adenocarcinoma in the jejunal pouch after proximal gastrectomy for early stage upper gastric cancer:...
TRANSCRIPT
CASE REPORT
Adenocarcinoma in the jejunal pouch after proximal gastrectomyfor early stage upper gastric cancer: report of a case
Takanori Kurokawa • Motoshi Kanai •
Yukihiro Kaneko • Hiroshi Takahashi •
Toshiji Motohara
Received: 4 April 2011 / Accepted: 6 June 2011 / Published online: 27 January 2012
� Springer 2012
Abstract An 84-year-old male was admitted to a local
clinic suffering from general fatigue with associated ane-
mia, and therefore was referred to our hospital. His medical
history included a proximal gastrectomy with the formation
of a jejunal pouch as a reconstructive treatment for early
upper gastric cancer at 78 years of age (6 years prior).
A type 2 tumor located in the jejunal pouch almost com-
pletely surrounded by small intestinal mucosa was dem-
onstrated by gastrointestinal endoscopy. The biopsy
specimens showed a moderately differentiated tubular
adenocarcinoma. Computed tomography showed no lym-
phadenopathy or hepatic metastases. A resection of the
residual stomach and jejunal pouch was performed. Based
on the histological findings from the resected specimen, the
tumor was considered to be primary adenocarcinoma in the
jejunal pouch. The postoperative course was uneventful,
and the patient has shown no evidence of any recurrence
during the 6-year period after the most recent surgery.
Keywords Jejunal cancer � Jejunal pouch interposition �Gastric cancer � After gastrectomy
Introduction
Recently, jejunal pouch interposition after gastrectomy has
become a common procedure in Japan. Cancer in the
jejunal pouch after gastrectomy is very rare, and only a
small number of cases have been reported [1–4]. All of
these cases were suture line recurrences in the pouch
caused by implantation with exfoliated cancer cells during
the surgery. We were unable to find any reports of primary
cancer in the jejunal pouch after gastrectomy. We herein
report the case of a patient suspected to have primary
adenocarcinoma in the jejunal pouch, which was detected
after proximal gastrectomy for early upper gastric cancer.
Case report
An 84-year-old male was admitted to a local clinic because
of general fatigue. He was suffering from anemia, and was
referred to our hospital in September 2004. He had under-
gone a proximal gastrectomy with jejunal pouch interposi-
tion to treat early upper gastric cancer in June 1998. During
the surgical procedure, the upper one-third of the stomach
was resected using an automatic suturing device (Nakay-
ama suturing instrument), and a jejunal pouch was produced
by means of another automatic suturing device (linear
cutter). Histologically, the tumor was a moderately differ-
entiated tubular adenocarcinoma invading the sub-mucosal
layer, without permeation of the lymphatic or venous cap-
illaries. The proximal and distal margins were free of cancer
cell invasion. No lymph node metastasis was seen
(Stage Ia), and the patient was followed up without adjuvant
chemotherapy. On admission to our hospital in November
2004, hematological studies revealed anemia (hemoglobin
8.3 mg/dl, hematocrit 25.1%). The serum levels of carci-
noembryonic antigen (CEA), and carbohydrate antigen
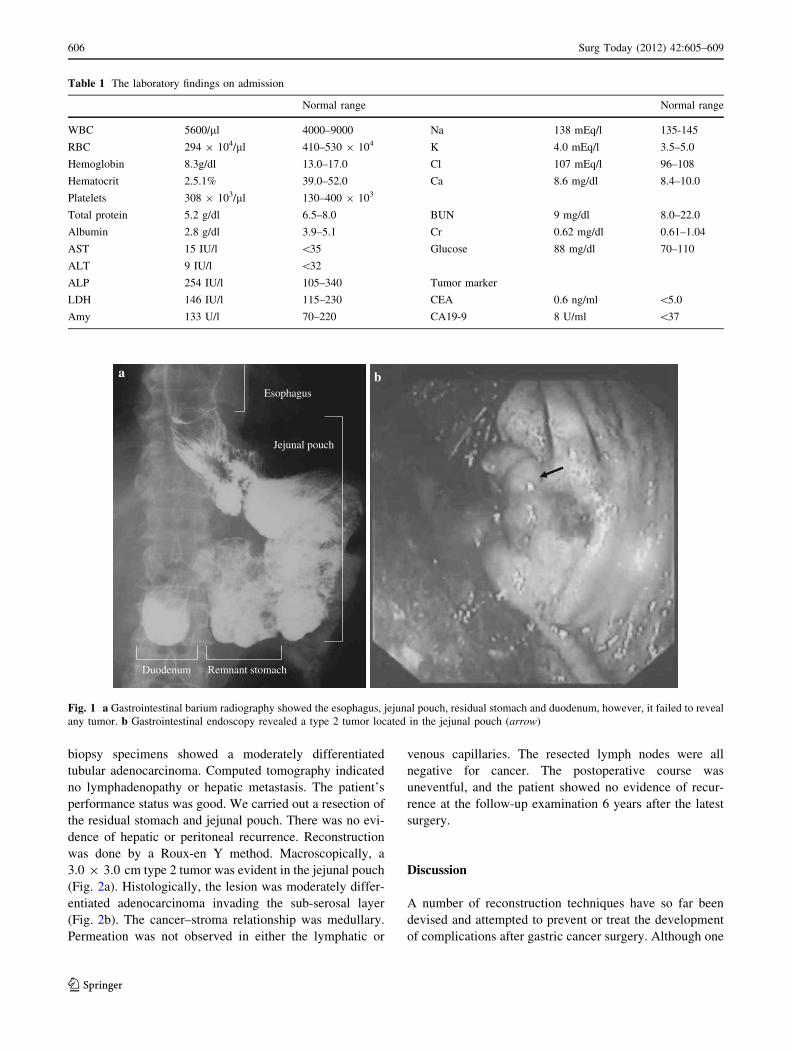
