adjuvant treatment of locally advanced head and ... - … · adjuvant treatment of locally advanced...
TRANSCRIPT

Adjuvant Treatment ofLocally Advanced Head
and Neck Cancer
Prof. Dr. Mahmut ÖzşahinLausanne University Medical Center (CHUV)
Switzerland

[email protected]+41 21 314 4603

Is Surgery + Postop RT Better ThanIs Surgery + Postop RT Better ThanConcurrent ChemoRT Without Surgery ?Concurrent ChemoRT Without Surgery ?
DFS, p = NS OS, p = NS

Historical Evaluation of Treatment OutcomeHistorical Evaluation of Treatment Outcomein High-Risk Resected Diseasein High-Risk Resected Disease
Historical cohorts Historical cohorts
L-R failureL-R failure ~ 25-60%~ 25-60%
Distant failureDistant failure ~ 15-25% ~ 15-25%
5-year OS5-year OS ~ 25-35% ~ 25-35%

Some MilestonesSome Milestonesof Pure Radio-Surgical Associationsof Pure Radio-Surgical Associations
First Evidence: Paper by Fletcher & Evers, 1970First Evidence: Paper by Fletcher & Evers, 1970
Higher doses to high-risk patients (R+):Higher doses to high-risk patients (R+):Marcus et al, 1979Marcus et al, 1979
Preop Preop vs.vs. postop setting, Tupchong et al, 1991 postop setting, Tupchong et al, 1991
Fletcher GH, Radiol 95, 185, 1970Fletcher GH, Radiol 95, 185, 1970Marcus RB, IJROBP, 5, 1943, 1979Marcus RB, IJROBP, 5, 1943, 1979Tupchong L, IJROBP, 20, 21, 1991Tupchong L, IJROBP, 20, 21, 1991

Preop Preop vsvs. Postop ?. Postop ?
Randomized study of preoperative vs.Randomized study of preoperative vs.postoperative radiation therapy in advanced headpostoperative radiation therapy in advanced headand neck carcinoma: long-term follow-up ofand neck carcinoma: long-term follow-up ofRTOG study 73-03RTOG study 73-03
POSTOP RT IS BETTER!
Tupchong et al, IJROBP 1991

Impact on Risk Factors on Postop RT OutcomeImpact on Risk Factors on Postop RT Outcomein Resectable H&N Cancerin Resectable H&N Cancer
Low-riskLow-riskno need for postop RTno need for postop RT Peters LJ, IJROBP 1993 Peters LJ, IJROBP 1993(5-yr LRC: 90%; OS: 83%)(5-yr LRC: 90%; OS: 83%)
Intermediate-riskIntermediate-risk(one adverse feature other than(one adverse feature other than ECE): ECE):LRC = 94% for <60 GyLRC = 94% for <60 Gy
High-riskHigh-risk(ECE + or 2+ adverse features):(ECE + or 2+ adverse features):5-yr LRC 68% even if doses >60 Gy5-yr LRC 68% even if doses >60 Gy

What postoperativeWhat postoperative
treatment fortreatment for
high-risk patients?high-risk patients?

Key Messages from the RTOG 8503 StudyKey Messages from the RTOG 8503 Study
•• High-risk patients with resectable diseaseHigh-risk patients with resectable diseasebenefit more adjuvant CT but differences arebenefit more adjuvant CT but differences arenot significant in terms of LRC and OSnot significant in terms of LRC and OScompared to postop RTcompared to postop RT
•• Patterns of failure modified by adjuvant CT:Patterns of failure modified by adjuvant CT:less nodal failures and distant metastasesless nodal failures and distant metastases
LLaramore et al, IJROBP 1991aramore et al, IJROBP 1991

Chemoradiation: RationaleChemoradiation: Rationale
•• To overcome radioresistanceTo overcome radioresistance
•• To increase local controlTo increase local control
•• To eradicate systemic micro metsTo eradicate systemic micro mets

