adjuvant therapy for pancreatic cancer: is …...– apact is the first adjuvant trial in pancreatic...
TRANSCRIPT

1
Adjuvant Therapy for Pancreatic Cancer: Is mFOLFIRINOX the New Standard?
Bassel F. El-Rayes, M.D.
Professor and Vice Chair
Director of the GI Oncology Program
Associate Cancer Center Director
Winship Cancer Institute of Emory University
Atlanta, Ga.

2
What is the Data Supporting FOLFIRINOX as Adjuvant Therapy?

3Winship Cancer Institute | Emory University
PRODIGE 24/CCTG PA.6 Trial: Study Design
Presented by Thierry Conroy ASCO 2018; published in NEJM Dec 20, 2018.
Stratification: • Center
• Resection margin (R0 vs R1)
• CA19-9 level (≤ 90 vs 91-179 U/mL)
• pN0 (< 12 vs ≥ 12 examined nodes)
vs pN1
R0 or R1 resected
pancreatic cancer
Postoperative
CT-scan mandatory
CA19-9 level < 180 U/mL
within 12 weeks
after surgery
R
A
N
D
O
M
I
Z
E
- 6 months of chemotherapy- CT scans: every 3 months
NCT01526135 mFOLFIRINOXOxaliplatin 85 mg/m², leucovorin 400 mg/m²,
Irinotecan 180 mg/m²*, all at D1
Fluorouracil continuous IV infusion 2.4 g/m² over
46 hours
Every 2 weeks; 12 cycles *Reduced to 150 mg/m² after patient 162
Gemcitabine1000 mg/m2, qw 3/4 weeks;
6 cycles
For both arms:
1:1
CT = computed tomography; IV = intravenous

4Winship Cancer Institute | Emory University
Key Inclusion Criteria
• Histologically confirmed resected pancreatic ductal adenocarcinoma
• Macroscopically complete resection (R0 or R1 resection)
• Patients able to receive chemotherapy within 12 weeks after resection
• ECOG PS 0-1
• Ages 18 to 79 years
• No prior radiotherapy or chemotherapy
• Adequate hematologic/blood chemistry levels
• Patient information and written informed consent
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.
ECOG PS = Eastern Cooperative Oncology Group Performance Status

5Winship Cancer Institute | Emory University
Key Exclusion Criteria
• Metastatic disease or macroscopic incomplete tumor removal (R2 resection)
• Postoperative CA 19-9 ≥ 180 U/ml assessed within 21 days of randomization
• Symptomatic heart failure or coronary heart disease
• Major comorbidity, active infection, history of HIV, or uncontrolled diabetes
• Inflammatory bowel disease, or occlusion or subocclusion of the intestine, or severe
postoperative uncontrolled diarrhea
• Concomitant occurrence of another cancer or significant history of cancer
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.

6Winship Cancer Institute | Emory University
Endpoints
Primary: DFS
Secondary:
• Toxicity (NCI-CTC version 4.0 grading)
• OS
• Cancer SS
• MFS
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.
DFS = disease-free survival; MFS = metastasis-free survival; OS = overall survival; SS = specific survival

Baseline Characteristics: Patients
CharacteristicmFOLFIRINOX
N = 247
Gemcitabine
N = 246P
Median age (years)
[range]
63
[30-79]
64
[30-81].09
Gender male 57.5 % 55.6 % .67
ECOG PS 0
1
49.8 %
50.2 %
52.5 %
47.5 %
.55
Diabetes 25.3 % 26.6 % .44
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.