(CA) 19-9 were within the normal limits (Table 1). Gas-
trointestinal barium radiography showed the esophagus,
jejunal pouch, residual stomach and duodenum; however, it
failed to identify any tumor (Fig. 1a). A type 2 tumor
located in the jejunal pouch was revealed through gastro-
intestinal endoscopy (Fig. 1b). An examination of the
T. Kurokawa (&) � M. Kanai � Y. Kaneko � H. Takahashi �T. Motohara
Department of Surgery, Hakodate Medical Association Hospital,
10-10, Tomioka-cho, Hakodate, Hokkaido 041-8522, Japan
e-mail: [email protected]
123
Surg Today (2012) 42:605–609
DOI 10.1007/s00595-012-0125-9
biopsy specimens showed a moderately differentiated
tubular adenocarcinoma. Computed tomography indicated
no lymphadenopathy or hepatic metastasis. The patient’s
performance status was good. We carried out a resection of
the residual stomach and jejunal pouch. There was no evi-
dence of hepatic or peritoneal recurrence. Reconstruction
was done by a Roux-en Y method. Macroscopically, a
3.0 9 3.0 cm type 2 tumor was evident in the jejunal pouch
(Fig. 2a). Histologically, the lesion was moderately differ-
entiated adenocarcinoma invading the sub-serosal layer
(Fig. 2b). The cancer–stroma relationship was medullary.
Permeation was not observed in either the lymphatic or
venous capillaries. The resected lymph nodes were all
negative for cancer. The postoperative course was
uneventful, and the patient showed no evidence of recur-
rence at the follow-up examination 6 years after the latest
surgery.
Discussion
A number of reconstruction techniques have so far been
devised and attempted to prevent or treat the development
of complications after gastric cancer surgery. Although one
Table 1 The laboratory findings on admission
Normal range Normal range
WBC 5600/ll 4000–9000 Na 138 mEq/l 135-145
RBC 294 9 104/ll 410–530 9 104 K 4.0 mEq/l 3.5–5.0
Hemoglobin 8.3g/dl 13.0–17.0 Cl 107 mEq/l 96–108
Hematocrit 2.5.1% 39.0–52.0 Ca 8.6 mg/dl 8.4–10.0
Platelets 308 9 103/ll 130–400 9 103
Total protein 5.2 g/dl 6.5–8.0 BUN 9 mg/dl 8.0–22.0
Albumin 2.8 g/dl 3.9–5.1 Cr 0.62 mg/dl 0.61–1.04
AST 15 IU/l \35 Glucose 88 mg/dl 70–110
ALT 9 IU/l \32
ALP 254 IU/l 105–340 Tumor marker
LDH 146 IU/l 115–230 CEA 0.6 ng/ml \5.0
Amy 133 U/l 70–220 CA19-9 8 U/ml \37
a bEsophagus
Jejunal pouch
Remnant stomachDuodenum
Fig. 1 a Gastrointestinal barium radiography showed the esophagus, jejunal pouch, residual stomach and duodenum, however, it failed to reveal
any tumor. b Gastrointestinal endoscopy revealed a type 2 tumor located in the jejunal pouch (arrow)
606 Surg Today (2012) 42:605–609
123

of these techniques, jejunal pouch interposition, has been
performed for many years, reports of cancer reoccurring in
the jejunal pouch after gastric cancer surgery are extremely
rare. Only five cases had been reported, as determined by
Medline searches (using the keywords ‘gastric cancer’,
‘recurrence’, and ‘jejunal pouch’) [1–4] (Table 2). These
recurrences developed between the 4th month and 3 years
following the initial surgery, and were typically elevated
tumors or ulcerative lesions that developed on the suture
line in the jejunal pouch or on the esophagojejunal
anastomosis. All of these cases were considered to be
relapses caused by implantation with exfoliated cancer
cells during the surgery.