EORTC 22931 and RTOG 9501EORTC 22931 and RTOG 9501Two Major Postop TrialsTwo Major Postop Trials
EORTC Trial 22931EORTC Trial 22931
Mainly based on Peters et al.Mainly based on Peters et al.
Stage III or IV diseaseStage III or IV diseaseOral cavity and oropharynx SCC with LN+ atOral cavity and oropharynx SCC with LN+ at
level IV or Vlevel IV or VVascular embolismsVascular embolismsPerineural diseasePerineural diseaseExtracapsular N spreadExtracapsular N spreadPositive surgical marginsPositive surgical margins
Peters et al, IJROBP 1993Peters et al, IJROBP 1993
RTOG Trial 9501RTOG Trial 9501
Gained from INT 0034-RTOG 8503Gained from INT 0034-RTOG 8503
2+ lymph nodes2+ lymph nodesExtracapsular N spreadExtracapsular N spreadPositive surgical marginsPositive surgical margins
Laramore et al, IJROBP 1991Laramore et al, IJROBP 1991

EORTC Study 22931EORTC Study 22931
A phase III randomized study on postoperativeA phase III randomized study on postoperativeradio- and chemotherapy in patients with locallyradio- and chemotherapy in patients with locally
advanced head and neck carcinomaadvanced head and neck carcinoma
•• Joint ProtocolJoint Protocol Head & Neck and Radiotherapy GroupsHead & Neck and Radiotherapy Groups
•• Date of activationDate of activation February 1994February 1994
•• Date of closureDate of closure October 2000October 2000
•• Patient accruedPatient accrued 334334


Eligibility CriteriaEligibility Criteria
♦♦ Histologically confirmed squamous-cell carcinomaHistologically confirmed squamous-cell carcinoma
♦♦ Primary surgery performed with curative intentPrimary surgery performed with curative intent
♦♦ Oral cavity, oropharynx, hypopharynx, and larynxOral cavity, oropharynx, hypopharynx, and larynx
♦♦ T3-4 any N T3-4 any N oror T1-2, N2-3, M0 T1-2, N2-3, M0 oror T1-2, N0-1 + high risk factor* T1-2, N0-1 + high risk factor*
♦♦ No distant metastases at the time of diagnosisNo distant metastases at the time of diagnosis
♦♦ Age between 18 and 70 yearsAge between 18 and 70 years
♦♦ PS 0-2 (WHO scale)PS 0-2 (WHO scale)
♦♦ Normal hematological, liver, and kidney functionNormal hematological, liver, and kidney function
♦♦ Informed consentInformed consent
♦♦ **insufficient resection margins, perineural involvement, vascularinsufficient resection margins, perineural involvement, vascularembolisms, or capsular rupture in neck nodesembolisms, or capsular rupture in neck nodes

Treatment SchemeTreatment Scheme
Postop XRT
66 Gy / 33 fr / 6.5 wks
Postop XRT
66 Gy / 33 fr / 6.5 wks
DDP 100 mg/m2 d 1, 22, 43
Randomize
Primary surgery
Primary endpoint Disease-free survival
Secondary endpoints Overall survival, Local control, Tolerance, Late complications

RecruitmentRecruitment
Institution Total Institution Total
Villejuif 9 1 Brussels – VU B 6
Lausanne 3 6 Brno 6
Gdansk 2 8 Zürich 5
Lille – C.O.L. 2 2 Düsseldorf 5
Bern 2 1 Ljubljana 5
Barcelona – H.V.H . 1 9 Glasgow 5
Grenoble 1 4 Rouen 3
Dijon - C.G.L 1 4 Nottingham 3
Nantes 1 4 Poitiers 2
Bellinzona 1 4 Nijmege n 2
Milano – I.N.T. 9 Izmir 2
Roma – I.R.E. 8 Total 334

T-classificationT-classification
T-classificat ion XRT XRT+DDP Total
T 1 16 (10%) 10 (6%) 27 (8%)
T 2 45 (27%) 38 (23%) 83 (25%)
T 3 50 (30%) 48 (29%) 98 (29%)
T 4 54 (32%) 69 (41%) 123 (37% )
No unbalance for age, sex, N stage, tumorNo unbalance for age, sex, N stage, tumordifferentiation, resection margins, or ECE +differentiation, resection margins, or ECE +

Main Site of Primary TumorMain Site of Primary Tumor

Surgical MarginsSurgical Margins

Number of Involved NodesNumber of Involved Nodes

Extranodal SpreadExtranodal Spread

Time Interval Between Surgery and RTTime Interval Between Surgery and RT

RT Dose Distribution (< 60 Gy)RT Dose Distribution (< 60 Gy)
Total dose
XR T XRT+DDP Total
55-59 Gy 1 1 2
50-54 Gy 4 4 8
< 50 Gy 2 3 5
«« On scheduleOn schedule » »: : Arm 1: 73.3%Arm 1: 73.3%
Arm 2: 75.2%Arm 2: 75.2%

