addressing the opioid crisis in ambulatory care -...
TRANSCRIPT

Addressing the Opioid Crisis in Ambulatory CareAlicia Agnoli MD MPH
Mary Ellen Benzik MD
Andrew Jorgensen MD
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Facilitated by Mara Laderman MSPH
L9These presenters have
nothing to disclose
April 21 2017930 AM ndash 1230 PM
Objectives
Understand the magnitude of the opioid crisis in the
United States
Describe different strategies to address multiple drivers
of the opioid crisis including physician prescribing
prescriber education treatment for opioid use disorder
and partnering with communities
Identify change ideas and strategies to overcome
barriers that they can test at their organization
Session Agenda
Faculty Introductions
Case Studies from three organizations (+ a break)
Table Top Discussions
Final QampA and wrap up
3
Faculty IntroductionsP4
5
New York Times httpwwwnytimescominteractive20160107usdrug-overdose-deaths-in-the-ushtml
Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Objectives
Understand the magnitude of the opioid crisis in the
United States
Describe different strategies to address multiple drivers
of the opioid crisis including physician prescribing
prescriber education treatment for opioid use disorder
and partnering with communities
Identify change ideas and strategies to overcome
barriers that they can test at their organization
Session Agenda
Faculty Introductions
Case Studies from three organizations (+ a break)
Table Top Discussions
Final QampA and wrap up
3
Faculty IntroductionsP4
5
New York Times httpwwwnytimescominteractive20160107usdrug-overdose-deaths-in-the-ushtml
Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Session Agenda
Faculty Introductions
Case Studies from three organizations (+ a break)
Table Top Discussions
Final QampA and wrap up
3
Faculty IntroductionsP4
5
New York Times httpwwwnytimescominteractive20160107usdrug-overdose-deaths-in-the-ushtml
Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Faculty IntroductionsP4
5
New York Times httpwwwnytimescominteractive20160107usdrug-overdose-deaths-in-the-ushtml
Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

5
New York Times httpwwwnytimescominteractive20160107usdrug-overdose-deaths-in-the-ushtml
Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Driver Diagram Addressing the opioid crisis in a
community
6
Address the opioid crisis in a
communityMeasuresbull Overdose ratebull Fatal overdose ratebull Individuals in treatmentbull Prescription opioid rate
Limit supply of opioids
Identify and manage opioid
dependent population
Treat individuals with opioid use
disorder
bull Prescribing practicesbull Dispensing practicesbull Diversionbull Pharmaceutical productionbull Availability of alternative pain
management treatment
This effort seeks to address treatment of both prescription and non-prescription opioids however it will not address supply of non-prescription opioids (namely heroin)
bull Compassionate consistent carebull Taperingbull Pain management educationbull Availability of alternative pain
management treatmentbull Education of patients and families
bull Identification individuals with opioid use disorder
bull Availability of detox facilitiesbull Availability of long-term ongoing
comprehensive addiction treatmentbull Availability of supportive social servicesbull Prevention of fatal overdose
Raise awareness of risk of opioid
addiction
bull Identification and education of patients at greater risk for addiction
bull Provider educationbull Adolescent educationbull Adult educationbull Reducing stigma around substance
abuse
Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Case Studies
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89
How Can Primary Care Address the Opioid Epidemic