Baseline Characteristics: Pancreatic Tumors
CharacteristicsmFOLFIRINOX
N = 247
Gemcitabine
N = 246P
Median size of primary tumor [mm, range] 30 [8-90] 30 [6-120] .50
T1-2/T3-4 (%) 12.5/87.5 9.8 /90.2 .33
N0/N1 (%) 22.3 /77.7 24.5 /75.5 .60
Stage: I/IIA/IIB/III-IV (%) 4.9/17.4 /74.1/3.6 5.7/19.1 /72.8/2.4 .81
Tumor grading :
well/moderately/poorly differentiated (%)30.6/54.1/15.3 33.9/53.7/12.5 .58
Whipple resection procedure (%) 82.1 76.8 .53
R1 resection (%) 40.1 45.7 .24
Venous resection (%) 21.3 28.2 .08
Lymphovascular emboli (%) 73.7 63.1 .02
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.
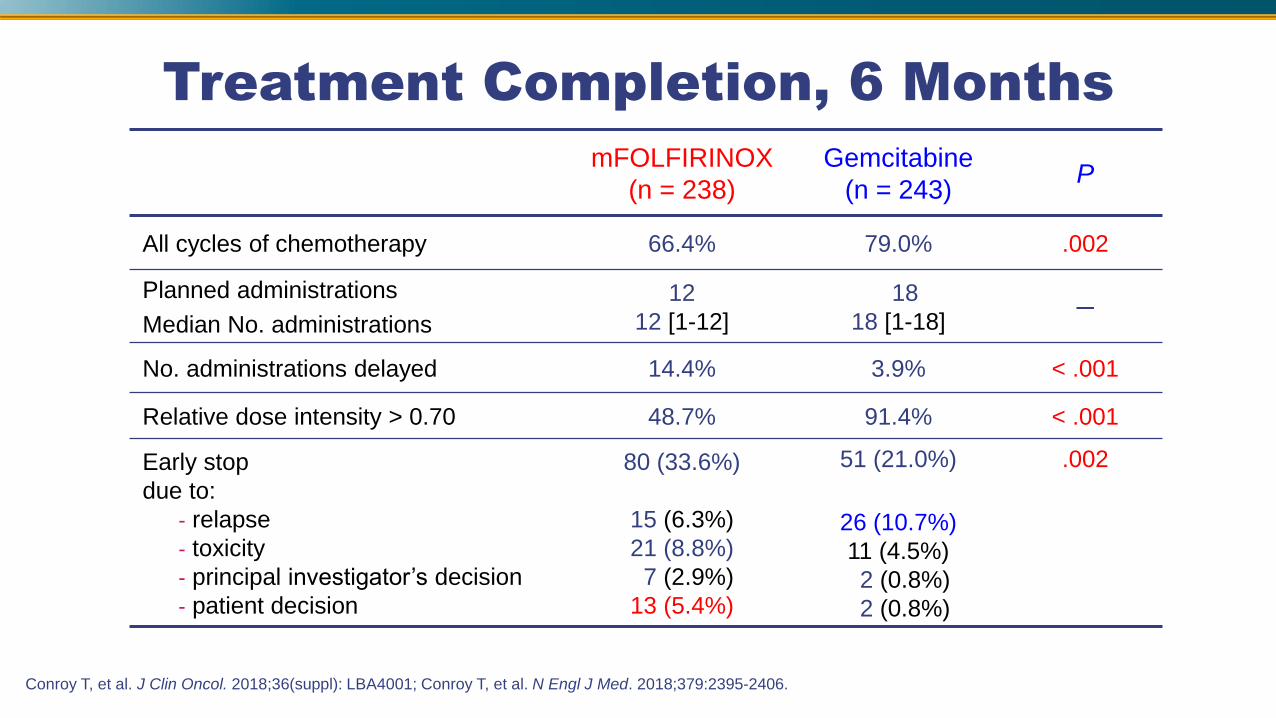
Treatment Completion, 6 Months
mFOLFIRINOX
(n = 238)
Gemcitabine
(n = 243)P
All cycles of chemotherapy 66.4% 79.0% .002
Planned administrations
Median No. administrations
12
12 [1-12]
18
18 [1-18]─
No. administrations delayed 14.4% 3.9% < .001
Relative dose intensity > 0.70 48.7% 91.4% < .001
Early stop
due to:
- relapse
- toxicity
- principal investigator’s decision
- patient decision
80 (33.6%)
15 (6.3%)
21 (8.8%)
7 (2.9%)
13 (5.4%)
51 (21.0%)
26 (10.7%)
11 (4.5%)
2 (0.8%)
2 (0.8%)
.002
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.

