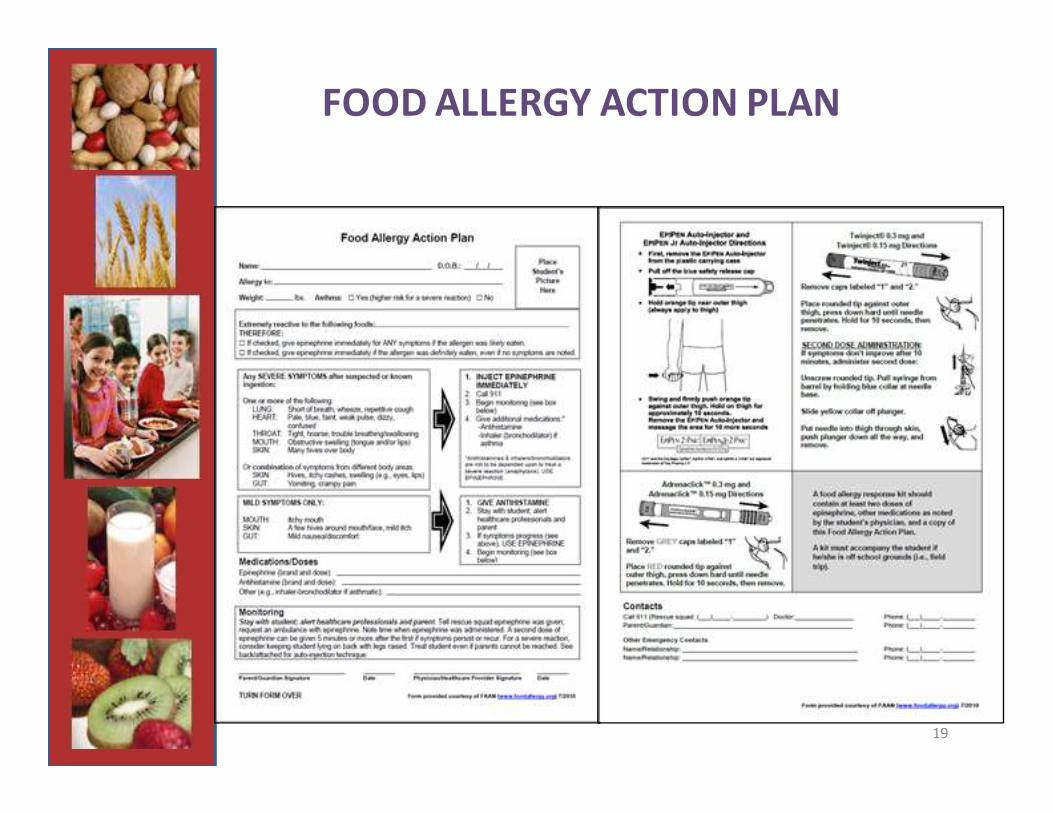
FOOD ALLERGY ACTION PLAN
20
MEDICATION PROTOCOLS: STORAGE,
ACCESS, AND ADMINISTRATION
• Allow for quick access
• Protect the safety of students and the
medications
• Follow state laws for storage, access, and
administration of medication
21
HEALTHY SCHOOL ENVIRONMENTS:
COMPREHENSIVE AND COORDINATED
APPROACH
Create a plan to manage food allergy
across the school system
• Classrooms
• Cafeteria
• Buses
• Field Trips
• Before/after school programs
• School sponsored events
22
COMMUNICATION AND CONFIDENTIALITY
• Comply with state and federal privacy and
confidentiality laws and accommodate parent
requests, as feasible
• Develop plans with the intent to inform all
personnel involved in the care of a student and
increase and enhance awareness of life-
threatening food allergies

23
EMERGENCY RESPONSE
• Food allergy as part of an “all-hazards
approach”
• Written emergency procedures for dealing with
a life-threatening food allergy reaction
- Assure rapid accessibility to epinephrine to prevent a
delayed response
• Roles and responsibilities
24
PROFESSIONAL DEVELOPMENT AND
TRAINING FOR SCHOOL PERSONNEL
• Check for compliance with policies and
procedures
• Provide annual training:
• District/school policies, procedures, and plans for
managing students with chronic health conditions
• Basic information such as signs, symptoms, and
risks associated with food allergy and anaphylaxis
• Strategies that reduce the risk of exposure to
identified allergens throughout the school day
25
AWARENESS EDUCATION FOR STUDENTS
• Educate all students on food allergy
• Incorporate food allergy awareness as part of
the district’s health education curriculum
• Provide annual education:• Support for classmates with chronic health conditions, such as food
allergy
• Knowledge of potential allergens and the signs, symptoms and
potential of a life-threatening reaction
• Importance of following district health and wellness policies and
relevant guidelines regarding hand washing, food-sharing, allergen-
safe zones, and student conduct.

