adjuvant chemotherapy with doxorubicin (adriamycin) and 5–fluorouracil in t3, nx, mo bladder...
TRANSCRIPT
British JourMI of Urology (1983). 55, 386391 0 1983 British Association of Urological Surgeons
Adjuvant Chemotherapy with Doxorubicin (Adriamycin) and 5-Fluorouracil in T3, NX, MO Bladder Cancer Treated with Radiotherapy
B. RICHARDS, J. R. G. BASTABLE, L. FREEDMAN, R. W. GLASHAN, GLYNIS HARRIS, D. W. W. NEWLING, M. R. G. ROBINSON, P. H. SMITH and THE YORKSHIRE UROLOGY CANCER RESEARCH GROUP*
Departments of Urology, York District Hospital, Huddersfield Royal Infirmary, Hull Royal Infirmary, Pontefract General Hospital and St James's University Hospital, Leeds, and MRC Cancer Trials Office, Cambridge
Summary-Radical radiotherapy alone has been compared with radical radiotherapy followed by chemotherapy using doxorubicin (Adriamycin) and 5-fluorouracil in a randomised prospective study on 129 patients presenting with T3, NX, MO transitional cell carcinoma of the bladder.
One hundred and ten patients were evaluable with a minimum follow-up of 2 years. The addition of this form of chemotherapy did not appear to influence the survival rate or the
proportion of patients free from tumour. It cannot be recommended for routine use in the primary treatment of infiltrating bladder cancer.
For many years the main thrust of the therapeutic attack on carcinoma of the bladder has been directed towards eradication of the primary tu- mow. This approach is rewarding as long as the disease is superficial, but the outlook for patients with infiltrating bladder cancer remains unsatis- factory, two-thirds of the patients being dead of their disease within 5 years of diagnosis.
The survival rate can be improved by the addition of radiotherapy to surgery (Whitmore et al., 1977a and b) and patients treated with a combination of surgery and radiotherapy probably do better than those treated with radiotherapy alone (Wallace and Bloom, 1976; Miller, 1977), especially if they are male and under the age of 65 (Bloom et al., 1982); but, sadly, the differences in survival rate after different forms of treatment for the primary tumour are relatively small when compared with the large number of patients who
Accepted for publication 2 February 1983.
* Other contributing members include W. A. F. McAdam (Airedale Hospital, Steeton), R. S. Adib (Wakefield), D. Ash (Cookridge Hospital, Leeds), J. G. McVie (Glasgow) and W. G. Jones (Cookridge Hospital).
die of their disease whatever the primary treatment.
The pattern of failure is important. Metastatic disease which was not evident at the time of primary therapy is a major determinant of patient survival (Smith and Whitmore, 1981). In one report, 34% of 281 patients with T3 bladder tumours died of distant metastases after treatment with radiotherapy (Rider and Evans, 1976). The figures are somewhat similar in other series-30 to 40% of patients dying of carcinoma of the bladder do so with distant metastases (Prout, 1977; Whitmore et al, 1977a and b). In 25% the primary tumour had apparently been adequately controlled (Reuben, 1971; Prout, 1977; Whitmore et al., 1977a and b) and in these patients metastases must have developed because of the presence of small deposits which were undetected at the time of the initial treatment. The presence of these microme- tastases has led to the advocacy of adjuvant chemotherapy, which might be more effective in the treatment of very small deposits than would be expected when the tumour loads are larger.
In 1977, the regimen of chemotherapy used by members of the Yorkshire Urology Cancer Re- search Group in the treatment of patients with
386
ADJUVANT CHEMOTHERAPY WITH DOXORUBICIN 387
advanced carcinoma of the bladder was a combina- tion of doxorubicin and 5-fluorouracil (Cross et al., 1976; Glashan et al., 1977). The combination of doxorubicin and 5-fluorouracil has been reported to give a response rate of approximately 35% in such cases (Cross et al., 1976; EORTC, 1977; Lindholmetal., 1980; Veronesi etal., 1982). In that year it was decided to initiate a randomised prospective trial to see whether the results of treatment of T3, NX, MO transitional cell carcino- ma of the bladder would be improved when this regime was added to standard therapy with radical irradiation.