Use of an Interdisciplinary team-based group visit model to provide BuprenorphineNaloxone (BN) in primary care PCMH clinic
Alicia Agnoli MD MPH
Greg Sawin MD MPH
Randi Sokol MD MPH MMedEd
Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Centers for Disease Control and Prevention Vital Signs Variation Among States in Prescribing of Opioid Pain Relievers and
Benzodiazepines mdash United States 2012 MMWR 2014 63(26)563-568
Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Gap between with pastyear OUD ampcombinedbuprenorphineamp methadonecapacity
OUD amp Treatment Capacity
Gap=914000
Jones CM et al Am J Public Health 2015
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89
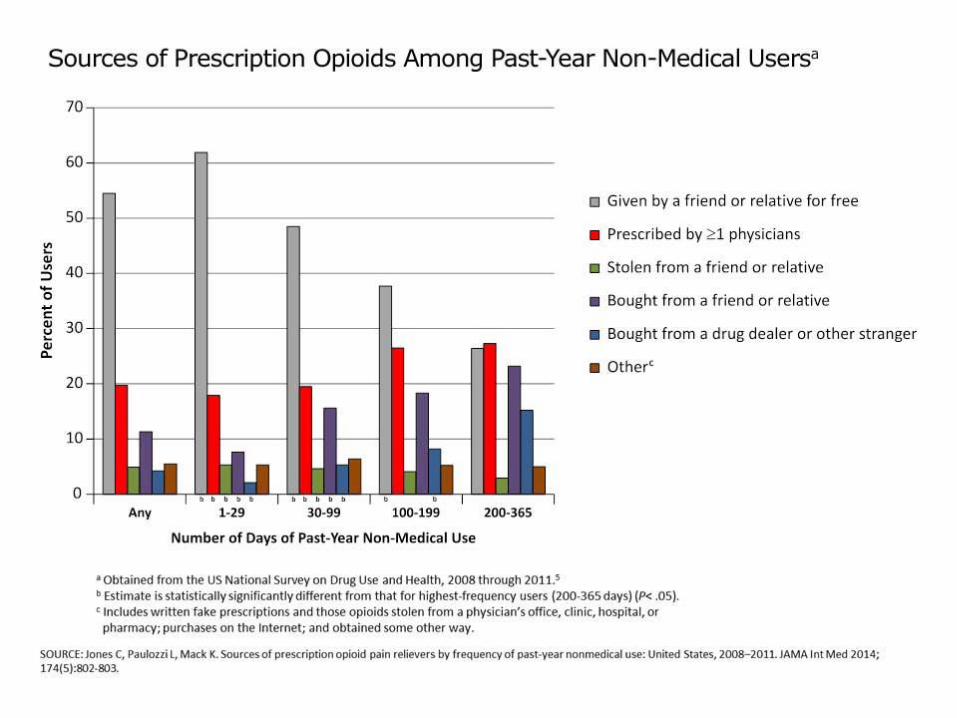
Asthma HTNAddiction
(ETOH Opiates)
Etiology
Lifetime
Prevalence (USA)129 90 9
Heritability
(genetics)036 - 07 025 - 05 034 ndash 055
EnvironmentAir quality SES
Cultural salt intake
stress
Peer group
behavior SES etc
Personal Choice Smoking Exercise Diet Exercise Decision to use
Relapsing Course
seeking care
each year to
achieve
symptomatic
relapse
70 50 30 ndash 50
Importance of
Patient
Engagement
Medication
Adherence Rates 40 40 50-70
Lifestyle
Adherence Rates 30 30
meeting national
quality goals 30- 50 30- 50
Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Chronic Disease Model Approach to OUD
+Medication
Manage Cravings
Prevent
Withdrawals
Behavioral Treatment
Develop healthy
coping skills
Build Community
Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Medication Assisted Treatment (MAT) for OUD
bull Methadone and buprenorphine
rarr most evidence for recovery
bull At 1 year 40-60 of patients maintained on
methadone or buprenorphine remain sober
bull Naltrexone - less effective
Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Office-Based Opioid Therapy (OBOT)
bull Buprenorphine MATbull Medically effective
bull Cost-effective
bull Safe
bull Higher patient satisfaction
bull Higher provider satisfaction
bull Underutilized
What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

What happens in group
bull Urine drug screens
(publically posted)settle (prior to group)
bull Introductions (3m)
bull Ground Rules (2m)
bull Didactic (10m)
bull Check-in(45m)
bull Prescriptions (we use
paper) (at end)
What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

What Happens Between Groups
bull RN amp MD call ldquostrugglingrdquo patients or new
patients to check in
bull Care coordination with psych SW PCP Parole
officers DCF patients currently inpatient (in
IOP detox residential)
bull Follow up with patientrsquos urine drug screens (ldquoso
your urine came back with cocaine in ithelliprdquo)
bull Ongoing screening of new patient referrals +
intake appts
bull Prepare didactics
rarr RN amp MD time ~5-6 hoursweek each
Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Resident perspective
bull deeper more authentic understanding of patients
bull value of team-based approach
Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Patient perspective group keeps them honest holds them accountable
Itrsquos showing up every week and knowing
that you have to be accountable for your
actions For me Irsquom all about
consequences hellip therersquos another 80 times
where Irsquove almost slipped up and thought
about this group and didnrsquot do it because
I didnrsquot want to look at all yrsquoall in the face
and say I did it again
Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Patient perspective Group fosters shared identity
Itrsquos good to have and to be in an atmosphere with those other people like you that understand youhellip
you know I feel like Irsquom not alone therersquos other people you know similar situations I have
support you know I donrsquot really have support outside of here My family you know theyrsquore
