adolescent health the adolescent physical karen weiss, pnp, ms, mph february 22, 2010
TRANSCRIPT
Adolescent HealthThe Adolescent Physical
Karen Weiss, PNP, MS, MPH
February 22, 2010

The Adolescent Physical
Three main groups provide screening guidelines for adolescent care:
* GAPS (Guidelines for Adolescent Preventive Services) by the AMA
* Bright Futures – AAP
* US Preventive Services Task Force

How Often Do Teens Need Physicals
Recommendations Differ:
Bright Futures: annual CPEs
GAPS: 3 CPEs during adolescence
• Early adolescence (11-13)
• Mid adolescence (15-17)
• Late adolescence (18-21)

Adolescent Physical Exam
• Height, weight, BP
• Hearing*
• Vision*
• Skin
• Mouth/Teeth
*recommendations differ
Adolescent Physical Exam
• Cardiovascular
• Musculoskeletal
• Breast
• Genitourinary
• Pubertal Maturation
BLOOD PRESSURE
• Systolic and/or diastolic BP > 95th percentile for gender, age and height on 3 occasions
• Refer if lifestyle changes (weight management and exercise) don’t help
HEIGHT, WEIGHT, BMI
RED FLAGS
• BMI 85th – 95th percentile = overweight
• BMI > 95th percentile = obese
• BMI < 5th percentile = underweight
• Significant changes from previous height, weight, BMI curves

Teen Perception of Weight
• Majority of teens not happy with their current weight -- whether or not they actually qualify as overweight!

What is a healthy weight?
• A healthy mind
• Healthy periods if you’re a girl
• Healthy bones
• Healthy heart
• A weight that lets your body do what it is supposed to do and mature the way it’s supposed to mature
What’s not a healthy weight
• What the latest People Magazine says
• What your coach says
• What your boyfriend/girlfriend says
• What your family says
• What the TV ads say
Underweight or Falling Off Curve: DDX
• Eating Disorder
• Gastrointestinal e.g. IBD, celiac
• Endocrine e.g. diabetes, hyper/hypothyroidism
• Malignancy
• Psychiatric e.g. depression, OCD
• Stimulant abuse
Did you know someone in high school or college with an eating disorder (or
suspect)?
Yes N
o
0%0%
1. Yes
2. No 10
Teen Eating Behaviors
• 45% of high school students were trying to lose weight
• 40% of students dieted to lose weight
• 12% of students fasted to lose weight
• 6% of students took diet pills to lose weight
• 4% of students vomited or took laxatives to lose weight
Eating Disorders Epidemiology
• Approximately 1-5% of teenage females have an eating disorder
• Percentage of male teens with eating disorders increasing; estimated at 5-10% of all diagnosed cases occur in males
• Age of onset getting younger
Eating Disorder Mortality
The National Eating Disorders Association estimates that 5-20% of people diagnosed
with anorexia will not survive complications associated with it.
• National Eating Disorders Association, 2006