26
A TOPIC NOT TO BE OVERLOOKED:
BULLYING
• Teasing or taunting for food allergy should never be allowed; bullying could come from students, teachers, staff, or parents
• For staff: Bullying prevention, including responsibility to address any harassment, hazing (e.g., forced consumption of the known allergen), or bullying and enforce consequences
• For students: Bullying prevention, including reporting any harassment, hazing or bullying to appropriate school personnel.
• School’s response to reported bullying should be made clear at the outset, should be followed through, and should be both therapeutic and punitive

27
AWARENESS EDUCATION AND RESOURCES
FOR PARENTS/CAREGIVERS
• Provide awareness education and resources
through use of qualified personnel. Increase
understanding of special needs of students
with food allergies.
• In-person education is desirable, but written
communications can also be effective
28
MONITORING AND EVALUATION
• Creating food allergy policy is a process that can be
modeled after CDC’s 6-Steps Framework
• Assess needs and review data
• Engage stakeholders
• Educate, practice and communicate about
policies and programs
• Focus the evaluation design
• Gather credible evidence and justify conclusions
• Implement needed changes and share lessons
learned
• Review and update policy and practices after an
incident of food allergic reaction and at least
annually

29
MONITORING AND EVALUATION
The guide’s policy component checklist:
• Systematic approach to managing food
allergies
• Gauges areas that need attention and
identifies specific actions for
improvement
• Tracks inclusion and implementation
of each element