Compliance with ChemotherapyCompliance with Chemotherapy
Cycle #Cycle # DoseDosereductionreduction
CourseCourseDelayedDelayed
BothBoth NotNotfullyfullygivengiven
FullyFullyCompletedCompleted
11 33 -- -- ---- 1717 147 (88%)147 (88%)
22 ---- 2121 22 1818 110 (66%)110 (66%)
33 33 2222 ---- 2525 82 (49%)82 (49%)

RESULTSRESULTS

Progression-Free SurvivalProgression-Free Survival(Primary Endpoint)(Primary Endpoint)

Overall SurvivalOverall Survival

Cumulative Incidence of LocoregionalCumulative Incidence of LocoregionalRelapsesRelapses

Cumulative Incidence of Late Adverse EffectsCumulative Incidence of Late Adverse Effects(grade 3 or more)(grade 3 or more)
P = NS

RTOG 9501/Intergroup StudyRTOG 9501/Intergroup Study

RTOG Trial 9501: Study DesignRTOG Trial 9501: Study Design
RR
AA
NN
DD
OO
MM
II
ZZ
EE
SS
TT
RR
AA
TT
II
FF
YY
Age:Age: <70 <70 ≥≥7070
Risk:Risk: micro +margin micro +margin ≥≥2 nodes2 nodesECEECE
RT aloneRT alone
RT/CT RT/CT
CompletelyCompletelyResectedResected
High-RiskHigh-RiskPathologyPathology
RT: 60 Gy/6 weeks, 2 Gy/fx (± 6 Gy RT: 60 Gy/6 weeks, 2 Gy/fx (± 6 Gy ““boostboost””))
Cisplatin: 100 mg/m Cisplatin: 100 mg/m22 IV days 1, 22, & 43 IV days 1, 22, & 43

Locoregional Control RateLocoregional Control Rate(Primary Endpoint)(Primary Endpoint)
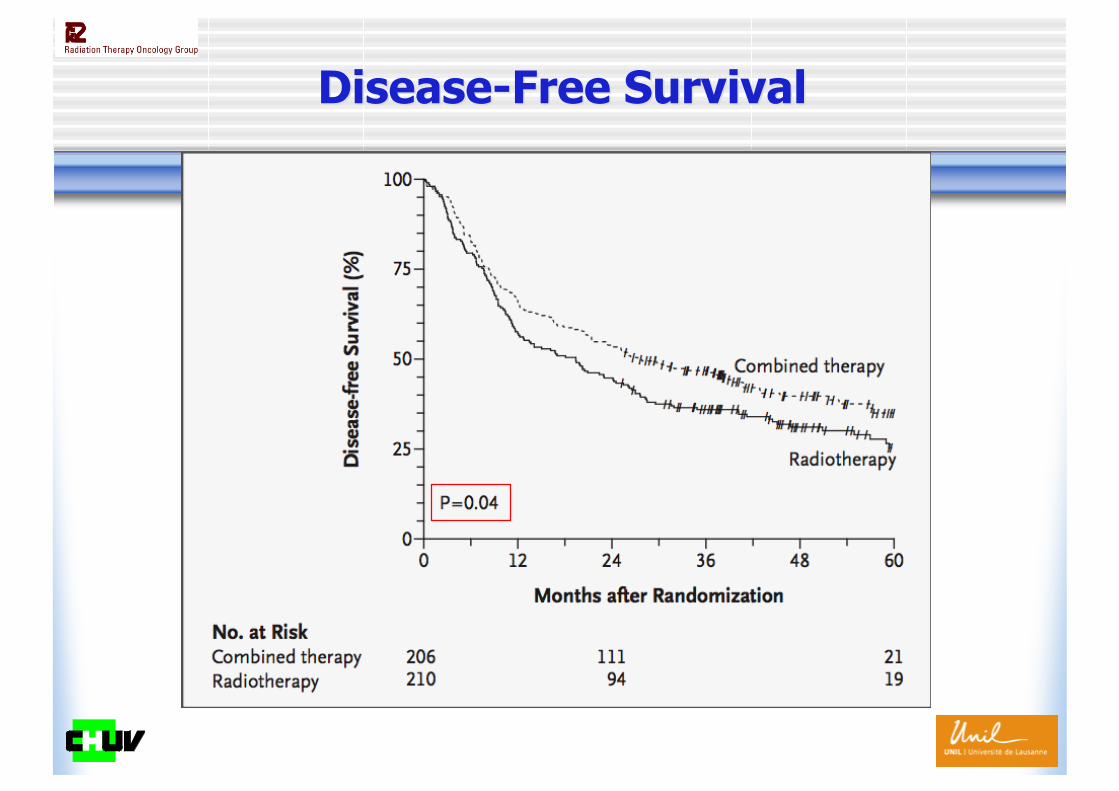
Disease-Free SurvivalDisease-Free Survival