Eating Disorder Diagnoses
• Anorexia
• Bulimia
• Eating Disorder Not Otherwise Specified (EDNOS)– Female Athlete Triad
DSM IV: Anorexia Nervosa
• Refusal to maintain body weight above the minimally normal ranges for age and height
• Intense fear of becoming fat
• Disturbance in manner in which body shape and weight are experienced
• Absence of 3 consecutive menstrual periods
DSM IV: Bulimia Nervosa
• Recurrent episodes of binge eating associated with lack of control
• Compensatory behavior 2 times a week or more for 3 months
• Self evaluation disproportionately influenced by body weight and shape
DSM IV: EDNOS
• Disorders of eating that don’t specifically meet all the criteria for any specific eating disorder
• Inappropriate behaviors e.g. repeated chewing and spitting out, but not swallowing, large amounts of food
• Binging without the regular compensatory behavior seen in bulimia nervosa
Eating Disorder Risk Factors
• Family history of eating disorder
• Familial relationship with food
• “High risk” sports
• Other illnesses (IBD, IDDM)
• ADHD?
Screening Questions
• How do you feel about your current weight
• How much would you like to weigh
• Do you or anyone else have concerns about your eating or exercise behaviors
• Do you ever fast, vomit, take laxatives or diet pills to control you weight
• LMP
When you suspect an eating disorder
• Rule out other medical illnesses• Full physical exam looking for signs of ED and
complications of malnutrition– Hair loss– Lanugo– Teeth enamel erosion– Sores on knuckles– Dry, yellowish skin– Bradycardia
• Labs
Initial Eating Disorder Labs
• CBC• Electrolytes• LFTs• Magnesium, Ca, Phosphorus• BUN/Creatinine, Albumin• ESR• TSH• FSH/LH/Prolactin• Tox Screen, Urine laxative screen
Complications of Eating Disorders
• Hematologic– Anemia
– Leukopenia
• Gastrointestinal– Constipation
– Esophageal rupture
– Acute pancreatitis
– Malabsorption
– Dental caries
• CNS– Cerebral atrophy– Impaired concentration
• Skeletal– Osteopenia– Pathological fracture
• Dermatologic– Hair loss– Brittle hair, nails
Complications of Eating Disorders
• Cardiovascular– Bradycardia
– Arrhythmias
– Congestive heart failure
• Endocrine– Pubertal delay
– Growth retardation
– Amenorrhea
• Serologic– Electrolyte
disturbances
When You Suspect an Eating Disorder – What next
• The team approach– Medical provider– Psychiatrist– Psychologist/social worker– Nurse– Nutritionist– Parents
SKIN
• Acne
• Striae
• Self inflicted lacerations
• Piercings, tattoos
• Lanugo
• Acanthosis nigricans
Acne
• 80-90% of teens afflicted
• Huge impact on sense of well being
• Teens with acne more likely to be depressed, suffer from low self esteem and withdraw socially compared to teens with clear complexion.