30
MONITORING AND EVALUATION
Instructions for the policy component checklist:
• Check “Included” or “Not Included” for whether or
not each element is in the policy
• If the element is included in the policy, check
if the element has been “Implemented” or
“Not Implemented” in practice
• Use notes section to document specific actions for
improvement
Optimal: Each element is both “Included” and
“Implemented” at the district and school levels
31
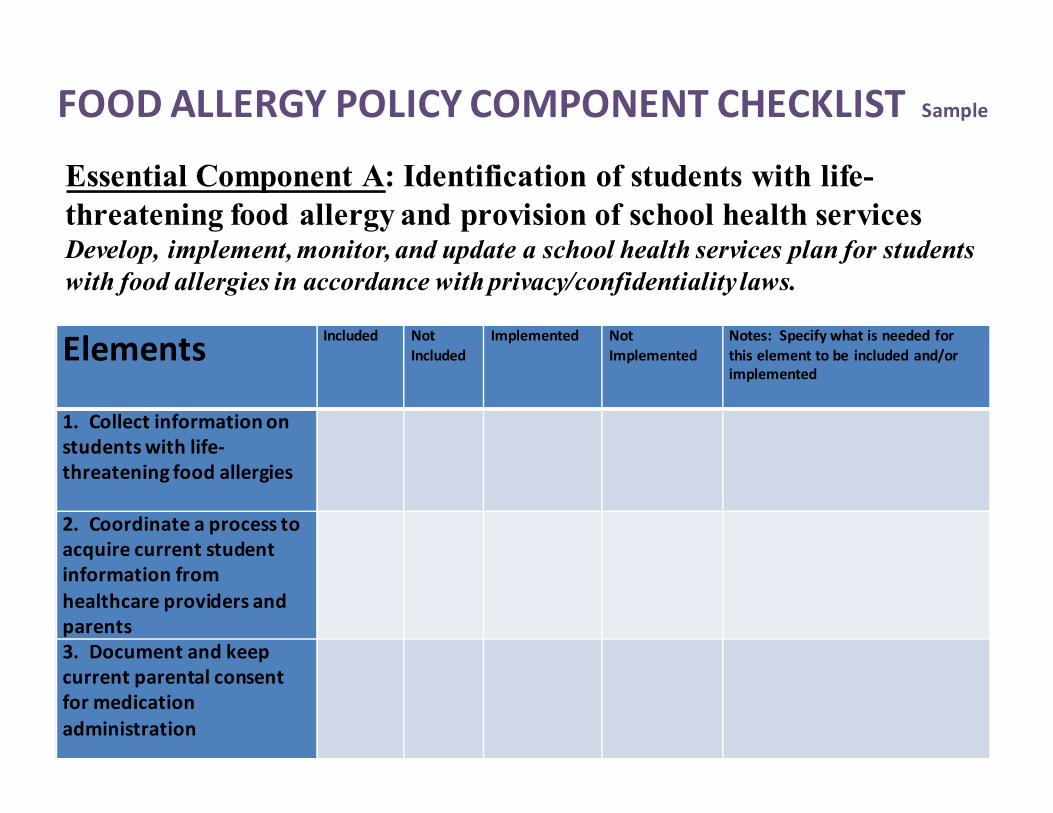
ElementsIncluded Not
Included
Implemented Not
Implemented
Notes: Specify what is needed for
this element to be included and/or
implemented
1. Collect information on
students with life-
threatening food allergies
2. Coordinate a process to
acquire current student
information from
healthcare providers and
parents
3. Document and keep
current parental consent
for medication
administration
Essential Component A: Identification of students with life-
threatening food allergy and provision of school health servicesDevelop, implement, monitor, and update a school health services plan for students
with food allergies in accordance with privacy/confidentiality laws.
FOOD ALLERGY POLICY COMPONENT CHECKLIST Sample
32
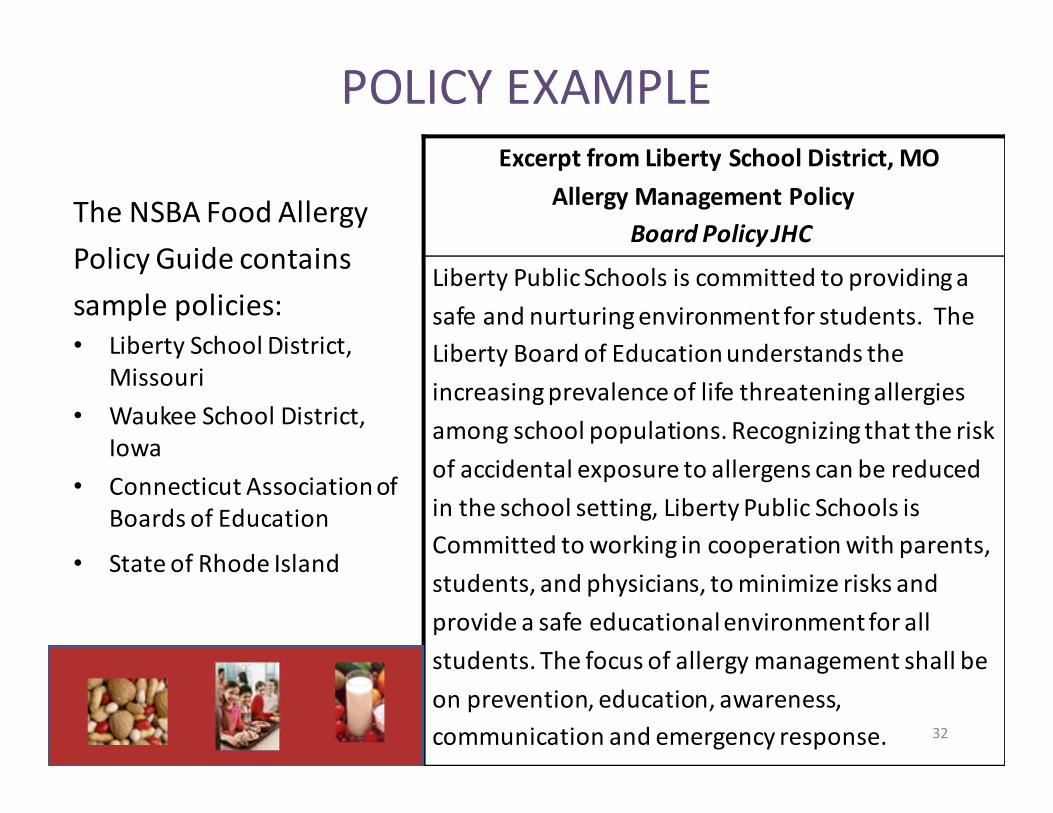
POLICY EXAMPLE
The NSBA Food Allergy
Policy Guide contains
sample policies:
• Liberty School District,
Missouri
• Waukee School District,
Iowa
• Connecticut Association of
Boards of Education
• State of Rhode Island
Excerpt from Liberty School District, MO
Allergy Management Policy
Board Policy JHC
Liberty Public Schools is committed to providing a
safe and nurturing environment for students. The
Liberty Board of Education understands the
increasing prevalence of life threatening allergies
among school populations. Recognizing that the risk
of accidental exposure to allergens can be reduced
in the school setting, Liberty Public Schools is
Committed to working in cooperation with parents,
students, and physicians, to minimize risks and
provide a safe educational environment for all
students. The focus of allergy management shall be
on prevention, education, awareness,
communication and emergency response.
33
REFERENCES
• American Academy of Allergy, Asthma, and Immunology (AAAAI) Board of Directors. (1998). Anaphylaxis in
schools and other child-care settings. Journal of Allergy and Clinical Immunology, 102, 173-176.
• Branum, A. M. & Lukacs, S. L. (2008). Food a llergy among U.S. children: Trends in prevalence and
hospitalizations. NCHS Data Brief (No. 10).
• Branum, A, M. & Lukacs, S.L. (2009). Food allergy among children in the United States. Pediatrics, 124, 1549-55.
• Bock, S.A., Muñoz-Furlong, A., & Sampson, H.A. (2007). Further fatalities due to anaphylactic reactions to food:
2001 to 2006. Journal of Allergy and Clinical Immunology, 119, 1016-1018.
• Centers for Disease Control and Prevention. (2009). Framework for program evaluation in public health. MMWR:
Recommendations and Reports. 48, 1-40. Retrieved from
http://www.cdc.gov/mmwr/preview/mmwrhtml/rr4811a1.htm
• Decker, W.W., Campbell, R.L., Manivannan, V., Luke, A., St Sauver, J.L., et a l. (2008). The etiology and incidence of
anaphylaxis in Rochester, Minnesota: A report from the Rochester Epidemiology Project. Journal of Allergy and
Clinical Immunology, 122, 1161-1165.
• Food Al lergy &Anaphylaxis Network (FAAN). (n.d.). Frequently asked questions. Retrieved from
http://www.foodallergy.org/questions.html
• Lieberman, J.A., Weiss, C., Furlong, T.J., Sicherer, M., Sicherer , S.H. (2010). Bullying among pediatric patients
with food allergy. Annals of Allergy, Asthma & Immunology, 105, 282-286.
• Massachusetts Department of Education. (2002). Managing life threatening food allergies in school. Retrieved
from http://www.doe.mass.edu/cnp/allergy.pdf
• National Association of School Nurses (NASN). (2010). Position s tatement: Delegation.
• NASN. (2004). Pos i tion statement: Rescue medications in school.