10Winship Cancer Institute | Emory University
Disease-Free Survival
0.00
0.25
0.50
0.75
1.00
Dis
ease
-fre
e s
urv
iva
l
247 210 156 118 80 60 46 29 21 11 2B:mFolfirinox
246 205 127 85 59 34 24 15 10 7 3A:Gemcitabine
Number at risk
0 6 12 18 24 30 36 42 48 54 60
Time (months)
A :Gemcitabine B:mFolfirinox
HR=0.58 CI95%[0.46-0.73]Stratified HR = 0.58 [95%CI: 0.46-0.73],
P < .0001
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.
No DFS events: 314
Median DFS:• 21.6 months [95% CI: 17.7-27.6]
with mFOLFIRINOX
• 12.8 months [95% CI: 11.7-15.2]
with gemcitabine
3-year DFS: • 39.7% [95% CI: 32.8-46.6]
with mFOLFIRINOX
• 21.4% [95% CI: 15.8-27.5]
with gemcitabine
CI = confidence interval; HR = hazard ratio

11Winship Cancer Institute | Emory University
Overall SurvivalMedian overall survival:
• 54.4 months [95% CI: 41.8–NR]
with mFOLFIRINOX
• 35.0 mos [95% CI: 28.7–43.9]
with gemcitabine
3-year overall survival:
No OS events = 192
• 63.4% (mFOLFIRINOX) vs
48.6 % gemcitabine
0.00
0.25
0.50
0.75
1.00
Overa
ll su
rviv
al
247 223 210 165 119 91 68 46 32 16 4B:mFolfirinox
246 233 215 171 120 81 55 33 18 9 4A:Gemcitabine
Number at risk
0 6 12 18 24 30 36 42 48 54 60
Time (months)
A :Gemcitabine B:mFolfirinox
HR=0.64 CI95%[0.48-0.86]Stratified HR = 0.64,
[95%CI: 0.48-0.86], P = .003
Conroy T, et al. J Clin Oncol. 2018;36(suppl): LBA4001; Conroy T, et al. N Engl J Med. 2018;379:2395-2406.
NR = not reached