Acne: Etiology
*Androgen stimulation causes increase in sebum production and increase in proprionibacterium acnes (gram positive anaerobe normally found in skin)
* Pores normally lined with epidermal cells. Cells abnormally sticky in teen with acne, follicle more likely to plug
Which of the following is true about acne?
1. A
cne
is w
orsen
ed ..
2. A
cne
is p
art o
f ado...
3. S
tress
can
cau
se ..
4. A
cne
should
be
m...
0% 0%0%0%
1. Acne is worsened by chocolate and fried food
2. Acne is part of adolescence and will go away on its own
3. Stress can cause or worsen acne
4. Acne should be managed by a specialist only
10
Acne: Contributing Factors
• Genetics – teens with XYY genotypes often have severe acne
• Oil based cosmetics
• Stress and emotional factors
• Climate factors

Acne Lesions
• Variety of different lesions - often present in combination
• Check face, chest and back– comedones (black heads, white heads)– papules– pustules– nodules– cysts– scarring
Acne Treatment
• Benzoyl peroxide (2.5%, 5%, 10%) -- the mainstay of treatment
– acts as topical antiseptic and reduces free fatty acids
– Can be combined with topical antibiotic like e-mycin or clindamycin
– Benzoyl peroxide is synergistic with tretinoin (Retin A). Can use one in AM and one in PM
• Tretinoin (Retin A) - increases cell turnover in follicles, expells existing comedones, prevents new lesions
• Topical Antibiotics (erythromycin, clindamycin) - use for patients with inflammatory acne in combination with Benzoyl Peroxide or Retin A
• Systemic Antibiotics (tetracycline, doxycycline, minocycline) - use with topical antibiotic