there but theyrsquore not -- my sisters arenrsquot addicts so they donrsquot understand it My parents donrsquot
understand it So it just feels good I donrsquot feel alone coming here
Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Patient perspective over time group creates supportive community
In the beginning I really didnrsquot care about
anybody I didnrsquot care about myself I didnrsquot
care what anybody had to say Irsquom like ldquoIs it
three orsquoclock yet Like can I get the fck out
of hererdquo Now I look forward to coming
coming here and seeing everybody
Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Clinic perspective
bull Destigmatizes addiction
bull Comprehensive care treat addiction while
treating other medical problems in 1 care
bull Lucrative + minimal staff
1 clinic session
-1 FD 1 RN 1 MA 1 MD
-20-30 patients
Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Estimated Staff Resource TimeWeek
(care of 40-50 pts)
Doctor 7 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours group prep
bull 3 hours screening + intakes
bull 2 hours coordinating care
bull 1 hour notes
LPN 10 hours
bull 2 hours group
bull 1 hour Team meeting
bull 3 hours intakes
bull 4 hours phone follow ups + care
coordination
Front Desk 3 hours
bull 2 hours calls appointment
managementscheule prep
bull 1 hr Team meeting
MA 7 hours
bull 2 hours group
bull 2 hours group prepfollow up
bull 3 hours paperwork
Resident 5 hours
bull 4 hours group afternoon
bull 1 hour didactic prep
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89
ReferencesBarry DT Moore BA Pantalon MV et al Patient Satisfaction with Primary Care Office-Based
BuprenorphineNaloxone Treatment Journal of General Internal Medicine 2007 22 (2) 242ndash45
Berger R Pulido C Lacro J Groban S Robinson S Group medication management for buprenorphinenaloxone in opioid-dependent veterans J Addict Med 20148(6)415-20
Center for Health Information and Analysis Access to Substance Use Disorder Treatment in Massachusetts April 2015
Clark RE Smanaliev M Baxter JD Leung GY The Evidence Doesnrsquot Justify Steps By State Medicaid Programs To Restrict Opioid Addiction Treatment With Buprenorphine Health Affairs 2011 30 (8) 1425ndash33
Clinical Guidelines for the Use of Buprenorphine in the Treatment of Opioid Addiction A Treatment Improvement Protocol TIP 41 Substance Abuse and Mental Health Services Administration 2004 Web
Cunningham CO Sohler NL McCoy K Kunins H Attending physiciansrsquo and residentsrsquo attitudes and beliefs about prescribing buprenorphine at an urban teaching hospital Fam Med 200638(5)336-40
ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

ReferencesNational Institute on Drug Abuse (NIDA) (2014) The Science of Drug Abuse and Addiction Treatment and Recovery
accessible at httpwwwdrugabusegovpublicationsdrugs-brains-behavior-science-addictiontreatment-recovery
Maremmani I Pani PP Pacini M Perugi G Substance use and quality of life over 12 months among buprenorphine maintenance-treated and methadone maintenance-treated heroine addicts J Subst Abuse Treat 2007 33(1) 91-98
Mattick RP Breen C Kimber J Davoli M Buprenorphine maintenance versus placebo or methadone maintenance for opioiddependence Cochrane Database Syst Rev 2014
Mitzner IL Eisenberg M Terra M MacVane C Himmelstein DU Woolhandler S Treating Opioid Addiction With Buprenorphine in Community-Based Primary Care Settings Ann Fam Med 2007 5(2) 146ndash150
Rowe T Jacapraro J and Rastegar D Entry into Primary Care-Based Buprenorphine Treatment Is Associated with Identification and Treatment of Other Chronic Medical Problems Addict Sci Clin Pract 2012 7 (1) 22ndash22
Rudd RA Aleshire N Zibbell JE Gladden MR Increases in Drug and Opioid Overdose Deaths mdash United States 2000ndash2014 Centers for Disease Control MMWR Morb Mortal Wkly Rep 2016 64(50) 1378-82