12
What Other Options Are Available for Adjuvant Therapy?
13Winship Cancer Institute | Emory University
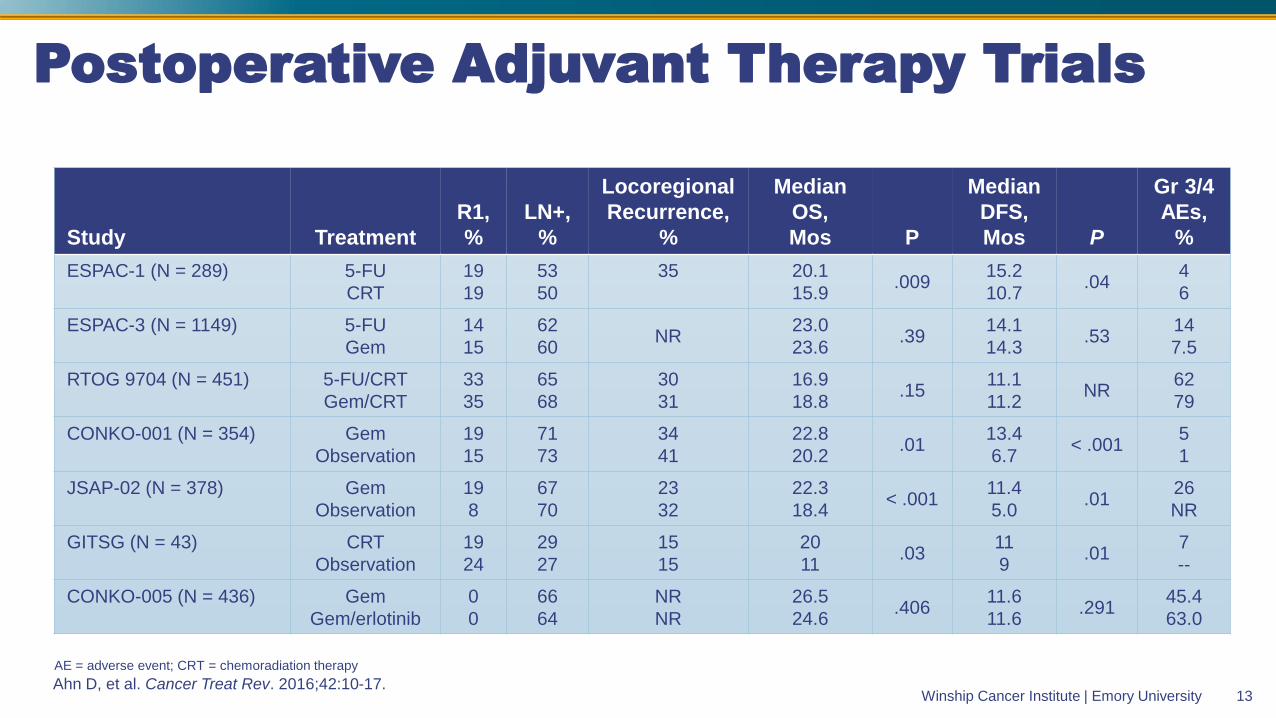
Postoperative Adjuvant Therapy Trials
Ahn D, et al. Cancer Treat Rev. 2016;42:10-17.
Study Treatment
R1,
%
LN+,
%
Locoregional
Recurrence,
%
Median
OS,
Mos P
Median
DFS,
Mos P
Gr 3/4
AEs,
%
ESPAC-1 (N = 289) 5-FU
CRT
19
19
53
50
35 20.1
15.9.009
15.2
10.7.04
4
6
ESPAC-3 (N = 1149) 5-FU
Gem
14
15
62
60NR
23.0
23.6.39
14.1
14.3.53
14
7.5
RTOG 9704 (N = 451) 5-FU/CRT
Gem/CRT
33
35
65
68
30
31
16.9
18.8.15
11.1
11.2NR
62
79
CONKO-001 (N = 354) Gem
Observation
19
15
71
73
34
41
22.8
20.2.01
13.4
6.7< .001
5
1
JSAP-02 (N = 378) Gem
Observation
19
8
67
70
23
32
22.3
18.4< .001
11.4
5.0.01
26
NR
GITSG (N = 43) CRT
Observation
19
24
29
27
15
15
20
11.03
11
9.01
7
--
CONKO-005 (N = 436) Gem
Gem/erlotinib
0
0
66
64
NR
NR
26.5
24.6.406
11.6
11.6.291
45.4
63.0
AE = adverse event; CRT = chemoradiation therapy

14Winship Cancer Institute | Emory UniversityOettle H, et al. JAMA. 2013;310:1473-1481.
CONKO 001: Gemcitabine vs Observation in Patients With Resected Pancreatic Cancer

15Winship Cancer Institute | Emory University
Median DFS
Gemcitabine: 13.4 months (95% CI, 11.6-15.3)
Observation: 6.7 months (95% CI, 6.0-7.5)
Hazard ratio, 0.55 (95% CI, 0.44-0.69)
Oettle H, et al. JAMA. 2013;310:1473-1481.
CONKO-001: DFS and OS
Median OS
Gemcitabine: 22.8 months (95% CI, 18.5-27.2)
Observation: 20.2 months (95% CI, 17.7-22.8)
Hazard ratio, 0.76 [95% CI, 0.61-0.95]
DFS OS

16Winship Cancer Institute | Emory UniversityNeoptolemos J, et al. Lancet. 2017;389:1011-1024.
ESPAC 4: Gemcitabine vs Gemcitabine Capecitabine in Resected Pancreatic Cancer

17Winship Cancer Institute | Emory University
ESPAC-4: Survival by Treatment
Neoptolemos J, et al. Lancet. 2017;389:1011-1024.

18Winship Cancer Institute | Emory UniversityNeoptolemos J, et al. Lancet. 2017;389:1011-1024.
ESPAC-4: Survival by Treatment

Abstract 4000
APACT: Phase III, Multicenter, International, Open-Label, Randomized
Trial of Adjuvant nab-Paclitaxel Plus Gemcitabine vs Gemcitabine for Surgically
Resected Pancreatic Adenocarcinoma
Margaret A. Tempero,1 Michele Reni,2 Hanno Riess,3 Uwe Pelzer,3 Eileen M. O’Reilly,4 Jordan Winter,5
Do-Youn Oh,6 Chung-Pin Li,7 Giampaolo Tortora,8,9 Heung-Moon Chang,10 Charles D. Lopez,11
Josep Tabernero,12 Eric Van Cutsem,13 Philip Philip,14 David Goldstein,15 Jordan D. Berlin,16
Stefano Ferrara,17 Mingyu Li,17 Brian Lu,17 Andrew Biankin18