Acne Treatment
• Hormonal therapy• OCPs now approved to treat acne in female teens• OCPs increase levels of sex hormone binding
globulin leading to decreased free testosterone levels. Also suppress gonadotropin secretion leading to decreased ovarian androgen production
• Choose an OCP that’s primarily estrogenic in effect (e.g. Desogen, Orthocylen or newer Yasmine)
Acne Treatment
• Accutane– Stops sebaceous glands production of sebum for duration
of treatment– Extremely affective for nodulo-cystic acne– Extremely teratogenic– Female teens must get HCG testing and sign contracts
committing to regular BCM use* pulled from market due to concerns re: increased risk of
IBD – Generic still available
* RXED by DERMATOLOGIST ONLY

Acne Treatment
• Takes a minimum of 8-12 weeks to see results
• Bring patient back in 8 weeks for follow up
Striae
• Typically occur due to rapid weight gain• Can occur in pubescent teens experiencing
rapid overall growth• Rarely due to endocrine problem (excess
adrenocortical activity) or potent topical steroid use
• Fade over time; cosmetic derm options available
Lacerations, Piercings, Tattoos
• Watch for allergic dermatitis secondary to dyes, metals and pigments
• Keloid scars
• Gang affiliations
• Self inflicted cuts
MOUTH & TEETH
• Caries• Gingivitis• Enamel erosion from self induced vomiting• Mucosal changes from chewing tobacco• Complications from tongue piercings
– tooth fractures and chipping– gingival injury– increased salivation
CARDIOVASCULAR
• Evaluate athletes for risk of sudden cardiac death (SCD)
Sudden Cardiac Death (SCD)
• Risk for high school and college athletes estimated to be quite low: between 1:200,000-1:300,000 per school year
• Some suggestion that this is underestimated
What findings are likely to indicate risk of SCD in a teen
Hea
rt M
urmur
FHx
of SCD
Hx
ches
t pai
n with
ex.
..
Hx
synco
pe or
nea
r ...
None
of the
abo
ve
All
of the
above
0% 0% 0%0%0%0%
1. Heart Murmur
2. FHx of SCD
3. Hx chest pain with exertion
4. Hx syncope or near syncope with exertion
5. None of the above
6. All of the above
10
SCD Etiology
• Congenital heart disorders most common cause– Hypertrophic Cardiomyopathy (HCM)
responsible for about 1/3 of cases– Other causes include arrhythmias, Marfans
Syndrome and electrical abnormalities e.g. Long QT Syndrome
Hypertrophic Cardiomyopathy
• Thickening of the heart muscle, most commonly at the septum
• Interferes with normal heart functioning by – Narrowing outflow of left ventricle to aorta– Decreases ability of heart to relax and fill with
blood during diastole– Disrupts normal mitral valve action
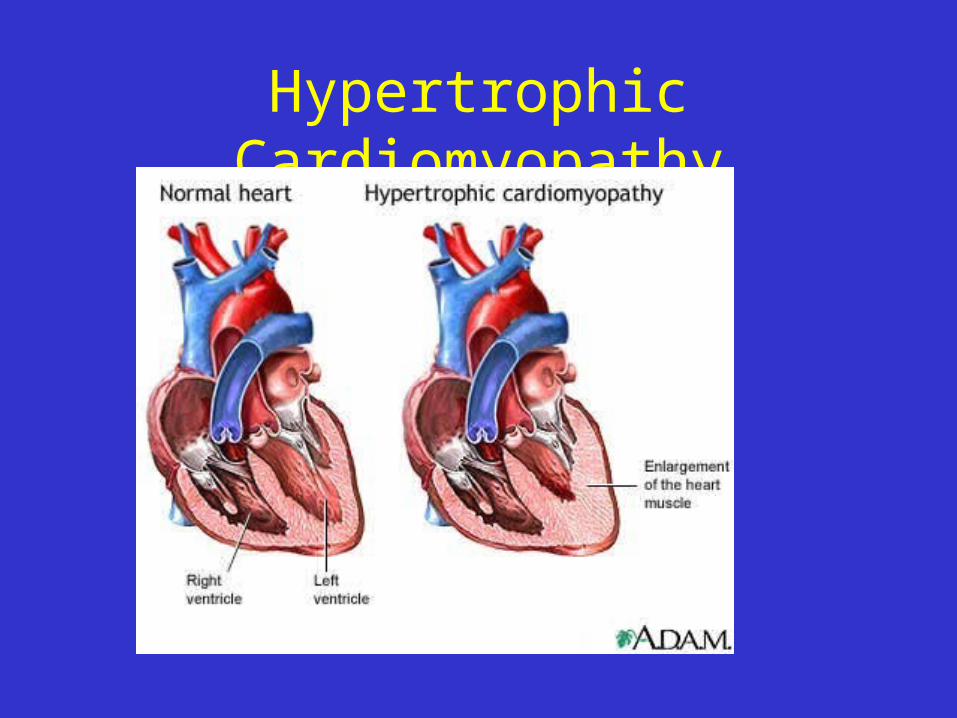
Hypertrophic Cardiomyopathy
Hypertrophic Cardiomyopathy
• Etiology– Genetic: An autosomal dominant disorder
Inheritance is responsible for 60-70% of HCM cases
– Acquired (secondary to high blood pressure, age)
– Unknown– Affects males and females equally
Sudden Cardiac Death Screening Questions
Family history of SCD
History of chest pain with exertion
History of dyspnea with exertion
History of syncope or near syncope
Sudden Cardiac Death Physical
• Heart Murmurs• Femoral pulses• Physical features of Marfans
– Arm span greater than body height– Long lanky frame– Spidery fingers– Chest wall abnormalities– Joint laxity