Patients and methods Patients with T3, NX, MO (UICC, 1978) transi- tional cell carcinoma of the bladder of any grade were eligible provided they were not more than 75 years old, had an adequate performance status, showed no evidence of heart disease or renal failure, and had not been previously treated with irradiation or chemotherapy.
Of 129 patients entered, 16 were excluded as ineligible (11 being over 75 years, four having metastases at entry to the study and one having a squamous cell carcinoma of the bladder). No information was available from a further three. This left 110 cases for analysis, submitted from eight institutions (Table 1). They were randomly allocated to one of two treatment groups, by telephoning a central office, with stratification by institution.
Table 1 Co-operating Hospitals and Investigators
Hospital Investigator Evaluable cases
Castleford Cookridge
Glasgow Huddersfield
(Royal Infirmary) Hull (Royal Infirmary) St James’s, Leeds Wakefield York District
M. R. G. Robinson D. Ash W. G. Jones J. G . McVie R. W. Glashan
D. W. W. Newling P. H. Smith R. S. Adib J. R. G . Bastable B. Richards
21 1 2 6
15
15 18 4
13 15
Total 110
Table 2 Patient Characteristics
High energy High energy Total radiation radiation +- chemotherapy
Age
Sex :
<60 years 15 360 years 40
Male 40 Female 15
G1 1 G2 20 G3 34 Not known
Radical radiotherapy: Received 45 Not received 10 Not known
Histological grade:
11 44
40 15
4 14 34 3
46 I 2
26 84
80 30
5 34 68 3
91 17 2
Totals 55 55 110
Group 1. Radical cobalt or supervoltage X-ray therapy, followed by at least four courses of chemotherapy.
Group 2. Radical radiotherapy as in group 1, with no chemotherapy.
The groups were comparable with regard to sex and histological grade. Those allocated to chemothera- py were marginally younger and had a slightly greater proportion of patients who, generally because of rapid progression of the disease, did not receive a radical course of radiotherapy (Table 2).
Chemotherapy Doxorubicin 50 mg/m2 and 5-fluorouracil 500 mg/ m2 were given into the side arm of a fast running infusion of 5% dextrose. The first injection was given within 3 months of the start of the radiothera- py. Courses were given at 3-weekly intervals to a total dose of at least 200 mg/m2 of doxorubicin, continuing up to a maximum of 550 mg/m2 of doxorubicin (1 1 doses) at the investigator’s discretion.
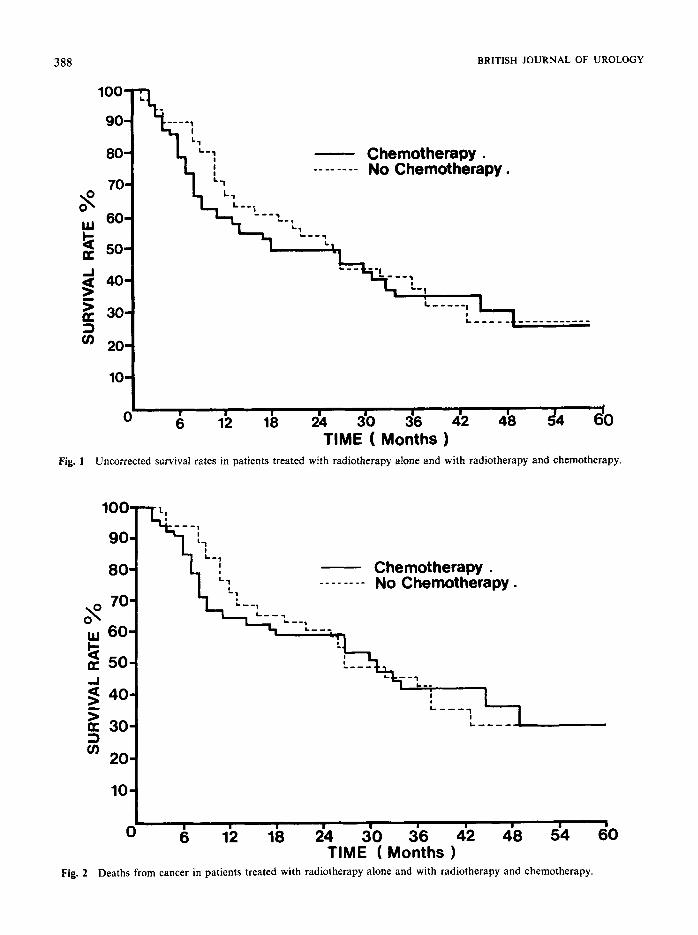
Results Figure 1 displays the uncorrected survival rates in the two groups of patients. There is a suggestion of increased mortality in the chemotherapy group in the first 24 months, but this is not statistically
388
10-
BRITISH JOURNAL OF UROLOGY
Fig.