Suture line recurrence is more frequently encountered in
colorectal cancers [5, 6]. Ryall [7, 8] reported that loose,
viable cancer cells may implant on freshly cut tissues
during surgery in cases of colorectal and breast cancer.
Umpleby [9] reported that exfoliated cells from colorectal
cancer were viable and that large numbers of cancer cells
were shed into the intestinal lumen, implanting on the
a bRemnant stomach Jejunal pouch
Fig. 2 a Surgically resected specimen revealed a type 2 tumor (arrow head) in the jejunal pouch. b Histologically, the lesion was a moderately
differentiated adenocarcinoma invading the subserosal layers (H&E 910)
Table 2 Cases of cancer arising in the jejunal pouch after gastrectomy
No. Author
report year
Age/
gender
Interval to
recurrence
Previous
treatment
Gross
appearance
Therapy Depth of
invasion
Lymph
node
metastasis
Histological
type
Outcome
1 Miyoshi
et al. [1]
74/M 4 months TG, DP, JPI Broad-based
elevated
tumor
Observation Unknown Unknown Well Dead
2 Nishimura
et al. [2]
57/F 3 years PG, JPI Elevated
tumor
RRSJ, RY T3 Positive Poorly Alive
3 Namikawa
et al. [3]
74/M 2 years
9 months
DG, B- II (first
operation) TG,
JPI, RY (second
operation)
Three
elevated
tumors
RRSJ, RY T2a Negative Moderately Alive
4 Shinohara
et al. [4]
60/F 1 year PG, JPI Elevated
tumor
RRSJ, RY T2 Negative Moderately Alive
5 74/M 1 year PG, S-JPI One elevated
tumors, two
ulcerative
lesions
RRSJ, RY T3
T2
Positive Moderately Alive
6 Our case
2010
84/M 6 years PG, JPI Type 2 tumor RRSJ,RY T3 Negative Moderately Alive
TG total gastrectomy, DP distal pancreatectomy, JPI jejunal pouch interposition, DG distal gastrectomy, B-II Billroth II reconstruction,
RY Roux-en Y reconstruction, PG proximal gastrectomy, S-JPI S-shaped jejunal pouch interposition, RRSJ resection of the residual stomach and
jejunal pouch
Surg Today (2012) 42:605–609 607
123

freshly reconstructed anastomosis. However, the exact
mechanism by which this occurs has not yet been
elucidated.
During our investigation, a type 2 tumor was identified in
the jejunal pouch 2 cm to the oral side from the suture line
between the residual stomach and the jejunal pouch. In
addition, although some of the tumors were found close
to the jejuno-jejunal suture line in the pouch, the
mucous membrane of the tumor margins was almost
circumferentially surrounded by small intestinal mucosa
(Fig. 3), and successive transitional areas of cells between
the small intestinal mucosa and tumor were observed
(Fig. 4). Similarly, when gastric cancer surgery had been
performed 6 years previously, then it was diagnosed
as moderately differentiated tubular adenocarcinoma.
However, the gastric cancer remained in the submucosa, and
no metastasis or invasion from the peritoneal side was
observed. Furthermore, no invasion into the lymphatic
Fig. 3 The histopathological
findings of the resected
specimen revealed that the
mucous membrane of the tumor
margins was almost
circumferentially surrounded by
small intestinal mucosa
Cancer cells
Fig. 4 The histopathological
findings revealed successive
transitional areas of cells
between the small intestinal
mucosa and tumor
608 Surg Today (2012) 42:605–609
123

vessels or veins was observed, and the possibility of metas-
tases from the submucosa to the jejunum was considered to
be low.