Overall SurvivalOverall Survival
NOT SIGNIFICANT!

Toxicity Summary (RTOG 9501)Toxicity Summary (RTOG 9501)
RTRT RT + CT RT + CTGradeGrade GradeGrade
22 33 44 22 33 44
Acute in-fieldAcute in-field 6565 44 00 77 77 8 8 00 other other --- N/A--- --- N/A--- 87 87 2929 22
LateLate 2929 66 00 28 28 1010 22
Any time*Any time* 8484 1212 00 106106 5050 44
40% 40% 6%6% 0 51% 0 51% 24%24% 2% 2%
*significant difference, p < 0.0001*significant difference, p < 0.0001 N/A = not assessed N/A = not assessed

EORTC andEORTC and
RTOG TrialsRTOG Trials
Are there any differences?Are there any differences?

Meta-Analysis of EORTC 22931 and RTOG 9501Meta-Analysis of EORTC 22931 and RTOG 9501

EORTC EORTC vsvs. RTOG Eligibility. RTOG Eligibility

EORTC EORTC vsvs. RTOG: Differences. RTOG: Differences

Primary EndpointsPrimary Endpoints

Overall SurvivalOverall Survival

Treatment Hazard RatiosTreatment Hazard RatiosLocoregional Control in All PatientsLocoregional Control in All Patients
P = significant
P = significant
P = significant for both

Treatment Hazard RatiosTreatment Hazard RatiosLocoregional Control in SubsetsLocoregional Control in Subsets
P = significant for both
P = NS for both
P = significant
P = significant
P = NS (0.10)
P = NS

Treatment Hazard RatiosTreatment Hazard RatiosDisease-Free Survival in All PatientsDisease-Free Survival in All Patients
P = significant
P = significant
P = significant for both

Treatment Hazard RatiosTreatment Hazard RatiosDisease-Free Survival in SubsetsDisease-Free Survival in Subsets
P = significant for both
P = NS for both
P = significant
P = significant
P = NS
P = NS