20Winship Cancer Institute | Emory University
APACT: Study Design
*No prior neoadjuvant, radiation, or systemic therapy
Phase III, multicenter, international, open-label, randomized trial
Patients ≥ 18 years of
age with confirmed
resected PDAC
(T1-3, N0-1, M0);
R0/R1; ECOG PS 0
or 1; CT without
evidence of disease
CA19-9 < 100 U/mL;
no prior therapy*
Ran
dom
ized 1
:1
Follow-up
Radiological evaluation
for ≤ 5 years after
last dose or until
recurrence, new cancer
therapy, or death; safety
assessment for 28 days
after last dose
nab-P + gem
nab-P 125 mg/m2 q w 3/4 +
Gem 1000 mg/m2 q w 3/4
× 6 cycles
Gem
Gem 1000 mg/m2 q w 3/4
× 6 cycles
End of treatment
Treat for 6 cycles
unless recurrence,
death, unacceptable
toxicity, consent
withdrawal, or
patient/physician
decision
• Randomized as early as possible after adequate recovery from surgery, but no later than 12 weeks
after surgery
• Stratification: resection status (R0 vs R1); lymph node status (LN+ vs LN−); geographic region (North
America, Europe, and Australia vs Asia Pacific)
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.
LN = lymph node; PDAC = pancreatic ductal adenocarcinoma