Sokol R et al Training Family Medicine Residents to Treat Opioid Use Disorder (OUD) with Buprenorphine-Naloxone (BN) via a Group Visit Team-based Approach Adv Med Educ Pract In Review
Sokol R et al Why Use Group Visits for Opioid Use Disorder Treatment in Primary Care A Patient-Centered Qualitative Study Substance Abuse In Review
Substance Abuse Treatment Group Therapy Treatment Improvement Protocol (TIP) Series No 41 Rockville MD Center for Substnce Abue Treatment Substance Abuse and Mental Health Services Administration (SAMHSA) 2005
Suzuki J Zinser J Klaiber B et al Feasibility of Implementing Shared Medical Appointments (SMAs) for Office-Based OpioidTreatment With Buprenorphine A Pilot Studyrdquo Subst Abuse 2015 36(2)166ndash169
Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Questions
Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Small Clinic Big IssuesAndrew Jorgensen MD FACP FAAPChief Medical Officer Outer Cape Health Services
Orlando Florida
Session Code
IHI SummitApril 20 ndash 22 2017
IHISummit
Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Opiate Overdose Deaths in Massachusetts34
Source Massachusetts Department of Public Health Data brief Opioid-related overdose deaths Among Massachusetts residents Boston Commonwealth of Massachusetts Department of Public Health 2017 Feb Available from httpwwwmassgoveohhsdocsdphstop-addictioncurrent-statisticsdata-brief-overdose-deaths-february-2017pdf
Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Opiate Overdose Deaths on Cape Cod
bull 395 overdose deaths on Cape Cod from 2000-2015
bull Barnstable County ranked No 3 for fatal overdoses in the state in
2015 with 303 deaths per 100000 people
35
Source Massachusetts Department of Public Health USCensus | Chart Gregory Bryant Cape Cod Times
bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

bull Rural FQHC formed 1987
bull Serves Eight outermost towns of Cape Cod
bull 200 square-mile catchment area
bull Designated by HRSA as underserved for Medical
Dental amp Mental Health
bull Closest Emergency Room is one hour away from
Provincetown
About Outer Cape Health Services36
OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

OCHS-Provincetown
bull 16 exam rooms
bull CHC farthest from a hospital
in Massachusetts (60 miles away)
bull Renovated 2010
OCHS-Wellfleet
bull 8 exam rooms
bull Oldest CHC building
in Massachusetts
(1966)
OCHS-Harwich
bull 5 small exam rooms
bull Rental space opened 2011
37
38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

38
Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Chronic pain case management
Two-pronged approach
bull Optimizing risk management by PCP team
bull Changing prescriber behavior
39
Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Chronic Pain Case Management
(CPCM) Program
bull Pilot began March 2015
bull Registry of patients receiving opiate Rxrsquos developed
bull Tiered consistent risk monitoring by nurse case
manager oversees registry
bull One-on-one meetings with providers
bull Team discussions
40
Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Chronic Pain Registry excerpt41
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89
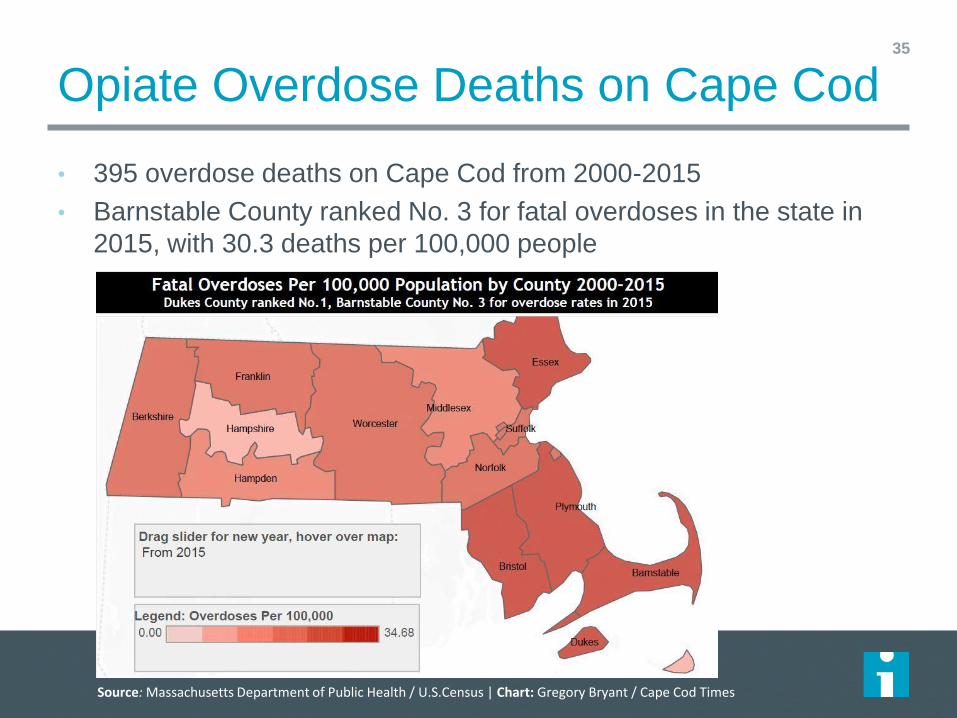
NIDA Opioid risk tool42
Source wwwdrugabusegovnidamed-medical-health-professional
Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Tiered risk structure43
CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

CPCM Workflow and Guidelines44
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier ldquoAverage
riskrdquo
CPCM 3 Risk Tier ldquoLow
riskrdquo
Tier description
High daily dose = MS equiv 100mg or
higherday or
Benzo use or
Red flags
or a combination of these risks
10-99 MS equivalentdaily
No benzo
No red flags
Bulk of patients
Low dose lt10 mg MS equivday