Treatment Hazard RatiosTreatment Hazard RatiosOverall Survival in All PatientsOverall Survival in All Patients
P = significant
P = NS
P = significant for both
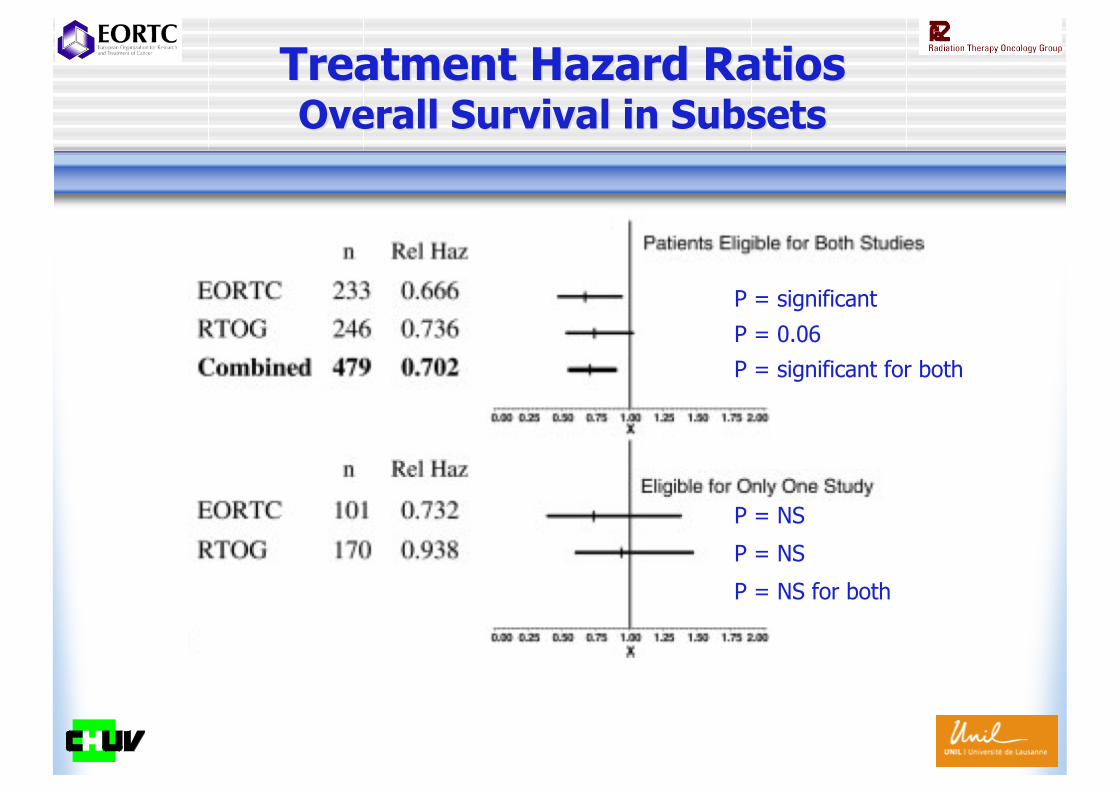
Treatment Hazard RatiosTreatment Hazard RatiosOverall Survival in SubsetsOverall Survival in Subsets
P = significant for both
P = NS for both
P = significant
P = 0.06
P = NS
P = NS

Overall SurvivalOverall SurvivalPatients Patients withwith positive margins and/or ECE positive margins and/or ECE

Overall SurvivalOverall SurvivalPatients Patients withoutwithout positive margins and ECE positive margins and ECE
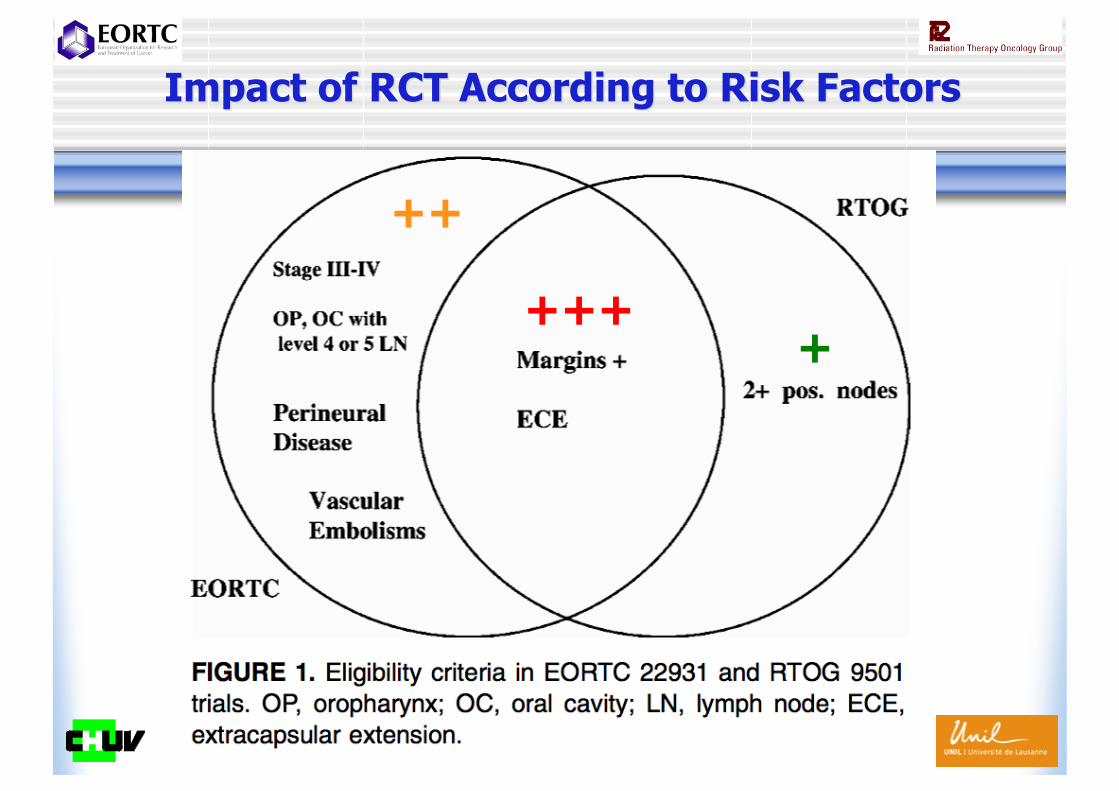
Impact of RCT According to Risk FactorsImpact of RCT According to Risk Factors
+++
++
+