80 L-1 - Chemotherapy . ! -- -_ -- _- Nn Chembtheraov .
60 U'
K
O t ' 6 12 18 24 30 36 42 48 54 60 TIME ( Months )
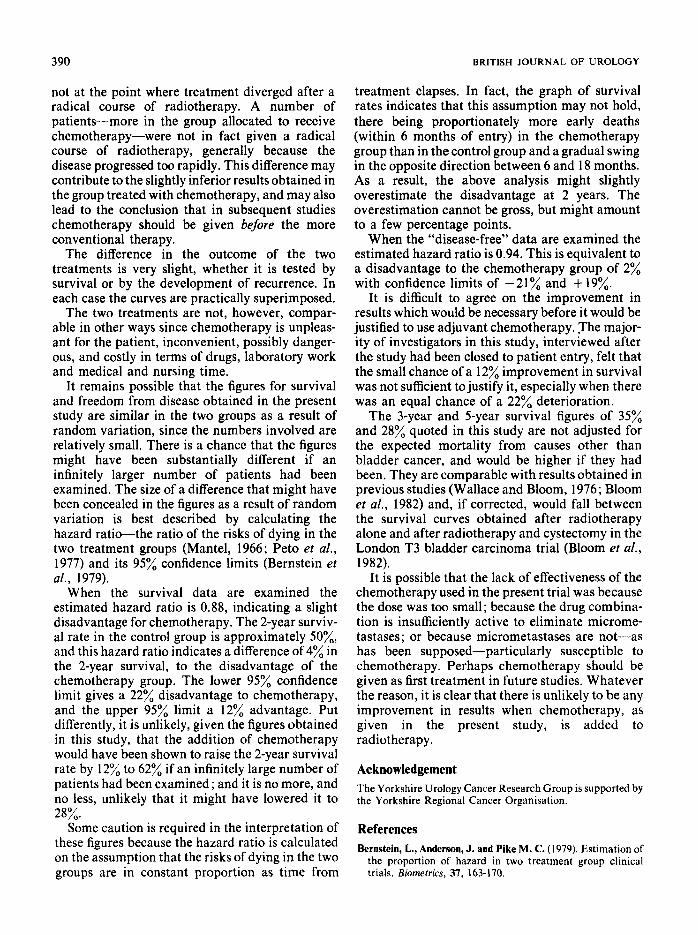
Fig. 2 Deaths from cancer in patients treated with radiotherapy alone and with radiotherapy and chemotherapy.
ADJUVANT CHEMOTHERAPY WITH DOXORUBICIN
100-
90-
80-
$70-
Q60- W
K
3 89
------, '
- Chemotherapy. -- - - - - - - No Chemotheraw .
Chemotherapy.
significant. By 3 years the survival rates are almost equal (35% in the chemotherapy group; 37% for no chemotherapy). The uncorrected survival rate for the few patients who have been followed for 5 years is 28% in each group.
The survival curves are equally similar when the death rate from cancer only is considered (Fig. 2).
The patients were assessed at 6,9 and 12 months and thereafter 6-monthly. Each assessment includ- ed general physical examination, cystoscopy, chest X-ray and measurement of liver function tests. The bone scan was carried out at 6 months and then annually.