21Winship Cancer Institute | Emory University
APACT: Statistical Design
Sample Size and Power Considerations
Endpoint nab-P + gem Gem
Primary (independently assessed DFS)
Median, months 18.5 13.5
HR for disease recurrence or death 0.73
Events required for 90% power at 2-sided α of 0.05, n 438
Secondary (OS)
Events to be analyzed as supportive analysis, n ≈ 630
Type 1 error control for OS None
• Primary endpoint: independently assessed DFS
– APACT is the first adjuvant trial in pancreatic ductal adenocarcinoma to use independently
assessed DFS as the primary endpoint
– Central review was conducted by radiologists not involved in the trial without clinical or
laboratory data
• Secondary endpoints: OS; safety
• Exploratory endpoints: Tumor & blood biomarker analysis; quality of life
• Prespecified sensitivity analyses included: investigator-assessed DFS
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.
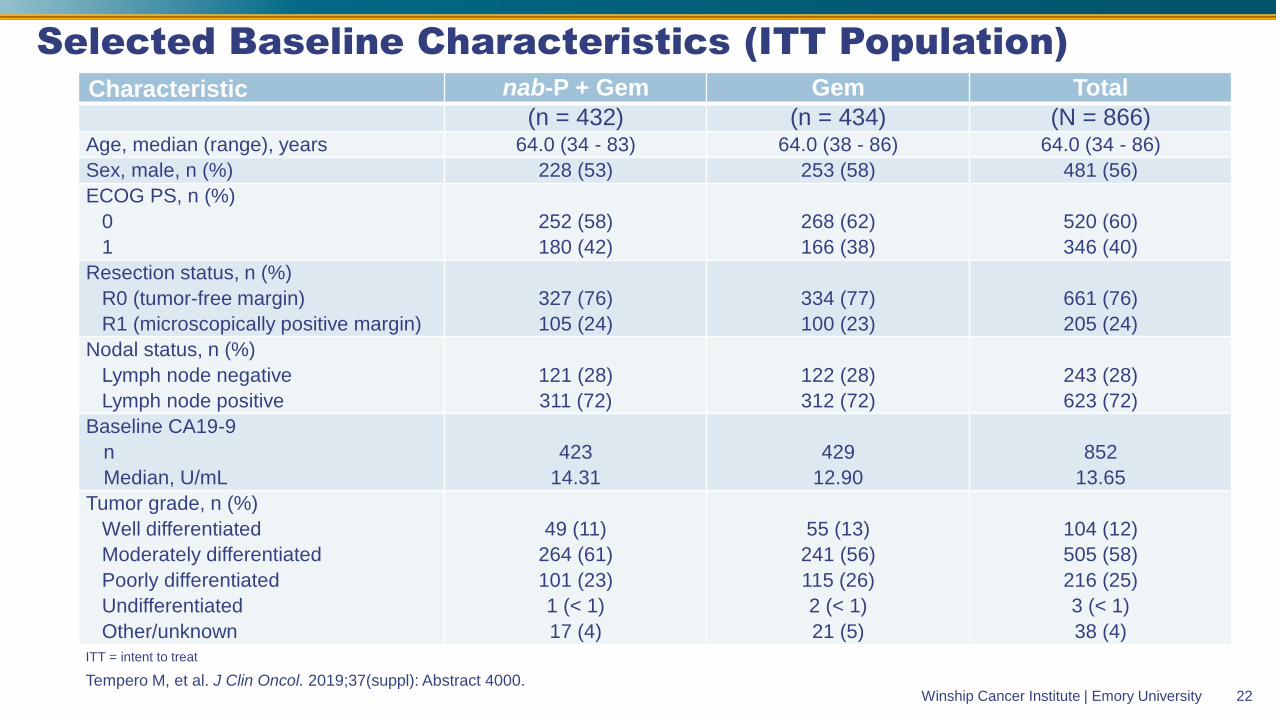
22Winship Cancer Institute | Emory University
Selected Baseline Characteristics (ITT Population)Characteristic nab-P + Gem Gem Total
(n = 432) (n = 434) (N = 866)Age, median (range), years 64.0 (34 - 83) 64.0 (38 - 86) 64.0 (34 - 86)
Sex, male, n (%) 228 (53) 253 (58) 481 (56)
ECOG PS, n (%)
0
1
252 (58)
180 (42)
268 (62)
166 (38)
520 (60)
346 (40)
Resection status, n (%)
R0 (tumor-free margin)
R1 (microscopically positive margin)
327 (76)
105 (24)
334 (77)
100 (23)
661 (76)
205 (24)
Nodal status, n (%)
Lymph node negative
Lymph node positive
121 (28)
311 (72)
122 (28)
312 (72)
243 (28)
623 (72)
Baseline CA19-9
n
Median, U/mL
423
14.31
429
12.90
852
13.65
Tumor grade, n (%)
Well differentiated
Moderately differentiated
Poorly differentiated
Undifferentiated
Other/unknown
49 (11)
264 (61)
101 (23)
1 (< 1)
17 (4)
55 (13)
241 (56)
115 (26)
2 (< 1)
21 (5)
104 (12)
505 (58)
216 (25)
3 (< 1)
38 (4)
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.
ITT = intent to treat

23Winship Cancer Institute | Emory University
Treatment Exposure and Dose Modifications (Treated Population)
Parameters nab-P + Gem Gem
Treatment exposure (n = 429) (n = 423)
Treatment duration, median (range), weeks 24.0 (0.7 - 33.0) 24.0 (1.3 - 31.9)
Treatment cycles, median (range), n 6.0 (1 - 6) 6.0 (1 - 6)
nab-P Gem
Relative dose intensity, median, % 75.1 80.0 91.2
Cumulative dose, median, mg/m2 1500 13,200 15,000
Dose modifications
Patients with ≥ 1 dose reduction, n (%) 273 (64) 266 (62) 213 (50)
• Overall, 69% of patients completed 6 treatment cycles (nab-P + gem, 66%; gem, 71%)
• 59% of patients on nab-P + gem received dosing of nab-P in cycle 6
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.

24Winship Cancer Institute | Emory University
Primary Endpoint:Independently Assessed DFS (ITT Population)
24
Median independently assessed DFS
nab-P + gem: 19.4 months
Gem: 18.8 months
(HR 0.88; 95% CI, 0.729 - 1.063; stratified log-rank P = .1824)
Number of events: 439
0
10
20
30
40
50
60
70
80
90
100
Pro
ba
bil
ity o
f D
FS
, %
30 6 9 12 18 21 24 30 33 36 39 42 484515 27 51 54
MonthsPatients at risk
391
368
432
434
338
309
279
235
236
183
167
147
138
127
121
116
99
98
88
88
54
59
43
42
20
15
2
1
14
10
204
157
112
105
2nab-P + Gem
Gem
nab-P + gem
Gem
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.