No benzo
No red flags
Problem List
RN selects tier using the description
above PCP input may be sought if
questions
March 2016 patient lists have been tiered
by DONMed Director as a starting point
using June data
RN can change the tier as doses reduce or
benzo use stops or red flag issues resolve
RN locates ldquodummy code CPCM1rdquo just as
you would find any ECW problem list
assessment code
Adds to lsquotop of problem listrsquo for easy
reference
Same
Dummy code CPCM2
Same
Dummy code CPCM3
PEG scale
MA asks pt to complete at visit prior to PCP
visit (paper form)
MA enters PEG info from form into ECW
HPI ldquoPEGrdquo at visit
For example P9 E8 G6=23
Discards paper form
Same Same
Opioid Risk Tool
Located in ROS
PCP completes risk assessment at least
once (not onceyear) for PCP information
about risk
Same Same
CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

CPCM Workflow and Guidelines45
CPCM 1 Risk Tier
ldquoHigh riskrdquo
CPCM 2 Risk Tier
ldquoAverage riskrdquo
CPCM 3 Risk Tier
ldquoLow riskrdquo
UDS capture by MARN
Monthly
At visit or
RX pickup
RN Prompts the prescription in med closet or
the OV note
RN reminds PCP to order UDS monthly
standing order
Quarterly
At visit or
RX pickup
RN Prompts the prescription or the OV note
RN reminds PCP to order monthly standing
order (in case random UDS requested by RN)
Annually
At visit or RX pickup
RN Prompts the prescription or the OV note
Monthly standing order UDS at RN discretion
(in case random UDS req by RN)
PMP (Physician Monitoring Program) check by RN delegate
Quarterly
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Delegates need to be notarized- see Medical
Director for details
Every 6 months
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
Annual check
RN printsign
To provider to signfile
MA delegate may be assigned to do this for
PCPs by RN
RN review of CPCM patient list at least monthly
To ensure PCP OV every 3 months per
policy
RN (who can assign MA) to reach out to
non-compliant pt to facilitate OV
To prompt upcoming OVs if
UDSContract due
To ensure new patients added appropriately
and promptly for CPCM
Same Same
Call-in for pill countsUDS
Random pill counts suggested quarterly
By RN or provider for any red flag or
concern
If patient seems inappropriate at RX pick-up
or OV call-in within week
DNKA call-in within week
Same Consider random pill count periodically otherwise
same
Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Bell curve of risk tiers46
Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Changing provider behavior
bull Follow new MA and CDC guidelines with frequent reminders
bull Expectations for tapering high MEQ
bull Optimizing safer strategies Honest group discussions
bull Regularly scheduled meetings with PCPs and RNs
bull Initially optional before regular meetings now part ofprovider meeting
bull Model best practices practice difficult conversations
bull Team-building team support critical
bull Quarterly statistic tracking
bull Existing general monthly peer review
47
Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Concurrent State Efforts48
Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Measures of success
bull Improvement in urine drug screening PMP annual
agreements (80 goal)
bull Decline in numbers of patients being prescribed high
dose opiates
bull More referrals to OCHS Behavioral Health
bull Improvement in PCP satisfaction with care for patients
with pain
49
Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Patient enrollment in CPCM program50
195
200
205
210
215
220
225
230
235
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Distribution of risk tiers51
0
10
20
30
40
50
60
70
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Tier 1 Tier 2 Tier 3
Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Results52