ECG Yes or No
• Frequently used in parts of Europe• Debate in US regarding cost-effectiveness• One large retrospective analysis in Europe
found that of athletes that died of sudden death, fewer than 1% were accurately diagnosed by physical and history alone. ECG findings abnormal in majority of patients with HCM and cardiac arrythmias.
MUSCULOSKELETAL
• Scoliosis
Scoliosis - Definition
• A lateral curvature of the spine greater than 10 degrees
Scoliosis - Epidemiology
• Usually develops in early adolescence
• Up to 1 in 25 children have some degree of scoliosis (males and females nearly equal)
• Only 4 in 1000 in the US have moderate to severe curves > 20 degrees
• Severe curves 5-7 times more common in females
Scoliosis - Etiology
• Most scoliosis is idiopathic
• Other causes include– congenital – neuromuscular – vertebral disease – spinal cord disease – disease associated
Scoliosis Screening
• Screening should be done at every visit starting in early adolescence
• Screening programs also held at many schools. Tend to pick up a lot of curves less than 10 degrees
Scoliosis Management
Management based on two key factors
1. Degree of curve
2. Teen’s Tanner Stage and whether or not female has achieved menarcheRemember - female’s growth velocity peaks in
the year or so before menarche then slows down considerably
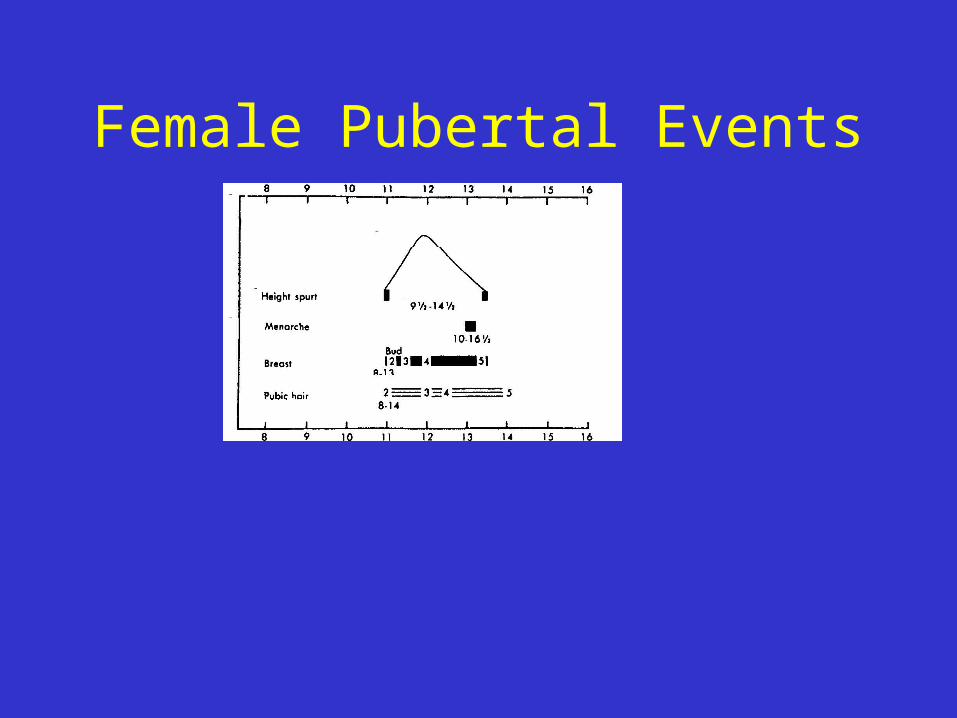
Female Pubertal Events
Scoliosis Management
• Radiographs• Females in early stages of puberty (tanner 1-3)
with curves of 20 degrees or more: refer to an orthopedist
• Tanner 1-3 with a curve of < 20 degrees: recheck and consider another xray in 6 months
• If curve has increased by 3-5 degrees, refer to an orthopedist
Scoliosis Management
• Tanner 4-5 females, past menarche, curves up to 30 degrees unlikely to progress
• Still, consider referral
• Consider xray or referral whenever you’re in doubt
• Scoliometers can be helpful office tools
Scoliosis Management
• BRACING
– Used for patients with progressing curves of 20-45 degrees
– Goal is to stop the progression of the curve until maturity achieved
– Not always effective. Compliance an issue
Scoliosis Management
• Surgery
– Used for curves of 50 degrees or more or for curves of 40-50 degrees in younger patients with significant growth left
• Exercise and OMT
– Traditionally not considered helpful
– Some studies now suggesting otherwise
BREAST