25Winship Cancer Institute | Emory University
Prespecified Sensitivity Analysis: Investigator Assessed DFS (ITT Population)
Median investigator assessed DFS
nab-P + Gem: 16.6 months
Gem: 13.7 months
(HR 0.82; 95% CI, 0.694 - 0.965; nominal P = .0168)
Number of events: 571
0
10
20
30
40
50
60
70
80
90
100
Pro
ba
bil
ity o
f D
FS
, %
30 6 9 12 18 21 24 30 33 36 39 42 484515 27 51 54
Months
406
384
432
434
355
330
287
247
246
202
183
159
160
142
141
127
118
106
98
92
59
59
46
42
24
14
2
1
16
9
216
175
128
116
2
nab-P + gem
Gem
Patients at risk
nab-P + Gem
Gem
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.

26Winship Cancer Institute | Emory University
Secondary Endpoint:Interim OS (ITT population)
26
Median interim OS (68% mature)
nab-P + gem: 40.5 months
Gem: 36.2 months
(HR 0.82; 95% CI, 0.680 - 0.996; nominal P = .045)
Number of events: 427; Median follow-up, 38.5 months
0
10
20
30
40
50
60
70
80
90
100
Months
Pro
ba
bil
ity o
f O
S, %
30 6 9 12 18 21 24 30 33 36 39 42 484515 27 51 54 57
427
415
432
434420
404
406
384
385
354
344
301
307
275
284
262
252
228
219
198
162
153
113
101
73
64
12
12
40
29
366
320
264
249
3
2 1
Patients at risk
nab-P + Gem
Gem
nab-P + gem
Gem
Tempero M, et al. J Clin Oncol. 2019;37(suppl): Abstract 4000.

27Winship Cancer Institute | Emory University
Safety (Treated Population)
Event, n (%) nab-P + Gem Gem
Safety summary (n = 429) (n = 423)
Patients with ≥ 1 grade ≥ 3 TEAE 371 (86) 286 (68)
Patients with ≥ 1 serious TEAE 176 (41) 96 (23)
Grade ≥ 3 hematologic TEAEs (occurring in ≥ 5% of patients in either treatment arm)
Any hematologic TEAEs 250 (58) 204 (48)
Neutropenia 212 (49) 184 (43)
Anemia 63 (15) 33 (8)
Leukopenia 36 (8) 20 (5)
Febrile neutropenia 21 (5) 4 (1)
Grade ≥ 3 nonhematologic TEAEs (occurring in ≥ 5% of patients in either treatment arm)
Peripheral neuropathy (SMQ)* 64 (15) 0
Fatigue 43 (10) 13 (3)
Diarrhea 22 (5) 4 (1)
Asthenia 21 (5) 8 (2)
Hypertension 17 (4) 27 (6)
*Reported as a group term.
MedDRA = Medical Dictionary for Regulatory Activities; SMQ = standardized MedDRA query; TEAE = treatment-emergent adverse event.
• TEAEs led to death in 2 patients in each arm
• Ten patients (16%) with grade ≥ 3 peripheral neuropathy improved to grade ≤ 1
• The incidence of TEAEs of special interest—gastrointestinal events, hepatic toxicity, and sepsis—was generally low in
both arms

28Winship Cancer Institute | Emory University
Conclusions
• The outcome of the gemcitabine single-agent arm has improved over time
– Better supportive care and patient selection
• mFOLFIRINOX is a very effective adjuvant therapy regimen with median OS in the range of 54 months and HR 0.64
– This regimen needs to be considered standard of care for patients with good performance status and who have recovered well post operatively
• Gemcitabine-based regimens have activity and should be considered standard for patients with borderline PS or prolonged recovery from surgery
– Gemcitabine capecitabine or gemcitabine nab-paclitaxel for patients with moderate PS (HR 0.8)
– Single-agent gemcitabine for patients with poor PS

29Winship Cancer Institute | Emory University
Thanks