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Controlled substance agreement status
Up to date Expired None on file
Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Results53
0
10
20
30
40
50
60
70
80
90
100
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016
PMP report status
Up to date Out of date Never
Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Results54
0
10
20
30
40
50
60
70
80
90
Jul 2016 Aug 2016 Sep 2016 Oct 2016 Nov-16 Dec-16 Jan-17 Feb-17
Urine drug screening
Up to date Out of date Never
Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Results55
82
84
86
88
90
92
94
96
Aug 2016 Sep 2016 Oct 2016 Nov 2016 Dec 2016 Jan 2017 Feb 2017
Office visits up to date
Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Reasons for discontinuation of Rx56
15
13
3
69
Diedmovedtransferred
Stopped prescribing due todiscordant UDS
Referred to pain specialist
Tapered off no longer needed
77 discontinued (82016 ndash 22017)
Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Challenges amp barriers
bull Changing behavior is hard work not just for patients but
for providers as well
bull Like all change processes providers have different
capacities for change
bull Nurse Care Manager is a grant funded position and it is
an effort to embed work in care teams
bull Morning discussion meeting useful but the work can
overwhelm other important efforts at the Health Center
57
Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Success stories
bull 54 year-old woman with chronic abdominal pain related to cirrhosis from Hepatitis C
bull Initially using Oxycodone 90 mg every 6 hours also using other high risk medications including clonazepam and Ritalin
bull Began seeing her when prior PCP retired patient very resistant to weaning
bull Worked closely with behavioral health team including co-located Psychiatrist to manage overall risk
bull Treated her Hepatitis C
bull Patient also worked on her abusive relationship with her husband
bull After 12 months no longer using any opiates
58
Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Future amp sustainability
bull Working on embedding care management in to primary
care teams as part of PCMH
bull Spread approach to other high risk medications such as
benzodiazepines
bull Integrate metrics in to overall quality improvement efforts
to help with sustainability
59
Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Remembering those lost to addiction60
Source Cape Cod Times
QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

QuestionsP61
Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Break
Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
System-Level Approach to Opioid Prescribing
Dr Mary Ellen Benzik
Chief Medical Officer
Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
MissionWe provide innovative high-value health care solutions to companiesimproving the health and well-being of the people we serve
VisionWe will transform the delivery of health care as a trusted partner to the companies we serve Together we will create a culture of health and become our patientsrsquo most cherished benefit
OUR GUIDING PRINCIPLE
Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
STEP 1 ndash CREATE THE CONVERSATION
bull Physician leadership
bull Create a clear message and a burning platform
ldquo This is a national crisis not a QuadMed crisis and we are a critical part of the solutionrdquo
78 people die every day in opioid-related deaths
28470 people a year
Equal to a ldquo911 eventrdquo every six weeks
Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
STEP 2 ndash COLLECT DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
Pro
vid
ers
Ph
ysic
ian
Lead
ers
hip
Exe
c Le
ade
rsh
ip
Clin
ical
Le
ade
rsh
ip
Co
mp
lian
ce
IT Qu
alit
y
Trai
nin
g
Lega
l
Lab
Op
era