• Asymmetry
• Tuberous breasts
• Masses
• Gynecomastia
• Clinical breast exam begins at age 20
• Self breast exams begin at age 20
Breast Asymmetry
• Common in early stages of development
• Usually resolves with time
• If persists, consider cyst, mass or abscess
• If no pathological etiology, cosmetic surgery can address
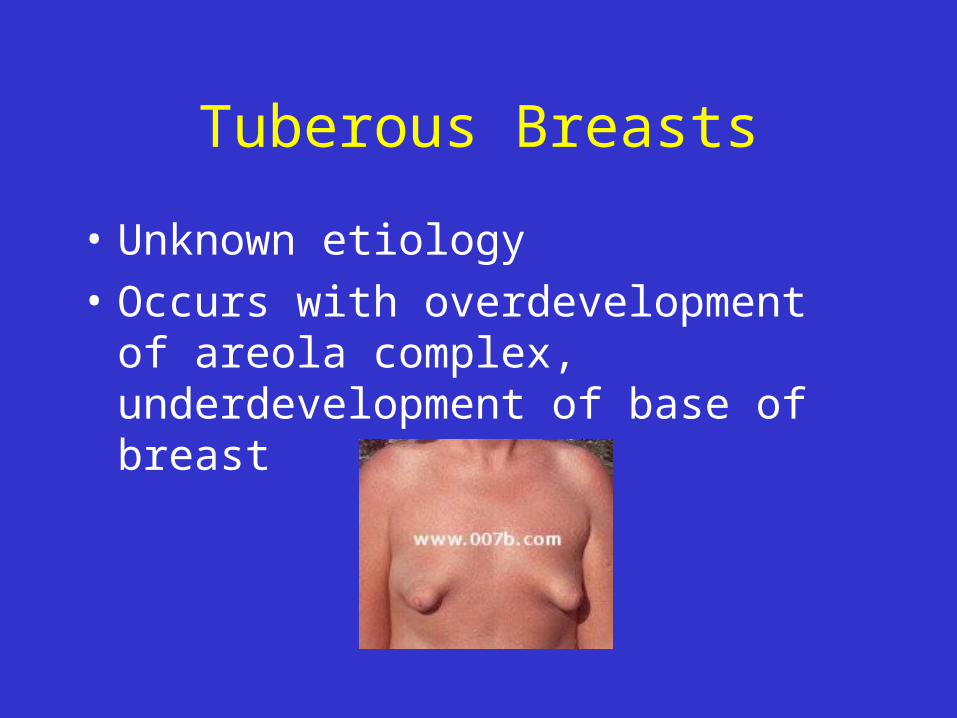
Tuberous Breasts
• Unknown etiology
• Occurs with overdevelopment of areola complex, underdevelopment of base of breast
Breast Masses
Fibroadenomas• Most commonly excised breast mass in teens• Approximately 10-15% occur in multiples• Rubbery, firm mobile masses. May last for
months - usually resolve on their own• Consider surgical removal for masses 2-4
cms or larger• Considered benign
Breast Masses
• Fibrocystic breast changes– Cord like thickenings and lumps, often tender before
menses (possibly due to estrogen/progesterone imbalance)
– Benign
• Breast Cysts– Common in teens, usually resolve within a few months
• Breast Cancer Rare in Teens
Gynecomastia
• An increase in breast tissue in males caused by imbalance between estrogen and androgen activity
• Vast majority related to puberty, considered benign, will resolve spontaneously
• Must rule out other less common causes
Gynecomastia - Other causes
• Obesity (Pseudo-gynecomastia)
• Drugs (Marijuana, cimetidine, digoxin)
• Testicular tumors
• Adrenal tumors
• Hyperthyroidism
• Liver disease
• Renal failure
• Androgen insensitivity
• Breast Masses
• Hyperprolactinemia
• Primary hypogonadism: e.g. Klinefelter syndrome (XXY)
• True hermaphroditism
Pubertal Gynecomastia
Pubertal peaks during genital stage 2-3 (age 13-14 years) and typically resolves within 1-2 years
Pubertal Gynecomastia - Diagnosis
• Careful history to rule out drugs or systemic illness
• Physical exam focusing on gonads, thyroid, signs of liver or renal disease
• Breast development typically bilateral • Breast exam:
– Palpate for masses– Palpate to determine whether tissue is breast tissue or
fatty tissue
Pubertal Gynecomastia
• Breast tissue feels rubbery, firm and freely movable
• Tissue is evenly distributed around areola
Gynecomastia - Management
• Observation ok assuming meets criteria for normal pubertal gynecomastia
• If secondary to drug use, need to address
• If etiology not obvious, further lab testing warranted– LH, Serum Testosterone, HCG, Estradiol