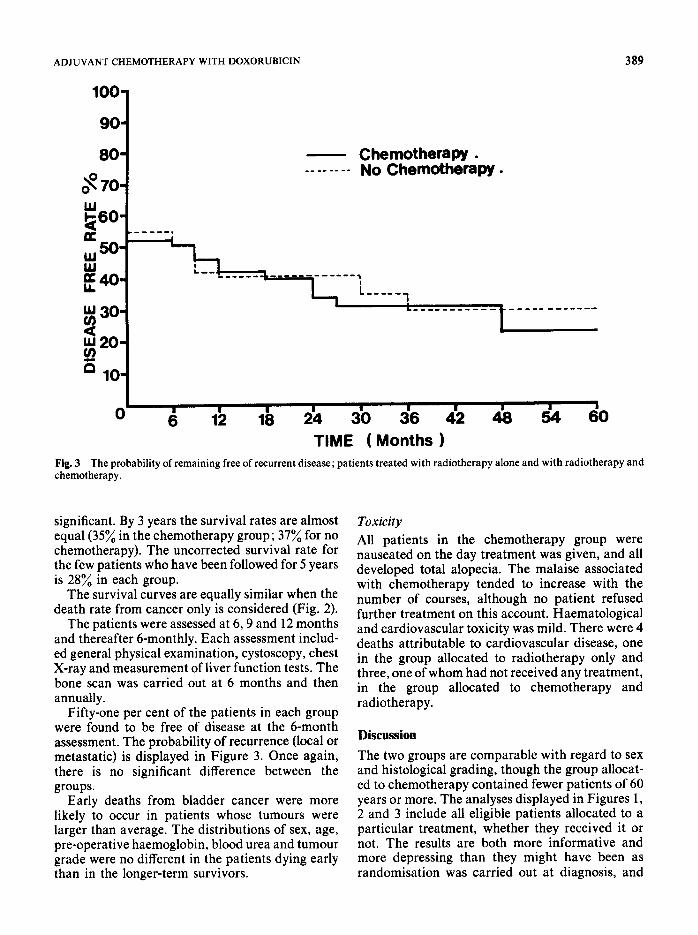
Fifty-one per cent of the patients in each group were found to be free of disease at the 6-month assessment. The probability of recurrence (local or metastatic) is displayed in Figure 3. Once again, there is no significant difference between the groups.
Early deaths from bladder cancer were more likely to occur in patients whose tumours were larger than average. The distributions of sex, age, pre-operative haemoglobin, blood urea and tumour grade were no different in the patients dying early than in the longer-term survivors.
Toxicity All patients in the chemotherapy group were nauseated on the day treatment was given, and all developed total alopecia. The malaise associated with chemotherapy tended to increase with the number of courses, although no patient refused further treatment on this account. Haematological and cardiovascular toxicity was mild. There were 4 deaths attributable to cardiovascular disease, one in the group allocated to radiotherapy only and three, one of whom had not received any treatment, in the group allocated to chemotherapy and radiotherapy.
Discussion The two groups are comparable with regard to sex and histological grading, though the group allocat- ed to chemotherapy contained fewer patients of 60 years or more. The analyses displayed in Figures 1, 2 and 3 include all eligible patients allocated to a particular treatment, whether they received it or not. The results are both more informative and more depressing than they might have been as randomisation was carried out at diagnosis, and
3 90 BRITISH JOURNAL OF UROLOGY
not at the point where treatment diverged after a radical course of radiotherapy. A number of patients-more in the group allocated to receive chemotherapy-were not in fact given a radical course of radiotherapy, generally because the disease progressed too rapidly. This difference may contribute to the slightly inferior results obtained in the group treated with chemotherapy, and may also lead to the conclusion that in subsequent studies chemotherapy should be given before the more conventional therapy.
The difference in the outcome of the two treatments is very slight, whether it is tested by survival or by the development of recurrence. In each case the curves are practically superimposed.
The two treatments are not, however, compar- able in other ways since chemotherapy is unpleas- ant for the patient, inconvenient, possibly danger- ous, and costly in terms of drugs, laboratory work and medical and nursing time.