A More Recent Meta-AnalysisA More Recent Meta-Analysis

Meta-Analysis: Four StudiesMeta-Analysis: Four Studies
EORTC 22931 (phase III) Bernier et al NEJM 2004RTOG 9501 (phase III) Cooper et al NEJM 2004Single center trial (phase III) Šmid et al IJROBP 2003Single center trial (phase III) Bachaud et al IJROBP 1996

Meta-Analysis: Winquist et al, H&N 2007Meta-Analysis: Winquist et al, H&N 2007Locoregional Control and Overall SurvivalLocoregional Control and Overall Survival
LOCOREGIONAL CONTROL
OVERALL SURVIVAL

Take Home Message
• Differences in eligibility criteria explain thedifferences in the outcome in the trials
• Postoperative RT/CT is superior to RT alone(Winquist et al, H&N 2007)
• The comparative analysis of EORTC and RTOGtrials supports the routine administration ofcombined RT/CT in patients with +marginsand/or ECE (Bernier et al, H&N 2005)
• Patients without +margins and ECE = ???

Postoperative accelerated RT (PORT) is feasibleCHUV study (phase II) Zouhair et al Radiother Oncol 2004
Accelerated PORT + CT is feasibleCHUV study (phase II) Ozsahin et al Ann Surg Oncol 2008
Accelerated PORT > standard PORTGenoa, Italy (phase III) Sanguineti et al IJROBP 2005Gliwice, Poland (phase III) Suwinski et al Radiother Oncol 2005Cairo, Egypt (phase III) Awwad et al Br J Cancer 2002
PORT + CT > PORTEORTC 22931 (phase III) Bernier et al NEJM 2004RTOG 9501 (phase III) Cooper et al NEJM 2004Metaanalysis Bernier et al Head & Neck 2005Metaanalysis Winquist et al Head & Neck 2007Single center trial (phase III) Šmid et al IJROBP 2003Single center trial (phase III) Bachaud et al IJROBP 1996
FutureAccelerated PORT + CT better than accelerated PORT ?Erbitux ? (RTOG randomized phase II study)Panitumumab ? (EORTC 22071 phase III study)
Current Status of Adjuvant TreatmentsCurrent Status of Adjuvant Treatments

Other Directions: ErbituxOther Directions: ErbituxRTOG 0234 Phase II Randomized TrialRTOG 0234 Phase II Randomized Trial
RRAANNDDOOMMIIZZEE
Arm 1Arm 1
60 Gy / 6 weeks60 Gy / 6 weeks+ weekly ERBITUX+ weekly ERBITUX
+ weekly CDDP + weekly CDDP
Arm 2 Arm 2
+ weekly ERBITUX + weekly ERBITUX 60 Gy / 6 weeks 60 Gy / 6 weeks
+ weekly docetaxel + weekly docetaxel
KPS:KPS:
8080––1001006060––7070
Risk category:Risk category:
Positive marginsPositive marginsHigh risk (High risk (≥≥ 2 positive 2 positivenodes or extranodalnodes or extranodalspread)spread)
RTOG 0234RTOG 0234n = 230n = 230
Stratify by:Stratify by:

Other Directions: IMRTOther Directions: IMRTBetter RT = Less Morbidity ?Better RT = Less Morbidity ?

Is There A Place For Preoperative RT ?Is There A Place For Preoperative RT ?
No Strong Evidence ButPromising Data
Especially For OralCavity Cancer

Thank you for your attention !