GU - MALE
• Sexual Maturity Rating
• Testicular volume (Tanner Staging)
• Testicular masses
• Hernia
• Varicocele
• Penile discharge

GU-Female
• Assess external anatomy and public hair
• Most practitioners stop once teen has had menarche unless teen sexually active or has specific complaints
• Once teen sexually active, exam based on concerns and complaints
PUBERTY
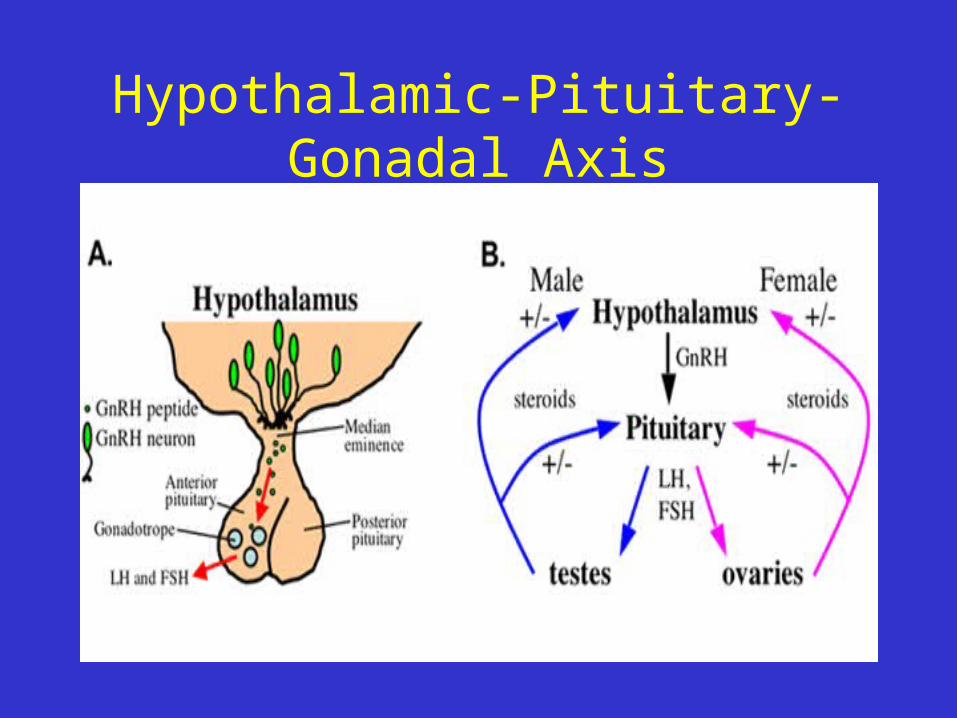
Hypothalamic-Pituitary-Gonadal Axis