The frequency of primary small intestine cancer is
0.3–4.9% of all gastrointestinal cancers [10–13]; moreover,
in autopsy cases, the frequency of primary small intestinal
cancer is very low as one-tenth of all metastatic cancer
cases [14]. Even though the precise origin of any tumor
requires some monoclonal evidence from a genetic analy-
sis, the present tumor was considered to be primary jejunal
cancer based on the findings of the above-mentioned his-
topathological examination. The prognosis of small intes-
tine primary adenocarcinoma is poor, with 5-year survival
rates ranging from 20 to 30% [12]. An early and accurate
diagnosis of small intestinal cancer is difficult because of
its rare clinical incidence and lack of specific symptoms
[15]. The favorable prognostic factors for adenocarcinoma
of the small intestine are an absence of nodal metastases
and a well-differentiated tumor grade [12]. The current
patient has remained free from disease after cancer resec-
tion for 6 years without adjuvant chemotherapy. To
improve the nutrition or quality of life after gastric cancer
surgery, the jejunal pouch has been developed, and its
usefulness has been reported [16–19]. Fortunately, the
incidence of cancer developing in the jejunal pouch is very
rare. Nevertheless, follow-ups are required in patients after
gastric reconstruction using a jejunal pouch to check for the
possibility of gastric cancer recurrence or primary adeno-
carcinoma in the pouch.
Conflict of interest Takanori Kurokawa and other co-authors have
no conflicts of interest to declare.
References
1. Miyoshi K, Fuchimoto S, Ohsaki T, Sakata T, Takeda I,
Takahashi K, et al. Suture line recurrence in jejunal pouch
replaced after total gastrectomy for gastric cancer. Gastric Can-
cer. 1999;2:194–7.
2. Nishimura M, Honda I, Watanabe S, Nagata M, Souda H, Miya-
zaki M. Recurrence in jejuna pouch after proximal gastrectomy
for early upper gastric cancer. Gastric Cancer. 2003;6:197–201.
3. Namikawa T, Kobayashi M, Okamoto K, Okabayashi T, Akimori
T, Sugimoto T, et al. Recurrence of gastric cancer in the jejunal
pouch after completion gastrectomy. Gastric Cancer. 2007;10:
256–9.
4. Shinohara T, Kashiwagi H, Nakada K, Nimura H, Ohmura Y,
Yanaga K. Suture line recurrence in the jejuna pouch after
curative proximal gastrectomy for gastric cancer: report of two
cases. Hepatogastroenterology. 2007;54:1902–4.
5. Umpleby HC, Fermor B, Symes MO, Willamson RC. Viability of
exfoliated colorectal carcinoma cells. Br J Surg. 1984;71:659–63.
6. Skipper D, Cooper AJ, Marston JE, Taylor I. Exfoliated cells and
in vitro growth in colorectal cancer. Br J Surg. 1987;74:1049–52.
7. Ryall C. Cancer infection and cancer recurrence. Lancet. 1907;II:
1311–6.
8. Ryall C. The technique of cancer operations, with relation to the
danger of cancer infection. BMJ. 1908;2:1005–8.
9. Umpleby HC, Fermor B, Symes MO, Williamson RCN. Isolation
of viable exfoliated colorectal cancer cells at the site of intestinal
transaction. Br J Surg. 1983;70:680–97.
10. Iiai T, Tani T, Suda T, Okamoto H, Hatakeyama K. Current
standard treatments for small intestinal cancer (in Japanese).
Geka (Surgery). 2001;63:1458–61.
11. Good CA. Tumor of the small intestine. AJR. 1963;89:685–705.
12. Oureil K, Adamus JT. Adenocarcinoma of the small intestine.
Am J Surg. 1984;147:66–71.
13. Hamano K. Small intestinal cancer (in Japanese). Syokakigeka
(Gastroenterological Surgery). 1990;13:953.
14. Harihara Y, Konishi T. Adenocarcinoma of the small intestine (in
Japanese). Geka (Surgery). 2003;65:1412–6.
15. Maekawa H, Sato K, Komatsu Y, Orita H, Sakurada M. Jejunal
cancer detected after a resection of bilateral ovarian metastasis:
report of a case. Surg Today. 2010;40:1084–7.
16. Nakane Y, Okumura S, Akehira K, et al. Jejunal pouch recon-
struction after total gastrectomy for cancer. A randomized con-
trolled trial. Ann Surg. 1995;222:27–35.
17. Zonca P, Maly T, Neoral C, Jacobi CA. Quality of life after
gastrectomy. Rozhl Chir. 2010;89:344–8.
18. Fein M, Fuchs KH, Thalheimer A, Freys SM, Heimbucher J,
Thiede A. Long-term benefits of Roux-en-Y pouch reconstruction
after total gastrectomy: a randomized trial. Ann Surg. 2008;247:
759–65.
19. Lee J, Hur H, Kim W. Improved long-term quality of life in
patients with laparoscopy-assisted distal gastrectomy with jejuna
pouch interposition for early gastric cancer. Ann Surg Oncol.
2010;17:2024–30.
Surg Today (2012) 42:605–609 609
123