tio
ns
HR
Fin
ance
Emp
loye
rs
Pai
n M
gmt
Exp
ert
s
2016
Educate providers
Share data
Create opioid prescribing policy
IT decision support
2017
Roll out policy
Monthly data sharing
Increase learning opportunities
Integrate KPIs bonus structure
Create strategy for our community
STEP 3 ndash DEVELOP A WORK PLAN
Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE PRESCRIBING POLICY
KEY FACTORS IN THE POLICY
1 Patient and provider to review and sign controlled substance policybull Patient agrees to use
one pharmacy bull To only take meds as prescribed bull Will have QM as their
medical home not obtaining narcotics from any other provider
bull Agree to urine drug testing and pill counts as deemed necessary by the provider
2 If a patient states their medication is stolen ndash a police report must be filed prior to replacing medication
3 A urine drug screen must be obtained when the medication is initially prescribed and as deemed necessary by the provider at least annually
Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
KEY FACTORS IN THE POLICY
4 State registries must be queried with each initial and refill prescription
5 A query score is to be generated ndash with an assessment for potential abuse or addiction
6 QuadMed providers are strictly prohibited from issuing prescriptions for controlled substances for the maintenance of drug
or alcohol addiction andor for detoxification treatment to patients If a QuadMed provider has a patient who is in need of addiction treatment the QuadMed provider should refer the patient to an existing facility through the following website findtreatmentsamhsagov
CONTROLLED SUBSTANCE PRESCRIBING POLICY
Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
IT TOOLS TO HELP US BE SUCCESSFUL
bull Workflow sheet
bull Capacity to query the state database from EMR
bull Tool to calculate the morphine mg equivalents in EMR
bull Linkage in the tool to find treatment programs in the area
bull Narcotic pain contract
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FEATURES
bull Document a patientrsquos pain score at its worst and best
bull Document neuropathic pain
bull Document hypersensitivity or fibromyalgia pain
bull Document location of pain intensity and how the pain affects the patientrsquos daily living
bull SOAPP and COMM tools are available within the form
Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CHRONIC PAIN QUESTIONNAIRE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FORM FEATURES
bull Compliance counters reset after one year
bull Morphine Milligram Equivalent (MME) calculator
bull Order urine drug screen and results
bull Document random pill count
bull Launch directly to state prescription monitoring program
bull Document medication contract on file
bull Opioid risk tool
bull Set next refill dates
bull Direct access to pain contracts
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Calculating the total daily dose of opioids helps identify patients who may benefit from closer monitoring reduction or tapering of opioids prescribing of naloxone or other measures to reduce risk of overdose
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FORM
Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTROLLED SUBSTANCE FLOWSHEETS
Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
CONTINUOUS QUALITY IMPROVEMENT
ldquoYou canrsquot manage what you canrsquot measurerdquo - Peter Drucker
bull Number of mg of morphine equivalents being prescribed by the network
bull Opioids with benzodiazepines (BZD) or antidepressants
bull Opioids with sleep apnea
bull Patients with high-dose opioids
ldquoIn God we trust everyone else must bring datardquo - Deming
Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
END OF 2017 DATA
Start of our QM journey into safe opioid prescribing