34
REFERENCES• New York State Department of Health, New York State Education Department, & New York Statewide School
Health Services Center. (2008). Making the difference: Caring for students with life-threatening food allergies.
• One Hundred Eleventh Congress of the United States of America. (2010). H.R. 2751: FDA Food Safety
Modernization Act. Retrieved from http://www.gpo.gov/fdsys/pkg/BILLS-111hr2751enr/pdf/BILLS-
111hr2751enr.pdf
• Rotrosen, D., & Fauci, A. (2008). Ra ising awareness of the personal and research challenges of
food a llergy. Retrieved from http://www3.niaid.nih.gov/news/newsreleases/2008/food_allergy08.htm
• Sheetz , A. H., Goldman, P. G., Mi l lett, K., Franks, J. C., McIntyre, C. L., Carrol l, C. R., et a l.,
(2004). Guidelines for managing life-threatening food allergies in Massachusetts schools. Journal of
School Health, 74, 155-160.
• Sicherer, S.H., Furlong, T.J., DeSimone, J., & Sampson, H.A. (2001). The U.S. peanut and tree
nut a l lergy registry: Characteristics of reactions in schools and child care. Journal of Pediatrics, 138, 560-565.
• Sicherer, S.H., Mahr, T., & the Section on Allergy and Immunology. (2010). Management of
food allergy in the school setting. Pediatrics, 126, 1232-1239.
• U.S. Department of Agriculture Food and Nutrition Service. (2001). Accommodating children with
special dietary needs in the school nutrition programs. Guidance for school food service staff.
Retrieved from http://www.fns.usda.gov/cnd/guidance/special_dietary_needs.pdf
• U.S. Department of Education. (2000). Office of Civil Rights memorandum regarding the prohibition
of disability harassment. Retrieved from http://www.ed.gov/about/offices/list/ocr/docs/disabharassltr.html
• U.S. Department of Education. (2007). Free appropriate public education for students with
disabilities: Requirements under Section 504 of the Rehabilitation Act of 1973. Retrieved from
http://www.ed.gov/about/offices/list/ocr/docs/edlite-FAPE504.html
• Young, M.C., Muñoz-Furlong, A., Sicherer, S.H. (2009). Management of food allergies in schools: A perspective
for a l lergists. Journal of Allergy and Clinical Immunology, 124, 175-182.
35
FOOD ALLERGY RESOURCES:
www.foodallergy.org
www.nasn.org
www.cdc.gov/healthyyouth/
National School Boards Association
Division of Adolescent and School Health (DASH)
www.nsba.org/schoolhealth
www.fns.usda.gov/cnd/guidance/special_dietary_needs.pdf

36
THANK YOU
WHAT QUESTIONS DO YOU
HAVE?
For more information contact:
National School Boards Association, School Health Programs703-838-6722
[email protected]/SchoolHealth