Hypothalamic-Pituitary-Gonadal Axis
• Well developed at time of birth
• Hypothalamic-Pituitary-Gonadal axis is downregulated during prepubertal years
• Decreased amplitude and frequency of GnRH pulses; decreased pituitary responsiveness to GnRH stimulation

Pubertal Maturation
• Significant increase in GnRH secretion, increase in pituitary responsiveness and increased secretion of LH and FSH
• Increased LH and FSH stimulate increased release of sex hormones (estrogen, testosterone) from gonads
• Unclear what exactly triggers puberty; thought to be based on multiple factors including
– Hormone Leptin (hormone produced in adipocytes)
– GPR54 Gene: affects GnRH

Delayed Puberty
• Delay in the age of onset of puberty or delay in the rate of progression of pubertal development
Male Pubertal Delay
• Genital Stage 1 (testes less than or equal to 2.5 cms) persists past 13.7 years
• Pubic Hair Stage 1 persists past 15.1 yrs
• Greater than 5 years pass before completion of genital growth
• Pubertal progression begins but then progress stalls

orchidometers
Female Pubertal Delay
• Breast stage 1 persists past 13.4 yrs
• No menarche by age 15 yrs
• Greater than 5 years have passed between onset of breast development (Tanner II) and menarche
• Pubertal progression begins but then progress stalls
Etiology of Pubertal Delay
Constitutional Delay vs. Pathophysiological
Constitutional Delay
• Late onset of puberty as a normal variant• Patients grow slowly through childhood, enter
puberty late then progress through at a normal rate• Thought to be caused by persistence of
prepubertal hypogonadotropic state• Responsible for 90-95% of diagnosed pubertal
delay• Often strong family history of constitutional delay
Pathophysiologic Delay
Where is the failure?
The hypothalamic-pituitary axis or the gonads (either not working well or missing)
Pathophysiologic Delay
Congenital– Turners Syndrome (45,XO or 45 XO/46,XX karyotype)
• Affects about 1 out of 2,500 females
• Short stature, webbed neck, low hairline at back of neck, broad chest with widely spaced nipples
• Ovaries are absent or underdeveloped
• Mild mental retardation
• Bone age normal or delayed
Pathophysiologic Delay
• Chronic diseases– Inflammatory bowel
disease– Hyper/hypothyroidism– Diabetes mellitis
• Immunologic– Juvenile rheumatoid
arthritis– Systemic lupus
erythematosus
• Tumors
– Pituitary adenoma
– Astrocytoma
– Hypothalamic glioma
• Psychosocial
– Anorexia
• Environmental
– Postradiation
– Chemotherapy
Delayed Puberty Exam
• Full PE with special attention to:– Breast and genital exam– Thyroid– Neurologic and Fundoscopic
• r/o intracranial mass
Delayed Puberty Labs
• Routine Labs (CBC, ESR, Chem profile)• UA• Thyroid function*• Gonadotropin levels (LH, FSH)*
– Low levels suggest prepubertal or hypothalamic-pituitary failure
– High levels suggest gonadal failure or absence
• Karyotype*• Growth hormone levels*
* order based on physical findings
Delayed Puberty Imaging
• Bone age– Can help differentiate constitutional delay from organic
disorders
– Bone age delayed in constitutional delay, hypothyroidism and chronic illness
• Pelvic Ultrasound• CT or MRI of head
– Assess pituitary and hypothalamus
– Assess for masses or lesions
Delayed Puberty Treatment
• Constitutional Delay– Reassurance– Occasionally drug therapy warranted
• Pathophysiological delay– Refer to endocrinologist
Amenorrhea
• Average age of menarche 12.5 years old
• Range anywhere from 9 to 16 years of age
• Usually earlier in African American teens
Primary Amenorrhea
• Primary Amenorrhea– No menarche by 16– Concern if 2-3 yrs past thelarche (breast
budding) or if patient is Tanner 5– Should be no more than 4 years between
Tanner 2 and menarche
• Secondary Amenorrhea– No menses for 6 months or no menses for the
length of time equal to 3 normal cycles
Causes of Secondary Amenorrhea
• Pregnancy
• Immature hypothalamic-pituitary-gonadal axis
• Thyroid problems
• Polycystic ovarian syndrome
• Female athlete triad
It is normal and expected for female athletes to have amenorrhea for extended periods of
time
Tru
e
Fal
se
0%0%
1. True
2. False10
Female Athlete Triad
• Combination of amenorrhea, osteoporosis and disordered eating
• Amenorrhea may be one of the first signs• Highest risk athletes: gymnasts, ballet
dancers, figure skaters• Strenuous exercise and weight loss suppress
the hypothalamic-pituitary axis and can cause amenorrhea
Screening for the Female Athlete Triad
• Diet History• Menstrual history• Exercise History
– Exercise patterns (hours per day, days per week)
– Additional exercise outside of required training– History of previous fractures– History of previous overuse injuries
Female Athlete Triad Diagnosis
• A diagnosis of exclusion.
• Not a clinical diagnosis or one that can be made by lab testing.
• A thorough history and PE to rule out other causes of amenorrhea must be conducted
Treatment for the Female Athlete Triad
Focus on adequate nutrition
• Healthy exercise options
• Hormone Replacement Therapy (HRT)– No published studies support or refute benefits
of HRT on bone mineral density– Consider using after 6 months of amenorrhea– OCP use may decrease risk of stress factors
Amenorrhea is not normal in the female athlete!
In Summary
• The teen years are essentially healthy ones• Most morbidity and mortality in teens is
preventable• Teens want to talk with their health care provider• An assurance of confidentiality (with caveats) is
key for effective communication• The HEEADS screen is an excellent tool• A comfortable interviewing style will increase
disclosure and facilitate effective interventions