October 6 2014Hydrocodone Class Change
Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
bull Analyzed data to select providers
bull Meet monthly to discuss the challenges and provide support to safely manage patients
bull Team controls the agenda and discussion topics to focus on areas of need
bull Will shape the program for the remainder of the group
PROVIDER LEARNING COHORT
Patients with MME gt 100 and BZD (July through December 2016) 60
36Patients with MME gt 100 (January 2017)
Count of PID Match Clinical_Date
RxResponsibleProvi
derLast MMEDay Jul Aug Sep Oct Nov Dec Grand Total
McGriff MD 2 14 16
120 2 2
180 2 12 14
Whyte MD 3 4 2 2 2 13
135 3 2 2 2 2 11
180 2 2
Ness MD 3 3 6
135 3 3
1425 1 1
150 1 1
180 1 1
Wyer MD 2 3 5
135 1 1
180 1 3 4
Ashbrooks MD 2 2 4
150 2 2 4
Peterson MD 1 1 1 1 4
120 1 1 1 1 4
Krueger MD 1 1 1 1 4
120 1 1 1 1 4
Bagshahi MD 2 2
120 2 2
Asmundsen PA 2 2
120 2 2
Brodie MD 1 1 2
120 1 1 2
Fakhoury MD 2 2
180 2 2
Grand Total 9 26 5 4 9 7 60
Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
SAFE PRESCRIBING
bull Integrated into QuadMed KPIsreported to the board
bull Metric is part of the management and provider bonus calculation
bull Peer review of charts for all providers prescribing opioids over 100 MME and concurrent BZD Providers role to limit the number of
patients to be peer reviewed Organizational support of the peer
review structure bull Mandatory completion of education and
knowledge assessment for all providers on the controlled substance policy with HR implications for non-compliance
Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
PROVIDERS RESPONSE bull ldquoThe policy gives me a frame to begin
the discussion with my patientsrdquo bull ldquoThe decision support tool helped me
learn about the MME and made it easy to do the right thingrdquo
bull ldquoThe learning cohort gives me the opportunity to work this through with other providersrdquo
PATIENT STORY bull Provider helped a patient move from
extremely high MME with BZD to a successful weaning of all her meds
bull ldquoShe was a new person more alive and engaging to everyone in the health centerrdquo
SAFE PRESCRIBING FEEDBACK
Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
IT TAKES A COMMUNITY ndash NEXT STEPS
1 IT clinical decision support bull Adding weaning template and
calculator to the EMR tools bull Adding discharge education bull Considering discharge information
on disposal of medications
2 Clinical aspects bull Getting health centers to utilize
their local 211 resources bull Signage in the health centers bull Standardization of the stocking
and prescribing of naloxone in the health centers
bull Continuing to adjust the policy
3 Monitoring and training bull Continued training using
computer-based resources bull Monthly data sharing at the
CMO forum bull Tracking and engaging with
all new providers at 30 60 and 90 days
4 Partnering with employers in high-risk geography
Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Experience Solutions Results
THANK YOU ndash KEY RESOURCES
bull httpswwwcdcgovdrugoverdoseindexhtml
bull wwwscopeofpainorg
bull wwwopiodprescribingorg
bull httpstoresamhsagovproductOpioid-Overdose-Prevention-Toolkit-Updated-2016All-New-ProductsSMA16-4742
Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Exercise
Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Topic Tables
1 Safe opioid prescribing ndash changing provider behavior at
the individual level
2 System changes to facilitate evidence-based care
3 Patient education about chronic pain pain
management and risks of opioids
4 Using teams to treat addiction in primary care
5 Making addiction treatment more accessibleavailable
6 Linking with community-based efforts
7 Other topics ndash please nominate
P88
Final QampA and Wrap UpP89

Final QampA and Wrap UpP89