It remains possible that the figures for survival and freedom from disease obtained in the present study are similar in the two groups as a result of random variation, since the numbers involved are relatively small. There is a chance that the figures might have been substantially different if an infinitely larger number of patients had been examined. The size of a difference that might have been concealed in the figures as a result of random variation is best described by calculating the hazard ratio-the ratio of the risks of dying in the two treatment groups (Mantel, 1966; Pet0 et al., 1977) and its 95% confidence limits (Bernstein et al., 1979).
When the survival data are examined the estimated hazard ratio is 0.88, indicating a slight disadvantage for chemotherapy. The 2-year surviv- al rate in the control group is approximately SO%, and this hazard ratio indicates a difference of 4% in the 2-year survival, to the disadvantage of the chemotherapy group. The lower 95% confidence limit gives a 22% disadvantage to chemotherapy, and the upper 95% limit a 12% advantage. Put differently, it is unlikely, given the figures obtained in this study, that the addition of chemotherapy would have been shown to raise the 2-year survival rate by 12% to 62% if an infinitely large number of patients had been examined; and it is no more, and no less, unlikely that it might have lowered it to 28%.
Some caution is required in the interpretation of these figures because the hazard ratio is calculated on the assumption that the risks of dying in the two groups are in constant proportion as time from
treatment elapses. In fact, the graph of survival rates indicates that this assumption may not hold, there being proportionately more early deaths (within 6 months of entry) in the chemotherapy group than in the control group and a gradual swing in the opposite direction between 6 and 18 months. As a result, the above analysis might slightly overestimate the disadvantage at 2 years. The overestimation cannot be gross, but might amount to a few percentage points.
When the “disease-free’’ data are examined the estimated hazard ratio is 0.94. This is equivalent to a disadvantage to the chemotherapy group of 2% with confidence limits of -21% and + 19%.
It is difficult to agree on the improvement in results which would be necessary before it would be justified to use adjuvant chemotherapy. The major- ity of investigators in this study, interviewed after the study had been closed to patient entry, felt that the small chance of a 12% improvement in survival was not sufficient to justify it, especially when there was an equal chance of a 22% deterioration.
The 3-year and 5-year survival figures of 35% and 28% quoted in this study are not adjusted for the expected mortality from causes other than bladder cancer, and would be higher if they had been. They are comparable with results obtained in previous studies (Wallace and Bloom, 1976; Bloom et al., 1982) and, if corrected, would fall between the survival curves obtained after radiotherapy alone and after radiotherapy and cystectomy in the London T3 bladder carcinoma trial (Bloom et al., 1982).
It is possible that the lack of effectiveness of the chemotherapy used in the present trial was because the dose was too small; because the drug combina- tion is insufficiently active to eliminate microme- tastases ; or because micrometastases are not-as has been supposed-particularly susceptible to chemotherapy. Perhaps chemotherapy should be given as first treatment in future studies. Whatever the reason, it is clear that there is unlikely to be any improvement in results when chemotherapy, as given in the present study, is added to radiotherapy.
Acknowledgement The Yorkshire Urology Cancer Research Group is supported by the Yorkshire Regional Cancer Organisation.
References Bernstein, L., Anderson, J. and Pike M. C. (1979). Estimation of
the proportion of hazard in two treatment group clinical trials. Biometrics, 37, 163-170.

ADJUVANT CHEMOTHERAPY WITH DOXORUBICIN 39 1
Bloom, H. J. G., Hendry, W. F., Wallace, D. M. and Skeet, R. G. (1982). Treatment of T3 bladder cancer: controlled trial of pre-operative radiotherapy in radical cystectomy versus radical radiotherapy. British Journal of Urology, 54, 136-151.
Cross, R. J., Glashan, R. W., Humphrey, C. S., Robinson, M. R. G., Smith, P. H. and Williams, R. E. (1976). Treatment of advanced bladder cancer with adriamycin and 5-fluorouracil. British Journal of Urology, 48, 609-615.
EORTC Urological Group B (1977). The treatment of advanced carcinoma of the bladder with a combination of adriamycin and 5-fluorouracil. European Urology, 3, 276-278.
Glashan, R. W., Houghton, A. L. and Robinson, M. R. G. (1977). A toxicity study of the treatment of T3 bladder tumours with a combination of radiotherapy and chemotherapy. British Journal of Urology, 49, 669-672.
Lindholm, C. E., Mattsson, W., Langeland, T. and Gynning, I. (1980). 5-fluorouracil and adriamycin in locally recurrent and/ or metastatic bladder cancer. In Bladder Tumours and other Topics in Urological Oncology, ed. Pavone-Macaluso, M., Smith, P. H. and Edsmyr, F. pp. 391-394. New York: Plenum Press.
Mantel, N. (1966). Evaluationof survivaldata and twonew rank order statistics arising in its consideration. Cancer Chemo- therapy Reports, 50, 163-170.
Miller, L. S. (1977). Bladder cancer: superiority of pre-operative irradiation in cystectomy in stages B2 and C. Cancer, 39,973- 980.
Peto, R., Pike, M. C., Armitage, T., Breslow, N. E., Cox, D. R., Howard, S. V., Mantel, N., McPherson, K., Peto, J. andsmith, P. G. (1977). Design and analysis of randomised clinical trials requiring prolonged observation of each patient. British Journal of Cancer, 35, 1-39.
Prout, G. R. (1977). The role of surgery in the potentially curative treatment of bladder carcinoma. Cancer Research,
Reuben, P. (1971). Current concepts in genito-urinary oncology: a multi-disciplinary approach. Journal of Urology, 106, 31 5- 338.
Rider, W. D. and Evans, D. H. (1976). Radiotherapy in the treatment of recurrent bladder cancer. British Journal of Urology, 48, 595-601.
Smith, J. A. and Whitmore, W. F. (1981). Regional lymph node metastases from bladder cancer. Journalof Urology, 126,591- 593.
37, 2764-2770.
UICC Union Internationale Contre le Cancer (1978). TNM Classijicaiion of Malignant Tumours. Third edition. Geneva : International Union against Cancer.
Veronesi, A., Magri, M. D., Figoli, F., Tuelli, U., Galligioni, E., Trovo, M. G., Merlo, A., Dal Bo, V., Tumulo, S. and Grigoletto, E. (1982). Combination chemotherapy with adriamycin and 5-fluorouracil in advanced carcinoma. Clinical Oncology, 8, 103-106.
Wallace, D. M. and Bloom, H. J. G. (1976). The management of deeply infiltrating (T3) bladder carcinoma : controlled trial of radical radiotherapy versus preoperative radiotherapy in radical cystectomy. British Journal of Urology, 48, 587-594.
Whitmore, W. F., Batata, M. A., Ghoneim, M. A., Grabstald, H. and Unal, A. (1977a). Radical cystectomy with or without prior irradiation in the treatment of bladder cancer. Journal of Urology, 118, 184-187.
Whitmore, W. F., Batata, M. A., Hdaris, B. S., Ready, G. N., Unal, A., Ghoneim, M. A., Grabstald, H. and Chu, F. (1977b). A comparative study of 2 pre-operative radiation regimes with cystectomy for bladder cancer. Cancer, 40, 1077-1086.
The Authors B. Richards, MD, MB,BChir, FRCS, Consultant Urologist,
J. R. G. Bastable, ChM, MB,ChB, FRCS, Consultant Urol-
L. Freedman, MA, DipStats, Medical Statistician, MRC
R. W. Glashan, MB,ChB, FRCSE, FRCS(Glas), Consultant
Glynis Harris, Data Manager, York District Hospital. D. W. W. Newling, MB,BChir, FRCS, Consultant Urologist,
M. R. G. Robinson, MB,BS, FRCS, Consultant Urologist,
P. H. Smith, MB,ChB, FRCS, Consultant Urologist, St James’s
York District Hospital.
ogist, York District Hospital.
Cancer Trials Office
Urologist, Huddersfield Royal Infirmary.
Hull Royal I n h a r y (Sutton).
Pontefract General Infirmary.
University Hospital.
Requests for reprints to: B. Richards, Department of Urology, York District Hospital, Wigginton Road, York YO3 7HE.